Embed Size (px)
Citation preview

Dr. Ang Boon SuenDepartment of PhysiologyDepartment of Physiology
6 Dec 2009
1

IntroductionThe fundamental goals of respiration are to provide O2 to the tissues and to remove CO22 2To achieve this, respiration can be divided into four major functions:
P l til tiPulmonary ventilationDiffusion of O2 and CO2 between the alveoli and the bloodand the bloodTransport of O2 and CO2; andRegulation of ventilation and other facets of grespiration.
2

Components of Respiratory SystemComponents of respiratory systemy y
Respiratory tract Ventilation– Ventilation
Alveolo-capillary membrane p y– Gas exchange
Blood + Peripheral cellsBlood + Peripheral cells – 02 utilization
3

Pulmonary ventilationPulmonary ventilation is the movement of air into andout of the lungsAi f f hi h tAir moves from an area of higher pressure to an area of lower pressure – pressure gradientThe process of pulmonary ventilation requires aThe process of pulmonary ventilation requires a pressure gradient between the outside of the body and the alveoliAt t th f i i ti i tiAt rest, the process of inspiration is an active processand expiration is a passive processInspiration needs muscular contraction. The chiefInspiration needs muscular contraction. The chief muscle of inspiration is the diaphragmExpiration is due to elastic recoils of the lungs and thoracic wall, and the inspiratory muscles relax.
4

Components of Respiratory TractConducting zone:
All the structures air passes through before reaching the respiratory zonezone.Mouth, nose, pharynx, trachea, glottis, larynx, bronchi
Respiratory zoneR i fRegion of gas exchange between air and blood.
bronchiolesalveoli
5

Mechanics of VentilationMechanics of ventilation include forces that support and move the chest wall & the lungs, together with resistances that they need to overcomeresistances that they need to overcomeTo understand the mechanisms involved in ventilation, it is necessary to identify the forces that are responsible for enlargement of thorax and lungRespiratory muscles are used to generate forces during ventilationduring ventilation
Inspiratory MusclesExpiratory Muscles
6
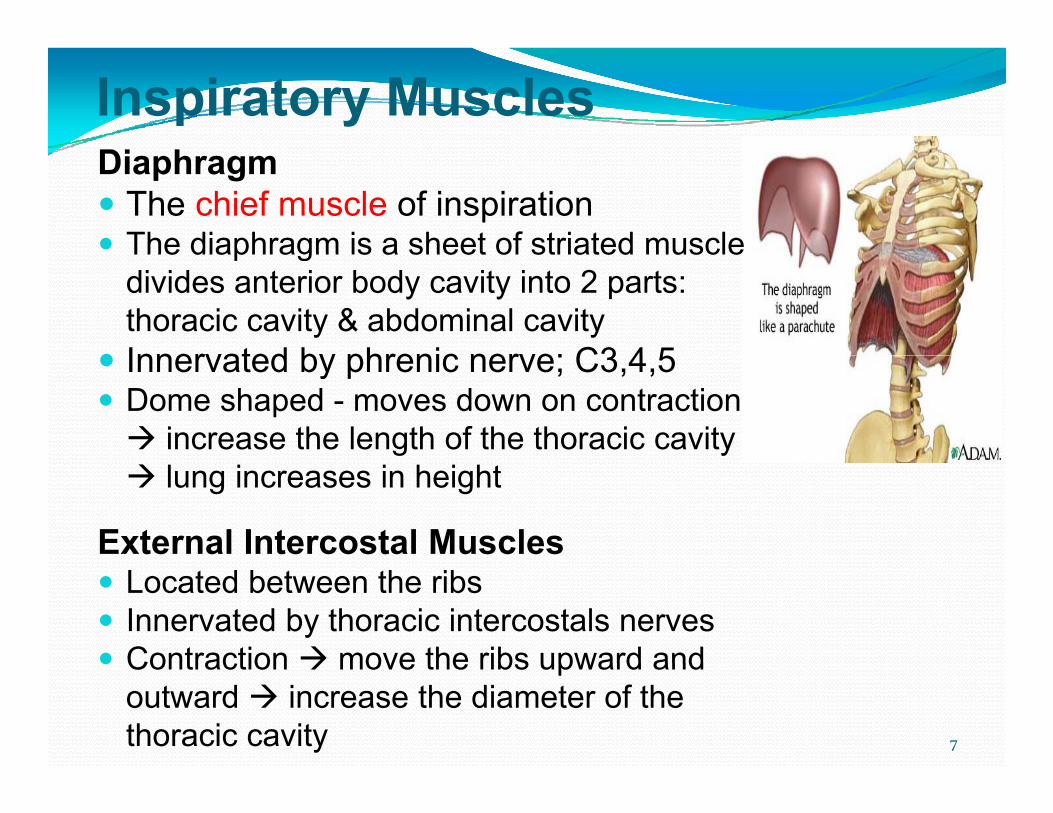
Inspiratory MusclesDi hDiaphragm
The chief muscle of inspirationThe diaphragm is a sheet of striated muscleThe diaphragm is a sheet of striated muscle divides anterior body cavity into 2 parts: thoracic cavity & abdominal cavityInnervated by phrenic nerve; C3 4 5Innervated by phrenic nerve; C3,4,5Dome shaped - moves down on contraction
increase the length of the thoracic cavity lung increases in height
External Intercostal MusclesLocated between the ribsInnervated by thoracic intercostals nervesContraction move the ribs upward andContraction move the ribs upward and outward increase the diameter of the thoracic cavity 7

Inspiratory MusclesyAccessory muscles of inspiration
Become important during exercise or respiratory g ydisstress – active breathingSternocleidomastoid muscles - which lift upward on the stern mthe sternum; Anterior serrati - which lift many of the ribs; and Scalene muscles - which lift the first two ribs.
8
Expiratory MusclesInvolved in active breathingAbdominal muscles: rectus abdominis, internalAbdominal muscles: rectus abdominis, internal and external oblique and transverse abdominis muscles
I t d b th i d l b i lInnervated by thoracic and lumbar spinal nervesContraction pull the ribs downward and squeeze the abdomen to increase abdominal pressure move the pdiaphragm upward and decrease the thoracic volume
Internal intercostals musclesC t ti lli th ib d dContraction pulling the ribs downward

Upper Airway MusclesyUpper airway muscles in the pharynx and larynx also contract in phase with breathing and important in determining airway resistancePharyngeal muscles: stiffens the soft palate and hold the tongue out of the way for breathing during inspirationtongue out of the way for breathing during inspirationLaryngeal muscles: dilate the airway during inspirationDilatation of nares by the alae nasi: decrease the yresistance to airflowMouth breathing: decrease the resistance to airflow
10

INSPIRATION
11
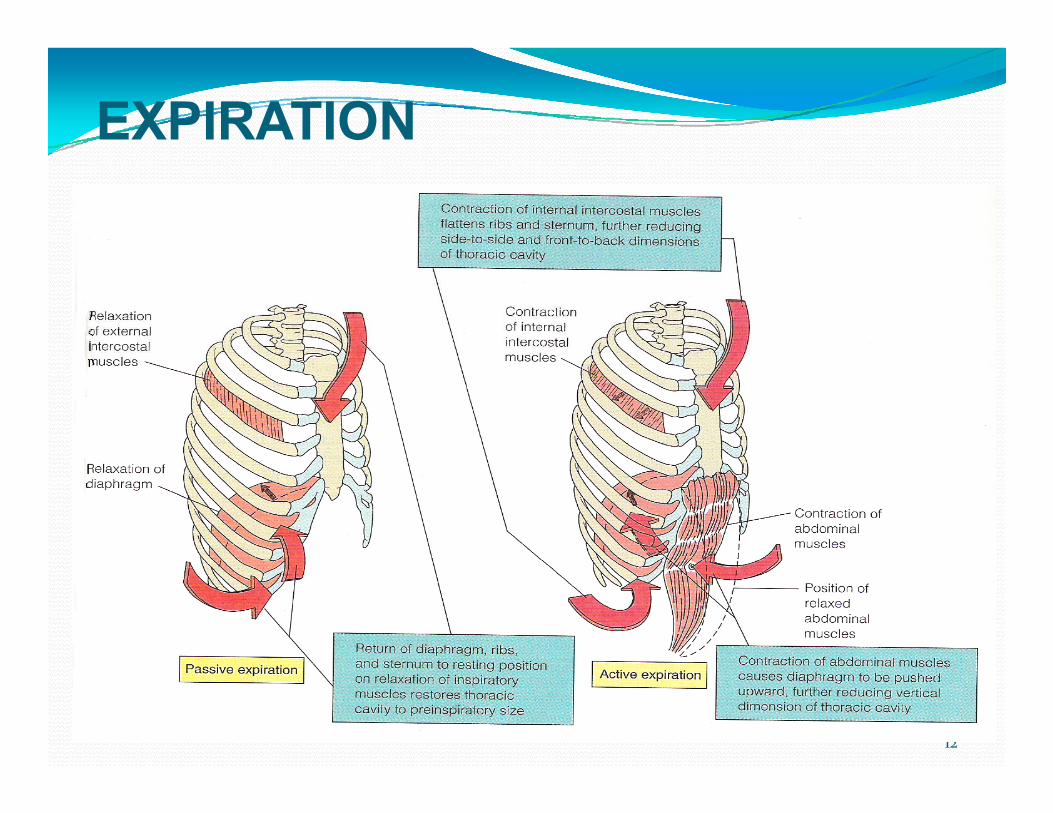
EXPIRATION
12
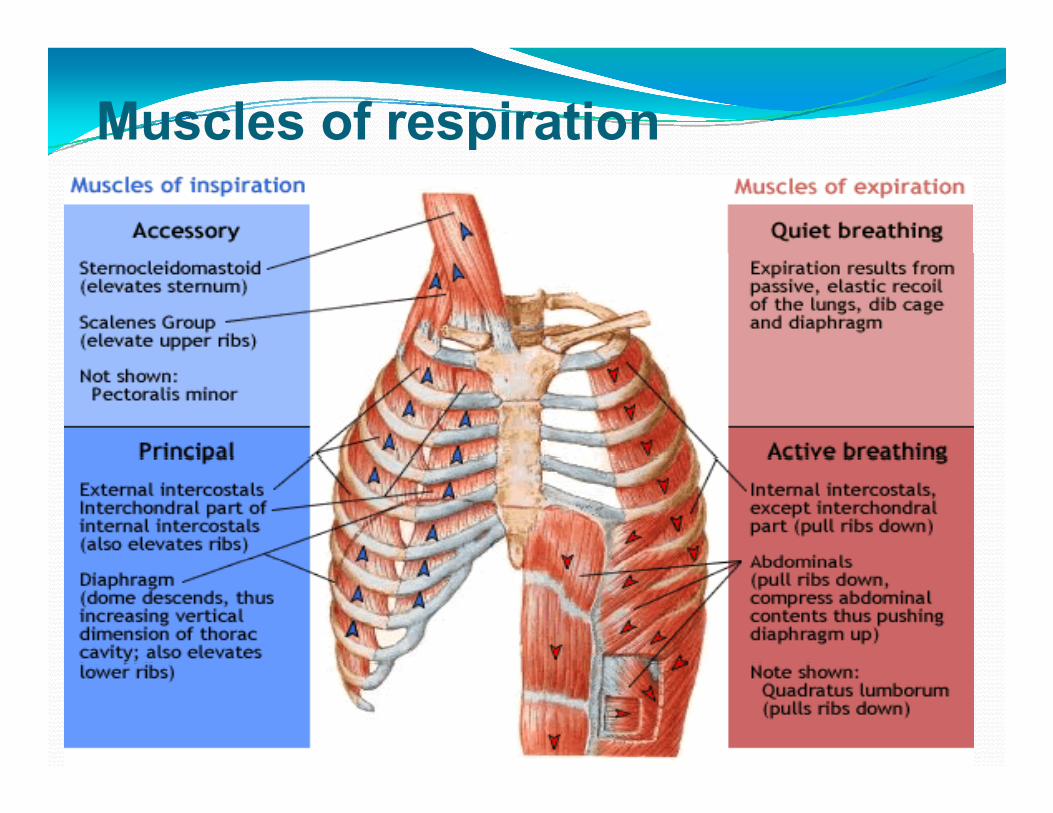
Muscles of respiration
13

Pressure changes during respirationg g
Different types of pulmonary pressuresIntra pulmonary (Intra-alveolar) pressureIntra pleural pressureTranspulmonary pressure

Pulmonary PressuresyIntra Pulmonary Pressure (Palv)
Also called intra alveolar pressurei th ithi th l li f th lis the pressure within the alveoli of the lungs.Is exactly same as the atmospheric pressureBecause the alveoli are directly connected to the atmosphere.It rises and falls during breathing During normal/quiet breathingDuring normal/quiet breathing
inspiration decreasing to -3mmHgexpiration raising to +3mmHg.
Forced/active breathing:Forced/active breathing:Extra muscles, including abs+/- 20-30 mmHg intrapulmonary pressure
15
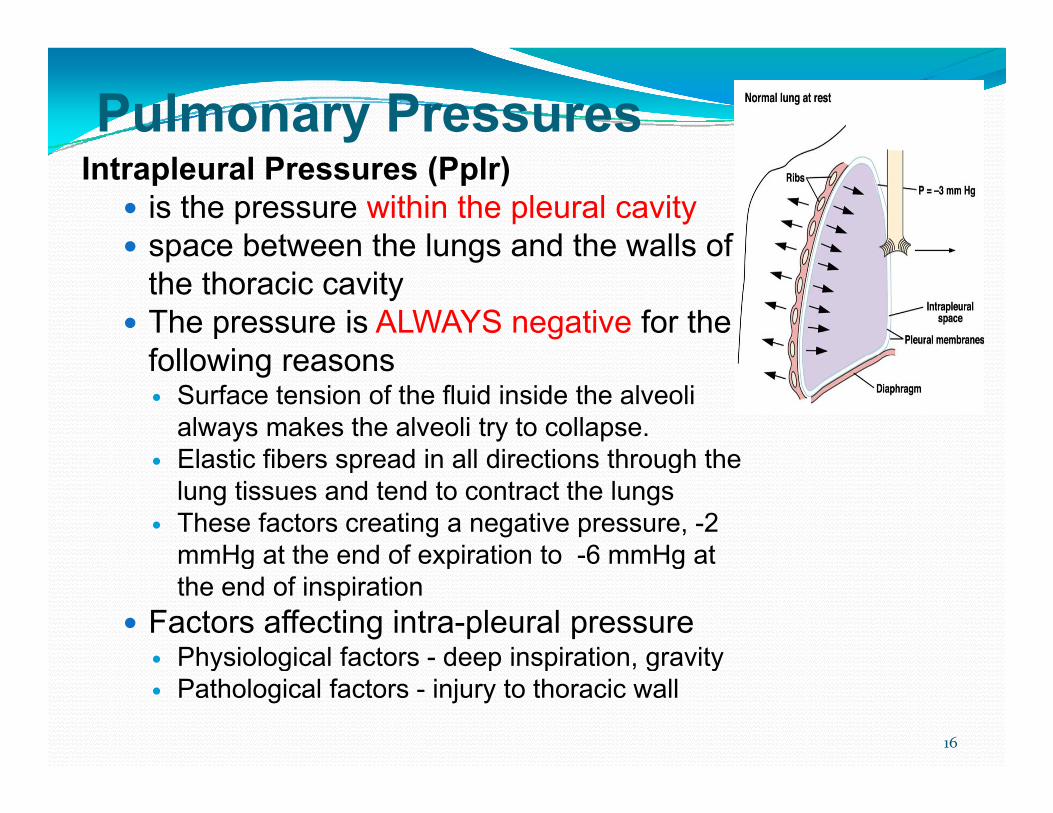
Pulmonary PressuresIntrapleural Pressures (Pplr)
is the pressure within the pleural cavityspace between the lungs and the walls ofspace between the lungs and the walls of the thoracic cavityThe pressure is ALWAYS negative for the following reasonsfollowing reasons
Surface tension of the fluid inside the alveoli always makes the alveoli try to collapse.Elastic fibers spread in all directions through theElastic fibers spread in all directions through the lung tissues and tend to contract the lungsThese factors creating a negative pressure, -2 mmHg at the end of expiration to -6 mmHg atmmHg at the end of expiration to 6 mmHg at the end of inspiration
Factors affecting intra-pleural pressurePhysiological factors - deep inspiration gravityPhysiological factors deep inspiration, gravityPathological factors - injury to thoracic wall
16

Pulmonary PressuresyTranspulmonary pressure (Tpp)
The pressure difference between i t l dintrapulmonary pressure and intrapleural pressure.
Tpp = Palv – Pplrpp pTpp is the distending pressure which helps to prevent airway collapse
Transthoracic pressure (Ttp)Transthoracic pressure (Ttp)The pressure difference between intrapulmonary pressure and atmospheric pressure
17

Pressure changes during respirationg gIntrapulmonay pressure
Reduces from 0 to -1mmHg during inspiration and comes back to 0 atinspiration and comes back to 0 at the end of inspirationIncreases to +1mmHg and comes back to 0 at the end of expirationback to 0 at the end of expiration
Intraplueural pressureAt the start of qiuet breathing, it q g,is -2mmHg. At the end of inspiration it becomes -6mmHg
18
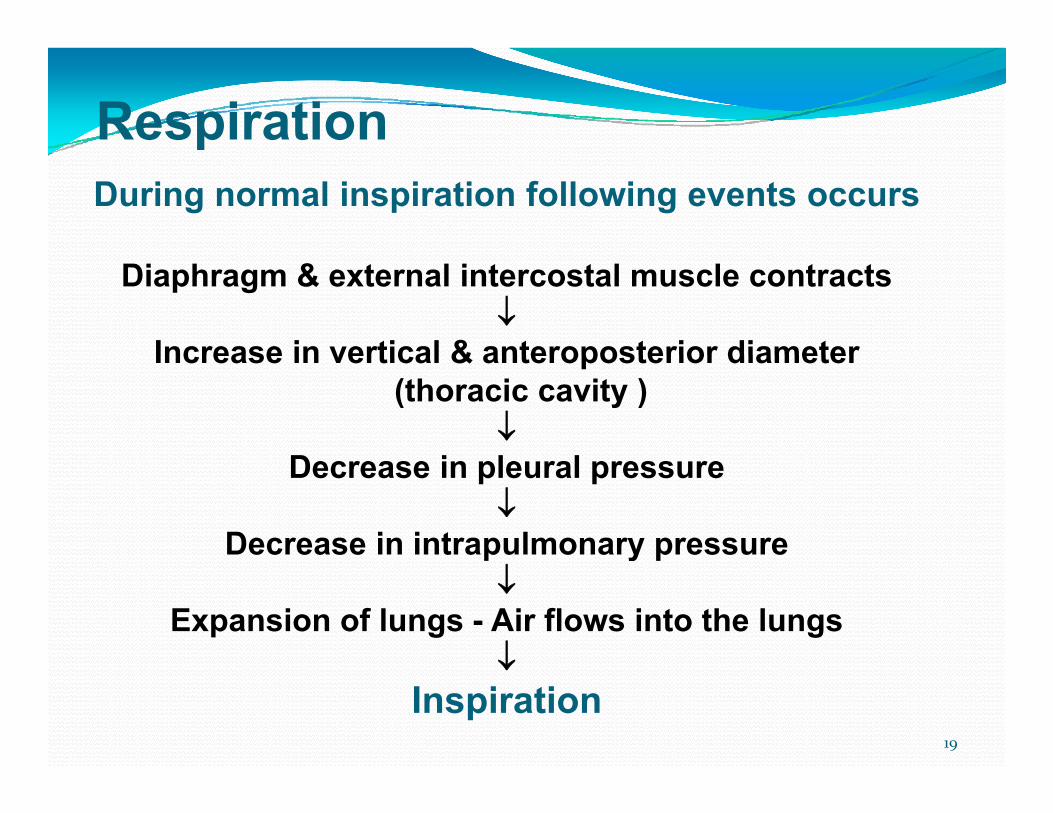
RespirationDuring normal inspiration following events occurs
Diaphragm & external intercostal muscle contracts ↓
Increase in vertical & anteroposterior diameterIncrease in vertical & anteroposterior diameter (thoracic cavity )
↓D i l lDecrease in pleural pressure
↓Decrease in intrapulmonary pressure p y p
↓Expansion of lungs - Air flows into the lungs
↓↓Inspiration
19
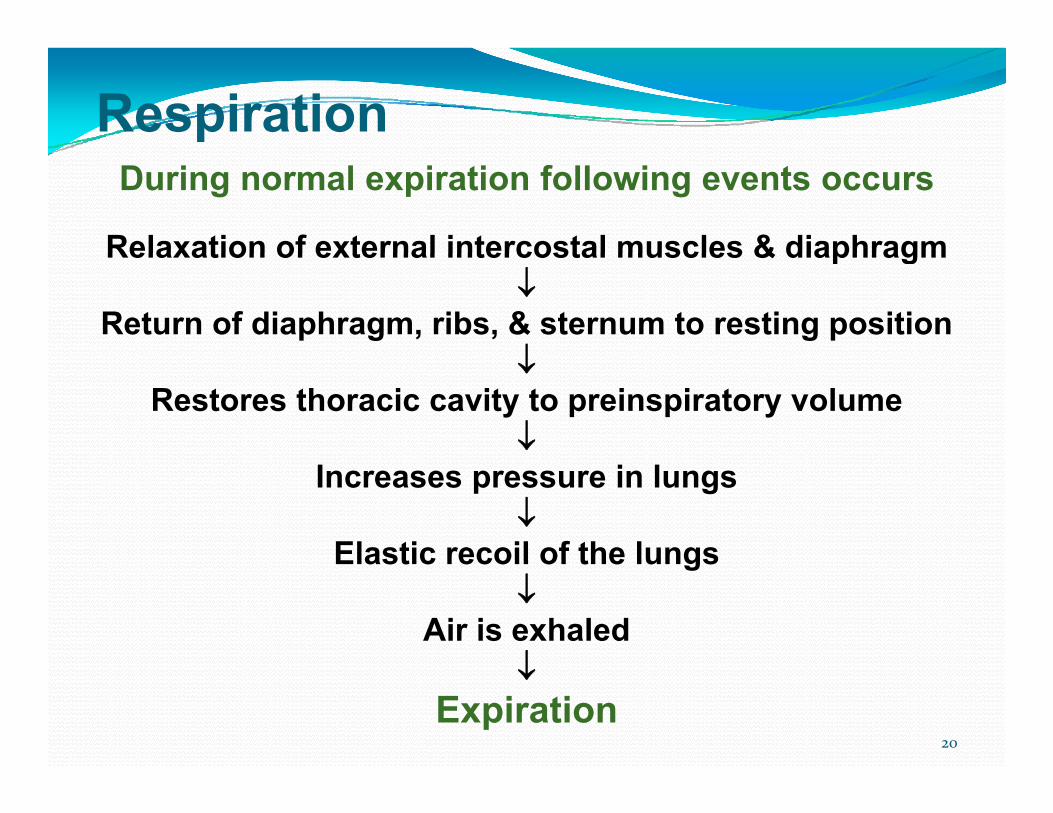
RespirationDuring normal expiration following events occurs
Relaxation of external intercostal muscles & diaphragmRelaxation of external intercostal muscles & diaphragm ↓
Return of diaphragm, ribs, & sternum to resting position ↓↓
Restores thoracic cavity to preinspiratory volume ↓
Increases pressure in lungs ↓
Elastic recoil of the lungsElastic recoil of the lungs ↓
Air is exhaled ↓↓
Expiration 20

Elastic properties of the lunggElastic behaviour of lung is due to the presence of
(i) elastin fibers( )(ii) collagen fibers(iii) surfactant
Elastic forces of the lung tissue (1/3) and the elastic forces created by surface tension (2/3) are the two main mechanisms involved in the tendency of the lung to recoil
Collapsing tendency of lungsg y gLungs are under constant threat of collapsing even under normal condition because of following reasons:
The elastic property of lung tissues, which induces the recoiling tendency of lungsrecoiling tendency of lungs Surface tension over the surface of the alveoli of lungs (it is the tension exerted over the alveolar membrane, by fluid secreted by the alveolar epithelium)by fluid secreted by the alveolar epithelium)
The factors preventing the collapsing tendency of lungs: g
Intrapleural pressure as it is negative Surfactant, which reduces surface tension
22

ComplianceIs defined as the change in volume per unit change in the pressure,C li ΔV/ΔPCompliance = ΔV/ΔP
Distensibility or stretchiness of lungs when under tensionA lung stretches easily (high compliance) does notA lung stretches easily (high compliance), does not necessary mean that it will return to its resting volume when the stretching force is release (elastance).The greater the amount of elastic tissue, the greater the elastance (elastic recoil force), but the lower the complianceFactors that affect Compliance:Factors that affect Compliance:
Elastic fibers in the alveoli Pulmonary surfactant in the alveolar fluid
23

Pressure-Volume Curverelating lung volume changes to changes in transpulmonaryrelating lung volume changes to changes in transpulmonarypressure,
the inspiratory compliance curve and the expiratory compliance curvei ll d th li di f th lis called the compliance diagram of the lungsThe characteristics of the compliance diagram are determined by the elastic forces of the lungs:
elastic forces of the lung tissue itself andelastic forces caused by surface tension of the fluid
Figure: Compliance Diagram of the Lungs
24

Pressure-Volume CurveCompliance diagrams of saline filled and air filledCompliance diagrams of saline-filled and air-filled.
The compliance diagram of the lungs demonstrate three important features
Th l l ti hi i liThe pressure–volume relationship is nonlinear changes with volume, the air curves show hysteresis, i.e., a difference between inflation and deflation, the curves are different for inflation with air and salinethe curves are different for inflation with air and saline
The curves also show the work required to expand air-filled and saline-filled lungs
It requires less work/pressure to expandIt requires less work/pressure to expandsaline-filled lung compared to air-filled lungsthe surface tension effect is not present,only tissue elastic forces are operative inonly tissue elastic forces are operative in the saline solution–filled lung
.

Pressure-Volume Curve (cont’)The transpleural pressures required to expand air-filled lungs are about three times as great as those required to expand saline solution–filled lungsgThis shows that the tissue elastic forces tending to cause collapse of the air-filled lung represent only about one third of the total lung elasticity, whereas the fluid-air surface tension g y,forces in the alveoli represent about two thirds
Comparison of the compliance diagrams of
26
p p gsaline-filled and air-filled lungs

Alveolar Surface TensionThin layer of fluid in alveoli causes inwardly directed force alveolar surface tensionCauses alveoli to remain as small as possible
27

SurfactantS f ti t i l t th t i ibl fSurface acting material or agent that is responsible for lowering the surface tension of a fluid is called surfactant. The surfactant present in the alveoli of lungs prevents the p g pcollapsing tendency of lungs. It is secreted by type II alveolar epithelial cells (surfactant secreting alveolar cells or pneumocytes)secreting alveolar cells or pneumocytes). Composition of surfactant:
Phospholipids & other lipids (90-95%), Proteins (alb globulin surfactant proteins)Proteins (alb, globulin, surfactant proteins)Carbohydrate, and ions.
28
SurfactantFunctions:
The surfactant reduces the surface tension in the alveoli of lungs and thereby prevents the collapsing tendency of lungs. The surfactant is responsible for stabilization of theThe surfactant is responsible for stabilization of the alveoli, which have the tendency to deflate. It plays an important role in the inflation of lungs during birth. The deficiency of surfactant causes respiratory distress syndrome or hyaline membrane disease (indistress syndrome or hyaline membrane disease (in infants) and adult respiratory distress syndrome (in adults).
29

Function of surfactantpromote alveolar stability
Alveoli are not bubbles, they are interdependent network of air resembling a sponge; tendency of one alveolus to collapse is opposed by elastic forces in adjacent alveoli
30
collapse is opposed by elastic forces in adjacent alveoli resisting further expansion

Function of surfactantReduce surface tension at low lung volumes (prevent atelectasis/lung collapse)collapse)
Surface tension tends to shrink the surface area and tends to decrease alveolar volume
The law of LaPlace relates the surface tension (T) and pressure (P) in a gas-filled, liquid-lined sphere with radius r;
P = 2T/rPressures inside the alveoli are inversely y
proportional to their radiusTherefore, smaller alveoli would collapse
and empty into larger alveoli if the
31
p y gsurface tension were equal in both alveoli

Function of surfactantReduce pulmonary capillary infiltration (keep alveoli dry)y)Surfactant reduces the transudation of liquid into the
alveolus by increasing the interstitial pressure to -4 mmHg (without surfactant pressure is 23 mmHg)mmHg (without surfactant, pressure is -23 mmHg)
32

Airway ResistanceyAirway resistance, Raw= ΔP/V Where, ΔP = pressure difference, (ΔP= Pmouth-Palveoli ) and
V = volume of airflow
Poiseuille-Hagen formula, air flowg ,V= ΔPπr4/8ηl
Where, r =radius of tube, η = viscosity, and l = length of the tubetube
Therefore, Raw =8ηl/πr4
Radius of the tube has critical importanceRadius of the tube has critical importance
33

Factors affecting airway resistance
Lung volumeLung volumeTone of the bronchial smooth muscleAirway generation y gType of flow
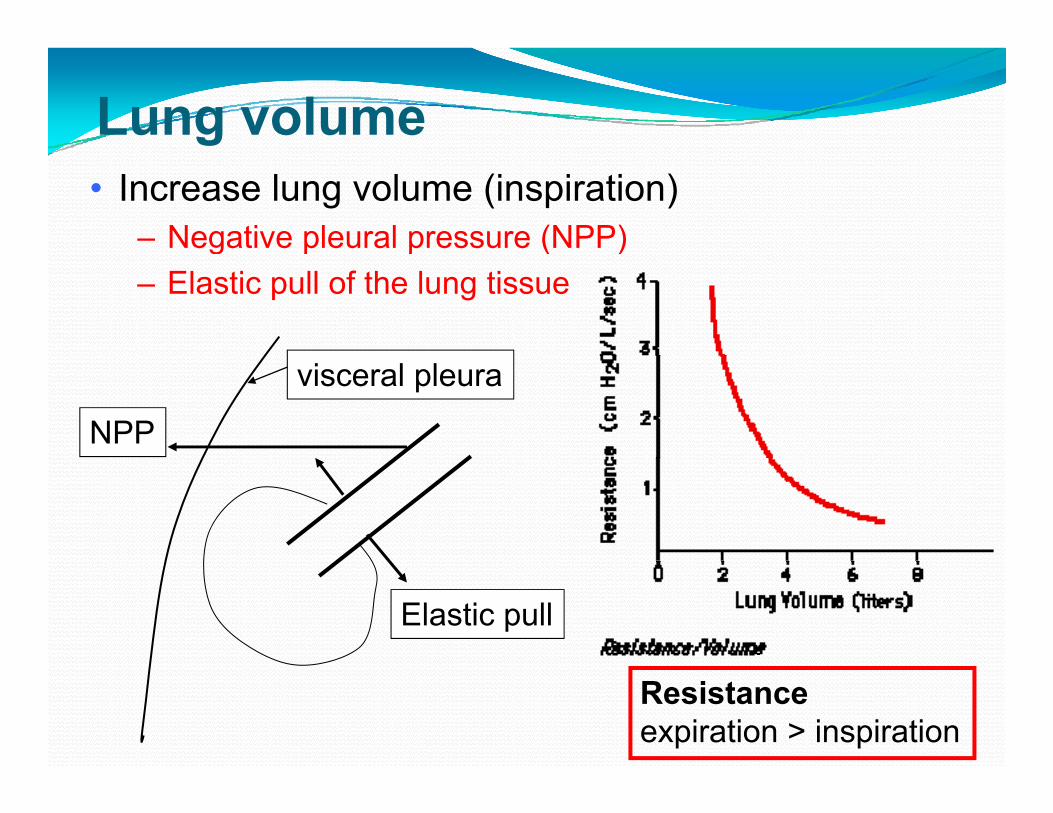
Lung volume• Increase lung volume (inspiration)
– Negative pleural pressure (NPP)g p p ( )– Elastic pull of the lung tissue
NPP
visceral pleura
Elastic pull
Resistanceexpiration > inspiration

Tone of the bronchial smooth muscler (airway diameter) is the primary determinantSmooth muscle tone responds to many stimulip y
Stimulus Bronchial constriction
Bronchial relaxation
Neural cholinergic β2 adrenergic
Neurohumoral acetylcholine norepinephrine
Chemical histamine prostaglandin EChemical histamine, leukotriene
prostaglandin E2
Physical smoke, dust
36
y ,

Airway generationTrachea and bigger airways upto 7th generation - 80% of RawTh hi h t i l i t iThe highest regional resistance is at generation 4, medium sized bronchi of short length and f b hi hfrequent branching, have an extreme turbulence Small airways represent silent zoneIn disease conditions, the smaller bronchioles often determine air flow resistance because of their smaller size (easily obstruct) and have greater % of smooth muscle gin the walls (easily constrict)
37

Type of flowResistance of turbulent flow is effectively greater than of laminar flowlaminar flowMedium sized bronchi of short length and frequent branching,
Laminar (streamlined flow)have an extreme turbulence
Turbulent flow in Central Airways

Measures of airway resistanceyAirflow - plethysmography
Force expiratory volume during the first secondForce expiratory volume during the first second(FEV1)
P k i t fl t (PEFR)Peak expiratory flow rate (PEFR)

Work of BreathinggThe work of breathing is best displayed on a pressure-volume curve. The total work of breathing of the cycle is the area contained in the loop.Work done by respiratory musclesIn normal breathing, most energy is used to expand lungsDuring heavy breathing most energy is used toDuring heavy breathing, most energy is used to overcome airway resistance
40
Work of BreathingWork of inspiration can be divided into three fractions
Compliance or elastic work (60-65%)required expanding the lungs against the lung and chest elastic forceselastic forces
Frictional work (28-35%) required overcoming airway resistance during the movement of air into the lungs
Tissue resistance work (2-7%)required overcoming the viscosity of the lung and chestrequired overcoming the viscosity of the lung and chest wall structures
41



















![2009222038 phase1[1]](https://img.dokumen.tips/doc/110x75/577d1fe31a28ab4e1e918ab5/2009222038-phase11.jpg)









