Embed Size (px)
Citation preview

The PDF of the article you requested follows this cover page.
This is an enhanced PDF from The Journal of Bone and Joint Surgery
1989;71:1548-1555. J Bone Joint Surg Am.SD Boden, PA Labropoulos, P McCowin, WF Lestini and SR Hurwitz
Mechanical considerations for the syndesmosis screw. A cadaver study
This information is current as of January 22, 2009
Reprints and Permissions
Permissions] link. and click on the [Reprints andjbjs.orgarticle, or locate the article citation on
to use material from thisorder reprints or request permissionClick here to
Publisher Information
www.jbjs.org20 Pickering Street, Needham, MA 02492-3157The Journal of Bone and Joint Surgery

1548 B. K. VAUGHN ET AL.
ThE JOURNAL OF BONE AND JOINT SURGERY
28. STULBERG, B. N. ; INSALL, J. N. ; WILLIAMS, G. W. ; and GHELMAN, BERNARD: Deep-Vein Thrombosis following Total Knee Replacement. AnAnalysis of Six Hundred and Thirty-eight Arthroplasties. J. Bone and Joint Surg. , 66-A: 194-201, Feb. 1984.
29. WHEELER, H. B. : Diagnosis of Deep Vein Thrombosis. Review of Clinical Evaluation and Impedance Plethysmography. Am. J. Surg. , 150(4A):7-13, 1985.
30. WINGERD, MAX; BERNHARD, V. M.; MADDISON, FRANK; and TOWNE, J. B.: Comparison of Caval Filters in the Management of VenousThromboembolism. Arch. Surg., 113: 1264-1271, 1978.
31 . WOOLSON, S. T. , and HARRIS, W. H.: Greenfield Vena Caval Filter for Management of Selected Cases of Venous Thromboembolic Diseasefollowing Hip Surgery. A Report of Five Cases. Clin. Orthop. , 204: 201-206, 1986.
Copyright 1989 by The Journal of Bone and Join: Surger, Incorporated
Mechanical Considerations for the Syndesmosis Screw
A CADAVER STUDY*t
BY SCOTT D. BODEN, M.D4, PANOS A. LABROPOULOS, M.D4, PHILIP MCCOWIN, M.D.1,
WILLIAM F. LESTINI, M.D4, AND SHEPARD R. HURWITZ, M.D4, WASHINGTON, D.C.
From the Department of Orthopaedic Surgery, George Washington University School of Medicine, Washington
ABSTRACT: The purpose of this study was to ex-amine the mechanical necessity of using a syndesmosisscrew to supplement rigid internal fixation of the fibulaand medial malleolus in the treatment of pronation-ex-ternal rotation fractures. The legs of thirty embalmedand five fresh cadavera were dissected and mountedthrough the tibia to a frame so that multiple radiographscould be made with a constant relationship between thespecimen and the x-ray apparatus A standardized pro-nation-external rotation load was applied to the foot,
and widening of the syndesmosis was studied on mortiseradiographs that were made after each experimentalstep.
On the basis of previous investigations, we devel-o_ a model for pronation-external rotation injuriesthat included disruption of the syndesmosis and inter-osseous membrane up to the level of the fibular fracture.Accordingly, multiple repaired fibular fractures couldbe simulated at several levels in the same specimen byincremental proximal division of the interosseous mem-brane. Specimens were separated into two groups.Group I consisted of thirteen specimens in which thedeltoid ligament, syndesmosis, and interosseous mem-brane were serially sectioned in 1.5-centimeter incre-ments. Group II (ten sections) was subjected to the sameprotocol, except that the deltoid ligament was kept intact
until the final step. The five fresh specimens were sec-
* No benefits in any form have been received or will be received from
a commercial party related directly or indirectly to the subject ofthis article.
No funds were received in support of this study.t Read in part at the Annual Meeting of The American Academy of
Orthopaedic Surgeons, Las Vegas, Nevada, February 1 1 , 1989.� Department of Orthopedic Surgery, 2150 Pennsylvania Avenue,
NW. , Washington, D.C. 20037. Please address requests for reprints toDr. Boden.
tioned in the same way as those in Group I.In Group I, since the simulated pronation-external
rotation injury included a deltoid tear, rigid medial fix-ation was not possible; accordingly, there was rigid fib-ular fixation only. In this group, the mean widening ofthe syndesmosis increased only gradually from 0.5 to 4.5millimeters as the level of fibular fracture rose from 1.5to fifteen centimeters proximal to the ankle. Measure-ments for the five fresh specimens were consistent withthose for the embalmed legs. In Group II, the pronation-external rotation injury was simulated with a medialmalleolar fracture rather than a deltoid tear. After sim-ulated rigid fixation of both the medial malleolus andthe fibula, only minimum widening of the syndesmosis(1.4 ± 03 millimeters) occurred, even when the fibularfracture was fifteen centimeters proximal to the ankle.The mean maximum widening of the syndesmosis inGroup II, in which division of the deltoid ligament was
the last step, was equivalent to that in Group I, vali-dating comparison of the two groups.
CLINICAL RELEVANCE: Considering the range ofclinically acceptable widening of the syndesmosis, thecritical transition zone for the level of a fibular fracturethat is fixed with a plate is three to 4.5 centimeters prox-imal to the ankle. When the fibular fracture is proximalto this level and rigid medial fixation is not possible, thesyndesmosis may have to be stabilized to supplement thefixation with the plate. However, rigid medial and lateralfixation should acceptably stabilize the syndesmosiswithout further additional supplementation. This studyprovides mechanical evidence that internal fixation ofpronation-external rotation injuries that include disrup-tion of the syndesmosis often does not need to be sup-plemented with trans-syndesmotic fixation.

r�1“l “
‘V
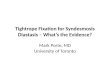
FIG. 1-A
MECHANICAL CONSIDERATIONS FOR THE SYNDESMOSIS SCREW 1549
VOL. 71-A, NO. 10, DECEMBER 1989
The need for trans-syndesmotic stabilization of the dis-
tal tibiofibularjoint after pronation-extemal rotation injuries
is controversial. Although the syndesmosis screw is used
after distal tibiofibular disruption, there are few guidelines
for use of the screw to treat specific fracture configurations.
Many authors have reported using the syndesmosis screw
for repair of most pronation-external rotation injuries�”930.
Others have claimed that such additional fixation is rarely
indicated2”2. Some authors have relied on intraoperative
assessment of instability of the syndesmosis”’617.
The syndesmosis screw is effective in stabilizing the
tibiofibularjoint to allow ligamentous healing, but a separate
procedure may be necessary to remove the screw, weight-
bearing is often delayed postoperatively, and the procedure
is not without complications4”’516’2733. Criteria for more
efficient use of the syndesmosis screw would be beneficial.
The purpose of this study was to determine the mechanical
necessity of use of a syndesmosis screw to supplement rigid
internal fixation of the fibula and medial malleolus in the
treatment of fractures that were produced by pronation and
external rotation. This task was undertaken with the hy-
pothesis that the syndesmosis screw may currently be over-
used.
We hypothesized that the anatomical configuration of
the uninjured soft tissues at the site of any pronation-external
rotation injury provides acceptable stability for the syndes-
mosis after rigid fixation of the fibula and the medial mab-
leolus without trans-syndesmotic fixation. Disruption of soft
tissue often plays a vital role in decreasing the stability of
a fracture24. Few anatomical studies have dealt with the
contribution of soft-tissue stabilization in pronation-external
rotation injuries of the ankle. In this type of injury, the
deltoid ligament or medial malleolus and the syndesmosis
are usually disrupted. However, the bevel of disruption of
the interosseous membrane is variable and is rebated to the
level of the fibular fracture. Although the physiological role
of the interosseous membrane is controversiaV4’262829, it has
been shown to be an important stabilizer of the ankle in the
absence of the deltoid ligament and the syndesmosis32’.
As far as we know, in the anatomical studies in which
the role ofthe interosseous membrane has been investigated,
the authors have treated it as a single structure and sectioned
it in its entirety3’22. We know of no study in which the effect
of sequentially sectioning the interosseous membrane after
disruption of the deltoid ligament and syndesmosis has been
examined. Such an experiment would help to determine the
contribution of the intact soft tissues in pronation-externab
rotation injuries that result in fibular fracture at various
levels. Accordingly, the experimental protocol was designed
to determine the maximum diastasis of the syndesmosis
possible for various configurations of pronation-external ro-
tation fractures that were treated without supplementing the
fibular and medial mableobar fixation with a syndesmosis
screw.
Materials and Methods
The begs of thirty embalmed and five fresh cadavera
were dissected to expose the deltoid ligament, the antero-
medial part of the joint capsule, the syndesmosis, and the
distal fifteen centimeters of the interosseous membrane.
Each specimen was mounted by bolting the tibia to a wooden
frame in 15 to 20 degrees of internal rotation. Multiple
*
Experimental configuration depicting a specimen mounted through the tibia to a wooden jig. Shown above is a stationary x-ray apparatus, whichenabled generation of reproducible mortise radiographs after each experimental step. The interosseous membrane and syndesmosis were exposed, anda 440-newton pronation-external rotation load was applied through the ankle via the distal lateral corner of the foot-plate (asterisk).

z
1550 S. D. BODEN ET AL.
ThE JOURNAL OF BONE AND JOINT SURGERY
radiographs were made, with a constant relationship be-
tween the specimen and the x-ray apparatus (Fig. 1-A). A
foot-plate was bolted to the foot and was loaded through a
rope-and-pulley system. A uniform pronation-external ro-
tation load of 440 newtons was applied at the distal lateral
corner of the foot-plate. When the frame and the pulley
system were designed, the direction of the pronation-exter-
nab rotation force was empirically chosen to produce max-
imum widening of the syndesmosis during preliminary
testing of specimens in which the interosseous membrane
had been sectioned to six centimeters proximal to the ankle.
The direction of the loading force was constant for all
specimens. In addition, the moments that were imposed on
the ankle were equal for all specimens, due to constant
placement of the center of rotation of the ankle relative to
FIG. 1-B
A 440-newton load was applied to the distal lateral corner of the foot-plate (asterisk) at angle r from the longitudinal axis (y) of the leg. Themoments that were imposed on the ankle were equal for all specimens,due to the standardized positioning of the center of rotation of the ankle(#{174})with respect to the point of loading on the foot-plate, which generatedthe same moment-arm in each specimen. The applied force (F) can beseparated into its components along the x axis (Fx) and y axis (Fy); theforce was perpendicular to the z axis, so that Fz = 0. The moments inthe various anatomical planes can be calculated from the moment-arm andthe component of the force perpendicular to the particular axis of rotation.(1) The dorsiflexion moment (rotation about the x axis) is the result of Fyapplied over moment-arm b. (2) The pronation moment (rotation about thez axis) is the result of Fy applied over moment-arm a. (3) The externalrotation moment (rotation about the y axis) is the result of Fx applied overmoment-arm b. r = 20 degrees, F = 440 newtons, a = eight centimeters,and b = twenty-four centimeters.
the foot-plate and to the point of origin of the load (Fig. 1-
B). Mortise radiographs were made, and the width of thesyndesmosis was measured one centimeter proximal to the
joint line, from the incisura to the medial part of the fibular
cortex (Fig. 2). The reproducibility of the measurements of
the syndesmosis was assessed by a paired t-test comparison
of determinations of baseline width as measured by two
observers on the thirty specimens.
Fracture Model
We developed a model for pronation-external rotation
injuries on the basis of the observations of Lauge-Hansen’
and others7 that the syndesmosis and interosseous membrane
are disrupted proximally up to the level of the fibubar frac-
ture. For a series of pronation-external rotation soft-tissue
injuries of different patterns, we studied the widening of
the syndesmosis, in response to loading of the ankle, before
and after osteotomy and rigid fixation of the bone (Fig. 3).
If widening of the syndesmosis under load were equal in
both situations, the model would allow simulation of rigidly
fixed fibular fractures at multiple levels in the same speci-
men, simply by creating the corresponding soft-tissue in-
jury. By obviating the necessity of breaking the bone and
x fixing it with a plate, the model enabled simulation of mul-
tiple repaired fractures at intervals along the fibula in each
specimen, which also could serve as its own control for
baseline width of the syndesmosis. Accordingly, by cab-
culating incremental widening of the syndesmosis over the
baseline width in each ankle, data from multiple specimens
could be pooled without being affected by the natural var-
iations in baseline width.
Since 30 to 60 per cent of pronation-externab rotation
injuries involve a deltoid tear rather than a medial malleolar
fracture9 I I two experimental groups were designed to study
residual instability of the syndesmosis after internal fixation
of both types of medial injury. In Group I, pronation-ex-
ternal rotation injury with a deltoid tear as the medial com-
ponent was simulated by sectioning the deltoid ligament
first. In Group II, pronation-externab rotation injury with a
repaired fracture of the medial mableolus was simulated and
the deltoid complex was left intact.
x For each of the first seven embalmed specimens, abaseline mortise radiograph was made with the specimen
under load. The medial malleolus was osteotomized at the
level of the joint and was fixed with two 4.5-millimeter
malleobar screws. Then another mortise radiograph was
made, with the specimen under load, and widening of the
syndesmosis compared with the baseline was calculated.
Next the deltoid ligament, the anteromedial aspect of the
joint capsule, and the syndesmosis were cut. The interos-
seous membrane of each specimen was cut at 1 .5, 3.5, 5.5,
7.5, 10.0, 12.5, or 15.0 centimeters proximal to the ankle.
Again, radiographs were made of the loaded specimen.
Next, the fibula was osteotomized at the most proximal
bevel of the section of the interosseous membrane and was
repaired with a six-hole compression plate and cortical
screws. Another mortise radiograph was made, with the

FIG. 2
The width of the syndesmosis (horizontal black line) was measured from the incisura (vertical black line) to the medial part of the fibular cortex onmortise radiographs, as demonstrated on a baseline specimen (left) and a specimen after the sectioning protocol was completed (right).
FIG. 3
MECHANICAL CONSIDERATIONS FOR THE SYNDESMOSIS SCREW 1551
VOL. 71-A, NO. 10, DECEMBER 1989
In a series of pronation-external rotation soft-tissue injuries of different patterns, the width of the syndesmosis was compared before and afterosteotomy and rigid fixation of the bone. The width of the syndesmosis was equal before medial malleolar osteotomy and fixation (A) and afterward(B). After section of the deltoid ligament, the anteromedial part of the joint capsule, the syndesmosis, and the interosseous membrane, the width ofthe syndesmosis was equal before fibular osteotomy and rigid fixation (C) and afterward (D). These observations helped to generate a model thatsimulated rigid fixation of fibular fractures at multiple levels in the same specimen, simply by creating the corresponding soft-tissue injury. By obviatingthe necessity of breaking and fixing the same bone with a plate at 1 .5-centimeter intervals, the model enabled each specimen to serve as its own controlfor the baseline width of the syndesmosis. Accordingly, data from multiple specimens could be pooled and compared with regard to incrementalwidening of the syndesmosis compared with the baseline of that particular leg, thereby minimizing the effect of interspecimen variability.

A
FIG. 4
The thirteen specimens in Group I were sequentially sectioned and the width of the syndesmosis was measured under load after each step. A . intactspecimen; B, division of the deltoid ligament, the anteromedial part of the capsule, and the syndesmosis; and C, D, and E, incremental division of theinterosseous membrane from 1 .5 to fifteen centimeters proximal to the ankle.
EE
z--az�Wa,
c1)�(1)0)
C,)W
z>-Co
U,z-JU,U)
WV) O� �E E
�2 � �1x �UJ�_ -JO ��u) � �2 2� �O
z 0>- -U)
E
U
0
0
EU
0
(0
0
0
E
0
0
EU0
0)
0
0
EU
�00
0
0
E
0
0
0
EU(1)C.)
0
0
E8a,0
0
On.
00
1552 S. D. BODEN ET AL.
THE JOURNAL OF BONE AND JOINT SURGERY
specimen under load, and the widening of the syndesmosis
was compared with that before osteotomy and fixation.
In addition, the five fresh specimens were used to de-
termine the sensitivity of widening of the syndesmosis to
variations in load by making measurements with loads of
1 10, 220, 330, and 440 newtons.
The remaining embalmed specimens were separated
into two groups to study instability of the syndesmosis as
a function of disruption of the syndesmosis and the inter-
osseous membrane.
Group I: In the thirteen specimens in Group I, the
deltoid ligament and anteromedial part of the capsule, the
STRUCTURES SECTIONED (LEVEL OF FIBULAR FRACTURE)
A = Group I : RIGID FIBULAR FIXATION, DELTOID TEAR (N = 13)
A = GROUP II : RIGID FIBULAR AND MEDIAL MALLEOLAR FIXATION (N = 10)
::�. SHADED BAND REPRESENTS PUBLISHED RANGE OF CLINICALLYS:::.ACCEPTABLE SYNDESMOSIS WIDENINGIOM = INTEROSSEOUS MEMBRANE LEVEL ABOVE THE ANKLE JOINT
FIG. 5
Widening of the syndesmosis after fixation of simulated pronation-external rotation fractures. The shaded band represents the clinically acceptablerange of widening of the syndesmosis. In Group 1 (open triangles), the range is no longer acceptable for a fibular fracture that is more than 3.0 to 4.5centimeters proximal to the joint. In Group II (solid triangles), the range remains clinically acceptable for fibular fractures that are fifteen centimetersproximal to the joint. However, after the deltoid ligament is sectioned, the maximum widening is equivalent to that in Group I.

MECHANICAL CONSIDERATIONS FOR THE SYNDESMOSIS SCREW 1553
VOL. 71-A, NO. 10, DECEMBER 1989
syndesmosis, and the interosseous membrane were sequen-
tially sectioned in 1 .5-centimeter increments (Fig. 4). The
width of the syndesmosis was measured on mortise radio-
graphs, with the specimen under load, that were made before
sectioning and after each experimental step, as was already
described. Widening of the syndesmosis was calculated as
the increase in the width of the syndesmosis compared with
the baseline measurement for the individual specimen. Five
fresh specimens were sectioned in the same way to assess
the effects of embalming on the experimental results.
Group II: The ten specimens in Group II were sectioned
according to the same protocol as was used for the specimens
in Group I, except that the deltoid ligament and anteromedial
part of the capsule were left intact. As a final step, however,
the medial structures were divided to measure the maximum
widening of the syndesmosis for comparison with Group I.
Results
In the thirty embalmed specimens, one observer de-
termined the baseline width of the syndesmosis to be 3.2
± 0.2 millimeters (mean and standard deviation). A second
observer determined the mean baseline width to be 3 . 1 ±
0.2 millimeters, and the interobserver variation was not
significant (p = 0.4). Measurement of the first seven em-
balmed specimens demonstrated that, in this pronation-ex-
ternal rotation injury model, widening of the syndesmosis
under load was equal for intact bone and for that treated
with an osteotomy and fixation with a compression plate.
Therefore, fibular fractures that had been fixed with a plate
at multiple levels in the same specimen were simulated by
incremental proximal division of the interosseous mem-
brane. Similarly, fixation of medial malleolar fractures was
accurately simulated by the unbroken malleolus. In the five
fresh specimens, widening of the syndesmosis was not af-
fected by varying the loading force from 1 10 to 440 new-
tons.
For the Group-I specimens, in which the deltoid big-
ament and anteromedial part of the capsule had been di-
vided, the mean widening of the syndesmosis with appli-
cation of load increased gradually from 0.5 to 4.5 milli-
meters as the level of disruption of the interosseous mem-
brane increased from 1 .5 to fifteen centimeters proximal to
the ankle (Fig. 5). The largest increase was from 1 .0 to 1.7
millimeters of widening, which occurred when the level of
the simulated fracture was moved from 3.0 to 4.5 centi-
meters proximal to the ankle. The mean amount of widening
of the syndesmosis for the fresh specimens was not signif-
icantly different from that for the embalmed specimens (p
= 0.66).
In Group II, the simulated pronation-externab rotation
injury included a medial malbeobar fracture rather than a
deltoid tear. When the medial malleobus and fibula were
intact, only minimum widening of the syndesmosis (1 .4 ±
0.3 millimeters) was possible under load, even when the
interosseous membrane was disrupted to fifteen centimeters
proximal to the ankle (Fig. 5). However, when the last step,
division of the deltoid ligament, was carried out, the mean
maximum widening of the syndesmosis in Group II was not
significantly different from that in Group I (p = 0.5).
Discussion
Pronation-external rotation injuries of the ankle com-
prise 13 to 45 per cent of malleobar fractures”69’3’9’23. Ac-
cording to Lauge-Hansen’s classification, these injuries
occur in four sequential stages: medial malbeolar fracture or
deltoid tear (Stage 1), anterior disruption of the syndesmosis
and interosseous membrane (Stage 2), fibular fracture (Stage
3), and posterior disruption of the syndesmosis (Stage 4)8.32#{149}
Pronation-external rotation fractures correspond to Type-C
fractures in the Danis-Weber classification, in which the
injury is labeled according to the relationship of the level
of the fibular fracture with respect to the syndesmosis’2”7.
The recent literature has emphasized the importance of
anatomical repair of the lateral malleolus in fractures of the
ankle31. Ramsey and Hamilton demonstrated that a one-
millimeter lateral displacement of the talus results in a 42
per cent reduction in tibiotalar contact20. Since most pro-
nation-external rotation injuries are associated with rupture
of the syndesmosis and interosseous membrane”32, many
surgeons supplement rigid fixation of the fibula and medial
mableolus with some type of trans-syndesmotic fixation5’33.
Although the syndesmosis screw is often employed, the few
published guidelines for its use have been vague and
21.12.19.30
To avoid unnecessary use of the syndesmosis screw,
it must be demonstrated that acceptable stability of the syn-
desmosis can be achieved without trans-syndesmotic fixa-
tion in certain situations. In our study in cadavera, disruption
of the syndesmosis and interosseous membrane resulted in
minimum widening ofthe syndesmosis, provided the deltoid
complex was intact. Accordingly, in this situation, rigid
fixation of the fibula and medial malleolus should restore
adequate stability to the syndesmosis without trans-syndes-
motic fixation. In contrast, when the deltoid complex was
disrupted, widening of the syndesmosis was greater and was
directly related to the amount of disruption of the interos-
seous membrane and, therefore, to the level ofthe pronation-
external rotation fracture of the fibula.
Discussion of these results in any clinical context must
include consideration of the potential inaccuracies of the
experimental design and the fracture model. Although frac-
tures of the ankle are generally protected in a cast after
internal fixation, this model tested the stability of an un-
protected syndesmosis. In addition, the simulated pronation-
external rotation injuries involved disruption of all ligaments
in the syndesmosis, corresponding to a Stage-4 Lauge-Han-
sen injury. Actually, after a pronation-external rotation in-
jury in which the posterior syndesmosis remains intact
(Stage 3), the syndesmosis may be more stable than is in-
dicated by this model.
Although most of the experimental data were generated
from embalmed specimens, the measurements were con-
sistent with those generated from fresh tissue. The results
from Group II (in which the deltoid ligament was intact)

1554 S. D. BODEN ET AL.
ThE JOURNAL OF BONE AND JOINT SURGERY
were consistent with reported observations from studies on
fresh cadavera3. The results from the embalmed specimens
in Group I (in which the deltoid ligament was divided) were
consistent with published observations3’22 and, more im-
portantly, were not significantly different from our own
measurements in five fresh specimens.
In addition to the potential inaccuracies of our model
resulting from the variable severity of the pronation-external
rotation injuries and the use of embalmed specimens, the
fact that we studied experimental rather than physiological
loading ofthe structures in the ankle deserves consideration.
Preliminary testing, confirmed in the five fresh specimens,
demonstrated that widening of the syndesmosis was rela-
tively insensitive to loading. Accordingly, the loading force
was selected to produce the maximum widening of the syn-
desmosis that was possible for a given fracture configuration
without resulting in permanent deformation or failure of the
remaining intact interosseous membrane24’29. The force was
also comparable with the force that the fibula and interos-
seous membrane might sustain during walking28.
With repeated loading of the interosseous membrane
in the twelve-step sectioning protocol, it is possible that the
intact interosseous membrane may have undergone pro-
gressive deformation and weakening; however, the equiv-
alent end-point in both Group I and Group II suggests that
this was not a major factor. In this model, the intact portion
of the interosseous membrane was not appreciably loaded
until the deltoid ligament had been divided. Accordingly,
although the interosseous membrane was loaded through
eleven cycles in Group-I specimens and only once in Group
11, the end-points of widening of the syndesmosis were thesame in both groups.
To facilitate clinical application of these results, we
measured the width of the syndesmosis by means of a com-
mon clinical modality - mortise radiographs - rather than
in a direct in vitro manner. Our mean baseline measurement
of the width of the syndesmosis was comparable with that
reported in the literature, when the same standard radio-
graphic technique was used#{176}’25.
Recent studies have demonstrated that the reduction of
the distal tibiofibubar syndesmosis correlates with the func-
tional outcome and the development of arthritis’8’23. In ad-
dition, one to two millimeters of widening of the syn-
desmosis, compared with the normal side, has yielded ac-
ceptable clinical results in the treatment of pronation-ex-
ternal rotation fractures’#{176}”8’25.
For fibular fractures that are fixed with a plate, we
determined the critical transition zone between a bevel of
fracture that results in clinically acceptable and one that
results in unacceptable widening of the syndesmosis to be
three to 4.5 centimeters proximal to the ankle (Fig. 5).
Therefore, we postulate that, when rigid medial fixation is
not possible, supplemental trans-syndesmotic stabilization
may be needed for fractures proximal to the transition zone,
but that such supplementation is not necessary for fractures
distal to this zone. If the deltoid complex is intact and rigid
medial fixation can be achieved, widening of the syndes-
mosis should remain in the clinically acceptable range with-
out trans-syndesmotic fixation, regardless of the level of
fibular fracture.
Conclusions
We explored the relationship between specific me-
chanical configurations and the need for trans-syndesmotic
fixation in an effort to aid decision-making in the operative
treatment of pronation-external rotation fractures of the an-
Ide. The need for trans-syndesmotic fixation to supplement
rigid fixation of the fibula and medial malleolus can be
determined by the height of the fibular fracture and the
competence of the deltoid ligament. Concern about extrap-
obation of data from cadavera to patients is justified; how-
ever, two points should be emphasized. First, even if the
precise bevel of the transition zone between the levels of a
fracture that will and will not result in unacceptable widen-
ing is slightly different in vivo, the observation that stability
of the syndesmosis is a function of the length of the intact
interosseous membrane when the deltoid ligament is dis-
rupted should still be valid. Second, since the experimental
design was chosen to favor overestimation of widening of
the syndesmosis, instability in vivo should be the same or
less.
In some injuries that result in the loss of the ability to
achieve rigid medial fixation operatively (that is, injuries
that include a deltoid tear), direct clinical application of
these results may foster more emphasis on fixation of the
syndesmosis than might be necessary. However, in all pron-
ation-externab rotation fractures that had rigid medial and
lateral fixation, the stability of the syndesmosis was clini-
cabby acceptable and overestimation would not affect op-
erative decisions.
Finally, these results suggest that acceptable stability
of the syndesmosis can be achieved after rigid internal fix-
ation without trans-syndesmotic fixation in many pronation-
external rotation fractures.
NOTE: The authors thank Mr. Jerry Gaskill for invaluable assistance with statistical analysisof the data.
References
1 . BOLIN , HJALMAR: The Fibula and Its Relationship to the Tibia and Talus in Injuries of the Ankle Due to Forced External Rotation. Acta Radiol.,56: 439-448, 1962.
2. BURWELL, H. N. , and CHARNLEY, A. D. : The Treatment of Displaced Fractures at the Ankle by Rigid Internal Fixation and Early Joint Movement.J. Bone and Joint Surg. , 47-B(4): 634-660, 1965.
3. CLOSE, J. R.: Some Applications of the Functional Anatomy of the Ankle Joint. J. Bone and Joint Surg. , 38-A: 761-781, July 1956.4. COLTON, C. L.: The Treatment of Dupuytren’s Fracture-Dislocation of the Ankle. J. Bone and Joint Surg. , 53-B(1): 63-71 , 1971.5. FARHAN, M. J., and SMITH, T. W. D.: Fixation of Diastasis of the Inferior Tibiofibular Joint Using the Syndesmosis Hook. Injury, 16: 309-311,
1985.6. JOY. GREGORY; PATZAKIS, M. J.; and HARVEY, J. P., JR.: Precise Evaluation ofthe Reduction ofSevere Ankle Fractures. Technique and Correlation
with End Results. J. Bone and Joint Surg. , 56-A: 979-993, July 1974.

MECHANICAL CONSIDERATIONS FOR THE SYNDESMOSIS SCREW 1555
7. KLEIGER, BARNARD: The Mechanism of Ankle Injuries. J. Bone and Joint Surg. , 38-A: 59-70, Jan. 1956.8. LAUGE-HANSEN, N. : Fractures of the Ankle. II. Combined Experimental-Surgical and Experimental-Roentgenologic Investigations. Arch. Surg.,
60: 957-985, 1950.9. LAUGE-HANSEN, N. : Fractures of the Ankle. IV. Clinical Use of Genetic Roentgen Diagnosis and Genetic Reduction. Arch. Surg. , 64: 488-500,
1952.10. LEEDS, H. C. , and EHRLICH, M. G. : Instability of the Distal Tibiofibular Syndesmosis after Bimalleolar and Trimalleolar Ankle Fractures. J. Bone
and Joint Surg. , 66-A: 490-503, April 1984.1 1 . LINDSJO, ULF: Operative Treatment of Ankle Fractures. Acta Orthop. Scandinavica, Supplementum 52, 1981.12. MAST, J. W. , and TEIPNER, W. A.: A Reproducible Approach to the Internal Fixation of Adult Ankle Fractures: Rationale, Technique, and Early
Results. Orthop. Clin. North America, 11: 661-679, 1980.13. MEYER, T. L., JR., and KUMLER, K. W.: A.S.I.F. Technique and Ankle Fractures. Clin. Orthop., 150: 211-216, 1980.14. MINNS, R. J. , and HUNTER, J. A. A. : The Mechanical and Structural Characteristics of the Tibio-Fibular Interosseous Membrane. Acta Orthop.
Scandinavica, 47: 236-240, 1976.15. OLERUD, C. : The Effect of the Syndesmotic Screw on the Extension Capacity of the Ankle Joint. Arch. Orthop. and Traumat. Surg. , 104: 299-
302, 1985.16. PANKOVICH, A. M.: Maisonneuve Fracture of the Fibula. J. Bone and Joint Surg. , 58-A: 337-342, April 1976.17. PANKOVICH, A. M.: Fractures of the Fibula Proximal to the Distal Tibiofibular Syndesmosis. J. Bone and Joint Surg., 60-A: 221-229, March
1978.18. PETTRONE, F. A.; GAIL, MITCHELL; PEE, DAVID; FITZPATRICK, THOMAS; and VAN HERPE, L. B.: Quantitative Criteria for Prediction ofthe Results
after Displaced Fracture of the Ankle. J. Bone and Joint Surg. , 65-A: 667-677, June 1983.19. PURVIS, G. D.: Displaced, Unstable Ankle Fractures. Classification, Incidence, and Management of a Consecutive Series. Clin. Orthop. , 165: 91-
98, 1982.20. RAMSEY, P. L. , and HAMILTON, WILLIAM: Changes in Tibiotalar Area of Contact Caused by Lateral Talar Shift. J. Bone and Joint Surg. , 58-A:
356-357, April 1976.21. RASMUSSEN, 0.; TOVBORG-JENSEN, I.; and BOE, S.: Distal Tibiofibular Ligaments. Analysis of Function. Acta Orthop. Scandinavica, 53: 681-
686, 1982.22. RIEGELS-NIELSEN, P.; CHRISTENSEN, J. ; and GREIFF, J.: The Stability of the Tibio-Fibular Syndesmosis following Rigid Internal Fixation for Type
C Malleolar Fractures: An Experimental and Clinical Study. Injury, 14: 357-360, 1983.23. ROBERTS, R. S.: Surgical Treatment of Displaced Ankle Fractures. Clin. Orthop., 172: 164-170, 1983.24. SARMIENTO, AuGUST0; LATTA, LOREN; ZILI0LI, ARMAND; and SINCLAIR, WILLIAM: The Role ofSoft Tissues in the Stabilization ofTibial Fractures.
Clin. Orthop., 105: 116-129, 1974.25. SCLAFANI, S. J. A.: Ligamentous Injury of the Lower Tibiofibular Syndesmosis: Radiographic Evidence. Radiology, 156: 21-27, 1985.26. SKRABA, J. S. , and GREENWALD, A. S.: The Role of the Interosseous Membrane on Tibiofibular Weightbearing. Foot and Ankle, 4: 301-304,
1984.27. SOLONEN, K. A. , and LAUTTAMUS, LEO: Operative Treatment of Ankle Fractures. Acta Orthop. Scandinavica, 39: 223-237, 1968.28. TAKEBE, KY0IcHI; NAKAGAWA, Moo; MINAMI, HISA0; KANAZAWA, HIDEKAZU; and HIROHATA, KAZUSHI: Role of the Fibula in Weight-Bearing.
Clin. Orthop. , 184: 289-292, 1984.29. VuKu�EvI�, SLOBODAN; STERN-PADOVAN, RANKA; VuK1�EvI�, DALIBOR; and KEROS, PREDRAG: Holographic Investigations of the Human Tibio-
fibular Interosseous Membrane. Clin. Orthop. , 151: 210-214, 1980.30. WILSON, F. C. , JR. , and SKILBRED, L. A.: Long-Term Results in the Treatment of Displaced Bimalleolar Fractures. J. Bone and Joint Surg. , 48-
A: 1065-1078, Sept. 1966.31. YABLON, I. G.; HELLER, F. G.; and SHOUSE, LEROY: The Key Role of the Lateral Malleolus in Displaced Fractures of the Ankle. J. Bone and
Joint Surg. , 59-A: 169-173, March 1977.32. YDE, JOHANNES: The Lauge Hansen Classification of Malleolar Fractures. Acta Orthop. Scandinavica, 51: 181-192, 1980.33. YDE, J. , and KRISTENSEN, K. D.: Inferior Tibio-Fibular Diastasis Treated by Staple Fixation. J. Trauma, 21: 483-485, 1981.
VOL. 71-A, NO. 10, DECEMBER 1989