Embed Size (px)
Citation preview

McKinsey & Company 1
Independent Pricing
Review
NATIONAL DISABILITY INSURANCE AGENCY
Final Report | February 2018

McKinsey & Company 2
Contents
Executive Summary ........................................................................................... 3
The NDIS and pricing ................................................................................... 3
The Independent Pricing Review process .................................................... 3
Feedback from consultation ......................................................................... 4
Key findings and supporting evidence .......................................................... 5
Recommendations ....................................................................................... 6
Implications .................................................................................................. 7
1 Introduction ................................................................................................... 9
1.1 Overview of the NDIS and NDIA ........................................................... 9
1.2 The role of price .................................................................................... 9
1.3 Background and scope of the IPR ....................................................... 10
1.4 Phases of the IPR ............................................................................... 11
1.5 Acknowledgements ............................................................................. 12
2 Input from submissions and consultation .................................................... 13
2.1 Provider economics ............................................................................. 14
2.2 NDIA processes and systems ............................................................. 16
2.3 Market growth and development ......................................................... 17
2.4 Planning process ................................................................................. 18
3 Key findings and supporting evidence ........................................................ 20
3.1 Market development ............................................................................ 20
3.2 Analysis of provider economics ........................................................... 24
3.3 Benchmarking with comparable schemes ........................................... 28
4 Recommendations ...................................................................................... 33
4.1 Approach to price setting ..................................................................... 34
4.2 National vs regional pricing ................................................................. 40
4.3 Pricing of one-to-one services with different levels of complexity ........ 47
4.4 Pricing of Short term accommodation services .................................... 56
4.5 Thin and undersupplied markets ......................................................... 58
4.6 Provider efficiencies and adequacy of provider returns ....................... 63
4.7 Price deregulation ............................................................................... 86
Appendix A: Differences in cost drivers between attendant care providers ....... 92
Appendix B: Summary of IPR recommendations .............................................. 94
Appendix C: Variation in attendant care cost drivers across jurisdictions .......... 97
Appendix D: Existing definitions of participant complexity within the NDIA ....... 99
Appendix E: Opportunities for attendant care providers to innovate ............... 100
Glossary and Abbreviations ............................................................................ 102
McKinsey & Company 3
Executive Summary
THE NDIS AND PRICING
The National Disability Insurance Scheme (NDIS) is a new way of providing support for
460,000 Australians with permanent and significant disabilities (‘participants’). It represents a
fundamental shift in how disability support is delivered. Under the NDIS, participants can
exercise choice and control by purchasing their supports directly from providers. This means
funding of disability supports will no longer take place through block funding for providers, but
rather through individualised support funding for participants.
Once the NDIS reaches maturity, it is intended that the market itself will set the price of
supports. However, temporary price controls are needed to ensure participants can access
affordable supports, while the market is still growing. The National Disability Insurance Agency
(NDIA) uses price caps on many supports and services to regulate price, but striking the right
balance is challenging. If prices are set too high, this will encourage the supply of supports,
but reduce the purchasing power of participants and negatively impact the sustainability of the
NDIS. If prices are set too low, this could lead to a supply shortfall in the market and
compromise participant outcomes.
Some providers of disability supports and other stakeholders have expressed views that
current price caps are too low and are hindering market development. These issues have
been raised in submissions by providers to the NDIA, as part of the NDIA FY2017/18 Price
Review, as well as to the Productivity Commission as part of the review of NDIS costs.
THE INDEPENDENT PRICING REVIEW PROCESS
In June 2017, the Board of the NDIA commissioned McKinsey & Company to undertake an
Independent Pricing Review (IPR) to investigate the appropriateness of the NDIA’s pricing
strategy and approach, and the suitability of current price levels for supports and services.
The scope of the IPR was defined by the NDIA Board in the Terms of Reference (TOR):
1. Provide recommendations in relation to improved pricing effectiveness, including but not
limited to:
– National versus regional pricing
– Pricing of services with different levels of complexity
– Pricing of respite services
– Thin and undersupplied markets, particularly in regional and remote areas
– Relative provider efficiencies, including overheads
– Adequacy of provider returns
– Effectiveness of the Hourly Return approach used to set prices

McKinsey & Company 4
2. Provide recommendations in relation to the potential early deregulation of price in more
mature sub-markets and the glide path for the eventual deregulation of price more
generally.
Over the last six months the IPR team has conducted its review, including extensive
consultations with stakeholders – providers, peak bodies, the NDIA, academics, and state and
territory governments. Through the provider consultation process, the IPR team engaged with
over 1000 individuals across Australia through 10 open forums, 9 webinars and 45 one-on-
one interviews, to understand how providers have been responding to current price settings.
The IPR team also undertook detailed analyses of provider economics, market development
and NDIA data. This report provides a summary of the evidence gathered by the IPR team,
and 25 recommendations for changes to the NDIA’s pricing approach and policies.
Recommendations are grouped by the items in the Terms of Reference.
FEEDBACK FROM CONSULTATION
Key issues raised by providers and other stakeholders in submissions and during the
consultation process were:
■ The NDIS requires a significant change in providers’ operating models and there are
administrative costs associated with transition; as well as opportunities to improve the
efficiency of the NDIA’s systems and processes, for example, the online portal.
■ Current loadings for complex participants do not fully reflect the additional costs of
serving these participants, such as higher wages for a more skilled workforce, additional
time required for training and reporting, and higher supervision ratios. In addition, there is
no clear definition of what constitutes ‘complex’, and as a result the high intensity loading
is applied inconsistently.
■ Current travel allowances do not adequately cover the costs of provider travel and
participant transport in regional areas and isolated communities.
Other issues were raised in relation to specific support types:
■ In attendant care, some providers, who have historically been funded by state-
administered block funding, are struggling to adjust their business models to operate
under the NDIS unit-funding model and the current level of price caps. To operate
profitably within the price caps requires improved levels of utilisation and overheads; and
better matching of skills to participant needs.
■ In therapy, the existing single price point does not reflect the diversity in therapy supports
and the travel allowance is insufficient for some participants in regional areas. In
addition, limiting therapists to recover the costs from a maximum of 2 hours of
cancellations per year is imposing additional costs on some therapists.
Additionally, issues regarding the price setting process and the opportunity for innovative price
setting were raised, including:
■ The price setting process could be more transparent, and providers would appreciate
earlier communication of changes to price level and/or structure to refresh service
agreements and adapt operating models.
McKinsey & Company 5
■ Some providers and participants expressed the desire for the NDIA to explore outcomes-
based approaches to pricing on the basis that would create better incentives to improve
outcomes than the current hourly rate approach.
KEY FINDINGS AND SUPPORTING EVIDENCE
To address the issues raised by providers and other stakeholders during consultation, and
to assess whether current price caps are adequate, the IPR team looked at three sources of
evidence: evidence of market development/supply shortages; provider economics and
operating models; and benchmarks of comparable schemes.
The key findings of the IPR are:
■ While there is not yet evidence of generalised supply shortages, data on market
development is mixed and there are certain markets for which undersupply is a risk in the
future:
– Across support types, provider entry and exit data suggests market growth is keeping
pace with demand and utilisation data does not provide compelling evidence of supply
shortages:
□ The rate of growth of month-to-month provider registration outpaced the rate of
growth of participant registration throughout 2017.
□ Utilisation data from the trial sites suggests lower than expected utilisation was
driven by participants being unfamiliar with the NDIS and how to use their supports,
rather than a supply shortage.
– In the attendant care market, there is not yet compelling evidence of participants
being unable to access supports, but there are signals that are concerning, including
a significant proportion of providers that currently have unprofitable operating models.
– There are cohorts of participants for which supply shortages are high-risk due to the
increased cost of service provision and limited availability of workforce, including
those who: are in outer regional, remote or very remote areas; have complex needs;
are from culturally and linguistically diverse backgrounds; are Aboriginal and Torres
Strait Islander Australians; or have acute care needs such as in crisis situations.
■ While some providers have operating models that are profitable at current price points,
many are struggling, particularly traditional providers delivering attendant care supports:
– In the attendant care market, there is significant variation (from <$40 to $55+ per
hour) in the cost of service delivery between providers. There are examples of low
cost models that are profitable at current price points, including the online platform
model and lean-operating model. However, many traditional providers are struggling
to operate profitably at current price points. This is attributable to a combination of
factors: higher overheads; challenges in adapting to unit pricing and NDIA systems
improvement opportunities; lower utilisation of workers; and higher labour costs.
– In therapy, the single price point is working for some providers, such as physio and
speech therapy providers and many sole traders. However, it is not working so well for
some others, such as psychological therapy for more complex participants.
McKinsey & Company 6
– In Supported Independent Living (SIL), Support Coordination and Plan Management,
feedback indicates that most providers can operate profitably at current price
caps/benchmarks for lower complexity participants. However, the rollout of a more
accurate SIL pricing process may make it more challenging for providers to cross-
subsidise other supports in the future.
■ Benchmarking of NDIA support price caps against comparable schemes highlighted that
the NDIA price is broadly aligned with prices of accident compensation schemes,
including the Transport Accident Commission and WorkSafe, although market prices for
some similar aged care services are higher.
RECOMMENDATIONS
Ultimately, the test of whether the price caps set by the NDIA are adequate is whether
participants can access the quality supports and services required to achieve their goals.
While there is not yet evidence of widespread supply gaps occurring, the Scheme is in a state
of transition and rapid growth, and the situation could change quickly. Further, the absence of
supply gaps does not diminish the fact that the current price caps are challenging, and many
providers are unable to operate profitably within those price caps. Providers and participants
have raised concerns that where providers are unable to supply services at a given price
level, new supply will not be made available quickly enough to ensure that participants have
access to an adequate level of support.
To proactively manage the key risk of supply gaps, the IPR team proposes three steps for the
NDIA to undertake. Firstly, the NDIA should collect and analyse a broader set of indicators of
market development and participant outcomes to both better monitor the risk of supply gaps
and build institutional capacity to avert supply challenges through market intervention.
Secondly, the NDIA should implement appropriate amendments to price loadings and policies,
to improve the economics of efficient providers and reduce the risk of supply shortages in
high-risk markets – particularly rural and remote, and highly complex participants. Those
changes include:
■ Adding a third tier to the complexity loading of 10%, to account for higher level of
skills/experience of workers and additional training required.
■ Allowing providers to charge up to 45 minutes of travel time in rural areas, and quote for
services in isolated regions.
■ Changing the cancellation policy to allow providers to charge participants for
cancellations after 3pm on the day before the service.
■ Removing the $1000 travel cap for therapy supports and aligning the travel policy with
attendant care travel policy.
■ Changing the therapy prices to better reflect different therapy types, and introducing a
second tier of pricing for therapy assistants.
■ Addressing specific NDIA systems and processes, such as portal functionality and
quoting, to enable providers to reduce administrative tasks and overhead costs.

McKinsey & Company 7
Finally, the NDIA should assess the implementation of a temporary price supplement to the
attendant care price cap to address short-term issues with provider economics. The IPR
team’s assessment is that while generalised supply gaps have not occurred to date, there is
a material risk of gaps emerging over the next year. Demand will continue to rapidly increase
as new participants enter the Scheme, and many providers are struggling to operate a
surplus at the price cap with their current operating model. There is a risk that profitable
providers will not grow quickly enough to supply the services required. The IPR team
proposes a model of Transitional Support for Overheads (TSO) in the form of a 2-3%
increase in the price cap of 1:1 attendant care for the next 12 months. This would apply in
addition to the normal annual indexation of the price cap. This adjustment reflects what the
IPR team believes are reasonable cost improvement assumptions for most providers to
achieve in the near term. The exact quantum of the TSO should be a policy decision the
NDIA makes in view of other more targeted interventions government will undertake in the
next 12 months to mitigate the risk of supply shortages. There should be a review in 12
months to determine whether any level of temporary support is required for a further period.
The expectation is that 12 months is a reasonable timeframe for providers to make the
necessary changes to their business models, and for the NDIA to assist and encourage the
development of efficient and effective alternative supply options (e.g. e-marketplaces), so
that the TSO would not need to be renewed.
Longer term, the development of a competitive marketplace should enable changes to the
Scheme’s current pricing model of price caps and fee-for-service. The IPR team’s
recommendations include actions that the NDIA can take to pilot and prepare for different
pricing models. Firstly, the NDIA should conduct a trial of outcomes-based pricing. This is an
appealing alternative to input-based pricing as it encourages providers to maximise outcomes,
rather than the volume of services provided. However, it is significantly more complex and
requires strong baseline data and measurement systems. A trial would provide valuable
learnings on how this approach might be implemented in some supports.
Deregulation of pricing remains an appropriate goal, but there is not yet a clear path towards
reaching it. To better prepare the market and the NDIS for deregulation, the IPR team
proposes strengthening and monitoring provider and participant readiness, including investing
in key infrastructure, such as an e-market. Trialling price deregulation in one geography or
support type market will also help the NDIA collect more detailed information on the impact of
deregulation on market development and participant outcomes.
IMPLICATIONS
In developing its recommendations, the IPR team has sought to address provider concerns in
a way that best balances potential trade-offs between participant outcomes, market
development and Scheme sustainability. The effectiveness and efficiency of pricing
mechanisms and levels was considered, subject to available data. Some recommendations go
directly to changing the effective price, such as Temporary Support for Overheads (TSO) and
a new complexity loading for very complex participants; some target root causes of the
problems, such as changes to cancellation and travel policies; and some propose stronger
market monitoring and intervention capabilities. Each of these recommendation types will
have different impacts on the three Scheme aspirations: better participant outcomes; a
growing market with innovative supports; and a financially sustainable scheme.

McKinsey & Company 8
In the aggregate, the IPR team estimates that the above recommendations will have a
potential financial impact of ~$250-420m per annum over the next 12 to 24 months, will
alleviate some of the financial pressure currently placed on some providers, and will improve
participant outcomes by addressing challenges that are impacting some providers’ abilities to
deliver quality services. Cost estimates have been made on the best data available. However,
data will remain incomplete until the Scheme becomes more mature. As a result, the IPR has
made a number of assumptions leading to a wide range of estimates.
Beyond the next 24 months, the IPR team believe it is possible to implement the IPR
recommendations and manage the Scheme so that it is financially sustainable and within the
current budget estimates. Approximately 50% of the total cost implication of the IPR
recommendations is temporary and will therefore not have an adverse impact on the
Scheme’s longer-term financial sustainability. Also, as the Scheme matures, the NDIA should
be able to offset any financial impact of these recommendations by appropriately assessing
their effectiveness and efficiency. For example, as evidence develops as to which
interventions are most effective in reducing costs associated with complexity, it should be
possible to reduce the number of complex participants and provider costs and prices. It should
also be possible to encourage more local providers in rural and remote areas that will assist in
reducing travel costs. There should also be some savings from introducing tiered therapy
pricing.

McKinsey & Company 9
1 Introduction
1.1 OVERVIEW OF THE NDIS AND NDIA
The National Disability Insurance Scheme (NDIS) is a new scheme designed to change the
way supports and services are provided to Australians with significant and permanent
disabilities (‘participants’). By 2020, the NDIS will provide about 460,000 people with the
reasonable and necessary supports they need to live an ordinary life. The NDIS is currently
in the transition period, with participants entering the Scheme according to an agreed phasing
plan.
The National Disability Insurance Agency (NDIA) is the statutory authority responsible for
administering the NDIS. The NDIA has three external aspirations (NDIA aspirations):1
1. Facilitate outcomes of economic and social independence and deliver an exceptional
service for participants, and their families, carers and providers (‘better participant
outcomes’).
2. Work with participants and other stakeholders to facilitate the growth of a market of
adequate size, quality and innovation (‘a growing market with innovative supports’).
3. Deliver a financially sustainable scheme based on insurance principles within agreed
funding (‘a financially sustainable Scheme’).
1.2 THE ROLE OF PRICE
The NDIS represents a fundamental shift in the way disability supports are provided. Under
the NDIS, people with disability will be able to exercise choice and control over the supports
they receive. This way of providing supports and services requires a transition from a prior
model of block funding for providers, to individualised funding for supports for participants.
In a mature market, participants exercising choice and control will drive the price of supports,
and in turn drive competition and innovation among providers. This is an important feature
of the NDIS. However, where the market is not sufficiently mature and where there is an
imbalance in bargaining power between participants and providers, price regulation helps
ensure value for money for participants.
The NDIA sets price caps for many supports. The price of supports has implications for the
NDIA aspirations, and trade-offs may be required among them (see Exhibit 1). For example,
higher prices may encourage the supply of supports, but reduce the purchasing power of
participants and negatively impact Scheme sustainability, whereas lower prices may increase
value for money but lead to a supply shortfall in the market. Ultimately, the test of whether the
price caps set by the NDIA are adequate is whether participants can access quality supports
and services required to achieve their goals.
1 NDIA: Corporate Plan 2017-21. The Corporate Plan outlines four aspirations for the NDIA: three ‘external aspirations’ and one ‘internal aspiration’, which is to build a high performing NDIA.

McKinsey & Company 10
EXHIBIT 1
1.3 BACKGROUND AND SCOPE OF THE IPR
Some providers of disability supports and other stakeholders have expressed concerns that
some of the current price caps are constraining market development and outcomes for
participants. These concerns were raised in submissions to the NDIA, as part of the NDIA
FY2017/18 Price Review, as well as to the Productivity Commission as part of its review of
NDIS costs. In June 2017, the Board of the NDIA commissioned McKinsey & Company to
undertake an Independent Pricing Review (IPR) to understand the significance of provider
concerns, and create an evidence base to inform decision making and help to mitigate the risk
of future supply shortages as the NDIS transitions to full scheme. The objective of the IPR
was to investigate the appropriateness of NDIA’s current pricing strategy and approach, and
assess the suitability of current price levels for supports and services.
The scope of the IPR was defined by the NDIA Board in the Terms of Reference:
1. Provide recommendations in relation to improved pricing effectiveness, including but not
limited to:
– National versus regional pricing
– Pricing of services with different levels of complexity
– Pricing of short-term accommodation (respite) services
Facilitate outcomes of economic
and social independence and
deliver an exceptional service for
participants, and their families,
carers and providers
Better participant outcomes 1
V
Work with participants and
other stakeholders to
facilitate the growth of a
market of adequate size,
quality and innovation
A growing market with
innovative supports
2
Deliver a financially
sustainable Scheme based
on insurance principles and
within the agreed funding
A financially
sustainable Scheme
3
Speed vs cost
Price impacts pace of market
development and Scheme cost
Value vs speed
Price impacts pace
of market
development and
participant value
for money
Cost vs value
Price impacts
participant value for
money (quality and
quantity of services)
and Scheme cost
Impact of price on three Scheme aspirations
SOURCE: NDIS Corporate Plan 2017-21
McKinsey & Company 11
– Thin and undersupplied markets, particularly in regional and remote areas
– Relative provider efficiencies, including overheads
– Adequacy of provider returns
– Effectiveness of the Hourly Return approach used to set prices
2. Provide recommendations in relation to the potential early deregulation of price in more
mature sub-markets and the glide path for the eventual deregulation of price more
generally.
Pricing of specialist disability accommodation (SDA) was excluded from the scope of the IPR
on the basis that there was separate work being undertaken by the NDIA on this topic.
This report provides a summary of the evidence and findings from provider consultation and
analysis conducted by the IPR team (Sections 2 and 3), and presents recommendations
against each item of the IPR Terms of Reference (Section 4).
1.4 PHASES OF THE IPR
Phase 1 (Jul-Aug 2017): Review of submissions and NDIA documents and initial assessment
of provider economics
The first phase of work consisted of reviewing and analysing the NDIA’s market stewardship
role, building a provider economics/cost model, and analysing supply challenges likely to
emerge at the sub-market level. Submissions to the NDIA and the Productivity Commission
were reviewed and documented, to identify priority issues for further consultation.
The IPR team also conducted analysis of comparable schemes, e.g. Accident Compensation,
Aged Care, and State-funded disability – to assess NDIA prices versus other relevant sectors.
Phase 2 (Sep-Oct 2017): Provider consultation and evaluation of options
Phase 2 focussed on engaging with providers and other stakeholders. The IPR team held ten
provider forums in: Adelaide (SA), Townsville (QLD), Melbourne (VIC) (2), Darwin (NT),
Canberra (ACT), Sydney (NSW) (2), Newcastle (NSW) and Campbell Town (TAS), with
~800 individuals attending in total. In addition, nine online forums were held, with a total
of 270 individuals joining from across Australia.
The IPR team engaged individually with 45 NDIS and aged care providers, and participated in
working groups with providers, peak bodies, advisory groups, and state and territory
governments. This included multiple consultations with the Independent Advisory Council
(IAC) representing participants.
Though no formal written submissions were requested, many providers chose to submit
supporting evidence/documentation to the IPR. In total ~20 written submissions were received
from across the sector; this was in addition to the submissions made to the Productivity
Commission and NDIA FY2017/18 Price Review.

McKinsey & Company 12
Phase 3 (Oct-Nov 2017): Development of draft recommendations
The third phase of work focused on summarising findings, conducting further analysis and
developing draft recommendations. The consultation phase highlighted examples of providers
operating profitably at current price points, as well as examples of providers who find the
current price points very challenging. Phase 3 involved collecting data on different operating
models to identify features of models that are working, and key drivers of cost in models that
are not. The IPR team engaged with providers to identify options for solutions that would help
improve provider economics.
In considering solution options, the IPR assessed the appropriateness of options in achieving
NDIA’s three aspirations- better participant outcomes, a growing market with innovative
supports, and a financially sustainable scheme. Implications of the recommendations were
assessed, and the effectiveness and efficiency of pricing mechanisms and levels were
considered, subject to available data.
Phase 4 (Dec 2017): Syndication and refinement of recommendations and preparation of final
report
The final phase of the IPR involved testing of recommendations with providers and other
stakeholders and preparation of the final report. The implications of recommendations were
identified and quantified, where possible, in terms of impact on the three NDIA aspirations.
Estimates of costs were made based on the best information available. Given a lack of
appropriate data as the Scheme matures, the IPR made several assumptions to inform
estimates of costs, leading to wide ranges in estimates presented in this report.
1.5 ACKNOWLEDGEMENTS
The IPR team is grateful for the cooperation of many providers and representatives of peak
bodies, member groups and state and territory governments, who generously gave up their
time to meet with the team and provide input to the IPR. The IPR would like to especially
thank the 45 providers who met one-on-one with the IPR team and shared detailed financial
information, modelling and analysis, as well as the IAC that invited the IPR to join four of its
meetings.
The IPR team would also like to acknowledge the many individuals within the NDIA who
shared their expertise and helped the team understand current practices related to pricing and
work underway in the NDIA.
Further, the IPR team would like to thank AlphaBeta Advisors who provided support to
McKinsey & Company throughout the entirety of the IPR.

McKinsey & Company 13
2 Input from submissions and consultation
The IPR team examined input from various sources, including:
■ Written submissions to the Productivity Commission report on NDIS Costs; the NDIA
FY2017/18 Price Review; and the IPR team.
■ Face-to-face consultation with providers to the NDIS; providers in adjacent sectors such
as aged care; peak bodies including the Independent Advisory Council (IAC)
representing participants; state and territory governments; and academics.
Provider submissions to the Productivity Commission report on NDIS Costs and the NDIA
FY2017/18 Price Review had different areas of focus. The Productivity Commission sought
responses on pricing with a holistic view of the disability market, whereas the NDIA
FY2017/18 Price Review sought responses focused on specific modelling assumptions
detailed in the 2017 Price Review – Discussion Paper.
The objective of consultation undertaken through the IPR was to identify a comprehensive list
of issues and challenges faced by providers that the IPR team could test for significance and
impact on the NDIA aspirations: improving participant outcomes, growing a market with
innovative supports, and a financially sustainable scheme. To do this, the IPR team consulted
with over 1000 provider representatives through provider forums; and consulted individually
with 45 providers that are broadly representative of the disability market, including providers
across NDIS support types, large and small providers, providers with new service models,
providers delivering services in regional and remote areas, and new entrants with potential to
scale in size.
This section of the report records the challenges and opportunities raised by stakeholders –
as was committed to do during consultation, prior to testing their significance on the NDIA
aspirations. Actions being taken to address some of these challenges, as advised by the
NDIA, are also recorded. Section 3, Key findings and supporting evidence, details evidence
the IPR team sought to test, challenge and validate opportunities, including those raised by
providers, that are within the scope of the TOR. Section 4, Recommendations, outlines the
IPR team’s recommendations to address the challenges and opportunities raised by providers
and other stakeholders, underpinned by further analysis and data to support how these
recommendations assist the NDIA in achieving its three aspirations.
The IPR team recognises that not all challenges and opportunities raised by providers are
specifically within the scope outlined in the TOR. However, where these challenges are likely
to have a flow on impact on provider economics, they have been noted below. Other
challenges that are less likely to impact on provider economics, but could assist the NDIA to
improve participant outcomes, will be raised separately with the NDIA.
Feedback received during consultation can be summarised into four areas:
■ Increasing price loadings to adequately cover the cost of service delivery for rural and
remote geographies, participant cohorts, and support types (see Section 2.1 below).
■ Reducing the cost of administration for providers by improving the NDIA’s provider-facing
systems and processes (see Section 2.2).

McKinsey & Company 14
■ Increasing the emphasis on policies that support the development and growth of the
market, including a greater focus on participant outcomes (see Section 2.3).
■ Improving aspects of participant planning quality and consistency that would assist
provider economics as well as participant outcomes (see Section 2.4).
While discussions with providers centred around challenges they are facing, most expressed
their strong support for the reforms and objectives of the NDIS, and aspirations of the NDIA,
as well as the positive work underway by the NDIA to achieve these aspirations and address
provider challenges. Several providers were also excited about their success in developing
new business models that could work successfully in helping participants achieve their
objectives, and improve their outcomes, in a financially sustainable way.
The remainder of this section summarises provider and other stakeholder feedback on the
following topics:
■ 2.1 Provider economics
■ 2.2 NDIA processes and systems
■ 2.3 Market growth and development
■ 2.4 Planning process.
2.1 PROVIDER ECONOMICS
Many providers raised challenges with the assumptions included in the NDIA’s 2017 Price
review – Discussion Paper, which detailed the input assumptions to be used by the NDIA to
model the price of attendant care (a combined category comprising Assistance with Daily
Living and Assistance with Social and Community Participation). In Section 3 – Key findings
and supporting evidence, the IPR team tests these challenges by benchmarking against other
schemes, and examining effective models that are working in the market, as well as those that
are not working.
These providers considered that the NDIA should continue to refine the following
assumptions:
■ The wage assumption. The NDIA assumes that the disability support worker will be
employed at a level 2.3 under the Social, Community, Home Care and Disability Services
Industry Award (SCHADS Award). Some providers believe the assumption is low and
does not allow for career progression. Other providers commented that they pay higher
wages due to Enterprise Bargaining Agreements (EBA) or a more mature workforce. By
way of contrast, some providers commented that they are successfully operating in a
consistent way with the wage assumption, utilising different mixes of part-time/full-time
employee models, casual employment and accessing new talent pools.
■ The utilisation assumption for support workers. The NDIA assumes a utilisation level of
95% for disability support workers. Some providers believe this level of utilisation is
difficult to achieve. Some providers that consulted with the IPR reported that 80-85%
utilisation of direct support staff is typical. By way of contrast, some are achieving 95% to
100% utilisation.

McKinsey & Company 15
■ The utilisation assumptions for supervisors. The NDIA assumes a 1/15 supervision ratio,
and a utilisation level of 95% for supervisors. Some providers believe this level of
supervision is difficult to achieve, and that it does not allow sufficient time to undertake
quality/compliance requirements and support worker management. Others are finding
that they do not require the level of supervision of 1/15 to offer quality support to the
participants they serve.
■ The overhead assumption. The NDIA assumes an overhead level of 10%, which equates
to 15% if a provider is not subject to payroll tax. Some providers are finding it difficult to
achieve this level of overheads, particularly those with higher expenditure on training,
reporting and participant engagement during transition. While the Department of Social
Services (DSS) and states and territories have provided funding to support transition,
some providers claim this is insufficient – given that the participant-driven service model
requires most providers to make new investments in areas such as training, IT,
marketing, and recruiting. Further, some providers noted that NDIS processes contribute
to higher overheads, e.g. through lost administration time associated with information
and communication technology (ICT) challenges. By way of contrast, some providers
reported that they are currently able to achieve an overhead level of 10%.
Providers also raised issues related to the higher cost of service provision for certain cohorts
of participants. This includes participants living in remote areas, with complex needs, and
those requiring Assistive Technology (AT). More specifically, they considered that the NDIA
should consider the following:
■ Remote loadings are not sufficient for some remote areas where there are high costs-to-
serve due to factors including extra travel time, lack of infrastructure and facilities, and
the cost of deploying/housing a workforce. In some cases, such as for communities in
the Northern Territory, air travel and overnight accommodation is necessary to reach
participants, and this cannot be claimed from the NDIA.
■ Travel is also a concern in some regional areas, as providers are not being fully
remunerated for travel in all circumstances.
■ The differentiation in price levels for support workers serving participants with complex
needs is not sufficient to cover the costs of a higher skilled worker with increased
qualifications or experience, which some providers believe are required to provide high
quality support to these participants. Some providers expressed a view that the current
price could discourage providers, both existing and new entrants, from serving
participants with complex needs and instead focus on those that can be served with a
lower cost support model.
The NDIA has recently announced the development of an independent provider
benchmarking function to generate important strategic information both for providers and the
NDIA. The initiative seeks to collate and share market knowledge on the cost structures and
pricing of providers. Participating providers will receive information that enables them to
understand how they are performing relative to their peers, and where there are specific
opportunities for organisational improvement. The data generated by the project will be at an
aggregate and anonymised level, and will provide government with a clearer sense of what
is happening in the sector, and where intervention by the NDIA may be necessary.

McKinsey & Company 16
2.2 NDIA PROCESSES AND SYSTEMS
Providers raised challenges relating to additional overhead costs associated with operating in
the NDIS, which they believe are partly attributable to NDIA processes and systems.
Opportunities identified by providers for the NDIA to improve system and processes include:
■ Reducing the administrative load when providers interact with the NDIS, including the
one-time costs associated with pre-planning and quoting (where applicable) when a
participant enters the NDIS, and ongoing administration such as billing, invoicing, and
reporting. For example:
– Improve the functionality and efficiency of the Provider Portal, as they consider errors
are still occurring and can be time consuming to resolve.
– Increase the speed at which SIL quotes can be created and processed. Some
providers commented that they have submitted reports between 100-200 pages in
length as part of the additional information they consider is required for ‘above
benchmark’ SIL quotes, while other providers reported that they have waited up to 3
months to receive a response from the NDIA on SIL quote outcomes.
– The quoting process for Assistive Technology and home modifications can
disadvantage the provider developing the initial quote, as they are required to spend
more time and effort to develop a quote together with a participant, typically in-home,
and often an assessor, usually an occupational therapist. As the NDIA requires at
least 3 quotes, additional providers are sent the initial quote to develop their own
quote in isolation from the participant and assessor. This advantages subsequent
providers by giving them the opportunity to undercut the initial quote due to the
reduced cost of quote development.
■ Improving the clarity and consistency in communication of policies to providers. Some
providers commented that they spend significant amounts of time contacting the NDIA,
and become frustrated with the inconsistency of responses from NDIA staff. Others
commented that they’re increasingly satisfied with NDIA staff responses.
■ Increasing the transparency of the price setting process, and the timeliness of
communications relating to price changes, to allow providers sufficient time to update
service agreements prior to pricing changes coming into effect.
The NDIA has advised the IPR team that they have made several improvements in the
design and functionality of the Provider Portal in the last 12-18 months in response to
feedback from providers. However, the NDIA also recognises there are opportunities to
further improve functionality and provider experience, and will continue focusing on this as
part of its ongoing work. The NDIA also has two projects underway to address the
challenges providers are facing relating to SIL: the SIL Tool project, and the SIL Redesign
project. Data from the NDIA shows the SIL Tool has reduced the processing time for SIL
quotes by up to 50%, however additional improvements will be required for the NDIA to
achieve its target of a 14-day turnaround time.

McKinsey & Company 17
2.3 MARKET GROWTH AND DEVELOPMENT
Providers raised issues about price levels inhibiting the growth and development of a skilled
workforce. Some providers believe there is a risk of supply shortage as demand increases
towards Full Scheme, and there are anecdotal reports that some providers are choosing to
reduce their services or not grow beyond their existing service levels due to pricing
constraints. Some providers believe there is also potential that new participants and
participants with complex needs could have difficulty finding a service provider if the market is
not growing at the necessary rate to meet demand. At the same time, these providers
recognise there are also new providers entering the market and some other existing providers
are expanding their services. Providers suggested:
■ Setting prices at a point that allows providers to attract and retain a more skilled
workforce to care for participants with complex needs. Some providers serving
participants without complex needs also raised this as an issue, as they are having
difficulty attracting highly skilled workers necessary for some categories of service.
■ Explicitly allowing a provision for training, as some providers believe the utilisation
assumption used in modelling is not sufficient to cover enough time for training, in
addition to other non-client facing activities such as incident management, administration
and reporting. This issue is more pronounced for providers serving participants with
complex needs.
■ Developing market infrastructure to increase the ability for the market to grow. For
example, there is no functioning e-market, and participants vary in their abilities to
exercise choice and control.
Some participants and providers suggest that the hourly rate approach to pricing does not
provide sufficient incentives to improve outcomes and consistent adherence to insurance
principles. Specifically, they requested the NDIA to consider the following:
■ An approach to pricing consistent with an outcome focus. Prices are currently focused on
units of care in hours. The IAC and some providers would like to see an incentive in the
pricing structure for providers to reduce a participant’s support needs over time. While
the focus on units of care helps to ensure participants receive a defined number of
service hours, it can also inhibit innovation by limiting flexibility in how participant
packages can be spent.
■ A more consistent adherence to insurance principles that focuses on early investment to
reduce participant needs over time and reduce their lifetime cost to the NDIS. Participant
plans should be looked at more holistically to understand how a greater investment in
capital supports such as Assistive Technology and home modifications could reduce the
need for other supports. Looking at capital supports in combination with opportunities to
reduce other supports, and focusing on quality as well as price could improve outcomes
for participants, as well as assist the sustainability of the NDIS.
The NDIA has advised the IPR team that it has identified initiatives to expand its monitoring
and support of market development. It is developing a market assessment framework, which
seeks to bring together disparate data sources and metrics into a coherent assessment
process. It is also investing in a benchmarking function to share market knowledge and
identify opportunities for providers to improve their businesses. The NDIA is also focused on
McKinsey & Company 18
increasing its understanding of how the NDIS is affecting participant outcomes through
regular surveys and participant consultation. For example, the Short-form Outcomes
Framework questionnaire has helped the NDIA build a baseline understanding of participant
outcomes during the NDIS transition period.
2.4 PLANNING PROCESS
The planning process is not formally within the scope of the IPR, as defined in the TOR.
During consultation, issues were raised by providers about how the quality and consistency of
plans could be improved to positively impact both participant outcomes and provider
economics, both initial plans and plan reviews:
■ Improving the planning process to support NDIA planners and Local Area Coordinators
(LACs) to consistently capture all the needs of a participant to deliver quality plans for
participants. This can reduce the time and resources providers invest to help some
participants rectify issues with their plans such as correcting plan errors and submitting
additional documentation to justify the need for additional funding in participant budgets.
It can also help reduce the time providers spend educating participants and their families
on how to engage with the NDIA and LACs, including how to utilise their plans with
providers. These improvements will benefit participant outcomes by ensuring they have
sufficient funds for specific functions. It is recognised by providers that there will always
be more opportunities to improve plans, and the role of the NDIA is to improve the
capabilities of its planners over time in identifying and planning for all needs of
participants and how to improve outcomes.
■ Improving the consistency in timing and communications for plan reviews, to make sure
providers are aware reviews are taking place. This would help providers understand
when they may need to update service agreements with participants, and alert them to
when there could be service continuity issues if there are changes to a participant’s
funding allocation across different supports.
The NDIA has advised the IPR team that significant improvements are underway to the
planning process to address many of the challenges raised by providers, and are currently
being implemented as part of the Participant and Provider Pathways Review. Piloting has
commenced in Victoria in December 2017, with improvements including:
■ A significantly re-designed planning process to make it easier for participants to see how
their goals have been recorded and linked to community, other government services and
funded supports.
■ Face-to-face planning meetings with an LAC, an NDIA planner and a participant to
improve plan quality and educate participants and their families on how to utilise
participant packages.
■ Participants being able to see a working version of their plan as it is developed and the
opportunity to ask questions and provide feedback during the planning meeting, to allow
for any queries to be discussed and addressed before the plan is finalised.
■ The use of simple language to improve communication.

McKinsey & Company 19
Some providers argue that the challenges described in this section are having an impact on
their abilities to operate at a sufficient surplus in the sector. In Section 3 – Key findings and
supporting evidence, and Section 4 – Recommendations, the IPR team has worked with the
providers, the NDIA and other stakeholders to explore the challenges raised by providers that
are within the scope of the TOR, to provide a sufficient evidence base to justify the need for
action, and propose recommendations relating to pricing that can be adopted by the NDIA to
address these challenges.

McKinsey & Company 20
3 Key findings and supporting evidence
To address the issues raised by providers and other stakeholders during consultation, and to
assess whether current price caps are adequate, the IPR team looked at three sources of
evidence:
■ 3.1. Evidence of market development and shortages in supply, including analysis of
the available market data such as utilisation rates, rates of market entry and exit, and
market surveys.
■ 3.2 Provider economics and models, including detailed bottom-up analysis of
providers’ costs-to-serve and comparison with the hourly rate model.
■ 3.3 Benchmarks from other schemes, including comparison of NDIS prices to state
accident compensation schemes and the Commonwealth’s aged care and veterans’
support programs.
3.1 MARKET DEVELOPMENT
Close to 11,000 service providers have been approved to cater to participants in the NDIS,
with approximately 5,000 service providers already active in supplying support services.2
Many of these service providers are small suppliers, with 60% of active providers catering to
fewer than 10 clients each. The larger providers account for most of the Scheme expenditure
to date. Approximately 70% of NDIS payments have been to providers which cater to 100 or
more participants each.3
The IPR team recognises that the provider market landscape is likely to change significantly in
response to providers shifting to a new consumer-driven, unit funded environment. For
example, the current provider landscape for in-home attendant care, a significant support type
in the Scheme, is dominated by not-for-profits and medium to large providers.4 Going
forward, new providers, many of whom are likely to be for-profit organisations, and could
leverage technology innovatively, are expected to enter the market, having identified a
profitable niche or operating model. Some existing providers will exit the support category
because they cannot adjust to this new market landscape, while providers who successfully
adjust their operating models are likely to expand to meet demand. It is unclear how quickly
this market adjustment and new provider entry will occur. A dynamic and responsive approach
to monitoring the market will be critical to ensuring there is sufficient and quality supply to
allow participants to continue to receive safe and quality supports.
The key test of whether current prices are adequate is whether participants can access the
quality supports and services needed to achieve their goals, as defined and funded in their
2 National Insurance Disability Agency: National Insurance Disability Scheme COAG Disability Reform Council Quarterly Report (30 September 2017).
3 Analysis based on NDIS payment data. 4 Not-for-profits consist of 62% of the disability sector, while 88% of in-home attendant care service volume in
2016-17 was delivered by medium to large providers.

McKinsey & Company 21
plans. Market data on participant and provider behaviour and intent offers the most direct
evidence of whether current prices are consistent with this test. Analysis of provider entry and
exit rates, utilisation rates, and participant outcomes reveals a market that is, to date,
providing the supply required to match demand. However, this evidence is not unequivocal.
Gaps in the available data and the volatility of a transitional and rapidly growing market mean
that this data does not yet provide certainty as to whether participants will be able to continue
to access the supports they need into the future.
The remainder of this section examines the available data sources on market development:
Provider entry and exit data
Provider entry and exit data offer evidence of a market that is growing to meet demand.
The number of registered providers more than doubled in FY16/17. The rate of growth of
quarter-to-quarter provider registration has outpaced the rate of growth of participant
registration throughout 2017. In the latest quarter, provider registrations grew by 21%, with a
total of 10,507 providers currently registered in the Scheme.5
In the trial regions, less than 15% of providers decreased or ceased supply during the trial,
whereas 30% of providers increased supply or entered after the trial began (FY13/14 to
FY15/16).6 The existence of some provider exits is also not in itself an indication of
inappropriate prices. It is to be expected that as providers adjust to the NDIS, some will be
unable to make enough changes to their business models and operations to supply services
at an efficient price, while others will choose to specialise in some supports but exit other
supports. It is also important to recognise that providers may have been willing to invest in the
trial to test whether they could develop an effective model, so limited exits during trial may
also not be predictive of future provider behaviour.
Participant utilisation data
Another key data point – utilisation – also does not provide compelling evidence of supply
shortages. The utilisation rate is the share of a participant’s budgeted supports that has been
used. The average utilisation rate across the Scheme in FY16/17 was 66%, which is well
below the expected utilisation of the Scheme at maturity of 85-95%.7 However, the available
evidence suggests that it is more likely caused by participants being unfamiliar with the
Scheme and how to use their supports, rather than a supply shortage. In the trial sites, the
average utilisation rate also started low, at 64%, but increased to 75% in the final year,
reaching 80% in some sites. This change occurred without a reduction in the average size of
plans, discounting the possibility that individual plans simply became more restrictive, despite
the number of participants increasing as the trial progressed. Evidence from transition also
indicates that the utilisation rate increases as participants spend more time in the Scheme and
move onto their second and subsequent plans. The share of participants with high utilisation
rates (>75%) almost doubles from first to subsequent plans. There is little participant survey
5 National Insurance Disability Agency: National Insurance Disability Scheme COAG Disability Reform Council Quarterly Report (30 September 2017).
6 Analysis based on NDIS payment data. 7 Average utilisation rate for FY16/17 as at December 2017. Utilisation rates continue to increase after the end of
the period being measured due to delays in claims and payment processing, so it is likely the final average utilisation rate for FY16/17 will be higher.

McKinsey & Company 22
data to understand the drivers of this utilisation rate. Surveys during the NDIS trial showed
that 27% of NDIS participants had at least some difficulty in accessing supports for which they
had funding. More recently, baseline outcomes performance reported quarterly by the NDIA
shows that 68% of participants nominate having no difficulty in accessing health services they
require. However, a similar metric for NDIS services is not reported.
Analysis of utilisation by support type shows utilisation rates are highest in the largest support
types and supports using attendant care, with the category of core daily care support services
having a utilisation rate of 73% (Exhibit 2). This category includes support services such as
assistance with daily living. Other support types reliant on attendant care, like assistance with
social and community participation (‘Community’) and support for capacity building daily
activities, have the next highest utilisation rates. The lowest utilisation rates are in capital and
intermediary supports, which are of concern but are less likely to represent an imminent
shortfall in critical supports.
EXHIBIT 2
Average utilisation of daily care (core) supports was higher than any other
support type
OtherSupport
Coordin-
ation
Community
41%
Daily care (Core)
58%
44%
Daily care
(Capacity
Building)
73%
48%
Column width scaled to the support’s share of FY2016/17 Scheme expenditure
Uti
lis
ati
on
ra
te
Supports using attendant care
price cap
100%
Target
(85-95%)1
Utilisation rate by support type
Average utilisation rate by support type FY2016/17, %
1 Target utilisation rate estimated based on consultation with the NDIA and review of annual budget papers.
SOURCE: Scheme Actuary, FY17 utilisation data by support category

McKinsey & Company 23
Aggregate analysis of firm entry/exit and utilisation data is complemented by anecdotal
evidence of new private sector investment and innovation. For example, firms such as HireUp
and BetterCaring8 have made large investments to build new digital infrastructure to provide
services in the disability services market. Such upfront investments offer evidence of the
private sector’s willingness to invest in this market. Similarly, the state government in New
South Wales sold its Home Care business for $114 million, indicating the willingness of private
capital to enter the disability services market.
Participant survey data
An evaluation of the NDIS trial by the National Institute of Labour Studies (NILS) revealed
most participants found supports for which they had funding. This survey was initiated in 2014
and therefore covers more of the early experience of the Scheme. Approximately 73% of
participants responded that they were able to access all supports for which they had funding.
The average number of different supports accessed by participants has increased to 3.3 from
2.2 since the introduction of the Scheme, and 44% of participants report having greater choice
and control over the supports they do receive since their enrolment in the NDIS. 9
More recent measurement of participant outcomes reveals that 71% of participants believe
that the NDIS has helped the level of choice and control they experience. 75% of participants
identify the NDIS as having helped their daily living conditions, and 63% identify that it has
helped their social, community, and civic participation.10
Evidence of provider intent
Other factors point to significant challenges as the Scheme continues to grow. The
Productivity Commission acknowledged several studies that point to a potential future shortfall
in supply to meet projected demand, with current workforce growth rate estimated between 6-
13% versus a required growth rate of 18%. However, this can partly be explained by the
ramp-up in demand that is expected, i.e. future growth rates are expected to be higher than
current growth rates. The Productivity Commission also identified several participant cohorts
for which a shortfall in supply is a risk. These included participants in remote and very remote
areas and participants with complex needs. While there is not yet evidence of a shortfall in
supply occurring across the Scheme, this is a risk that needs to be closely monitored.
Furthermore, some providers reported to the IPR team during its consultation process that
they were drawing on surpluses and other funding sources, and cross-subsidising some
support types, to continue to serve participants while they transition. They are concerned as
to whether they can achieve a sustainable operating model in the future. Some major
providers also reported that due to challenging economics operating in the Scheme, they are
not accepting new participants for some services and are planning to reconsider their support
8 Better Caring is not a registered provider under the NDIS, but has a profitable operating model in the disability services market supporting self-managed participants.
9 National Institute of Labour Studies: NDIS Survey of people with disability, their family and carers (2014 – 2017), available at http://ndisevaluation.net.au/information/ndis-survey.cfm
10 National Insurance Disability Agency: National Insurance Disability Scheme COAG Disability Reform Council Quarterly Report (30 September 2017).

McKinsey & Company 24
offerings in 2018. Ongoing close market surveillance and liaison with providers will be
essential for identifying the intention of large providers to exit or reduce services.
3.2 ANALYSIS OF PROVIDER ECONOMICS
The financial sustainability of providers in the NDIS is critical to ensuring ongoing supply of
supports to participants. While providers may be able to absorb losses for a period, operating
in the NDIS needs to be attractive in the long term for enough providers to meet the growth in
demand.
To understand the economics of providers in the NDIS, the IPR team gathered evidence from
various sources, including a detailed cost-to-serve analysis of a sample of NDIS providers.
The IPR team is grateful for the cooperation of many providers, who generously shared
detailed financial information to enable the team to analyse their costs-to-serve.
The remainder of this section examines the evidence available on the following:
■ 3.2.1 Cost of transitioning to the NDIA
■ 3.2.2 Overview of provider economics across support types
■ 3.2.3 Provider economics in attendant care
Cost of transitioning to the NDIS
For providers across all support types, the cost of transitioning to the NDIS and interacting
with the NDIA’s systems and processes added materially to their cost base and affected their
short term financial position.
Moving to a unit-funded, consumer-driven environment has required providers to employ new
staff to process payments and invest in IT systems and marketing. Some providers estimate
that these costs have added 1.5% to their annual expenditure.11 This is detailed further in
Section 4.6.1.
Improving the NDIA’s systems and processes related to the portal and planning as articulated
in Section 4.6.2, would reduce administrative costs and cash flow risk. Anecdotal evidence
indicates that these improvements could amount to ~0.5% of total annual expenditure for
some providers.12 Anecdotal evidence also indicates that the cumulative effect of unapproved
SIL quotes, unresolved portal errors and expired plans has resulted in cash flow risk for some
providers; one large provider submitted that at one point they were owed ~10% of their total
revenue in services unclaimed. The IPR team has been advised by the NDIA that substantial
improvements to the portal have been made in the last 12-18 months, and the NDIA currently
has a significant program of work underway, the Provider Pathway Project, to review and
address the issues noted above.
11 Based on 45 one-on-one interviews with providers in September 2017, in which three large providers (revenue > 50 million in FY16/17) gave detailed evidence of these costs.
12 Based on 45 one-on-one interviews with providers in September 2017, in which three large providers (revenue > 50 million in FY16/17) gave detailed evidence of these costs.

McKinsey & Company 25
Overview of provider economics across support types
Across all support types there were examples of providers operating profitably, and examples
of providers struggling (see Exhibit 3).
EXHIBIT 3
In Supported Independent Living (SIL), Therapy, Support Coordination and Plan
Management, analysis indicated that most providers can operate profitably at current price
points/benchmarks. However, the costs involved in meeting quoting requirements and delays
in approving quotes in SIL are impacting provider overheads.13 In addition, the rollout of the
new SIL pricing process may reduce surpluses that providers are generating, and reduce their
ability to cross-subsidise other services.
In attendant care, there was a higher proportion of providers who submitted they were unable
to operate profitably. Given the emphasis from providers on the challenges associated with
profitably delivering attendant care, the IPR team conducted detailed analysis of provider
economics for this support type.
13 Anecdotal evidence from provider consultation indicates that SIL quoting requirements can be onerous: some providers have submitted reports of 100-200 pages in length to justify above benchmark quotes. NDIA data indicates that the average time to approve a SIL quote in Jul-Sept 2017 was 40 days, down from 107 days pre-July 2017.
SOURCE: Provider Consultation, Sep-Oct 2017
1 Numbers in brackets represent percentage of Scheme spend in FY17, based on payments data provided by the NDIA
Support type1 ChallengingWorking economically
Short term
accommodation
(1.7%)
▪ Providers serving complex participants
▪ Providers operating on weekends/
holiday periods/ overnight
▪ (Limited) Providers serving less complex
participants with lower care ratios
Assistance with daily
life and social/
community
participation
(36.1%)
▪ Providers serving complex participants
or operating in low density areas
▪ Providers with more qualified,
specialist or experienced workforces
▪ Providers with EBAs that are more
generous than the Award
▪ Tech-enabled for-profit providers serving
participants with lower complexity needs or
strong informal supports
▪ Some incumbents with economies of scale
▪ New entrants with lean operating models
Life skills and support
coordination
(5.3%)
▪ Providers serving complex participants,
where plans do not adequately cover
coordination activities undertaken
▪ Support coordination and plan management
providers for low complexity participants
▪ Some employment service providers
Supported independent
living (39.0%)
▪ Providers serving complex participants
with onerous quoting requirements
▪ Emergency/crisis situations
▪ Some SIL providers, as SIL is a quoted item
Therapy
(5.0%)
▪ Remote/rural areas where lots of travel
is required
▪ Some psychotherapy service providers
▪ Some therapy providers (e.g. sole traders in
physio, speech)
▪ Providers in high density, metro areas
Provider cohorts where pricing is working economically versus where it
is challenging
McKinsey & Company 26
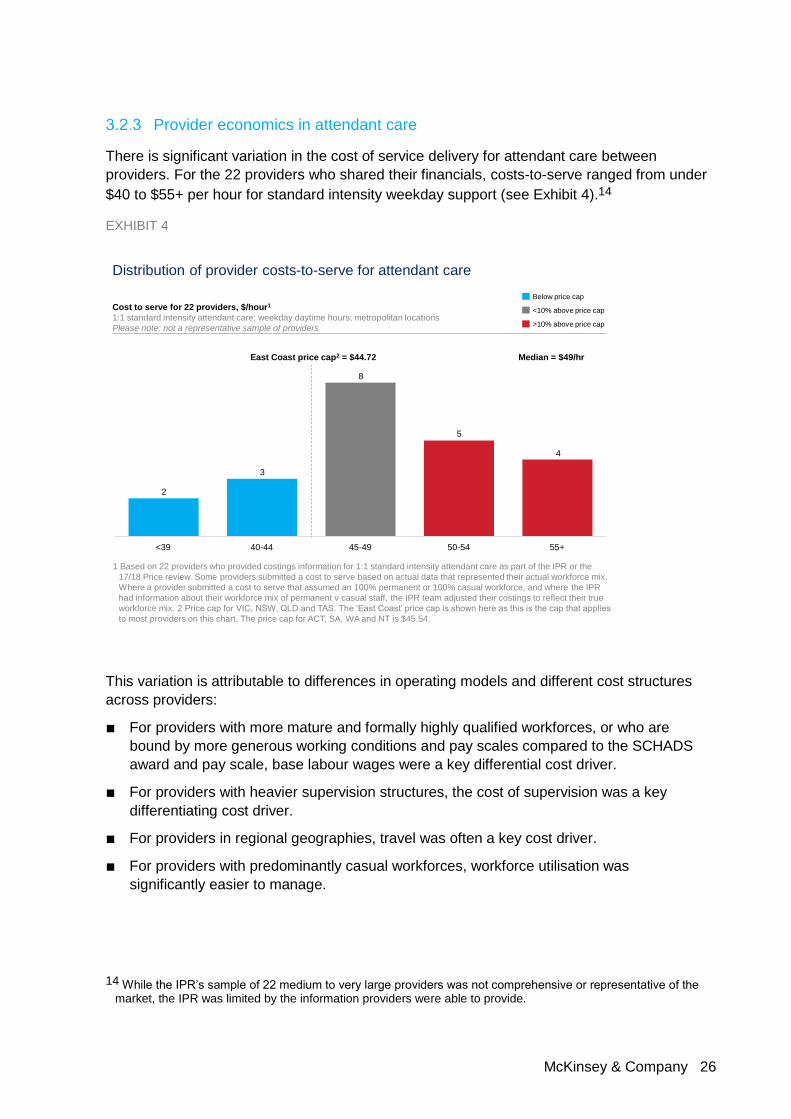
Provider economics in attendant care
There is significant variation in the cost of service delivery for attendant care between
providers. For the 22 providers who shared their financials, costs-to-serve ranged from under
$40 to $55+ per hour for standard intensity weekday support (see Exhibit 4).14
EXHIBIT 4
This variation is attributable to differences in operating models and different cost structures
across providers:
■ For providers with more mature and formally highly qualified workforces, or who are
bound by more generous working conditions and pay scales compared to the SCHADS
award and pay scale, base labour wages were a key differential cost driver.
■ For providers with heavier supervision structures, the cost of supervision was a key
differentiating cost driver.
■ For providers in regional geographies, travel was often a key cost driver.
■ For providers with predominantly casual workforces, workforce utilisation was
significantly easier to manage.
14 While the IPR’s sample of 22 medium to very large providers was not comprehensive or representative of the market, the IPR was limited by the information providers were able to provide.
4
5
8
3
2
45-4940-44<39 55+50-54
East Coast price cap2 = $44.72
1 Based on 22 providers who provided costings information for 1:1 standard intensity attendant care as part of the IPR or the
17/18 Price review. Some providers submitted a cost to serve based on actual data that represented their actual workforce mix.
Where a provider submitted a cost to serve that assumed an 100% permanent or 100% casual workforce, and where the IPR
had information about their workforce mix of permanent v casual staff, the IPR team adjusted their costings to reflect their true
workforce mix. 2 Price cap for VIC, NSW, QLD and TAS. The ‘East Coast’ price cap is shown here as this is the cap that applies
to most providers on this chart. The price cap for ACT, SA, WA and NT is $45.54.
Median = $49/hr
Distribution of provider costs-to-serve for attendant care
Cost to serve for 22 providers, $/hour1
1:1 standard intensity attendant care; weekday daytime hours; metropolitan locations
Please note: not a representative sample of providers
<10% above price cap
>10% above price cap
Below price cap

McKinsey & Company 27
■ There was significant variation in the cost of corporate or indirect overheads between
providers, with expenditure on corporate overheads as a percentage of direct labour
costs ranging from less than 10% to over 20%.15
For a more detailed summary of key drivers of differences in costs between providers, see
Appendix A.
Participant characteristics can also influence provider economics. Margins were more
compressed (or negative) for providers operating in areas with low density of participants, e.g.
rural, remote and very remote areas, and for those serving participants with complex needs.
On the other hand, the profitability of some providers can be in part attributed to their focus on
specific participant segments. Providers who serve participants at the lowest end of the
complexity spectrum often have lower labour and supervisory costs. These providers
submitted that it is not necessary to pay a highly qualified or trained worker to deliver
attendant care supports to participants that are not medically or behaviourally complex, for
whom the risk of incidents is extremely low. Rather what they focussed on ensuring was that
they had support workers with the right mindset, compassion and soft skills to deliver high
quality support.16 Providers who serve participants with predictable and high volumes of care
are also able to operate profitably in attendant care, because workforce rostering and
utilisation is easier to manage.
While a substantial number of providers assessed are not yet able to operate profitably at the
current price cap, there are some providers who submitted they are able to deliver
1:1 standard intensity attendant care at a sustainable surplus, while complying with their
award or enterprise agreement obligations. These providers often have lean operating
models, leverage technology successfully, or are sole traders. Some of these providers have
operated in the sector for some time, while others are new providers that entered the disability
space in response to the NDIS opportunity.
■ Traditional providers with lean operating models: Some traditional providers who run
extremely efficient operations and have achieved a degree of scale are able to operate
profitably. These providers exhibited some, or all, of the following characteristics: lean
corporate overheads facilitated by effective investments in IT systems; effective rostering
systems and a mix of casual and permanent staff to maximise staff utilisation; and/or a
supervision model where supervisors only focus on quality assurance and co-ordination,
while rostering work is done by a separate team. Providers in this group submitted they
can achieve corporate overheads of ~10% of direct labour costs. Providers in this group
who hire predominantly casual workers can maximise the amount of time their workers
perform client-charging work and achieve 95+% workforce utilisation rates. These
15 Data based on information from 22 providers who provided detailed financial information to the IPR. Corporate overheads refers to costs that are not directly attributable to client care (e.g. IT, HR, rent, marketing, business development, senior management salaries).
16This is particularly relevant in the context that there will be more than 100,000 people who receive NDIS funding who did not previously receive disability funding, A segment of the 100 000 new participants will have a psychosocial disability and may need highly qualified workers to support them. A segment of the new participants whom will have lower packages relative to participants who were existing recipients of State block funding, are likely to be at the lower complexity end of the spectrum. For these participants, a support worker with the right mindset may be more appropriate than a highly qualified worker.

McKinsey & Company 28
working models provide insights on tactics that can be used by struggling traditional
providers to improve their financial performance.
■ Tech-enabled providers: These providers serve participants via online platforms, which
allow participants to book and manage their own care schedule directly, reducing the
work required to be completed by a provider and minimising corporate overheads.
Support workers are typically casual, allowing providers to achieve high utilisation levels,
as staff will only work when there is known demand from a participant. These providers
estimate their cost of service delivery is up to ~20% lower than the current price cap.
These providers also leverage technology to manage quality and safety: customers are
able provide feedback after every shift online and an algorithm helps detect potential
problems with service quality or customer satisfaction. However, this operating model
relies on participants or their carers having the capacity and desire to manage their own
supports. These providers currently only serve a small proportion of the market, and
while this model appears to hold significant potential, it is unclear as yet what percentage
of the standard intensity attendant care market this model will be able to serve at full
Scheme.
■ Sole traders: Sole traders can deliver attendant care significantly below the current price
cap. This is because a self-employed support worker does not incur the supervisory or
corporate overhead expenses of a small provider. While sole traders currently deliver
less than 1% of service volume in in-home attendant care market, the emergence of e-
marketplaces connecting self-employed care workers and participants could see a
significant growth in this group of providers.17
The IPR believes these profitable and successful operating models offer valuable lessons to
learn from for other providers who are struggling.
3.3 BENCHMARKING WITH COMPARABLE SCHEMES
There are several other State and Commonwealth schemes in Australia that offer comparable
supports to their participants, including state accident compensation schemes and the
Commonwealth’s aged care sector. There is also significant overlap in the provider markets
that service these other schemes. For example, ~90% of providers in one of the benchmarked
schemes are also registered NDIS providers.18
To assess the adequacy of NDIS price caps for various supports, the IPR team benchmarked
prices against available prices in the other schemes. The IPR team undertook detailed
benchmarking for attendant care and therapy supports. Attendant care was chosen given the
large proportion of Scheme spend attendant care represents, and given the recent scrutiny on
the price cap for 1:1 attendant care (see Section 4.6.3.1). Therapy supports was chosen
17NDIA data. Sole-traders that are registered NDIS providers can serve all NDIS participants, whereas sole traders that are not registered NDIS providers cannot serve Agency-managed participants.
18 McKinsey analysis, conducted by checking providers in the comparable scheme with NDIS registration data.

McKinsey & Company 29
because the single NDIS price cap for therapy appeared to be inconsistent with the multiple
price levels, and structure, of other comparable schemes.
Attendant care
Benchmarking the unit price of 1:1 attendant care under the NDIS with comparable schemes
is complicated by a variety of factors: each scheme has a different funding model, different
cohorts of clients, different business rules associated with care delivery (e.g. travel rules,
cancellation policy, funding for training), and different fee structures (e.g. weekly price cap
versus hourly price caps, composite versus time differentiated price caps). For instance, the
Transport Accident Commission (TAC) and Worksafe have composite price caps in which the
price cap for 1:1 care does not vary for time of the day or day of the week. By way of contrast,
the NDIS rates are specific to the time of the day and day of the week. While TAC and
Worksafe attendant care standard price caps do not vary for complex participants, the NDIS
price caps differentiate for ‘higher intensity’ and ‘standard intensity’ prices.
It is also important to recognise that other government schemes such as the TAC and
Worksafe are significantly smaller than the NDIS, and revenue from these schemes is less
likely to be the primary source of revenue for providers. Further, providers under other
government schemes such as Worksafe are often guaranteed they will serve a participant for
a set amount of time, and this demand certainty allows providers to manage their business
and workforce planning more efficiently.
Despite these limitations in comparing across schemes, benchmarking is nonetheless useful
to understand whether NDIS prices are broadly aligned with prices of other schemes. This
benchmarking highlighted that the NDIS prices for standard intensity attendant care are in fact
broadly aligned with prices of the accident compensation schemes, although market prices for
many aged care services are higher (see Exhibit 5). While the NDIS composite price is higher
than the composite rate for other schemes, other schemes provide more generous conditions
associated with the delivery of care.19 For example, TAC and WorkSafe offer establishment
fees of ~$1200, compared to $500 in the NDIS. TAC also reimburses providers for training at
a rate of $43.10 per hour, compared to no specific provision for training reimbursement under
the NDIS.
19 The NDIS composite rate is a weighted average of the various NDIS standard intensity time of the day and day of the week price caps.

McKinsey & Company 30
EXHIBIT 5
Therapy
The NDIA has a single price cap in place for all therapy supports delivered by a qualified
therapist under the NDIS. The price cap allows therapists to charge participants up to
$175.57/hr for the delivery of services in a participant’s own environment, which for a child
could be in their home or at school, or in a therapist’s office.20 When a participant requires
therapy supports to be delivered in their own environment, a therapist can make a separate
claim for travel against a participant’s package to reimburse them for the costs they incur. The
NDIA has created a separate allowance in participant packages for therapy travel, which is
capped at $1000 each year per therapy support type. The current travel policy allows
therapists to claim travel time at the hourly rate of the service being delivered for travel over
10km.21
Other comparable insurance schemes in Australia offer different therapy prices dependent on
the number and complexity of the conditions experienced by the participant. Examples include
the TAC, WorkSafe, Department of Veterans Affairs (DVA), and NSW State Insurance
Regulatory Authority (SIRA). The categorisation of the number and complexity of conditions
vary by scheme. To simplify, the IPR team has named them Level 1, Level 2, and Level 3,
with the number of conditions and/or complexity of the support increasing with each level (see
20 NDIA: 2017/18 NDIS Price Guide VIC-NSW-QLD-TAS (version release date July 2017), p. 61 21 NDIA: 2017/18 NDIS Price Guide VIC-NSW-QLD-TAS (version release date July 2017), p. 15
1. Benchmarking the unit price of 1:1 attendant care under the NDIS with comparable schemes is difficult for a variety of factors: each Scheme has a
different funding model, serve different cohorts of clients, different business rules associated with care delivery (travel rules, cancellation policy,
funding for training etc) and fee schedules with different fee structures (e.g. weekly price cap vs hourly price caps, composite vs time differentiated
price caps). 2. We sampled a range of aged care home care providers in metro regions in Sydney and Melbourne for their weekday daytime
attendant care prices. These rates were private rates, meaning they are not necessarily fully government subsidised. 3. NDIS composite rate for
Eastern States, based on actual distribution of service volume between time of the day and day of the week;. 4. IQRS accredited rate. 5. For these
Government Schemes, we estimated the composite rate. Where the Government Scheme provided a weekly cap, we divided this cap by the
recommended number of hours of care per week. Where the Government Scheme provided different rates for time of the day and day of the week,
we estimated the distribution of service volume to calculate a composite rate. 6. 2015/16 Report on the Operation of the Aged Care Act 1997, p9
and 10. 7. NDIA 2017 Corporate Plan, p11. 8. TAC 2017 Annual report, p6. 9. Worksafe Victoria Annual Report 2017, p57 and 15.
Price for 1:1 attendant care, $/hr1
The NDIS attendant care price cap is aligned with comparable
compensation schemes, although market prices for aged care appear higher Scheme or
Provider
Time of the day,
day of the week
Government
Scheme 25
Composite rate (est.)
Government
Scheme 15
Composite rate (est.)
Composite rate (actual)3
Composite rate (actual)4
Government
Scheme 35
Composite rate (est.)
Sample of aged
care providers2
Weekday, daytime rate
Composite rate (actual)4
Cost and scale
FY 2016/17:~$1.35b in support services, ~49k supported clients8
At full scale:
~$22b, 460k participants7
FY 2015/16:
~$17b, 1.3m people received aged care support6
FY 2016/17:$ 0.2b in gross claims paid, ~26k total annual standard claims9
46.00
44.72
45.64
45.94
46.73
47.74
49.40
51.56
46.00 59.30
Weekday, daytime rate
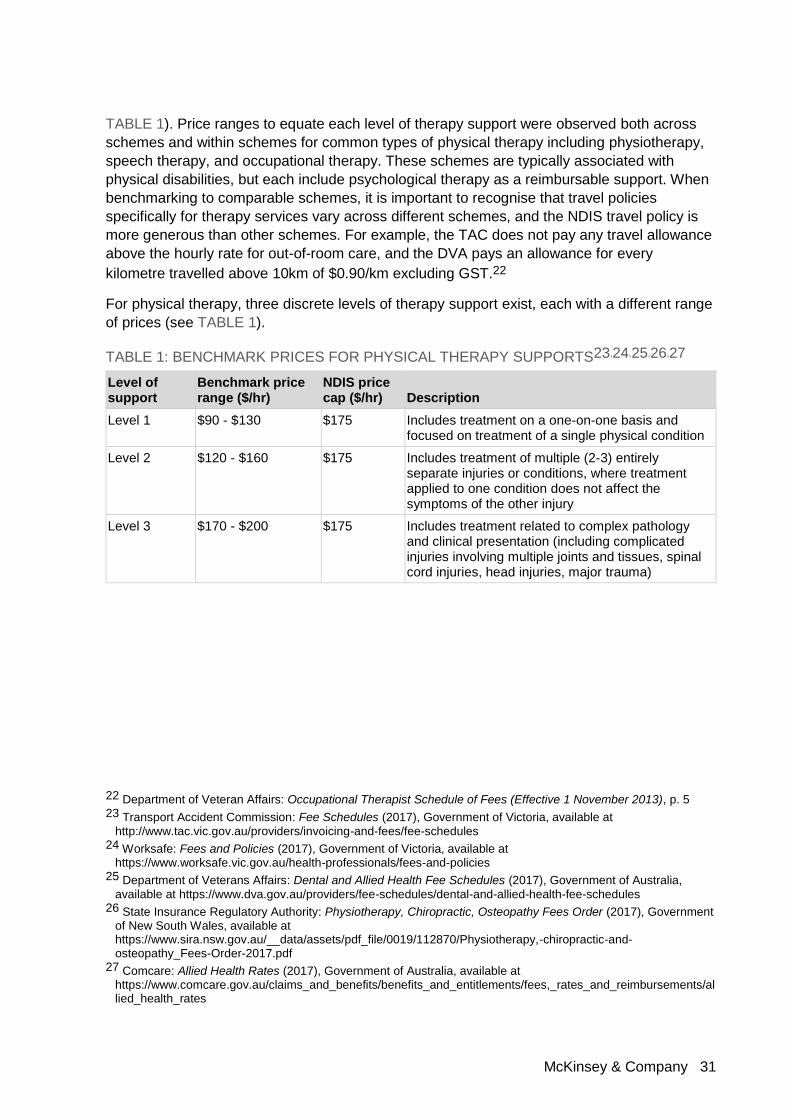
McKinsey & Company 31
TABLE 1). Price ranges to equate each level of therapy support were observed both across
schemes and within schemes for common types of physical therapy including physiotherapy,
speech therapy, and occupational therapy. These schemes are typically associated with
physical disabilities, but each include psychological therapy as a reimbursable support. When
benchmarking to comparable schemes, it is important to recognise that travel policies
specifically for therapy services vary across different schemes, and the NDIS travel policy is
more generous than other schemes. For example, the TAC does not pay any travel allowance
above the hourly rate for out-of-room care, and the DVA pays an allowance for every
kilometre travelled above 10km of $0.90/km excluding GST.22
For physical therapy, three discrete levels of therapy support exist, each with a different range
of prices (see TABLE 1).
TABLE 1: BENCHMARK PRICES FOR PHYSICAL THERAPY SUPPORTS23,24,25,26,27
Level of support
Benchmark price range ($/hr)
NDIS price cap ($/hr) Description
Level 1 $90 - $130 $175 Includes treatment on a one-on-one basis and focused on treatment of a single physical condition
Level 2 $120 - $160 $175 Includes treatment of multiple (2-3) entirely separate injuries or conditions, where treatment applied to one condition does not affect the symptoms of the other injury
Level 3 $170 - $200 $175 Includes treatment related to complex pathology and clinical presentation (including complicated injuries involving multiple joints and tissues, spinal cord injuries, head injuries, major trauma)
22 Department of Veteran Affairs: Occupational Therapist Schedule of Fees (Effective 1 November 2013), p. 5 23 Transport Accident Commission: Fee Schedules (2017), Government of Victoria, available at
http://www.tac.vic.gov.au/providers/invoicing-and-fees/fee-schedules 24 Worksafe: Fees and Policies (2017), Government of Victoria, available at
https://www.worksafe.vic.gov.au/health-professionals/fees-and-policies 25 Department of Veterans Affairs: Dental and Allied Health Fee Schedules (2017), Government of Australia,
available at https://www.dva.gov.au/providers/fee-schedules/dental-and-allied-health-fee-schedules 26 State Insurance Regulatory Authority: Physiotherapy, Chiropractic, Osteopathy Fees Order (2017), Government
of New South Wales, available at https://www.sira.nsw.gov.au/__data/assets/pdf_file/0019/112870/Physiotherapy,-chiropractic-and-osteopathy_Fees-Order-2017.pdf
27 Comcare: Allied Health Rates (2017), Government of Australia, available at https://www.comcare.gov.au/claims_and_benefits/benefits_and_entitlements/fees,_rates_and_reimbursements/allied_health_rates

McKinsey & Company 32
For psychological therapy, the entry level of support is at a higher level of complexity than
Level 1 physical therapy, and more equivalent to Level 2 physical therapy (see TABLE 2).
TABLE 2: BENCHMARK PRICES FOR PSYCHOLOGICAL THERAPY SUPPORTS
Level of support
Benchmark price range ($/hr)
NDIS price cap ($/hr) Description
Level 1 $160 - $180 $175 Includes psychological therapy on a one-to-one basis focused on treatment of a psychological disability in a low risk environment
Level 2 $190 - $240 $175 Complex psychological therapy requiring a very skilled and experienced clinical professional, often necessary where a participant poses a high risk to themselves or others because of their disability
The findings outlined in this section form the basis of the suite of recommendations detailed in
the following section. Recommendations are grouped by the items of the Terms of Reference.
Under each item, further detail is also provided on the issues and evidence relevant to the
topic.

McKinsey & Company 33
4 Recommendations
As outlined in Section 3.1, the fundamental test of whether price caps are adequate is whether
participants can access quality supports and services. There is not yet compelling evidence of
supply shortages occurring, other than what was recently observed in short term
accommodation and has now been addressed through price changes. However, there is still a
risk of future supply shortage, particularly for participants in rural, remote and very remote
areas and those with complex needs. The IPR team’s analysis also identified a significant
number of providers that have not yet developed a profitable operating model, particularly in
the service category of attendant care.
To improve provider economics and confidence in the NDIS, minimise the risk of supply
shortages in the future, and assist the NDIA to achieve its aspirations, the IPR team has made
25 recommendations, detailed in this section. These recommendations are designed to target
the root cause of issues identified through consultation and further analysis.
Together, these recommendations will have a positive impact on provider economics,
improving overall industry margins by 2% to 4%, with even higher margin improvements for
providers serving participants with complex needs or in rural, remote and very remote areas.
Examples of these recommendations that will have a direct impact on provider economics are:
■ Adding a third tier to the complexity loading of 10%, to account for higher level of
skills/experience of workers and additional training required.
■ Allowing providers to charge up to 45 minutes of travel time in rural areas.
■ Allowing providers to quote on the delivery of services in isolated regions.
■ Changing the cancellation policy to allow providers to charge participants for
cancellations. after 3pm on the day before the service.
■ Removing the $1000 travel cap for therapy supports and align the travel policy with
attendant care travel policy.
■ Changing the therapy prices to better reflect different therapy types, and introduce a
second tier of pricing for therapy assistants.
■ Continuing to improve NDIA systems and processes (e.g. portal functionality, quoting) to
enable providers to reduce administrative tasks and reduce costs.
■ Introducing temporary overhead assistance equivalent to a 2% to 3% loading on the
price for providers delivering attendant care for the next 12 months.
The recommendations in this section have been grouped according to items in the IPR’s
Terms of Reference (see Section 1.4). There were some issues raised during the consultation
phase that were outside the scope of this review. These issues have been captured and will
be raised separately with the NDIA.
The structure of this section is as follows:
■ Section 4.1: Approach to price setting, covering Recommendations 1 to 2
■ Section 4.2: National versus regional pricing, covering Recommendations 3 to 5

McKinsey & Company 34
■ Section 4.3: Pricing of services with different levels of complexity, covering
Recommendations 6 to 9
■ Section 4.4: Pricing of short-term accommodation (respite) services, covering
Recommendation 10
■ Section 4.5: Thin and undersupplied markets, covering Recommendations 11 to 12
■ Section 4.6: Provider efficiencies and adequacy of provider returns, covering
Recommendations 13 to 21
■ Section 4.7: Price deregulation, covering Recommendations 22 to 25
4.1 APPROACH TO PRICE SETTING
The NDIA sets price caps for an hour of service for most support services supplied in the
NDIS. The price caps are reviewed annually and a new price guide is published, though the
NDIA has also twice amended prices outside the annual review process. In assessing the
approach to price setting used by the NDIA, the IPR considered both the process for setting
price caps, and the way in which price caps are applied as an hourly (or other time-based)
rate.
Section 4.1 covers the following topics:
■ 4.1.1 Determining appropriate price caps
■ 4.1.2 Alternatives to an hourly rate
The use of price ranges and deregulated pricing are considered separately in Section 4.7.
Determining appropriate price caps
Issues and evidence
The NDIA has amended prices through its annual price reviews as well as interim changes
where required. The current price caps are a result of the NDIA FY2017/18 Price Review
concluded in June 2017 and a change to short term accommodation price caps from 30
October 2017. The NDIA FY2017/18 Price Review was based on an assessment of the
underlying methodology used to estimate the hourly costs of personal care and community
supports, feedback from the disability services sector including 82 provider submissions
directly in response to the annual review process, new economic data such as increases in
the Wage Price Index, and an assessment of the impact of proposed changes by external
consultancy HoustonKemp. The annual price adjustment also accounted for changes in the
national minimum wage and the operation of the Equal Remuneration Order (ERO).28 This led
to several changes. For example, base prices for the support type ‘Assistance with daily living’
were increased by 4.5%, loadings for remote and very remote areas were increased, and the
28 The Equal Remuneration Order is an order made by the Fair Work Commission in 2012 which required wages in the social and community services industry to be increased regularly to 2020. The ERO increases occur each December according to a prescribed formula.

McKinsey & Company 35
cancellation policy of therapy services was amended. The NDIA published the amended Price
Guide on 12 June 2017 before it took effect on 1 July 2017. These changes were then
followed by a tailored change to price caps for short term accommodation services,
announced on 18 October this year, with the new prices being revealed a week later and
taking effect two weeks later, on 30 October.
The NDIA does not yet have a comprehensive evidence base to inform its regular pricing
decisions, but it has been increasing its scope of data collection. For example, the NDIA does
not keep a collated record of supply shortfalls identified by LACs and regional offices, nor
does it directly survey participants on whether they experienced shortages in supply of
supports for which they had funding.29 However, it has developed and implemented a Short-
form Outcomes Framework questionnaire which measures participant outcomes and it is
deploying a benchmarking survey of providers to understand evolving cost structures across
the NDIS. The NDIA is also working with DSS to develop a set of metrics to monitor market
development, as well as developing a market intervention strategy to identify and respond to
instances in which prices have been unable to attract sufficient supply.
Recommendations
1: The NDIA should include a broader set of indicators of participant outcomes and market development in its price setting process, and clarify its methodology for implementing price setting decisions.
The NDIA’s current process for setting prices and ensuring provision of services for
participants can be enhanced. The IPR team recommends a four-step process (see Exhibit 6).
This process should apply to the annual price reviews, as well as any interim adjustments
which may be necessary in response to changing market conditions. The IPR team
recommends that the NDIA considers the following four steps as it develops its market
intervention strategy:
1. Continuous market monitoring
2. Focused data collection on at-risk markets
3. Data analysis and policy decision
4. Implementation of decision
The most significant departure of this prescribed process from NDIA’s current practice is to
include a more thorough assessment of the risk of supply shortages, including a more
comprehensive analysis of alternative supply options and the range and distribution of costs to
serve of providers. The driving question should be whether participants are able to access all
the services for which they have funding. In the case of an existing provider no longer being
able to offer services, participants will require options to access alternative providers. Where
there are signals that participants are at risk of not being able to access services, the NDIA
should assess options to intervene through evaluating impact on the NDIA aspirations.
29 The NDIA does monitor the number and broad category of complaints lodged by participants, as well as tracking the overall participant satisfaction rate, which has consistently been above 85%. However, neither of these are directly related to observations of supply gaps in the Scheme.

McKinsey & Company 36
It is important that the price-setting process continually balances the NDIA aspirations, which
can involve trade-offs. This is because in an immature and developing market, price caps not
only regulate provider competition but also act as a signal of efficient prices, enable value-for-
money for participants, and affect the long-term development of the NDIS.
EXHIBIT 6
Step 1: Routine market monitoring
The NDIA should complement its existing initiatives to advance its market monitoring
capabilities through three additional initiatives: collecting data on the share of participants
affected by supply gaps, extending its provider consultation and feedback processes, and
collating market data and sharing internally to all relevant decision-makers.
The NDIA should collect more comprehensive data on the ability of participants to find the
supports they require across each geographical region and support type. The most desirable
way to collect this information is regular surveying of participants. This could be done through
a new survey, or by expanding the existing participant assessment in the Short-form
Outcomes Framework.
Secondly, the NDIA should establish proactive and regular consultations with providers,
including surveys, to assess provider experience and intent. The NDIA should construct a
representative sample of new and mature providers to gauge their financial sustainability,
intent for growth, self-assessment of ability to cater to demand, and knowledge of any current
or emerging supply gaps. Whilst some of this data is currently collected by other
The process for testing whether to amend price caps should incorporate
thorough market monitoring and transparent decision making
Routine market monitoring
▪ The NDIA should expand its
data collection on participant
experience and provider
intent.
▪ The Provider, Market and
Sector development team
should collate data from
across the NDIA to identify
any markets at risk of supply
shortage.
Focussed data collection on
at-risk markets
▪ The Provider, Market and
Sector development team
should work with LACs,
regional offices and existing
initiative such as the provider
benchmarking survey to better
understand the at-risk markets.
Data analysis and policy decision
▪ Ensure analysis is shared
regularly within the NDIA to
inform pricing decisions, for
example by establishing a
pricing reference group
▪ Continue to balance Scheme
aspirations in making pricing
decisions
Implementation of decision
▪ Make decision at annual price
review, or through interim
adjustment if needed
▪ Announce intervention to market,
including clear statement of
assumptions and market data
1
2
3
4

McKinsey & Company 37
organisations, the NDIA should have access to a more regular and reliable source of data that
it can rely on for its own decision making.
The above sources of data should be part of a regular monitoring framework which also
incorporates existing market data such as utilisation rates and evidence of provider entry or
exit (see Exhibit 7). See Section 4.5.1 for a detailed discussion of the relevant metrics.
Finally, all relevant market information should be collated and analysed by the Provider,
Market and Sector development team. Regional offices, LACs, the Scheme Actuary and other
parts of the NDIS should share the relevant data with this team. The data and analysis should
then be regularly reported to key stakeholders within the NDIA such as the Chief Executive
Officer (CEO) and the Board. This will enable rapid identification of any markets that may be
at high risk of undersupply and a consistent flow of information within the NDIA.
If this market monitoring process reveals any markets that are at risk of developing supply
gaps, the NDIA should take immediate steps to collect more focussed data on those at-risk
markets.
EXHIBIT 7
Step 2: Focussed data collection on at-risk markets
More focussed data collection on specific markets should include investigating the causes of
participants being unable to access supports, through LAC feedback and qualitative research
with participants. It may also include assessing the economic performance of providers to
Supply in Scheme markets can be evaluated through considering a
mix of indicators from surveys, utilisation rates and entry/ exit dataDiscussion on limitations
Provider intent may be informed by non-
Scheme features
However, reason for withdrawal/
expansion is not as relevant as identifying
the outcomes that are consistent with
existing price settings
Benchmark entry/ exit rates are difficult to
establish due to volatility in transitioning
markets
However, the data can be used to identify
outlier markets which warrant further
investigation
Utilisation rates are affected by many non-
supply factors, e.g. plan quality
However, comparing to average utilisation
rates and measuring change over time
can help to determine markets in which
persistent low utilisation is likely to be due
to insufficient supply.
Indicator and relevant metrics
Provider
intent
Rates of
market
entry/ exit
Utilisation
rate
Broad surveys may be too expensive or
time-consuming to be sufficiently
representative and timely
Consider focusing on “at-risk” markets
which show other indicators of supply
shortages, such as low rates of market
entry or poor utilisation rates
Participant
experience
Data Source
1.1: Share of participants with
funding who had difficulty or
were unable to find services
Participant survey, e.g. “In the past year, did you have
difficulty or were you unable to access supports because of a
lack of suppliers in your market?”
Compare across respondent region and support type
1.2: Share of participants
who are unsatisfied with
quality of services accessed
Participant survey, e.g. “Were you satisfied with the quality of
supports you have received in the past year?”
Compare across region and support-types of respondents
2.1: Share of providers
intending to grow/ shrink
number of participants served
Provider survey, e.g. “Are you intending to serve more
participants in the next year than you did in the last?”
Compare across respondent region and support type.
2.2: Share of providers
intending to expand into/
withdraw from support types/
regions.
Provider survey, e.g. “Are you intending to expand the
number of regions in which you operate?
Compare across respondent region and support type.
4.2: Number and share of
providers which expanded
into new markets.
NDIA payment and claims data
Number of providers who sought payments from more
regions/ support types in this year than last
4.1: Number and share of
providers which withdrew
from current markets.
NDIA payment and claims data
Number of providers who sought payments from fewer
regions/ support types in this year than last
3.1: Level of utilisation by
support type and geography
(“utilisation rate”)
NDIA planning and claims data
Share of funds allocated in participant plan which were
disbursed in the relevant time period
Compare relative averages and distribution across markets
3.2: Change in utilisation rate
over time by support type and
geography
NDIA planning and claims data
Percentage point change in utilisation rate from one time
period to the next
2
4
3
1
McKinsey & Company 38
understand whether the supply gap is likely to worsen over time. If this data confirms that
providers are struggling to provide the required supports in a financially sustainable fashion,
and supply gaps are likely to continue, the NDIA should proceed to evaluate the effectiveness
of different interventions to address this risk of supply shortage.
In some cases, this market monitoring process will identify instances where participants
require a more immediate solution than amendments to price controls or related policies. This
is discussed in further detail in Section 4.5 (Thin and undersupplied markets).
Step 3: Policy decision
The data collected by the NDIA should inform its annual price review, but also inform any
interim price or non-price interventions that may be required. Interim interventions should be
used where there is an immediate market concern, as was the case with the change of short
term accommodation prices in October 2017. Once the NDIA has assessed markets that need
intervention, it should identify intervention options which may involve targeted adjustments to
specific policies or terms of business (e.g. travel or remoteness policies), non-price levers
such as changes to the planning process or NDIA’s systems and processes, or changes to
prices.
The identified policy options should be assessed against each of the NDIA aspirations, to test
which options will have the most favourable impact on all aspirations while ensuring that
participants are able to access all the services for which they have funding. This should be
done with input from all relevant parts of the NDIA, so that information on how the options will
affect each of participant outcomes, market development, and Scheme sustainability can be
fully considered. The assessment of policy options should be coordinated by the Provider,
Market and Sector development team and made available to all relevant decision makers,
including the CEO and the Board.
The NDIA should consider the addition of new organisational mechanisms to support this
stronger internal collaboration and ensure proper governance of the pricing process. It may be
appropriate to establish a pricing reference group with participation from all relevant parts of
the NDIA, such as the Scheme Actuary, senior management, the Provider, Market and Sector
development team etc. For pricing decisions which affect a smaller part of the market or
Scheme spend, the NDIA may consider authorising the CEO or the Provider, Market and
Sector development team to make policy decisions. Regardless of the model chosen, the
NDIA should be satisfied that holistic information is available on the rationale and
consequences of changes in price levels or other policies.
Step 4: Implementation of decision
The NDIA should give providers sufficient notice of price changes that result from the annual
price reviews. The IPR team recommends that this notification period be one month for core
and capacity building supports. A notification period of a month will allow organisations to
calculate the impact of new prices and make informed business decisions. It will also allow
providers to communicate and advocate for their new prices to participants. Price changes
should also be scheduled to take effect at the beginning of the financial year to align with the
corporate planning procedures of providers. The NDIA should also make clear the reasoning
for price decisions and disclose relevant market data.

McKinsey & Company 39
For interim price adjustments where a single support service or market is being affected, a
shorter notice period of two weeks would be acceptable. This is because by their nature
interim pricing decisions need to be implemented more rapidly, and are likely to affect a
smaller proportion of the Scheme.
Alternatives to an hourly rate
Issues and evidence
It is important to differentiate between the funding model and the pricing approach of the
NDIS. The NDIS funds individual supports for participants, to help them achieve their goals
and desired outcomes. Under the previous block-funding model, providers were funded to
deliver a range of services to a participant over a quarter or year.
The predominant mechanism for setting prices across the NDIS is a cap on the hourly (or
other time-based) rate that can be charged for providing the relevant support service. Under
this approach, providers are paid for their ‘inputs’.
Input-based pricing, sometimes referred to as fee-for-service, rewards providers for work
done, and creates a transparent price that can be used to stimulate provider efficiency.
However, this form of pricing is sometimes criticised for creating incentives for providers to
increase volume of services, rather than focusing on how to improve outcomes.
Outcome-based pricing is an alternative method which remunerates service providers based
on an agreed improvement in the service user’s outcomes resulting from the provision of
services. For example, employment services could be priced based on whether users of the
services are able to obtain and maintain stable employment. An example of such a payment
model for providers is the Federal Government’s jobactive program. Outcome-based pricing
encourages innovation by prioritising the delivery of the desired outcomes at the lowest cost.
It encourages providers to find more productive ways to deliver services, rather than
rewarding providers who simply provide the highest volume of services. However, this method
requires outcomes which are able to be clearly defined and monitored so that the
improvements can be measured and an appropriate price established. The method also
requires careful design choices so that providers are not encouraged to deliver short-term
measurable outcomes at the expense of more sustainable, long-term improvements in a
participant’s welfare.
Recommendations
2: The NDIA should continue to use an hourly rate approach, but trial outcomes-based pricing
The current measures of participant outcomes are not yet sufficiently defined or tested to
support an outcomes-based pricing model. Currently the NDIA is measuring progress of
participants against multiple outcomes through the Short-form Outcomes Framework
questionnaire, and as part of participant plan reviews. However, many of these outcomes are
broadly defined such as increased choice and control or community participation. Given that
many participants are receiving different supports from a range of providers, it will be difficult
to attribute improvements in outcomes to a specific support. In addition, there are not yet clear

McKinsey & Company 40
outcomes baselines for most services, or alignment on evidence-based approaches to test
and monitor improvements in outcomes. As a result, outcomes-based pricing approaches will
require further development and testing before becoming a viable alternative to the current
hourly rate approach.
The NDIA should start to build its capability to design and manage outcome-based pricing
through a trial for a support service which is amenable to outcomes measurement. Services
which are most amenable to outcome measurements include employment services, learning
supports, and some types of physical or behavioural therapy. For example, the NDIA could
pay providers of employment supports a bonus based on their ability to find stable
employment for participants. To encourage long-term improvements in outcomes, such
bonuses could be paid out in part at the time of placing a participant in a job, and in part at the
12-month mark if the participant continues to be in work. For behavioural supports, the NDIA
could reward providers based on their ability to reduce the incidence of certain behaviours or
behavioural interventions such as restrictive practices. Before commencing any trial, the NDIA
will need to be satisfied that it has a good understanding of baseline outcomes in that market,
and the capability to both monitor and price outcomes going forward. A trial would develop the
NDIA’s capacity in designing outcomes-based pricing systems, offer useful insights on
whether the NDIA is able to sufficiently monitor outcomes, test whether providers can adjust to
this model of service provision, and provide evidence for whether such a system improves
participant outcomes.
4.2 NATIONAL VS REGIONAL PRICING
One of the questions posed for the IPR team was whether there are significant differences in
the costs of serving participants within and across states and territories.
Within states and territories, the cost of service provision varies by geography due to travel
and other service delivery costs associated with remote and very remote areas. For example,
in very remote areas providers often incur higher wages, higher accommodation and food
costs and higher staff turnover. To compensate providers for these costs, the NDIA applies
loadings to prices of 25% in very remote areas and 20% in remote areas.
Once travel and remoteness are accounted for, there is little difference in cost structures
within a state. In the disability sector, approximately 80% of the cost of service provision is
labour, and labour costs are typically based on the SCHADS Award.30 Most providers pay
their workers in line with these award rates or their EBAs, with no further adjustments for the
location of service provision.
Across states, labour costs vary a little due to some small differences in award rates. These
differences are minor (under 3%) and will converge by 2020.31 The NDIA currently has two
30 Estimate based on independent modelling of the IPR, consultation with providers and comparison with modelling of comparable Schemes. The NDIA’s current pricing methodology makes a similar assumption as to share of labour costs.
31 See Appendix C for further detail on SCHADS Awards by state. Convergence of national awards is a result of the Equal Remuneration Order (ERO) made by the Fair Work Commission in 2012. For full detail on the ERO and SCHADS Awards rates, see: https://www.fairwork.gov.au/pay/minimum-wages/social-and-community-services-industry-pay-rates.

McKinsey & Company 41
price guides – one for Eastern states (NSW, VIC, QLD, TAS) and one for Western states
(ACT, NT, SA, WA). The difference in prices between these guides does not correlate with
differences in SCHADS Awards or other cost differences between those states. The current
disparity between these price guides appears to be based on legacy arrangements among
jurisdictions, rather than any direct correlation with regional costs.
Section 4.2 covers the following topics:
■ 4.2.1 Service provision in remote and very remote regions
■ 4.2.2 Service provision in rural areas
■ 4.2.3 Single national price
Service provision in remote and very remote regions
Issues and Evidence
The NDIS operates in several regions which are located far from existing providers and
workforces. These regions are categorised as remote or very remote, depending on
classification systems that assess a combination of population size and distance factors.
The NDIA is currently changing the classification system it uses from ‘Remoteness Areas’
(RA),32 which ranges from category 1 to 5 by increasing remoteness, to the ‘Modified Monash
Model’ (MM), which ranges from category 1 to 7 in the same way.33
‘Remote’ regions are those classified as ‘MM 6’ and are broadly comparable to RA – 4.
Examples include the Central Highlands region in Queensland and Western NSW. ‘Very
remote’ regions are those with the ‘MM 7’ classification and are broadly comparable to RA – 5.
Examples of the most remote regions catered to by the NDIS include the unincorporated
regions of far western NSW, the Central Desert region in the Northern Territory, and the
Central Highlands region in Queensland.
The cost of service provision in remote and very remote areas is often higher than in other
regions due to travel and other service delivery costs – for example, higher wages, higher
accommodation and food costs, and higher staff turnover. To compensate providers for these
costs, the NDIA applies loadings to prices of 25% in very remote areas and 20% in remote
areas. These percentages are based on loadings developed by the Independent Hospital
Pricing Authority (IPHA). Some providers stated that the remoteness loadings are inadequate
in situations where air travel or long-distance road travel is required to serve isolated
communities, or where local market infrastructure is limited.
In the absence of local supply, providers sometimes need to resort to fly-in, fly-out (FIFO) or
drive-in, drive-out (DIDO) service models to reach isolated communities that may be located
tens to hundreds of kilometres from the nearest town (e.g. Palm Island). Furthermore, the cost
of running and maintaining off-road vehicles is very high. Providers have reported to the IPR
32 Remoteness Area classifications are based on the Accessibility/Remoteness Index of Australia (ARIA) and the Australian Statistical Geography Standard (ASGS).
33 See National Disability Insurance Agency: Rural and Remote Strategy 2016 – 2019 (February 2016) for more detail on how the NDIA classifies areas according to remoteness.
McKinsey & Company 42
team that they could spend up to $2,000 per vehicle per month for leasing (or depreciation)
and operational costs. Due to the remote areas that they cater to, there are few opportunities
for economies of scale and some providers maintain fleets with tens of vehicles. Many of
these costs can be avoided if service delivery was instead conducted by more local
workforces but this is difficult in the short term.
Many isolated communities are discrete Indigenous communities. In these communities,
service provision must account for a range of cultural factors such as: gender matching for
workforce and clients, family-based decision making, differences in conceptualisation of
disability, and travel challenges for participants that may result in unexpected cancellations.
Providers indicated that catering to remote and very remote areas often requires an
investment to build up foundational market infrastructure. For example, participants in the
region might not yet have been identified by the NDIA, nor is there an understanding within
the community of the value of disability support services. One provider consulted by the IPR
team illustrated this issue with recent experience. The provider described a market in remote
North Queensland with a population of approximately 1,000 people (60% of whom were of
CALD background) where just one NDIS participant had been identified, even though a
greater need for support existed. The provider worked with health care providers and the local
community to identify a further dozen people in need of disability supports and facilitated their
introduction to the NDIS. This provider has been able to introduce sustainable services in
these regions but the market is unlikely to be large enough for two providers, and the provider
is unlikely to be able to invest in developing other new markets without some support for the
upfront investment that is required.
Recommendations
3: In very remote/isolated areas, the NDIA should work with other community services and providers to support local workforce development to deliver services in the most efficient way possible. In regions with limited local supply, allow providers to quote on cost of delivering NDIS services in the short term to ensure supply.
The challenges described above are not unique to the NDIS. Many other government
services, such as health and education, have faced similar challenges in providing services to
remote and very remote communities. While price is one lever that can help encourage
supply, a more holistic approach is needed.
The NDIA should prioritise identifying areas and individuals that constitute either thin markets
at risk of under-supply or underpenetrated markets with unmet demand. Analysis to identify
these markets should leverage data on participant residences and support requirements,
provider office locations and support offerings, and plan utilisation. Many of the isolated
communities falling into this category will be discrete Indigenous communities (including ATSI
participants) that will require a coordinated and culturally sensitive approach to service
provision.
The NDIA should then work with other community services and providers to support local
workforce development that increases the reliability and quality of care while driving down the
cost of supply. This could include working with the Aboriginal Medical Services (AMS) to
deliver services in predominantly Indigenous communities. Extending the reach of the AMS

McKinsey & Company 43
may be preferable to new providers who have little experience working with Indigenous
communities.
Whilst development of a local workforce is preferable, there will be some regions where this
is not possible in the short term and where cost of service provision is high. In these areas,
the NDIA should establish a quoting system by which providers can bid for supplying services
to underserved areas. In some regions, it may be feasible to establish panels of providers to
quote on service delivery, to streamline the procurement process. While the quoting method
is bureaucratically more demanding, other policy options are unlikely to address the lack of
supply in these areas. For example, adjustments to the price loadings for remote areas (20%)
and very remote areas (25%) are unlikely to cater to the full spectrum of challenges that
providers face. The variability in cost of service provision and the non-price challenges that
must be overcome (e.g. engaging with local communities) require a coordinated effort from
the NDIA, other mainstream services, and providers.
Implications
Participant outcomes and market development will be improved at lower cost if the NDIA
successfully works with existing health service providers and communities to develop local
capacity. However, this may not be able to be achieved immediately.
In the short term, establishing the operational capacity to manage a quoting process will be
important. It is expected that higher prices are likely to result from this process in isolated
areas, but given the small proportion of participants in these regions, Scheme expenditure will
not increase significantly. This process is likely to lead to more sustainable coverage of these
areas and improvement in participant outcomes, including ATSI communities.
Service provision in rural areas
Issues and evidence
Some of the challenges associated with service provision in remote/very remote areas are
relevant to providers serving rural areas as well. While price loadings exist for MM 6 and MM
7 areas, providers serving individuals and communities in ‘outer regional’ or ‘rural’ areas,
which correspond anecdotally to MM 4 and MM 5 areas, cite geographic spread and high
travel costs as contributing to higher costs. As a result, it appears that some providers have
terminated services to participants living more than a certain distance away from offices or
have expressed plans to withdraw services from rural communities.
MM4 areas are defined as areas in Remoteness Area 2 (RA2) and Remoteness Area 3 (RA3),
per the Australian Standard Geographical Classification, that are not in MM3, and are within
10 km road distance of a town with population between 5,000 and 15,000 people. MM5 areas
are all other areas in RA2 and RA3. Provider travel times to and between participants in MM 4
and MM 5 areas exceed 20 minutes, the current limit on time that attendant care providers
can charge for travel between participants, in a significant number of cases. Providers cite
averages that are often closer to 30-45 minutes due to low participant density and geographic
spread of rural farms and communities. In extreme cases, providers in rural areas take an
hour to several hours to reach the site of support service provision. In practice, many
providers absorb all travel costs, inclusive of the first 20 minutes of travel, due to a reluctance

McKinsey & Company 44
to reduce service levels, as plans are often insufficient to cover travel times while still ensuring
that clients receive necessary supports. Participants may also expect to be charged for and
receive a full hour of service due to unclear communication and insufficient participant
education.
Several providers have instituted policies that stipulate a radius outside of which they are no
longer able to provide service. For example, upon transitioning to the NDIS, a provider in
regional Victoria has chosen to no longer serve clients located more than 10 kilometres from
its office, while a provider in regional New South Wales has chosen to only serve participants
located within 30 minutes from an office. Travel costs often compound other challenges of
rural service delivery including lack of appropriate facilities and extreme weather, and
inefficient staff rostering. Some providers consulted by the IPR team expressed an intent to
withdraw from such areas due to these location-specific costs of service. For example, a
provider in Queensland identified that supports in the Charters Towers regions (MM 4) were
financially unsustainable as it involved costs associated with servicing regional areas which
were not adequately recognised by the current NDIS pricing arrangements. These difficulties
are currently challenging to identify or diagnose, as travel expenses are not monitored as a
separate line item in the NDIA payments system. It is instead included as a part of the care
provided. There is therefore no ongoing record of providers’ travel times.
It is important to note that as the Scheme matures, development of local workforces will help
alleviate this problem. It is expected that participants in rural areas – in particular in MM4,
which is defined as being within 10km of a town of 5,000-15,000 people – will be served by
local providers. However, the IPR recognises that development of these local workforces
takes time, and there needs to be a mechanism to ensure that participants in these areas are
not disadvantaged in the short term, by compensating providers for costs incurred.
Recommendations
4: The NDIA should clearly define rural areas and lift travel allowance from 20 minutes to 45 minutes for providers serving a participant located in MM5 (or ARIA equivalent) and MM4 in the short term. Adjust participant plans to account for travel and track travel as a separate line item.
While the NDIA released a Rural and Remote Strategy in February 2016, some providers
noted continued ambiguity over the official definition of ‘rural’. Thus, ‘rural’ areas should first
be formally defined with reference to a consistent geographical category. This classification
could rely on either the Modified Monash Model (likely Levels 4 and 5), or on Remoteness
Areas calculated with reference to the Accessibility/Remoteness Index of Australia (ARIA).
Once this definition is in place, adjustment to the provider travel policy would be the most
direct and cost-effective way to support supply. To compensate providers for high travel times
in rural areas, the NDIA should increase the 20-minute travel cap for providers of eligible
supports, and should align this travel policy with that of therapy (see Section 4.6.4 for
recommendations relating to travel for therapy supports). The IPR believes a travel cap of 45
minutes is more appropriate.
The IPR team recognises the risk that more generous compensation of travel costs may
create an incentive for some providers to use travelling workforces rather than the more
efficient model of building local workforces, which is a core aspiration for the NDIA. However,

McKinsey & Company 45
workforce development in small towns of less than 15,000 people can often be challenging in
the short term. Therefore, the IPR recommends that this change in policy be applied to
participants in MM4 and MM5 in the near term, but changed in the medium term (3 to 4 years)
to apply only to participants in MM5. A travel cap of 45 minutes is unlikely to cover all costs of
travel to participants in MM5. Providers will need to look for opportunities to cluster
participants and coordinate service provision to reduce travel times.
This policy does not remove the commercial incentive for participants to choose providers who
are able to provide services without the additional expense of travel costs. As such, the IPR
team believes this travel adjustment is an acceptable balancing of competing priorities In the
medium term, the NDIA could explore mechanisms to reduce the incentive for providers to
travel, such as planning processes that only allow providers to charge for travel where there
are no local alternatives.
An alternative option would be to add a price loading to rural areas, as is done with remote
and very remote areas. The Health system, via the General Practice Rural Incentives
Program, and Aged Care system, via the viability supplement and home care subsidy rates,
currently provide additional compensation for service in MM 4-5 areas. However, it is mainly
travel driving the increased cost of service to participants in rural areas. More than doubling
the travel time allowed to be claimed by providers would provide a more targeted and effective
intervention than a broad price loading, which does not account for the specific amount of
travel a provider undertakes.
Travel should be tracked as a separate line item in NDIA payment data. This will allow the
NDIA to monitor travel costs and better understand how providers and participants are
allocating the costs of travel. Such monitoring will also allow the NDIA to understand whether
more generous travel pricing provides a perverse incentive for providers to travel long
distances rather than invest in local workforce development, or to encourage participants to
attend the provider premises. This monitoring and better understanding of travel behaviour
might then pave the way for the deregulation of travel costs. Removing travel caps to allow
complete fungibility of travel versus direct service funding would enable providers to charge
for any amount of travel (subject to agreement with participants), affording participants
maximum choice and control and requiring providers to reduce travel costs to remain
competitive. In some areas with high participant density and sufficient supply, travel
deregulation may be appropriate provided participants can make informed choices between
providers located at varying distances from their residence. Participants, planners, and LACs
would require education to understand the availability of supply for each participant as well as
the outcome implications of trading off travel and direct service. The NDIA should maintain
travel caps in the near term, including an expanded cap for travel in rural areas, with the
option of exploring travel deregulation as the NDIS matures.
Service provision in rural areas can also be affected by restrictions on the ability of
participants to transport themselves to and from support services. This was an issue
highlighted by providers during the IPR team’s consultation process (see Section 2). However,
this issue is beyond the remit of the IPR. The NDIA could work with LACs, planners as well as
the states and other local authorities to understand if a participant has public transport
available to them and the capability to utilise the service. The IPR team recognises that
solutions to transport will have implications for the adequacy of supply and support access in
remote and rural areas.

McKinsey & Company 46
Implications
The short-term implications of this change in travel policy for Scheme expenditure is difficult
to estimate with precision as the NDIA does not currently track travel as a separate item. For
instance, a provider who charges for an hour of service provision may have had no travel, or
have used the full travel entitlement of 20 minutes and provided 40 minutes of care.
The IPR has made a number of assumptions to estimate potential costs, based on available
information. Assuming a quarter of the participants who receive supports in regional areas
(MM 4 and MM 5) are now provided services which attract additional travel entitlements, and
that 45 minutes of travel is charged for approximately every four hours of support provided,
the additional annual cost to the NDIS would be approximately $75 million.
Increasing the amount of travel time providers can charge will require planning process
adjustments. Participants living in rural areas who require providers to travel to them, and who
can only be served by providers requiring more than 20 minutes travel, should be given
proportionally larger plan allocations to account for the cost of travel within these areas. As
with other changes to price caps which affect how plans are constructed, participant education
initiatives and additional coordination of support should be offered in parallel, to ensure that
participants are able to factor in provider travel times when exercising choice and control.
As the Scheme matures and local workforces develop, the NDIA should review this policy and
assess whether other incentives may be more appropriate to encourage local supply and
reduce the incentive for providers to travel long distances to deliver supports.
Single national price
Issues and evidence
The NDIA currently has two different price guides, with typically lower prices in Eastern states
(NSW, VIC, QLD, TAS) and higher prices in Western states (ACT, NT, SA, WA). For example,
the price for ‘assistance with self-care activities during daytime weekdays’ differs by 1.8%
between the two guides. In the ACT, NT, South Australia or Western Australia, providers can
charge $45.54, while in the remaining states the cap is $44.72. The differences between other
prices range from 0-12%. For example, higher intensity group care on Sundays is capped at
$57.18 in ACT and the western states and territories, while it is capped at $52.84 in the other
states.
There is no clear rationale for maintaining separate price guides. Current disparity between
the Eastern and Western price guides appears to be based largely on legacy arrangements
between jurisdictions, rather than on a direct correlation with regional costs. Whilst there is
currently some minor variation in labour costs between states, it is not correlated to the
division of price guides. Analysis of labour costs other than award wages, such as payroll tax,
leave entitlements and workers compensation requirements, does not show a consistent
difference between the eastern states and western states.34
34 See Appendix C for more details on differences in award rates between States and analysis of other cost differences.

McKinsey & Company 47
Recommendations
5: The NDIA should converge the two Price Guides and move toward a single national price guide by 2021.
In the absence of stronger justification for differentiated price guides across states, the NDIA
should progressively converge prices to promote pricing simplicity, ease of communication,
and systems efficiency for providers operating across multiple states. This price convergence
should occur by 2021.
It is the IPR team’s view that the NDIA should not attempt to capture the price differences
between each state through tailored state-specific price guides, as this is likely to lead to
significant pricing complexity and may also fracture a national market. Cost differences within
states, driven for example by remoteness of a region, are more important factors, and these
are accounted for through specific policies (see Sections 4.2.1 and 4.2.2 above).
Implications
Transition to a single national price guide will need to occur over the next three years. This
can be done by adjusting the relative rates of annual inflation between the eastern and
western price guides such that the two price guides converge over time. Once implemented,
providers operating nationally will benefit from the simplicity of one national price guide.
4.3 PRICING OF ONE-TO-ONE SERVICES WITH DIFFERENT LEVELS
OF COMPLEXITY
The NDIA recognises participants entering the NDIS will have a range of disability types,
levels of functional impairment, and requirements of a support worker to meet their needs.
A two-tiered pricing structure is in place to allow a high intensity rate to be charged by a
provider. The high intensity rate is set at 5.5% higher than the standard rate, applicable where
a participant’s complex needs require assistance from a support worker with a higher skill
level. Support workers serving participants with complex needs are sometimes exposed to
a higher level of safety risk, which can be to a participant or to themselves, and the higher skill
levels and pay rates ensure the support worker is fit to provide quality services to participants
in these environments. Examples of environments with greater safety risk could include a
support worker serving a participant with medical needs where health-related intervention is
a core component of service delivery, or serving a participant with behaviours of concern that
could result in the participant attempting to self-harm or harm the support worker.
The key concerns raised by providers related to the quantum of the high intensity loading
being insufficient to cover the cost of employing a higher skilled worker, and the loading not
accounting for the additional time required to service participants with complex needs,
including team meetings, report writing, training, and more frequent incident management.
Additional concerns included the inconsistent application of high intensity loading across Core
Support Items in the Price Guide. Examples include centre-based care having no high
intensity rate, and not allowing for increased carer ratios, and the inconsistent allocation of the
high intensity loading across participants. Currently, responsibility falls on a provider to agree
with a participant that a high intensity loading is necessary for them to receive the level of care
that will help them achieve their desired outcomes.

McKinsey & Company 48
This section covers the following topics:
■ 4.3.1 Definition of complexity and quantum of the high intensity rate
■ 4.3.2 Participants with extreme behaviours of concern
■ 4.3.3 Consistency of pricing for participants with complex needs across core supports
Definition of complexity and quantum of the high intensity rate
Issues and evidence
There is no simple definition communicated to the sector of what complexity means in a
pricing context, and as a result, the term complexity is used inconsistently. Providers link
complexity to the ratio of care a participant requires i.e. the number of carers, the number
of hours of care a participant has allowance for in their plans, also referred to as ‘intensity
of care’, and more subjectively, to how difficult a provider believes it is to serve a participant.
There are cohorts of participants that require support workers with specific skillsets above the
level of a typical support worker, which cost providers more to employ. Providers are not
consistently receiving a high intensity loading to serve these participants due to the lack of
clarity in the definition of complexity. The link between a participant’s needs, the cost drivers
of a provider, and price is not clear, which leads to inconsistent application of the high
intensity price loading. The policy placing the responsibility on providers to determine whether
a participant should be charged a high intensity rate exacerbates the issue, as providers each
have their own definition of complexity.
Provider submissions to the IPR showed that many providers employ support workers serving
participants without complex needs between SCHADS Level 2.2 to Level 2.4. This is
consistent with NDIA expectations and the responsibilities outlined in the Award for a Social
and Community Services Employee Level 2.35 To serve participants with complex needs,
providers often employ support workers at a base wage level between a SCHADS 2.4 and 3.3
to match the workers increased level of skill and experience. There is evidence of some
providers employing workers up to and above SCHADS Level 4. For participants classified as
having complex needs because of a medical condition, additional skills of a support worker
can include the ability to recognise the need for health-related intervention, and administer
medication by injection, or feeding through a nasogastric tube. For participants classified as
having complex needs because of behaviours of concern, additional skills of a support worker
can include the ability to recognise symptoms or presentations of mental illness and intervene
to de-escalate violent behaviours. To serve participants with complex needs resulting from
medical or behavioural presentations, support workers are required to exercise judgement
based on prior knowledge and experience to determine the course of action necessary to
35 The Award states the responsibilities of a Level 2 employee are: ‘(k) implementing client skills and activities programmes under limited supervision either individually or as part of a team as part of the delivery of disability services’ and ‘(l) supervising or providing a wide range of personal care services to residents under limited supervision either individually or as part of a team as part of the delivery of disability services’. The Fair Work Commission: Social, Community, Healthcare and Disability Services Industry Award 2010 (updated 29 July 2017), p. 52

McKinsey & Company 49
address the situation. These attributes closely align to the characteristics necessary of a Level
3 employee.36
The high intensity loading of 5.5% is intended to provide additional funds where a participant
requires assistance from a support worker with additional skills or experience relevant to a
participant’s complex needs. The loading provides enough funding to allow an employer to
pay a support worker between a SCHADS 2.4 and 3.1, which is at the lower end of the wage
level currently being paid by providers, assuming a base level of SCHADS 2.3, which is
consistent with the rate paid by many providers for participants without complex needs. This
could be adequate in some situations such as feeding through a nasogastric tube in a
standard environment. However, where a participant has very serious behaviours of concern,
or a combination of medical needs and behaviours of concern, a worker with a higher level of
skill may be required.
Many providers raised concerns about the high intensity loading not taking into consideration
the incremental ongoing training and development requirements for support workers serving
complex participants. Submissions to the IPR indicated providers are conducting
approximately 3-4 hours of additional training for these support workers each quarter. These
training sessions often bring together groups of support workers and other professionals to
discuss individual client situations and techniques that have been used or developed to deliver
improved outcomes. As the sessions are often internal, the costs incurred by providers are for
support worker time, with no opportunity to recover the cost for the delivery of the training.
Providers serving participants with complex needs reported that they spend more time on
incident management and reporting than other providers, due to the nature of the disabilities
of the participants cohorts they serve. One small provider estimated spending over 200 hours
per year on incident management, with an average of one incident per fortnight, and each
incident requiring a review, report, care team meetings, and a response plan. This was
estimated to have up to a 2-3% impact on the provider’s overall margin. While not all incidents
are avoidable, providers are expected to have effective internal processes to prevent and
respond to incidents.
36 The Award states the characteristics of a Level 3 employee include: ‘General features of this level involve solving problems of limited difficulty using knowledge, judgment and work organisational skills acquired through qualifications and/or previous work experience. Assistance is available from senior employees. Employees may receive instruction on the broader aspects of the work. In addition, employees may provide assistance to lower classified employees.’ The Fair Work Commission: Social, Community, Healthcare and Disability Services Industry Award 2010 (updated 29 July 2017), p. 54

McKinsey & Company 50
Recommendations
6: The NDIA should develop a definition for complexity linked to the skills required to meet participant’s needs, and use its specialised planning resources to classify what skills are required, and which participants require higher skilled support workers.
The NDIA should develop a definition for what complexity means in a pricing context and
communicate it to the sector. The definition must create a clear link between a participant’s
needs and the cost drivers for a provider, that can be translated into price. To serve
participants with complex needs, providers employ support workers with additional skills and
experience, and are required to compensate them with a higher base wage level. The
increased cost of employing these support workers should be translated into the price. The
NDIA can leverage most of the existing definition for high intensity supports in the Price
Guide, but the focus should be on skill level rather than on qualifications, as in some cases
additional qualifications may not develop the specific skills necessary to serve a participant’s
complex needs.
This revised definition should include a clear link between a participant and their needs, and
the relevant and most significant cost driver of a provider being support worker wages.
Examples of participants that would be defined as complex in a pricing context include
participants that exhibit rapid, severe and frequent escalation of violent or self-harm
behaviour, including some participants in the psychosocial and cognitive disability participant
cohorts, and participants that require health-related intervention as part of ongoing support. In
both situations, participants may require a support worker with additional skills to serve them.
The skill level required to service a participant increases with the severity of a participant’s
complex needs, and there should be different tiers of pricing to match the different levels of
skills needed.
The NDIA should use the specialist team of planners it is developing as part of the Participant
Pathway project to develop a set of criteria to determine whether a participant’s requirements
are complex for the purposes of pricing. The objective of the criteria should be to determine
whether a participant requires a higher skilled or qualified support worker for their needs.
The NDIA should assign the responsibility of classifying participants with complex needs for
the purposes of pricing to the specialist planning team. Planners have visibility into participant
records and complexity classifications throughout the participant pathway (see Appendix D –
Existing definitions of complexity that exist within the NDIA), and under the revised pathway
should have face to face interactions with participants to understand their needs and goals.
Each of these sources of information should allow a planner to determine if a participant
requires a support worker with additional skills or experience, and hence a price loading.
As the specialist team builds capability, it should develop and refine the service models used
for participants with complex needs, both health and behaviour related, to make sure
participants receive plans that meet their needs and deliver the best possible outcomes. It
may be difficult for the planning team to build expertise quickly, and in the short-term the NDIA
should consider leveraging industry experts for support until the team is able to manage most
of the cases in-house. The team could continue to reach out to outside experts for advice in
very difficult cases which are outside its area of expertise.

McKinsey & Company 51
7: The NDIA should add an additional tier to the high intensity loading to allow a provider to recover the cost of a support worker with a higher level of skill than can be procured with the current high intensity loading.
The current loading may be sufficient to employ a higher skilled support worker for some
complex needs, such as health-related intervention in a standard environment. However, it
may be less suitable for situations where a participant has serious behaviours of concern, or a
combination of medical needs and behaviours of concern. A third tier classification of ‘Very
Complex’, should allow a provider to employ a mix of support workers at SCHADS Level 3.1
or Level 3.2. The loading should also take into consideration the incremental ongoing training
and development necessary for support workers serving very complex participants estimated
at 1%. The specialist planning team should be responsible for assessing and classifying
participants considered to be Very Complex. The IPR team recognises that there is a small
number of participants for whom it is very difficult develop prices due to the nature of their
disabilities and the environments necessary to deliver their services, and believe a quoting
process is the most appropriate mechanism to ensure they receive the supports required to
meet their needs (see Section 4.3.2). TABLE 3 describes the characteristics of participants
that would be classified as Standard, Complex, Very Complex, and Quoted.
Incidents are more likely to occur for providers serving participants with complex needs.
Providers incur costs associated with incidents such as the time spent on team briefing
meetings and incident report writing. Providers are expected to have effective internal
processes to prevent and respond to incidents, but it is recognised that not all incidents are
avoidable.
The introduction of the NDIS Quality and Safeguarding Framework will have some
implications for providers on the scope of incident reporting requirements. Given the
operational implications of this are not yet known, the IPR recommends that the NDIA revisits
this recommendation in the future to evaluate if providers need to be compensated for the
costs of incident reporting – for example by introducing an incident reporting line item in the
Price Guide to allow for providers to charge for time spent on this activity.
TABLE 3: DESCRIPTION OF PROPOSED LEVELS FOR PARTICIPANTS WITH COMPLEX NEEDS
Classification Participant characteristics
Standard (no price loading)
■ No health-related intervention needs (e.g. feeding through a nasogastric tube, ventilation support)
■ None or mild behaviours of concern
Complex (5.5% price loading)
■ Health-related intervention needs (e.g. feeding through a nasogastric tube, ventilation support)
■ Mild-moderate behaviours of concern (e.g. infrequent rapid escalation of challenging behaviour)
Very Complex (10% price loading)
■ Combination of health-related intervention needs and mild-moderate behaviours of concern
■ Severe behaviours of concern (e.g. rapid, severe and frequent escalation of challenging behaviour)
Quoted ■ Extreme behaviours of concern – see Section 4.3.2 for further details

McKinsey & Company 52
Implications
The NDIA has commenced work to establish specialist planning teams as they develop the
new participant pathway. The specialist team will need to be trained to categorise participants
with complex needs as informed by the tool/set of criteria defined by the NDIA. It is important
that the team monitors the outcomes of their categorisations to help improve accuracy and
consistency over time.
An improved definition of complexity and allocation process will ensure providers are able to
charge a higher rate to participants that require a higher skilled support worker. This will allow
providers to recover the increased cost of direct supports required to service the complex
participant cohort. It will be important to engage with the relevant segments of the sector, both
participant and provider representatives, when developing the final set of characteristics to be
used during the complexity classification. This will limit the number of times providers request
the NDIA to review participant categorisations. In a situation where a provider challenges a
participant’s categorisation, a process needs to be put in place to allow individual cases to
quickly be reviewed by the NDIA if a provider can provide evidence to show the categorisation
is not correct. It should be noted that it is possible some participants are currently being
charged the high intensity rate that would not apply under a new definition. To reduce the
financial impact on providers, the definition should be phased in for participants already in the
NDIS as their plans come up for review.
The expected cost of the additional tier of price loading for participants with complex needs is
between $100m-$140m, which represents 0.5%-0.7% of costs at Full Scheme37. The IPR
team expects the costs to be at the lower end of the range, as the improved definition and
classification process for participants with complex needs will limit the number of participants
that receive the price loading to only those that require a support worker with additional skills.
It is possible the price increase could be absorbed by the utilisation levels within participant
budgets, meaning there could be no impact on the funding envelope. The suggested
approach is to fix each of the definition and classification issues related to complexity before
adjusting the price. This will ensure price loadings are only applied to participants considered
to have complex needs under the improved definition of complexity.
Participants with extreme behaviours of concern
Issues and evidence
Participants with extreme behaviours of concern include participants that are subject to orders
under the justice system, also referred to as forensic disability participants, and previous
offenders no longer subject to orders. Participants with extreme behaviours of concern are not
explicitly recognised in NDIS pricing. Forensic disability participants are typically individuals
with cognitive impairments that have committed criminal offences in the past, but are unable
to be institutionalised due to their condition. They often fall at the extreme end of the spectrum
of behaviours of concern. Providers have historically served this participant cohort with a very
37 Based on 12% of participants qualifying for the complex level (a 6% loading) and 10% of participants qualifying for the very complex level (a 10% loading), with a margin of error of +/- $20m, and assuming all participant plans are adjusted to compensate for the change in policy

McKinsey & Company 53
skilled workforce, such as tertiary educated support workers, and it is not possible for them to
recover costs at the high intensity rate set in the Price Guide.
There is legislation in place that details the responsibilities of the NDIS to participants that
have been offenders under the criminal justice system. The NDIS (Supports for Participants)
Rules 2013, made for the purposes of Sections 33 and 34 of the National Disability Insurance
Scheme Act 2013, outline that forensic disability services are to be funded and delivered as
part of the NDIS.38 Services to be provided to this participant cohort are legislated under a
number of state-based Acts related to the nature of the offence and disability of the
participant.39 A provider requires extensive knowledge of the legislative environment to deliver
services to this participant cohort, who often need intensive supports and services, delivered
by very skilled and experienced professionals. As the services necessary for a participant can
vary significantly from one circumstance to another, it is very difficult for the NDIA to develop
pricing schedules and plans that meet the needs of participants while also adhering to state-
specific legislation.
Providers serving forensic disability participants, often referred to as forensic providers, are
exposed to increased risk compared to providers focused on other participant cohorts. Under
state-based criminal justice system Acts, the management and directors of a provider can be
held criminally liable if a participant under their care re-offends. NDIA policy does not allow
providers to deliver all support items from the Support Coordination support category, to
mitigate the risk of a conflict of interest. There are cases of forensic service providers pulling
out of Support Coordination or refusing to provide the services to participants not in their care
to minimise risk, as the providers do not want to be held criminally liable in a situation where
they are not in full control of a participants care. This puts the specific sub-market at risk of
supply shortages.
The NDIA has put rules in place for the Support Coordination support category to mitigate the
risk of conflicts of interest, specifically for Local Area Coordinators (LACs), which are included
in the NDIS Partners in the Community Program: Program Guidelines (August 2016).40 There
are three Support Items within the Support Coordination support category relevant to the
discussion: Support Connection, Coordination of Supports, and Specialist Support
Coordination. Participants that are classified as Supported or General during the pre-planning
phase, meaning it is easier for the planning team to engage with a participant throughout the
participant pathway, receive Support Connection. Support Connection is delivered by LACs,
38 Section 7.23 explains the meaning of a person not in custody: ‘person not in custody means a person who is subject to the justice system (including relevant elements of the civil justice system), but is not in a custodial setting (for example, a person on bail, a person under a community based order that places controls on the person to manage risks to the individual or to the community, a former prisoner on parole, or a person in home detention)’. Section 7.24 goes on to explain the NDIS responsibilities for a person not in custody ‘The NDIS will be responsible for: (a) in relation to a person not in custody –reasonable and necessary supports on the same basis as all other persons’. National Disability Insurance Scheme Act 2013 (the Act): National Disability Insurance Scheme (Supports for Participants) Rules 2013, Section 7.23 and 7.24, p. 20
39 In Victoria, this can include Supervision Orders under the Serious Sex Offender and Detention Supervision Act 2009 and the Crimes (Mental Impairment and Unfitness to be Tried) Act 1997, Parole Orders (and Bail Conditions) under the Crimes Act 1958 and Corrections Act 1986, and Community Treatment Orders under the Mental Health Act (2014).
40 Section 4.1.1.3 states ‘An Applicant which applies to deliver LAC Services, must not be a Registered Provider of Supports as defined under section 9 of the NDIS Act’. NDIA: NDIS Partners in the Community (Round One) – Program Guidelines, Section 4, p. 9
McKinsey & Company 54
and it is not possible for LACs to deliver Support Connection and provide services to the
participant. Participants classified as Intensive or Super Intensive during the pre-planning
phase, meaning it is more difficult to engage with a participant throughout the participant
pathway, receive Coordination of Supports and/or Specialist Support Coordination. These
Support Items are delivered by providers, not by LACs. It is possible for a provider to deliver
Coordination of Supports and/or Specialist Support Coordination and be a participant’s service
provider, but the provider must ensure they proactively manage conflicts of interest, as per the
Terms of Business for Registered Providers (July 2016).41
The NDIA is currently addressing cases of participants with extreme behaviours of concern
out of their regional offices, and providers have communicated that in some cases they have
been allowed to develop quotes to deliver services to this participant cohort. However, there
are examples of providers being advised that they need to follow the Price Guide, and price
according to the high intensity rate. There is not yet a consistent approach for addressing the
needs of this participant cohort.
Recommendations
8: The NDIA should develop a consistent process for participants with extreme behaviours of concern that acknowledges the specialised needs of the participant cohort, and the environment providers operate in. Providers serving this cohort should quote on the delivery of services to these participants, and be allowed to deliver all services they require to be adequately supported i.e. all Support Coordination items.
The quotes, which would include a detailed support plan for a participant, would be submitted
directly to the specialist planning team (see Section 4.3.1) for review and approval. A quoting
mechanism will be most effective for this participant cohort given that the number of
participants in this cohort is very small, the number of providers servicing the participant
cohort is also very small, effectively making it a thin market, and the services necessary to
support participants will vary significantly from one individual to another.
Allowing providers to deliver all Support Coordination services will ensure individuals in this
participant cohort receive the services they require to be adequately supported, and help to
eliminate the risk of supply shortages leading to participants not being able to procure
services. Detailed reviews of the quotes submitted to the specialist planning team to ensure
participants are only receiving the supports required to meet their needs can help the NDIA
protect against conflicts of interest.
Implications
The NDIA will need to set up a quoting process to allow providers to submit quotes for review
and approval. For the NDIA to review and approve quotes, the capability of the specialist
planning team needs to be place with a clear understanding of the needs of the forensic
disability participant cohort as well as of the legislative environment in which forensic service
providers operate. To speed up the quoting process and ensure forensic disability participants
41 The Terms state ‘Registered Providers must ensure that they proactively manage perceived and actual conflicts of interest, including through development and maintenance of organisational policies’ NDIA: Terms of Business for Registered Providers (effective 18 April 2016), p. 3

McKinsey & Company 55
can move into a care environment as quickly as possible, the NDIA may identify a list of
preferred providers in each state that can be contacted at short notice.
From a participant perspective, allowing forensic service providers to deliver all supports to
them could be considered as a conflict that limits choice and control. Considering the
legislative environment providers operate in, it is unlikely a participant will receive a range of
services from multiple providers. It is a better outcome for the participants to have the services
available to them than not at all due to providers not wanting to take on additional risk.
Consistency of pricing for participants with complex needs across core supports
Issues and evidence
There are inconsistencies with the application of high intensity loadings and care ratios across
different core supports. Support items including ‘Assistance with self-care activities’ and
‘Assistance to access community, social/recreational activities’ allow providers to charge a
high intensity loading where assistance is required from a support worker with additional skills
or experience relevant to the participant’s complex needs. The support items also allow
providers to charge different prices dependent on the care ratio necessary to support a
participant. This can either be a lower care ratio, such as 1:2 or 1:3, where a single support
worker can service multiple participants at the same time, or higher care ratio, such as 2:1 or
3:1, where multiple support workers are required to serve a single participant.
The support item ‘Group based activities in a centre’, does not allow providers to charge a
high intensity loading, meaning providers cannot be compensated for the additional cost they
incur for a highly skilled support worker if a participant with complex needs chooses to utilise
the service. This support item is also set at a price between the 1:2 and 1:3 care ratio for
Assistance with self-care activities and Assistance to access community, social/recreational
activities, and does not provide the flexibility to providers to either increase or decrease the
price based on the number of participants in the group.
Recommendations
9: The NDIA should update the pricing structure for the core support item ‘Group based activities in a centre’, to allow providers to charge a high intensity loading where a more skilled worker is required to serve a participant, and set prices consistent with the care ratio required to serve a participant.
The NDIA should ensure pricing for ‘Group based activities in a centre’ adopts the same
approach used for other core supports, including Support Items ‘Assistance with self-care
activities’ and ‘Assistance to access community, social/recreational activities’. This
recommendation is not designed to encourage a participant to lead a life with a high intensity
of support. Rather, it is expected that as the Scheme matures and evidence develops,
providers and the NDIA will be able to assess which interventions are most effective in
supporting participants with complex behaviours and needs to achieve improved outcomes
and, in some cases, no longer require high intensity support.

McKinsey & Company 56
Implications
Participants with complex needs utilising ‘Group based activities in a centre’ will be required to
pay a higher price for the service. They will need to choose whether they would like to
continue utilising the services at the higher price, or if their funding can be used more
effectively with a different mix of services.
4.4 PRICING OF SHORT TERM ACCOMMODATION SERVICES
The NDIA recognises participants may at times have periods where their support
arrangements need to be different from the regular level of support they receive. Short-term
accommodation (STA), also known as Respite, is a Core Support available to participants to
provide third-party care in a group based facility or in-home support. The service is often used
by participants whose regular support is delivered at home by family members, allowing family
members the opportunity to have some time off from being the primary care giver. It also gives
participants the opportunity to socialise with peers in a safe environment.
At the time of the provider consultation phase of the IPR, a flat price of $501.71/day42 was in
place for STA, and most concerns by providers related to the lack of price differentiation. The
key concern voiced by providers was that a single price for the STA support item did not
reflect variations in the cost of service delivery by the day of the week, or by the care ratio
necessary to serve a participant. Providers also raised the issue that there was no allowance
in the price to compensate them for the capital invested in the facilities. After the completion of
the consultation phase of the IPR, the NDIA announced price changes effective 30 October
2017 to address issues related to the STA price.
Issues and evidence
Under a single price point, many providers found it difficult to operate economically on
weekends and public holidays, when they were required to pay penalty rates to support
workers, and when participants required higher care ratios such as one-on-one support. As a
result, providers began to withdraw services from the market, either by closing their facilities
on specific days of the week, by no longer providing services to participants that required high
care ratios, or by shutting down their short-term accommodation services completely.
Recently, this issue became acute in the ACT, where providers Duo and Carers ACT closed
their short-term accommodation services, and Marymead, the only other provider, signalled
they were going to follow, having already restricted services to participants that required low
care ratios on specific days of the week that did not involve substantially higher labour costs.
The NDIA responded to the market reaction and revised the price of STA, releasing a new
price schedule, effective 30 October 2017. The NDIA adjusted the price, basing it on the price
of attendant care, to better reflect the variable costs of service delivery on different days of the
week and at different care ratios for participants, and capital employed in facilities. The
revised pricing schedule includes differentiated prices for weekdays, weekends, and public
holidays, as well as for care ratios of 1:4, 1:2, and 1:1 support needs. Each of the prices also
42 NDIA: 2017/18 NDIS Price Guide VIC-NSW-QLD-TAS (version release date July 2017), p. 40

McKinsey & Company 57
includes a capital allowance. The NDIA has established a process for participants who are
fully utilising their plans to review participant budgets and ensure participants are not
disadvantaged by the price increases.
Recommendations
10: The NDIA should continue to refine the assumptions for high intensity rates, active overnight, and capital allowances used to develop the new STA price schedule, to ensure they reflect the cost of service delivery.
The IPR team agrees with the approach used by the NDIA to develop a differentiated price
schedule based on the price of attendant care, that is more reflective of the cost of service
delivery for providers. Assumptions around provider operating models have been used to
develop the new pricing schedule, and the NDIA should continue to refine each of these to
reflect an efficient provider’s costs.
The NDIA has applied the high intensity loading to each care ratio to build up the new STA
pricing schedule. This high intensity loading should only be used where a participant
requires assistance from a support worker with additional skills or experience relevant to the
participant’s complex needs. Participants with complex needs are less likely to be served
under low care ratios. The NDIA should consider using the standard intensity rate for lower
care ratios (1:4 and 1:2), and in those special cases have two prices for a 1:1 care ratio, one
price based on the standard rate (for participants with high physical disabilities) and one
price based on the high intensity rate for participants with complex needs.
For each care ratio, the assumption made in the price is that the support worker will be
required to work 8 hours of an active overnight shift, meaning the support worker is required
to be awake and active throughout the night. Provider consultation raised the point that this
should only be necessary in extreme cases, and it would be reasonable to assume that for
participants without complex needs, a support worker works a night-time sleepover shift, with
up to two hours of active overnight hours to allow for disruptions during the night. The NDIA
should consider using an overnight shift with up to two hours of active overnight for low care
ratios, and an active overnight shift only when a high care ratio is required for a participant
with highly complex behavioural needs.
An accommodation allowance of $200 per night has been included to cover board and meals
throughout the new pricing schedule. The $200 figure is the average cost of i) accommodation
costs for a day of respite in aged care facilities ($140), based on rates set by the Australian
Government for My Aged Care, and ii) accommodation costs for a day in acute care or a
hospital setting ($260), as sourced from the Independent Hospital Pricing Authority (IHPA).
The NDIA should continue to refine the capital allowance by reviewing the operating costs of
providers. A review of the financials of providers that made submissions related to STA
indicated accommodation and other overhead costs could be below $100 per day. This is from
a small sample of providers, but it indicates that the operating costs are much less
comparable to hospitals, and the aged care comparison of $140 per day could be a more
reasonable assumption.

McKinsey & Company 58
4.5 THIN AND UNDERSUPPLIED MARKETS
A ‘thin’ or ‘undersupplied’ market is one in which there is a persistently low level of supply
relative to demand. This is often due to structural features of the market that makes it
expensive or difficult for providers to compete effectively. Thin markets are a key policy
concern for the NDIS as the presence of thin and undersupplied markets can compromise
participant outcomes in that region.
While price caps may have an impact on thin and undersupplied markets, other policy
considerations can often be more important. Once a market has been assessed as thin or
undersupplied, increasing prices can be a way to attract new suppliers and investment.
However, some structural features cannot be overcome by price alone. This includes when
the suppliers do not have the capacity to cater to some specialised markets, or when the
market has structural features such as geographical isolation which make it difficult for
providers to operate in these areas.
The NDIA should bolster its market evaluation framework to identify thin markets before they
develop, invest in market development infrastructure, and make pricing changes where
necessary.
Section 4.5 covers the following topics:
■ 4.5.1 Process to identify thin and undersupplied markets
■ 4.5.2 Addressing emerging thin and undersupplied markets
Process to identify thin and undersupplied markets
Issues and evidence
The NDIS is too young and the available data too incomplete to make a definitive assessment
of whether certain markets are at risk of being thin or undersupplied. The NDIS has only been
in operation for more than 12 months in a few geographic regions. 79% of supports committed
in the latest financial year were in NSW, ACT and Victoria, with the NDIS yet to be rolled out
in much of Queensland, Tasmania and the western states and territories. NDIS expenditure
on support services in FY 2016/17 was 15% of the projected annual expenditure by 2021. Not
only is the NDIS in its early stage, there are also some limitations to the current data on
market supply. For example, comprehensive surveys of participants and providers are limited
to the trial sites or have only just been initiated in other parts of the Scheme. More discussion
of this evidence is presented in Section 3.1 – Market Development. It is too early to form
definitive assessments about which markets are likely to emerge as thin or undersupplied, as
any evidence of supply gaps may be a product of temporary transitional pressures, or reflect
gaps in data collection.
The NDIA is currently designing a market analysis and intervention strategy to identify thin
and undersupplied markets. It is also developing a strategy to maintain critical supports which
will support its efforts to identify short-term responses to supply gaps. These strategies are yet
to be finalised and implemented. The NDIA does not currently have a framework with clearly
identified metrics and data sources to ensure that its monitoring strategies are more
comprehensive and transparent.

McKinsey & Company 59
Recommendations
11: As part of its market intervention strategy, the NDIA should adopt a clear set of metrics to more comprehensively identify and respond to risks of thin markets emerging.
The NDIA should include a clear set of metrics and data sources within a robust evaluation
framework to test markets for potential undersupply. The IPR team recommended above the
adoption of a clear and robust market evaluation and decision-making process to set
appropriate price levels (see Section 4.1.1). The foundation of this process is a
comprehensive understanding of market indicators to understand whether there is sufficient
supply in each Scheme market. The following section identifies the key metrics that the NDIA
should monitor, the data sources it can rely on, and the teams within the NDIA that should
have responsibility for collection and analysis of these metrics.
The IPR team recognises that no single set of Scheme-wide indicators can offer a definitive
answer on whether supply challenges are likely to occur in each rapidly changing market.
Therefore, the focus of the monitoring framework should be on identifying the markets that
most warrant further investigation. The NDIA should err on the side of caution when identifying
thin markets. Identifying the markets ‘most at risk’, rather than whether they are currently
undersupplied or not, will position the NDIA well to respond to emerging supply challenges.
Participant survey data
The NDIA should have a regularly updated awareness of the share of participants who are
unable to access supports for which they have a budgeted plan, and the share of participants
who are satisfied with the quality of supports to which they have access. This can be
constructed through a participant survey, as well as by accessing informal information flows
from LACs and planners. As NDIS-wide participant surveys may be more difficult to update
continuously, the NDIA can target participant surveys in markets that demonstrate other
indicators of supply shortages.
The NDIA currently conducts a regular participant survey through its Short-form Outcomes
Framework assessment. The NDIA should include in this survey a question as to whether
participants were able to access supports for which they had funding, and if not, if this was
due to a lack of available providers. The NDIA currently reports on the share of participants
who identified having difficulty in accessing health services, but this question is not specific to
either NDIS-supported services or difficulty caused by a lack of adequate supply. The NDIA
should also collate instances of participants contacting their LACs to report an inability to find
providers. The results of these queries should be included by the Provider, Markets and
Sector development team in its regular assessment of markets and reported to senior
management.
Provider intent
Understanding whether providers intend to expand services to a new market, continue in
current markets, or withdraw from the markets in which they provide support services, is a
good leading indicator of the adequacy of supply in the future. The NDIA can monitor this
intent through provider surveys and regular consultation with providers. Where indications
exist of provider exit, more thorough consultation should be conducted to inform the NDIA’s
understanding of provider economics, participant demand, and Scheme performance in that

McKinsey & Company 60
area. This will inform whether the prices in that market should be changed, including through
interim pricing adjustments.
The provider benchmarking initiative currently being developed by the NDIA will give some
indirect indication of provider economics and intent.43 The NDIA also manages relationships
with providers through its regional offices and LAC network. However, standardised and
regular reporting of provider intent should be part of its permanent market monitoring
framework.
Utilisation rate
The utilisation rate is the share of a participant’s budgeted plan that has been used to
purchase services. It is calculated annually and, since services provided in one year may not
be claimed for reimbursement until some months later, updated retrospectively. If a
participant were unable to find providers of sufficient quality to meet their needs as specified
in their plan, it would be reflected in the utilisation rate, and could signpost a lack of
appropriate supply in that market.
Utilisation rates should be used by comparing changes in relative levels to overcome some
of the metric’s shortfalls. Absolute levels of utilisation rates are less informative because they
may be affected by many factors other than supply. The most important of these is the
content of the plans themselves; a utilisation rate might appear high simply because the
plans catered for inadequate supports in the first place. Similarly, plans that provide for more
services than required in a support category may appear underutilised, even though the
participants are accessing all the high-quality support they require. Some plan managers
who were consulted by the IPR team reported that their participants sometimes had spare
allocations for capital equipment in case some of it was damaged and needed to be
replaced. Such items are only intended to be used infrequently and could account for low
utilisation rates in some support markets.
Despite these alternate explanations for any given level of a utilisation rate, observing the
relative rates across markets, and the change in rates over time, will give some indication of
which markets may be experiencing supply shortfalls.
The Scheme Actuary currently collects and shares utilisation data quarterly. The IPR team
proposes the Provider, Markets and Sector development team should identify quarterly
markets in the Scheme with low levels of relative utilisation using more tailored samples of
participant utilisation rates, e.g. support type by geography, or a subset of participant
characteristics within a geography. Markets with utilisation rates that are persistently lower
than other markets can be investigated using surveys and interviews, through working with
LACs, regional offices, participants and providers in that market.
Rates of market entry and exit
Rates of market entry and exit are a basic measure of the willingness of providers to supply
disability support services in the NDIS at existing price levels. A combination of registration
and payment data can help inform this measure. Registration data indicates instances where
firms enter or exit the NDIS, but a provider can register while not actively providing supports
43 National Disability Insurance Agency: Overview of benchmarking project, available at https://www.ndis.gov.au/providers/market-information-useful-links/benchmarking-Project-Overview
McKinsey & Company 61
and stop providing supports without deregistering. Analysis of payment data to identify
provider activity offers the most direct observation of market supply. It is recognised that
provider entry and exit rates will be affected by many commercial (and other) factors that are
not a result of just the price level. However, significant variations in provider entry or exit rates
in some markets should serve as a trigger for further investigation.
The Scheme Actuary currently collects and reports payment data which shows rolling
averages of provider entry and exit. This should be reviewed monthly by the Provider, Market
and Sector development team, who should work with the Scheme Actuary to identify the
markets by support type or geography which are experiencing the highest net declines in
provider activity. This should be a trigger for further investigation in the relevant markets.
Addressing emerging thin and undersupplied markets
Issues and evidence
Provider submissions to the IPR during the consultation process for this review identified
some markets as being at risk of undersupply due to the additional expense and difficulty in
catering to them. These included markets for participants in remote regions and those with
complex needs. These markets were also identified by the Productivity Commission as
potential thin or undersupplied markets.44
Remote and very remote areas account for 3-5% of the current committed supports in the
Scheme. Provider consultation and market data suggest a risk of undersupply in these
markets. The non-financial obstacles to providing services in remote and very remote areas,
include insufficient information about the participants in that region, limited Scheme
infrastructure such as LACs, and the lack of a local workforce. Providers also revealed
difficulties in travel to and from these areas which made service provision unsustainable (see
Section 4.2.1).
Participants with very complex needs are defined here to include those that most require
assistance from a support worker with additional skills and experience due to a medical need
or challenging behaviour (see Section 4.3 for further detail). Based on the current application
of ‘high intensity’ loadings, this cohort is estimated to comprise approximately 4% of
participants enrolled in the Scheme but 13% of expenditure in the latest financial year.45
Service provision to these participants is highly specialised and the participant density is low,
creating a risk of undersupply that should be monitored and addressed (see Section 4.3.3).
Across all markets, as the Scheme transitions, the current assessment of market supply will
change. Participants will change their demand patterns, new suppliers will come online while
others leave, and Scheme infrastructure will be developed that helps participants and
providers find each other – through LACs, and events at which providers can present their
44 Productivity Commission: National Disability Insurance Scheme (NDIS) Costs (19 October 2017) , pp. 268 –
270. 45 Share of participants who have been assessed as Level 13 – 15 according to the Disability Severity Indicator. It
should be noted that this current definition of complexity does not adequately capture all participants with complex needs (see Section 4.3.1).

McKinsey & Company 62
services, for example. These changes can continually affect the adequacy of supply in the
market and must be proactively monitored by the NDIA.
Recommendations
The supply challenges faced by the markets identified above can be addressed in part
through changes to pricing and related policies. These changes are briefly outlined below, and
discussed in more detail in the relevant other sections of this report:
■ In very remote areas, including isolated Indigenous communities, the NDIA can work with
providers to develop local workforces, and allow providers to quote on services to ensure
supply in the short term (see Section 4.2.1).
■ In rural areas, the NDIA can amend travel policies to enable providers to recoup costs
associated with delivering services to participants in these areas (see Section 4.2.2).
■ For participants with complex needs, the NDIA should more clearly define these
participants, and adopt a more appropriate tiered pricing structure to reflect the costs
of providing services for these participants (see Section 4.3).
In some cases, thin and undersupplied markets will require immediate intervention to ensure
the provision of critical supports. For example, participants with daily care needs may require
assistance in locating providers if a major provider in an already thin market were to withdraw.
The NDIA is undertaking an initiative to ensure access to critical supports at any time, and
facilitating a provider of last resort solution to address this scenario. In these circumstances, a
price solution alone may not address the short-term requirements of participants, and LACs
will likely play a significant role to help participants find suitable providers.
12: The NDIA should invest in Scheme infrastructure such as an e-market tool, which would empower participants in thin or undersupplied markets to find suitable providers.
One of the priorities for the NDIA as the NDIS has developed has been ensuring participants
can connect with providers. To assist in this, the NDIA is establishing a ‘Provider Finder’,
which enables a participant to search by postcode for a provider in his or her area. This is a
useful tool for identifying providers, but does not yet let participants compare prices or transact
directly through the platform. As the market grows, an e-market tool with this functionality will
empower participants and increase price transparency and competition amongst providers. In
addition to helping the NDIA address thin and undersupplied markets, easier identification of
services and prices could support a faster transition towards deregulated prices (see
Section 4.7).
An e-market would enable a participant to search by support type or features of the provider,
such as location, price-range, or quality rating, and could also allow participants and providers
to book support services on the platform. The e-market will not be a suitable solution for all
providers and participants, for example where there are difficulties in accessing the internet
or navigating an online portal. As such, the NDIA through its regional offices and LAC network
should also continue experimenting with other forms of Scheme infrastructure, such as
physical market fairs where participants can come to one place to meet providers and
compare offerings.

McKinsey & Company 63
In addition to its own activities, the NDIA can speed up the process of delivering an e-market
by allowing private firms to develop and compete on online marketplace platforms. There are
firms that are already providing similar products, but some are not registered in the NDIS,
meaning Agency-managed participants cannot access supports on these platforms. The NDIA
should explore options to incentivise private providers to build e-market tools.
4.6 PROVIDER EFFICIENCIES AND ADEQUACY OF PROVIDER RETURNS
Section 3 of this report included analysis on provider economics and benchmarking with other
schemes. The IPR team found that across all support types there were examples of providers
operating profitably, as well as examples of providers struggling (see Exhibit 3). The
successful models provide inspiration for how the market can innovate and drive efficiencies,
while providing high quality services to participants that meet their needs. However, some
providers, particularly those providing attendant care services, are struggling to make the
transition to the NDIS.
The IPR team has focused on the adequacy of provider returns for attendant care and
therapy. Attendant care was chosen given the large proportion of Scheme spend it represents,
and given the recent scrutiny on the price cap for 1:1 attendant care. Therapy supports was
chosen because the single NDIS price cap for therapy appeared to be inconsistent with the
multiple price levels, and structure, of other comparable schemes.
Section 4.6 covers the following topics:
■ 4.6.1 Costs of transitioning to the NDIS that impact provider returns
■ 4.6.2 Administrative costs related to operating within the NDIS
■ 4.6.3 Attendant care adequacy of provider returns and efficiencies
■ 4.6.4 Therapy adequacy of provider returns and efficiencies
The cost of transitioning to the NDIS
Section 4.6.1 provides context for all of Section 4.6 by outlining the transitional costs and
organisational challenges providers across all supports face as they move to a unit-funded,
consumer-driven environment under the NDIS. It also provides an overview of federal and
state and territory government spending to date to support NDIS transition, specifically as it
relates to supporting provider readiness.
4.6.1.1 Changes providers must adapt to under the NDIS
Transitioning to the NDIS requires existing providers to develop new organisational
capabilities and make significant changes and innovations to their systems and process.
This requires significant investment by providers. This was recognised by DSS in a 2015
document.
‘A substantial proportion of existing service providers are unlikely to operate effectively in the
new environment without significant transformation…Providers long accustomed to block
funding will require support to transition to business models responsive to individualised

McKinsey & Company 64
funding, and to diversify their service offerings to meet the support requirements of NDIS
participants’.
Sector Development Fund Strategy and Operational and Guidelines, Department of Social Services,
December 2015
Anecdotal evidence from provider consultations indicated that the cost of transition could
amount to 1.5% of total annual expenditure for a provider.46 The four biggest transitional
changes to which providers must adapt are: a shift from block funding to unit funding;
adapting to a consumer-driven service environment; a shift from payment in advance to
payment in arrears; and compliance with a new quality and safeguards framework. Many
providers have invested in IT, organisational capability, and organisational restructures.
Shift from block funding to unit funding
The shift from receiving and reporting against block funding every quarter, to claiming and
reporting against individual units of service, has created challenges for providers.
First, many providers are struggling to manage the additional administrative burden of unit-
funding. Anecdotal evidence from consultation suggests many providers have hired new
corporate staff to manage payments and invoicing, increasing corporate overhead costs.
Second, providers have had to invest to understand whether they can deliver services under
NDIS pricing. The unit costing regime requires providers to accurately measure each
component of their service delivery, including on-costs and corporate overheads. Anecdotal
evidence suggests many providers of disability support services did not understand their unit
cost to serve prior to the NDIS. Nor did they possess data or organisational capability to
measure unit costs, and therefore did not understand whether they could deliver services
profitably within NDIS price caps. Not understanding whether they could deliver services
within the price caps, or whether they had the short-term financial resilience to cope with
transition, was a significant source of stress for many organisations. Many larger
organisations hired external consultants to help them understand their unit costs to serve,
while the federal government and state governments have also funded programs to help
develop this capability in the sector.
Adapting to a consumer-driven service environment
In a new consumer-driven, competitive service delivery environment, providers must develop
marketing capabilities to attract and retain customers. There is broad recognition amongst
providers that this capability is underdeveloped in this sector, and many providers are
investing significantly in their direct-to-customer marketing capabilities:
■ One industry expert states: ‘There is a low level of sophistication in understanding the
marketing funnel and the sequence of events through the activities of reaching,
engaging, converting and servicing customers’.
■ In transitioning to the NDIS, one provider invested in 10 full-time equivalent (FTE) staff to
perform sales and relationship management functions at a cost of $750 000 per year,
46 Based on data from 3 large providers with revenue of over 50 million in FY16/17. Included spending on IT, new business teams and NDIS transition teams.

McKinsey & Company 65
and incurred marketing and other new costs of $250 000. This represents an increase of
over 1% to their total annual expenditure.
The empowerment of participants to choose not only their supports and providers, but also to
have a greater say in when these are received, has also been challenging for providers. There
is greater pressure to ensure that service times meet the needs of the participant, rather than
the rostering requirements of the provider. This means providers are required to manage more
peaks and troughs in demand between days of the week and hours of the day, making it more
difficult to plan consecutive client bookings. Some providers have introduced a new human
resources role to manage these new challenges, while others have invested in workforce
rostering systems. Many providers have moved towards more casualised workforces to
manage this challenge.
Shift from payment in advance to payment in arrears
Prior to the introduction of the NDIS, most disability organisations were paid by state and
territory governments in advance on a quarterly basis. The switch from payments in advance
to payments in arrears has represented a short-term cash flow challenge for providers, who
now need to fund salaries and other expenses for a period in transition before they receive
payments.
Compliance with a new quality and safeguarding framework
The NDIS Quality and Safeguarding Framework, released by the Council of Australian
Governments Disability Reform Council in February 2017, introduces a nationally consistent
system for regulating the safety and quality of disability services in Australia.47
The new framework will, among other things, introduce a new risk-based provider
registration system. Registered providers whose registration group is deemed to be lower
risk will only undergo a simple, periodic verification process while providers delivering higher-
risk supports will be required to gain third party quality assurance certification.48 In addition,
all providers and workers will be required to comply with a new code of conduct, registered
providers and their employees will be required to undertake a mandatory compulsory
orientation module, and registered providers will be required to have effective internal
complaints arrangements.49
In the short term, the new framework represents an added compliance cost for providers,
who will have to adapt internal systems and processes to comply with these new standards.
In the longer term, the framework may represent a cost efficiency for national providers –
who will only need to comply with one set of standards, as opposed to one in each
jurisdiction.
47Department of Social Services: NDIS Quality and Safeguarding framework, factsheet for providers, available at
https://www.dss.gov.au/sites/default/files/documents/04_2017/ndis_quality_and_safeguarding_framework_fact_sheet_for_providers_final_2.pdf
48 Department of Social Services: NDIS Quality and Safeguarding framework, factsheet for providers, available at https://www.dss.gov.au/sites/default/files/documents/04_2017/ndis_quality_and_safeguarding_framework_fact_sheet_for_providers_final_2.pdf
49 Department of Social Services: NDIS Quality and Safeguarding framework, factsheet for providers, available at https://www.dss.gov.au/sites/default/files/documents/04_2017/ndis_quality_and_safeguarding_framework_fact_sheet_for_providers_final_2.pdf

McKinsey & Company 66
4.6.1.2 Federal and state and territory government funding for provider
readiness to date
To date, federal and state and territory governments have committed significant funds to
support the NDIS transition. At the federal level, the Sector Development Fund (SDF), a pool
of $146 million administered by DSS from 2012/13-2017/18,50 has funded provider readiness
projects under the primary outcome area of ‘building disability sector capacity and service
provider readiness’.51 At the state and territory level governments have also invested
significantly in the transition, often over and above the money they have received via SDF
funding. For instance, the NSW Government spent over $30 million between 2009-2016 on
NDIS sector development and capacity building.52
Of the money dedicated to provider readiness, some has been used to fund publicly
accessible education tools that give providers practical business advice to assist the transition
to the NDIS world, and some has been used to provide direct individualised provider support,
financial and non-financial. It is unclear how much of this funding has been provided as
funding to support provider education, versus direct financial assistance to providers.
Examples of provider readiness initiatives funded by federal and state and territory
governments include:
■ Education tools for all providers: The SDF funded a ‘Unit Costing Tool Project’ in New
South Wales, which developed a suite of resources to help providers develop the
capability to operating in a unit-funded NDIS world.53
■ Direct individualised non-financial assistance: The SDF funded contractors to give
providers in South Australia one-on-one support in helping them transform their business
models, including assistance with financial and costing analysis, bookkeeping, IT and
data management integration, and marketing and communication.54
■ Direct individualised financial assistance: The NSW Government’s Round 1
Transition Assistance Program (TAP), launched in 2016, provided over $ 4 million in
financial assistance to small and medium providers regional areas. Providers with less
than $3 million in annual turnover were offered up to $35,000 to help with readiness
activities like updating business plans or purchasing software.55 In TAP Round 2,
50 The Fund was administered by the NDIA between 2013-2014. 51 This is one of five outcome areas funded by the SDF. It is unclear at the time of writing this report, how much of
the $146 million to date has been committed to this outcome area. The SDF is now closed for new applications. 52 Audit Office of New South Wales: New South Wales Auditor-General’s Report Performance Audit: Building the
readiness of non-government sector for the NDIS (February 2017), available at http://www.audit.nsw.gov.au/news/building-the-readiness-of-the-non-government-sector-for-the-ndis
53 National Disability Insurance Agency: State and Territory Government SDF activities, available at https://www.ndis.gov.au/sdf_state_territory.html
54 National Disability Insurance Agency: State and Territory Government SDF activities, available at https://www.ndis.gov.au/sdf_state_territory.html
55 NSW Government Department of Family and Community Services: Funding boost to help regional NSW to get NDIS-ready (19 July 2016), available at https://www.facs.nsw.gov.au/about_us/media_releases/media_release_archive/funding-boost-to-help-regional-nsw-get-ndis-ready

McKinsey & Company 67
launched in 2017, the NSW Government awarded a further $600,000 in grants to
providers.56
The effectiveness of this spending is not yet clearly established. Two audits have noted that
these interventions have not been systematically evaluated. 57 Therefore, there is an
opportunity for federal and state and territory governments to review the effectiveness of
spending on provider readiness to date where possible, to evaluate the effectiveness of future
interventions, and to assess whether any further support for provider readiness is required.
Costs of interacting with the NDIA
Issues and evidence
In addition to the expected costs associated with transition to the NDIS, consultation with
providers revealed opportunities for the NDIA to improve its systems and processes, and
reduce the administrative costs and cash flow risk of providers. Sections 2.2 and 2.4
summarised the provider feedback relating to the portal, NDIA responsiveness and planning
raised in consultation, while Section 3.2 quantified the potential impact of these issues on
provider financials based on a small sample of provider submissions. This sample indicated
that the Agency could reduce provider costs by ~0.5% of total annual expenditure through
improvements to its systems and processes.58
This section highlights a measures the NDIA should prioritise to address key provider
feedback relating to NDIA systems and processes raised in consultation. The focus of the IPR
is pricing and these recommendations are made in the context of the relative emphasis placed
on these issues in consultation, and through an assessment of relative impact of these issues
on provider economics.
The IPR team has been advised by the NDIA that there are multiple initiatives currently
underway as part of the Participant and Provider Pathway Reviews that go to addressing the
issues outlined in Sections 2.2 and 2.4, or to implementing some of the recommendations
below.
56 Consultation with the NSW Government Department of Family and Community Services. 57 The Australian National Audit Office’s audit of the Management of Transition of the Disability Services Market
(November 2016) found ‘limited evidence of evaluation of some higher cost projects’ funded by the SDF. Australian National Audit Office: National Disability Insurance Scheme – Management of Transition of the Disability Services Market (November 2016), available at https://www.anao.gov.au/work/performance-audit/national-disability-insurance-scheme-transition-disability-services. The NSW Audit Office’s performance audit on ‘Building the readiness of the non-government sector for the NDIS’ (February 2017) found the overall
impact of the NSW Department of Family and Community Services spending on provider capability was not clear, as baseline information on provider capability was not collected and targets for improvement in provider capability were not set. Audit Office of New South Wales: New South Wales Auditor-General’s Report Performance Audit: Building the readiness of non-government sector for the NDIS (February 2017), available at
http://www.audit.nsw.gov.au/news/building-the-readiness-of-the-non-government-sector-for-the-ndis 58 Based on 45 one-on-one interviews with providers in September 2017, in which three large providers (revenue
> 50 million in FY16/17) gave detailed evidence of these costs.
McKinsey & Company 68
Recommendations
13: The NDIA should prioritise the implementation of measures to continue to improve its portal, responsiveness and communication as part of the Participant and Provider Pathway Reviews.
Portal
■ Allow for automatic notification of plan review commencement, if participant
consent is provided: The NDIA has advised the IPR team that as of December 2017,
changes to the portal will allow providers to view relevant sections of a participant’s plan,
including plan start and end dates, given the participant has a current service booking
with the provider and the participant has provided their consent. The IPR team
recommends the Agency also consider allowing providers to receive an automatic
notification through the portal that a plan review has been triggered, given the participant
has a current service booking with the provider and the participant has provided their
consent.
■ Provide more detailed descriptions of claim rejection reasons: The NDIA should
consider providing a more detailed description of the cause of payment rejection in the
portal.
■ Improve provider education tools: The NDIA should continue simplifying and
improving tools (like the provider toolkit) that educate providers how to navigate and
troubleshoot portal issues. In the medium term, the NDIA should consider setting up a
dummy portal that peak bodies and the NDIA can use to train providers on how to use
the portal. This recommendation should be considered after changes in the provider
pathway project have been implemented, and the new portal has been standardised.
■ Consult with providers when designing portal improvements: The NDIA should
consider making future improvements to the portal by consulting with a representative
group of providers. The NDIA advised the IPR that this is already underway.
Agency responsiveness and communications
■ Stream call centre inquiries: The NDIA should upskill call centre staff and stream call
centre inquiries to specialist teams, to ensure that most provider inquiries are resolved by
staff with the knowledge and the authority to resolve the issue. The IPR has been
advised by the NDIA that there are current initiatives underway to address these issues.
■ Improve response times for SIL quote approvals: The NDIA should aim to further
reduce the average time it takes to process a SIL quote, building on its success to date
in reducing the time required. The NDIA’s current target is 14 days.
■ Improve communication of policy and process changes: The NDIA should build on
recent improvements such as the provider toolkit to clearly communicate all planned
policy and process changes to providers, as far ahead of time as possible, and
preferably through a single touchpoint. The IPR has been advised that the NDIA is aware
of these issues and has recently implemented initiatives to address them e.g. the
provider e-newsletter has been recently revised to include more ‘need to know’
information that is valued by providers.

McKinsey & Company 69
Planning
The IPR team will not make any recommendations relating to the planning process as this is
outside of the IPR’s TOR. Moreover, the NDIA has advised the IPR team that most of the
planning issues raised in Section 2.4 are being considered and addressed as part of the
Participant and Provider Review projects.
Attendant care supports
Attendant care refers to ‘Assistance with daily living’ and ‘Assistance with social and
community participation’. ‘Assistance with daily living’ involves assisting with, and/or
supervising personal tasks of daily life to develop the skills of the participant to live as
independently as possible. ‘Assistance with social and community participation’ involves the
provision of support to enable a participant to independently engage in community, social and
recreational activities. Together these supports account for 45% of committed scheme spend
at full Scheme. Attendant care can be provided by one carer to one participant (one to one) as
well as by one carer to more than one participant in the case of ‘Assistance with social and
community participation’ (group care).
Pricing for ‘Supported Independent Living’ (SIL) is derived from the price cap for attendant
care. If SIL is included together with all other supports involving attendant care, together they
are estimated to account for 75% of committed scheme spend at full scheme.59
This section covers the following topics:
■ 4.6.3.1 Base price for one to one attendant care
■ 4.6.3.2 Cancellation policy for attendant care
■ 4.6.3.3 Group price for attendant care
4.6.3.1 Base price for one to one attendant care
Issues and evidence
Attendant care supports are currently subject to price caps. There are different price limits for
the provision of these supports:
■ At different times of day i.e. daytime, evening
■ At different days of the week i.e. weekdays, Saturdays, Sundays and public holidays
■ By the complexity of the care required i.e. standard and higher intensity
■ By the location of the service i.e. metropolitan, remote or very remote.
The base price of one to one (1:1) attendant care (daytime, weekday, standard intensity,
metropolitan location) is subject to a price limit set by the NDIA of $44.72 in the 2017/18 Price
Guide for Victoria, New South Wales, Queensland and Tasmania, and $45.54 in the
59 Source: NDIA Scheme Actuary.

McKinsey & Company 70
Australian Capital Territory, Northern Territory, South Australia and Western Australia. The
NDIA also sets service definitions, payment rules and terms of business that affect the cost of
service delivery for this support.
The price of 1:1 attendant care has come under recent scrutiny.
■ The price of 1:1 attendant care was the focus of the NDIA's FY2017/18 Price Review.
The NDIA published a discussion paper ‘2017 Price Controls Review’ in March 2017 and
invited providers to give feedback on questions related to the price setting process and
the adequacy of pricing for attendant care.
– The NDIA found that ‘divergent facts and views were presented’ with some providers
submitting that ‘existing prices did not allow for recovery of costs’, and some
participants submitting that ‘providers were overpricing supports in some
categories’.60
– In June 2017, the NDIA increased the base price of attendant care by 4.5% to $44.72,
reflecting the increase in the national minimum wage, the Equal Remuneration Order
and the impact of inflation.61
■ More broadly, the NDIA’s view on the pricing of attendant care is reflected in its March
2017 submission to the Productivity Commission Costs Paper, which states that
‘Contradictory views in the provider population might be evidence that some are
struggling to adjust to a funding model that is based on market principles. There is also
evidence of a wide variety in operating costs under pre-NDIS approaches where
efficiency was not a key consideration’.62
■ The Productivity Commission in its NDIS Costs Paper (October 2017) noted, based on
anecdotal evidence from provider submissions, that attendant care price caps may be
too low to achieve safe and quality outcomes, with estimates of the shortfall as a
percentage of the current price cap varying considerably.63
One objective of the NDIS is to develop an efficient market of providers while providing safe
and high quality supports for participants.
In assessing the price of 1:1 standard intensity attendant care, the IPR team examined
evidence of supply shortages, benchmarked NDIA price caps against comparable schemes,
and consulted with providers about their unit cost to serve. Detailed findings relating to these
60 National Disability Insurance Agency: Letter from David Bowen to providers outlining the outcome of the FY17-18 Review (12 June 2017), available at https://www.ndis.gov.au/news/letter-to-ndia-registered-providers.html
61 The 4.5% increase was based on the rise in the national minimum wage (3.3% from 1 July 2017) and the application of the Equal Remuneration Order (1.7% in some disability roles from 31 December 2016) for labour costs, and inflation (2.1% for the 12 months to 31 March 2017) for non-labour costs. Labour costs and non-labour costs were assumed to constitute 80% and 20% of the cost base for attendant care respectively. National Disability Insurance Agency: Letter from David Bowen to providers outlining the outcome of the FY17-18 Review (12 June 2017), available at https://www.ndis.gov.au/news/letter-to-ndia-registered-providers.html
62 National Disability Insurance Agency: NDIA Submission to Productivity Commission Issues Paper on NDIS Costs (March 2017), p. 101, available at https://www.pc.gov.au/__data/assets/pdf_file/0013/216031/sub0161-ndis-costs.pdf
63 Productivity Commission: National Disability Insurance Scheme (NDIS) Costs (October 2017), p. 300, available at https://www.pc.gov.au/inquiries/completed/ndis-costs/report/ndis-costs.pdf

McKinsey & Company 71
are presented in Section 3. The IPR team recognises the limitations of each of these
evidence sources.
The IPR team found no conclusive evidence of general supply shortages in the standard
intensity attendant care market, with the NDIS price caps for attendant care being
comparable to similar government funded schemes. The IPR team also found that some
providers with different operating models currently deliver attendant care at a profit, but
many providers in the market are struggling to make an adequate return. Based on a sample
set of 22 providers who shared detailed operating cost breakdowns with the IPR team, the
median cost to serve was ~$49 per hour, or ~10% higher than the current price cap (see
Exhibit 4), with some providers stating they are cross-subsiding the loss on this support from
other NDIS or non-NDIS funding sources, including state and territory government block
funding.64
Many providers with profitable operating models in attendant care have recently started their
business and specifically designed it to work for the NDIS, or are for-profit organisations,
while many providers who are finding it difficult to deliver services under NDIS unit prices are
incumbents or more traditional providers.
While there is no single model of care that will work for all providers and participants, and
acknowledging the substantial investment providers have already made in transforming their
organisations, the significant variation in cost to serve across the market indicates there are
opportunities to innovate and lessons to be learned from operating models that are working
well in standard intensity attendant care. Providers will generally need to achieve corporate
overheads of 10-15% and improve workforce utilisation rates to above 90% to make a profit
while complying with SCHADS award obligations. To do this, most existing providers will be
required to adjust their operating models, driving efficiencies and innovation through
technology and other operational improvements.
While this transformation will be challenging, examples of providers who are delivering quality
supports at a profit suggest that it is achievable. Appendix E provides examples of strategies
employed by some providers that have operating models that work under current prices. The
NDIA’s recently announced independent provider benchmarking function will also be a key
reference point for providers as they make this transformation. In its first phase, this provider
benchmarking project, run by an independent third-party survey manager, will survey
providers for detailed information about their input costs for delivering attendant care, as well
as for provider (e.g. provider scale, workforce mix, industrial agreements) and client
characteristics (e.g. client complexity, location). The customised reports produced for
participating providers will benchmark providers’ input costs against similar providers in the
sector. This will be an important piece of strategic information in helping providers understand
how they are performing relative to their peers, potential drivers in variations in their input
costs, and in identifying where there are specific opportunities to for improvement.
The IPR team also recognises that provider adjustment will take time: 88% of in-home care
service volume under the NDIS is delivered by medium and large providers (see Exhibit 8)
64 Data based on information from 22 providers who provided detailed financial information to the IPR. While the IPR’s sample of 22 providers was not comprehensive or representative of the market, the IPR was limited by the information providers were able to provide.
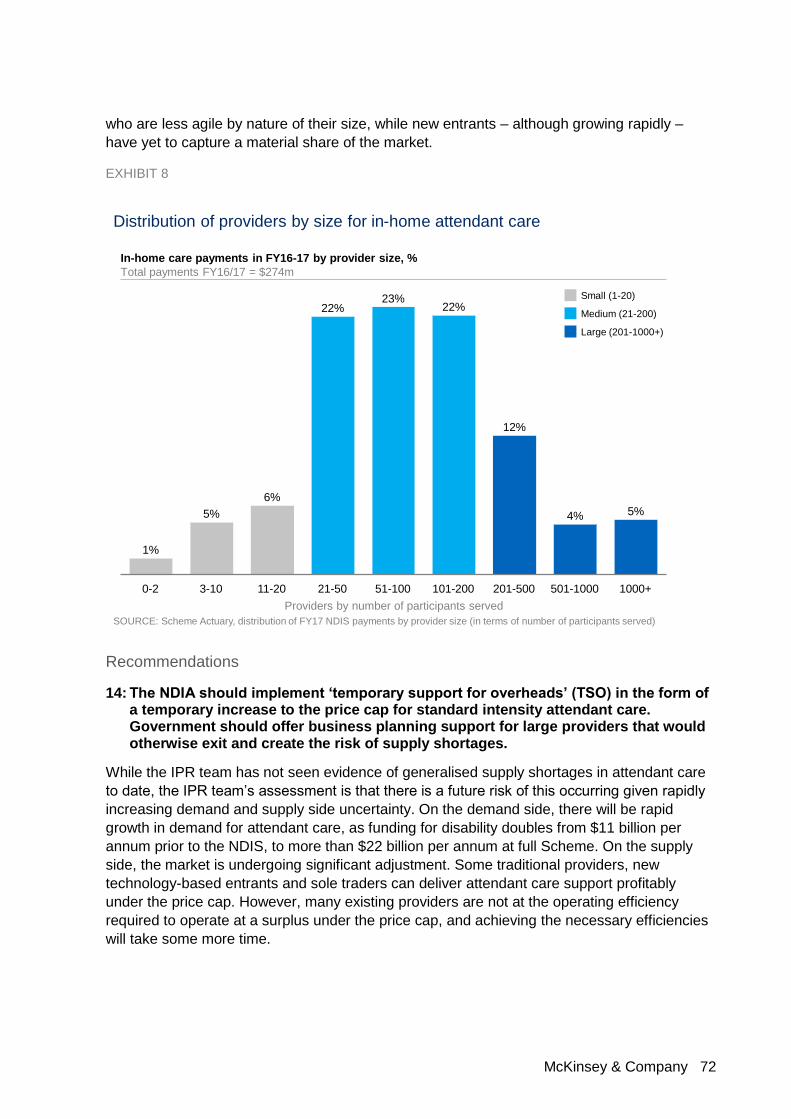
McKinsey & Company 72
who are less agile by nature of their size, while new entrants – although growing rapidly –
have yet to capture a material share of the market.
EXHIBIT 8
Recommendations
14: The NDIA should implement ‘temporary support for overheads’ (TSO) in the form of a temporary increase to the price cap for standard intensity attendant care. Government should offer business planning support for large providers that would otherwise exit and create the risk of supply shortages.
While the IPR team has not seen evidence of generalised supply shortages in attendant care
to date, the IPR team’s assessment is that there is a future risk of this occurring given rapidly
increasing demand and supply side uncertainty. On the demand side, there will be rapid
growth in demand for attendant care, as funding for disability doubles from $11 billion per
annum prior to the NDIS, to more than $22 billion per annum at full Scheme. On the supply
side, the market is undergoing significant adjustment. Some traditional providers, new
technology-based entrants and sole traders can deliver attendant care support profitably
under the price cap. However, many existing providers are not at the operating efficiency
required to operate at a surplus under the price cap, and achieving the necessary efficiencies
will take some more time.
101-20051-10021-50
22%
201-500 501-1000 1000+
5%
12%
23%
4%
22%
5%
3-10
6%
1%
11-200-2
Small (1-20)
Medium (21-200)
Large (201-1000+)
SOURCE: Scheme Actuary, distribution of FY17 NDIS payments by provider size (in terms of number of participants served)
Distribution of providers by size for in-home attendant care
In-home care payments in FY16-17 by provider size, %
Total payments FY16/17 = $274m
Providers by number of participants served

McKinsey & Company 73
The IPR team also notes the evidentiary difficulty of detecting how quickly the market is
adjusting in a timely way, as articulated in Section 3.1. Critically, there is not one or a set of
leading indicators that currently conclusively predict future generalised supply shortages.
In this uncertain context, and given the essential daily support that attendant care provides
participants, the IPR team believes it is prudent to act cautiously and pre-emptively using a
combination of price and non-price instruments to mitigate the risk of market failure.
The IPR team recommends the NDIA implement ‘temporary support for overheads’ (TSO) in
the form of an increase of 2-3% in the price cap of 1:1 attendant care for 12 months. The TSO
should apply in addition to ordinary annual indexation of the price. The presumption should be
that the TSO is a one-off measure and will not be extended. The IPR believes that 12 months
is a reasonable time frame for providers to implement changes to operating models to reduce
overhead costs, and for the NDIA to assist and encourage the development of efficient and
effective alternative supply options, such as e-marketplaces. At the end of the 12 months, the
loading would be removed by reducing the annual indexation of the price by the TSO amount
of 2-3%.
Before the end of this 12 months, there should be a review that examines the progress
providers have made in transforming their business models and the ongoing risk of supply
shortages. The expectation should be that providers have improved their performance
sufficiently that they no longer require the TSO. Government should also consider using non-
price instruments such as business planning support for providers to address the risk of
supply shortages in attendant care, if further funding becomes available for this purpose.
In developing this recommendation, the IPR considered several alternatives including funding
providers for specific activities (e.g. training, IT investments) and by-application support for
providers. Given there is no legislative mechanism for NDIA to fund providers directly, and
that a policy that advantaged one provider over another was unfavourable, the TSO was
selected as the most appropriate option.
The specific quantum of the TSO increase should be a policy decision the NDIA makes in
view of other more targeted interventions government will undertake to mitigate the risk of
supply shortages. Based on current information, a 2-3% TSO adjustment reflects what the IPR
team believes are reasonable assumptions for providers to achieve in the short term. While no
one model of care will work for the entire market, if a 3% TSO is applied, providers will be able
to achieve a ~5 % margin under the price cap if they can meet the following benchmarks:65
■ Labour costs (including supervisors): SCHADs 2.3 support worker; 1:15 span of
control, SCHADs 3.2 supervisor
■ Workforce mix: 80% full-time or part-time workforce, 20% casual workforce
65 Assumes the midpoint where an assumption range was provided. Analysis assumes labour costs in NSW as of November 2017, and the $44.72 price cap for attendant care in the Victoria, New South Wales, Queensland and Tasmania. The IPR recognises that on 1 December 2017 pay rates under the SCAHDS award were adjusted to reflect an increase from the Equal Remuneration Order (ERO). This will compress provider margins by ~2% for 6 months, until the Agency’s July 2018 price increase, which should adjust the new price to reflect the 1 December 2017 ERO increase.

McKinsey & Company 74
■ Workforce utilisation: 90-95% utilisation of full-time and part-time workforce, 100%
utilisation of casual workforce
■ Corporate overheads: 10-15% corporate overheads as a % direct of labour costs.
These benchmarks should be achievable, as some providers are demonstrating they are able
to operate more efficiently than these benchmarks, as described in Section 3.2. Some of
these providers have already reduced corporate overheads to 10% and below. Improvements
in utilisation above 90% should be realised as providers improve their rostering and adjust
their workforce mix; and, labour costs can be reduced by creating different workforce pools for
standard and high intensity participants. While achieving these efficiencies will be challenging
for some providers, existing providers demonstrate they are attainable.
The IPR team recommends that the government fund business planning services for large
providers who deliver high volumes of service in attendant care that are at risk of ceasing
service provision, but who have the willingness to develop and implement an action plan to
deliver attendant care profitably in the future. This focus on providers who deliver high
volumes of service reflects the fact that the exit of these providers would increase the risk of
supply shortages.
The TSO adjustment should not be made available to SIL. The high volume and certainty of
demand for SIL allows providers to manage their business and workforce planning more
effectively, and reduces the need for SIL providers to undergo large scale business model
changes to adapt to the NDIS.
Implications
The quantum and the timing of the TSO balances the need to ensure the market has sufficient
support to adjust, with the aspiration to achieve an efficient, high quality market of providers.
The TSO will relieve some pressure on providers as they transform their operating models,
while any targeted planning support will help protect against identified supply risks.
Implementing the TSO in conjunction with other recommendations relating to attendant care
will improve the margins of providers, recognising that the TSO willonly last for 12 months.
The other recommendations that will improve margins both in the short and long term, are the
addition of a very high intensity rate for the most complex participants, adjustments to travel
and cancellation policies, and the NDIA’s ongoing work to improve the design of its systems
and processes. The aggregate effect of these recommendations is that providers who were
previously making a small loss on attendant care will now be able to provide the service at a
profit while they adjust and improve their business models.
4.6.3.2 Cancellation policy for attendant care
Issues and evidence
Under the Price Guide, a provider can charge a maximum of 8 booking cancellations a year
against a participant’s plan for assistance with self-care activities and assistance to access
community, social and recreational activities. A provider can only charge a booking
cancellation if there are unforeseen circumstances, and the participant agrees that they (the
participant), did not comply with the agreed requirements in the service agreement. The

McKinsey & Company 75
NDIA’s Price Guide does not distinguish between cancellations made far in advance and
those made at short notice. The Price Guide also stipulates that providers are expected to
have business arrangements in place to minimise the risk of participant cancellations, no
shows or late changes.
Providers submitted that this policy does not reflect the frequency at which cancellations occur
in this sector, particularly for medically or behaviourally complex participants. They submitted
that where more than 8 cancellations occur per participant, this policy can be loss-incurring
given providers’ obligation under the SCHADS award to pay full-time and part-time employees
as if they had worked a cancelled shift, if notification is not provided prior to 5pm the day
before the scheduled service.
Recommendations
15: The cancellation policy for attendant care should be amended so that up to a certain threshold, providers can charge against a participant’s plan for up to 90% of the entire duration of the scheduled service if the participant makes a short notice cancellation. Above this threshold, providers will need to demonstrate they are actively working with participants to minimise the risk of cancellations in order to continue charging for cancellations.
The Price Guide should distinguish between short-notice cancellations and other
cancellations.
For short-notice cancellations, the cancellation policy for attendant care should be amended
so that providers can charge against a participant’s plan for up to 90% of the entire duration
of the scheduled service.66 A short-notice cancellation should be defined as occurring where
the participant provides notice of cancellation after 3pm on the day before the scheduled
service. This amended policy is designed to bring the NDIA’s cancellation policy in line with
providers’ obligations under the SCHADS award. The 3pm cut-off time recognises that
providers need time to redeploy a support worker or to give them notice of a cancelled shift
before 5pm on the day before the scheduled service, as required under the SCHADS award
for a full-time or part-time employee. Limiting providers to charging 90% provides an
incentive to redeploy the worker if possible to recover overheads. It also provides an
incentive for the provider to work with participants to reduce the volume of cancellations to
the extent possible. If the worker can be redeployed by the provider, the provider should not
charge the cancelling participant.
For other cancellations, where the participant has provided notice of cancellation prior to
3pm the day before the scheduled service, no cancellation fee should be able to be charged
against a participant’s plan. This is because providers are not obligated under the SCHADS
award to pay full-time and part-time employees for a cancelled shift if notification is provided
prior to 5pm the day before the scheduled service.
Additionally, the NDIA should introduce a new core support line item in the Price Guide for
short-notice cancellations. This will allow the NDIA to monitor the volume of short-notice
cancellations for two purposes. The first purpose is to provide better information on which
participant cohorts have a defensible and higher risk of cancellations from their condition, for
66 The terms of each provider’s cancellation policy should be clearly laid out in the service agreement between the provider and the participant.

McKinsey & Company 76
example a high risk of hospitalisation. The Scheme Actuary already factors in a level of
cancellations into plan packages, but a line item would provide better information and may
allow for a reduction in planned cancellations for certain cohorts of participants. The second
purpose is that data on cancellations will allow the NDIA to detect anomalies in the volume
of cancellations, and work with providers and participants to reduce the level of cancellations
as appropriate.
The NDIA should also introduce a policy that above a specific threshold, providers will not be
able to charge for short-notice cancellations unless they submit a report to the NDIA
outlining the circumstances of each above-threshold cancellation, and actions taken to work
with participants to minimise the risk of their short-notice cancellations. This threshold could
be defined by the number of short-notice cancellations per participant per provider, or the
percentage of short notice cancellations per participant per provider. The NDIA should
consult with experienced practitioners in the disability sector to determine what a reasonable
threshold should be.
Implications
This revised policy minimises the financial loss incurred by providers on short-notice
cancellations and recognises that while providers should work with participants to minimise
short notice cancellations, providers should also not bear financial risk for these incidents.
It also incentivises positive behaviour by all actors in the market: participants are incentivised
to give sufficient notice, while providers are incentivised to work with participants and
implement processes to minimise risk of cancellations.
It is not expected that this change in policy will have an adverse impact on participant
outcomes or Scheme costs. In most cases, the cost of cancellations will be absorbed by
participants’ budgets. If the nature of a participant’s disability makes him or her more
susceptible to cancellations, then the participant’s budget should be increased accordingly.
It is expected this will be a small proportion of participants.
4.6.3.3 Group pricing for attendant care
Issues and evidence
The NDIS has separate pricing schedules in place for the delivery of group-based community,
social and recreational activities; and centre-based group care.
The current price schedule for group-based community, social and recreational activities
assumes the price per participant is inversely proportionate to the number of participants in a
group. The price per participant for a group of 1 support worker to 2 participants (1:2 care
ratio) is half the price of a 1:1 care ratio. The price per participant for a group of 1 support
worker to 3 participants (1:3 care ratio) is one third price of a 1:1 care ratio. For example,
using the current price for attendant care of $44.72/hr67, a provider will receive the same total
of $44.72 whether a support worker delivers one hour of care to one participant, or a group of
two or three participants.
67 NDIA: 2017/18 NDIS Price Guide VIC-NSW-QLD-TAS (version release date July 2017), p. 29

McKinsey & Company 77
Some providers believe the pricing of group care in the community does not consider the
incremental fixed costs they incur when an additional participant is added to a care setting.
These fixed costs include overhead costs for scheduling and invoicing, and the costs
associated with completing case notes or outcome journals for a participant. Providers believe
that in a 1:1 care setting it is possible to complete case notes during a consultation, however
in group sessions this is difficult as there are greater demands on a support workers time due
to the increased number of participants they are caring for. Some providers also believe that
delivering care in a group setting requires a more highly skilled worker, because they need the
skills and experience to manage multiple participants at the same time. For group-based
community, social and recreational activities, it is possible to charge a high intensity rate when
serving participants with complex needs. However, some providers believe that even for
participants without complex needs, a higher skilled worker is required for group settings.
Providers that deliver care to large group sizes believe the Price Guide should include prices
for groups larger than 3 participants to 1 support worker. The Price Guide displays prices for
groups of up to 3 participants per support worker, but there are no prices indicated for groups
of 4 or 5 participants per support worker. Some providers told the IPR team that because they
do not believe the prices for group supports are correct, they stopped delivering care to small
groups and only deliver care to groups of 4 or 5 participants, and charge them the price for a
group size of 3 participants to 1 support worker. This results in their receiving more than
$44.72 per hour as each of the 4 or 5 participants pays one third of the hourly rate. The NDIA
is aware of this practice by providers, and is allowing it to take place because there is no
policy that mandates providers need to charge a price below the 1:3 rate for groups with more
than 3 participants.
The pricing schedule for centre-based group care is different to the pricing schedule for group
care in the community, and some providers delivering centre-based group care believe it is
difficult for them to operate with a surplus at the current price cap. The Price Guide has a flat
hourly rate for centre based group care, and providers are not able to vary the price paid per
participant based on the number of participants in a group, or to reflect the cost of a higher
skilled support worker when they are caring for participants with complex needs (see Section
4.3.2). Some providers also believe the price does not consider the incremental fixed costs
incurred when an additional participant is added to a care setting, as discussed for group
based community, social and recreational activities, as well as the costs of operating a facility,
and the capital providers have invested to make the facilities fit-for-purpose for participants,
such as investment in modifications.
Some providers also raised the issue of cancellations impacting their ability to operate with a
surplus. When a single participant in a group cancels, it is not possible for a provider to charge
a higher rate to the other participants in a group to compensate for the difference in revenue.
This results in the provider receiving less revenue than was expected if they delivered the
support to the remaining participants in the group.

McKinsey & Company 78
Recommendations
16: The NDIA should implement a new pricing schedule for group care (both community based and centre based) outlined in Table 4 that allows providers to recover additional costs incurred for groups, while still retaining the incentives and efficiencies of group based care. It should also assess whether a capital allowance should be provided for centre based care based on whether there is demand to increase the number of centres.
The price schedule of group based community, social and recreational activities should
reflect the additional overhead costs for scheduling and invoicing, the additional
administrative time required to write case notes/populate outcome journals, and consider an
allowance for a higher skilled or experienced worker if it is determined to be appropriate for
participants without complex needs. The price schedule should maintain high intensity
loadings which can be applied above the standard rate for participants with complex needs.
Section 4.3.1 includes a discussion on price loadings for participants with complex needs.
This recommendation is not designed to encourage a participant to lead a life with a high
intensity of support. Rather, it is expected that as the Scheme matures and evidence
develops, providers and the NDIA will be able to assess which interventions are most
effective in supporting participants with complex behaviours and needs to achieve improved
outcomes and, in some cases, no longer require high intensity support.
TABLE 4 shows a comparison of the current price per participant without complex needs for
1:2, 1:3, and 1:4 care ratios compared to price ranges calculated using assumptions for the
incremental fixed costs discussed above. Using data from a small sample of providers for the
share of overheads scheduling and invoicing account for (10-20%), the amount of time spent
per participant writing notes (3-5 mins/hr), and the SCHADS level of support workers for
group care ratios (Level 2.3-3.1). The NDIA should conduct further work to refine the cost
driver assumptions used to develop the new group prices. Once the assumptions have been
refined by the NDIA, it can create a pricing schedule for group sizes larger than 1 support
worker to 3 participants, up to a level deemed to be appropriate for a single support worker
to be able to manage. This pricing schedule should be included in the Price Guide. TABLE 4
indicates prices for group based community, social and recreational activities for groups of
up to 4 participants per support worker.
To support centre based group care, the NDIA should remove the flat pricing schedule that
currently exists and adopt the same approach proposed for group based community, social
and recreational activities. It should also assess whether a capital allowance is required based
on whether there is demand to increase the number of centres. This should involve an
assessment of the future demand for these services relative to the current supply.
TABLE 4: EXAMPLE OF PRICING SCHEDULE FOR GROUP BASED COMMUNITY, SOCIAL, AND
RECREATIONAL ACTIVITIES
Care ratio Current price per participant
Price per participant (without complex needs) including incremental fixed costs
1 staff – 1 participant $44.72/hr $44.72/hr
1 staff – 2 participants $22.36/hr $25.04/hr - $29.07/hr
1 staff – 3 participants $14.91/hr $16.76/hr - $19.68/hr
1 staff – 4 participants No price - providers use $14.91/hr $12.97/hr - $15.20/hr

McKinsey & Company 79
Care ratio Current price per participant
Price per participant (without complex needs) including incremental fixed costs
1 staff – 5+ participants No price - providers use $14.91/hr NDIA to determine the largest group size they will set prices for.
Implications
Increasing the price of group based care to reflect the incremental costs of service delivery
could result in more supply of group care entering the market. This could be beneficial to
participants, particularly for those with higher needs that cannot be cared for in large group
sizes. By giving participants greater opportunity to access group care, they could choose to
spend more of their budget on group care rather than 1:1 care, giving them more funds to
utilise on other supports.
Once the NDIA has finalised a new pricing schedule for group care, they will need to ensure
providers adopt the new prices and discontinue the current practice of charging the price
of 1 staff to 3 participants for groups of 4 or more. The NDIA should consider including audits
of group care delivery in their existing provider audit process to help enforce the use of the
updated pricing schedule.
Therapy supports
The NDIA recognises therapeutic supports may be necessary for many participants to help
build capacity to participate in the broader community. For example, for young participants (0-
6 years), early intervention in the form of medical and disability therapy supports may help
build their capacity to become more independent.
In therapy supports, participants, providers and other stakeholders identified an opportunity to
differentiate pricing for different types of services to better match market rates for services,
and enable the NDIS to provide better value for money to participants. This was supported by
the IPR’s benchmarking with other comparable schemes described in Section 3.3.2 above.
Some providers delivering specialised therapy, for example clinical psychology, believe the
price is not adequate for their participants. Other providers also raised the issue that the
current description for therapy assistants does not reflect the activities undertaken, and that
the price is not adequate to recover their costs, which leads them to serve participants with
qualified therapists when the support could have been delivered by a therapy assistant at a
lower price. Providers also raised issues relating to travel and cancellation policies, and NDIA-
required report writing.
This section provides recommendations and rationale for:
■ 4.6.4.1 Differentiated pricing for therapy supports delivered by a qualified therapist
■ 4.6.4.2 Pricing for therapy supports delivered by therapy assistants
■ 4.6.4.3 Travel policy
■ 4.6.4.4 Cancellation policy
■ 4.6.4.5 NDIA-required report writing

McKinsey & Company 80
4.6.4.1 Differentiated pricing for therapy supports delivered by a qualified
therapist
Issues and evidence
Providers, participant bodies, and other stakeholders raised issues associated with the single
price of therapy. Some providers consider that the current price is more than adequate for
many therapy supports, but where more complex therapy is required, for example complex
psychological therapy delivered by a clinical psychologist, the price is not adequate.
Participant bodies and other stakeholders have raised issues about the single price being too
high where standard therapy is required. For example, for a typical physiotherapy
consultation, participants are being charged a price higher price than the market rate for the
service.
While the NDIA has a single price for therapy supports, other comparable insurance schemes
in Australia have differentiated pricing. Examples include the TAC, WorkSafe, Department of
Veterans Affairs (DVA), and NSW State Insurance Regulatory Authority (SIRA). Section 3.3,
Benchmarking with comparable schemes, indicates that there is opportunity to differentiate
the price of therapy supports based on the type of therapy being delivered, and level of
service a participant requires to meet their needs.
Recommendation
17: The NDIA should develop differentiated price levels for physical therapy and psychological therapy based on price levels being paid in comparable schemes.
Physical therapy should be differentiated across three levels of care, and psychological
therapy across two levels of care (TABLE 5 and TABLE 6).
TABLE 5: RECOMMENDED PRICES FOR PHYSICAL THERAPY SUPPORTS
Level of support
Proposed price ($/hr) Description
Level 1 $110 - $120 The delivery of therapy for a single physical condition (which can result in multiple symptoms) in a low risk environment. An example is occupational therapy to develop the balance of a child with low level cerebral palsy that has a low level of severity on the Gross Motor Function Classification System (GMFCS).
Level 2 $140 - $150 The delivery of therapy for multiple physical conditions where treatment of one condition does not affect symptoms from another condition e.g. occupational therapy for a child with a middle level of severity on the GMFCS that results in multiple physical conditions; can also include treatment of a single physical condition if a participant also has mild-moderate behaviours of concern.
Level 3 $180 - $190 The delivery of therapy to participants with extreme presentations, e.g. occupational therapy for a child with cerebral palsy that has a high level of severity on the GMFCS, that results in physical conditions such as convulsions or spasms or swallowing difficulty such as dysphagia; can also include a combination of physical disabilities and severe behaviours of concern.

McKinsey & Company 81
TABLE 6: RECOMMENDED PRICES FOR PSYCHOLOGICAL THERAPY SUPPORTS
Level of support
Proposed price ($/hr) Description
Level 1 $160 - $170 The delivery of therapy focused on treatment of a psychological disability in a low risk environment. Typically administered by a registered psychologist.
Level 2 $210 - $220 The delivery of therapy focused on the treatment of a complex psychological disability where a very skilled and experienced clinical professional is necessary. Often necessary where a participant poses a high risk to themselves or others due to their disability. Typically administered by a clinical psychologist.
For each level of care in physical therapy and psychological therapy, the NDIA will need to
define the characteristics of the type of therapy support a participant should expect to receive,
and a provider should expect to deliver. The NDIA should work with therapy providers and the
broader therapy market to develop these characteristics.
Implications
Providers of Level 1 and 2 therapy will have price caps lower than the current NDIA price cap.
Providers of Level 3 therapy will be able to charge prices higher than the existing price cap for
participants that require a high level of support due to their disability. When using the
increased prices, providers will need to justify that the higher level of service is necessary to
serve a participant. The NDIA will need to reflect the changes to therapy prices in the
packages developed for participants. These changes should consider a participant’s physical
and psychological conditions, and reflect their likelihood to need a higher proportion of one
level of therapy compared to another.
4.6.4.2 Differentiated pricing for therapy supports delivered by a therapy
assistant
Issues and evidence
The current Price Guide describes therapy assistants as ‘Program to empower participants &
improve interactions between participants & their social networks. Assistance to engage
effectively in the community through a group approach to help achieve goals, gain insight into
their lives & make informed decisions’ and prices these supports at $41.71/hr68. Consultation
with providers suggests that this description does not accurately reflect the role of therapy
assistants, and that the price for a therapy assistant should be at least the same as the price
of attendant care because therapy assistants, at a minimum, require the same level of skill as
a standard level support worker. They believe the price of a therapy assistant should reflect
the cost of a higher skilled support worker due to the increased difficulty of the support being
delivered.
Providers believe they can utilise therapy assistant in two ways. The first is to have a therapy
assistant to help deliver therapy supports, for example to help deliver hydrotherapy by
68 NDIA: 2017/18 NDIS Price Guide VIC-NSW-QLD-TAS (version release date July 2017), p. 61

McKinsey & Company 82
supporting a participant to stand in the water, while a physical therapist instructs a
consultation. The second is in situations where a consultation could be delivered
independently and in full by a therapy assistant with adequate qualifications (such as an
exercise scientist). This might occur in the case of a physical therapy consultation where a
treatment schedule has been developed by a physiotherapist with input from an exercise
scientist, but can be delivered independently by the exercise scientist. The Price Guide does
not currently allow for these two types of roles, and as a result there are examples of
providers serving participants with physiotherapists at $175.57/hr69 when an exercise scientist
could be delivering the consultation at a much lower rate.
Recommendations
18: The NDIA should amend the description for therapy assistants and introduce two tiers of prices for therapy assistants – one that is comparable to the attendant care price, and a second that is for the delivery of therapy supports by a professional with a lower level of skill than a qualified therapist.
A Level 1 therapy assistant could support the delivery of therapy services and be priced in the
range of $44.72-$49.20/hr. The activities performed by this type of therapy assistant is
comparable to those performed by a disability support worker, but with a focus on capacity
building. The relevant benchmark is therefore the attendant care price, and this is consistent
with the price set by other similar schemes such as the Transport Accident Commission
(TAC). The low end of the price range reflects the current price of attendant care, and the high
of the range reflects the price proposed for a highly skilled support worker delivering care to a
participant with very complex needs. This is the current price of attendant care plus an
additional 10% price loading, and should be the absolute upper bound of the price of a Level 1
therapy assistant. This price is aligned with external benchmarks for a Level 1 therapy
assistant. The TAC prices Allied Health Assistants at $37.04/hr and prices therapy supports
for Independently Reviewed against Quality Standards (IRQS) Providers at $46.73/hr.
A Level 2 therapy assistant should deliver therapy supports where a qualified therapist has
developed a treatment plan with input from an exercise scientist, and a consultation can be
delivered by a qualified professional that is not a qualified therapist. This could be an
employee with a qualification in exercise science or human movement that has the skill and
knowledge to deliver a treatment plan they have helped develop at a high level of quality.
The price of a Level 2 therapy assistant should be above the price of a Level 1 therapy
assistant ($44.72-$49.20/hr) and below the proposed price of Level 1 physical therapy ($110-
$120/hr). The market for the delivery of some therapy supports by professionals such as
exercise scientists is new and growing, therefore data on pricing is limited. Discussions with
some therapy providers and an observation of a small sample of private market rates suggest
the price of a Level 2 therapy assistant should be between $70-90/hr, however the NDIA
should conduct further analyses to refine and validate the price, and verify the relevant
benchmark.
69 NDIA: 2017/18 NDIS Price Guide VIC-NSW-QLD-TAS (version release date July 2017), p. 61

McKinsey & Company 83
Implications
Increasing the price of a standard therapy assistant to be comparable to the price of attendant
care will allow providers to recover the costs of employing workers with the same level of skill
as a support worker. Introducing a second tier to the therapy assistant price could allow
participants to receive some therapy supports at a lower price when the support is not
required to be delivered by a qualified therapist, and can be delivered with a high level of
quality by a professional with a lower skill level. This could represent value for money for
some participants, as they could utilise Level 2 therapy assistants where they were previously
seeing a qualified therapist, and redirect the funds they save to other supports.
4.6.4.3 Travel policy for therapy supports
Issues and evidence
Many providers believe the $1000 travel cap for therapy supports and the approach defined
by the NDIA to calculate travel costs are appropriate for participants that are located close to
a therapist or do not require frequent support. However, when a participant requires a provider
to travel a reasonable distance on a frequent basis, the therapy travel policies can make it
difficult for some providers to profitably serve participants, even in a metropolitan area.
For attendant care supports, there is no monetary cap on the amount a provider can charge a
participant for travel. It is a different case for therapy as a $1000 per annum cap exists, and in
situations where a moderate amount of travel is required, the therapy travel cap can run out
quickly, as it equates to less than 6 hours of travel that a provider can charge over a year at
the current therapy price cap of $175.57/hr70.
Separating therapy support funding from therapy travel has positive and negative
consequences. Placing a limit on the amount a therapist can charge for travel incentivises
participants to receive supports from providers where less travel is needed to reach them.
However, there are examples of providers ceasing to serve participants that have funds
remaining in their plans for therapy supports, because they have exhausted the $1000
allowance that providers can charge for travel.
The policy providers are required to follow to charge for travel is also making it difficult for
providers, as the calculation does not allow providers to charge for the first 10km of travel.
Beyond 10km providers can charge up to the hourly rate of therapy supports based on the
distance travelled, with the assumption being that the average speed of travel is always
60km/hr. For core supports such as attendant care, providers can charge the first 20 minutes
of travel between participants (excluding travel to the first participant).
An effective travel policy should encourage participants to find services that require less travel
where adequate supply is available, and discourage providers from serving participants where
more travel is required if there are closer options available. The policy should also
acknowledge that there are situations where travel is necessary, and allow providers to be
70 NDIA: 2017/18 NDIS Price Guide VIC-NSW-QLD-TAS (version release date July 2017), p. 61

McKinsey & Company 84
remunerated for a reasonable amount of travel. However, the policy should only apply where
the participant cannot travel to the provider.
Recommendations
19: The NDIA should align the travel policy for therapy supports to the travel policy for attendant care by removing the $1000 travel cap, allowing providers to charge up to 20 minutes at the hourly rate when travelling between participants.
The travel policy for therapy should be consistent with the travel policy for attendant care,
where there is no travel cap or separate travel allowance, and a provider can charge the first
20 minutes of travel between participants. The policy should also follow the approach
suggested in Section 4.2.2, where providers serving participants located in rural areas (MM 4
and MM 5) can charge up to 45 minutes at the hourly rate when travelling between
participants.
Implications
The NDIA will need to communicate with participants receiving therapy supports in-home that
they will no longer have a separate budget for provider travel, and that a provider will be able
to charge travel against their combined therapy budget with no maximum set by the NDIA.
Participants will need to take this into consideration when they select a provider. If the
preference of the participant is to receive supports from a therapist located far from their home
they may receive less supports, as the provider will be able to charge up to 20 minutes in a
metro area (45 minutes in rural areas) each time they travel to the participant.
The NDIA will need to communicate with providers that there are limitations on the amount of
travel time they can be reimbursed for each time they visit a participant. If a provider chooses
to serve a participant located outside of the area they can service based on the time caps set
for metro and rural areas, they will not be reimbursed for the incremental travel time.
4.6.4.4 Cancellation policy for therapy supports
Issues and evidence
The therapy cancellation policy limits the number of hours a provider can charge to a
maximum of 2 cancelled hours per year, compared to a maximum of 8 booking cancellations
per year for core support items including Assistance with self-care activities and Assistance to
access community, social/recreational activities. Providers believe 2 hours is insufficient as
many participants cancel more than 2 hours of services per year. For example, participants
with health-related needs may cancel due to hospitalisation due to their condition, and
participants with behaviours of concern may cancel due to sudden escalations of behaviour.
Currently providers are often required to absorb the cost of cancellations over 2 hours, even
where they are short-notice, as it is typically very difficult to substitute in another patient on
short notice, especially when services are delivered in-home.

McKinsey & Company 85
Recommendations
20: The cancellation policy for therapy should be amended so that up to a certain threshold, providers can charge against a participant’s plan for up to 90% of the scheduled service if the participant makes a short notice cancellation. A cancellation line item should be created as a governance mechanism for the NDIA.
The cancellation policy for therapy should follow the same approach as that suggested for
attendant care (see Section 4.6.3.2). A short notice cancellation should be defined as
occurring where a participant provides notice of cancellation after 3pm the day before the
scheduled service. A cancellation line item should be introduced in the Price Guide to enable
the NDIA to monitor the volume of cancellation by providers, which will help build an
understanding of participant cohorts with higher risks of cancellations, and help detect
anomalies in the volume of cancellations. Providers should not charge a cancellation where
they have been able to substitute another customer.
The NDIA also should introduce a policy that above a specific threshold, providers will not be
able to charge for cancellations unless they submit a report to the NDIA outlining the
circumstances of each above-threshold cancellation, and actions taken to work with
participants to minimise the risk of their cancellations.
Implications
As discussed in Section 4.6.3.2 the proposed policy minimises the financial loss incurred by
providers on short-notice cancellations and recognises that while providers should work with
participants to minimise short notice cancellations, providers should also not bear the
financial risk for this occurring.
4.6.4.5 NDIA-required reports for therapy supports
Issues and evidence
Some providers indicated they were confused about whether they could be reimbursed for the
time they spend developing reports for participants. The NDIA has set the expectation that
providers are required to develop progress reports for participants, the Price Guide states
‘Therapists will be expected to provide progress reports to the participant and NDIS at agreed
times’.71 Currently there are some therapy providers that believe they can be reimbursed for
report writing, and charge the time against a participant’s package. However, there are other
providers that do not believe it is possible to charge a participant for report writing, and they
are absorbing the cost of the time to develop a report.
There are two types of reports therapists typically write: end-of-session notes and progress
reports. Therapists write end-of-session notes to capture what has taken place during an
individual consultation. This is a standard activity and should be considered as being included
in the hourly rate for the support. Therapists write progress reports upon request, often by a
third party, where information is sought to understand how a participant’s condition is
71 NDIA: 2017/18 NDIS Price Guide VIC-NSW-QLD-TAS (version release date July 2017), p51

McKinsey & Company 86
improving due to their therapy. This is not considered a standard activity and therefore should
be reimbursed separately.
Comparable schemes such as SIRA, TAC, and Worksafe each reimburse providers for
reports, and have discrete line items in their fee schedules for reports requested by the
insurers. SIRA has a single line item for report writing, and TAC and Worksafe have multiple
line items for the development of the initial treatment plan, and also for treatment reviews. For
each of the schemes, they will only allow a provider to charge for the reports if they have been
specifically requested by an agent within insurer.
To provide therapy supports in the NDIS there are two types of reports that a provider must
deliver to help the NDIA track a participant’s progress: 1) at the commencement of supports,
the NDIA requires a report to be submitted including the assessment of a participant, their
goals, and the care plan developed to achieve those goals; and 2) as a participant progresses
through their care plan, the NDIA requires a therapist to submit one or more reports per year
to the NDIS to communicate the progress a participant has made against their goals, including
evidence of specific areas of improvement and outcomes that have been achieved. The
progress reports also include recommendations from a therapist on what they believe a
participant’s new or revised goals should be based on their progress at the time, and a
proposal for a new or revised care plan to support a participant to achieve those goals.
Recommendations
21: The NDIA should allow providers to charge participants for the time spent writing reports that are requested by the NDIA. A new line item should be introduced for tracking purposes.
The time that a therapist can charge does not include time spent at the end of a consultation
writing notes, which is factored into the rate paid for the consultation. However, for additional
reports mandated by the NDIA, providers should be allowed to charge for time spent
developing these reports at the same rate as a regular consultation, as they are an essential
part of the service being delivered to a participant. This should be communicated to the
market to ensure there is consistent application across all therapy providers.
Implications
The impact on participants of allowing therapists to be reimbursed for the development of
NDIA-required progress reports is expected to be small, as it should occur no more than once
or twice a year. Adding a separate line item in the Price Guide for NDIA-required reports will
allow the NDIA to track therapists that are charging participants for report writing, to make
sure it is only occurring when they have requested a report to be written by a therapist.
4.7 PRICE DEREGULATION
The deregulation of NDIS prices offers some compelling advantages for providers and
participants operating in a mature market. The effect of current NDIS price controls is that
nearly all transactions take place at the specified price cap. Forcing the market to a single
regulated price introduces the risk that the market will be undersupplied (if the price is too
low), or that participants will not be able to achieve value for money (if the price is too high). In
McKinsey & Company 87
a market like disability services, regulated prices also restrict the ability of providers to offer a
range of different service types and thereby limit participants’ ability to choose the best mix of
quality and price that suits their needs for any service. Deregulation also has the benefit of
reducing bureaucracy, making it easier for participants and providers to interact with the NDIS.
However, price deregulation comes with risks if implemented in an underdeveloped market. In
particular, it may result in providers charging higher prices and participants receiving less
value for money.
To navigate this choice, the NDIA should collect more information to understand the likely
impact of deregulation of prices, prepare participants and providers for deregulation, and
undertake trial(s) before deregulating prices across large portions of the market.
This section covers the following topics:
■ 4.7.1 Developing more information and insights on self-managed participants
■ 4.7.2 Assessing and advancing participant and provider readiness for de-regulation
■ 4.7.3 Conducting a deregulation trial
Developing more information and insights on self-managed participants
Issues and evidence
There is currently limited information to understand how the NDIS would operate if prices were
deregulated. One source of possible insight is the experience of self-managed participants,
who operate in a commercial environment that is broadly comparable to a deregulated market.
These participants are allocated a budgeted plan through the same process as all other
participants. However, the providers they choose and manage are not bound by the NDIA’s
price caps in providing support services to them72. This is therefore somewhat comparable to
the experience of participants in a deregulated market.
According to the latest NDIA data, 18% of Scheme participants have at least partially self-
managed plans73. Anecdotal evidence from participants who self-manage their supports
suggests there are many benefits of self-managing, including much greater flexibility in how
funds are used across support categories. However, further analysis is required to understand
whether this experience is likely to be replicated across the Scheme as a result of broader
price deregulation.
There is currently only partial data available on the experience of self-managed participants.
Through auditing processes, the NDIA has the potential to gather data on how self-managed
participants allocate funds within their budgeted plans. The NDIA also collects participant
outcomes data which can be used to track the performance of self-managed participants
against those of Agency-managed or plan-managed participants.
72 Note: providers serving both self-managed and NDIA-managed participants typically charge both groups of participants at the price cap. Therefore, only a small part of the self-managed market is effectively operating as per a deregulated market.
73 Source: Scheme Actuary

McKinsey & Company 88
Recommendations
22: The NDIA should collect and analyse information on the experience of self-managed participants to help inform its assessment of price deregulation.
A better understanding of the outcomes of self-managed participants can help the NDIA
understand the opportunities and challenges of potential price deregulation.
The NDIA should collect information on:
■ The pricing of support services provided to self-managed participants, including prices
relative to the rest of the Scheme, the distribution of prices within the market for self-
managed participants, and the responsiveness of prices to competitive pressure.
■ Outcomes for self-managed participants.
■ The supply response to price changes for supports catering to self-managed participants.
This information can be gathered through existing sources, as well as through new initiatives.
Data on outcomes of self-managed participants can be gathered by categorising responses to
the Short-form Outcomes Framework survey. Comparing self-managed participants with
Agency-managed participants may be affected by some sampling bias, as self-managed
participants are likely to have better support structures around them, which could lead to
better outcomes. Therefore, it will be more useful for the NDIA to compare changes within
cohorts over time, rather than across cohorts.
Some general scheme data, such as utilisation rates, are also already being collected by the
NDIA and could be monitored by the participant’s type of support management. The NDIA is
planning to collect more thorough data on which supports are being accessed by self-
managed participants, and for what prices, as part of its assurance process for self-managed
participants.
Implications
The NDIA will need to collate the information it has on self-managed participants from the
Scheme Actuary, the Provider, Market and Sector Development team, and its quality and
safeguards assurance processes.
The NDIA will also need to expand its data collection and analysis efforts in some instances,
including amending the Short-form Outcomes Framework survey or other participant
consultation as necessary. The NDIA should also include queries specific to self-managed
participants in its regular consultation with providers, including through LACs, its annual
request for submissions into the pricing process, and ad hoc consultations throughout each
year.
Assessing and advancing participant and provider readiness
Issues and evidence
Deregulated markets will allow providers and participants to transact freely without being
bound by price caps. The NDIS marketplace is yet to be guided by a clear set of pre-
conditions which would need to be satisfied for such transactions to function effectively. Price
McKinsey & Company 89
controls cannot be relinquished until the NDIA is satisfied that such pre-conditions have been
articulated and satisfied.
A broad review of provider and participant capacity makes clear that it remains too early for
the Scheme to pursue price deregulation across markets at this point in time. Most providers
and participants have spent under a year in the Scheme, and the Scheme continues to grow
rapidly from quarter to quarter. As such, there is little stable evidence to evaluate the
performance and capabilities of participants and providers in the Scheme. Even in existing
competitive and well-supplied markets like those for some forms of therapy, it is important to
observe participant and provider behaviour over a longer timeframe.
The NDIA supports the capability development of participants and providers through various
initiatives. This ranges from core elements of the NDIS such as LACs, through to the release
of market information such as the Market Position Statements. Others, such as support
coordinators or online marketplaces, also work to expand the capacity of participants and
providers to locate and compare with each other.
Recommendations
23: The NDIA should collect information on and assess the readiness of participants and providers for price deregulation.
The NDIA can test the readiness of the market for price deregulation by considering the
commercial and other characteristics required to operate in a deregulated market. Before
deregulating a market, the following conditions should be met:
■ Participants must first have a thorough awareness of their supports and prices in their
market.
■ Participants must have the ability to exercise choice and control by switching between
providers as required. The development of the e-market would support this by giving
participants greater information about alternative providers and greater transparency on
the range of prices charged in the market.
■ Providers must have the commercial capacity to make efficient pricing decisions.
■ Providers must have the ability to provide sufficient supply to drive competition and
moderate price fluctuations.
The required information can be collected through participant and provider consultation,
analysis of existing market and NDIA data, and by collating NDIA experience from its network
of LACs and regional offices. This assessment of the readiness of markets for deregulation
should consider specific markets and not just the Scheme in aggregate. Different markets
within the Scheme – be they geographic regions or various support types – will be ready for
deregulation at different times. Deregulation should, therefore, not be considered as a single
event to be rolled out across the Scheme, but rather as a process to be introduced to markets
as they become sufficiently mature.
24: The NDIA should provide more comprehensive market data to support the development of provider and participant capacity.
The NDIA should make available more detailed market information on participants’ demand
for services, and the available supply of support services. In addition to market overviews

McKinsey & Company 90
presented in its Market Position Statements, the NDIA can provide further evidence of what
support services participants are demanding and accessing in each market – defined by
support type and geographic region – and the state of supply in those markets. This could
take the form of more detailed Market Position Statements, the Provider Finder, or e-markets
(see Section 4.5). Market information can also be disseminated through the NDIA’s existing
LACs and regional office network, as well as through support coordinators. Information on
where participants are located, their patterns of demand, and the current state of service
provision in a given market are very relevant to providers making pricing or supply decisions.
Ensuring that such market data is available will likely lead to increased competition in the
market, and improve the readiness for price deregulation.
Implications
Ensuring timely access to detailed market data will promote participant outcomes in the short
term. It will also support market development in the medium to long term, with the potential to
accelerate readiness for price deregulation across markets.
Conducting a deregulation trial
Issues and evidence
It is essential that price deregulation begins with a trial, given the limited information currently
available on how the disability support services market in Australia would operate in a
deregulated pricing environment, as well as the lack of directly comparable markets
elsewhere.
A trial will allow the NDIA to collect more detailed information on the impact of deregulation.
This information can help the NDIA confirm its assessment of the readiness of markets for
deregulation, and help refine the design choices to be made in implementing deregulation.
A deregulation trial would involve the removal of price caps in a specified market, defined by
support type or region.
Recommendations
25: The NDIA should pursue a trial of price deregulation in one market, once the preconditions for deregulation have been satisfied.
The market chosen for deregulation should have well-equipped participants and providers as
identified in Section 4.7.2, as well as meet three additional criteria:
■ The chosen market should have been active in the Scheme for at least 2 years. This will
allow the NDIA to assess whether the information collected about that market reflects a
stable state.
■ The chosen market should be clearly defined and demarcated from the remainder of the
Scheme. For geographies, this would mean that the defined area is aligned to other
boundary definitions affecting how businesses operate (e.g. state borders, remoteness
thresholds).
■ The market should be one in which the NDIA is satisfied that it has monitoring capacity
and a good understanding of Scheme and market performance to date.

McKinsey & Company 91
Some therapy supports and well-defined geographical areas such as the ACT have been
identified to the IPR team by providers and other Scheme stakeholders as potential
candidates for deregulation. These do not yet appear to be ready for deregulation as the
Scheme is still in its early stages and there is insufficient evidence that providers and
participants have the capacity to navigate a deregulated market. The NDIA should monitor the
progress of these and other markets against the above criteria to identify a suitable market for
a deregulation trial.
The NDIA could consider transitioning toward the trial by replacing prescriptive price caps with
suggested price ranges as a way of testing market capacity for price competition. To do this, a
price guide for that market would identify two prices for a given support item, a lower price
which is nominated as the suggested efficient price, and a higher price which acts as the price
cap. Even though the current price is only a price cap for most support services, the great
majority of providers charge at this price point, and there is no way to indicate an efficient
price using a single price cap.
The introduction of deregulated pricing in a chosen trial market should be accompanied by
enhanced safeguards and monitoring in that area. The NDIA should be able to identify risks of
supply shortages or where providers are charging well above their cost to serve to the
detriment of participants’ ability to secure plan outcomes.
Implications
Designing and delivering a deregulation trial will require an investment of resources from the
NDIA in the medium term. However, a well delivered deregulation trial will provide a lower risk
way to test the proposed preconditions for deregulation of prices and ultimately, promote a
more innovative and sustainable Scheme.

McKinsey & Company 92
Appendix A: Differences in cost drivers
between attendant care providers
Summary of key differences in cost drivers between attendant care providers
The following table summarises some differences in cost drivers between providers, and
explains the significant variation in cost to serve between different attendant care providers.
TABLE 7:
Issue Provider feedback
Labour costs ■ Some providers found it difficult to manage labour costs under the current price. This was particularly true for providers who had a mix of complex and standard intensity clients, and therefore had more qualified or mature workforces. For instance, for some providers, the average worker had a Cert IV qualification and was paid at SCHADS 2.3. By contrast providers who focus on participants at the lowest end of the complexity spectrum submitted it was neither necessary nor proportionate to pay a highly qualified worker to deliver attendant care; rather it was the support worker’s mindset that was important.
■ Under the SCHADS Award, employers pay casual workers a 25% loading on the base salary of an FTE. The more expensive base wage of and fixed cost of onboarding and training a casual worker is offset by a various factors: first, casual workers have lower on-costs as they are not entitled to annual or sick leave; second, it is easier to manage the utilisation rates of casual workers; finally, anecdotal evidence suggests employers with heavily casualised workforces tend to pay lower base salaries. Depending on the difference in utilisation and base salary paid to casual workers vis a vis FTEs, casual workers can be either more or less expensive to hire.
Workforce utilisation
■ Factors that make workforce utilisation difficult to manage include: unchargeable time spent travelling to clients, particularly in regional and remote areas; the frequency of cancellations in the sector; and, the time required for care co-ordination (e.g. team meetings, debriefing) and reporting, particularly for behaviourally and medically complex participants. Utilisation is particularly challenging to manage in areas of lower population density and for providers with less casualised workforces.
■ Utilisation was significantly easier to manage for providers with highly casualised workforces, as staff are only rostered when there is known demand. However, because casual workers are paid a 25% loading under the SCHADs award (which is only partially offset by the lower on-costs associated with casual workers), whether a casual worker is more expensive to employ than a permanent employee depends on how well an employer can utilise its casual workers relative to its permanent workforce.
Supervision structures
■ Some providers had heavy supervision structures, reflecting the complex participants in their client mix. For instance, some providers have 2 layers of supervision consisting of a supervisor and a team leader. Providers who only serviced lower complexity participants with strong informal supports had minimal supervision in their operating models, rather relying on instant customer feedback to detect potential risks to service quality.
Corporate overheads
■ This was a key differentiating cost driver between providers. Traditional providers that had achieved relatively efficient overheads had typically invested in IT and had achieved a degree of scale. Online platform providers also leveraged

McKinsey & Company 93
Issue Provider feedback
technology to minimise overhead costs, while sole traders incurred very low overhead costs.
Other issues ■ Training: While there are currently no legislative requirements for disability support workers to undergo specific trainings, some providers, particularly those with complex participants in their client mix, require their staff to complete a mandatory training as a matter of internal policy.74
74 Some of these trainings include: First Aid, Manual Handling, Corporate Induction, Medication and infection control; CPR; Epilepsy; Diabetes; Bowel care; Oxygen Training; Management of PEG feeding.

McKinsey & Company 94
Appendix B: Summary of IPR
recommendations
Below is a summary of the IPR team’s recommendations, as well as an assessment of the
potential impact of these recommendations on the NDIA’s three aspirations. Cost estimates
have been made on the best information available. Where information is incomplete due to
immaturity of the Scheme, the IPR has made a number of assumptions, which has led to wide
ranges in estimates. In the aggregate, the IPR team estimates that the recommendations
made in this report will have a potential financial impact of ~$250-420m per annum over the
next 12 to 24 months, but will alleviate some of the financial pressure currently placed on
some providers, and will improve participant outcomes by addressing challenges that are
impacting some providers’ abilities to deliver quality services.
Beyond the next 24 months, the IPR team believe it is possible to implement the IPR
recommendations and manage the Scheme so that it is financially sustainable and within the
current budget estimates. Approximately 50% of the total cost implication of the IPR
recommendations is temporary and will therefore not have an adverse impact on the
Scheme’s longer-term financial sustainability. Also, as the Scheme matures, the NDIA should
be able to offset any financial impact of these recommendations by appropriately assessing
their effectiveness and efficiency. For example, as evidence develops as to which
interventions are most effective in reducing costs associated with complexity, it should be
possible to reduce the number of complex participants and provider costs and prices. It should
also be possible to encourage more local providers in rural and remote areas that will assist in
reducing travel costs. There should also be some savings from introducing tiered therapy
pricing.

McKinsey & Company 95
EXHIBIT 9
EXHIBIT 10
Summary of recommendations (1/3)Short term = < 1 year Medium term = 1-2 years Long term = 3+ years
Neutral/No impact
Potential significant negative impact
E.g. >$50m for Scheme sustainability
Positive impact
Potential minor negative impact
E.g. <$50m for Scheme sustainability
($Xm) = Value used by IPR team to calculate the total financial impact of
recommendations if different from range provided by the Scheme Actuary
1 $26m assumes 25% of participants in ARIA-outer regional get the additional loading and the impact of the loading is only 10% (i.e. 45 mins hr travel for every 6.75 hrs of care). $75m
assumes 25% of participants in MM4 and MM5 receive a loading and the impact of the loading is 20%. If all participants in MM4 and MM5 received the additional loading (and impact was
20%), this would equate to a cost of $296m. The IPR does not believe this to be a likely scenario.
2 Based on 12% of participants qualifying for the complex level (a 6% loading) and 10% of participants qualifying for the very complex level (a 10% loading), with a margin of error of +/- $20m
to account for uncertainty in data, and assuming all participant plans are adjusted to compensate for the change in policy
Price-
setting
process
National
vs
regional
pricing
Comp-
lexity
Direct impact on NDIA aspirations
Market
development
Participant
outcomes
Scheme
sustainability
Implications
Implementation
timeframe
Short-term1 Include a broader set of indicators of participant outcomes and market
development in its price setting process, and clarify the methodology for making
price setting decisions.
Medium-term2 Continue to use an hourly rate approach, but trial outcomes-based pricing.
$26-75m1
Short-term4 Clearly define rural areas and lift the travel allowance from 20 mins to 45 mins for
providers serving a participant located in MM5 (or ARIA equivalent) and MM4 in
the short term. Adjust plans to account for travel and track as a separate line item.
Medium-term3 In very remote/isolated areas, work with other community services and providers to
support local workforce development to deliver services in the most efficient way
possible. In regions with limited local supply, allow providers to quote on cost of
delivering NDIS services in the short term to ensure supply.
Long-term5 Converge the two Price Guides and move toward a single national price guide
by 2021.
Short-term9 Update the pricing structure for the core support item ‘Group based activities in a
centre’ to allow providers to charge a high intensity loading where a more skilled
worker is required to serve a participant, and set prices consistent with the care
ratio required to serve a participant.
Short-term8 Develop a consistent process for participants with extreme behaviours of concern
that acknowledges the specialised needs of the participant cohort, and the
environment providers operate in. Providers serving this cohort should quote on
the delivery of services to these participants, and also be allowed to deliver them
all of the services they require to be adequately supported (i.e. all Support
Coordination items).
Medium-term6 Develop a definition for complexity linked to the skills required to meet participant’s
needs, and use specialised planning resources to classify what skills are required,
and which participants require higher skilled support workers.
$100m –
$140m2
Medium-term
(require
definition first)
7 Add an additional tier to the high intensity loading to allow a provider to recover the
cost of a support worker with a higher level of skill than can be procured with the
current high intensity loading.
Recommendation
Summary of recommendations (2/3)
1 $130m assumes 2% TSO for the 12 months in FY18/19, $190m assumes 3% TSO for the 12 months in FY18/19. Assumes TSO is applied to attendant care supports only (excludes SIL).
Thin
markets
Relative
provider
efficienci
es and
ade-
quacy
of
provider
returns
Long-term13 Prioritise the implementation of measures to continue to improve the NDIA’s portal,
responsiveness and communication as part of the Participant and Provider
Pathway Reviews.
Short-term16 Implement a new pricing schedule for group care (both community based and
centre based) that allows providers to recover additional costs incurred for groups,
while still retaining the incentives and efficiencies of group based care. Also assess
whether a capital allowance should be provided for centre based care based on
whether there is demand to increase the number of centres.
$130-190m1
Short-term14 Implement ‘temporary support for overheads’ (TSO) in the form of a temporary
increase to the price cap for standard intensity attendant care. Government should
offer business planning support for large providers that would otherwise exit and
create the risk of supply shortages.
Short-term
15 Amend the cancellation policy so that up to a certain threshold, providers can
charge against a participant’s plan for up to 90% of the entire duration of the
scheduled service if the participant makes a short notice cancellation. Above this
threshold, providers will need to demonstrate they are actively working with
participants to minimise the risk of cancellations in order to continue charging for
cancellations.
Short-term17 Develop differentiated price levels for physical therapy and psychological therapy
based on price levels being paid in comparable schemes.
Short-term11 Adopt a clear set of metrics to more comprehensively identify and respond to risks
of thin markets emerging.
Medium-termInvest in Scheme infrastructure such as an e-market tool, which would empower
participants in thin or undersupplied markets to find suitable providers. 12
18 Amend the description for therapy assistants and introduce two tiers of prices for
therapy assistants – one that is comparable to the attendant care price, and a
second that is for the delivery of therapy supports by a professional with a lower
level of skill than a qualified therapist.
Short-term
Short-term10 Continue to refine the assumptions for high intensity rates, active overnight, and
capital allowances used to develop the new STA price schedule, to ensure they
reflect the cost of service deliverySTA
Direct impact on NDIA aspirations
Market
development
Participant
outcomes
Scheme
sustainability
Implications
Implementation
timeframeRecommendation
Short term = < 1 year Medium term = 1-2 years Long term = 3+ years
Neutral/No impact
Potential significant negative impact
E.g. >$50m for Scheme sustainability
Positive impact
Potential minor negative impact
E.g. <$50m for Scheme sustainability
($Xm) = Value used by IPR team to calculate the total financial impact of
recommendations if different from range provided by the Scheme Actuary

McKinsey & Company 96
EXHIBIT 11
Summary of recommendations (3/3)
Price
deregula-
tion
23 Collect information on and assess the readiness of all participants and providers
for deregulation.
Medium-term
24 Provide more comprehensive market data to support the development of provider
and participant capacity
Medium-term
Amend the cancellation policy for therapy so that up to a certain threshold,
providers can charge against a participant’s plan for up to 90% of the scheduled
service if the participant makes a short notice cancellation. Create a cancellation
line item as a governance mechanism for the NDIA
20 Short-term
Medium-term22 Collect and analyse information on the experience of self-managed participants to
help inform NDIA’s assessment of deregulation.
25 Pursue a trial of price deregulation in one market, once the preconditions for
deregulation have been satisfied
Medium-term
Relative
provider
efficien-
cies and
ade-
quacy
of
provider
returns21 Allow providers to charge participants for the time spent writing reports that are
requested by the NDIA. Introduce a new line item for tracking purposes.
Short-term
Short-termAlign the travel policy for therapy supports to the travel policy for attendant care by
removing the $1000 travel cap, and allowing providers to charge up to 20 minutes
at the hourly rate when travelling between participants.
19
Direct impact on NDIA aspirations
Market
development
Participant
outcomes
Scheme
sustainability
Implications
Implementation
timeframeRecommendation
Short term = < 1 year Medium term = 1-2 years Long term = 3+ years
Neutral/No impact
Potential significant negative impact
E.g. >$50m for Scheme sustainability
Positive impact
Potential minor negative impact
E.g. <$50m for Scheme sustainability
($Xm) = Value used by IPR team to calculate the total financial impact of
recommendations if different from range provided by the Scheme Actuary

McKinsey & Company 97
Appendix C: Variation in attendant care cost
drivers across jurisdictions
EXHIBIT 12
Labour costs make up 80% of the costs of attendant care services (which account for
approximately 75% of NDIS expenditure)75. There is currently some variation in labour costs
between states, but they are not correlated to the differences in prices between the Eastern
Price Guide and Western Price Guide. For example, New South Wales and Victoria are
covered by the same Price Guide but include Award provisions for Level 2.3 workers with
slightly different pay rates. Similarly, the ACT and Western Australia have the same Award
rate for Level 2.3 workers despite being covered by different Price Guides.
Analysis of other labour costs such as payroll tax, leave entitlements and workers
compensation requirements does not show a consistent difference between the eastern states
versus the western states. For example, the payroll tax rate in South Australia and Victoria
(which are administered by different price guides) is similar at just under 5% annual rate and
annual threshold of approximately $600,000. Meanwhile, the ACT and Western Australia are
SCHADS awards are broadly comparable across states and territories
STATE Relevant Award (adjusted to 2016/17 per Equal
Remuneration Order)
Hourly pay rate of full
or part time worker at
Level 2.3
Hourly pay rate of full
or part time worker at
Level 3.2
NSW Social, Community, Home Care and Disability Services
Industry Award 2010 [MA000100] and Social and
Community Services Employee (State) Award [AN120505]
(NSW)
$25.52 (Grade 1)
$25.97 (Grade 2)
$28.21
ACT Social, Community, Home Care and Disability Services
Industry Award 2010 [MA000100] and Social and Social
and Community Services (ACT) Award 2001 [AP808334]
$25.52 $27.68
Victoria Social, Community, Home Care and Disability Services
Industry Award 2010 [MA000100] and Social and
Community Services – Victoria – Award 2000 [AP796561]
$25.52 (Youth or
welfare worker) –
$26.11 (Community
development worker)
$27.35 (Youth or welfare
worker)
$27.59 (Social worker)
South Australia Social, Community, Home Care and Disability Services
Industry Award 2010 [MA000100] and Social and
Community Services Award [AN150140] (SA)
$25.71 $27.68
Western Australia Social, Community, Home Care and Disability Services
Industry Award 2010 [MA000100] and Social and
Community Services – Western Australia Award 2002
[AP815319]
$25.52 $27.35 – $27.68
(Depending on
experience)
NT Social, Community, Home Care and Disability Services
Industry Award 2010 [MA000100] and Social and
Community Services Industry – Community Services
Workers – Northern Territory Award 2002 [AP817216]
$25.75 $27.76
Queensland Social, Community, Home Care and Disability Services
Industry Award 2010 [MA000100] and Social and
Community Services (Queensland) Award 2001
[AP808848]
$25.52 $27.35
Source: Social, Community, Home Care and Disability Services Industry Award 2010, accessed in November 2017.

McKinsey & Company 98
administered by the same guide but the former has a payroll tax rate 1.35 percentage points
higher and an annual threshold $1.15 million higher. Similarly, the qualifying period for long
service leave is 15 years in Victoria and WA (again, there are different price guides), while it is
10 years in NSW which is regulated by the same price guide as Victoria. Finally, workers
compensation premiums are higher in the ACT and Tasmania, while Western Australia has
much lower premiums than South Australia. Non-labour components of cost such as utilities,
rent, and cost of goods vary within states as much as they do vary between states.

McKinsey & Company 99
Appendix D: Existing definitions of
participant complexity within the NDIA
The NDIA currently uses three discrete approaches to categorise participants with complex
needs through the pre-planning, planning, and plan implementation phases of the participant
pathway. There is no relationship between any of the three approaches, and they are used in
isolation. This means specific characteristics relating to a participant’s level of need that
surface during pre-planning or planning phases are not always used to inform whether they
receive a high intensity loading during plan implementation.
During the pre-planning phase participants are segmented based on ‘streaming factors’ that
are designed around workflow, to help the NDIA understand the amount of time required to
keep a participant engaged in the participant pathway. These factors include behaviours of
concern, involvement in multiple service systems (e.g. the justice system or Child Protection),
and the level of informal supports. Participants are streamed into four categories – General,
Supported, Intensive, and Super Intensive, with the greater the intensity the more time/effort
required to be spent on participant.
As participants progress to the planning phase, they are assessed using a Disability Severity
Indicator, which measures of the impact of the disability on the participant's day-to-day life, to
determine their level of functional impairment. The level of functional impairment, together with
to the participant’s age and location, are used to determine the level of funding a participant
receives. Participants are allocated a rating between 1-15 describing their level of functional
impairment, as follows: 1-5 Low level of disability-high functional capacity; 6-10 Medium
functional capacity; (11-15) High level of disability-low functional capacity.
Once a participant receives a plan and selects the providers to deliver their services, providers
assess the participant based on a range of additional factors, such as disability type, budget,
personal/family situation, to determine if they should be charged at a standard intensity rate or
a high intensity rate. The Price Guide notes that a provider can charge a high intensity rate
where a participant requires assistance from a support worker with additional qualifications or
experience relevant to the participant’s complex needs. High intensity rates can be considered
when assistance is required to manage challenging behaviours, or when active support is
required due to high medical support needs, such as unstable seizure activity or respiratory
support.

McKinsey & Company 100
Appendix E: Opportunities for attendant care
providers to innovate
The IPR team has identified three broad areas where traditional providers of attendant care
can innovate and drive efficiency, based on the information it received in provider
consultation.
Going forward, the new benchmarking project should provide tailored and strategic
information to providers to help them understand how their input costs benchmark against
their peers, and where there are specific opportunities to drive efficiency. In the longer term,
the aspiration of this benchmarking project is to link data collected on provider input costs, to
information about service quality and participant outcomes. This will build a more wholistic
picture of how the sector can drive better participant outcomes with greater efficiency.
A. Achieve efficiencies in corporate overheads
The significant variation in provider cost to serve from the sample of cost inputs submitted to
the IPR team indicates that, there is significant opportunity for some providers to improve
their corporate overhead efficiencies.
Medium to large providers should be investing in technology (for attendance, online booking,
automation, rostering) to achieve efficiencies in indirect overheads, while smaller providers
should consider using shared services.
B. Optimise staff mix and staff rostering
Workforce planning and support worker utilisation is critical under the NDIS now that
providers are only for funded for units of direct client service. Providers are facing a
heightened need to maximise the time staff spend performing-chargeable activities. In
response, providers should improve their ability to predict demand for services, and use this
information to optimise their workforce mix (e.g. full-time, part-time and casual workers) and
workforce rostering.
The IPR team notes that predicting and optimising staff mix and staff rostering may be
particularly difficult in the current NDIS context for a number of reasons: first, providers may
not have the data and capability to analyse historical demand for services; second, even if
providers had this data, the transition to full Scheme will means historical demand may not
be the best predictor of future demand; finally, in rostering staff, providers of disability staff
need to optimise for many variables (including participant needs, participant preferences,
staff skill, staff available, staff preference, and staff geography) to ensure it can supply
adequate and high quality services.
While these workforce utilisation challenges exist in many other industries, the relatively
fragmented nature of disability care means many traditional providers do not have the
financial capacity or the scale to justify investing in digital solutions that could assist
providers improve workforce.
C. Segment service lines based on participant needs
Many providers currently maintain the same staff pool and supervision structures across all
their participants. This is often driven by rostering, which is easier to do if all staff are

McKinsey & Company 101
capable of serving the most complex participants the provider serves, that is they are trained
to the highest common denominator.
Providers should identify participant segments and design customer-centric operating
models to ensure staffing and supervision structures are commensurate with the participant
segment’s needs.
The level of staff qualification, training, experience, and supervision, and therefore the labour
costs involved in delivering safe and high quality care varies significantly between
participants at different points on the complexity spectrum: At the lowest end of the
spectrum, soft skills rather than formal certifications are more important to delivering a high
quality service; At the highest end of the spectrum, formal qualifications and experience are
needed to deliver supports safely to medically and behaviourally complex participants. This
was recognised by the Quality and Safeguarding Framework.
These changes will be easier to implement for smaller providers with defined customer
segments and new entrants into the market who focus on specific customer segments. Large
providers should also have sufficient scale in a geography to better design service models
around different participant segments, although the challenge and time taken for
transformation is not underestimated.

McKinsey & Company 102
Glossary and Abbreviations
TABLE 8:
Abbreviation Meaning
AMS Aboriginal Medical Services
ARIA Accessibility/Remoteness Index of Australia
Assistive Technology Any device or system using a device that allows individuals to perform tasks that would otherwise be more difficult, unsafe or not possible. It does not include items for treatment, mainstream technology without modifications.
ATSI Aboriginal and/or Torres Strait Islander
Attendant Care Refers to all supports which are either assistance with daily living or assistance with social and community participation.
Award Regulatory instrument which outlines the minimum pay rates and conditions of employment for a particular industry and/or occupation.
Board The corporate governing board of the National Disability Insurance Agency
CALD Culturally and linguistically diverse
CEO Chief Executive Officer of the National Disability Insurance Agency
COAG Council of Australian Governments
DIDO Drive-in, drive-out; refers to services provided by non-local workforces who are required to drive to/from a separate town or region.
DVA Department of Veterans Affairs
DSS, or ‘the Department’ The Commonwealth Department of Social Services
Eastern Price Guide NDIS Price Guide Victoria, New South Wales, Queensland Tasmania released by the NDIA, the latest of which is valid from 1 July 2017
EBA Enterprise Bargaining Agreement
ECEI Early Childhood Early Intervention [x]
NDIA Aspirations The three external aspirations of the NDIA as identified in its Corporate Plan 2016 – 2021: better participant outcomes, a growing market with innovative supports (‘market development’), and a financially sustainable scheme (‘Scheme sustainability’).
FIFO Fly-in, fly-out; refers to services provided by non-local workforces who are required to fly to/from a separate town or region.
FTE Full-time equivalent
Full Scheme Refers to the fully implemented state of the NDIS, estimated to operate from 2020.
FY Financial Year
IAC Independent Advisory Council
ICT Information and communication technology
IHPA Independent Hospital Pricing Authority
IPR Independent Pricing Review
IT Information Technology
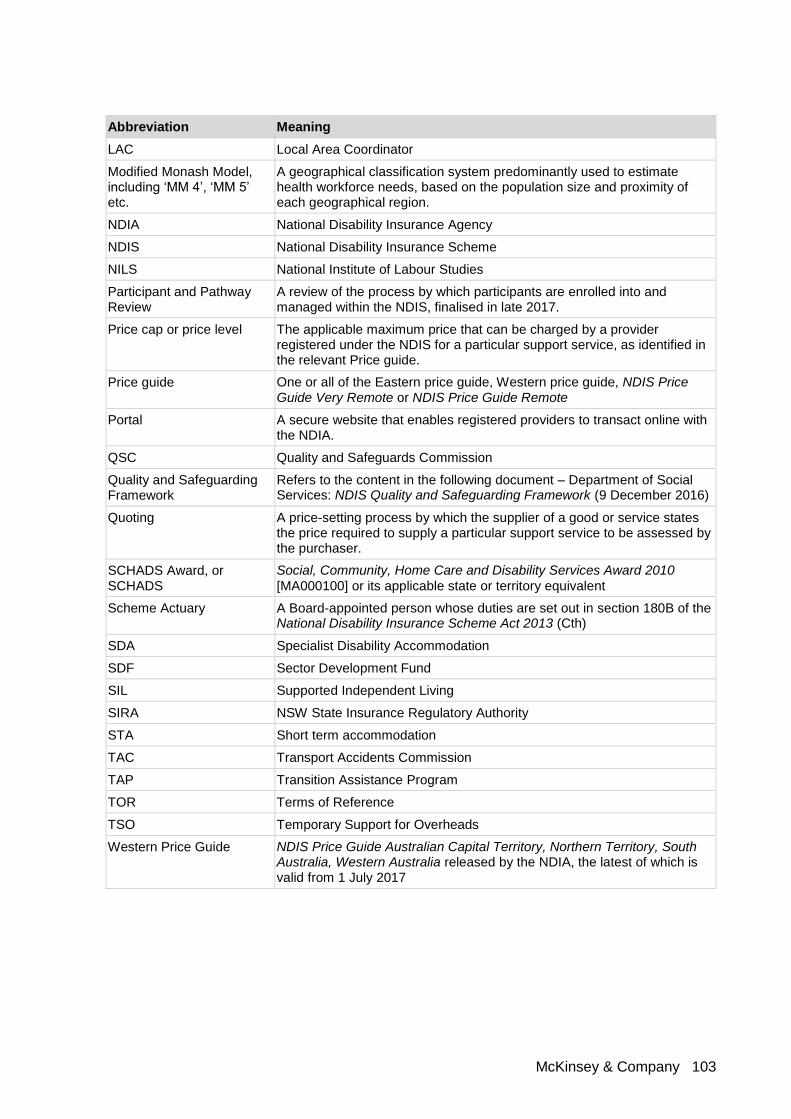
McKinsey & Company 103
Abbreviation Meaning
LAC Local Area Coordinator
Modified Monash Model, including ‘MM 4’, ‘MM 5’ etc.
A geographical classification system predominantly used to estimate health workforce needs, based on the population size and proximity of each geographical region.
NDIA National Disability Insurance Agency
NDIS National Disability Insurance Scheme
NILS National Institute of Labour Studies
Participant and Pathway Review
A review of the process by which participants are enrolled into and managed within the NDIS, finalised in late 2017.
Price cap or price level The applicable maximum price that can be charged by a provider registered under the NDIS for a particular support service, as identified in the relevant Price guide.
Price guide One or all of the Eastern price guide, Western price guide, NDIS Price Guide Very Remote or NDIS Price Guide Remote
Portal A secure website that enables registered providers to transact online with the NDIA.
QSC Quality and Safeguards Commission
Quality and Safeguarding Framework
Refers to the content in the following document – Department of Social Services: NDIS Quality and Safeguarding Framework (9 December 2016)
Quoting A price-setting process by which the supplier of a good or service states the price required to supply a particular support service to be assessed by the purchaser.
SCHADS Award, or SCHADS
Social, Community, Home Care and Disability Services Award 2010
[MA000100] or its applicable state or territory equivalent
Scheme Actuary A Board-appointed person whose duties are set out in section 180B of the National Disability Insurance Scheme Act 2013 (Cth)
SDA Specialist Disability Accommodation
SDF Sector Development Fund
SIL Supported Independent Living
SIRA NSW State Insurance Regulatory Authority
STA Short term accommodation
TAC Transport Accidents Commission
TAP Transition Assistance Program
TOR Terms of Reference
TSO Temporary Support for Overheads
Western Price Guide NDIS Price Guide Australian Capital Territory, Northern Territory, South Australia, Western Australia released by the NDIA, the latest of which is valid from 1 July 2017