Embed Size (px)
Citation preview

UnitedHealthcare respects the expertise of the physicians, health care professionals, and their staff who participate in our network. Our goal is to
support you and your patients in making the most informed decisions regarding the choice of quality and cost-effective care, and to support practice
staff with a simple and predictable administrative experience. The Policy Update Bulletin was developed to share important information regarding
Oxford® Medical and Administrative Policy.*
*Where information in this bulletin conflicts with applicable state and/or federal law, UnitedHealthcare follows such applicable federal and/or state law
May 2018
policy update bulletin Medical & Administrative Policy Updates

2 Oxford® Policy Update Bulletin: May 2018
Oxford® Medical and Administrative Policy Updates
Overview
Oxford
Tips for using the Policy Update Bulletin:
From the table of contents, click the policy title to be
directed to the corresponding policy update summary.
From the policy updates table, click the policy title to view a
complete copy of a new, updated, or revised policy.
Policy Update Classifications
New
New clinical coverage criteria and/or documentation review
requirements have been adopted for a health service (e.g., test, drug,
device or procedure)
Updated
An existing policy has been reviewed and changes have not been made
to the clinical coverage criteria or documentation review requirements;
however, items such as the clinical evidence, FDA information, and/or
list(s) of applicable codes may have been updated
Revised
An existing policy has been reviewed and revisions have been made to
the clinical coverage criteria and/or documentation review requirements
Replaced
An existing policy has been replaced with a new or different policy
Retired
The health service(s) addressed in the policy are no longer being
managed or are considered to be proven/medically necessary and are
therefore not excluded as unproven/not medically necessary services,
unless coverage guidelines or criteria are otherwise documented in
another policy
Note: The absence of a policy does not automatically indicate or imply
coverage. As always, coverage for a health service must be determined
in accordance with the member’s benefit plan and any applicable
federal or state regulatory requirements. Additionally, UnitedHealthcare
reserves the right to review the clinical evidence supporting the safety
and effectiveness of a medical technology prior to rendering a coverage
determination.
This bulletin provides complete details on Oxford® Clinical,
Administrative and Reimbursement Policy updates. The inclusion of
a health service (e.g., test, drug, device or procedure) in this
bulletin indicates only that UnitedHealthcare has recently adopted a
new policy and/or updated, revised, replaced or retired an existing
policy; it does not imply that Oxford® provides coverage for the
health service. In the event of an inconsistency or conflict between
the information provided in this bulletin and the posted policy, the
provisions of the posted policy will prevail. Note that most benefit
plan documents exclude from benefit coverage health services
identified as investigational or unproven/not medically necessary.
Physicians and other health care professionals may not seek or
collect payment from a member for services not covered by the
applicable benefit plan unless first obtaining the member’s written
consent, acknowledging that the service is not covered by the
benefit plan and that they will be billed directly for the service.
A complete library of Oxford® Medical and
Administrative Policies is available at
OxfordHealth.com > Providers > Tools & Resources >
Medical Information > Medical and Administrative Policies.

3 Oxford® Policy Update Bulletin: May 2018
Oxford® Medical and Administrative Policy Updates
In This Issue
Oxford
Clinical Policy Updates Page
NEW
Benlysta® (Belimumab) - Effective May 1, 2018 ................................................................................................................................................... 7 Crysvita® (Burosumab-Twza) - Effective May 1, 2018 ........................................................................................................................................... 7 Enzyme Replacement Therapy - Effective May 1, 2018 .......................................................................................................................................... 8
UPDATED
Chelation Therapy for Non-Overload Conditions - Effective May 1, 2018 ................................................................................................................ 14 Cochlear Implants - Effective Jun. 1, 2018 ......................................................................................................................................................... 14 Computerized Dynamic Posturography - Effective May 1, 2018 ............................................................................................................................. 15 Deep Brain and Cortical Stimulation - Effective May 1, 2018 ................................................................................................................................ 15 Embolization of the Ovarian and Iliac Veins for Pelvic Congestion Syndrome - Effective May 1, 2018 ......................................................................... 15 Infertility Diagnosis and Treatment - Effective Jun. 1, 2018 ................................................................................................................................. 15 Injectable Chemotherapy Drugs: Application of NCCN Clinical Practice Guidelines - Effective Jun. 1, 2018 ................................................................. 15 Otoacoustic Emissions Testing - Effective Jun. 1, 2018 ........................................................................................................................................ 15 Site of Service Guidelines for Certain Outpatient Surgical Procedures - Effective May 1, 2018 .................................................................................. 16 Thermography - Effective May 1, 2018 .............................................................................................................................................................. 16 Vaccines - Effective May 1, 2018 ...................................................................................................................................................................... 16
REVISED
Ablative Treatment for Spinal Pain - Effective Jun. 1, 2018 .................................................................................................................................. 16 Actemra® (Tocilizumab) Injection for Intravenous Infusion - Effective Jun. 1, 2018 ................................................................................................ 18 Benlysta® (Belimumab) - Effective Aug. 1, 2018 ................................................................................................................................................. 20 Chromosome Microarray Testing (Non-Oncology Conditions) - Effective Jun. 1, 2018 .............................................................................................. 21 Drug Coverage Criteria - New and Therapeutic Equivalent Medications - Effective Jun. 1, 2018 ................................................................................ 24 Drug Coverage Guidelines - Effective May 1, 2018 .............................................................................................................................................. 24
o Adagen (Pegademase Bovine) .................................................................................................................................................................... 24 o Aldurazyme® (Laronidase) ......................................................................................................................................................................... 24 o Benlysta (Belimumab) ............................................................................................................................................................................... 24 o Crysvita (Burosumab-Twza) ....................................................................................................................................................................... 25 o Elaprase (Idursulfase) ............................................................................................................................................................................... 25 o Fabrazyme® (Agalsidase Beta) .................................................................................................................................................................... 25 o Kanuma (Sebelipase Alfa) .......................................................................................................................................................................... 26 o Lumizyme (Alglucosidase Alfa) .................................................................................................................................................................... 26 o Mepsevii (Vestronidase Alfa-Vjbk) ............................................................................................................................................................... 26 o Naglazyme (Galsulfase) ............................................................................................................................................................................. 26

4 Oxford® Policy Update Bulletin: May 2018
Oxford® Medical and Administrative Policy Updates
In This Issue
Oxford
o Vimizim (Elosulfase Alfa) ............................................................................................................................................................................ 26 Drug Coverage Guidelines - Effective Jun. 1, 2018 .............................................................................................................................................. 26
o Actemra (Tocilizumab) ............................................................................................................................................................................... 26 o Actiq (Brand Only) (Fentanyl Citrate) .......................................................................................................................................................... 26 o Afstyla (Antihemophilic Factor [Recombinant] Single Chain) ........................................................................................................................... 26 o Atorvastatin (Generic Lipitor) 10mg, 20mg................................................................................................................................................... 26 o Belsomra (Suvorexant) .............................................................................................................................................................................. 26 o Benznidazole ............................................................................................................................................................................................ 26 o Bupropion (SR) (Generic Zyban) ................................................................................................................................................................. 27 o Carospir Suspension (Spironolactone).......................................................................................................................................................... 27 o Chantix (Varenicline Tartrate) ..................................................................................................................................................................... 27 o Cimduo (Lamivudine/Tenofovir DF) ............................................................................................................................................................. 27 o Cimzia (Certolizumab Pegol) ....................................................................................................................................................................... 27 o Cosentyx (Secukinumab) ........................................................................................................................................................................... 27 o Daraprim (Pyrimethamine) ......................................................................................................................................................................... 27 o Enbrel (Etanercept) ................................................................................................................................................................................... 27 o Ergomar (Ergotamine Tartrate) ................................................................................................................................................................... 27 o Farydak (Panobinostat) .............................................................................................................................................................................. 27 o Fentanyl Citrate (Generic Actiq) .................................................................................................................................................................. 27 o Grastek (Timothy Grass Pollen Allergen Extract) ........................................................................................................................................... 28 o Jakafi (Ruxolitinib) .................................................................................................................................................................................... 28 o Kineret (Anakinra) .................................................................................................................................................................................... 28 o Korlym (Mifepristone) ................................................................................................................................................................................ 28 o Lidocaine Patch ......................................................................................................................................................................................... 28 o Lemtrada (Alemtuzumab) .......................................................................................................................................................................... 28 o Linzess (Linaclotide) .................................................................................................................................................................................. 28 o Lynparza (Olaparib) .................................................................................................................................................................................. 28 o Lyrica CR (Pregabalin) ............................................................................................................................................................................... 28 o Mekinist (Trametinib) ................................................................................................................................................................................ 28 o Migranal (Dihydro-Ergotamine) (Brand) ....................................................................................................................................................... 28 o Migranal (Dihydro-Ergotamine) (Generic) ..................................................................................................................................................... 28 o Movantik (Naloxegol)................................................................................................................................................................................. 28 o Nicotine OTC Products ............................................................................................................................................................................... 28 o Ninlaro (Ixazomib) .................................................................................................................................................................................... 28 o Odactra (House Dust Mite Allergen Extract) .................................................................................................................................................. 29 o Oralair (Sweet Vernal, Orchard, Perennial Rye, Timothy and Kentucky Blue Grass, Mixed Pollens Allergen Extract) ............................................... 29 o Prolia, Xgeva (Denosumab) ........................................................................................................................................................................ 29 o Radicava (Edaravone)................................................................................................................................................................................ 29 o Ragwitek (Short Ragweed Pollen Allergen Extract) ........................................................................................................................................ 29 o Rexulti (Brexpiprazole) .............................................................................................................................................................................. 29

5 Oxford® Policy Update Bulletin: May 2018
Oxford® Medical and Administrative Policy Updates
In This Issue
Oxford
o Rhopressa (Netarsudil) .............................................................................................................................................................................. 29 o Rozerem (Ramelteon) ................................................................................................................................................................................ 29 o Simponi (Golimumab) ................................................................................................................................................................................ 29 o Simponi Aria (Golimumab) ......................................................................................................................................................................... 29 o Simvastatin (Generic Zocor) 5mg, 10mg, 20mg, 40mg .................................................................................................................................. 29 o Sutent (Sunitinib) ..................................................................................................................................................................................... 30 o Symfi (Efavirenz/Lamivudine/Tenofovir Disoproxil Fumarate) ......................................................................................................................... 30 o Smyfi Lo (Efavirenz/Lamivudine/Tenofovir Disoproxil Fumarate) ..................................................................................................................... 30 o Symproic (Naldemedine) ............................................................................................................................................................................ 30 o Tafinlar (Dabrafenib) ................................................................................................................................................................................. 30 o Tamiflu Capsules (Brand Only) (Oseltamivir Phosphate) ................................................................................................................................. 30 o Test Strips and Meters (Diabetic) ................................................................................................................................................................ 30 o Trulance (Plecanatide) ............................................................................................................................................................................... 30 o Viberzi (Eluxadoline) ................................................................................................................................................................................. 30 o Vyzulta (Latanoprostene Bunod) ................................................................................................................................................................. 30 o Zelboraf (Vemurafenib) ............................................................................................................................................................................. 30 o Zolpimist (Zolpidem Tartrate) ..................................................................................................................................................................... 30 o Zypitamag (Pitavastatin) ............................................................................................................................................................................ 30
Electrical Stimulation for the Treatment of Pain and Muscle Rehabilitation - Effective Jun. 1, 2018 ............................................................................ 31 Entyvio® (Vedolizumab) - Effective Jun. 1, 2018 ................................................................................................................................................. 34 Enzyme Replacement Therapy - Effective Aug. 1, 2018 ....................................................................................................................................... 35 Exondys 51™ (Eteplirsen) - Effective Jun. 1, 2018 .............................................................................................................................................. 43 Ilaris® (Canakinumab) - Effective Jun. 1, 2018 ................................................................................................................................................... 44 Infliximab (Remicade®, Inflectra™, Renflexis™) - Effective Jun. 1, 2018 ................................................................................................................ 47 Ocrevus™ (Ocrelizumab) - Effective Jun. 1, 2018 ............................................................................................................................................... 50 Orencia® (Abatacept) Injection for Intravenous Infusion - Effective Jun. 1, 2018 .................................................................................................... 53 Preventive Care Services - Effective Jun. 1, 2018 ............................................................................................................................................... 55 Radicava™ (Edaravone) - Effective Jun. 1, 2018 ................................................................................................................................................. 59 Radiology Procedures Requiring Precertification for eviCore healthcare Arrangement - Effective Jun. 1, 2018 ............................................................. 59 Simponi Aria® (Golimumab) Injection for Intravenous Infusion - Effective Jun. 1, 2018 ........................................................................................... 60
Administrative Policy Updates
NEW
New York & Connecticut Participating Surgeons Using Non- Participating Providers for Intraoperative Neuro-Monitoring (IONM) - Effective Jun. 1, 2018 62
UPDATED
Accreditation Requirements for Radiology Services - Effective May 1, 2018 ............................................................................................................ 64

6 Oxford® Policy Update Bulletin: May 2018
Oxford® Medical and Administrative Policy Updates
In This Issue
Oxford
REVISED
Ambulance Services - Effective Jun. 1, 2018 ...................................................................................................................................................... 65
Reimbursement Policy Updates
UPDATED
Maximum Frequency Per Day - Effective May 7, 2018 ......................................................................................................................................... 69 Services and Modifiers Not Reimbursable to Healthcare Professionals - Effective May 7, 2018 .................................................................................. 69
7 Oxford® Policy Update Bulletin: May 2018
Clinical Policy Updates
Oxford
Policy Title Effective Date Coverage Rationale
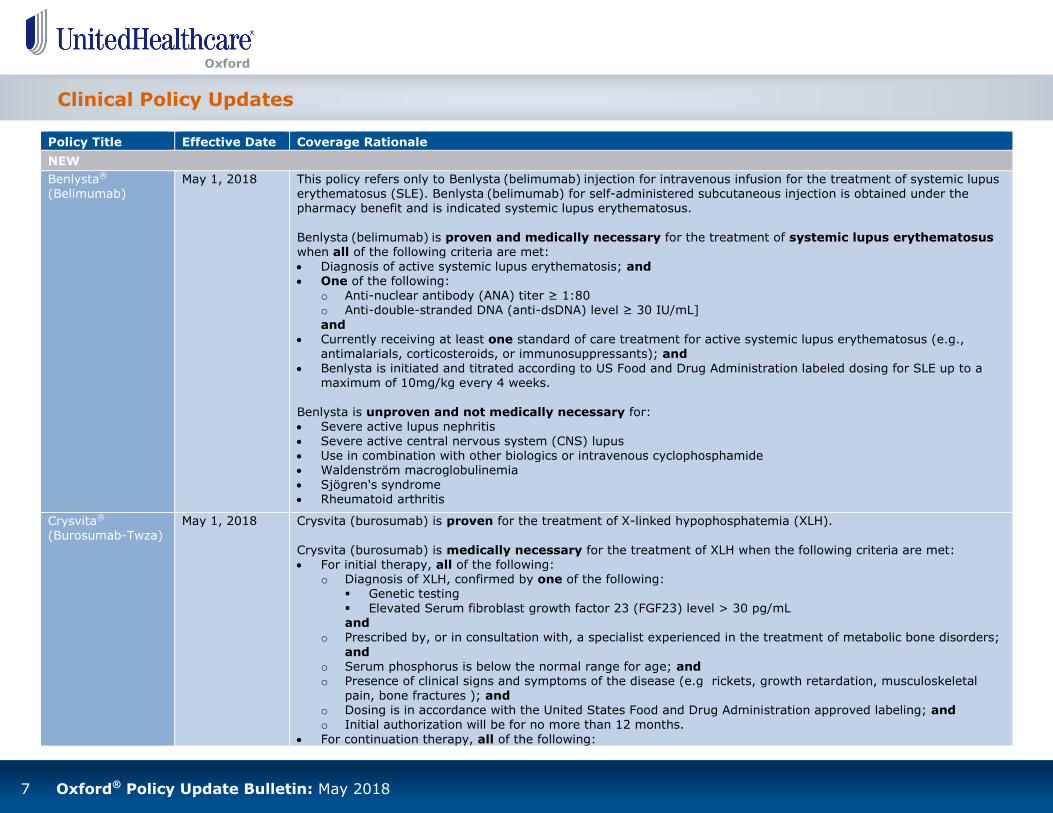
NEW
Benlysta® (Belimumab)
May 1, 2018 This policy refers only to Benlysta (belimumab) injection for intravenous infusion for the treatment of systemic lupus erythematosus (SLE). Benlysta (belimumab) for self-administered subcutaneous injection is obtained under the pharmacy benefit and is indicated systemic lupus erythematosus.
Benlysta (belimumab) is proven and medically necessary for the treatment of systemic lupus erythematosus when all of the following criteria are met:
Diagnosis of active systemic lupus erythematosis; and One of the following:
o Anti-nuclear antibody (ANA) titer ≥ 1:80 o Anti-double-stranded DNA (anti-dsDNA) level ≥ 30 IU/mL]
and Currently receiving at least one standard of care treatment for active systemic lupus erythematosus (e.g.,
antimalarials, corticosteroids, or immunosuppressants); and Benlysta is initiated and titrated according to US Food and Drug Administration labeled dosing for SLE up to a
maximum of 10mg/kg every 4 weeks.
Benlysta is unproven and not medically necessary for: Severe active lupus nephritis
Severe active central nervous system (CNS) lupus Use in combination with other biologics or intravenous cyclophosphamide Waldenström macroglobulinemia Sjögren's syndrome Rheumatoid arthritis
Crysvita® (Burosumab-Twza)
May 1, 2018
Crysvita (burosumab) is proven for the treatment of X-linked hypophosphatemia (XLH).
Crysvita (burosumab) is medically necessary for the treatment of XLH when the following criteria are met:
For initial therapy, all of the following: o Diagnosis of XLH, confirmed by one of the following:
Genetic testing
Elevated Serum fibroblast growth factor 23 (FGF23) level > 30 pg/mL and
o Prescribed by, or in consultation with, a specialist experienced in the treatment of metabolic bone disorders;
and o Serum phosphorus is below the normal range for age; and o Presence of clinical signs and symptoms of the disease (e.g rickets, growth retardation, musculoskeletal
pain, bone fractures ); and o Dosing is in accordance with the United States Food and Drug Administration approved labeling; and o Initial authorization will be for no more than 12 months.
For continuation therapy, all of the following:

8 Oxford® Policy Update Bulletin: May 2018
Clinical Policy Updates
Oxford
Policy Title Effective Date Coverage Rationale
NEW
Crysvita® (Burosumab-Twza) (continued)
May 1, 2018 o Patient has previously received treatment with burosumab; and o Prescribed by, or in consultation with, a specialist experienced in the treatment of metabolic bone disorders;
and
o Patient has experienced normalization of serum phosphate while on therapy; and o Patient has experienced a positive clinical response to burosumab (e.g., enhanced height velocity,
improvement in skeletal deformities, reduction of fractures, reduction of generalized bone pain); and
o Dosing is in accordance with the United States Food and Drug Administration approved labeling; and o Reauthorization will be for no more than 12 months.
Enzyme Replacement Therapy
May 1, 2018
This policy refers to the following enzyme replacement therapy products: Adagen (pegademase bovine) Aldurazyme (laronidase) Elaprase (idursulfase)
Fabrazyme (agalsidase beta) Kanuma (sebelipase alfa) Lumizyme (alglucosidase alfa) Mepsevii (vestronidase alfa-vjbk) Naglazyme (galsulfase)
Vimizim (elosulfase alfa)
Adagen (pegademase bovine) is medically necessary for the treatment of severe combined immunodeficiency disease (SCID) associated with a deficiency of adenosine deaminase (ADA) when the following criteria are met: For initial therapy, all of the following:
o Diagnosis of SCID; and o Deficiency of adenosine deaminase is confirmed by any of the following:
Deficiency or absence of ADA in plasma, lysed erythrocytes, fibroblasts (cultured from amniotic fluid), or chorionic villus
Increase in deoxyadenosine triphosphate (dATP) levels in erythrocyte lysates compared to laboratory standard
Decrease in ATP concentration in erythrocytes Molecular genetic confirmation of mutations in both alleles of the ADA1 gene Positive screening by T cell receptor excision circles (TRECs);
and o One of the following:
Patient is not a suitable candidate for hematopoietic cell transplantation (HCT) Patient has failed HCT; and
o Dosing is in accordance with the United States Food and Drug Administration approved labeling: dosing is
started at 10 U/kg for the first dose, and titrated up to a maximum dose of 30 U/kg per week; and

9 Oxford® Policy Update Bulletin: May 2018
Clinical Policy Updates
Oxford
Policy Title Effective Date Coverage Rationale
NEW
Enzyme Replacement Therapy
(continued)
May 1, 2018
o Initial authorization will be for no more than 12 months. For continuation therapy, all of the following:
o Patient has previously received treatment with pegademase therapy; and
o Patient has experienced a positive clinical response to pegademase therapy (e.g., normalization of plasma ADA activity, erythrocyte dATP levels, improvement of disease symptoms, etc.); and
o Dosing is in accordance with the United States Food and Drug Administration approved labeling: appropriate
maintenance dosing, up to a maximum dose of 30 U/kg per week; and o Reauthorization will be for no more than 12 months.
Aldurazyme (laronidase) is medically necessary for the treatment of Mucopolysaccharidosis I (MPS I)
when the following criteria are met: For initial therapy, all of the following:
o Diagnosis of any of the MPS I syndromes confirmed by one the following: Hurler variant (severe mucopolysaccharidosis I; also MPS IH) Hurler-Scheie variant (attenuated mucopolysaccharidosis I; also MPS IHS) Scheie variant (attenuated mucopolysaccharidosis I; also MPS IS);
and o Diagnosis of MPS I is confirmed by either of the following:
Deficiency or absence of fibroblast or leukocyte enzyme activity of alpha-L-iduronidase enzyme activity Molecular genetic confirmation of mutations in the alpha-L-iduronidase gene; and
o Presence of clinical signs and symptoms of the disease (e.g., asymptomatic with affected older sibling, cardiac abnormalities, corneal clouding, dysostosis multiplex, hepatomegaly, restrictive lung disease, etc.);
and o Dosing is in accordance with the United States Food and Drug Administration approved labeling:
Administered dose does not exceed 0.58 mg/kg intravenously once every week; and o Initial authorization will be for no more than 12 months.
For continuation therapy, all of the following: o Patient has previously received treatment with laronidase therapy; and
o Patient has experienced a positive clinical response to laronidase therapy (e.g., improved endurance,
improved functional capacity, reduced urine dermatan sulfate/heparan sulfate excretion, etc.); and o Dosing is in accordance with the United States Food and Drug Administration approved labeling:
administered dose does not exceed 0.58 mg/kg intravenously once every week; and o Reauthorization will be for no more than 12 months.
Elaprase (idursulfase) is medically necessary for the treatment of Mucopolysaccharidosis II (MPS II,
Hunter Syndrome) when the following criteria are met: For initial therapy, all of the following:
o Diagnosis of MPS II confirmed by one the following:

10 Oxford® Policy Update Bulletin: May 2018
Clinical Policy Updates
Oxford
Policy Title Effective Date Coverage Rationale
NEW
Enzyme Replacement Therapy
(continued)
May 1, 2018
Deficiency in iduronate 2-sulfatase enzyme activity as measured in fibroblasts or leukocytes combined with normal enzyme activity level of another sulfatase
Molecular genetic testing for deletion or mutations in the iduronate 2-sulfatase gene;
and o Presence of clinical signs and symptoms of the disease (e.g., hepatosplenomegaly, skeletal deformities,
dysostosis, neurocognitive decline, cardiovascular disorders, etc.); and
o Dosing is in accordance with the United States Food and Drug Administration approved labeling: administered dose does not exceed 0.5 mg/kg intravenously once every week; and
o Initial authorization will be for no more than 12 months. For continuation therapy, all of the following:
o Patient has previously received treatment with idursulfase therapy; and o Patient has experienced a positive clinical response to idursulfase therapy (e.g., improved endurance,
improved functional capacity, reduced spleen volume, reduced urine GAG excretion, etc.); and o Dosing is in accordance with the United States Food and Drug Administration approved labeling:
administered dose does not exceed 0.5 mg/kg intravenously once every week; and o Reauthorization will be for no more than 12 months.
Fabrazyme (agalsidase beta) is medically necessary for the treatment of Fabry disease when the
following criteria are met: For initial therapy, all of the following:
o Diagnosis of Fabry disease as confirmed by one the following: Absence or deficiency (< 5% of mean) of normal alpha-galactosidase A (α-Gal A) enzyme activity) in
leukocytes, dried blood spots, or serum analysis
Molecular genetic testing for deletion or mutations in the galactosidase alpha gene; and
o Presence of clinical signs and symptoms of the disease (e.g., Acroparesthesias, angiokeratomas, whorls, anhidrosis/hypohidrosis, renal disease, exercise/heat/cold intolerance, etc.); and
o Dosing is in accordance with the United States Food and Drug Administration approved labeling: administered dose does not exceed 1 mg/kg intravenously every two weeks; and
o Initial authorization will be for no more than 12 months.
For continuation therapy, all of the following: o Patient has previously received treatment with agalsidase therapy; and o Patient has experienced a positive clinical response to agalsidase therapy (e.g., improved renal function,
reduction in mean plasma GL-3 levels, decreased GL-3 inclusions, etc.); and o Dosing is in accordance with the United States Food and Drug Administration approved labeling:
administered dose does not exceed 1 mg/kg intravenously every two weeks; and
o Reauthorization will be for no more than 12 months.
Kanuma (sebelipase alfa) is medically necessary for the treatment of Lysosomal acid lipase deficiency

11 Oxford® Policy Update Bulletin: May 2018
Clinical Policy Updates
Oxford
Policy Title Effective Date Coverage Rationale
NEW
Enzyme Replacement Therapy
(continued)
May 1, 2018
[LAL-D, Wolman disease (WD), cholesteryl ester disease (CESD)] when the following criteria are met: For initial therapy, all of the following:
o Diagnosis of lysosomal acid lipase deficiency [LAL-D, Wolman disease (WD), cholesteryl ester disease
(CESD)] as confirmed by one the following: Absence or deficiency lysosomal acid lipase activity by dried blood spot test Molecular genetic testing for deletion or mutations in the lipase A, lysosomal acid type (LIPA) gene;
and o Presence of clinical signs and symptoms of the disease (e.g., abdominal distention, hepatosplenomegaly,
liver fibrosis, ascities, etc.); and o Dosing is in accordance with the United States Food and Drug Administration approved labeling by one of
the following: For rapidly progressive disease presenting within the first 6 months of life: administered initial starting
dose is 1 mg/kg intravenously once weekly, up to a maximum of 3 mg/kg once weekly Pediatric and adult patients with disease: administered dose does not exceed 1 mg/kg intravenously
every other week; and
o Initial authorization will be for no more than 12 months. For continuation therapy, all of the following:
o Patient has previously received treatment with sebelipase therapy; and o Patient has experienced a positive clinical response to sebelipase therapy [e.g., improved disease symptoms,
improvement of laboratory values (LFTs, cholesterol, triglycerides), etc.]; and o Dosing is in accordance with the United States Food and Drug Administration approved labeling by one of
the following:
For rapidly progressive disease presenting within the first 6 months of life: administered dose is 1 mg/kg intravenously once weekly, up to a maximum of 3 mg/kg once weekly
Pediatric and adult patients with disease: administered dose does not exceed 1 mg/kg intravenously every other week;
and o Reauthorization will be for no more than 12 months.
Lumizyme (alglucosidase alfa) is medically necessary for the treatment of Pompe disease when the following criteria are met: For initial therapy, one of the following:
o All of the following for infantile-onset Pompe disease: Diagnosis of infantile-onset Pompe disease as confirmed by one the following:
- Absence or deficiency (<1% of the lab specific normal mean) acid alpha-glucosidase deficiency
(GAA) activity in skin fibroblasts - Molecular genetic testing for deletion or mutations in the GAA gene; and
12 Oxford® Policy Update Bulletin: May 2018
Clinical Policy Updates
Oxford
Policy Title Effective Date Coverage Rationale
NEW
Enzyme Replacement Therapy
(continued)
May 1, 2018
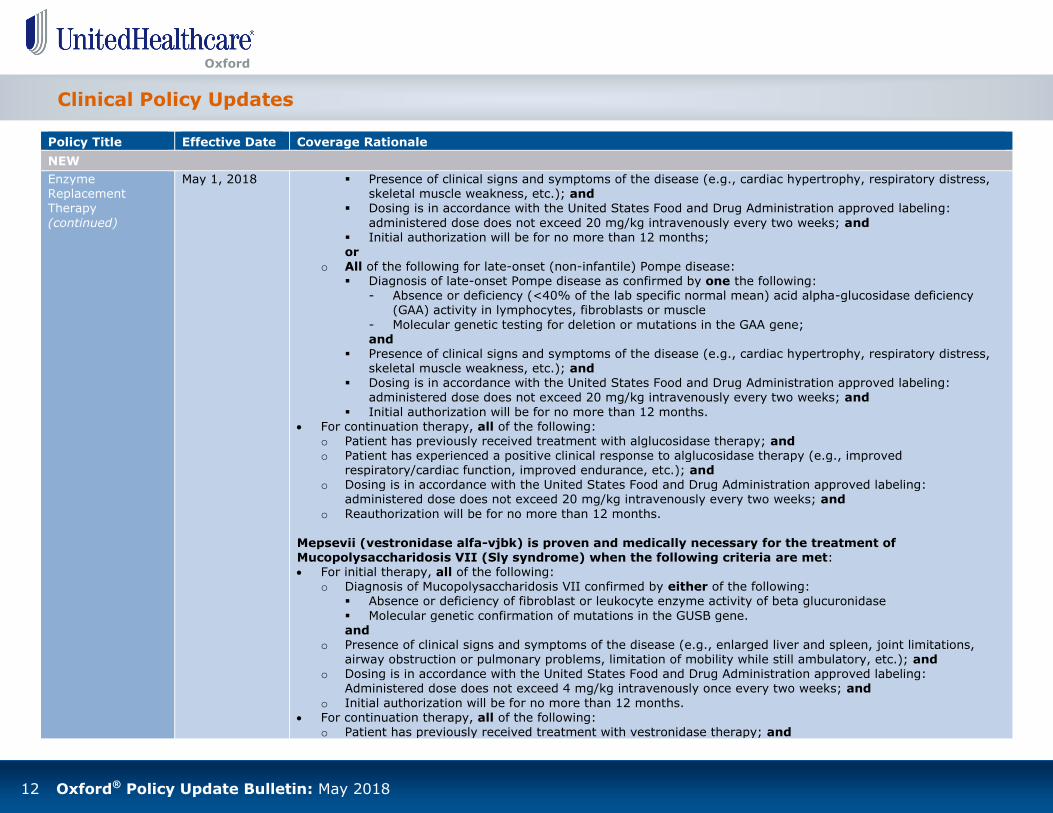
Presence of clinical signs and symptoms of the disease (e.g., cardiac hypertrophy, respiratory distress, skeletal muscle weakness, etc.); and
Dosing is in accordance with the United States Food and Drug Administration approved labeling:
administered dose does not exceed 20 mg/kg intravenously every two weeks; and Initial authorization will be for no more than 12 months; or
o All of the following for late-onset (non-infantile) Pompe disease: Diagnosis of late-onset Pompe disease as confirmed by one the following:
- Absence or deficiency (<40% of the lab specific normal mean) acid alpha-glucosidase deficiency (GAA) activity in lymphocytes, fibroblasts or muscle
- Molecular genetic testing for deletion or mutations in the GAA gene; and
Presence of clinical signs and symptoms of the disease (e.g., cardiac hypertrophy, respiratory distress, skeletal muscle weakness, etc.); and
Dosing is in accordance with the United States Food and Drug Administration approved labeling: administered dose does not exceed 20 mg/kg intravenously every two weeks; and
Initial authorization will be for no more than 12 months. For continuation therapy, all of the following:
o Patient has previously received treatment with alglucosidase therapy; and o Patient has experienced a positive clinical response to alglucosidase therapy (e.g., improved
respiratory/cardiac function, improved endurance, etc.); and o Dosing is in accordance with the United States Food and Drug Administration approved labeling:
administered dose does not exceed 20 mg/kg intravenously every two weeks; and
o Reauthorization will be for no more than 12 months. Mepsevii (vestronidase alfa-vjbk) is proven and medically necessary for the treatment of Mucopolysaccharidosis VII (Sly syndrome) when the following criteria are met: For initial therapy, all of the following:
o Diagnosis of Mucopolysaccharidosis VII confirmed by either of the following:
Absence or deficiency of fibroblast or leukocyte enzyme activity of beta glucuronidase
Molecular genetic confirmation of mutations in the GUSB gene. and
o Presence of clinical signs and symptoms of the disease (e.g., enlarged liver and spleen, joint limitations, airway obstruction or pulmonary problems, limitation of mobility while still ambulatory, etc.); and
o Dosing is in accordance with the United States Food and Drug Administration approved labeling: Administered dose does not exceed 4 mg/kg intravenously once every two weeks; and
o Initial authorization will be for no more than 12 months. For continuation therapy, all of the following:
o Patient has previously received treatment with vestronidase therapy; and

13 Oxford® Policy Update Bulletin: May 2018
Clinical Policy Updates
Oxford
Policy Title Effective Date Coverage Rationale
NEW
Enzyme Replacement Therapy
(continued)
May 1, 2018
o Patient has experienced a positive clinical response to vestronidase therapy (e.g., improved endurance, improved functional capacity, improved pulmonary function, etc.); and
o Dosing is in accordance with the United States Food and Drug Administration approved labeling:
Administered dose does not exceed 4 mg/kg intravenously once every two weeks; and o Reauthorization will be for no more than 12 months.
Naglazyme (galsulfase) is medically necessary for the treatment of Mucopolysaccharidosis VI (Maroteaux-Lamy syndrome) when the following criteria are met: For initial therapy, all of the following:
o Diagnosis of Mucopolysaccharidosis VI confirmed by either of the following:
Absence or deficiency of fibroblast or leukocyte enzyme activity of N-acetylgalactosamine 4-sulfatase (arylsulfatase)
Molecular genetic confirmation of mutations in the ASB gene (5q13-q14); and
o Presence of clinical signs and symptoms of the disease (e.g., kyphoscoliosis, genu valgum, pectus carinatum, gait disturbance, growth deficiency, etc.); and
o Dosing is in accordance with the United States Food and Drug Administration approved labeling: administered dose does not exceed 1 mg/kg intravenously once every week; and
o Initial authorization will be for no more than 12 months. For continuation therapy, all of the following:
o Patient has previously received treatment with galsulfase therapy; and o Patient has experienced a positive clinical response to galsulfase therapy (e.g., improved endurance,
improved functional capacity, reduced urine dermatan sulfate excretion, etc.); and
o Dosing is in accordance with the United States Food and Drug Administration approved labeling: administered dose does not exceed 1 mg/kg intravenously once every week; and
o Reauthorization will be for no more than 12 months. Vimizim (elosulfase alfa) is medically necessary for the treatment of Mucopolysaccharidosis type IVA (MPS IVA; Morquio A syndrome) when the following criteria are met:
For initial therapy, all of the following:
o Diagnosis of Morquio A syndrome confirmed by either of the following: Absence or deficiency of fibroblast or leukocyte GALNS enzyme activity Molecular genetic testing for mutations in the GALNS gene (16q24.3); and
o Presence of clinical signs and symptoms of the disease (e.g., kyphoscoliosis, genu valgum, pectus carinatum, gait disturbance, growth deficiency, etc.); and
o Dosing is in accordance with the United States Food and Drug Administration approved labeling: administered dose does not exceed 2 mg/kg IV once every week; and
o Initial authorization will be for no more than 12 months.

14 Oxford® Policy Update Bulletin: May 2018
Clinical Policy Updates
Oxford
Policy Title Effective Date Coverage Rationale
NEW
Enzyme Replacement Therapy
(continued)
May 1, 2018 For continuation therapy, all of the following: o Patient has previously received treatment with elosulfase alfa therapy; and o Patient has experienced a positive clinical response to elosulfase alfa therapy (e.g., improved endurance,
improved functional capacity, reduced urine keratan sulfate excretion); and o Dosing is in accordance with the United States Food and Drug Administration approved labeling:
administered dose does not exceed 2 mg/kg IV once every week; and
o Reauthorization will be for no more than 12 months.
Policy Title Effective Date Summary of Changes
UPDATED
Chelation Therapy
for Non-Overload Conditions
May 1, 2018 Updated coverage rationale; replaced language indicating:
o “[The listed service] is proven and medically necessary” with “[the listed service] is proven and/or medically necessary”
o “[The listed services] are unproven and not medically necessary” with “[the listed services] are unproven and/or not medically necessary”
Updated supporting information to reflect the most current description of services, clinical evidence, and references
Cochlear Implants Jun. 1, 2018 Replaced references to “patient” with “individual” Updated benefit considerations:
o Replaced reference to “Covered Health Service” with “Covered Health Care Service”
o Replaced language indicating “cochlear implant monitoring (remapping and reprogramming of implant) and rehabilitation following the cochlear implant surgery is usually billed as aural rehabilitation and is not covered as a speech therapy benefit” with “cochlear implant monitoring (remapping and reprogramming of implant) and rehabilitation following the cochlear implant surgery is usually billed as aural rehabilitation and is covered as an outpatient rehabilitation therapy benefit”
Updated coverage rationale; replaced language indicating: o “[The listed service] is proven and medically necessary” with “[the listed service] is proven and/or medically
necessary”
o “[The listed service] is unproven and not medically necessary” with “[the listed service] is unproven and/or not medically necessary”
o “There is insufficient high quality evidence in the published clinical literature demonstrating the safety and efficacy of cochlear hybrid implants in the management of individuals with severe hearing loss” with “there is insufficient high quality evidence in the published clinical literature demonstrating the efficacy of cochlear
hybrid implants in the management of individuals with severe hearing loss” Updated list of applicable HCPCS codes:
o Added V5273 o Removed L8621, L8622, L8623, L8624, and L8629
Updated supporting information to reflect the most current clinical evidence and references

15 Oxford® Policy Update Bulletin: May 2018
Clinical Policy Updates
Oxford
Policy Title Effective Date Summary of Changes
UPDATED
Computerized Dynamic Posturography
May 1, 2018 Updated non-coverage rationale; replaced language indicating “[the listed service] is unproven and not medically necessary” with “[the listed service] is unproven and/or not medically necessary”
Updated supporting information to reflect the most current clinical evidence and references
Deep Brain and Cortical Stimulation
May 1, 2018 Updated coverage rationale: o Replaced references to:
“Patients” with “individuals” “Patient population” with “population” or “study population” “Patient selection criteria” with “selection criteria”
o Replaced language indicating: “[The listed services] are proven and medically necessary” with “[the listed services] are proven and/or
medically necessary” “[The listed services] are unproven and not medically necessary” with “[the listed services] are unproven
and/or not medically necessary” o Removed reference to specific directional deep brain stimulation device/product name (Infinity™ DBS
System) o Added reference link to the U.S. Food and Drug Administration (FDA) section of the policy for information
regarding directional deep brain stimulation devices
Updated supporting information to reflect the most current clinical evidence and FDA information
Embolization of the Ovarian and Iliac Veins for Pelvic Congestion Syndrome
May 1, 2018 Updated non-coverage rationale; replaced language indicating “[the listed service] is unproven and not medically necessary” with “[the listed service] is unproven and/or not medically necessary”
Updated supporting information to reflect the most current description of services, clinical evidence, and references
Infertility Diagnosis and Treatment
Jun. 1, 2018 Added definition of: o Preimplantation Genetic Diagnosis (PGD) o Preimplantation Genetic Screening (PGS)
Updated supporting information to reflect the most current references
Injectable Chemotherapy Drugs: Application
of NCCN Clinical Practice Guidelines
Jun. 1, 2018 Updated list of applicable HCPCS codes: o Added J0202 o Removed J9010
Otoacoustic Emissions Testing
Jun. 1, 2018
Updated list of related policies; added reference link to the policy titled Preventive Care Services Updated coverage rationale
o Replaced language indicating:
“[The listed service] is proven and medically necessary” with “[the listed service] is proven and/or

16 Oxford® Policy Update Bulletin: May 2018
Clinical Policy Updates
Oxford
Policy Title Effective Date Summary of Changes
UPDATED
Otoacoustic Emissions Testing (continued)
Jun. 1, 2018 medically necessary” “[The listed services] are not proven and medically necessary” with “[the listed services] are unproven
and/or not medically necessary”
o Replaced reference(s)to: “Patients” with “individuals” “Patient populations” with “populations”
Updated list of applicable ICD-10 diagnosis codes; added F44.6, F68.10, F68.12, F68.13, H91.01, H91.02, H91.03, and H91.09
Updated supporting information to reflect the most current description of services, clinical evidence, and references
Site of Service Guidelines for Certain Outpatient Surgical Procedures
May 1, 2018 Updated supporting information to reflect the most current references; no change to coverage rationale or list of applicable codes
Thermography May 1, 2018 Updated non-coverage rationale; replaced language indicating “[the listed service] is unproven or not medically necessary” with “[the listed service] is unproven and/or not medically necessary”
Updated list of applicable CPT codes: o Modified table heading; removed descriptor classifying codes as “non-reimbursable”
Updated supporting information to reflect the most current clinical evidence, FDA information, and references
Vaccines May 1, 2018 Updated coverage rationale; replaced reference to “ACIP definitive (‘shall’) recommendation” with “ACIP definitive (e.g., should, shall, is) recommendation”
Updated supporting information to reflect the most current references
Policy Title Effective Date Summary of Changes Coverage Rationale
REVISED
Ablative Treatment for Spinal Pain
Jun. 1, 2018
Updated list of related policies; added reference link to the
policy titled Office Based Program
Revised conditions of coverage/precertification
requirements; replaced language indicating “pulsed radiofrequency ablation (unlisted CPT code 64999) requires Medical Director review in all sites of service” with “CPT codes 64633, 64635,
Thermal radiofrequency ablation of facet joint nerves is proven and medically necessary for chronic cervical, (C3-4 and below), thoracic
and lumbar pain when confirmed by: Positive response to medial branch block at the side and level of the
proposed ablation Confirmation of needle placement by fluoroscopic guided imaging
Operative notes document: o Temperature 60 degrees celsius or more o Duration of ablation at least 40 seconds
A repeat thermal radiofrequency ablation of the same facet joint nerves is proven and medically necessary when:

17 Oxford® Policy Update Bulletin: May 2018
Clinical Policy Updates
Oxford
Policy Title Effective Date Summary of Changes Coverage Rationale
REVISED
Ablative Treatment for Spinal Pain (continued)
Jun. 1, 2018
and 64999 (when used for pulsed radiofrequency ablation) require precertification with
Medical Director review in all sites of service”
Performed at a frequency of six months or longer (maximum of 2 times over a 12 month period), and
There has been a 50% or greater documented reduction in pain for 10 to
12 weeks following the previous ablation. Thermal radiofrequency ablation of facet joint nerves is unproven
and not medically necessary: When there has been no positive response to medial branch block
injection; or When performed more frequently than every six months
For additional information regarding frequency guidelines, refer to the Clinical Evidence section of the policy.
Documentation requirements for the aforementioned procedures must include: Temperature of procedure Duration of ablation
Specific identification of side and level of medial branch blocks Specific identification of side and level of ablation
Percentage of pain relief with prior ablation if applicable Duration of improvement from previous ablation if applicable. Thermal radiofrequency ablation is unproven and not medically necessary for treating ALL other pain indications including but not limited to:
Diabetic neuropathy Sacroiliac pain Complex regional pain syndrome or regional pain disorders and
syndromes in the absence of spinal pain
Definitive clinical and/or imaging findings identifying a condition requiring surgical treatment
Identified specific causes of spinal pain (e.g., disc herniation) requiring
definitive treatment
Studies of radiofrequency ablation for other conditions were limited,
uncontrolled, and insufficient to support conclusions regarding efficacy or duration of effect. Additional well-designed, longer-term randomized controlled trials are required to evaluate the safety and efficacy of radiofrequency ablation and to compare this technique with other medical or

18 Oxford® Policy Update Bulletin: May 2018
Clinical Policy Updates
Oxford
Policy Title Effective Date Summary of Changes Coverage Rationale
REVISED
Ablative Treatment for Spinal Pain (continued)
Jun. 1, 2018
surgical therapies for pain. The following ablation procedures are unproven and not medically
necessary for treating spinal pain: Pulsed radiofrequency therapy of the facet nerves of the cervical,
thoracic, or lumbar region, sacral nerve root or dorsal root ganglion
Endoscopic radiofrequency ablation (rhizotomy) Cryoablation (cryodenervation, cryoneurolysis, cryosurgery, or
cryoanesthesia) Chemical ablation (including but not limited to alcohol, phenol or sodium
morrhuate Laser ablation (including pulsed, continuous, or low level) There is insufficient evidence to establish the efficacy of the ablation therapies bulleted immediately above to reduce or relieve spinal pain. Studies are limited by small sample size retrospective and case series
studies. The clinical value needs to be examined in well-designed, randomized controlled trials with large sample size and long term follow-up.
Actemra® (Tocilizumab) Injection for Intravenous Infusion
Jun. 1, 2018
Revised conditions of coverage/precertification requirements; added language to indicate: o Requests for hospital
outpatient facility infusion of Actemra require additional precertification with review by a Medical Director or their designee; refer to the policy titled Specialty Medication
Administration - Site of Care
Review Guidelines
Please refer to Injectable Chemotherapy Drugs: Application of NCCN Clinical Practice Guidelines for updated information based upon the National Comprehensive Cancer Network (NCCN) Drugs & Biologics Compendium®
(NCCN Compendium®) for oncology indications.
This policy refers only to Actemra (tocilizumab) injection for intravenous infusion for the treatment of rheumatoid arthritis, polyarticular juvenile idiopathic arthritis, systemic juvenile idiopathic arthritis, and cytokine release syndrome. Actemra for self-administered subcutaneous injection is obtained under the pharmacy benefit and is indicated in the treatment of rheumatoid arthritis and giant cell arteritis.
Actemra is proven and medically necessary for the treatment of: Polyarticular juvenile idiopathic arthritis when ALL of the
following criteria are met: o Diagnosis of polyarticular juvenile idiopathic arthritis (PJIA); and o Actemra is initiated and titrated according to US Food and Drug
Administration labeled dosing for polyarticular juvenile idiopathic
arthritis up to a maximum of (or equivalent dose and interval schedule):

19 Oxford® Policy Update Bulletin: May 2018
Clinical Policy Updates
Oxford
Policy Title Effective Date Summary of Changes Coverage Rationale
REVISED
Actemra® (Tocilizumab) Injection for
Intravenous Infusion (continued)
Jun. 1, 2018
10mg/kg every 4 weeks for patients weighing < 30kg 8mg/kg every 4 weeks for patients weighing ≥ 30kg; and
o Patient is not receiving Actemra in combination with either of the following: Biologic disease-modifying antirheumatic drug (DMARD) [e.g.,
Enbrel (etanercept), Humira (adalimumab), Cimzia (certolizumab), Simponi (golimumab)]
Janus kinase inhibitor [e.g., Xeljanz (tofacitinib)]
Rheumatoid arthritis when ALL of the following criteria are met: o Diagnosis of moderate to severely active rheumatoid arthritis (RA);
and o History of failure, contraindication, or intolerance to at least one
non-biologic DMARD [e.g., methotrexate, leflunomide, sulfasalazine, hydroxychloroquine, minocycline, etc.]; and
o Actemra is initiated and titrated according to US Food and Drug Administration labeled dosing for rheumatoid arthritis up to a
maximum of 800mg every 4 weeks (or equivalent dose and interval schedule); and
o Patient is not receiving Actemra in combination with either of the following: Biologic DMARD [e.g., Enbrel (etanercept), Humira
(adalimumab), Cimzia (certolizumab), Simponi (golimumab)] Janus kinase inhibitor [e.g., Xeljanz (tofacitinib)]
Systemic juvenile idiopathic arthritis when ALL of the following
criteria are met: o Diagnosis of systemic juvenile idiopathic arthritis (SJIA); and
o Actemra is initiated and titrated according to US Food and Drug
Administration labeled dosing for systemic juvenile idiopathic arthritis up to a maximum of (or equivalent dose and interval schedule): 12mg/kg every 2 weeks for patients weighing < 30kg 8mg/kg every 2 weeks for patients weighing ≥ 30kg; and
o Patient is not receiving Actemra in combination with either of the
following: Biologic DMARD [e.g., Enbrel (etanercept), Humira
(adalimumab), Cimzia (certolizumab), Simponi (golimumab)]

20 Oxford® Policy Update Bulletin: May 2018
Clinical Policy Updates
Oxford
Policy Title Effective Date Summary of Changes Coverage Rationale
REVISED
Actemra® (Tocilizumab) Injection for
Intravenous Infusion (continued)
Jun. 1, 2018 Janus kinase inhibitor [e.g., Xeljanz (tofacitinib)]
Cytokine release syndrome when ALL of the following criteria are
met: o Diagnosis of chimeric antigen receptor (CAR) T cell-induced cytokine
release syndrome (CRS); and
o Actemra is prescribed according to US Food and Drug Administration labeled dosing for CRS: 12mg/kg for patients weighing < 30kg 8mg/kg for patients weighing ≥ 30kg; up to a maximum of
800mg per infusion and
o Actemra is prescribed for a maximum of 4 doses
Benlysta® (Belimumab)
Aug. 1, 2018
Updated list of related policies; added reference link to the policy titled Specialty Medication Administration – Site of Care
Review Guidelines Revised conditions of
coverage/precertification requirements to indicate: o Precertification with review
by a Medical Director or their
designee through Oxford’s Medical Management is required
o New Jersey Small Group members should refer to their certificate of coverage
for precertification guidelines
and quantity limit guidelines o Requests for hospital
outpatient facility infusion of Benlysta require additional precertification with review by a Medical Director or their designee; refer to the policy
titled Specialty Medication Administration - Site of Care
This policy refers only to Benlysta (belimumab) injection for intravenous infusion for the treatment of systemic lupus erythematosus (SLE). Benlysta
(belimumab) for self-administered subcutaneous injection is obtained under the pharmacy benefit and is indicated systemic lupus erythematosus.
Benlysta (belimumab) is proven and medically necessary for the treatment of systemic lupus erythematosus when all of the following criteria are met: Diagnosis of active systemic lupus erythematosis; and One of the following:
o Anti-nuclear antibody (ANA) titer ≥ 1:80 o Anti-double-stranded DNA (anti-dsDNA) level ≥ 30 IU/mL] and
Currently receiving at least one standard of care treatment for active systemic lupus erythematosus (e.g., antimalarials, corticosteroids, or immunosuppressants); and
Benlysta is initiated and titrated according to US Food and Drug
Administration labeled dosing for SLE up to a maximum of 10mg/kg every 4 weeks.
Benlysta is unproven and not medically necessary for: Severe active lupus nephritis Severe active central nervous system (CNS) lupus Use in combination with other biologics or intravenous cyclophosphamide
Waldenström macroglobulinemia Sjögren's syndrome

21 Oxford® Policy Update Bulletin: May 2018
Clinical Policy Updates
Oxford
Policy Title Effective Date Summary of Changes Coverage Rationale
REVISED
Benlysta® (Belimumab) (continued)
Aug. 1, 2018 Review Guidelines
Rheumatoid arthritis
Chromosome Microarray Testing
(Non-Oncology Conditions)
Jun. 1, 2018
Changed policy title; previously titled Chromosome Microarray
Testing Updated list of related policies:
o Added reference link to the policy titled Molecular
Oncology Testing for Cancer Diagnosis, Prognosis, and Treatment Decisions
o Removed reference link to the policy titled Gene Expression Tests for Cardiac
Indications Revised coverage rationale:
o Replaced reference to “patients” with “individuals”
o Replaced language indicating: “[The listed services] are
proven and medically necessary” with “[the listed services] are proven and/or medically necessary”
“Genome-wide comparative genomic
hybridization microarray testing and single nucleotide polymorphism (SNP) chromosomal microarray analysis are unproven and not
medically necessary for all other patient populations and conditions [not listed as
Genome-wide comparative genomic hybridization microarray testing or single nucleotide polymorphism (SNP) chromosomal microarray
analysis is proven and/or medically necessary for evaluating an embryo/fetus in the following cases: Women undergoing invasive prenatal testing (i.e., amniocentesis,
chorionic villus sampling or fetal tissue sampling)
Intrauterine Fetal Demise or Stillbirth Genome-wide comparative genomic hybridization microarray testing or SNP chromosomal microarray analysis is proven and/or medically necessary for evaluating individuals with one or more of the following:
Multiple anomalies not specific to a well-delineated genetic syndrome and cannot be identified by a clinical evaluation alone
Non-syndromic Developmental Delay/Intellectual Disability Autism spectrum disorders Genome-wide comparative genomic hybridization microarray testing or SNP chromosomal microarray analysis are unproven and/or not
medically necessary for all other populations and conditions including but not limited to the following: For evaluating an embryo/fetus in the following cases:
o Preimplantation Genetic Diagnosis (PGD) in embryos o Preimplantation Genetic Screening (PGS) in embryos
Epilepsy
There is insufficient evidence in the clinical literature demonstrating that genome-wide comparative genomic hybridization microarray testing or SNP chromosomal microarray analysis has a role in clinical decision-making or has a beneficial effect on health outcomes for other indications such as PGD in embryos, PGS in embryos, or epilepsy. Further studies are needed to determine the analytic validity, clinical validity and clinical utility of this test
for indications other than those listed above as proven/medically necessary. Note: Genome-wide comparative genomic hybridization microarray testing or SNP chromosomal microarray analysis for the evaluation of cancer is

22 Oxford® Policy Update Bulletin: May 2018
Clinical Policy Updates
Oxford
Policy Title Effective Date Summary of Changes Coverage Rationale
REVISED
Chromosome Microarray Testing (Non-Oncology
Conditions) (continued)
Jun. 1, 2018
proven and/or medically necessary]” with “genome-wide
comparative genomic hybridization microarray testing or SNP
chromosomal microarray analysis are unproven and/or not medically necessary for all other
populations and conditions [not listed as proven and/or medically necessary]”
o Updated list of populations and conditions for which
genome-wide comparative genomic hybridization
microarray testing or SNP chromosomal microarray analysis is unproven and/or not medically necessary: Added epilepsy
Removed diagnosis, management, and prognosis of cancer
Replaced “preimplantation genetic diagnosis or screening in
embryos” with
“Preimplantation Genetic Diagnosis (PGD) and Preimplantation Genetic Screening (PGS) in embryos”
o Modified language pertaining
to clinical evidence/study findings to indicate there is insufficient evidence in the
addressed in the policy titled Molecular Oncology Testing for Cancer Diagnosis Prognosis, and Treatment Decisions. Genetic Counseling
Genetic counseling is strongly recommended prior to this test in order to
inform persons being tested about the advantages and limitations of the test as applied to a unique person.

23 Oxford® Policy Update Bulletin: May 2018
Clinical Policy Updates
Oxford
Policy Title Effective Date Summary of Changes Coverage Rationale
REVISED
Chromosome Microarray Testing (Non-Oncology
Conditions) (continued)
Jun. 1, 2018
clinical literature demonstrating that genome-wide comparative genomic
hybridization microarray testing or SNP chromosomal microarray analysis has a
role in clinical decision-making or has a beneficial effect on health outcomes for other indications such as
PGD in embryos, PGS in embryos, or epilepsy
o Added language to indicate genome-wide comparative genomic hybridization microarray testing or SNP
chromosomal microarray analysis for the evaluation of
cancer is addressed in the policy titled Molecular Oncology Testing for Cancer Diagnosis Prognosis, and Treatment Decisions
Added definition of: o Preimplantation Genetic
Diagnosis (PGD) o Preimplantation Genetic
Screening (PGS) o Prenatal Diagnosis
Updated list of applicable CPT
codes: o Added 81479 o Removed 0004M
Reformatted list of applicable ICD-10 diagnosis codes; transferred content to embedded
Excel file format Updated supporting information
to reflect the most current

24 Oxford® Policy Update Bulletin: May 2018
Clinical Policy Updates
Oxford
Policy Title Effective Date Summary of Changes Coverage Rationale
REVISED
Chromosome Microarray Testing (Non-Oncology
Conditions) (continued)
Jun. 1, 2018 description of services, clinical evidence, and references
Drug Coverage Criteria - New and Therapeutic Equivalent
Medications
Jun. 1, 2018 Revised list of medications requiring precertification through the pharmacy benefit manager (PBM):
o Added Cimduo, Rhopressa, Symfi, Symfi Lo, Tamiflu Capsules (brand only), and Zypitamag
o Removed Actiq, Carospir Suspension, and Lyrica CR
Refer to the policy for complete details on Drug Coverage Criteria - New and Therapeutic Equivalent Medications.
Policy Title Effective Date Drug/Medication Status Summary of Changes
REVISED
Drug Coverage Guidelines
May 1, 2018 Adagen (Pegademase Bovine)
New Added language to indicate precertification is required through the Pharmacy Benefit Manager (PBM)
Added precertification guidelines; refer to Precertification Guidelines: Enzyme Replacement Therapy for complete details
Aldurazyme®
(Laronidase)
Revised Added language to indicate precertification is not required however it is
strongly recommended o While no penalty will be imposed for failure to request a pre-service
review, if you do not request one, a medical necessity review will be conducted post-service to determine coverage
o It is the referring physician’s responsibility to provide medical
documentation to demonstrate clinical necessity for the medication o Beginning Aug. 1, 2018, precertification will be required
Added precertification guidelines; refer to Precertification Guidelines: Enzyme Replacement Therapy for complete details
Benlysta (Belimumab)
Revised
Added language to indicate precertification is not required however it is strongly recommended o While no penalty will be imposed for failure to request a pre-service
review, if you do not request one, a medical necessity review will be conducted post-service to determine coverage
o It is the referring physician’s responsibility to provide medical

25 Oxford® Policy Update Bulletin: May 2018
Clinical Policy Updates
Oxford
Policy Title Effective Date Drug/Medication Status Summary of Changes
REVISED
Drug Coverage Guidelines (continued)
May 1, 2018 Benlysta (Belimumab) (continued)
Revised documentation to demonstrate clinical necessity for the medication o Beginning Aug. 1, 2018, precertification will be required
Added precertification guidelines; refer to Precertification Guidelines:
Enzyme Replacement Therapy for complete details
Crysvita (Burosumab-Twza)
New Added language to indicate precertification is not required however it is strongly recommended
o While no penalty will be imposed for failure to request a pre-service review, if you do not request one, a medical necessity review will be conducted post-service to determine coverage
o It is the referring physician’s responsibility to provide medical documentation to demonstrate clinical necessity for the medication
o Beginning Aug. 1, 2018, precertification will be required o Added precertification guidelines; refer to the following policies for
complete details: o Precertification Guidelines: Crysvita (Burosumab-Twza)
o Precertification Guidelines: Review at Launch for New to Market Medications
Elaprase (Idursulfase) Revised Added language to indicate precertification is not required however it is strongly recommended o While no penalty will be imposed for failure to request a pre-service
review, if you do not request one, a medical necessity review will be
conducted post-service to determine coverage o It is the referring physician’s responsibility to provide medical
documentation to demonstrate clinical necessity for the medication o Beginning Aug. 1, 2018, precertification will be required
Added precertification guidelines; refer to Precertification Guidelines: Enzyme Replacement Therapy for complete details
Fabrazyme® (Agalsidase Beta)
Revised Added language to indicate precertification is not required however it is strongly recommended
o While no penalty will be imposed for failure to request a pre-service review, if you do not request one, a medical necessity review will be conducted post-service to determine coverage
o It is the referring physician’s responsibility to provide medical
documentation to demonstrate clinical necessity for the medication o Beginning Aug. 1, 2018, precertification will be required
Added precertification guidelines; refer to Precertification Guidelines: Enzyme Replacement Therapy for complete details

26 Oxford® Policy Update Bulletin: May 2018
Clinical Policy Updates
Oxford
Policy Title Effective Date Drug/Medication Status Summary of Changes
REVISED
Drug Coverage Guidelines (continued)
May 1, 2018 Kanuma (Sebelipase Alfa)
New
Added language to indicate precertification is required through the Pharmacy Benefit Manager (PBM)
Added precertification guidelines; refer to Precertification Guidelines:
Enzyme Replacement Therapy for complete details
Lumizyme (Alglucosidase Alfa)
New Added language to indicate precertification is required through the Pharmacy Benefit Manager (PBM)
Added precertification guidelines; refer to Precertification Guidelines: Enzyme Replacement Therapy for complete details
Mepsevii (Vestronidase Alfa-Vjbk)
New Added language to indicate precertification is required through the Pharmacy Benefit Manager (PBM)
Added precertification guidelines; refer to Precertification Guidelines: Enzyme Replacement Therapy for complete details
Naglazyme (Galsulfase) New Added language to indicate precertification is required through the
Pharmacy Benefit Manager (PBM) Added precertification guidelines; refer to Precertification Guidelines:
Enzyme Replacement Therapy for complete details
Vimizim (Elosulfase Alfa) New Added language to indicate precertification is required through the
Pharmacy Benefit Manager (PBM) Added precertification guidelines; refer to Precertification Guidelines:
Enzyme Replacement Therapy for complete details
Drug Coverage Guidelines
Jun. 1, 2018 Revised conditions of coverage; added instruction to refer to the policy titled Supply Limits: New Jersey Benefit Maximum Limits for details on applicable benefit guidelines for Jersey (NJ) plan members
Actemra (Tocilizumab) Updated Updated step therapy guidelines; refer to Step Therapy Guidelines:
Actemra (Tocilizumab) for complete details
Actiq (Brand Only) (Fentanyl Citrate)
Revised Removed therapeutic equivalent guidelines and corresponding reference link to policy titled Drug Coverage Criteria - New and Therapeutic Equivalent Medications
Updated medication/drug name to include “Brand Only”
Afstyla (Antihemophilic
Factor [Recombinant] Single Chain)
Updated Updated prior authorization/medical necessity guidelines; refer to Prior
Authorization/Medical Necessity Guidelines: Afstyla for complete details
Atorvastatin (Generic Lipitor) 10mg, 20mg
Updated Updated prior authorization/notification guidelines; refer to Prior Authorization/Notification Guidelines: Cardiovascular Disease Prevention
Zero Cost Share for complete details
Belsomra (Suvorexant) Updated Updated step therapy guidelines; refer to Step Therapy Guidelines: Belsomra for complete details
Benznidazole
New
Added language to indicate precertification is required through the
Pharmacy Benefit Manager (PBM) Added prior authorization/notification guidelines; refer to Prior

27 Oxford® Policy Update Bulletin: May 2018
Clinical Policy Updates
Oxford
Policy Title Effective Date Drug/Medication Status Summary of Changes
REVISED
Drug Coverage Guidelines (continued)
Jun. 1, 2018 Benznidazole (continued)
New Authorization/Notification Guidelines: Benznidazole for complete details
Bupropion (SR) (Generic Zyban)
Revised Updated medication/drug name to include “SR” Added supply limit guidelines; refer to Supply Limit Guidelines: HCR
Tobacco Cessation - Supply Limits Override - NJ Fully Insured for complete details
Carospir Suspension
(Spironolactone)
Revised Added prior authorization/medical necessity guidelines; refer to Prior
Authorization/Medical Necessity Guidelines: Carospir for complete details Removed therapeutic equivalent guidelines and corresponding reference
link to policy titled Drug Coverage Criteria - New and Therapeutic Equivalent Medications
Chantix (Varenicline Tartrate)
Revised Added supply limit guidelines; refer to Supply Limit Guidelines: HCR Tobacco Cessation - Supply Limits Override - NJ Fully Insured for
complete details
Cimduo (Lamivudine/ Tenofovir DF)
New Added language to indicate precertification is required through the Pharmacy Benefit Manager (PBM)
Added therapeutic equivalent guidelines; refer to Therapeutic Equivalent
Guidelines: Drug Coverage Criteria - New and Therapeutic Equivalent Medications for complete details
Cimzia (Certolizumab Pegol)
Updated Updated prior authorization/notification guidelines; refer to Prior Authorization/Notification Guidelines: Cimzia (Certolizumab Pegol) for complete details
Cosentyx (Secukinumab) Updated Updated prior authorization/notification guidelines; refer to Prior
Authorization/Notification Guidelines: Cosentyx for complete details
Daraprim (Pyrimethamine)
Revised Revised prior authorization/medical necessity guidelines; refer to Prior Authorization/Medical Necessity Guidelines: Daraprim for complete details
Enbrel (Etanercept) Updated Updated prior authorization/notification guidelines; refer to Prior Authorization/Notification Guidelines: Enbrel (Etanercept) for complete
details
Ergomar (Ergotamine Tartrate)
Updated Updated prior authorization/medical necessity guidelines; refer to Prior Authorization/Medical Necessity Guidelines: Migranal for complete details
Farydak (Panobinostat) Revised Revised prior authorization/notification guidelines; refer to Prior Authorization/Notification Guidelines: Farydak for complete details
Fentanyl Citrate (Generic Actiq)
New Added language to indicate precertification is required through the Pharmacy Benefit Manager (PBM)
Added prior authorization/notification guidelines; refer to Prior
Authorization/Notification Guidelines: Actiq (Fentanyl Citrate) for complete details

28 Oxford® Policy Update Bulletin: May 2018
Clinical Policy Updates
Oxford
Policy Title Effective Date Drug/Medication Status Summary of Changes
REVISED
Drug Coverage Guidelines (continued)
Jun. 1, 2018 Grastek (Timothy Grass Pollen Allergen Extract)
Updated Updated prior authorization/medical necessity guidelines; refer to Prior Authorization/Medical Necessity Guidelines: Grastek (Timothy Grass Pollen Allergen Extract) for complete details
Jakafi (Ruxolitinib) Revised Revised prior authorization/notification guidelines; refer to Prior Authorization/Notification Guidelines: Jakafi for complete details
Kineret (Anakinra) Updated Updated prior authorization/notification guidelines; refer to Prior
Authorization/Notification Guidelines: Kineret (Anakinra) for complete
details
Korlym (Mifepristone) Updated Updated prior authorization/notification guidelines; refer to Prior Authorization/Notification Guidelines: Korlym for complete details
Lidocaine Patch Updated Updated prior authorization/notification guidelines; refer to Prior Authorization/Notification Guidelines: Lidocaine Patch for complete
details
Lemtrada (Alemtuzumab)
Updated Updated list of applicable HCPCS codes; replaced J9010 with J0202
Linzess (Linaclotide) Updated Updated prior authorization/notification guidelines; refer to Prior
Authorization/Notification Guidelines: Linzess (Linaclotide) for complete
details
Lynparza (Olaparib) Revised Revised prior authorization/notification guidelines; refer to Prior Authorization/Notification Guidelines: Lynparza for complete details
Lyrica CR (Pregabalin) Revised Added step therapy guidelines; refer to Step Therapy Guidelines: Lyrica
CR for complete details Removed therapeutic equivalent guidelines and corresponding reference
link to policy titled Drug Coverage Criteria - New and Therapeutic Equivalent Medications
Mekinist (Trametinib) Revised Revised prior authorization/notification guidelines; refer to Prior
Authorization/Notification Guidelines: Mekinist (Trametinib) for complete details
Migranal (Dihydro-
Ergotamine) (Brand)
Updated Updated prior authorization/medical necessity guidelines; refer to Prior
Authorization/Medical Necessity Guidelines: Migranal for complete details
Migranal (Dihydro-
Ergotamine) (Generic)
Updated Updated prior authorization/medical necessity guidelines; refer to Prior
Authorization/Medical Necessity Guidelines: Migranal for complete details
Movantik (Naloxegol) Updated Updated prior authorization/notification guidelines; refer to Prior Authorization/Notification Guidelines: Movantik for complete details
Nicotine OTC Products Revised Added supply limit guidelines; refer to Supply Limit Guidelines: HCR
Tobacco Cessation - Supply Limits Override - NJ Fully Insured for complete details
Ninlaro (Ixazomib) Updated Updated prior authorization/notification guidelines; refer to Prior Authorization/Notification Guidelines: Ninlaro for complete details

29 Oxford® Policy Update Bulletin: May 2018
Clinical Policy Updates
Oxford
Policy Title Effective Date Drug/Medication Status Summary of Changes
REVISED
Drug Coverage Guidelines (continued)
Jun. 1, 2018 Odactra (House Dust Mite Allergen Extract)
Updated Updated prior authorization/medical necessity guidelines; refer to Prior Authorization/Medical Necessity Guidelines: Odactra for complete details
Oralair (Sweet Vernal, Orchard, Perennial Rye, Timothy and Kentucky Blue Grass, Mixed
Pollens Allergen Extract)
Updated Updated prior authorization/medical necessity guidelines; refer to Prior Authorization/Medical Necessity Guidelines: Oralair (Sweet Vernal, Orchard, Perennial Rye, Timothy and Kentucky Blue Grass, Mixed Pollens Allergen Extract) for complete details
Prolia, Xgeva (Denosumab)
Revised Revised coverage guidelines to indicate precertification is required through Oxford’s Medical Management
Radicava (Edaravone) Revised Added notation to indicate administration of Radicava in a hospital outpatient facility (including any ambulatory infusion suite associated with the hospital) requires precertification with review by a Medical Director or their designee; refer to Specialty Medication Administration –
Site of Care Review Guidelines
Ragwitek (Short Ragweed Pollen Allergen Extract)
Updated Updated prior authorization/medical necessity guidelines; refer to Prior Authorization/Medical Necessity Guidelines: Ragwitek (Short Ragweed Pollen Allergen Extract) for complete details
Rexulti (Brexpiprazole) Revised Revised prior authorization/medical necessity guidelines; refer to Prior Authorization/Medical Necessity Guidelines: Rexulti for complete details
Rhopressa (Netarsudil) New Added language to indicate precertification is required through the Pharmacy Benefit Manager (PBM)
Added therapeutic equivalent guidelines; refer to Therapeutic Equivalent Guidelines: Drug Coverage Criteria - New and Therapeutic Equivalent
Medications for complete details
Rozerem (Ramelteon) Updated Updated step therapy guidelines; refer to Step Therapy Guidelines: Rozerem (Ramelteon) for complete details
Simponi (Golimumab) Updated Updated prior authorization/notification guidelines; refer to Prior
Authorization/Notification Guidelines: Simponi (Golimumab) for complete details
Simponi Aria (Golimumab)
Updated Updated list of related policies: o Modified reference link Precertification Guidelines: Simponi Aria®
(Golimumab) Injection for Intravenous Infusion to reflect title change o Added reference link to Precertification Guidelines: Specialty
Medication Administration – Site of Care Review Guidelines (previously listed under Notes section only)
Simvastatin (Generic Zocor) 5mg, 10mg, 20mg, 40mg
Updated Updated prior authorization/notification guidelines; refer to Prior Authorization/Notification Guidelines: Cardiovascular Disease Prevention Zero Cost Share for complete details

30 Oxford® Policy Update Bulletin: May 2018
Clinical Policy Updates
Oxford
Policy Title Effective Date Drug/Medication Status Summary of Changes
REVISED
Drug Coverage Guidelines (continued)
Jun. 1, 2018 Sutent (Sunitinib) Revised Revised prior authorization/notification guidelines; refer to Prior Authorization/Notification Guidelines: Sutent for complete details
Symfi (Efavirenz/ Lamivudine/Tenofovir Disoproxil Fumarate)
New Added language to indicate precertification is required through the Pharmacy Benefit Manager (PBM)
Added therapeutic equivalent guidelines; refer to Therapeutic Equivalent Guidelines: Drug Coverage Criteria - New and Therapeutic Equivalent
Medications for complete details
Smyfi Lo (Efavirenz/Lamivudine/ Tenofovir Disoproxil Fumarate)
New Added language to indicate precertification is required through the Pharmacy Benefit Manager (PBM)
Added therapeutic equivalent guidelines; refer to Therapeutic Equivalent Guidelines: Drug Coverage Criteria - New and Therapeutic Equivalent Medications for complete details
Symproic (Naldemedine) New Added prior authorization/notification guidelines; refer to Prior
Authorization/Notification Guidelines: Symproic for complete details
Tafinlar (Dabrafenib) Revised Revised prior authorization/notification guidelines; refer to Prior Authorization/Notification Guidelines: Tafinlar for complete details
Tamiflu Capsules (Brand
Only) (Oseltamivir Phosphate)
Revised Added language to indicate precertification is required through the
Pharmacy Benefit Manager (PBM) Added therapeutic equivalent guidelines; refer to Therapeutic Equivalent
Guidelines: Drug Coverage Criteria - New and Therapeutic Equivalent Medications for complete details
Test Strips and Meters (Diabetic)
Revised Updated prior authorization/notification guidelines; refer to Prior Authorization/Notification Guidelines: Test Strips for complete details
Added notation to indicate Contour Next test strips do not require precertification
Trulance (Plecanatide) Revised Revised prior authorization/medical necessity guidelines; refer to Prior Authorization/Medical Necessity Guidelines: Trulance for complete details
Viberzi (Eluxadoline) Updated Updated prior authorization/medical necessity guidelines; refer to Prior Authorization/Medical Necessity Guidelines: Viberzi for complete details
Vyzulta (Latanoprostene Bunod)
Revised Added step therapy guidelines; refer to Step Therapy Guidelines: Vyzulta for complete details
Zelboraf (Vemurafenib) Revised Revised prior authorization/notification guidelines; refer to Prior
Authorization/Notification Guidelines: Zelboraf for complete details
Zolpimist (Zolpidem Tartrate)
Updated Updated step therapy guidelines; refer to Step Therapy Guidelines: Zolpimist (Zolpidem Tartrate) for complete details
Zypitamag (Pitavastatin) New Added language to indicate precertification is required through the
Pharmacy Benefit Manager (PBM) Added therapeutic equivalent guidelines; refer to Therapeutic Equivalent
Guidelines: Drug Coverage Criteria - New and Therapeutic Equivalent

31 Oxford® Policy Update Bulletin: May 2018
Clinical Policy Updates
Oxford
Policy Title Effective Date Drug/Medication Status Summary of Changes
REVISED
Drug Coverage Guidelines (continued)
Jun. 1, 2018 Medications for complete details
Policy Title Effective Date Summary of Changes Coverage Rationale
REVISED
Electrical Stimulation for the Treatment of Pain and Muscle Rehabilitation
Jun. 1, 2018
Replaced references to “patients” with “individuals”
Revised coverage rationale; replaced language indicating: o “[The listed services] are
proven and medically necessary” with “[the listed
services] are proven and/or medically necessary”
o “[The listed services] are unproven and not medically
necessary” with “[the listed services] are unproven
and/or not medically necessary”
o “Peripheral subcutaneous field stimulation (PSFS) or peripheral nerve field stimulation (PNFS) is unproven and not medically
necessary for treating pain” with “peripheral subcutaneous field
stimulation (PSFS) or peripheral nerve field stimulation (PNFS) is unproven and/or not
medically necessary for all indications, including but not limited to pain and opioid management”
o “Evidence for the effectiveness of PSFS or
When used for walking, functional electrical stimulation (FES), a form of neuromuscular electrical stimulation (NMES) is proven and/or medically necessary when used as one component of a comprehensive rehabilitation program in persons with paralyzed lower limbs due to spinal cord injury (SCI) with ALL of the following characteristics: Intact lower motor units (L1 and below) (both muscle and peripheral
nerves); Muscle and joint stability for weight bearing at upper and lower
extremities that can demonstrate balance and control to maintain an upright support posture independently;
Demonstrate brisk muscle contraction to NMES and have sensory perception of electrical stimulation (ES) sufficient for muscle contraction;
Possess high motivation, commitment and cognitive ability to use such devices for walking;
Able to transfer independently and can demonstrate independent standing tolerance for at least 3 minutes;
Demonstrate hand and finger function to manipulate controls; Post recovery from SCI and restorative surgery of at least 6 months; No hip and knee degenerative disease and no history of long bone
fracture secondary to osteoporosis. FES is unproven and/or not medically necessary for treating ANY
other indication not listed above as proven and medically necessary, including but not limited to: Disuse muscle atrophy in persons with SCI. Disuse muscle atrophy in persons with multiple sclerosis (MS).
Gait disorders (e.g., foot drop) of central neurologic origin, including but not limited to stroke or MS.
Further studies are needed to confirm that FES promotes bone remineralization and prevents or reverses muscle atrophy. Only a few studies have looked at FES as a modality of treatment of MS, and the results are

32 Oxford® Policy Update Bulletin: May 2018
Clinical Policy Updates
Oxford
Policy Title Effective Date Summary of Changes Coverage Rationale
REVISED
Electrical Stimulation for the Treatment of Pain
and Muscle Rehabilitation (continued)
Jun. 1, 2018
PNFS based on controlled studies is lacking; randomized controlled trials
(RCTs) are needed to evaluate the efficacy of this treatment” with “evidence
for the effectiveness of PSFS or PNFS based on controlled studies is limited; additional studies are needed to
evaluate the efficacy of this treatment”
Updated supporting information to reflect the most current clinical evidence, FDA information, and references
limited and conflicting regarding whether FES improves treatment outcomes in MS when offered in addition to other rehabilitative treatment modalities. There is insufficient evidence in the peer reviewed literature that use of FES
will improve health outcomes in individuals with gait disorders. Published studies have included small heterogeneous patient populations, short-term follow-ups, and various treatment protocols, outcome measures, and FES
devices. NMES is proven and/or medically necessary for treating Disuse muscle atrophy if:
The nerve supply to the muscle is intact; and The disuse muscle atrophy is not of neurological origin but originates
from conditions such as casting, splinting or contractures; or To improve wrist and finger function and prevent or correct shoulder
subluxation in persons with partial paralysis following stroke.
NMES is unproven and/or not medically necessary for treating ANY other indication not listed above as proven and medically necessary.
There is insufficient evidence in the peer reviewed literature that use of ES will improve health outcomes for the treatment of multiple conditions other than those identified above as proven. Overall, studies in the form of RCTs and case series included small, heterogeneous patient populations and short-term follow-ups. Some systematic reviews have reported that no
improvement was seen with NMES, outcomes were conflicting and/or in some cases, when improvement was noted, the effects did not last. Heterogeneity of treatment regimens and outcome measures make it difficult to establish that NMES resulted in meaningful clinical outcomes (e.g., decrease pain, functional improvement, improvement in quality of life (QOL) and ability to carry out activities of daily living (ADLs) for these other
conditions and indications.
Interferential therapy (IFT) is unproven and/or not medically necessary for treating the following indications: For the treatment of musculoskeletal disorders or injuries. For stimulating healing of nonsurgical soft tissue injuries. To facilitate the healing of bone fractures.
There is limited evidence from the available studies to conclude that IFT reduces the pain or promotes healing of bone fractures, musculoskeletal or

33 Oxford® Policy Update Bulletin: May 2018
Clinical Policy Updates
Oxford
Policy Title Effective Date Summary of Changes Coverage Rationale
REVISED
Electrical Stimulation for the Treatment of Pain
and Muscle Rehabilitation (continued)
Jun. 1, 2018 nonsurgical soft tissue injuries. Although a few studies reported some improvement in pain or disability following IFT for these conditions, none of the double-blind, randomized, placebo-controlled studies reported a positive
treatment effect of IFT for nonsurgical soft tissue injuries or bone fractures. Pulsed electrical stimulation (PES) is unproven and/or not medically
necessary for treating osteoarthritis (OA). There is insufficient evidence to conclude that PES provides health benefits to individuals with OA. RTCs are necessary to assess the durability of this procedure in comparison to other types of treatment.
Peripheral subcutaneous field stimulation (PSFS) or peripheral nerve
field stimulation (PNFS) is unproven and/or not medically necessary for all indications, including but not limited to pain and opioid management. Evidence for the effectiveness of PSFS or PNFS based on controlled studies is limited. Additional studies are needed to evaluate the efficacy of this
treatment.
Microcurrent electrical nerve stimulation (MENS) therapy is unproven and/or not medically necessary. There is insufficient evidence to conclude that MENS is safe and effective. Robust clinical trials are needed to evaluate this therapy in comparison to other types of treatment.
Percutaneous electrical nerve stimulation (PENS) or percutaneous neuromodulation therapy (PNT) is unproven and/or not medically necessary for treating pain. There is limited evidence in the peer reviewed literature to support that PENS
or PNT will improve health outcomes in individuals with pain. RCTs assessing larger patient groups and long-term follow up are needed to further clarify its role.
Dorsal root ganglion (DRG) stimulation is unproven and/or not medically necessary. There is limited evidence in the peer reviewed literature to support that DRG stimulation will improve health outcomes in individuals with pain. RCTs assessing larger patient groups and long-term follow up are needed to further clarify its role.

34 Oxford® Policy Update Bulletin: May 2018
Clinical Policy Updates
Oxford
Policy Title Effective Date Summary of Changes Coverage Rationale
REVISED
Entyvio® (Vedolizumab)
Jun. 1, 2018
Updated list of related policies; added reference link to the policy titled Acquired Rare
Disease Drug Therapy Exception Process
Revised conditions of
coverage/precertification requirements; added language to indicate: o Requests for hospital
outpatient facility infusion of Entyvio require additional precertification with review by a Medical Director or their designee; refer to the policy titled Specialty Medication
Administration - Site of Care Review Guidelines
Updated supporting information to reflect the most current references
Entyvio (vedolizumab) is proven and medically necessary for the treatment of:
Crohn's disease when all of the following criteria are met:
For initial therapy, all of the following: o Diagnosis of moderately to severely active Crohn’s disease (CD);
and o One of the following:
History of failure, contraindication, or intolerance to at least one of the following conventional therapies:
- Tumor necrosis factor (TNF) blocker [e.g., Humira (adalimumab), Cimzia (certolizumab)]
- Immunomodulator (e.g., azathioprine, 6-mercaptopurine) - Corticosteroid
Corticosteroid dependent (e.g., unable to successfully taper corticosteroids without a return of the symptoms of CD)
and o Entyvio is initiated and titrated according to US Food and Drug
Administration (FDA) labeled dosing for Crohn’s disease up to a maximum of 300mg every 8 weeks (or equivalent dose and interval schedule); and
o Patient is not receiving Entyvio in combination with either of the following:
Tumor necrosis factor (TNF) blocker [e.g., Humira (adalimumab), Cimzia (certolizumab)]
Tysabri (natalizumab); and o Initial authorization will be for no more than 14 weeks
For continuation therapy, all of the following: o Documentation of positive clinical response to Entyvio; and
o Entyvio dosing for Crohn’s disease is in accordance with the FDA
labeled dosing up to a maximum of 300mg every 8 weeks (or equivalent dose and interval schedule); and
o Reauthorization will be for no more than 12 months. Ulcerative colitis when all of the following criteria are met:
For initial therapy, all of the following:
o Diagnosis of moderately to severely active ulcerative colitis (UC); and
o One of the following:

35 Oxford® Policy Update Bulletin: May 2018
Clinical Policy Updates
Oxford
Policy Title Effective Date Summary of Changes Coverage Rationale
REVISED
Entyvio® (Vedolizumab) (continued)
Jun. 1, 2018 History of failure, contraindication, or intolerance to at least one of the following conventional therapies: - Tumor necrosis factor (TNF) blocker [e.g., Humira
(adalimumab), Simponi (golimumab)] - Immunomodulator (e.g., azathioprine, 6-mercaptopurine) - Corticosteroid
Corticosteroid dependent (e.g., unable to successfully taper corticosteroids without a return of the symptoms of UC)
and o Entyvio is initiated and titrated according to US Food and Drug
Administration labeled dosing for ulcerative colitis up to a maximum of 300mg every 8 weeks (or equivalent dose and interval schedule); and
o Patient is not receiving Entyvio in combination with either of the following: Tumor necrosis factor (TNF) blocker [e.g., Humira (adalimumab),
Simponi (golimumab)] Tysabri (natalizumab); and
o Initial authorization will be for no more than 14 weeks. For continuation therapy, all of the following:
o Documentation of positive clinical response to Entyvio; and o Entyvio dosing for ulcerative colitis is in accordance with the FDA
labeled dosing up to a maximum of 300mg every 8 weeks (or
equivalent dose and interval schedule); and o Reauthorization will be for no more than 12 months.
Enzyme Replacement Therapy
Aug. 1, 2018
Updated list of related policies; added reference link to the policy titled Specialty Medication Administration – Site of Care
Review Guidelines
Revised conditions of coverage/precertification requirements to indicate: o Precertification with review
by a Medical Director or their designee through Oxford’s Medical Management is
required o New Jersey Small Group
This policy refers to the following enzyme replacement therapy products: Adagen (pegademase bovine) Aldurazyme (laronidase) Elaprase (idursulfase)
Fabrazyme (agalsidase beta)
Kanuma (sebelipase alfa) Lumizyme (alglucosidase alfa) Mepsevii (vestronidase alfa-vjbk) Naglazyme (galsulfase) Vimizim (elosulfase alfa) Adagen (pegademase bovine) is medically necessary for the
treatment of severe combined immunodeficiency disease (SCID) associated with a deficiency of adenosine deaminase (ADA) when the

36 Oxford® Policy Update Bulletin: May 2018
Clinical Policy Updates
Oxford
Policy Title Effective Date Summary of Changes Coverage Rationale
REVISED
Enzyme Replacement Therapy
(continued)
Aug. 1, 2018
members should refer to their certificate of coverage for precertification guidelines
and quantity limit guidelines o Requests for hospital
outpatient facility infusion of
enzyme replacement therapy products addressed in this policy require additional precertification with review
by a Medical Director or their designee; refer to the policy titled Specialty Medication Administration - Site of Care Review Guidelines
following criteria are met: For initial therapy, all of the following:
o Diagnosis of SCID; and
o Deficiency of adenosine deaminase is confirmed by any of the following: Deficiency or absence of ADA in plasma, lysed erythrocytes,
fibroblasts (cultured from amniotic fluid), or chorionic villus Increase in deoxyadenosine triphosphate (dATP) levels in
erythrocyte lysates compared to laboratory standard Decrease in ATP concentration in erythrocytes
Molecular genetic confirmation of mutations in both alleles of the ADA1 gene
Positive screening by T cell receptor excision circles (TRECs); and
o One of the following: Patient is not a suitable candidate for hematopoietic cell
transplantation (HCT) Patient has failed HCT;
and o Dosing is in accordance with the United States Food and Drug
Administration approved labeling: dosing is started at 10 U/kg for the first dose, and titrated up to a maximum dose of 30 U/kg per week; and
o Initial authorization will be for no more than 12 months. For continuation therapy, all of the following:
o Patient has previously received treatment with pegademase therapy; and
o Patient has experienced a positive clinical response to pegademase therapy (e.g., normalization of plasma ADA activity, erythrocyte
dATP levels, improvement of disease symptoms, etc.); and
o Dosing is in accordance with the United States Food and Drug Administration approved labeling: appropriate maintenance dosing, up to a maximum dose of 30 U/kg per week; and
o Reauthorization will be for no more than 12 months. Aldurazyme (laronidase) is medically necessary for the treatment of
Mucopolysaccharidosis I (MPS I) when the following criteria are met: For initial therapy, all of the following:
o Diagnosis of any of the MPS I syndromes confirmed by one the

37 Oxford® Policy Update Bulletin: May 2018
Clinical Policy Updates
Oxford
Policy Title Effective Date Summary of Changes Coverage Rationale
REVISED
Enzyme Replacement Therapy
(continued)
Aug. 1, 2018
following: Hurler variant (severe mucopolysaccharidosis I; also MPS IH) Hurler-Scheie variant (attenuated mucopolysaccharidosis I; also
MPS IHS) Scheie variant (attenuated mucopolysaccharidosis I; also MPS
IS);
and o Diagnosis of MPS I is confirmed by either of the following:
Deficiency or absence of fibroblast or leukocyte enzyme activity of alpha-L-iduronidase enzyme activity
Molecular genetic confirmation of mutations in the alpha-L-iduronidase gene;
and o Presence of clinical signs and symptoms of the disease (e.g.,
asymptomatic with affected older sibling, cardiac abnormalities, corneal clouding, dysostosis multiplex, hepatomegaly, restrictive lung
disease, etc.); and o Dosing is in accordance with the United States Food and Drug
Administration approved labeling: Administered dose does not exceed 0.58 mg/kg intravenously once every week; and
o Initial authorization will be for no more than 12 months. For continuation therapy, all of the following:
o Patient has previously received treatment with laronidase therapy;
and o Patient has experienced a positive clinical response to laronidase
therapy (e.g., improved endurance, improved functional capacity, reduced urine dermatan sulfate/heparan sulfate excretion, etc.); and
o Dosing is in accordance with the United States Food and Drug Administration approved labeling: administered dose does not
exceed 0.58 mg/kg intravenously once every week; and
o Reauthorization will be for no more than 12 months. Elaprase (idursulfase) is medically necessary for the treatment of Mucopolysaccharidosis II (MPS II, Hunter Syndrome) when the following criteria are met: For initial therapy, all of the following:
o Diagnosis of MPS II confirmed by one the following: Deficiency in iduronate 2-sulfatase enzyme activity as measured
in fibroblasts or leukocytes combined with normal enzyme

38 Oxford® Policy Update Bulletin: May 2018
Clinical Policy Updates
Oxford
Policy Title Effective Date Summary of Changes Coverage Rationale
REVISED
Enzyme Replacement Therapy
(continued)
Aug. 1, 2018
activity level of another sulfatase Molecular genetic testing for deletion or mutations in the
iduronate 2-sulfatase gene;
and o Presence of clinical signs and symptoms of the disease (e.g.,
hepatosplenomegaly, skeletal deformities, dysostosis, neurocognitive
decline, cardiovascular disorders, etc.); and o Dosing is in accordance with the United States Food and Drug
Administration approved labeling: administered dose does not exceed 0.5 mg/kg intravenously once every week; and
o Initial authorization will be for no more than 12 months. For continuation therapy, all of the following:
o Patient has previously received treatment with idursulfase therapy; and
o Patient has experienced a positive clinical response to idursulfase therapy (e.g., improved endurance, improved functional capacity,
reduced spleen volume, reduced urine GAG excretion, etc.); and o Dosing is in accordance with the United States Food and Drug
Administration approved labeling: administered dose does not exceed 0.5 mg/kg intravenously once every week; and
o Reauthorization will be for no more than 12 months. Fabrazyme (agalsidase beta) is medically necessary for the
treatment of Fabry disease when the following criteria are met: For initial therapy, all of the following:
o Diagnosis of Fabry disease as confirmed by one the following: Absence or deficiency (< 5% of mean) of normal alpha-
galactosidase A (α-Gal A) enzyme activity) in leukocytes, dried blood spots, or serum analysis
Molecular genetic testing for deletion or mutations in the
galactosidase alpha gene; and
o Presence of clinical signs and symptoms of the disease (e.g., Acroparesthesias, angiokeratomas, whorls, anhidrosis/hypohidrosis, renal disease, exercise/heat/cold intolerance, etc.); and
o Dosing is in accordance with the United States Food and Drug
Administration approved labeling: administered dose does not exceed 1 mg/kg intravenously every two weeks; and
o Initial authorization will be for no more than 12 months.

39 Oxford® Policy Update Bulletin: May 2018
Clinical Policy Updates
Oxford
Policy Title Effective Date Summary of Changes Coverage Rationale
REVISED
Enzyme Replacement Therapy
(continued)
Aug. 1, 2018
For continuation therapy, all of the following: o Patient has previously received treatment with agalsidase therapy;
and
o Patient has experienced a positive clinical response to agalsidase therapy (e.g., improved renal function, reduction in mean plasma GL-3 levels, decreased GL-3 inclusions, etc.); and
o Dosing is in accordance with the United States Food and Drug Administration approved labeling: administered dose does not exceed 1 mg/kg intravenously every two weeks; and
o Reauthorization will be for no more than 12 months.
Kanuma (sebelipase alfa) is medically necessary for the treatment of Lysosomal acid lipase deficiency [LAL-D, Wolman disease (WD), cholesteryl ester disease (CESD)] when the following criteria are met: For initial therapy, all of the following:
o Diagnosis of lysosomal acid lipase deficiency [LAL-D, Wolman disease (WD), cholesteryl ester disease (CESD)] as confirmed by one the
following: Absence or deficiency lysosomal acid lipase activity by dried
blood spot test Molecular genetic testing for deletion or mutations in the lipase
A, lysosomal acid type (LIPA) gene;
and o Presence of clinical signs and symptoms of the disease (e.g.,
abdominal distention, hepatosplenomegaly, liver fibrosis, ascities, etc.); and
o Dosing is in accordance with the United States Food and Drug Administration approved labeling by one of the following:
For rapidly progressive disease presenting within the first 6
months of life: administered initial starting dose is 1 mg/kg intravenously once weekly, up to a maximum of 3 mg/kg once weekly
Pediatric and adult patients with disease: administered dose does not exceed 1 mg/kg intravenously every other week;
and
o Initial authorization will be for no more than 12 months. For continuation therapy, all of the following:
o Patient has previously received treatment with sebelipase therapy;

40 Oxford® Policy Update Bulletin: May 2018
Clinical Policy Updates
Oxford
Policy Title Effective Date Summary of Changes Coverage Rationale
REVISED
Enzyme Replacement Therapy
(continued)
Aug. 1, 2018
and o Patient has experienced a positive clinical response to sebelipase
therapy [e.g., improved disease symptoms, improvement of
laboratory values (LFTs, cholesterol, triglycerides), etc.]; and o Dosing is in accordance with the United States Food and Drug
Administration approved labeling by one of the following:
For rapidly progressive disease presenting within the first 6 months of life: administered dose is 1 mg/kg intravenously once weekly, up to a maximum of 3 mg/kg once weekly
Pediatric and adult patients with disease: administered dose does
not exceed 1 mg/kg intravenously every other week; and
o Reauthorization will be for no more than 12 months.
Lumizyme (alglucosidase alfa) is medically necessary for the treatment of Pompe disease when the following criteria are met:
For initial therapy, one of the following: o All of the following for infantile-onset Pompe disease:
Diagnosis of infantile-onset Pompe disease as confirmed by one the following: - Absence or deficiency (<1% of the lab specific normal mean)
acid alpha-glucosidase deficiency (GAA) activity in skin fibroblasts
- Molecular genetic testing for deletion or mutations in the GAA gene;
and Presence of clinical signs and symptoms of the disease (e.g.,
cardiac hypertrophy, respiratory distress, skeletal muscle weakness, etc.); and
Dosing is in accordance with the United States Food and Drug
Administration approved labeling: administered dose does not exceed 20 mg/kg intravenously every two weeks; and
Initial authorization will be for no more than 12 months; or
o All of the following for late-onset (non-infantile) Pompe disease: Diagnosis of late-onset Pompe disease as confirmed by one the
following: - Absence or deficiency (<40% of the lab specific normal
mean) acid alpha-glucosidase deficiency (GAA) activity in

41 Oxford® Policy Update Bulletin: May 2018
Clinical Policy Updates
Oxford
Policy Title Effective Date Summary of Changes Coverage Rationale
REVISED
Enzyme Replacement Therapy
(continued)
Aug. 1, 2018
lymphocytes, fibroblasts or muscle - Molecular genetic testing for deletion or mutations in the GAA
gene;
and Presence of clinical signs and symptoms of the disease (e.g.,
cardiac hypertrophy, respiratory distress, skeletal muscle
weakness, etc.); and Dosing is in accordance with the United States Food and Drug
Administration approved labeling: administered dose does not exceed 20 mg/kg intravenously every two weeks; and
Initial authorization will be for no more than 12 months. For continuation therapy, all of the following:
o Patient has previously received treatment with alglucosidase therapy; and
o Patient has experienced a positive clinical response to alglucosidase therapy (e.g., improved respiratory/cardiac function, improved
endurance, etc.); and o Dosing is in accordance with the United States Food and Drug
Administration approved labeling: administered dose does not exceed 20 mg/kg intravenously every two weeks; and
o Reauthorization will be for no more than 12 months. Mepsevii (vestronidase alfa-vjbk) is proven and medically necessary
for the treatment of Mucopolysaccharidosis VII (Sly syndrome) when the following criteria are met: For initial therapy, all of the following:
o Diagnosis of Mucopolysaccharidosis VII confirmed by either of the following: Absence or deficiency of fibroblast or leukocyte enzyme activity
of beta glucuronidase
Molecular genetic confirmation of mutations in the GUSB gene. and
o Presence of clinical signs and symptoms of the disease (e.g., enlarged liver and spleen, joint limitations, airway obstruction or pulmonary problems, limitation of mobility while still ambulatory, etc.); and
o Dosing is in accordance with the United States Food and Drug Administration approved labeling: Administered dose does not exceed 4 mg/kg intravenously once every two weeks; and

42 Oxford® Policy Update Bulletin: May 2018
Clinical Policy Updates
Oxford
Policy Title Effective Date Summary of Changes Coverage Rationale
REVISED
Enzyme Replacement Therapy
(continued)
Aug. 1, 2018
o Initial authorization will be for no more than 12 months. For continuation therapy, all of the following:
o Patient has previously received treatment with vestronidase therapy;
and o Patient has experienced a positive clinical response to vestronidase
therapy (e.g., improved endurance, improved functional capacity,
improved pulmonary function, etc.); and o Dosing is in accordance with the United States Food and Drug
Administration approved labeling: Administered dose does not exceed 4 mg/kg intravenously once every two weeks; and
o Reauthorization will be for no more than 12 months. Naglazyme (galsulfase) is medically necessary for the treatment of Mucopolysaccharidosis VI (Maroteaux-Lamy syndrome) when the following criteria are met: For initial therapy, all of the following:
o Diagnosis of Mucopolysaccharidosis VI confirmed by either of the following:
Absence or deficiency of fibroblast or leukocyte enzyme activity of N-acetylgalactosamine 4-sulfatase (arylsulfatase)
Molecular genetic confirmation of mutations in the ASB gene (5q13-q14);
and
o Presence of clinical signs and symptoms of the disease (e.g., kyphoscoliosis, genu valgum, pectus carinatum, gait disturbance, growth deficiency, etc.); and
o Dosing is in accordance with the United States Food and Drug Administration approved labeling: administered dose does not exceed 1 mg/kg intravenously once every week; and
o Initial authorization will be for no more than 12 months.
For continuation therapy, all of the following: o Patient has previously received treatment with galsulfase therapy;
and o Patient has experienced a positive clinical response to galsulfase
therapy (e.g., improved endurance, improved functional capacity, reduced urine dermatan sulfate excretion, etc.); and
o Dosing is in accordance with the United States Food and Drug Administration approved labeling: administered dose does not exceed 1 mg/kg intravenously once every week; and

43 Oxford® Policy Update Bulletin: May 2018
Clinical Policy Updates
Oxford
Policy Title Effective Date Summary of Changes Coverage Rationale
REVISED
Enzyme Replacement Therapy
(continued)
Aug. 1, 2018 o Reauthorization will be for no more than 12 months. Vimizim (elosulfase alfa) is medically necessary for the treatment of
Mucopolysaccharidosis type IVA (MPS IVA; Morquio A syndrome) when the following criteria are met: For initial therapy, all of the following:
o Diagnosis of Morquio A syndrome confirmed by either of the following: Absence or deficiency of fibroblast or leukocyte GALNS enzyme
activity
Molecular genetic testing for mutations in the GALNS gene (16q24.3);
and o Presence of clinical signs and symptoms of the disease (e.g.,
kyphoscoliosis, genu valgum, pectus carinatum, gait disturbance, growth deficiency, etc.); and
o Dosing is in accordance with the United States Food and Drug Administration approved labeling: administered dose does not
exceed 2 mg/kg IV once every week; and o Initial authorization will be for no more than 12 months.
For continuation therapy, all of the following: o Patient has previously received treatment with elosulfase alfa
therapy; and
o Patient has experienced a positive clinical response to elosulfase alfa therapy (e.g., improved endurance, improved functional capacity, reduced urine keratan sulfate excretion); and
o Dosing is in accordance with the United States Food and Drug Administration approved labeling: administered dose does not exceed 2 mg/kg IV once every week; and
o Reauthorization will be for no more than 12 months.
Exondys 51™ (Eteplirsen)
Jun. 1, 2018
Revised conditions of coverage/precertification requirements; added language to indicate: o Requests for hospital
outpatient facility infusion of Exondys 51 require
additional precertification with review by a Medical
Exondys 51™ (eteplirsen) may be covered for the treatment of Duchenne muscular dystrophy (DMD) in patients who meet ALL of the following criteria:
For initial therapy, all of the following: o Diagnosis of Duchenne muscular dystrophy by, or in consultation
with, a neurologist with expertise in the diagnosis of DMD; and o Submission of medical records (e.g., chart notes, laboratory values)
confirming the mutation of the DMD gene is amenable to exon 51 skipping; and

44 Oxford® Policy Update Bulletin: May 2018
Clinical Policy Updates
Oxford
Policy Title Effective Date Summary of Changes Coverage Rationale
REVISED
Exondys 51™ (Eteplirsen) (continued)
Jun. 1, 2018 Director or their designee; refer to the policy titled Specialty Medication
Administration - Site of Care Review Guidelines
o Submission of medical records (e.g., chart notes, laboratory values) confirming patient has a 6-Minute Walk Time (6MWT) ≥ 300 meters while walking independently (e.g., without side-by-side assist, cane,
walker, wheelchair, etc.) prior to beginning Exondys 51 therapy;and o Exondys 51 is prescribed by, or in consultation with, a neurologist
with expertise in the treatment of DMD; and
o Exondys 51 dosing for DMD is in accordance with the United States Food and Drug Administration approved labeling: maximum dosing of 30 mg/kg infused once weekly; and
o Initial authorization will be for no more than 8 weeks.
For continuation therapy, all of the following: o Exondys 51 is prescribed by, or in consultation with, a neurologist
with expertise in the treatment of DMD; and o Submission of medical records (e.g., chart notes, laboratory values)
demonstrating that the patient continues to have a 6-Minute Walk Time (6MWT) ≥ 300 meters while walking independently (e.g.,
without side-by-side assist, cane, walker, wheelchair, etc.). This must be measured no earlier than 4 weeks prior to a continuation
request; and o Exondys 51 dosing for DMD is in accordance with the United States
Food and Drug Administration approved labeling: maximum dosing of 30 mg/kg infused once weekly; and
o Reauthorization will be for no more than 6 months.
Exondys 51 will not be covered for other forms of muscular dystrophy.
Ilaris® (Canakinumab)
Jun. 1, 2018
Revised conditions of coverage/precertification requirements; added language
to indicate:
o Requests for hospital outpatient facility infusion of Ilaris require additional precertification with review by a Medical Director or their designee; refer to the policy titled Specialty Medication
Administration - Site of Care Review Guidelines
Ilaris® (canakinumab) is proven and medically necessary for: The treatment of Cryopyrin-Associated Periodic Syndromes (CAPS) in
patients who meet ALL of the following criteria:
For initial therapy, all of the following: o One of the following, as diagnosed by, or in consultation with, a
rheumatologist or immunologist with expertise in the diagnosis of the following: Familial Cold Autoinflammatory Syndrome (FCAS) Muckle-Wells syndrome (MWS)
and o Ilaris dosing for FCAS/MWS is in accordance with the United States

45 Oxford® Policy Update Bulletin: May 2018
Clinical Policy Updates
Oxford
Policy Title Effective Date Summary of Changes Coverage Rationale
REVISED
Ilaris® (Canakinumab) (continued)
Jun. 1, 2018
Food and Drug Administration approved labeling: maximum dosing of 3mg/kg up to 150 mg every 8 weeks; and
o Initial authorization will be for no more than 12 months.
For continuation therapy, all of the following: o Patient is currently on Ilaris therapy for one of the following:
FCAS
MWS
and o Ilaris dosing for FCAS/MWS is in accordance with the United States
Food and Drug Administration approved labeling: maximum dosing of 3mg/kg up to 150 mg every 8 weeks; and
o Documentation of positive clinical response to Ilaris therapy; and o Reauthorization will be for no more than 12 months.
The treatment of Tumor Necrosis Factor (TNF) Receptor-Associated Periodic Syndrome (TRAPS) in patients who meet ALL of the following criteria:
For initial therapy, all of the following:
o Diagnosis of TRAPS by, or in consultation with, a rheumatologist or immunologist with expertise in the diagnosis of TRAPS. and
o Ilaris dosing for TRAPS is in accordance with the United States Food and Drug Administration approved labeling: maximum dosing of 4 mg/kg up to 300mg every 4 weeks; and
o Initial authorization will be for no more than 12 months.
For continuation of therapy, all of the following: o Patient is currently receiving Ilaris therapy for TRAPS; and o Documentation of a positive clinical response to therapy, defined as a
decrease in frequency or severity of attacks; and
o Ilaris dosing for TRAPS is in accordance with the United States Food and Drug Administration approved labeling: maximum dosing of 4
mg/kg up to 300mg every 4 weeks; and o Reauthorization will be for no more than 12 months.
The treatment of Hyperimmunoglobulin D (Hyper-IgD) Syndrome (HIDS)/Mevalonate Kinase Deficiency (MKD) in patients who meet ALL of the following criteria: For initial therapy, all of the following:
o One of the following, as diagnosed by, or in consultation with, a

46 Oxford® Policy Update Bulletin: May 2018
Clinical Policy Updates
Oxford
Policy Title Effective Date Summary of Changes Coverage Rationale
REVISED
Ilaris® (Canakinumab) (continued)
Jun. 1, 2018
rheumatologist or immunologist with expertise in the diagnosis of the following: HIDS
MKD and
o Ilaris dosing for HIDS/MKD is in accordance with the United States
Food and Drug Administration approved labeling: maximum dosing of 4 mg/kg up to 300mg every 4 weeks; and
o Initial authorization will be for no more than 12 months. For continuation of therapy, all of the following:
o Patient is currently receiving Ilaris for one of the following: HIDS MKD and
o Documentation of a positive clinical response to therapy, defined by a decrease in frequency or severity of attacks; and
o Ilaris dosing for HIDS/MKD is in accordance with the United States Food and Drug Administration approved labeling: maximum dosing of
4 mg/kg up to 300mg every 4 weeks; and o Reauthorization will be for no more than 12 months.
The treatment of Familial Mediterranean Fever (FMF) in patients who meet ALL of the following criteria:
For initial therapy, all of the following: o Diagnosis of FMF by, or in consultation with, a rheumatologist or
immunologist with expertise in the diagnosis of FMF; and o History of failure, contraindication, or intolerance to colchicine; and o Ilaris dosing for FMF is in accordance with the United States Food and
Drug Administration approved labeling: maximum dosing of 4 mg/kg
up to 300mg every 4 weeks; and
o Initial authorization will be for no more than 12 months. For continuation of therapy, all of the following:
o Patient is currently receiving Ilaris for FMF; and o Documentation of a positive clinical response to therapy, defined by
a decrease in index disease flare or normalization of CRP; and o Ilaris dosing for FMF is in accordance with the United States Food and
Drug Administration approved labeling: maximum dosing of 4 mg/kg up to 300mg every 4 weeks; and
o Reauthorization will be for no more than 12 months.

47 Oxford® Policy Update Bulletin: May 2018
Clinical Policy Updates
Oxford
Policy Title Effective Date Summary of Changes Coverage Rationale
REVISED
Ilaris® (Canakinumab) (continued)
Jun. 1, 2018 The treatment of Systemic Juvenile Idiopathic Arthritis (SJIA) in patients who meet ALL of the following criteria: For initial therapy, all of the following:
o Diagnosis of SJIA by, or in consultation with, a rheumatologist or immunologist with expertise in the diagnosis of SJIA; and
o Ilaris dosing for SJIA is in accordance with the United States Food
and Drug Administration approved labeling: maximum dosing of 4 mg/kg up to 300mg every 4 weeks; and
o Patient is not receiving Ilaris in combination with another biologic [e.g., Actemra]; and
o Initial authorization will be for no more than 12 months. For continuation of therapy, all of the following:
o Patient is currently receiving Ilaris for SJIA; and o Documentation of a positive clinical response to therapy; and o Ilaris dosing for SJIA is in accordance with the United States Food
and Drug Administration approved labeling: maximum dosing of 4
mg/kg up to 300mg every 4 weeks; and o Patient is not receiving Iliaris in combination with another biologic
[e.g., Actemra]; and o Reauthorization will be for no more than 12 months.
Ilaris is not proven or medically necessary for the management or treatment of cardiovascular disease.
Infliximab (Remicade®, Inflectra™, Renflexis™)
Jun. 1, 2018
Revised conditions of coverage/precertification requirements; added language to indicate: o Requests for hospital
outpatient facility infusion of
Remicade, Inflectra, and
Renflexis require additional precertification with review by a Medical Director or their designee; refer to the policy titled Specialty Medication Administration - Site of Care Review Guidelines
This policy refers to the following infliximab products: Inflectra™ (infliximab-dyyb) Remicade® (infliximab) Renflexis™ (infliximab-abda) A. Preferred Product
Remicade® (infliximab) is the preferred infliximab product. Coverage will be provided for Remicade® contingent on the coverage criteria in the Diagnosis-Specific Criteria section.
Coverage for Inflectra™ (infliximab-dyyb) or Renflexis™ (infliximab-abda) will be provided contingent on the criteria in this section and the coverage criteria in the Diagnosis-Specific Criteria section. In order to continue coverage, members already on Inflectra™ or Renflexis™ will be required to change therapy to Remicade® unless they meet the criteria in

48 Oxford® Policy Update Bulletin: May 2018
Clinical Policy Updates
Oxford
Policy Title Effective Date Summary of Changes Coverage Rationale
REVISED
Infliximab (Remicade®, Inflectra™,
Renflexis™) (continued)
Jun. 1, 2018
this section.
Preferred Product Criteria
Treatment with Inflectra™ (infliximab-dyyb), Renflexis™ (infliximab-abda) or other infliximab biosimilar is medically
necessary for the indications specified in this policy when the following criteria are met: o Both of the following:
One of the following: - Both of the following:
o History of a trial of at least 14 weeks of Remicade resulting in minimal clinical response to therapy and
residual disease activity. o Physician attests that in their clinical opinion the clinical
response would be expected to be superior with Inflectra or other infliximab biosimilar product, than experienced with Remicade.
or - Both of the following:
o History of intolerance or adverse event to Remicade. o Physician attests that in their clinical opinion the same
intolerance or adverse event would not be expected to occur with Inflectra or other infliximab biosimilar product.
and Both of the following:
- Patient has NOT had a loss of a favorable response after established maintenance therapy with Remicade or other infliximab product.
- Patient has NOT developed neutralizing antibodies to any
infliximab product that has led to an attenuation of efficacy of therapy.
B. Diagnosis-Specific Criteria
“Infliximab” will be used to refer to all infliximab products.
Infliximab is proven and medically necessary for the treatment of: o Ankylosing spondylitis when the following criterion is met:
Diagnosis of ankylosing spondylitis (AS).

49 Oxford® Policy Update Bulletin: May 2018
Clinical Policy Updates
Oxford
Policy Title Effective Date Summary of Changes Coverage Rationale
REVISED
Infliximab (Remicade®, Inflectra™,
Renflexis™) (continued)
Jun. 1, 2018
o Crohn’s disease when the following criterion is met: One of the following:
- Diagnosis of fistulizing Crohn’s disease (Crohn’s Disease
Activity Index (CDAI) ≥ 220 and ≤ 400); or - Both of the following:
o Diagnosis of moderately to severely active Crohn’s
disease; and o History of failure, contraindication, or intolerance to at
least one conventional therapy (e.g., corticosteroids, 6-mercaptopurine, azathioprine, methotrexate, etc.).
o Noninfectious uveitis when BOTH of the following criteria are met: Diagnosis of refractory noninfectious uveitis that is causing or
threatening vision loss (e.g., noninfectious uveitis associated with Behçet’s or Reiter’s syndromes); and
History of failure, contraindication, or intolerance to ALL of the
following: - Topical corticosteroids;
- Systemic corticosteroids; - Immunosuppressive drugs (e.g., azathioprine, cyclosporine,
or methotrexate). o Plaque psoriasis when BOTH of the following criteria are met:
Diagnosis of chronic severe plaque psoriasis i.e., extensive
and/or disabling); and Patient is a candidate for systemic therapy.
o Psoriatic arthritis when the following criterion is met: Diagnosis of psoriatic arthritis (PsA).
o Rheumatoid arthritis when BOTH of the following criteria are met:
Diagnosis of moderately to severely active rheumatoid arthritis
(RA); and One of the following:
- Member is receiving concurrent therapy with methotrexate; - History of contraindication or intolerance to methotrexate.
o Sarcoidosis when ALL of the following criteria are met: Diagnosis of sarcoidosis; and
History of failure, contraindication, or intolerance to corticosteroids (e.g., prednisone, methylprednisolone); and
History of failure, contraindication, or intolerance to one

50 Oxford® Policy Update Bulletin: May 2018
Clinical Policy Updates
Oxford
Policy Title Effective Date Summary of Changes Coverage Rationale
REVISED
Infliximab (Remicade®, Inflectra™,
Renflexis™) (continued)
Jun. 1, 2018 immunosuppressant (e.g., methotrexate, cyclophosphamide, azathioprine).
o Ulcerative colitis when BOTH of the following criteria are met:
Diagnosis of moderately to severely active ulcerative colitis (UC); and
History of failure, contraindication, or intolerance to at least one
conventional therapy e.g., 6-mercaptopurine, aminosalicylate, azathioprine, corticosteroids.
There may be other conditions that qualify as serious, rare diseases for
which the use of infliximab may be appropriate. Please refer to the Benefit Considerations section of the policy for additional information.
Infliximab is unproven and not medically necessary in the treatment of: o Still’s disease
o Sjogren’s syndrome o Graft-vs-host disease
o Myelodysplastic syndromes o Undifferentiated spondyloarthropathy o Reiter’s syndrome o Hidradenitis suppurativa o Wegener’s granulomatosis
o Juvenile idiopathic arthritis (juvenile rheumatoid arthritis)
Infliximab is unproven and not medically necessary for the treatment of the above conditions because statistically robust randomized controlled trials are needed to address the issue of whether Infliximab has sufficient superiority in clinical efficacy compared to other available treatments to
justify the inherent clinical risk in the use of a monoclonal antibody anti-
tumor necrosis factor agent.
Ocrevus™ (Ocrelizumab)
Jun. 1, 2018
Updated list of related policies; added reference link to the policy titled Specialty Medication Administration - Site of Care Review Guidelines
Revised conditions of
coverage/precertification requirements; added language
Please refer to the policy titled Injectable Chemotherapy Drugs: Application of NCCN Clinical Practice Guidelines for updated information based upon the National Comprehensive Cancer Network (NCCN) Drugs & Biologics Compendium® (NCCN Compendium®) for oncology indications. Ocrevus (ocrelizumab) is proven and medically necessary for:
Primary Progressive Multiple Sclerosis Ocrevus is medically necessary for the treatment of primary

51 Oxford® Policy Update Bulletin: May 2018
Clinical Policy Updates
Oxford
Policy Title Effective Date Summary of Changes Coverage Rationale
REVISED
Ocrevus™ (Ocrelizumab) (continued)
Jun. 1, 2018
to indicate: o Requests for hospital
outpatient facility infusion of
Ocrevus require additional precertification with review by a Medical Director or their
designee; refer to the policy titled Specialty Medication Administration - Site of Care Review Guidelines
progressive multiple sclerosis (PPMS) when ALL of the following criteria are met: o Diagnosis of primary progressive multiple sclerosis (PPMS); and
o One of the following: Initial therapy for ocrelizumab when meeting both of the
following:
- Patient is not receiving ocrelizumab in combination with any of the following: Disease modifying therapy (e.g., interferon beta
preparations, daclizumab, dimethyl fumarate, glatiramer
acetate, natalizumab, fingolimod, or teriflunomide) B cell targeted therapy (e.g., rituximab, belimumab,
ofatumumab) Lymphocyte trafficking blockers (e.g., alemtuzumab,
mitoxantrone) and
- Initial dosing: One time 300 mg intravenous course of doses on days 1 and 15.
or Continuation therapy for ocrelizumab when meeting all of the
following: - Patient has previously received treatment with ocrelizumab;
and
- Documentation of positive clinical response to ocrelizumab therapy; and
- Patient is not receiving ocrelizumab in combination with any of the following: Disease modifying therapy (e.g., interferon beta
preparations, daclizumab, dimethyl fumarate, glatiramer
acetate, natalizumab, fingolimod, or teriflunomide)
B cell targeted therapy (e.g., rituximab, belimumab, ofatumumab)
Lymphocyte trafficking blockers (e.g., alemtuzumab, mitoxantrone)
and Continued dosing: One 600 mg intravenous dose every 6
months. Relapsing Forms of Multiple Sclerosis
Ocrevus is medically necessary for the treatment of relapsing

52 Oxford® Policy Update Bulletin: May 2018
Clinical Policy Updates
Oxford
Policy Title Effective Date Summary of Changes Coverage Rationale
REVISED
Ocrevus™ (Ocrelizumab) (continued)
Jun. 1, 2018
forms of multiple sclerosis (MS) when BOTH of the following criteria are met: o Diagnosis of relapsing forms of multiple sclerosis (MS) (e.g.,
relapsing-remitting MS, secondary-progressive MS with relapses, progressive-relapsing MS with relapses); and
o One of the following:
Initial therapy for ocrelizumab meeting all of the following: - Patient has history of failure following a trial for at least 4
weeks or history of intolerance or contraindication to one of the following:
interferon β-1a (Avonex®, Rebif®, Plegridy™) interferon β-1b (Betaseron® or Extavia®) glatiramer acetate (Copaxone®) dimethyl fumarate (Tecfidera®) teriflunomide (Aubagio®) fingolimod (Gilenya®)
alemtuzumab (Lemtrada®) natalizumab (Tysabri®)
daclizumab (Zinbryta™) and
- Patient is not receiving ocrelizumab in combination with any of the following: Disease modifying therapy (e.g., interferon beta
preparations, daclizumab, glatiramer acetate, natalizumab, fingolimod, or teriflunomide)
B cell targeted therapy (e.g., rituximab, belimumab, ofatumumab)
Lymphocyte trafficking blockers (e.g., alemtuzumab, mitoxantrone)
and
- Initial dosing: One time 300 mg intravenous course of doses on days 1 and 15.
or Continuation therapy for ocrelizumab when meeting all of the
following: - Patient has previously received treatment with ocrelizumab;
and - Documentation of positive clinical response to ocrelizumab
therapy; and

53 Oxford® Policy Update Bulletin: May 2018
Clinical Policy Updates
Oxford
Policy Title Effective Date Summary of Changes Coverage Rationale
REVISED
Ocrevus™ (Ocrelizumab) (continued)
Jun. 1, 2018 - Patient is not receiving ocrelizumab in combination with any of the following: Disease modifying therapy (e.g., interferon beta
preparations, daclizumab, dimethyl fumarate, glatiramer acetate, natalizumab, fingolimod, or teriflunomide)
B cell targeted therapy (e.g., rituximab, belimumab,
ofatumumab) Lymphocyte trafficking blockers (e.g., alemtuzumab,
mitoxantrone) and
- Continued dosing: One 600 mg intravenous dose every 6 months.
Ocrevus is unproven and not medically necessary for the treatment of: Lupus nephritis
Rheumatoid arthritis Systemic lupus erythematosus
Orencia® (Abatacept) Injection for Intravenous Infusion
Jun. 1, 2018
Revised conditions of coverage/precertification requirements; added language to indicate: o Requests for hospital
outpatient facility infusion of Orencia require additional precertification with review by a Medical Director or their designee; refer to the policy titled Specialty Medication
Administration - Site of Care
Review Guidelines
This policy refers to Orencia (abatacept) injection for intravenous infusion. Orencia is proven and medically necessary for the treatment of: Polyarticular juvenile idiopathic arthritis when all of the following
criteria are met:
o Diagnosis of moderately to severely active polyarticular juvenile idiopathic arthritis (PJIA); and
o Orencia is initiated and titrated according to US Food and Drug Administration labeled dosing for polyarticular juvenile idiopathic arthritis up to a maximum of (or equivalent dose and interval schedule):
10mg/kg every 4 weeks for patients weighing <75kg
1,000mg every 4 weeks for patients weighing ≥75kg and
o Member is not receiving Orencia in combination with either of the following: Biologic disease-modifying antirheumatic drug (DMARD) [e.g.,
Enbrel (etanercept), Humira (adalimumab), Cimzia (certolizumab), Simponi (golimumab)]
Janus kinase inhibitor [e.g., Xeljanz (tofacitinib)] Rheumatoid arthritis when all of the following criteria are met:

54 Oxford® Policy Update Bulletin: May 2018
Clinical Policy Updates
Oxford
Policy Title Effective Date Summary of Changes Coverage Rationale
REVISED
Orencia® (Abatacept) Injection for
Intravenous Infusion (continued)
Jun. 1, 2018
o Diagnosis of moderately to severely active rheumatoid arthritis; and o Orencia is initiated and titrated according to US Food and Drug
Administration labeled dosing for rheumatoid arthritis up to a
maximum of (or equivalent dose and interval schedule): 500mg every 4 weeks for patients weighing <60kg 750mg every 4 weeks for patients weighing 60kg to 100kg
1,000mg every 4 weeks for patients weighing >100kg and
o Member is not receiving Orencia in combination with either of the following:
Biologic DMARD [e.g., Enbrel (etanercept), Humira (adalimumab), Cimzia (certolizumab), Simponi (golimumab)]
Janus kinase inhibitor [e.g., Xeljanz (tofacitinib)] Psoriatic arthritis when all of the following criteria are met:
o Diagnosis of active psoriatic arthritis (PsA); and o Orencia is initiated and titrated according to US Food and Drug
Administration labeled dosing for psoriatic arthritis up to a maximum of (or equivalent dose and interval schedule):
500mg every 4 weeks for patients weighing <60kg 750mg every 4 weeks for patients weighing 60kg to 100kg 1,000mg every 4 weeks for patients weighing >100kg and
o Patient is not receiving Orencia in combination with any of the
following: Biologic DMARD [e.g., Enbrel (etanercept), Humira
(adalimumab), Cimzia (certolizumab), Simponi (golimumab)]
Janus kinase inhibitor [e.g., Xeljanz (tofacitinib)]
Phosphodiesterase 4 (PDE4) inhibitor [e.g., Otezla (apremilast)]
Orencia is unproven and not medically necessary for the treatment
of: Multiple sclerosis Systemic lupus erythematosus Graft versus host disease (GVHD) Uveitis associated with Behçet's disease

55 Oxford® Policy Update Bulletin: May 2018
Clinical Policy Updates
Oxford
Policy Title Effective Date Summary of Changes Coverage Rationale
REVISED
Preventive Care Services
Jun. 1, 2018
Revised coverage rationale for Women’s Health; added language to indicate the
following services are covered under the Preventive Care Services benefit effective Jun. 1,
2018: o Screening for diabetes
mellitus for those with a history of gestational
diabetes o Screening for urinary
continence, annually Revised list of applicable
procedure and diagnosis codes for:
Preventive Care Services
Diabetes Screening
o Updated service description; added instruction to refer to the Screening for Diabetes Mellitus After Pregnancy section of policy for
information on additional diabetes screening benefits
Gestational Diabetes Mellitus
Screening o Updated service description;
added instruction to refer to
the Screening for Gestational Diabetes Mellitus and Screening for Diabetes Mellitus After Pregnancy
sections of policy for information on additional diabetes screening benefits
Wellness Examinations
o Updated service description/language
Refer to the policy for complete details on the coverage guidelines for Preventive Care Services.

56 Oxford® Policy Update Bulletin: May 2018
Clinical Policy Updates
Oxford
Policy Title Effective Date Summary of Changes Coverage Rationale
REVISED
Preventive Care Services (continued)
Jun. 1, 2018
pertaining to Health Resources and Services Administration (HRSA)
coverage requirements; added “screening for urinary incontinence” to list of
services included in codes for wellness examinations
Expanded Women’s
Preventive Health
Screening for Gestational
Diabetes Mellitus o Updated service description;
added instruction to refer to the Screening for Diabetes Mellitus After Pregnancy
section of policy for
additional information
Screening for Diabetes Mellitus After Pregnancy (new to policy)
o Added service description to indicate: The Women’s Preventive
Services Initiative [HRSA Requirement (Dec. 2017)] recommends:
Women with a history of gestational diabetes mellitus
(GDM) who are not currently pregnant and who have not previously been
diagnosed with type 2 diabetes mellitus should be screened for diabetes mellitus
Initial testing should ideally occur within

57 Oxford® Policy Update Bulletin: May 2018
Clinical Policy Updates
Oxford
Policy Title Effective Date Summary of Changes Coverage Rationale
REVISED
Preventive Care Services (continued)
Jun. 1, 2018
the first year postpartum and can be conducted as
early as 4-6 weeks postpartum
Women with a
negative initial postpartum screening test result should be rescreened
at least every 3 years for a minimum of 10 years after pregnancy
See the Gestational Diabetes Mellitus
Screening, Diabetes Screening, and
Screening for Gestational Diabetes Mellitus sections of policy for additional information
o Added list of applicable CPT
codes: 36415, 36416, 82947, 82948, 82950, 82951, 82952, and 83036
o Added list of applicable ICD-10 diagnosis codes: Z00.00, Z00.01, or
Z13.1; and
Z86.32 o Added preventive benefit
instructions to indicate: The service is payable
when the listed diagnosis code requirements are
met No benefit age limit
applies

58 Oxford® Policy Update Bulletin: May 2018
Clinical Policy Updates
Oxford
Policy Title Effective Date Summary of Changes Coverage Rationale
REVISED
Preventive Care Services (continued)
Jun. 1, 2018
CPT codes 36415 and 36416 are payable when billed with all of the
following: One of the
[listed/required]
diabetes screening procedure codes; and
The [listed/required]
diagnosis codes If a diabetes diagnosis
code is present in any position, the preventive benefit will not be applied; see the list of
applicable diabetes diagnosis codes
Screening for Urinary Incontinence (new to policy)
o Added service description to indicate the Women’s Preventive Services Initiative recommends screening women for urinary incontinence annually
o Added instruction to see the Wellness Examinations section of the policy for
applicable codes and preventive benefit instructions
Updated supporting information
to reflect the most current references

59 Oxford® Policy Update Bulletin: May 2018
Clinical Policy Updates
Oxford
Policy Title Effective Date Summary of Changes Coverage Rationale
REVISED
Radicava™ (Edaravone)
Jun. 1, 2018 Updated list of related policies; added reference link to the policy titled Specialty Medication
Administration - Site of Care Review Guidelines
Revised conditions of
coverage/precertification requirements; added language to indicate: o Requests for hospital
outpatient facility infusion of Radicava require additional precertification with review by a Medical Director or their designee; refer to the policy titled Specialty Medication
Administration - Site of Care Review Guidelines
Updated coverage rationale; reformatted/clarified coverage criterion addressing applicable diagnosis and treating physician
Radicava (edaravone) is proven and medically necessary for the treatment of amyotrophic lateral sclerosis (ALS) in patients who meet all of the following criteria:
For initial therapy, all of the following: o Submission of medical records (e.g., chart notes, previous medical
history, diagnostic testing including: imaging, nerve conduction
studies, laboratory values) to support the following: Diagnosis of “definite” or “probable” ALS per the EL Escorial / revised Airlie House diagnostic criteria, and prescribed by, or in consultation with, a neurologist with expertise in the diagnosis of ALS; and
o Submission of the most recent ALS Functional Rating Scale-Revised (ALSFRS-R) score confirming that the patient has scores ≥ 2 in all items of the ALSFRS-R criteria at the start of treatment; and
o Submission of medical records (e.g., chart notes, laboratory values) confirming that the patient has a % forced vital capacity (%FVC) ≥ 80% at the start of treatment; and
o Radicava dosing for ALS is in accordance with the United States Food and Drug Administration approved labeling; and
o Initial authorization will be for no more than 6 cycles (64 doses over 168 days).
For continuation therapy, all of the following: o Diagnosis of “definite” or “probable” ALS per the revised EL Escorial
and Airlie House diagnostic criteria, and prescribed by, or in
consultation with, a neurologist with expertise in the diagnosis of ALS; and
o Patient is currently receiving Radicava therapy; and o Patient is not dependent on invasive ventilation or tracheostomy;
and o Radicava dosing for ALS is in accordance with the United States Food
and Drug Administration approved labeling; and
o Authorization will be for no more than 6 cycles (60 doses over 168 days).
Radiology Procedures Requiring Precertification for eviCore healthcare
Arrangement
Jun. 1, 2018
Reformatted and revised the Oxford Radiology Prior Notification/Authorization Crosswalk Table: o Transferred content to
embedded Excel file format o Added language to indicate
Refer to the policy for complete details on Radiology Procedures Requiring Precertification for eviCore healthcare Arrangement.

60 Oxford® Policy Update Bulletin: May 2018
Clinical Policy Updates
Oxford
Policy Title Effective Date Summary of Changes Coverage Rationale
REVISED
Radiology Procedures Requiring
Precertification for eviCore healthcare Arrangement
(continued)
Jun. 1, 2018 precertification given with CPT code 74177 will be allowed for claims submitted
with CPT codes 72194 and 74170
Simponi Aria® (Golimumab) Injection for
Intravenous Infusion
Jun. 1, 2018
Revised conditions of coverage/precertification requirements; added language
to indicate: o Requests for hospital
outpatient facility infusion of Simponi-Aria require additional precertification with review by a Medical Director or their designee;
refer to the policy titled Specialty Medication Administration - Site of Care Review Guidelines
This policy refers only to Simponi Aria (golimumab) injection for intravenous infusion for the treatment of ankylosing spondylitis, psoriatic arthritis, and rheumatoid arthritis. Simponi, for self-administered subcutaneous injection,
is obtained under the pharmacy benefit and is indicated in the treatment of rheumatoid arthritis, psoriatic arthritis, ankylosing spondylitis and ulcerative colitis. Simponi Aria is proven and/or medically necessary for the treatment of: Ankylosing spondylitis when all of the following criteria are met:
o Diagnosis of active ankylosing spondylitis (AS); and o Simponi Aria is initiated and titrated according to US Food and Drug
Administration labeled dosing for ankylosing spondylitis, up to a maximum of 2mg/kg every 8 weeks (or equivalent dose and interval schedule); and
o Patient is not receiving Simponi Aria in combination with either of
the following: Biologic disease-modifying antirheumatic drug (DMARD) [e.g.,
Enbrel (etanercept), Humira (adalimumab), Cimzia (certolizumab), Orencia (abatacept)]
Janus kinase inhibitor [e.g., Xeljanz (tofacitinib)] Psoriatic arthritis when all of the following criteria are met:
o Diagnosis of active psoriatic arthritis (PsA); and
o Simponi Aria is initiated and titrated according to US Food and Drug Administration labeled dosing for psoriatic arthritis up to a maximum of 2mg/kg every 8 weeks (or equivalent dose and interval schedule); and
o Patient is not receiving Simponi Aria in combination with either of the following: Biologic disease-modifying antirheumatic drug (DMARD) [e.g.,
Enbrel (etanercept), Humira (adalimumab), Cimzia (certolizumab), Orencia (abatacept)]

61 Oxford® Policy Update Bulletin: May 2018
Clinical Policy Updates
Oxford
Policy Title Effective Date Summary of Changes Coverage Rationale
REVISED
Simponi Aria® (Golimumab) Injection for
Intravenous Infusion (continued)
Jun. 1, 2018 Janus kinase inhibitor [e.g., Xeljanz (tofacitinib)] Phosphodiesterase 4 (PDE4) inhibitor [e.g., Otezla (apremilast)]
Rheumatoid arthritis when all of the following criteria are met:
o Diagnosis of moderately to severely active rheumatoid arthritis (RA); and
o One of the following:
Patient is receiving concurrent therapy with methotrexate History of contraindication or intolerance to methotrexate and
o Simponi Aria is initiated and titrated according to US Food and Drug
Administration labeled dosing for rheumatoid arthritis up to a maximum of 2mg/kg every 8 weeks (or equivalent dose and interval schedule); and
o Patient is not receiving Simponi Aria in combination with either of the following: Biologic disease-modifying antirheumatic drug (DMARD) [e.g.,
Enbrel (etanercept), Humira (adalimumab), Cimzia (certolizumab), Orencia (abatacept)]
Janus kinase inhibitor [e.g., Xeljanz (tofacitinib)]

62 Oxford® Policy Update Bulletin: May 2018
Administrative Policy Updates
Oxford
Policy Title Effective Date Administrative Guidelines
NEW
New York & Connecticut Participating
Surgeons Using Non- Participating Providers for
Intraoperative Neuro-Monitoring (IONM)
Jun. 1, 2018
Notice of Revision: The following Administrative Policy has been modified; revisions to the original policy update announcement are outlined in red below. Please take note of the amended guidelines to be applied beginning Jun. 1, 2018.
NY and CT Participating Providers Using Non-Participating IONM Providers
The following procedures and responsibilities apply to Participating Providers located in NY and CT when providing services to members enrolled on NY and/or CT products in an outpatient or inpatient facility setting that involve
intraoperative neuro-monitoring (IONM). Services performed by a Participating Provider located in NY or CT and meeting the following criteria must ensure that the IONM provider utlized is participating with the Oxford network. Member is enrolled on a NY or CT product; and Service is being provided in an outpatient or inpatient facility setting; and Involve intraoperative neuro-monitoring (IONM).
Outpatient and Inpatient Facility Place Codes
Place Code Description
15 Mobile diagnostic unit
19 Off campus - outpatient hospital
21 Inpatient Hospital
22 On campus - outpatient hospital
24 Ambulatory surgical center
99 Other unlisted factilty
If the Participating Provider intends to utilize an IONM provider that does not participate in the Oxford network, the provider is required to: Verbally discuss options and financial impact with the Member
o The Participating Provider must review this policy and the Non-Participating Provider Consent Form with the Member. The discussion must explain Participating and Non-Participating IONM Provider alternatives and provide
the Member with an understanding of all the providers involved in the Member’s care. The discussion must include a conversation explaining the financial impact of using a Non-Participating
IONM Provider. A copy of the Non-Participating Provider Consent Form must be provided to the Member.
o The discussion must occur no more than 90 days, and no less than 14 days before, the scheduled date of the procedure.
o If the Member does not sign the form at the end of the discussion, explain that it needs to be completed and

63 Oxford® Policy Update Bulletin: May 2018
Administrative Policy Updates
Oxford
Policy Title Effective Date Administrative Guidelines
NEW
New York & Connecticut Participating
Surgeons Using Non- Participating Providers for
Intraoperative Neuro-Monitoring (IONM) (continued)
Jun. 1, 2018
returned no less than 14 days before the scheduled date of the procedure. o The discussion must then be noted in the Member’s medical record.
Obtain a completed Non-Participating Provider Consent Form
o The member will need to agree or disagree to receive IONM services from a Non-Participating Provider by marking the appropriate box on the Non-Participating Provider Consent Form. The member must then sign and date the form and return the form to the Participating Provider no less than 14 days before the
scheduled date of the procedure. If the Member: Does not agree to the use of a Non-Participating IONM Provider: Following the discussion, if the
Participating Provider: - Is unable to locate a Participating IONM Provider, they must contact the health plan for assistance in
locating a Participating IONM Provider. - Still wants to recommend the Non-Participating IONM Provider, they must contact Oxford to request
and initiate an In-Network Exception request. Does agree to the use of a Non-Participating IONM Provider: The Participating Provider must
ensure that the Member understands the financial obligations of using a Non-Participating IONM Provider.
- For Members with out-of-network benefits: Non-Participating IONM Providers will be paid at the out-of-network benefit level. Out-of-network cost shares and deductibles will apply. In addition,
Members may be responsible to the Non-Participating IONM Provider for any amount above the amount paid by the health plan, as determined by the Member’s out-of-network benefit; or
- For Members with only in-network benefits: Non-Participating IONM Provider claims will be denied because the Member has no coverage for services provided by Non-Participating Providers. Members will therefore be responsible for the entire cost of the service(s).
o The Participating Provider must then sign and date the form to acknowledge the Member’s decision. o The Non-Participating Provider Consent Form must be kept on file by the Participating Provider. o A separate Non-Participating Provider Consent Form is required for every service when the Participating
Provider wants to refer to or involve a Non-Participating IONM Provider in a member’s care. o The Non-Participating Provider Consent Form will only be valid for 90 days from the date of member
signature.
o Oxford may request a copy of the completed Non-Participating Provider Consent Form from the Participating
Provider (who is required to keep the form on file) in order to conduct standard business. When requested, the Participating Provider must provide a copy of the Non-Participating Provider
Consent Form within 15 days of the request. If a copy of the completed Non-Participating Provider Consent Form is not received within 15 days of the
request, the Participating Provider’s claim will be denied administratively for failure to comply with this protocol.
In these instances, the Participating Provider is prohibited from balance billing the Member. Any payment previously made for the surgical service will be subject to recovery. The Participating
provider cannot balance bill the member for claims denied for administrative reasons.

64 Oxford® Policy Update Bulletin: May 2018
Administrative Policy Updates
Oxford
Policy Title Effective Date Administrative Guidelines
NEW
New York & Connecticut Participating
Surgeons Using Non- Participating Providers for
Intraoperative Neuro-Monitoring (IONM) (continued)
Jun. 1, 2018 Participating IONM Providers
When a Participating Provider performs services in an outpatient or inpatient facility setting using a Participating IONM Provider, there will be no additional requirements to fulfill. A Non-Participating Provider Consent Form is not required.
Non-Compliance With This Policy
Oxford may request a copy of the completed Non-Participating Provider Consent Form from the Participating Provider
(who is required to keep the form on file) in order to conduct standard business. When requested: The Participating Provider must provide a copy of the Non-Participating Provider Consent Form within 15 days of
the request. If a copy of the completed Non-Participating Provider Consent Form is not received within 15 days of the
request, as proof that they discussed the member’s options for selecting a Participating or Non-Participating IONM Provider, in advance of the service, the Participating Provider’s claim will be denied administratively for failure to comply with the protocol.
In these instances, the Participating Provider is prohibited from balance billing the member. Any payment previously made for the service will be subject to recovery. The Participating Provider cannot balance bill the member for claims denied for administrative reasons.
In-Network Exception Requests
If requesting an In-Network Exception to have a Non-Participating IONM Provider covered as if they were participating with the Oxford network, the Participating Provider must make the exception request. The exception request will not be accepted from the Non-Participating IONM Provider. The In-Network Exception request must be made no less than 14 days in advance of the scheduled procedure in
order to avoid delays in care and alleviate potential complications with the patient’s required preparations for the procedure.
If the Participating Provider requests an In-Network Exception less than 14 days in advance of the scheduled procedure, the In-Network Exception request will be processed per Oxford’s standard guidelines, however the Participating Provider will receive an administrative denial for their claim for failure to follow protocol.
Policy Title Effective Date Summary of Changes
UPDATED
Accreditation Requirements for Radiology Services
May 1, 2018 Updated policy guidelines: o Modified list of modalities/procedures for AIUM accreditation; removed echocardiography (previously listed in
error; no change to accreditation guidelines) o Updated reference link to eviCore healthcare Accreditation Fax Cover Sheet; redirected from “Prior
Authorization and Notification App” to “eviCore healthcare website”

65 Oxford® Policy Update Bulletin: May 2018
Administrative Policy Updates
Oxford
Policy Title Effective Date Summary of Changes Administrative Guidelines
REVISED
Ambulance Services
Jun. 1, 2018
Changed policy title; previously titled Transportation Services
Revised conditions of
coverage/precertification guidelines; added language to indicate:
o Precertification with review by a Medical Director or their designee is required for all requests for out-of-the-
country transportation o In the event precertification
for air or water transportation is not feasible due to time constraints related to medical
emergencies, Oxford will require review of clinical
notes post-service and prior to payment
Revised coverage rationale:
o Replaced references to: “Patient” with “member”
“Transportation” with “ambulance”
Emergency Ambulance (Ground, Water, or Air) o Added language to indicate
the following Emergency
ambulance services are covered: Ground ambulance
transportation requiring basic life support or advanced life support
Treatment at the scene
(paramedic services) without ambulance transportation
Note: Refer to Oxford’s Ambulance policy for additional information regarding the reimbursement of ambulance transportation services. Indications for Coverage
Emergency Ambulance (Ground, Water, or Air)
Coverage includes Emergency ambulance transportation (including wait time and treatment at the scene) by a licensed ambulance service from the
location of the sudden illness or injury, to the nearest hospital where services can be performed.
Emergency transportation to an acute care hospital and/or hospital Emergency facility does not require notification, precertification or certification.
The following Emergency ambulance services are covered: Ground ambulance transportation requiring basic life support or
advanced life support
Treatment at the scene (paramedic services) without ambulance transportation
Wait time associated with covered ambulance transportation To a hospital that provides a required higher level of care that was not
available at the original hospital Air Ambulance
As a general guideline, when it would take a ground ambulance 30-60 minutes or more to transport a member whose medical condition at the time of pick-up required immediate and rapid transport due to the nature and/or severity of the member’s illness/injury, air transportation may be appropriate.
Air Ambulance transportation should meet the following criteria: The member’s destination is an acute care hospital, and The member’s condition is such that the ground ambulance (basic or
advanced life support) would endanger the member’s life or health, or Inaccessibility to ground ambulance transport or extended length of time
required to transport the member via ground ambulance transportation
could endanger the member, or Weather or traffic conditions make ground ambulance transportation
impractical, impossible, or overly time consuming.

66 Oxford® Policy Update Bulletin: May 2018
Administrative Policy Updates
Oxford
Policy Title Effective Date Summary of Changes Administrative Guidelines
REVISED
Ambulance Services (continued)
Jun. 1, 2018
Wait time associated with covered ambulance transportation
To a hospital that provides a required higher level of care that
was not available at the original hospital
o Removed duplicative language pertaining to
precertification requirements (see the Conditions of Coverage section of the policy)
Non-Emergency Ambulance (Ground or Air)
o Modified language to indicate coverage includes non-
Emergency ambulance transportation by a licensed ambulance service (either ground or air ambulance, as we determine appropriate)
between facilities only when the transport meets one of the following: From an out-of-Network
Hospital to the closest Network Hospital when
Covered Health Care
Services are required To the closest Network
Hospital or facility that provides the required Covered Health Care Services that were not
available at the original Hospital or facility
From a Short-Term
Additional Information
Emergency ambulance coverage includes supplies that are needed for advanced life support or basic life support to stabilize a member’s medical
condition. Non-Emergency Ambulance (Ground or Air)
Coverage includes Non-Emergency ambulance transportation by a licensed ambulance service (either ground or Air Ambulance), between health care facilities only when the transport meets one of the following: From an out-of-network hospital or facility to the closest Network
hospital when Covered Health Care Services are required. To the closest Network hospital or facility that provides the required
Covered Health Care Services that were not available at the original hospital
From a Short-Term Acute Care Facility to the closest Network Long-Term Acute Care Facility (LTAC), Network Inpatient Rehabilitation Facility, or other Network Sub-Acute facility where the required Covered Health Care
Services can be delivered.
Additional Information
Non-emergent transportation and is covered only when the member’s specific benefit document includes coverage for non-emergent ambulance/transportation and/or coverage is required due to federal or state mandates.
Ambulance transportation that is done for convenience of the patient is not covered. Please see the Coverage Limitations and Exclusions section of the policy for more information on non-covered ambulance
transportation. Coverage Limitations and Exclusions
The following services are not eligible for coverage: Ambulance services from providers that are not properly licensed to be
performing the ambulance services rendered. Air Ambulance transportation that does not meet the covered indications
in the Air Ambulance criteria listed above. Non-ambulance transportation. Non-ambulance transportation is not
covered even if rendered in an Emergency situation. Examples include but are not limited to:

67 Oxford® Policy Update Bulletin: May 2018
Administrative Policy Updates
Oxford
Policy Title Effective Date Summary of Changes Administrative Guidelines
REVISED
Ambulance Services (continued)
Jun. 1, 2018
Acute Care Facility to the closest Network Long-Term Acute Care Facility
(LTAC), Network Inpatient Rehabilitation Facility, or other Network
Sub-Acute Facility where the required Covered Health Care Services can be delivered
o Added reference link to the Coverage Limitations and Exclusions section of the policy for additional information on non-covered ambulance transportation
Coverage Limitations and Exclusions
o Replaced reference to “air ambulance” with “air ambulance transportation”
o Removed language indicating ambulance
transportation that violates the notification criteria listed in the Indications for Coverage section of the policy is not covered
o Modified list of examples of
excluded ambulance
transportation for member convenience or other miscellaneous reasons to reflect/include: Member wants to be at a
certain hospital or facility
for personal/ preference reasons
Member is in foreign
o Commercial or private airline or helicopter o A police car ride to a hospital o Medi-van or wheel chair van transportation
o Taxi ride, bus ride, etc. Ambulance transportation when other mode of transportation is
appropriate. Except as indicated under the Indications for Coverage
section of the policy, ambulance services when transportation by other means would not endanger the member’s health are not covered.
Ambulance transportation to a home, residential, domiciliary or custodial facility is not covered.
Ambulance transportation for member convenience or other miscellaneous reasons for member and/or family. Examples include but are not limited to: o Member wants to be at a certain hospital or facility for
personal/preference reasons o Member is in foreign country, or out of state, and wants to come
home for a surgical procedure or treatment (this includes those recently discharged from inpatient care)
o Member is going for routine service and is medically able to use another mode of transportation
o Member is deceased and family wants transportation to the coroner’s office or mortuary
Ambulance transportation deemed not appropriate. Examples include but
are not limited to: o Hospital to home o Home to physician’s office o Home (e.g., residence, nursing home, domiciliary or custodial
facility) to a hospital for a scheduled service Out-of-Country Transportation
When a member has traveled outside of the United States, Mexico, Canada and the U.S. Territories, Emergency transportation to the nearest hospital
and/or hospital Emergency facility does not require notification, precertification or certification. However, Oxford should be notified of an admission within 48 hours or as soon as possible, consistent with the member's certificate. Refer to the policy titled Emergency Room Visits (Including Coverage for Members Outside of the United States for additional information on coverage

68 Oxford® Policy Update Bulletin: May 2018
Administrative Policy Updates
Oxford
Policy Title Effective Date Summary of Changes Administrative Guidelines
REVISED
Ambulance Services (continued)
Jun. 1, 2018 country, or out of state, and wants to come home for a surgical procedure
or treatment (this includes those recently discharged from
inpatient care) Member is going for a
routine service and is medically able to use
another mode of transportation
Member is deceased and family wants transportation to the coroner’s office or
mortuary Out-of-Country
Transportation o Removed duplicative
language pertaining to precertification requirements (see the Conditions of
Coverage section of the policy)
Updated definitions: o Added definition of
“Emergency” o Removed definition of:
Air Ambulance
Fixed Wing Aircraft Rotary Wing Aircraft
Updated list of applicable HCPCS
codes; revised description for
A0427
for services received outside of the United States, Mexico, Canada, and the U.S. Territories.

69 Oxford® Policy Update Bulletin: May 2018
Reimbursement Policy Updates
Oxford
Policy Title Effective Date Summary of Changes
UPDATED
Maximum Frequency Per Day
May 7, 2018 Updated Maximum Frequency Per Day Code List (attachment file designating the maximum frequency per day value assignments for CDT, CPT, and HCPCS codes) to reflect quarterly code edits:
o Added 0012M, 0013M, 0035U, 0036U, 0037U, 0038U, 0039U, 0040U, 0041U, 0042U, 0043U, 0044U, 0492T, 34711, 64913, 86008, 99494, A4225, A9515, A9587, E0953, E0954, J1428, J1555, J1726, J2182, J2326, J2350, J2786, K0903, Q2041, Q5103, and Q5104
o Revised value assignments for 0394T, 0395T, 0398T, 0450T, 22854, 22859, 23101, 64636, 74713, 93592,
95886, A0384, A0392, A0396, A0422, A4224, A4337, A5200, A9575, B4081, B4082, B4083, B4164, B4172, B4176, B4178, B4180, H0003, J0638, J1575, and J3060
Updated list of Codes Restricting Modifiers LT and RT (attachment file listing codes that allow up to the MFD limit
with "bilateral" or "unilateral or bilateral" in the description or where the concept of laterality does not apply) to reflect quarterly code edits; added 0012M, 0013M, 0035U, 0036U, 0037U, 0038U, 0039U, 0040U, 0041U, 0042U, 0043U, 0044U, Q2041, Q5103, and Q5104
Services and Modifiers Not Reimbursable to Healthcare
Professionals
May 7, 2018
Updated list of Status E and X Codes to reflect quarterly code edits; added G9873, G9874, G9875, G9876, G9877, G9878, G9879, G9880, G9881, G9882, G9883, G9884, G9885, G9890, and G9891





























