Embed Size (px)
Citation preview
Mechanical Complications of Mechanical Complications of Myocardial InfarctionMyocardial Infarction
Armed Forces Academy of Medical Sciences
EpidemiologyEpidemiology
1.5 Million MI’s yearly in U.S.30% mortality
– decline by 30% in last decade– In hospital mortality ~5%
50% of deaths occur in first hr. secondary to ventricular arrhythmias- later lecture
Mechanical complications responsible for 15% of deaths
Mechanical ComplicationsMechanical Complications
Free Wall RupturePseudoaneurysmRupture of Intraventricular septumRupture of Papillary Muscle
LV Free Wall RuptureLV Free Wall Rupture
Mean Age 698-15% of all deaths from MI10% of hospital deathsPeaks 3-6 days post MI, 25% within 24 hrs.
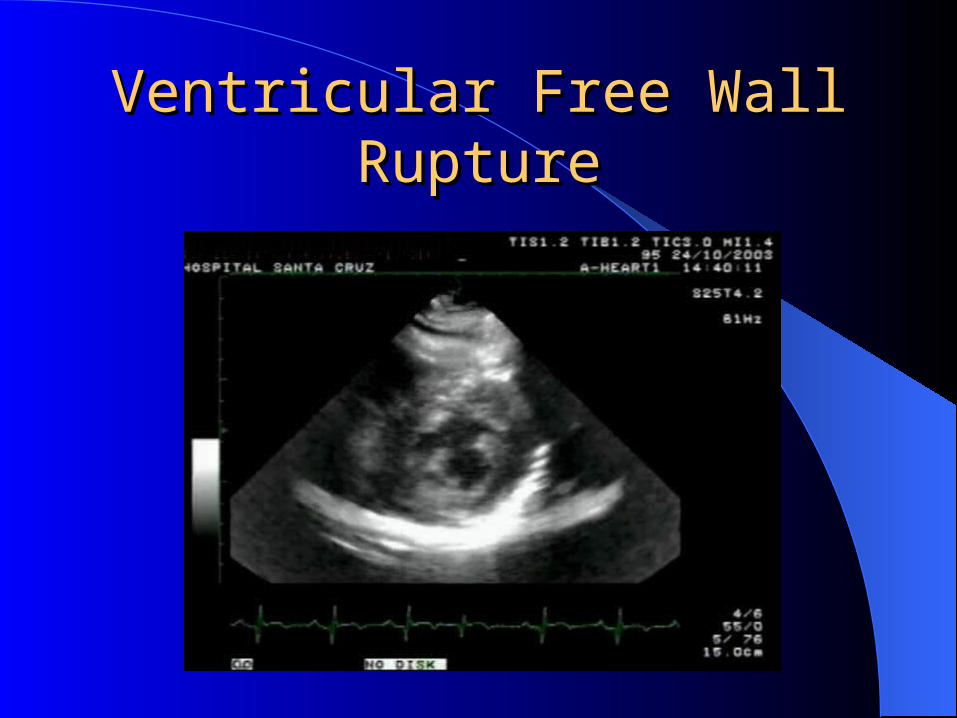
Ventricular Free Wall RuptureVentricular Free Wall Rupture

LV Free Wall RuptureLV Free Wall RupturePathophysiologyPathophysiology
Usually involves anterior or lateral walls in distribution of terminal LAD
Large, transmural MI’s involving > 20% of myocardium.
Tear in myocardium or dissecting hematoma at junction of infarct and normal muscle. Shearing effect produces laceration of myocardial microstructure
LV Free Wall RuptureLV Free Wall RuptureRisk FactorsRisk Factors
Sustained HTNAGE, Female sexFirst MI, Normal LV function
– Increased shearing forces
Corticosteroids, NSAID’s– Impaired wound healing
Late use of Thrombolytics– decreased incidence with early therapy
Persistent occlusion, lack of collaterals
LV Free Wall RuptureLV Free Wall RuptureClinical CourseClinical Course
Ruptured free wall leads to hemopericardium and death through tamponade, cardiogenic shock
Nausea, hypotension, pericardial pain, agitation– ? prodromal bleeding, seen in 80% of pts with rupture
25% have new murmurDeviation from expected Evolutionary T-wave
pattern- 94% of pts.EMD, Bradydysrhythmias, AIVR common
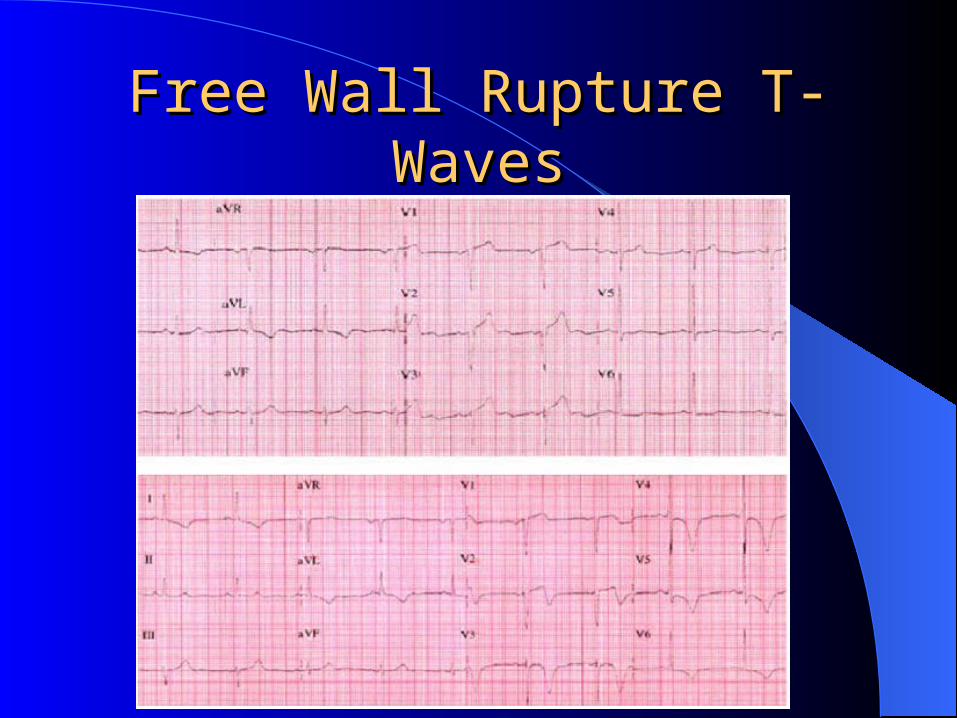
Free Wall Rupture T-WavesFree Wall Rupture T-Waves
LV Free Wall RuptureLV Free Wall RuptureDiagnosisDiagnosis
Death often occurs prior to imaging . SCD 70%
Echo shows pericardial effusion, tamponadeOrganized thrombus in pericardial spaceIncomplete rupture may be missed by TTE,
TEEPA catheter shows equalization of
pressures-tamponade
LV Free Wall RuptureLV Free Wall RuptureManagementManagement
90% medical mortality; sugical case reports of correction
Inotropic agentsVolume LoadingPericardiocentesis
LV Free Wall RuptureLV Free Wall RuptureManagementManagement
IABP, hemodynamic stabilizationCoronary Angiography controversialBlind bypass of palpable lesionsInfarctectomy with closure of viable
myocardium– avoid suture in infarcted tissue
Dacron, Teflon or Pericardial patch
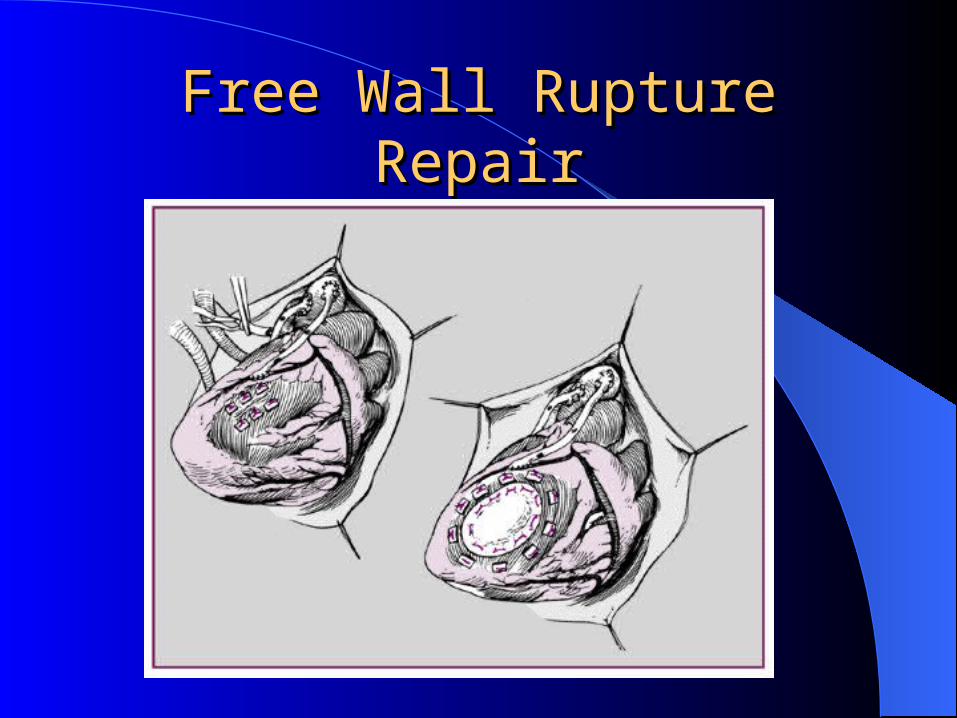
Free Wall Rupture RepairFree Wall Rupture Repair
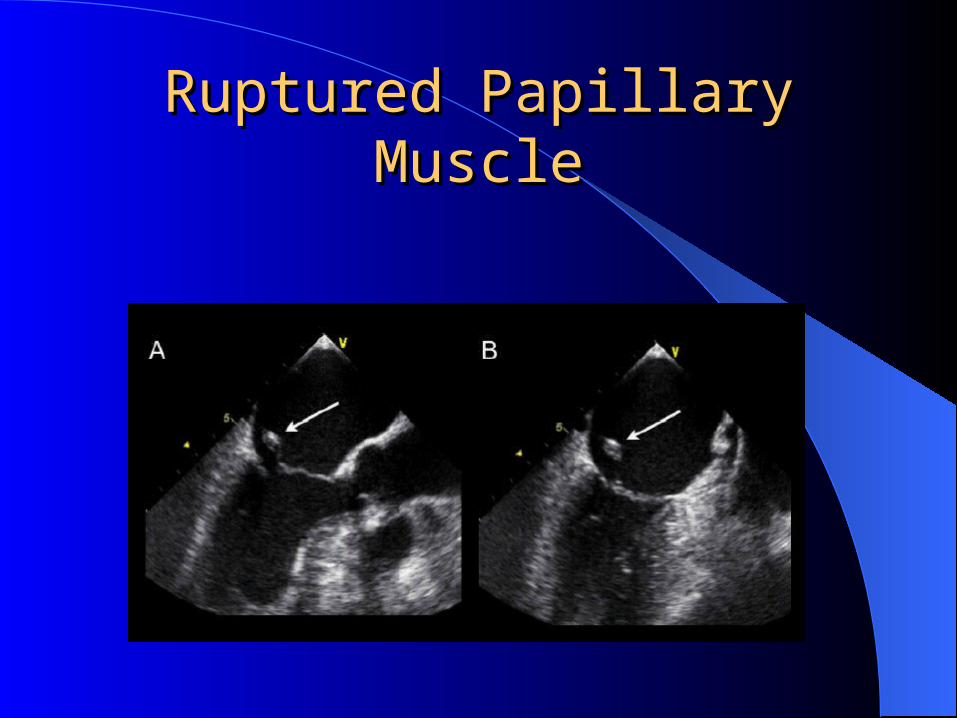
Ruptured Papillary MuscleRuptured Papillary Muscle
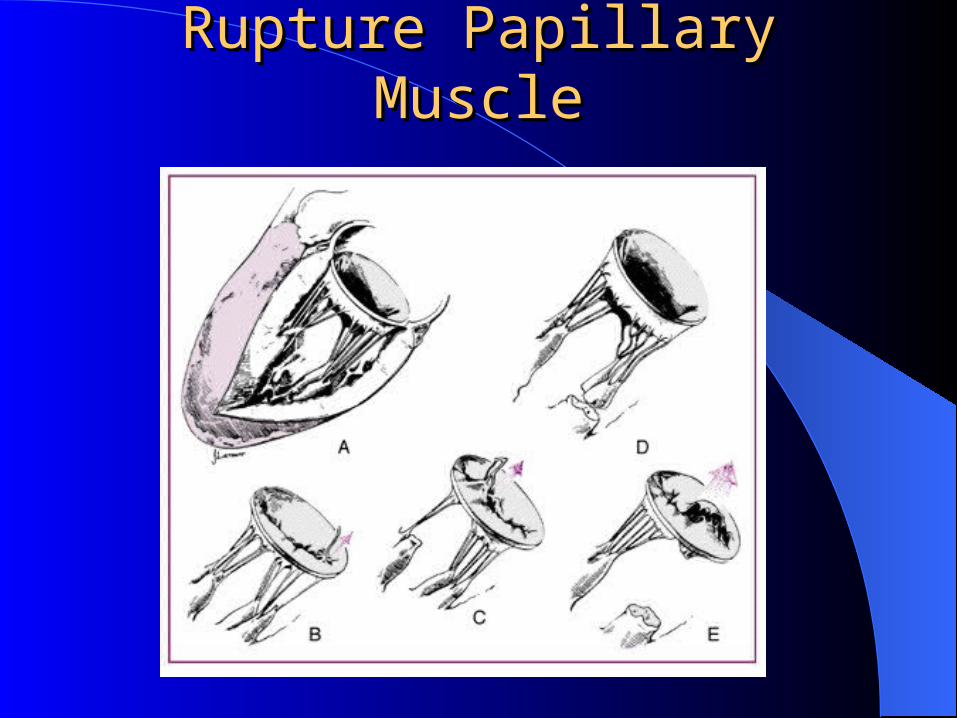
Rupture Papillary MuscleRupture Papillary Muscle
Papillary Muscle RupturePapillary Muscle Rupture
MR Transiently present in up to 80% of MI pts.– usually of no hemodynamic significance
Mitral Annular Dilitation, Wall motion asynergy, Papillary muscle dysfunction/rupture
0.9-5% of all deaths from MI 50% mortality within 24hrs., 80% within 2 weeks
Papillary Muscle RupturePapillary Muscle Rupture Inferior MI leads to rupture of Postero-medial pap
muscle/AMI-antero-lateral pap muscle (rare)– PM pap muscle single supply from PDA– AL pap muscle dual supply from LAD/Cx
Complete transection incompatible with life Occurs with small infarctions, moderate CAD
– 50% have subendocardial infarct, single vessel dz– Greater shearing forces
Length of coronary vessels, subendocardial location may predispose to ischemia
Papillary Muscle RupturePapillary Muscle RupturePresentationPresentation
Mean age 65Peak incidence 3-5 days post-MI75% Inferior MINew Holosytolic Murmur in 50%
– pressure equalization may blunt murmur
Acute hemodynamic decompensation, pulmonary edema
Papillary Muscle RupturePapillary Muscle RuptureDiagnosisDiagnosis
Physical exam often non-diagnosticEcho may visualize chordal rupture, head of
pap muscle, flail leafletLV fxn well preserved in setting of
hemodynamic decompensationCoronary angiography prior to surgery if
condition permits
Papillary Muscle RupturePapillary Muscle RuptureManagementManagement
33% immediate death, 50% at 24 hrs., 80% within 2 weeks
Afterload reduction, vasodilatorsIABP-afterload reductionMV replacement or repair
– may be delayed up to 6 weeks if pt. stable to allow myocardial healing s/p MI
– 50% of those initially stabilized will decompensate
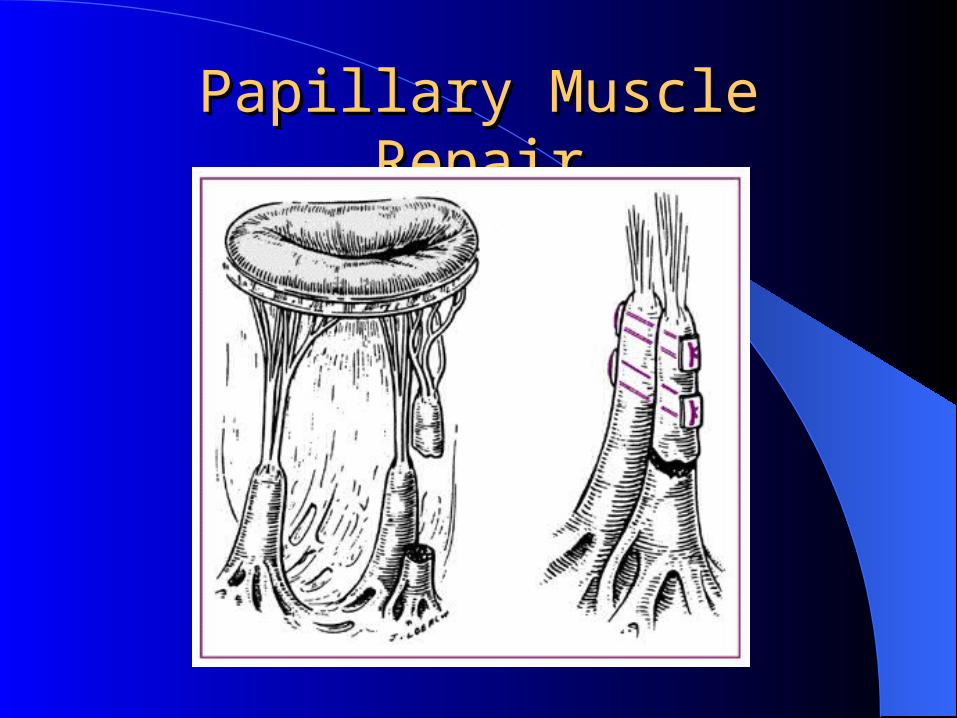
Papillary Muscle RepairPapillary Muscle Repair
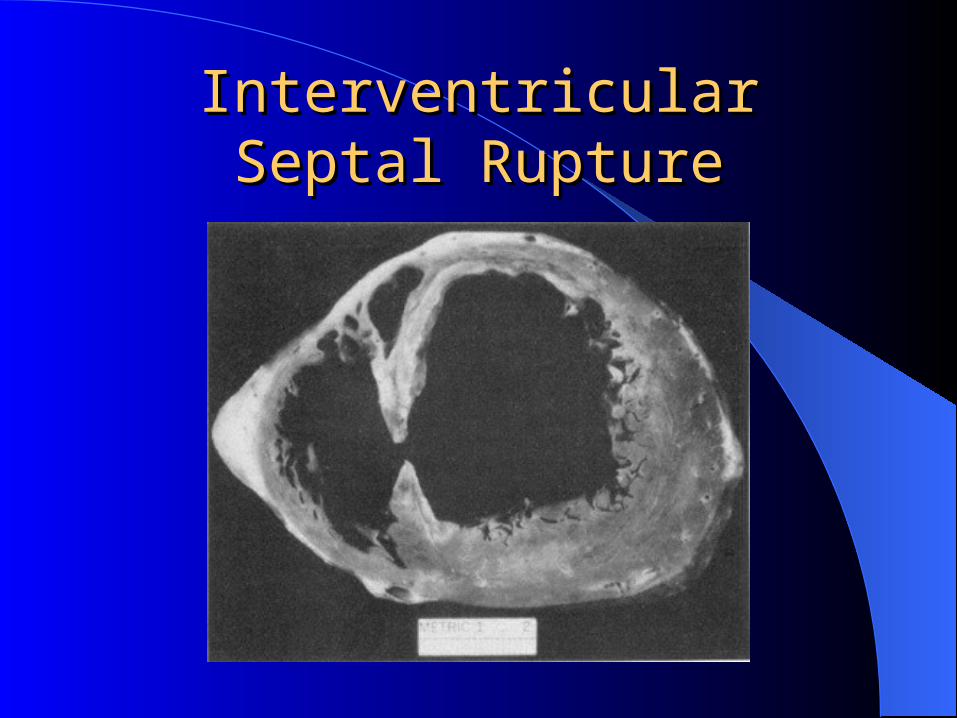
Interventricular Septal RuptureInterventricular Septal Rupture
Interventricular Septal RuptureInterventricular Septal Rupture
0.5-2 Percent of MI’s5 % of peri-infarction deathsMean Age 63HypertensionPoor collateral network
Interventricular Septal RuptureInterventricular Septal RuptureRisk FactorsRisk Factors
Large Transmural InfarctionsAnterior-Apical, Inferior-BasalVirtually all patients have severe, multi-
vessel CADFirst MI
Interventricular Septal RuptureInterventricular Septal RuptureClinical FeaturesClinical Features
Harsh, Loud Holosystolic Murmur at LLSB with thrill (50%)
Acute right sided heart failureMay have increased chest pain, SOBCardiogenic Shock
Interventricular Septal RuptureInterventricular Septal RuptureDiagnosisDiagnosis
Step up in oxygen saturation of RVAngiography if hemodynamically stable for
coronary anatomy, ventriculographyEcho
– Highly sensitive (96%) with careful apical-basal, and anterior-posterior sweeps of septum
– doppler to detect complex defects
Intraventricular Septal RuptureIntraventricular Septal RuptureManagementManagement
Diuretics, Ionotropes, Vasodilators-enhance forward flow, decrease shunting.
IABPSurgical repair
– 25% mortality at 24 hrs., 65% at 2 weeks without surgery
Cardiogenic shock 100% mortality without surgeryLV Fxn, magnitude of shunt do not correlate with
outcome
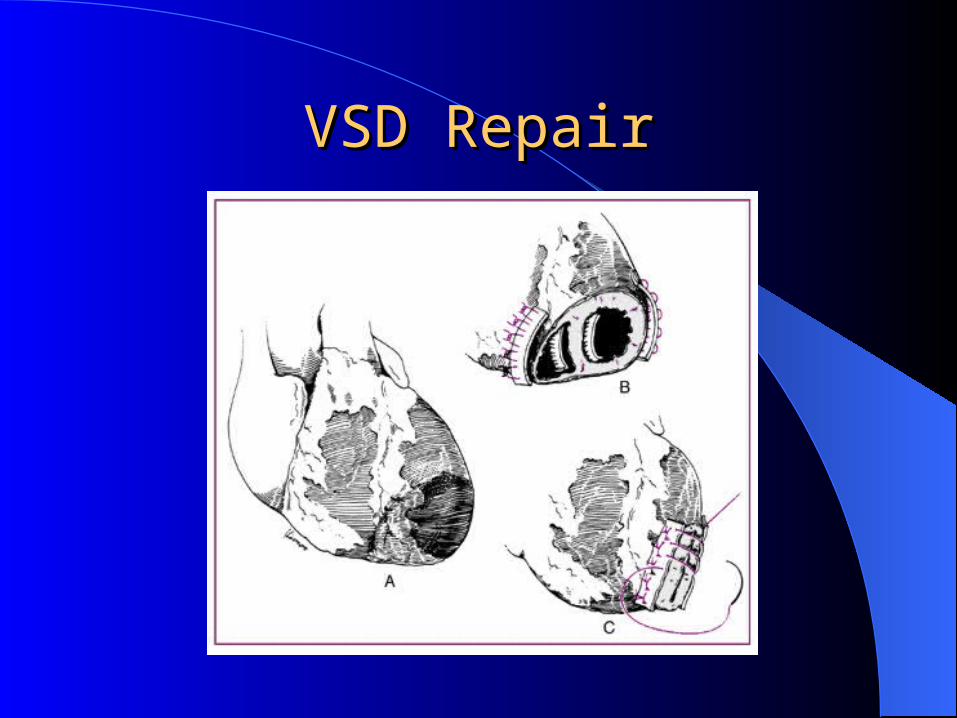
VSD RepairVSD Repair
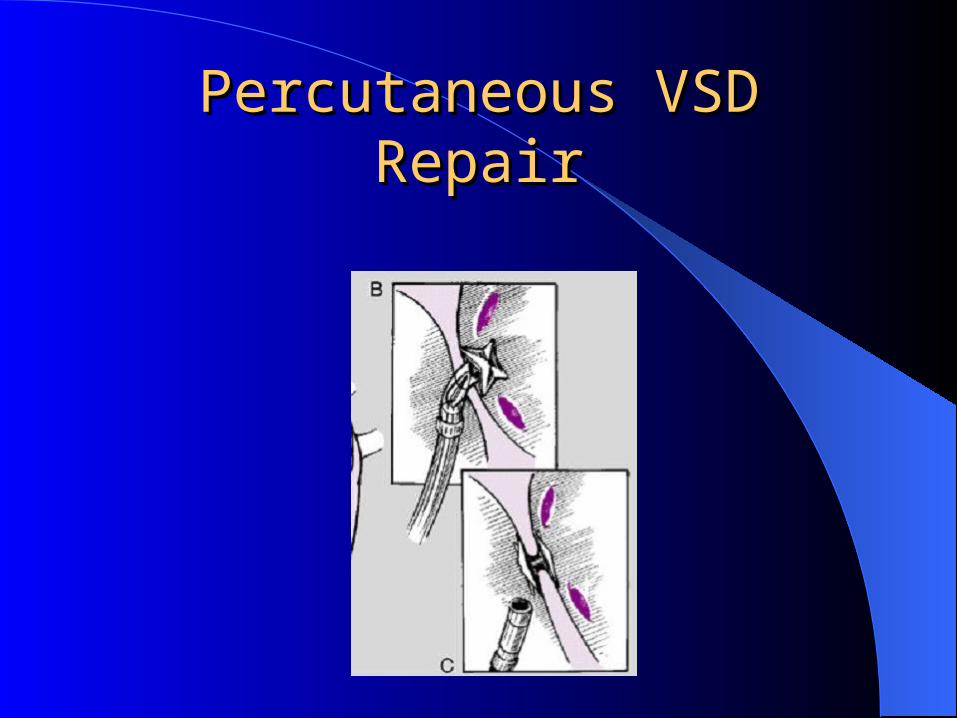
Percutaneous VSD RepairPercutaneous VSD Repair

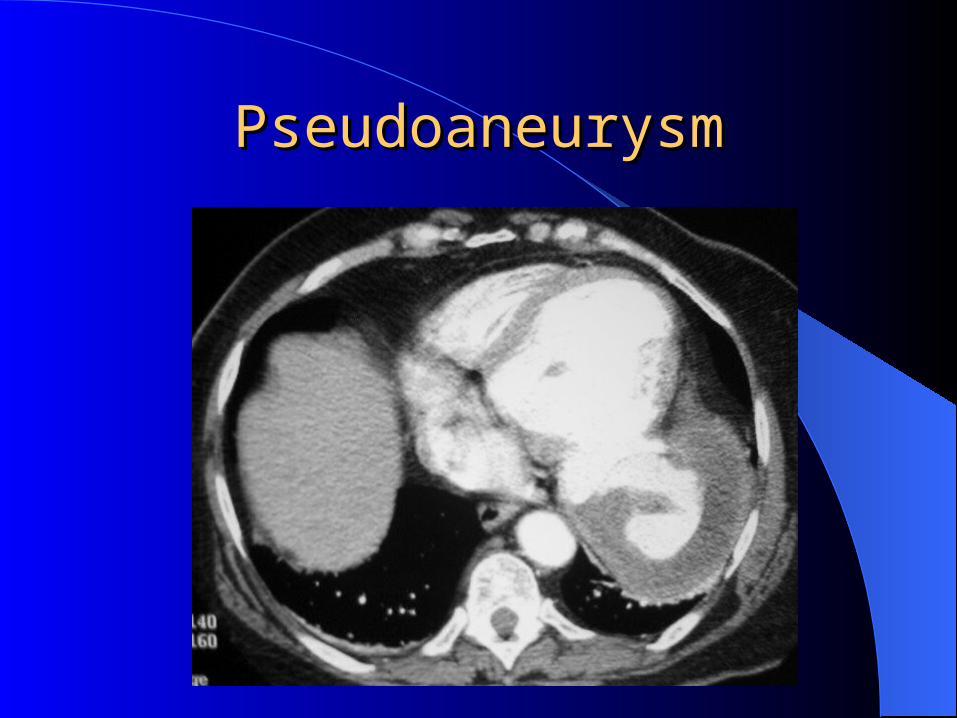
LV PseudoaneurysmLV Pseudoaneurysm
Rare complication of MIResults from incomplete rupture of wall
sealed by thrombus and pericardium
PseudoaneurysmPseudoaneurysm
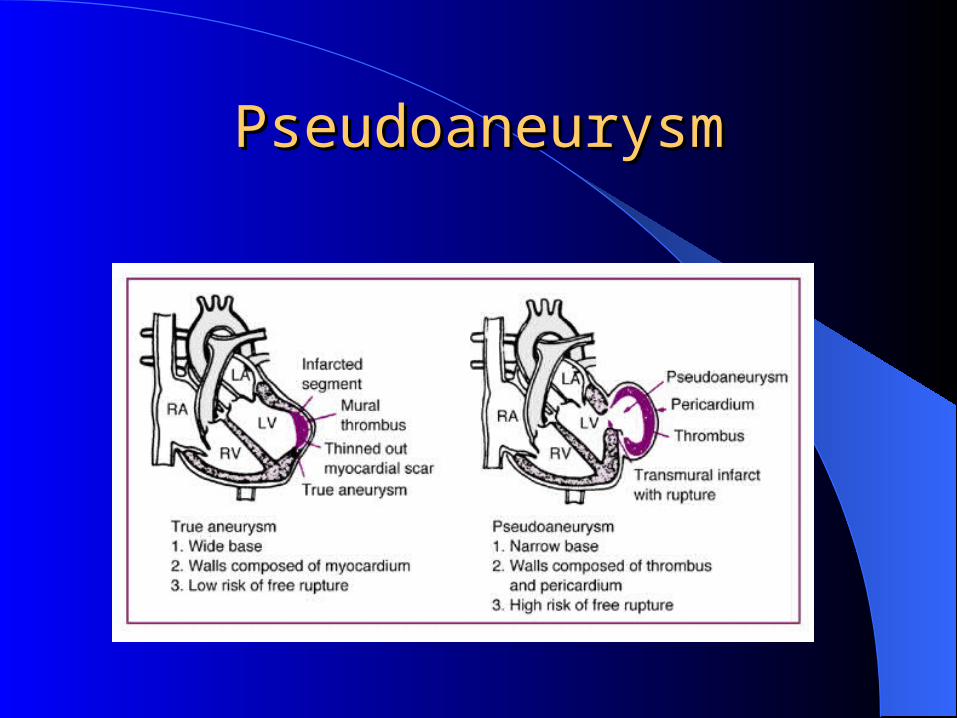
PseudoaneurysmPseudoaneurysm
LV PseudoaneurysmLV PseudoaneurysmDiagnosisDiagnosis
Difficulty to distinguish from true anuerysmTo and Fro murmurPericardial friction rubEnlarging LV bulge on lateral or posterior
wallNarrow neck seen on Echo, or LV gram
LV pseudoaneurysmLV pseudoaneurysmManagementManagement
High propensity ruptureUrgent surgical repair indicatedTechnique similar to free wall ruptureSurvival 90% in stable pts.