Embed Size (px)
Citation preview

McMaster Clinical Education Guidelines Version Date: December 2010
1
Clinical Educational Guideline for the diagnosis and treatment of Acute Coronary Syndrome. Authors: Teresa Chan*, Damon Atrie*, Claire Kenny-Scherber*, Julien Payrastre* Committee members: Julian Owen, Jay MacDonald∂, Karen Schiff∂, Suneel Upadhye∂, **, Bandar Baw*. *Resident, Royal College Emergency Medicine program, Michael G. DeGroote School of Medicine, McMaster University. ∂Assistant Clinical Professor, Department of Medicine, Michael G. DeGroote School of Medicine, McMaster University. ** Associate Member, Dept. of Clinical Epidemiology, McMaster University. G. DeGroote School of Medicine, McMaster University.
Last Edit: December 2010
Introduction
This series of Clinical Education Guidelines focus on teaching Evidence-Based Medicine to medical students who are preparing to embark into residency programs of Emergency Medicine and those junior learners who are seeking up to date information while doing clinical rotation in the Emergency departments. Based on Problem-Based Learning (PBL), the guidelines adapt the presenting complaints to the emergency department as fulcrums to explore each emergency differential diagnosis separately. The first edition of this series is anchored by the presenting complain of undifferentiated chest pain. Chest pain is one of the top five most common presenting symptoms to the emergency department1. More than 50% of these patients are admitted to the hospital with diagnosis spectrum of non-specific “Chest pain”2. These guidelines were not designed to alter this number but rather it was intended to be an educational tool to help the emergency medicine learners especially at their initial steps. It also serves as a cornerstone for an Evidence-Based Curriculum of Emergency Medicine for clinical clerks. This guideline is expected to be followed by subsequent guidelines of other presenting complaints to the emergency department. Methodology
The detailed methodology of this project is documented separately. The following is a brief summary of the methodology of development for these guidelines. Initially clinical diagnoses of undifferentiated chest pain were ranked by emergency medicine attending physicians in terms of their importance for clinical clerks using Likert scales. The top five differential diagnoses were Acute Coronary Syndrome (ACS), Community Acquired Pneumonia (CAP), Acute Aortic Dissection (AAD), Pneumothorax (PTX), and Pulmonary Embolism (PE). Current guidelines, recent literature and reviews were then compiled, then were used by the authors to create the clinical education guidelines for each topic. The evidence was then reviewed by the committee members and a consensus was reached for recommendations and levels of evidence. Three main clinical questions were answered. For instance if with talking about ACS then the main three questions were:
1- What are the important elements of clinical assessment (history/physical examination) utilized in the diagnosis of ACS?
2- What are the important elements of investigations and risk assessment of ACS?
3- What are the important initial interventions for treating ACS in the ED?
Strength of Recommendation (SOR) and Level of Evidence (LOE):
The Clinical Education Guidelines for undifferentiated chest pain study group agreed to use the GRADE (Grading of Recommendations Assessment, Development and Evaluation) as its grading system3. The Level of Evidence (LOE) in the GRADE system is classified into one of four levels: High, Moderate, Low or very low quality. It is based on the study type i.e. Randomized Controlled Trials (RCTs) versus observational studies and can be either upgraded or down graded according to multiple factors including effect size, variability in the results and critical outcomes4. The GRADE system classifies recommendations as either (strong or weak for using) or (strong or weak against using) the intervention5. These recommendations are not based on LOE only but on the patient’s values and preferences and other management strategies also. Introduction to this Topic Acute Coronary Syndrome (ACS) is a spectrum of diseases including ST-Elevation Myocardial Infarction (STEMI), Non- ST-Elevation Myocardial Infarction (NSTEMI), Stable Angina (SA), Unstable Angina (UA), and Prinz Metal Angina. The common pathological features underlying ACS is diminished coronary blood supply that fails to meet the demand of the myocardial muscles, which leads to ischemia or infarction. ACS is one of the few diagnoses in medicine that attracted researchers’ attention and underwent extensive studies specially the management part of STEMI and NSTEMI. Although chest pain is the most common presenting complaint of ACS to the emergency department, about one third of MI patients present to ED with symptoms other than chest pain.25 These patients usually present late with “angina equivalents” including: shortness of breath, syncope/presyncope, weakness, and sweating.

McMaster Clinical Education Guidelines Draft Copy – Version 10.0, December 2010
2
CRITICAL QUESTION 1.1 What are the important risk factors and elements of history that the learner should identify when determining the likelihood of ACS when assessing an adult patient with undifferentiated chest pain in the ED? Patient Management Recommendations Strong Recommendation for Usage, High LOE 1.1.1 Every patient with suspected ACS should have their vital signs
measured and undergo a thorough cardiovascular and chest examination.6
1.1.2 Diabetes; defined as history of diabetes regardless of duration of
disease, need for medication, or a fasting blood sugar greater than 7 mmol/l; is an independent risk factor in patients with UA/NSTEMI.6
Strong Recommendation for Usage, Moderate LOE 1.1.3 Positive history of prior MI, angina, CABG, or PCI is important. History
should elucidate type of chest pain, associated symptoms, specific sex and age-related differences, HTN, pertinent negatives for differentials of chest pain, risk of bleeding, and clinical signs of cerebrovascular disease.7,8
Summary of Important Elements of History The most important aspects of history are to delineate past medical history of diabetes, prior CAD/CABG/PCI, HTN, and sex and age related differences in ACS presentation. It is also important to consider the differential diagnosis of chest pain and note pertinent negatives on history, making other differentials less likely. Risk of bleeding and history or symptoms of CVD are important to note as they will modify treatment options. Pertinent Information on History More detailed information about pertinent elements on history in evaluating the likelihood of ACS in an adult presenting in the emergency department with chest pain. Table 1.1 Pertinent History When Evaluating a Patient for STEMI 7,9 Sign/Symptom Description Chest Discomfort Graded on scale of 1 to 10, crushing pain/heartburn, substernal
location +/- originate/radiation to neck, jaw, interscapular area, upper extremities, and epigastrum, duration > 30 min, wax and wane, remitting
Associated Symptoms
Nausea, vomiting, diaphoresis, weakness, profound fatigue, dizziness, lightheadedness, syncope, paresthesia
Sex/Age Women: sx of STEMI at older age/later after onset of symptoms, elderly less likely to complain of chest discomfort, more likely SOB, syncope, nausea
DM Impaired pain recognition, ++ with automonic neuropathy, may interpret SOB, nausea, vomiting, fatigue, diaphoresis as high/low glucose
CVD Past hx TIA, amaurosis fugax, face/limb weakness/clumsiness, face/limb numbness/sensory loss, ataxia, vertigo, ischemic stroke, ICH, SAH, dementia/cognitive impairment
Table 1.2 | Differential Diagnosis of STEMI7
Condition Classical Presentation Aortic Dissection Searing/ripping/tearing CP radiates to back/lower
extremities, worse at onset, lasts for hours, major pulses absent, +/- AR murmur
Peptic Ulcer Disease Chest/epigastric pain, +/- posterior radiation, syncope, hematemesis, melena
Pericarditis Pleuritic pain, +/- radiation to shoulder, relieved by sitting up/leaning forward, pericardial rub
Pulmonary Embolus SOB, pleuritic pain, hemoptysis Costochrondritis Sharp, knife-like pain, localized tenderness Pneumothorax Acute SOB, pleuritic pain, decrease in breath sounds,
hyperresonance over one lung field
Table 1.3 | Pertinent Positives on History in Evaluating ACS6,8 Risk Factor Definition/Comment Gender Men and women present differently, men with UA have less
favourable outcomes Age Elderly increased risk underlying multivessel CAD, worse
outcomes Prior angina Chest/arm pain/discomfort similar to prior episodes of
documented angina Prior MI High risk of obstructive CAD and multivessel disease Prior CHF Hx of SOB, fluid retention, low cardiac output, crackles, JVD,
pulmonary edema, higher risk of ACS Prior PCI PCI (balloon angioplasty, atherectomy, stent, or other) before
current presentation Post CABG Higher risk of extensive CAD and LV dysfunction, ~20% pts
presenting with UA/NSTEMI have previous CABG Stenosis >50% CAD at coronary angiography with >50% stenosis in a major
coronary artery Stroke Loss of neurological function caused by ischemic event, residual
symptoms >24 hrs after onset TIA Focal neurological deficit, resolved spontaneously without
symptoms by 24 hrs PVD Claudication with exercise or at rest, amputation for arterial
vascular insufficiency, vascular reconstruction, bypass surgery, or percutaneous intervention to the extremities, aortic aneurysm, ankle brachial index less than 0.8, bruits
HTN HTN diagnosed and treated with medication, diet, and/or exercise, BP >140/90 on 2 occasions, use of antihypertensive medications, increased risk of ACS, poor outcome
Smoking Hx cigarette smoking: current, recent, former, never Dyslipidemia Hx dyslipidemia diagnosed and/or tx by physician. Family Hx Blood relatives with angina, MI, sudden cardiac death, <55 years COPD Hx COPD/tx with pharmacological therapy/ FEV1 < 75%, room air
pO2 < 60%, or room air pCO2 > 50%, acute worsening of COPD may intensify ischemic symptoms
Anginal Episodes # episodes of angina in last 24 hours, changes in duration, frequency, and intensity
Secondary causes of angina
Fever, anemia, hypoxemia, tachycardia, thyrotoxicosis, severe valvular disease
CRITICAL QUESTION 1.2 What are the important aspects of the physical exam that the learner should identify when determining the likelihood of ACS when assessing an adult patient with undifferentiated chest pain in the ED?
Patient Management Recommendations
Strong Recommendation for Usage, Moderate LOE 1.2.1 Physical exam should include ABCs, vital signs, general observation,
jugular venous distention, pulmonary rales, cardiac murmurs and gallops, stroke, pulses, systemic hypoperfusion. A brief, focused, and limited neurological examination looking for prior stroke/cognitive deficits should be performed on STEMI patients before administration of fibrinolytic therapy.7
Pertinent Information on Physical Examination More detailed information about pertinent elements on physical examination in evaluating the likelihood of ACS in an adult presenting in the emergency department with chest pain.

McMaster Clinical Education Guidelines Draft Copy – Version 10.0, December 2010
3
Table 1.4 Physical Exam Findings in ACS7,9 General Restless, agitated, clenched fist
Vitals Low-grade fever, small volume pulses, fast, slow, or irregular pulse (atrial or ventricular arrythmias, heart block), HTN and tachycardia (increased sympathetic tone with anterior MI), hypotension and bradycardia (increased vagal tone with inferior-posterior MI)
Skin Cool, clammy, pale, cyanotic
CVS Anterior MI → may lead to ventricular aneurysm or LV dyskinesis →Paroxismal “ectopic” systolic impulse, first degree AV block, decreased LV contractility → soft S1 Decreased LV compliance → S4 gallop LBBB → severe LV dysfunction → paradoxically split S2 CHF indicates severe LV dysfunction → S3 gallop, pulmonary rales, pulses alternans, peripheral edema RV infarct → JVD, Kussmaul's sign, → BP, RV S3 and S4 gallops, clear lungs Papillary muscle rupture → VSR systolic murmur, LSB thrill, MR systolic murmur Transmural MI/ Dressler's syndrome → pericardial friction rub Cardiac rupture →cardiac tamponade Aortic dissection → AR murmur, absent pulses
CNS Altered mental status
Renal Oliguria
Table 1.5 Screening Neurological Exam Findings in STEMI7
Cognitive Memory loss, dysarthria, aphasia, hemispatial neglect Motor Facial asymmetry, pronotor drift, reflex symmetry, limb dysmetria Sensory Loss of sensation to pinprick
Table 1.6 Characteristics of Sequelae of MI7 Injury Ventricular Septal
Rupture Ventricular Free Wall Rupture
Papillary Muscle Rupture
Time course
Bimodal peak: <24 hours, 3-5 days
Bimodal peak: <24 hours, 3-5 days
Bimodal peak: <24 hours, 3-5 days
Signs CP, SOB, ↓BP Anginal, pleuritic, or pericardial chest pain, syncope, ↓BP, arrythmia, nausea, restless, sudden death
Abrupt onset SOB, pulmonary edema, ↓BP
Physical Exam
Harsh holosystolic murmur, thrill, S3, loud S2, pulmonary edema, RV and LV failure, cardiogenic shock
JVD, pulsus paradoxus, EM dissociation, cardiogenic shock
Soft murmur, no thrill, RV overload, severe pulmonary edema, cardiogenic shock
Table 1.7 Clinical Features That Increase the Probability of MI
Clinical Feature Positive LR (95% CI)
Chest Pain Radiation
Both arms 9.7 (4.6-20) 11 Left arm 2.2 (1.6-3.1) 11 Right shoulder 2.9 (1.4-6.0) 11
Sweating 2.92 (CI Value not available)12 S3 3.2 (1.6-6.5) 11 SBP < 80 3.1 (1.8-5.2) 11 Pulmonary crackles 2.1 (1.4-3.1) 11 Diaphoresis 2.0 (1.9-2.2) 11 Nausea/Vomiting 1.9 (1.7-2.3) 11 History of MI 1.5-3.0 (CI Value not available) 11
Table 1.8 Clinical Features That Decrease the Probability of MI
Clinical Feature Negative LR (95% CI) Pleuritic chest pain 0.2 (0.2-0.3) 11 Sharp/Stabbing chest pain 0.3 (0.2-0.5) 11 Positional chest pain 0.3 (0.2-0.4) 11 Chest pain reproduced by palpation 0.2-0.411
Current Controversies: Likelihood ratios (LR) of the other signs and symptoms were even lower and could not be used to exclude acute MI or ACS. In patients with low, moderate, and high pre-test probability of AMI the presence of the signs and symptoms listed above is insufficient to definitively confirm acute myocardial infarction. Bottom Line: Based on the JAMA Rational Clinical Exam article and this meta-analysis, the only important finding is pain radiating down both arms. There is no clinically significant role for other signs and symptoms in the diagnosis of AMI or ACS. Chest-wall tenderness on palpation, pleuritic chest pain, positional chest pain, and sharp/stabbing chest pain are useful in ruling out AMI or ACS in low-prevalence settings.
CRITICAL QUESTION 2.0 What are the key diagnostic tests that can aid the student in confirming or rejecting the diagnosis of ACS when assessing an adult patient with undifferentiated chest pain in the ED? The presentation of ACS can vary from clinically evident to extremely subtle. So far we have discussed some of the signs and symptoms that a patients may present with. It is often taught that 90% of a diagnosis in medicine is made based on the history and 10% on the physical exam. In this model, the diagnostic test exists to confirm your diagnosis. Although this is mostly true of STEMI, the technical diagnosis rests on the electrocardiographical (ECG) finding of ST segment elevation. In this section we will cover the evidence behind risk stratification, ECG interpretation, and biomarkers. In other words, we will discuss the diagnosis of ACS. CRITICAL QUESTION 2.1 How should the ECG be used in ACS? Patient Management Recommendations Strong Recommendation for Usage, High LOE 2.1.1 One millimeter of ST elevation in two contiguous leads is concerning for STEMI.7
2.1.2 A 15 lead ECG should be performed in any patient suspected of having an inferior MI. 7 ST elevation of 1mm in V1 and in V4R is the most predictive finding for right ventricular ischemia7 Strong Recommendation for Usage, Moderate LOE 2.1.3 Appropriately trained EMS should do a 12-lead on any patient suspected of having a STEMI. 7 2.1.4 A physician should interpret a patient’s ECG within 10 minutes of arrival. 7
2.1.5 50% of the time, these ST changes will disappear within 10 hours.7 2.1.6 Serial ECGs should be preformed every 5-10 minutes or continual ECG monitoring should be performed if the index of suspicion for STEMI remains high but the first ECG is not diagnostic. 7 Bottom Line: The ECG in ACS Often, during ACS a patient’s first contact with the medical system is with EMS. The AHA recommends that if they are trained to do so, EMS should perform a 12-lead ECG. Once in the department the patient should have an ECG within 10 minutes. The ECG should be interpreted with special attention to the ST segment looking for any elevation or depression. ST elevation of 1mm in two consecutive leads, or 2mm in one lead should raise concern for STEMI. Inverted T-waves or ST depression may indicate an NSTEMI/UA. If possible, the patient’s ECG should be compared to a previous ECG, looking for any new or dynamic changes. If the
McMaster Clinical Education Guidelines Draft Copy – Version 10.0, December 2010
4
patient has findings consistent with an inferior MI then a 15-lead ECG should be done to look for RV involvement. If there are no findings of STEMI on the ECG but the clinician continues to be concerned that STEMI may be occurring then serial ECGs should be performed at 5-10 minute intervals. Finally, a normal ECG does not rule out ACS as 1-6% of suspected patients end up having an NSTEMI and a further 4% are diagnosed with UA. 7
CRITICAL QUESTION 2.2 How should cardiac markers be used in suspected ACS? Patient Management Recommendations Strong Recommendation for Usage, High LOE 2.2.1 Cardiac serum markers should be part of the management of STEMI but not delay therapy.7 2.2.2 Cardiac serum markers cannot be used to include or exclude acute non-AMI coronary syndromes.13 2.2.3 At 8hrs, a single negative CK-MB, TnT, or TnI has a sensitivity of 90% and at 12 hours it is nearly 100% sensitive in NSTEMI.13
Strong Recommendation for Usage, Moderate LOE 2.2.4 The optimum biomarkers in STEMI are the cardiac Troponin T (cTnT) and Troponin I (cTnI).7 Bottom Line: Cardiac Markers in ACS The use of cardiac markers is an integral part of the ACS work-up. Although less important in STEMI, it separates the diagnosis of NSTEMI from UA. Of note, waiting for results of cardiac markers should not delay the management of STEMI. The 2004 ACC/AHA STEMI guidelines state that cardiac troponin is the optimum biomarker for MI. the GUSTO III trial showed that troponin elevated within 6 hours of symptom onset was associated with higher mortality. However, it may take as long as 8-12 hours for the troponin to rise after an MI, so values should be re-tested at this interval. Finally, some other markers, including CK, CK-MB, and myoglobin, are sometimes discussed. Although these have interesting potential to increase sensitivity and specificity, their use has so far shown no advantage over troponin7.
CRITICAL QUESTION 2.3 How should imaging be used in suspected ACS? Patient Management Recommendations Strong Recommendation for Usage, Moderate LOE 2.3. 1 Patients suspected of ACS should have a portable chest x-ray but this should not delay reperfusion. 7 2.3.2. If a patient with ACS is suspected of having aortic dissection they should undergo an initial chest x-ray and advanced imaging as indicated to clarify the diagnosis. 7 *See Clinical Education Guideline on Acute Aortic Dissection for further details. Weak Recommendation for Usage, Low LOE 2.3.3 If the diagnosis of STEMI is unclear due to LBBB, pacemaker or other factors, then portable echocardiography is reasonable to clarify the diagnosis.7 Bottom Line: Imaging in suspected ACS Often, patients with suspected ACS will have a chest x-ray as part of their initial investigations. This x-ray is used to evaluate the presence of CHF, cardiomegaly, or mediastinal widening, as well as to search for non-cardiac causes of chest pain. The ACC/AHA guidelines state that although STEMI patients should have a chest x-ray, this should not delay reperfusion. They also state that if aortic
dissection is a possibility on the differential that this should be immediately clarified via more advanced imaging techniques. Finally, if the diagnosis of STEMI is in doubt due to an ECG confounded by LBBB, pacing or other factors, portable echocardiography to detect wall motion abnormalities is a reasonable option.
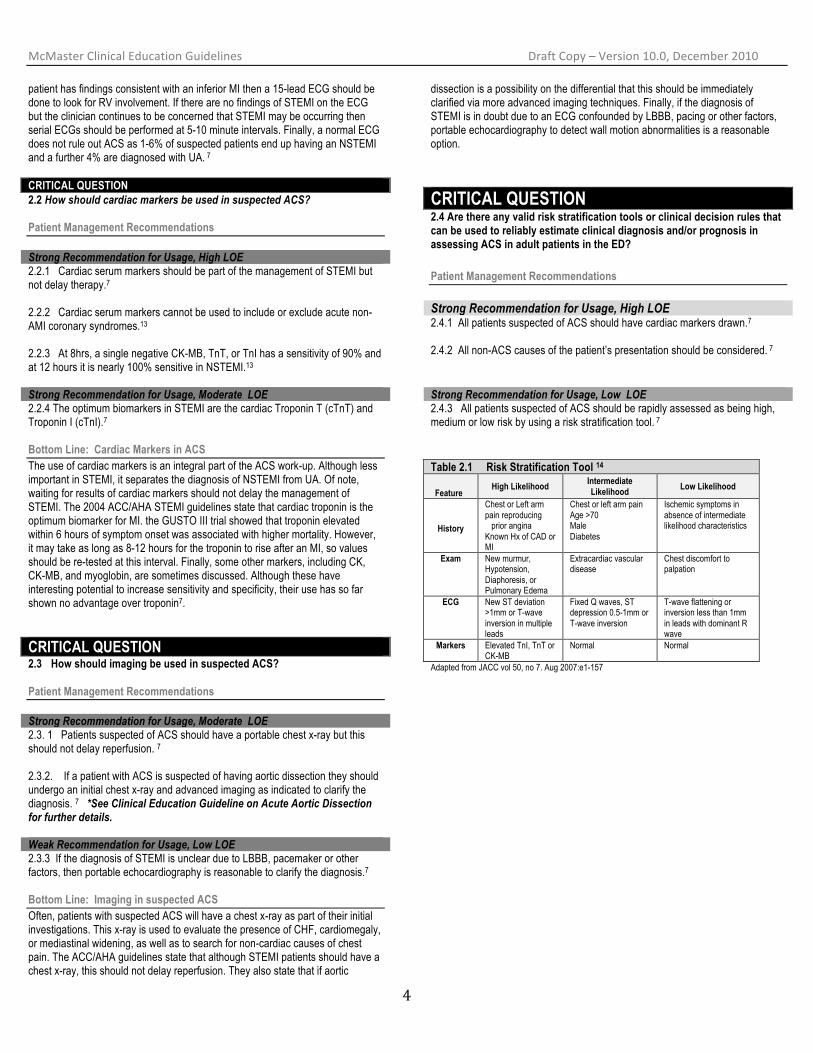
CRITICAL QUESTION 2.4 Are there any valid risk stratification tools or clinical decision rules that can be used to reliably estimate clinical diagnosis and/or prognosis in assessing ACS in adult patients in the ED? Patient Management Recommendations Strong Recommendation for Usage, High LOE 2.4.1 All patients suspected of ACS should have cardiac markers drawn.7 2.4.2 All non-ACS causes of the patient’s presentation should be considered. 7 Strong Recommendation for Usage, Low LOE 2.4.3 All patients suspected of ACS should be rapidly assessed as being high, medium or low risk by using a risk stratification tool. 7 Table 2.1 Risk Stratification Tool 14
Feature High Likelihood Intermediate
Likelihood Low Likelihood
History
Chest or Left arm pain reproducing prior angina Known Hx of CAD or MI
Chest or left arm pain Age >70 Male Diabetes
Ischemic symptoms in absence of intermediate likelihood characteristics
Exam New murmur, Hypotension, Diaphoresis, or Pulmonary Edema
Extracardiac vascular disease
Chest discomfort to palpation
ECG New ST deviation >1mm or T-wave inversion in multiple leads
Fixed Q waves, ST depression 0.5-1mm or T-wave inversion
T-wave flattening or inversion less than 1mm in leads with dominant R wave
Markers Elevated TnI, TnT or CK-MB
Normal Normal
Adapted from JACC vol 50, no 7. Aug 2007:e1-157

McMaster Clinical Education Guidelines Draft Copy – Version 10.0, December 2010
5
Table 2.2 TIMI Risk Score7 1 point each for:
• Age >65, • >2 risk factors for CAD* • prior 50% coronary stenosis • ST segment deviation at presentation • two anginal events in 24hrs • elevated cardiac markers, use of aspirin in past 7 days
TIMI Risk Score 14 day all-cause mortality, MI, or need for revascularization as a %
0-1 2 3 4 5
6-7
4.7% 8.3%
13.2% 19.9% 26.2% 40.9%
*Risk Factors defined as: Diabetes, Cigarette smoking, HTN (BP 140/90 mm Hg or on antihypertensive medication), Low HDL cholesterol, Family history of premature CAD (CAD in male first-degree relative, or father less than 55, or female first-degree relative or mother less than 65). Bottom Line: Early risk stratification is a tool that allows us to quickly assess the likelihood that a patient presenting with ACS-like symptoms does in fact have ACS. All patients suspected of ACS should be risk stratified. Table 1 is an example of how to risk stratify a patient. This stratification will affect the pre-test probability of our diagnostic tests and the eventual disposition of the patient. For example, we are more likely to admit a 90 year-old man with diabetes and previous CABG who presents with chest pain than an 18 year-old healthy male with the same complaint. The TIMI score (Table 2) is a validated tool to predict 14 day mortality from ACS. It is recommended that a score be used to help in risk stratification. In addition, all patients suspected of ACS should have cardiac markers measured. Finally, the work-up of all patients with suspected ACS should include non-cardiac causes of their symptoms. If the patient is unstable or the learner has any concerns, the attending physician should be contacted immediately.
CRITICAL QUESTION 3.0 What are the important initial interventions for treating ACS in an adult patient being assessed in the ED? The general initial treatment for the ACS consists of oxygen, nitroglycerin, cardiac monitoring, and establishment of peripheral IV lines. In addition, the medical student should also be familiar with the specific initial treatment of ACS. These specific treatments are gathered in one mnemonic: ABC of ACS. For the purposes of clarity and flow, the upcoming section is going to discuss the treatment of the separate classes of ACS in sequence:
1. STEMI (ST-elevation myocardial infarction) 2. NSTEMI/UA (non-ST elevation myocardial infarction/unstable
angina) Subsection 1 | STEMI 3.0: Subsection 1 - What is the management of ST-Elevation Myocardial Infarction (STEMI)? CLINICAL QUESTION 3.1 What is the role of anti-platelet therapies in the setting of STEMI? Other than Acetylsalicylic Acid (ASA), what are alternative antiplatelet agents and what are the indications for using these? Patient Management Recommendations Strong Recommendation For Usage, High LOE 3.1.1 Aspirin should be given to patients to chew who have not taken aspirin
before presentation with STEMI at a dose of 162mg. 7 Strong Recommendation For Usage, Moderate LOE 3.1.2 Clopidogrel usage in those patients who have STEMI is recommended
if the patient is to undergo an invasive management strategy such as Percutaneous Coronary Intervention (PCI). For clarification, please see section below Ancillary therapies after PCI. In patients undergoing fibrinolysis, patients are preferably given other anticoagulants (such as the Heparin class of medication). 7
Weak Recommendation Against Usage, Low LOE 3.1.3 Ibuprofen should not be used since it blocks the antiplatelet effects of
aspirin. 7 Aspirin Low dose 162mg or more produces a rapid, clinical antithrombotic effect which nearly completely stops thromboxane A2 production. Suspected STEMI should be given aspirin 162 mg in the first 24 hours, and then continued with 75-162mg daily. Chewable aspirin is more easily absorbed and data support that it is more quickly absorbed than one swallowed whole in early hours after infarct (especially if opiate therapy is given as analgesia during the STEMI treatment).
A Anti platelets Anti thrombotic, and Analgesics B Beta-blocker C Clot buster (for STEMI only)
Facts about ASA7
ASA alone for treatment of evolving acute MI has an ARR of 2.4% and RRR of 23% in 35-day mortality.
ASA + Streptokinase has an ARR of 5.2% (RRR 42%).
Fact excerpted from ACC/AHA guidelines

McMaster Clinical Education Guidelines Draft Copy – Version 10.0, December 2010
6
There is no evidence to show that there is a time-dependent relationship of aspirin on early mortality. Meta-analysis demonstrated that ASA reduces coronary reocclusion and recurrent ischemic events after fibrinolytic therapy. Alternative routes: ASA 300 mg suppositories can be used safely in patients with severe nausea and vomiting or upper GI disorders. Dosing of ASA Suspected STEMI should be given aspirin 162 mg in the first 24 hours, and then continued with 75-162mg daily. For daily maintenance doses of aspirin, there is thought to be a dose-dependent relationship for major bleeds. Data from the CURE trial shows that bleed risks was 2.0% in patients taking <100mg of aspirin, 2.3% in those with 100-200mg, 4% with >200mg per day. Bottom Line Suffice it to say that optimal anti-platelet therapy is determined by a number of factors, however, in the emergent setting the mainstay of these medications is ASA 162mg oral, chewed. CLINICAL QUESTION 3.2 What is the role of oral beta-blocker therapy in the setting of acute MI (both STEMI and UA/NSTEMI)? Patient Management Recommendations All below recommendations are for both STEMI and UA/NSTEMI unless otherwise documented. Strong Recommendation for Usage, High LOE 3.2.1 All patients after STEMI and UA/NSTEMI except those at low risk
(normal or near-normal ventricular function, successful reperfusion, absence of significant arrhythmias) and those with contraindications should receive betablocker therapy. Treatment should begin within a few days of the event, if not initiated acutely, and continue indefinitely.7, 8, 16.
Strong Recommendation Against Usage, High LOE 3.2.2 Contraindications to Betablocker therapy include14:
1) signs of heart failure, 2) evidence of low output state, 3) increased risk for cardiogenic shock, or 4) other relative contraindications to beta blockade (PR interval
greater than 0.24 seconds, second- or third-degree heart block, active asthma, or reactive airway disease).
Strong Recommendation, Moderate LOE 3.2.3 May give IV beta-blockers promptly to STEMI and UA/NSTEMI
patients without contraindications (as listed above), especially if a tachyarrhythmia or hypertension is present. 7,14
Strong Recommendation Against Usage, Moderate LOE 3.2.4 Do not administer Beta-blockers or calcium channel antagonists to
patients in a low-output state due to pump failure, signs of HF, contraindications or other risk factors for Cardiogenic Shock (e.g. age >70; Systolic BP < 120mmHg, Sinus Tachycardia >110 or HR <60; increased time since onset of symptoms of chest pain). 7,14
Beta-adrenergic blockade In the Post-MI setting Beta-adrenergic blockers (a.k.a. Beta blockers) competitively block catecholamine effect on cell-surface receptors. There are two types of Beta receptors – Beta-1 and Beta-2. Beta-1 are located mainly in the myocardium, blocking these receptors decreases sinus node rate, AV node conductivity, and myocardial contractility. Beta-2 receptors are found on smooth muscle –e.g. vascular and brochial structures – so blocking these can result in vasoconstriction & brochoconstriction. Contraindications to Beta-blockade Low Flow States: After an acute coronary occlusion, LV function may acutely decrease (due to acute rise in LV filling pressures, acute systolic/diastolic dysfunction. This can lead to rapid redistribution of fluid into the lung tissues (namely the interstitium, which may extravasate into the alveoli). Pulmonary congestion/edema occurs, and iss presence on examination or x-ray increases the risk of dying) 20-40% 30-day mortality. 14
The mainstay of management is preload reduction (nitrates, morphine, diuretics) and avoidance of negatively inotropic agents (beta-blockers, calcium channel antagonists). 14
CAVEAT: In the stable, non-acute patient with LV-dysfunction, beta-blockade is highly advised as beta-blockers are beneficial as a maintenance medication in patients with poor LV function/CHF.
Other contraindications to Beta-blocker use include14: • known severe asthma (may induce bronchospasm) • allergy
NB: With respect to the use of Beta-blockers, the guidelines and recommendations for management are virtually identical for STEMI and UA/NSTEMI. Current Controversies Currently there has been some substantial controversy over the use of beta blockers in the acute setting, which bears weight especially in the emergent treatment of both STEMI and UA/NSTEMI conditions. In the ACC/AHA guidelines of 2004, there was a blanket recommendation for the use of IV beta blockade in the first 24-hours after an acute coronary event. 7,16 Since then, the language of this statement has been amended (to include data gathered in the COMMIT study). The new 2007 update excludes those patients with contraindications such as: hypotension, low-output state, increased risk for cardiogenic shock, frank cardiac failure, heart block.14 CLINICAL QUESTION 3.3 What are the indications for fibrinolytic therapy in an adult patient being assessed for STEMI in the ED? Strong Recommendation for Usage, High LOE
COMMIT/CCS-2 (Metoprolol)
47,852 patients with suspected MI, Randomized to receive metoprolol (up to 3 doses of 5mg IV each in the first 15 minutes, then 200mg po daily) or matching placebo.
Fifteen minutes after IV doses, a 50 mg tablet of metoprolol or placebo and was administered orally, repeated q6h during Day 0 and 1 of hospitalization. Afterwards 200mg daily of controlled release.
No significant decrease of composite death, reinfarction, cardiac arrest, and death during scheduled treatment period. (per 1000 patients, 5 less reinfarction, 5 less VFib, but 11 more cardiogenic shock). Metoprolol caused more persistent hypotension, and more bradycardia.

McMaster Clinical Education Guidelines Draft Copy – Version 10.0, December 2010
7
3.3.2 In centres lacking PCI, fibrinolysis has a mortality benefit in STEMI patients with symptom (e.g. characteristic ischemic chest pain) onset within 12 hours who meet one of these conditions on ECG: ST elevation greater than 1 mm in at least 2 contiguous limb leads or greater than 2 mm in at least 2 contiguous limb leads without features of non-infarction cases of ST-elevation.
OR Presumed new onset left bundle branch block that may be obscuring ST-segment analysis in patients with a clinical picture highly consistent with MI.17
3.3.1 If a STEMI patient presents to a centre without PCI facilities, fibrinolysis should be administered if the STEMI is identified less than 3 hours after symptom onset and the expected time until PCI is obtained (“door-to-balloon time”) is greater than 90 minutes. 17
Fibrinolysis in the Setting of STEMI All of the fibrinolytic agents used in STEMI are plasminogen activators. Their mechanism of action is to expose, directly or indirectly, the active enzymatic centre of plasmin, which in turn degrades the fibrin clots responsible for STEMI. Bottom Line: Indications for Fibrinolysis Although the history and physical examination are important parts of any assessment in the ED, STEMI is a rather unique case where a diagnostic investigation (the ECG, in this case) provides most of the information about treatment. It should also be noted that although benefit can be gained up to 12 hours following onset of symptoms, STEMI is a true time-dependent emergency and the greatest benefit is seen with early administration of fibrinolysis. As such, it is not appropriate to delay treatment to confirm the diagnosis of STEMI if clinical suspicion is high. Remember, “time equals muscle”! CLINICAL QUESTION 3.4 What are the contraindications for fibrinolytic therapy? Strong Recommendation Against Usage, High LOE 3.4.1 The absolute contraindications to fibrinolytic therapy are7:
• Any prior ICH • Known structural cerebral vascular lesion (i.e. AVM) • Known malignant intracranial neoplasm (primary or metastatic) • Ischemic stroke within 3 months EXCEPT acute ischemic stroke
within 3 hours • Suspected aortic dissection • Active bleeding or bleeding diathesis (excluding menses) • Significant closed head or facial trauma within 3 months
Weak Recommendation Against Usage, Low LOE 3.4.2 The relative contraindications to fibrinolytic therapy include7:
• History of chronic severe, poorly controlled hypertension • Severe uncontrolled hypertension on presentation (SBP greater than
180 mm Hg or DBP greater than 110 mm Hg) • History of prior ischemic stroke greater than 3 months, dementia, or
known intracranial pathology not covered in contraindications • Traumatic or prolonged (greater than 10 minutes) CPR or major
surgery (less than 3 weeks) • Recent (within 2 to 4 weeks) internal bleeding • Noncompressible vascular punctures • For streptokinase/anistreplase: prior exposure (more than 5 days ago)
or prior allergic reaction to these agents • Pregnancy • Active peptic ulcer • Current use of anticoagulants: the higher the INR, the higher the risk
of bleeding Bottom Line: Contraindications & Cautions for Fibrinolysis use in STEMI7 The absolute contraindications for fibrinolysis are conditions which greatly increase the risk of hemorrhage, especially intracranial hemorrhage. As such, the absolute contraindiations for fibrinolysis in the setting of STEMI include any prior intracranial bleed, a known structural cerebrovascular abnormality (i.e. atrioventricular malformation), known malignant intracranial neoplasm, suspected aortic dissection, bleeding disorder or active bleeding, significant closed head/facial trauma within 3 months. An ischemic stroke within 3 months (but not an acute ischemic stroke within 3 hours) is also a contraindication. STEMI patients at high risk of ICH should receive PCI instead of fibrinolysis. Relative contraindications are factors which may increase the risk of hemorrhage. It is up to the clinician to administer fibrinolysis when a relative contraindication exists. The relevant contraindications for lysis in STEMI include a history of severe poorly controlled hypertension; systolic BP greater than 180 mm Hg or diastolic BP greater than 110 mm Hg on presentation to the ED, a history of prior ischemic stroke greater than 3 months, dementia, or known intracranial pathology not in the contraindications; traumatic CPR or CPR for longer than 10 minutes; major surgery within 3 weeks; internal bleeding within 2-4 weeks; noncompressible vascular punctures; prior allergic reaction to fibrinolytics; pregnancy; active peptic ulcer disease; current use of anticoagulants. CLINICAL QUESTION 3.5 How should the main complications of fibrinolytic therapy be treated? Strong Recommendation for Usage, Moderate LOE 3.5.1 If patients receiving fibrinolysis have clinical symptoms of ICH,
fibrinolytic, antiplatelet, and anticoagulant therapies should be stopped and imaging of the brain should be obtained as soon as possible.7
3.5.2 Fresh frozen plasma, cryoprecipitate, protamine, and platelet infusions
should be given and neurology and/or neurosurgery should be consulted if ICH is confirmed on imaging.7
3.5.3 Expert consultation of neuroscience specialist should be sought
emergently and management of ICP should be initiated at their discretion.7
Complications of Fibrinolysis The main complications of fibrinolytic therapy are ICH and other moderate or severe bleeding. Most of these complications occur in the first 24 hours following treatment. If the patient suffers a change in neurological status during or after

McMaster Clinical Education Guidelines Draft Copy – Version 10.0, December 2010
8
reperfusion therapy, the reason for the change is ICH until proven otherwise. ICH is treated as described above.
CLINICAL QUESTION 3.6 Which fibrinolytic should be used in STEMI? Patient Management Recommendations Strong Recommendation for Usage, Moderate LOE 3.6.1 TNK should be used for its side-effect profile and relative ease of
use.18 Choice of Fibrinolytic There are currently four thrombolytics available for use: t-PA, streptokinase, r-PA, and TNK. Though there are no guidelines governing choice, TNK has become the gold standard of use in the ED based on results from the ASSENT-2 trial. In this study, TNK was shown to be equivalent to t-PA in mortality with similar ICH rates but fewer systemic bleeding complications in the TNK Group. TNK also has the advantage of single bolus administration.18
CLINICAL QUESTION 3.7 What is the role of anticoagulants or antiplatelets if a STEMI
patient is undergoing fibrinolysis? (i.e. What ancillary therapy should be used with fibrinolysis to prevent re-thrombosis?)
Patient Management Recommendations Strong Recommendation for Usage, High LOE 3.7.1 Unfractionated heparin (UFH) should be given intravenously
following TNK, especially to patients who are at increased risk of clot formation (i.e. atrial fibrillation).7
Strong Recommendation for Usage, Moderate LOE 3.7.2 In the absence of renal failure, low-molecular weight heparin
(LMWH) can be an acceptable alternative to UFH for patients less than 75 years old.7
Weak Recommendation for Usage, Low LOE 3.7.3 Fondaparinux (2.5 mg subcutaneous daily) should be given to STEMI
patients who have been given a thrombolytic, especially those patients receiving streptokinase.19
CLINICAL QUESTION 3.8 When should Percutaneous Coronary Interventions be performed? Strong Recommendation for Usage, Moderate LOE 3.8.1 Primary PCI should be performed in patients with STEMI if it can be
done with a door-to-balloon time of 90 minutes by an experienced provider.7
3.8.2 If symptoms began within 3 hours and the expected door-to-balloon
time minus the expected door-to-needle time is within 1 hour, PCI is generally preferred as long as it can be performed expediently. If this time is greater than 1 hour, fibrinolytic therapy is generally preferred. If symptom duration is greater than 3 hours, primary PCI is generally preferred and should be performed with as short a door-to-balloon time as possible, with 90 minutes as the goal.7
Bottom Line: Primary PCI In centres capable of offering PCI, patients who receive it experience lower short-term mortality rates, lower re-infarction rates, and less hemorrhagic strokes than patients who are fibrinolysed. However, there is an increased risk for major
bleeding, of which ICH is the most catastrophic. PCI also provides the opportunity to risk-stratifying patients for future infarction since the coronary arteries are directly visualized. As mentioned above, primary PCI should be performed if it can be done with a door-to-balloon time of 90 minutes by experienced providers. However, there are often delays in getting patients to the cardiac catheterization laboratory such as practicing in a remote location. It is for this reason that the ACC and AHA have devised the recommendations above addressing issues around prolonged symptom duration. We should note that there is no evidence that routine immediate or early PCI following fibrinolysis is safe, feasible, and superior to conservative management in STEMI.20
CLINICAL QUESTION 3.9 When should facilitated PCI be performed? Patient Management Recommendations Weak Recommendation Against Usage, Moderate LOE 3.9.1 A strategy of facilitated PCI might be considered in higher-risk patients
when PCI is not immediately available.7 Bottom Line: Facilitated PCI7 Facilitated PCI is planned immediate PCI following an initial pharmacological regimen that may include fibrinolysis and antiplatelet therapy. Potential risks of this procedure include increased bleeding complications (especially in older patients). The high systemic cost of this treatment is a potential limitation to its widespread acceptance.
CLINICAL QUESTION 3.10 When should rescue PCI be performed? Strong Recommendation for Usage, High LOE 3.10.1 Within 18 hours in patients with signs of cardiac decompensation such
as CHF and cardiogenic shock.7 3.10.2 Within 12 hours for patients with sustained or recurrent myocardial
ischemia.7 Bottom Line: Rescue PCI Rescue PCI is PCI undertaken if medical therapy (i.e. fibrinolysis) has failed. Persistence of persisting ischemic chest pain, continuing ST-segment elevation, and hemodynamic and/or electrical instability are all important signs of failed fibrinolysis. In such cases, rescue PCI should be performed in accordance with the guidelines above. Although rescue PCI is associated with improved clinical outcomes for STEMI patients after failed fibrinolysis, these benefits must be interpreted in the context of potential risks. A 2007 systematic review showed that rescue PCI was associated with no significant reduction in all-cause mortality, but that it was associated with significant risk reductions in heart failure and re-infarction when compared with conservative treatment.21
CLINICAL QUESTION 3.7 What is the role of anticoagulants or antiplatelets if a STEMI
patient is undergoing PCI? (i.e. What ancillary therapy should be administered with PCI to avoid re-thrombosis?)
Patient Management Recommendations

McMaster Clinical Education Guidelines Draft Copy – Version 10.0, December 2010
9
Strong Recommendation for Usage, High LOE 3.7.4 UFH should be given to all patients receiving PCI.7 3.7.5 In patients in whom PCI is planned, oral clopidogrel should be
given.7 Weak Recommendation for Usage, Low LOE 3.7.6 If not giving UFH, fondaparinux should be considered (in consultation
with an expert) in patients undergoing PCI.22 Bottom Line: Ancillary Therapy For the same reasons discussed in the fibrinolysis section, anticoagulants and antiplatelet agents are needed in patients receiving PCI. The OASIS-5 trial showed that using upstream fondaparinux rather than enoxaparin significantly reduced the risk of major bleeding thus it is the drug of choice when PCI is planned.22 This, of course should, be discussed with an expert consultant .
ST-Elevation Myocardial Infarction Summary STEMI is the most severe type of ACS and the ED plays a crucial role in its initial management. Since time equals muscle, it follows that all patients suffering a STEMI should receive rapid evaluation for reperfusion therapy and have a reperfusion strategy implemented soon following entry into the ED.7 In general, there are two ways to achieve reperfusion in STEMI: pharmaceutical reperfusion (fibrinolysis) and angioplasty (percutaneous coronary intervention, PCI). Taking into account a host of factors including time of symptom onset, severity and location of injury, patient risk factors, and availability of timely PCI, STEMI patients must be expediently and carefully given treatment in order to effectively manage this true time-dependent emergency.

McMaster Clinical Education Guidelines Draft Copy – Version 10.0, December 2010
10
Subsection 2 | UA/NSTEMI 3.1 Subsection 2 What is the management of Unstable Angina or Non ST-elevation MI (NSTEMI)?
CRITICAL QUESTIONS 3.1 What is the role of anti-platelet therapies in the setting of
NSTEMI/UA? Other than Acetylsalicylic Acid (ASA), what are alternative antithrombotic agents and what are the indications for using these?
Strong Recommendation for Usage, High LOE 3.1.4 In UA/NSTEMI patients, aspirin should be given as soon as possible
after hospital presentation and continued as a daily dose in patients not known to be intolerant of the medication.
3.1.5 Clopidogrel (loading dose followed by daily maintenance dose*) should be given to UA/NSTEMI patients who are unable to take ASA because of hypersensitivity or major gastrointestinal intolerance. 14 *NB: Dosing for Clopidogrel is still somewhat uncertain. Current guidelines suggest 300 mg loading then 75 mg maintenance. Higher doses (600-900mg) are thought to induce more rapid antiplatelet action, but safety and efficacy is not proven. 14
3.1.6 For UA/NSTEMI patients where an initial invasive strategy is chosen,
antiplatelet therapy in addition to aspirin should be initiated before diagnostic angiography with either clopidogrel (loading dose followed by maintenance dose*) or an intravenous GP IIb/IIIa inhibitor. Consultation with accepting cardiologist should be undertaken before utilization, especially prior to PCI. In concert with your local Cardiologist, it may be reasonable to being GP IIb/IIIa inhibitor such as abciximab prior to an invasive strategy. 14 *NB: Dosing for Clopidogrel is still somewhat uncertain. Current guidelines14 suggest 300 mg loading then 75 mg maintenance. Higher doses (600-900mg) are thought to induce more rapid antiplatelet action, but safety and efficacy is not proven. 14
3.1.1.4 For UA/NSTEMI patients in where an initial conservative (i.e. non-
invasive) strategy is selected, clopidogrel (loading dose followed by daily maintenance dose) should be added to ASA and anticoagulant therapy as soon as possible after admission.
Optimal Antiplatelet therapy in UA/NSTEMI In this population, admission is indicated in order to allow the patient to undergo further diagnostic tests to determine the optimal antiplatelet regime for maintance of health. Upon admission, these patients will receive initial management including unfractionated heparins and may require PCI/Diagnostic Angiography. The patient may also undergo a stress test for further diagnostic confirmation. Select patients may be deemed candidates for coronary artery bypass graft (CABG) surgery, and this will alter their disposition upon admission. Bottom Line: Suffice it to say, that optimal anti-platelet therapy is determined by a number of factors, however, in the emergent setting the mainstay of these medications is:
1) ASA 162-325mg oral, chewed 2) Clopidogrel 300mg oral, loading dose; then 75 mg oral daily 3) If true ASA allergy – Use Clopidogrel (First Line).
CLINICAL QUESTION 3.2 What is the role of oral beta-blocker therapy in the setting of acute MI (both STEMI and UA/NSTEMI)?
Patient Management Recommendations See section 3.2 under STEMI subsection – as the management with respect to oral beta-blockers is similar.
CRITICAL QUESTIONS 3.7 What is the role of anticoagulant therapies after UA/NSTEMI? What is the anticoagulant of choice for either NSTEMI or UA? Patient Management Recommendations Strong Recommendation for Usage, High LOE 3.7.7 Anticoagulant therapy should be added to antiplatelet therapy in
UA/NSTEMI patients as soon as possible after presentation. Regardless of invasive vs. conservative strategy, use some form of anticoagulant therapy (e.g. enoxaparin, UFH or fondaparinux.)
Special Note: Anticoagulation in patients already on Warfarin For UA/NSTEMI patients who may otherwise require anticoagulation for ACS spectrum disease states, but whom are already therapeutic on warfarin, clinical judgment regarding the addition of anticoagulation. Anticoagulation after an NSTEMI or with UA The Non-STEMI (NSTEMI) and Unstable Angina (UA) are within the spectrum of Acute Coronary Syndrome (ACS). The pathophysiology of STEMI, NSTEMI and UA are similar, and usually involve an atherosclerotic plaque rupture and activation of coagulation pathways (e.g. platelets) which in turn lead to thrombus formation along exposed/damaged endothelial lining of coronary blood vessels. This occlusive event leads to an ischemic period for the myocardium – and the extent of myocardial damage dictating the subtype of ACS. The EKG changes and/or subsequent rise in biomarkers of this – i.e. Troponin or CK-MB – are a reflection of severity of ischemia in the myocardium. Understanding the pathophysiology of ACS allows one to imagine that utilizing antithombotic/anticoagulant and antiplatelet agents (in addition to anti-ischemic ones) might assist in the prevention of extended or increased myocardial damage. In fact, this is the case, as in certain patient populations, the early use of antiischemic, antithrombotic/anticoagulant and antiplatelet agents ultimately decrease the adverse sequelae such as heart failure, a second MI and death. This section will be limited to a discussion of Anticoagulation (antithrombotic) agents and their role in management of NSTEMI/UA.

McMaster Clinical Education Guidelines Draft Copy – Version 10.0, December 2010
11
The Heparins Heparin is a saccharide which inhibits the coagulation factors found innately within the blood. The options in the Emergency Department are:
a. Unfractionated Heparin (UFH) b. Low Molecular Weight Heparins (LMWH)
a. Enoxaparin b. Dalteparin c. Tinzaparin
c. Fondaparinux (which is a LMWH specifically targeting Xa) The following is a chart of their action and mechanisms:
Direct Thrombin Inhibitors There are a few other anticoagulants available for anticoagulation post-UA/NSTEMI, however, these do not play a role in the Emergency Department setting. Hirudin, the original Direct Thrombin Inhibitor, was studied in two large trials (GUSTO IIb, OASIS) and found to have some benefit but major bleeding consequences. Hirudin also causes thrombocytopenia (at the same rate as UFH) which the studies showed to have a significant increase in Death (odds ratio 6.7). Major benefit of Hirudin was its role in UA patients who were to undergo PCI (Helvetica Trial). Bivalirudin (TIMI 7, Bivalirudin Angioplasty Study) is a synthetic version of Hirudin. It has been shown to be more effective than UFH in UA patients undergoing PCI, and has a lower risk of major hemorrhage. The ACUITY trial showed that Bivalirudin required clopidogrel pre-treatment prior to PCI (unless a GP IIb/IIIa inhibitor was used instead).
CRITICAL QUESTION 3.3 When should patients receive the initial invasive strategy?
Patient Management Recommendations
Strong Recommendation for Usage, Moderate LOE 3.3.1 Patients who are identified as high-risk should receive urgent
catheterization and revascularization. 14
3.3.2 Patients who present to the ED with ongoing ischemic symptoms or hemodynamic/electrical instability should receive urgent catheterization and revascularization even if there are no ischemic ST changes within minutes to a few hours of arrival because of their level of illness.14
3.3.3 Patients who fail medical therapy (refractory angina or angina at rest or with minimal activity despite vigorous medical therapy) or in whom objective evidence of ischemia (dynamic ECG changes, high-risk stress test) is identified should undergo invasive evaluation.
Bottom Line: The Initial Treatment Strategies in UA/NSTEMI 14 Two treatment pathways exist for treating UA/NSTEMI patients: an initial invasive strategy and an initial conservative strategy. Choosing the right strategy for each individual ACS patient depends on risk stratifying for an adverse outcome. Several risk stratification tools have been validated for use in ACS patients. These are quite useful in guiding the type and intensity of therapy by identifying patients who are the most likely to benefit from more aggressive (and risky) investigation and treatment. The TIMI risk calculator, as discussed earlier, is one such tool. However, it should not be the only factor in deciding which strategy is chosen. In addition to risk stratification tools, clinicians use their judgment in initiating a pathway. For example, it should come as no surprise that the initial invasive strategy is indicated in a patient who has a left ventricular ejection fraction below 40%, a high-risk stress test, elevated troponins, and sustained ventricular tachycardia. The initial invasive strategy identifies high-risk patients and involves invasive diagnostic evaluation before undergoing a stress test or failing medical treatment first. Patients receiving the initial invasive strategy receive the appropriate UA/NSTEMI medications but also undergo coronary angiography within 4 to 24 hours of admission and revascularization will be performed if needed. If an unstable UA/NSTEMI patient presents to the ED, they should receive urgent catheterization and revascularization
Table 3.1 Heparin and Heparin-‐like Agents used in ACS Heparin Biochemical Action Notes on Usage Limitations Unfractionated Heparin (UFH)
Acts on Heparin-‐Antithrombin (a.k.a. Antithrombin III) – and increases the rate of metabolism of Thrombin (Factor II) and Factor Xa. It also acts, but on a lesser extent on, factors XIIa, XIa, and IXa.
The “original” anticoagulant. Found to be less effective than many of the other heparins. Better when it is given as an infusion. Mainly works at inhibiting the action of Thrombin & Factor Xa.
Is a large molecule. Thought to be less effective than other heparins (including LMWH, Synthetic Heparins) because it may be too large to penetrate into a clot complex and begin its action. Major Complications: -‐ major bleeding -‐ thrombocytopenia -‐ reactivation of ischemia after heparin is d/c’d
Low Molecular Weight Heparin (LMWH) Most effective Enoxaparin Also Dalteparin Tinzaparin
Acts on Heparin-‐Antithrombin (a.k.a. Antithrombin III) – and increases the rate of metabolism of Factor Xa. It does not act as strongly on Thrombin compared to UFH. (Don’t prolong aPTT)
All are dosed adjusted for weight – doesn’t need to be monitored the same way. Enoxaparin is as good as (if not better than) UFH – shown in studies including ESSENCE, TIMI 11B, SYNERGY. Dalteparin, Tinzaparin thought to be similar in efficacy to UFH.
Not as easily monitored as UFH. Not as easily reversed (important if going to PCI). If CABG is planned withint 24 hours, UFH is preferred over both fondaparinux/enoxaprin.
Fondaparinux OASIS-‐5 trial
The synthetic heparin pentasaccharide fondaparinux, acts through antithrombin to exclusively neutralize factor Xa.
OASIS-‐5 showed similar efficacy to Enoxaprin. Had a significantly decreased amount of bleeding.
If CABG is planned withint 24 hours, UFH is preferred over both fondaparinux/enoxaprin.
Above summarized from ACC/AHA 2007 Guidelines ad www.uptodate.com1 NB: A caution about making direct comparisons between the agents is the relative age of each of these heparin-‐related therapies. UFH studies were mainly done prior to the advent of clopidigrel. The combination therapies of ASA + clopidogrel were not standard of care, as they are now, and therefore the outcomes of these studies cannot be compared fairly.

McMaster Clinical Education Guidelines Draft Copy – Version 10.0, December 2010
12
even without ECG changes. The initial conservative strategy, on the other hand, involves initiating an invasive evaluation only if the patient remains symptomatic after a trial of medical therapy or if there is objective evidence of myocardial ischemia, such as dynamic ECG changes or a high-risk stress test. In summary, all patients receive coronary angiography in the invasive stream but those who are identified as high-risk or unstable will receive it more urgently than others. Figure 1 displays the algorithms for both treatment strategies in UA/NSTEMI. Figure 1: UA/NSTEMI Algorithm for Invasive vs. Conservative Management Algorithm for early invasive vs. early conservative management strategies in NSTEMI/UA. Adapted from Anderson et al (2007).
CLINICAL QUESTION 3.2.5 Is there a mortality benefit when using the early invasive
strategy?
Patient Management Recommendations
Strong Recommendation for Usage, High LOE 3.2.5.1 Cochrane Review16 concluded that an early invasive strategy is
preferable to a conservative strategy in the treatment of UA/NSTEMI. Mortality and MI assessed at 2-5 years in two trials were significantly decreased by an invasive strategy. The composite endpoint of death or non-fatal MI was significantly decreased by an invasive strategy. The incidence of refractory angina were both significantly decreased by an invasive strategy, as were early and intermediate rehospitalization rates.16
UA/NSTEMI Summary
UA/NSTEMI are common within the ACS spectrum – and in the emergency department, early diagnosis & management can decrease the morbidity and mortality from this condition. With this condition, it is even more important to establish key historical and physical exam features as the diagnosis of UA and NSTEMI are harder than at the other end of the ACS spectrum. Diagnoses do play a role as Cardiac Markers are very key in determining NSTEMI, but with UA, often you history and exam are the most crucial elements for diagnosis. As with STEMI, time equals muscle, and early usage of antiplatelet or anticoagulation therapies can optimize patients whether or not they are undergoing early conservative medical management or PCI.

McMaster Clinical Education Guidelines Draft Copy – Version 10.0, December 2010
13
CRITICAL QUESTION 3.8 What are the optimal initial adjunctive management strategies for Acute Coronary Syndrome (ACS)? Initial Management of ACS There are certain adjunctive therapies to ACS management which are famously ubiquitous and commonplace – however are not supported by evidence as many of the other previously discussed therapies. To this point, we have only discussed the “A” (aspirin) in the well-known “MONA” mnemonic – since it is the only therapy within this classic management of ACS that has been supported by strong evidence. Below is a discussion of the other adjunctive therapies including Oxygen, Nitrates and Morphine/Opioid therapies for pain-control.
CLINICAL QUESTION 3.8.1 What is the role of adjunctive therapies such as Oxygen? Strong Recommendation for Usage, High LOE 3.8.1.1 Supplemental oxygen (by mask or by nasal prongs) should be given to
patients who have an arterial oxygen saturation of less than 94% and evidence of respiratory distress.
Current Controversy To date, the major international guidelines on ACS (AHA/ACC, ESC) have suggested that the delivery of oxygen be utilized based on animal studies (on canine specimens). No major human trial exists, however a recent metaanalysis (Wijesinghe et al., 2009) suggests that there are very few studies looking at the risk/harm relationship of supplemental oxygen – and the authors of this paper suggest that the use of oxygen supplementation in uncomplicated MI may increase infarction and possibly increase mortality because of alterations to hemodynamics (i.e. decrease coronary blood flow). Bottom Line: The role of oxygen, its long-/short-term outcomes, its effects on human hemodynamics and its role in the initial acute coronary syndrome management has recently been called into question. For now, its use should be limited to those patients with clinical evidence of respiratory distress and an oxygen saturation of 94% or less, but the evidence to support its use is minimal, and there is likely a role for further study in the area.
CLINICAL QUESTION 3.8.2 What is the role of adjunctive therapies such as IV Nitroglycerin?
Strong Recommendation for Usage, Low LOE 3.8.2.1 Patients with ACS (STEMI, NSTEMI, UA) with ongoing ischemic pain
or discomfort should receive sublingual nitroglycerin (NTG) at a dose of 0.4mg every 5 minutes for a total of 3 doses. After the three doses, if pain or discomfort persists, patient should be assessed (including for contraindications) for intravenous (IV) NTG. 14
3.8.2.2 In the setting of ACS, intravenous NTG therapy should be given for
the following indications: a. ongoing ischemic discomfort
b. control of hypertension c. management of heart failure or pulmonary congestion. 14
3.8.2.3 The delivery of NTG therapy should not prevent the delivery of other proven mortality-reducing interventions (i.e. Aspirin, Beta-blocker). 14
Strong Recommendation Against Usage, High LOE 3.8.2.4 Nitrates should not be administered to patients with:
a.hypotension (Systolic BP < 90mmHg or 30mmHg below baseline), b. severe bradycardia ( < 50 beats per minute[bpm])
c. tachycardia (> 100 bpm) d. suspected RV infarct. 14
Strong Recommendation Against Usage, Moderate LOE 3.8.2.5 Intravenous NTG therapy is contraindicated after the recent use of
phosphodiesterase inhibitor. Use of sildenafil within the last 24 hours, or tadalafil within the last 48 hrs are considered contraindication of intravenous NTG. Time for administration of nitrates post-vardenafil has not been determined.14
Nitroglycerin and Why it Works The biological rationale behind nitroglycerine (NTG) is that it:
• reduces myocardial oxygen demand (peripheral vasodilation à increased venous capacitance à venous pooling à decreased preload à decreased ventricular tension)
• enhances oxygen delivery to the myocardium by promoting dilataton of large coronary arteries (since normal flow-mediated dilation does not occur well in atherosclerotic coronary vasculature).
• Possibly has inhibitory affects on platelet aggregation The evidence behind the use of this therapy is not strong. The majority of studies are small, and there was a suggested 35% reduction in mortality rates in early pre-fibrinolytic era trials, but newer studies (including the Italian GISSI-3 trial) post-reperfusion techniques have failed to show benefit. The 2007 ACC/AHA guidelines on UA/NSTEMI explain that rationale for using NTG in UA/NSTEMI is extrapolated from biological plausibility and clinical experience. Contraindications The use of IV nitroglycerin therapy should not be initiated if: • The patient has recently used a phosophodiesterase inhibitor. These
agents inhibit an enzyme (phosphodiesterase) which degrades cyclic guanosine monophosphate (cGMP). cGMP is a regulator for vascular smooth muscle relaxation by nitric oxide. Without regulation of phosphodiesterase, there is a prolonged and exaggerated response to nitrates (including symptoms such as profound hypotension, MI, death). Recent use is defined differently for each agent (see below for list):
o sildenafil à within the last 24h o tadalafil à within the last 48h o vardenafil à unknown duration.
• There is hypotension (Systolic BP < 90mmHg, or an absolute drop of 30mmHg from baseline)
• There is a possible RV infarct (usually, only confirmed on 15 lead ECG, but should be suspected with inferior MI’s [ST segment elevation in II, III, aVF). These lesions can lead to RV failure, and using pre-load reducers (i.e. nitroglycerin, morphine) can precipitate profound hypotension in an RV infarct.
Bottom Line: Although the biologic basis for use of IV nitroglycerin is strong, there is little evidence to support its benefit in the post-reperfusion era. Use of this therapy is largely guided by clinical observations (Level of Evidence: C) – especially in the UA/NSTEMI population. The far more important knowledge from this section is to know the list of contraindications for intravenous NTG therapy (e.g. hypotension, phosophdiesterase inhibitor use) as these can be potentially fatal.
CLINICAL QUESTION 3.8.3 What is the role of adjunctive therapies such as Morphine or other opioids?

McMaster Clinical Education Guidelines Draft Copy – Version 10.0, December 2010
14
Weak Recommendation against Usage, Low LOE 3.8.3.1 In unstable angina & NSTEMI there may be an increased association
with mortality in a large registry (CRUSADE study).

McMaster Clinical Education Guidelines Draft Copy – Version 10.0, December 2010
15
Listing of References:
1. McCaig LF, Nawar EW, National Hospital Ambulatory Medical Care Survey: 2004 emergency department summary, Adv Data. 2006 Jun 23;(372):1-29.
2. Wackers F.J., Chest pain in the emergency department: role of cardiac imaging, Heart 2009;95;1023-1030.
3. Guyatt G et al., recommendations quality of evidence and strength of GRADE: an emerging consensus on rating, BMJ, 2008;336;924-926.
4. Guyatt G et al., important to clinicians? What is "quality of evidence" and why is it, BMJ, 2008;336;995-998.
5. Guyatt G et al., Going from evidence to recommendations, BMJ 2008;336;1049-1051.
6. Cannon, C. P. et al. ACC Clinical Data Standards – Reference Guide: American College of Cardiology Key Data Elements and Definitions for Measuring the Clinical Management and Outcomes of Patients With Acute Coronary Syndromes. American College of Cardiology Web site, 2001, http://www.acc.org/clinical/data_standards/ACS/acs_index.ht
7. Antman et al. ACC/AHA Guidelines for the Management of Patients With ST-Elevation Myocardial Infarction. A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol 2004 e1-e211
8. Antman et al. ACC/AHA Guidelines for the Management of Patients With ST-Elevation Myocardial Infarction- Executive Summary. A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation 2004
9. Gibler W. B. et al Practical Implementation of the Guidelines for Unstable Angina/Non–ST-Segment Elevation Myocardial Infarction in the Emergency Department. A Scientific Statement From the American Heart Association Council on Clinical Cardiology, Circulation 2005
10. Antman et al. ACC/AHA Pocket Guideline Based on the ACC/AHA Guidelines for the Management of Patients With ST-Elevation Myocardial Infarction . A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. July 2004
11. Panju et al. Is this patient having a myocardial infarction? The Rational Clinical Exam. 2009. 461-470
12. Bruyninckx, R. Signs and symptoms in diagnosing acute myocardial infarction and acute coronary syndrome: a diagnostic meta-analysis. British Journal of General Practice, February 2008, e1-e8
13. ACEP Guidelines?? 14. Anderson et al. ACC/AHA 2007 guidelines for the management of
patients with unstable angina/non–ST-elevation myocardial infarction: a report of the ACC/AHA Task Force on Practice Guidelines: developed in collaboration with ACEP, ACP, SAEM, SCAI, and STS. J Am Coll Cardiol. 50:e1–157 (2007).
15. Hess (CJEM) Diagnostic accuracy of clinical prediction rules to exclude acute coronary syndrome in the emergency department setting: a systematic review. Hess EP, Thiruganasambandamoorthy V, Wells GA, Erwin P, Jaffe AS, Hollander JE, Montori VM, Stiell IG. CJEM. 2008 Jul;10(4):373-82.
16. Wijesinghe et al., Heart 2009;95:198–202. 17. Fesmire et al. Clinical Policy: Indications for Reperfusion Therapy in
Emergency Department Patients with Suspected Acute Myocardial Infarction. Annals Emerg Med. 48(4):358-383 (2006).
18. Van de Werf et al. Single-bolus tenecteplase compared with front-loaded alteplase in acute myocardial infarction: the ASSENT-2 double-blind randomised trial. Lancet. 354:716-22 (1999).
19. Peters RJ et al. The role of fondaparinux as an adjunct to thrombolytic therapy in acute myocardial infarction: a subgroup analysis of the OASIS-6 trial. Eur Heart J. 29:324–331 (2008).
20. Cantor WJ, Brunet F, Siegler CP, Kiss A, Morrison LJ. Immediate angioplasty after thrombolyis: a systematic review. CMAJ. 173(12):1473-1481 (2005).
21. Wijeysundera et al. Rescue Angioplasty or Repeat Fibrinolysis After Failed Fibrinolytic Therapy for ST-Segment Myocardial Infarction: A Meta-Analysis of Randomized Trials. JACC. 49(4):422-30 (2007).
22. Mehta et al. Efficacy and Safety of Fondaparinux Versus Enoxaparin in Patients With Acute Coronary Syndromes Undergoing Percutaneous Coronary Intervention: Results From the OASIS-5 Trial. JACC. 50(18): 1742-1751 (2007).
23. Hoenig MR et al. Early invasive versus conservative strategies for unstable angina & non-ST-elevation myocardial infarction in the stent era. Cochrane Database of Systematic Reviews. Issue 3 (2006).
24. Wijesinghe et al., Heart 2009;95:198–202. 25. Canto JG, Shlipak MG, Rogers WJ, et al. Prevalence, clinical
characteristics, and mortality among patients with myocardial infarction presenting without chest pain. J Am Med Assoc 2000; 283:3223–9.
26. Meine TJ, Roe MT, Chen AY, Patel MR, Washam JB, Ohman EM, Peacock WF, Pollack CV Jr, Gibler WB, Peterson ED. Association of intravenous morphine use and outcomes in acute coronary syndromes: results from the CRUSADE Quality Improvement Initiative. Am Heart J. 2005;149:1043–1049.





























