Embed Size (px)
Citation preview

NEWBORN METABOLIC SCREENING INITIATIVE: ACTION PLAN REPORT, NOVEMBER 30, 2010 (FINAL)
Page 1 of 71
NEWBORN METABOLIC SCREENING INITIATIVE: ACTION PLAN REPORT
Maximizing Opportunities for Newborn Metabolic Screening: Quality, Performance, Action
Respectfully Submitted by:
Alberta Heath Services Provincial Newborn Metabolic Screening Steering Committee
Population and Public Health November 30, 2010 (FINAL)

NEWBORN METABOLIC SCREENING INITIATIVE: ACTION PLAN REPORT, NOVEMBER 30, 2010 (FINAL)
Page 2 of 71
NEWBORN METABOLIC SCREENING INITIATIVE: ACTION PLAN REPORT, NOVEMBER 30, 2010 (FINAL)
Page 3 of 71
FORWARD PURPOSE OF THE ACTION PLAN In June 2010, the Alberta Newborn Metabolic Screening Program Policy Document, March 2010 (2010 NMS Policy Document1
to continue to offer the Newborn Metabolic Screening Program (NMS) to all Albertans and their infant children in accordance with the policies and standards of the NMS program, as set out in the “Alberta Newborn Metabolic Screening Program Policy Document” dated March 2010 (Alberta Health and Wellness, directive from J.G. Ramator, Deputy Minister of Health and Wellness to Alberta Health Services).
) was received by Alberta Health Services (AHS) as a directive from Alberta Health and Wellness (AHW) (see Appendix A). As a response to the directive, AHS presents the Newborn Metabolic Screening Initiative: Action Plan Report (Action Plan). The purpose of the Action Plan is to demonstrate AHS’ ongoing commitment
The Action Plan outlines the actions recommended by AHS to address the standards and sub-standards in the 2010 NMS Policy Document and serves as the foundation for a comprehensive Newborn Metabolic Screening (NMS) Program in Alberta. In addition, the Action Plan addresses the areas for improvement identified in the 2009 NMS Audits conducted by AHS and AHW.
ORGANIZATION OF ACTION PLAN An Executive Summary is provided on page 4 and includes an overview and summary of the:
Newborn Metabolic Screening Initiative Development of the Action Plan Proposed NMS Program Operational Model Recommended Action Plan and Implementation Budget estimates
Within the body of the report, the Action Plan is organized into eight main sections (noted in bold). Background Information is provided on newborn metabolic screening, the 2009 NMS Audits, and the formation of the Newborn Metabolic Screening Initiative. The Current State of the NMS Program is illustrated by an overview of the Newborn Metabolic Screening Pathway, available NMS Program performance measurement data, and a synopsis of the action planning process. An Operational Model is proposed comprised of a Quality Management Framework and an Action Plan Governance Structure. An Action Plan is outlined with an overview of recommended actions and a detailed action chart including sub-actions, roles, dependencies, and timelines. A staged approach to Implementation and the Future State are described, and an Evaluation Plan is included. The Budget Estimate provides a high-level summary of the incremental costs required to improve and integrate the NMS Program across Alberta to meet the 2010 NMS Policy Document standards and sub-standards.
NEWBORN METABOLIC SCREENING INITIATIVE: ACTION PLAN REPORT, NOVEMBER 30, 2010 (FINAL)
Page 4 of 71
TABLE OF CONTENTS Forward ......................................................................................................................................................... 3
Purpose of the Action Plan .................................................................................................................... 3 Organization of Action Plan ................................................................................................................... 3
Executive Summary ...................................................................................................................................... 5 Background ................................................................................................................................................... 6
Newborn Metabolic Screening .............................................................................................................. 6 Developmental Timelines ...................................................................................................................... 6 Newborn Metabolic Screening Initiative ................................................................................................ 7
Current State ................................................................................................................................................. 9 NMS Program Responsibilities ............................................................................................................. 9 Newborn Metabolic Screening Pathway ............................................................................................. 10 NMS Program Performance Measurement ......................................................................................... 11 Development of the Action Plan .......................................................................................................... 13
Operational Model ....................................................................................................................................... 17 NMS Program Quality Management Framework ................................................................................ 17 Action Plan Governance Structure ...................................................................................................... 18
Action Plan .................................................................................................................................................. 21 Overview of Actions ............................................................................................................................ 21
Implementation ............................................................................................................................................ 32 Implementation Exemplars .................................................................................................................. 32 Staged Approach to Implementation ................................................................................................... 32
Future State ............................................................................................................................................... 34 Evaluation Plan ........................................................................................................................................... 35
Current Performance Measurement and Evaluation........................................................................... 35 Future Performance Measurement and Evaluation ............................................................................ 35 Reporting to Alberta Health and Wellness .......................................................................................... 35
Budget Estimate .......................................................................................................................................... 36 High Level Budget Estimate ................................................................................................................ 36
Conclusion................................................................................................................................................... 38 References .................................................................................................................................................. 39 Appendices…………………………………………………………………………………………………............41

NEWBORN METABOLIC SCREENING INITIATIVE: ACTION PLAN REPORT, NOVEMBER 30, 2010 (FINAL)
Page 5 of 71
EXECUTIVE SUMMARY The purpose of the Newborn Metabolic Screening (NMS) Program is to offer timely screening to all infants born in Alberta. Early detection and treatment reduces morbidity and mortality, and can make the difference between healthy development and lifelong impairment.
Alberta Health Services (AHS) developed the Newborn Metabolic Screening Initiative: Action Plan Report (Action Plan) in response to a directive from Alberta Health and Wellness (AHW). The goals of the Action Plan are to ensure integration and coordination along the Newborn Metabolic Screening Pathway and to improve NMS Program infrastructure, processes, outputs, and outcomes. The Newborn Metabolic Screening Pathway includes registration, sample collection, transportation, analysis, reporting, follow-up and work-up.
The Action Plan was created with extensive enterprise-wide consultation as Phase One of the Newborn Metabolic Screening Initiative. The plan outlines the 16 actions and 60 sub-actions recommended to address the standards and sub-standards in the Alberta Newborn Metabolic Screening Program Policy Document, March 2010 (2010 NMS Policy Document2
An Operational Model is proposed which consists of a NMS Program Quality Management (QM) Framework and a supporting NMS Action Plan Governance Structure. The purpose of the NMS Program QM Framework is to maximize screening opportunities and reduce the risk of missing a newborn, screen, result, and/or follow-up. The Governance Structure includes Steering and Implementation Committees and Interdisciplinary Project Teams.
), serves as the foundation for a comprehensive NMS Program, and addresses the areas for improvement identified in the 2009 NMS Audits.
A staged approach to implement the Action Plan is recommended based on priorities, interdependencies, timelines, funding, and infrastructure. Implementation of the Action Plan in Year 1 (2011-2012) is estimated to be $2,498,000 and includes approximately $1,518,700 of one-time project costs and $979,200 recurring costs. In Year 2 (2012-2013), the estimated cost drops to $1,482,090. The annualized on-going cost of the Action Plan is estimated to be $1,331,300 for year 3 and beyond.
Achieving the Action Plan deliverables will require a collaborative effort across AHS and strong partnerships with AHW, First Nations Inuit Health - Alberta Region (FNIH), physicians, registered midwives, nurse practitioners, and parents/guardians. Many of these actions are interdependent and will require extensive coordination by the NMS Action Plan Implementation Committee and the NMS Interdisciplinary Project Teams under the umbrella of the Steering Committee. Success will be measured by the number of deliverables completed on time, projects coming in on budget, the number of standards and sub-standards achieved, and the integration of the NMS Program Quality Management Framework and Action Plan Governance Structure in all aspects of the NMS Program.
NEWBORN METABOLIC SCREENING INITIATIVE: ACTION PLAN REPORT, NOVEMBER 30, 2010 (FINAL)
Page 6 of 71
BACKGROUND NEWBORN METABOLIC SCREENING Every year, a small number of infants are born with metabolic diseases that can result in physical disabilities, developmental delays, other health problems, and in some instances, death.3
While relatively rare, some disorders included in newborn metabolic screen manifest early in life. Without timely screening and intervention, infants affected with these disorders will become ill and may suffer irreversible brain damage soon after birth. Between April 1, 2007 and March 31, 2010, 163 infants in Alberta had a confirmed diagnosis as a result of newborn metabolic screening.
In Alberta, the Newborn Metabolic Screening (NMS) Program screens for 17 inherited disorders (14 metabolic disorders, 2 endocrine disorders, and cystic fibrosis). The purpose of this population-based screening program is to offer timely screening to all infants born in Alberta and facilitate early recognition and treatment of these disorders before the onset of clinical symptoms.
4
Population-based newborn metabolic screening reduces the financial burden associated with providing long term care to infants or children diagnosed with one of these disorders. If left untreated, the cost to the individual, their family, the health care system, and society can be sizeable.
Early detection and treatment reduces morbidity and mortality, and can make the difference between healthy development and lifelong impairment.
For every case of PKU detected through early screening, it has been estimated that about $293,000 in long-term care costs are avoided. Overall in Alberta, the early detection of metabolic disorders through the NMS screening program helps reduce long term costs of affected children by an estimated $700,000 per year. 5
DEVELOPMENTAL TIMELINES
The NMS Program began in Alberta in 1967 with the introduction of screening for phenylketonuria (PKU). In 1977, screening for congenital hypothyroidism was added to the testing menu, and in 1990 screening for biotinidase deficiency became part of the routine screen.6 In April 2007, Alberta Health and Wellness (AHW) expanded the NMS Program to include 17 inherited disorders.7
AHW has been, and continues to be responsible for setting the overall strategic direction for the NMS Program. Until April 2009, nine Regional Health Authorities (RHAs) were responsible for the delivery of services related to NMS screening, follow-up, and treatment services.
Since the merger into one provincial health authority, Alberta Health Services (AHS) has assumed the NMS Program roles and responsibilities of the former RHAs.
In June 2009, AHW and AHS Health Promotion, Disease and Injury Prevention (HPDIP) within Population and Public Health (PPH) completed a collaborative record audit related to newborn metabolic screening. Later that year, an individual case audit was conducted by AHW and HPDIP related to a delay in screening and follow-up.

NEWBORN METABOLIC SCREENING INITIATIVE: ACTION PLAN REPORT, NOVEMBER 30, 2010 (FINAL)
Page 7 of 71
A number of re-occurring concerns emerged during the NMS 2009 Audits, demonstrating a need to make improvements in the following areas8
Data management
:
Documentation processes Communication with other program partners [First Nations Inuit Health - Alberta Region
(FNIH), primary care providers including registered midwives] Transportation Consistency of processes across the former RHAs
In early 2010, a NMS Steering Committee was established to address the audit concerns and work toward the development, implementation, and evaluation of standardized provincial operational policies and procedures related to NMS sample collection.
On April 30th, 2010, AHW released the Alberta Newborn Metabolic Screening Program Policy Document, March 2010 (2010 NMS Policy Document9). In June 2010, the 2010 NMS Policy Document came from AHW as a directive to AHS. The standards and sub-standards set forth in the 2010 NMS Policy Document exceeded the scope of the 2008 AHW NMS standards10
NEWBORN METABOLIC SCREENING INITIATIVE
in detailing the roles and responsibilities of AHS. It was determined addressing the 2010 NMS Policy Document exceeded the mandate of the original NMS Steering Committee. As a result, the NMS Steering Committee established in early 2010 was disbanded June 30, 2010. A new AHS NMS Provincial Steering Committee was convened in July 2010 to address the scope of the 2010 NMS Policy Document through the Newborn Metabolic Screening Initiative.
The overarching goal of the Newborn Metabolic Screening Initiative is to build a comprehensive, enterprise-wide NMS Program that achieves the standards and sub-standards set forth in the 2010 NMS Policy Document. AHS has developed a four phase strategy to achieve this goal.
In Phase One, key stakeholders have worked collaboratively to develop a Newborn Metabolic Screening Initiative: Action Plan Report (Action Plan) to improve NMS Program service delivery and program coordination in order to meet the 2010 NMS Policy Document standards and sub-standards. The Action Plan is the foundation for the development of a comprehensive NMS Program over time. Issues pertaining to the NMS Program identified during the Action Plan Phase, not related to attaining the 2010 NMS Policy Document standards and sub-standards, were deemed out of scope for Phase One and will be further assessed and addressed during subsequent phases of this initiative. Phase Two will focus on implementation of the Action Plan and will commence January 2011. Phase Three will focus on program evaluation, with program maintenance beginning in Phase Four. Timelines for Phases Three and Four will be determined in the Implementation Phase.
Phase 1 Action Plan Oct 31 2010
Phase 2 Implementation
Jan 2011
Phase 3 Program
Evaluation
Phase 4 Program
Maintenance
NEWBORN METABOLIC SCREENING INITIATIVE: ACTION PLAN REPORT, NOVEMBER 30, 2010 (FINAL)
Page 8 of 71
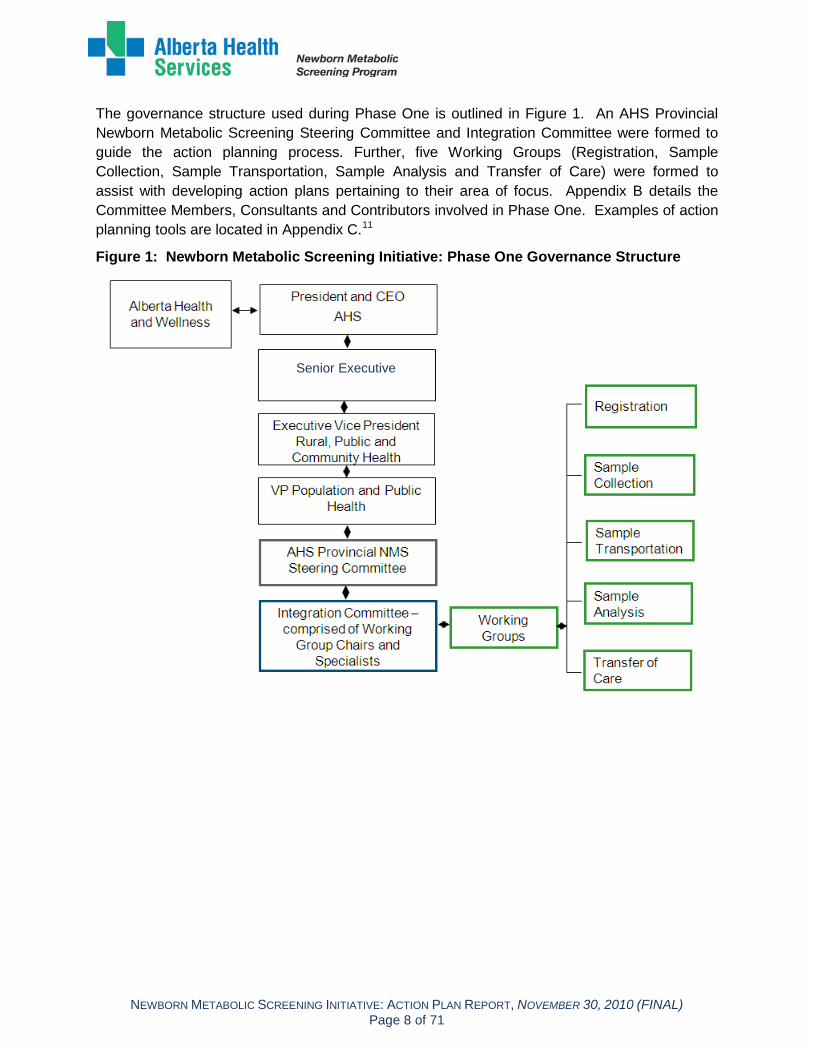
The governance structure used during Phase One is outlined in Figure 1. An AHS Provincial Newborn Metabolic Screening Steering Committee and Integration Committee were formed to guide the action planning process. Further, five Working Groups (Registration, Sample Collection, Sample Transportation, Sample Analysis and Transfer of Care) were formed to assist with developing action plans pertaining to their area of focus. Appendix B details the Committee Members, Consultants and Contributors involved in Phase One. Examples of action planning tools are located in Appendix C.11
Figure 1: Newborn Metabolic Screening Initiative: Phase One Governance Structure
Senior Executive

NEWBORN METABOLIC SCREENING INITIATIVE: ACTION PLAN REPORT, NOVEMBER 30, 2010 (FINAL)
Page 9 of 71
CURRENT STATE NMS PROGRAM RESPONSIBILITIES The NMS Program is a collaborative program between AHW, AHS, FNIH, and primary care providers, including physicians, nurse practitioners, and registered midwives. Responsibilities within the NMS Program are as follows: AHW is responsible for setting the policies and standards for the program including
determining the disorders screened for, monitoring compliance with 2010 NMS Policy Document, and maintaining the NMS Application. AHW may also perform program surveillance.
AHS HPDIP is responsible for the overall coordination of the NMS Program within AHS including monitoring and reporting on program performance as directed by AHW.
FNIH is responsible for services to their clients located in First Nations communities including specimen collection, recollection, documentation, and transportation of the specimen to the NMS Laboratory (NMS Lab) in Edmonton.
Within AHS, service delivery models and mechanisms vary across Zones. Responsibilities for the NMS Program are enterprise-wide and include the following areas:
Parents/Guardians are responsible for providing informed consent for their infant’s newborn metabolic screening as per the AHS Consent to Treatment/Procedure(s) Policy PRR-01 and AHS Consent to Treatment/Procedure(s): Minors/Mature Minors Policy PRR-01-03.
Health Information Management (HIM) in each Zone is responsible for registering newborns in Person Directory (PD) and creating Unique Lifetime Identifiers (ULIs) for all newborns born in Alberta.
Hospital Lab Services and Postpartum Units in each Zone are responsible for providing NMS information to parents/guardians and collecting the NMS sample from newborns in hospital at or after 24 hrs of age and before 72 hours of age.
Neonatal Intensive Care Units/Special Care Nurseries (NICU/SCN) in each Zone are responsible for providing NMS information to parents/guardians, collecting the NMS sample from newborns in the NICU/SCN after 24 hrs of age, as well as conducting any necessary sample recollections.
Public Health Nursing Services in each Zone are responsible for providing NMS information to parents/guardians; determining if the NMS sample collection occurred in hospital; arranging for/or carrying out sample collection in the home, clinic, or lab as needed; delivering the sample to the lab; finding missing data and/or families; and arranging for sample recollection if required.
Community Lab Services in each Zone are responsible for NMS sample collection for newborns not screened in hospital, and referred by public health nursing and/or the postpartum unit.
NEWBORN METABOLIC SCREENING INITIATIVE: ACTION PLAN REPORT, NOVEMBER 30, 2010 (FINAL)
Page 10 of 71
Lab Services in each Zone are responsible for sample transportation to the NMS Lab in Edmonton.
The NMS Lab within the University of Alberta Hospital (UAH) is responsible for sample analysis, monitoring sample quality, providing results to the NMS Application program within AHW and the Electronic Medical Record (NetCare), reporting results and providing consultations to primary care providers and Specialty Clinics regarding appropriate follow-up and confirmatory testing, and reporting the incidence of disorders to AHW.
The Molecular Diagnostic Lab (MD Lab) is responsible for the DNA testing component of sample analysis for cystic fibrosis (CF) screening, and reporting CF results to the NMS Lab.
Children’s Hospitals’ Specialty Clinics and Specialty Diagnostic Laboratories (Endocrinology, Cystic Fibrosis, Metabolic) in Calgary and Edmonton Zones, in collaboration with primary care providers, are responsible for the work-up and follow-up of infants with critical or double borderline results including providing an urgent clinical assessment, arranging for diagnostic testing, making diagnoses, initiating treatment and case management, and notifying the NMS Lab on the outcome of the diagnostic work-up.
Primary care providers [family physicians, pediatricians, nurse practitioners (NPs), registered midwives] are responsible for providing information to parents/guardians, collecting samples in accordance with AHW policies if required (applies to NPs, registered midwives), being involved in the work-up and follow-up of infants with critical or double borderline results including providing an urgent clinical assessment, arranging for diagnostic testing, making diagnoses, initiating treatment and case management as required, and notifying the NMS Lab on the outcome of the diagnostic work-up.
Although a number of AHS Zones and Portfolios currently provide various services within the Newborn Metabolic Screening Pathway, the NMS Program is not coordinated provincially nor integrated within AHS. Access to screening services is not equitable across Alberta, especially for those living in rural and remote communities.
NEWBORN METABOLIC SCREENING PATHWAY The stages of the Newborn Metabolic Screening Pathway as it is currently being delivered across Alberta include:
Registration: When infants are born in Alberta, they are registered in the PD, an Alberta Health Care ULI is created, and a notification of birth is sent to Public Health Nursing within the applicable Zone.
Sample Collection: A blood sample is collected from the newborn by heel prick between 24-72 hours after birth, as close to 24 hours as possible. Collection may occur in the hospital, in a community lab, or by a public health nurse during a home or clinic visit.
Transportation: After collection, the sample is transported to the NMS Lab in Edmonton. Transportation time varies depending on the location.

NEWBORN METABOLIC SCREENING INITIATIVE: ACTION PLAN REPORT, NOVEMBER 30, 2010 (FINAL)
Page 11 of 71
Analysis: Sample analysis is carried out at the NMS Lab in Edmonton to screen for 17 disorders. CF analysis is performed by the MD Lab.
Reporting: All results are reported to primary care providers, birth hospitals, AHW NMS Application, NetCare, and primary care providers’ office systems. Critical and double borderline results are phoned/faxed to primary care providers and Specialty Clinics.
Follow-up and Work-up: For all critical and double borderline results, families are contacted and urgent arrangements are made for the infant to receive clinical assessments and diagnostic tests as soon as possible.
A detailed overview of the Current State NMS Program Process Map can be found in Appendix D. Refer to Figure 2 for an overview of the Newborn Metabolic Screening Pathway.
Figure 2: Newborn Metabolic Screening Pathway: October 2010
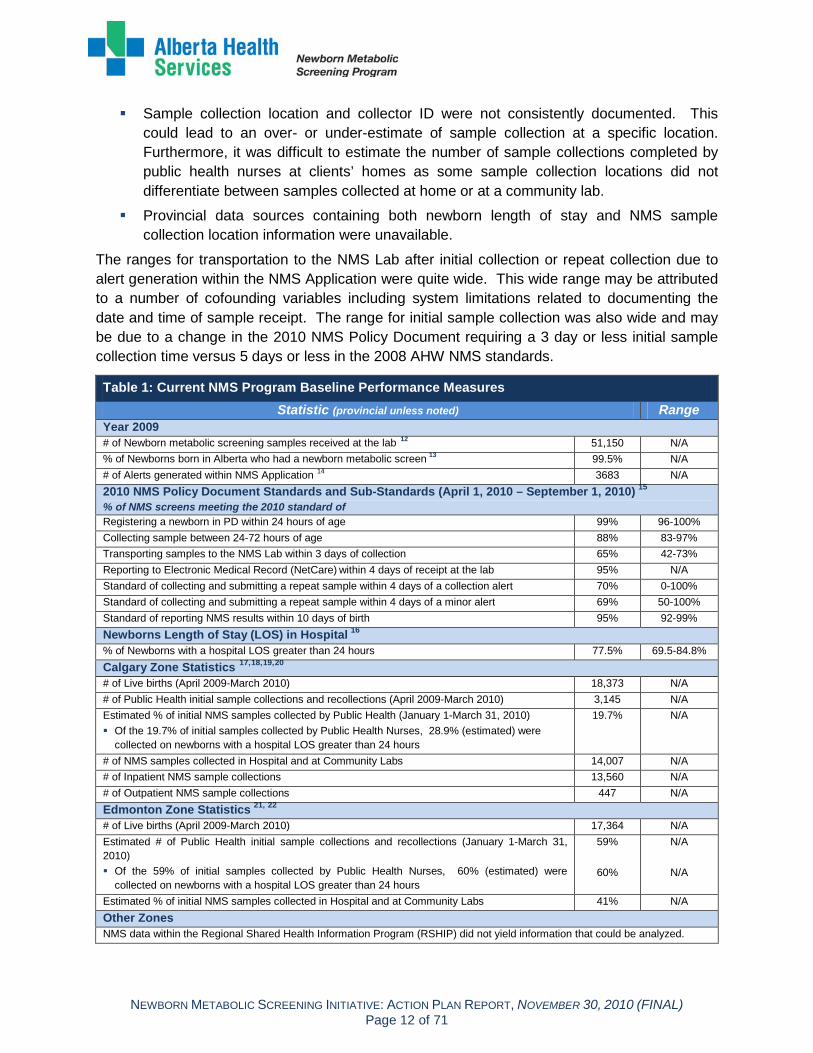
NMS PROGRAM PERFORMANCE MEASUREMENT During the action planning process, potential data sources were explored to identify existing baseline performance measures for the Current State NMS Program. Baseline performance measures related to the 2010 NMS Policy Document standards and sub-standards were determined using data from the NMS Application (April 1, 2010-September 1, 2010). Length of stay data and Zone specific statistics were difficult to collect and gathered from a number of sources over different time periods. Table 1 breaks down performance measures and length of stay data by data source and time frame.
While compiling baseline performance measures, the following limitations were identified:
Data accuracy was not verified within the databases.
NEWBORN METABOLIC SCREENING INITIATIVE: ACTION PLAN REPORT, NOVEMBER 30, 2010 (FINAL)
Page 12 of 71
Sample collection location and collector ID were not consistently documented. This could lead to an over- or under-estimate of sample collection at a specific location. Furthermore, it was difficult to estimate the number of sample collections completed by public health nurses at clients’ homes as some sample collection locations did not differentiate between samples collected at home or at a community lab.
Provincial data sources containing both newborn length of stay and NMS sample collection location information were unavailable.
The ranges for transportation to the NMS Lab after initial collection or repeat collection due to alert generation within the NMS Application were quite wide. This wide range may be attributed to a number of cofounding variables including system limitations related to documenting the date and time of sample receipt. The range for initial sample collection was also wide and may be due to a change in the 2010 NMS Policy Document requiring a 3 day or less initial sample collection time versus 5 days or less in the 2008 AHW NMS standards.
Table 1: Current NMS Program Baseline Performance Measures Statistic (provincial unless noted) Range
Year 2009 # of Newborn metabolic screening samples received at the lab 12 51,150 N/A % of Newborns born in Alberta who had a newborn metabolic screen 13 99.5% N/A # of Alerts generated within NMS Application 14 3683 N/A 2010 NMS Policy Document Standards and Sub-Standards (April 1, 2010 – September 1, 2010) 15
% of NMS screens meeting the 2010 standard of
Registering a newborn in PD within 24 hours of age 99% 96-100% Collecting sample between 24-72 hours of age 88% 83-97% Transporting samples to the NMS Lab within 3 days of collection 65% 42-73% Reporting to Electronic Medical Record (NetCare) within 4 days of receipt at the lab 95% N/A Standard of collecting and submitting a repeat sample within 4 days of a collection alert 70% 0-100% Standard of collecting and submitting a repeat sample within 4 days of a minor alert 69% 50-100% Standard of reporting NMS results within 10 days of birth 95% 92-99% Newborns Length of Stay (LOS) in Hospital 16
% of Newborns with a hospital LOS greater than 24 hours
77.5% 69.5-84.8% Calgary Zone Statistics 17,18,19,20
# of Live births (April 2009-March 2010)
18,373 N/A # of Public Health initial sample collections and recollections (April 2009-March 2010) 3,145 N/A Estimated % of initial NMS samples collected by Public Health (January 1-March 31, 2010) Of the 19.7% of initial samples collected by Public Health Nurses, 28.9% (estimated) were
collected on newborns with a hospital LOS greater than 24 hours
19.7%
N/A
# of NMS samples collected in Hospital and at Community Labs 14,007 N/A # of Inpatient NMS sample collections 13,560 N/A # of Outpatient NMS sample collections 447 N/A Edmonton Zone Statistics 21, 22
# of Live births (April 2009-March 2010)
17,364 N/A Estimated # of Public Health initial sample collections and recollections (January 1-March 31, 2010) Of the 59% of initial samples collected by Public Health Nurses, 60% (estimated) were
collected on newborns with a hospital LOS greater than 24 hours
59%
60%
N/A
N/A
Estimated % of initial NMS samples collected in Hospital and at Community Labs 41% N/A Other Zones NMS data within the Regional Shared Health Information Program (RSHIP) did not yield information that could be analyzed.
NEWBORN METABOLIC SCREENING INITIATIVE: ACTION PLAN REPORT, NOVEMBER 30, 2010 (FINAL)
Page 13 of 71
DEVELOPMENT OF THE ACTION PLAN A team of 142 health professionals, consultants/specialists, executives, and support staff across Alberta invested 12 weeks in the development of the Action Plan. The creation of the NMS Program Operational Model and Action Plan involved extensive Working Group involvement, numerous meetings and consultations with Integration and Steering Committee members, coordination and synthesizing by the HPDIP NMS Core Planning Group, and additional consultations, feedback, and validation with key stakeholders. Refer to Appendix B for details on committee members, consultants, and contributors.
The action planning process began with the creation of detailed Working Group specific process maps. Each Working Group then completed an assessment tool for each of the 17 standards and 50 sub-standards which included reviewing: current processes, procedures, and guidelines staff training and education resources parent resources evaluation criteria, indicators, data sources, and outcomes adequate resources (i.e., staffing, infrastructure, services)
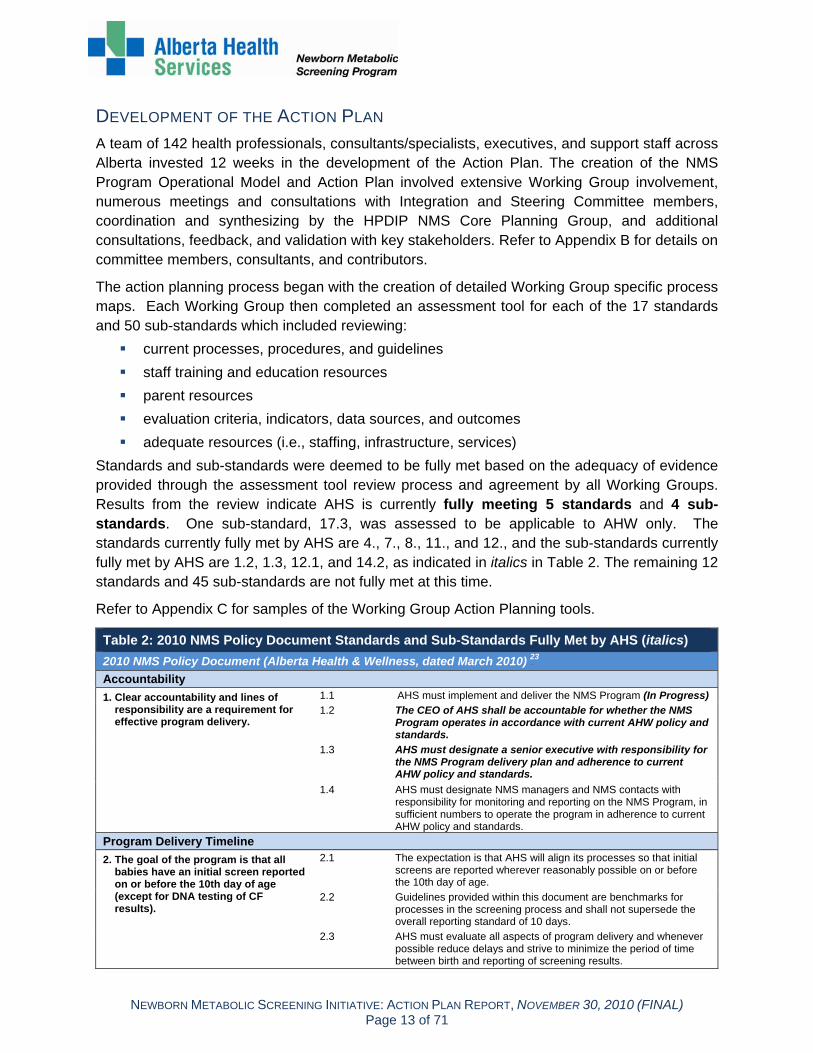
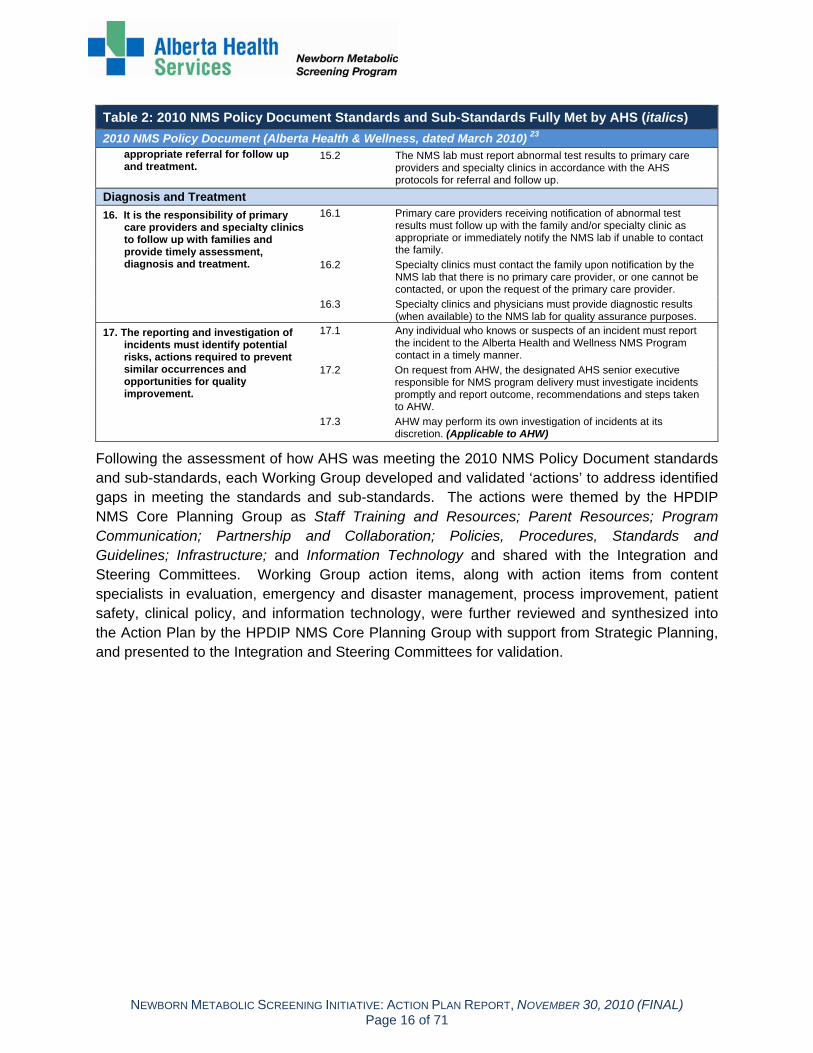
Standards and sub-standards were deemed to be fully met based on the adequacy of evidence provided through the assessment tool review process and agreement by all Working Groups. Results from the review indicate AHS is currently fully meeting 5 standards and 4 sub-standards. One sub-standard, 17.3, was assessed to be applicable to AHW only. The standards currently fully met by AHS are 4., 7., 8., 11., and 12., and the sub-standards currently fully met by AHS are 1.2, 1.3, 12.1, and 14.2, as indicated in italics in Table 2. The remaining 12 standards and 45 sub-standards are not fully met at this time.
Refer to Appendix C for samples of the Working Group Action Planning tools.
Table 2: 2010 NMS Policy Document Standards and Sub-Standards Fully Met by AHS (italics) 2010 NMS Policy Document (Alberta Health & Wellness, dated March 2010) 123
Accountability 1. Clear accountability and lines of
responsibility are a requirement for effective program delivery.
1.1 AHS must implement and deliver the NMS Program (In Progress)
1.2 The CEO of AHS shall be accountable for whether the NMS Program operates in accordance with current AHW policy and standards.
1.3 AHS must designate a senior executive with responsibility for the NMS Program delivery plan and adherence to current AHW policy and standards.
1.4 AHS must designate NMS managers and NMS contacts with responsibility for monitoring and reporting on the NMS Program, in sufficient numbers to operate the program in adherence to current AHW policy and standards.
Program Delivery Timeline 2. The goal of the program is that all
babies have an initial screen reported on or before the 10th day of age (except for DNA testing of CF results).
2.1 The expectation is that AHS will align its processes so that initial screens are reported wherever reasonably possible on or before the 10th day of age.
2.2 Guidelines provided within this document are benchmarks for processes in the screening process and shall not supersede the overall reporting standard of 10 days.
2.3 AHS must evaluate all aspects of program delivery and whenever possible reduce delays and strive to minimize the period of time between birth and reporting of screening results.

NEWBORN METABOLIC SCREENING INITIATIVE: ACTION PLAN REPORT, NOVEMBER 30, 2010 (FINAL)
Page 14 of 71
Table 2: 2010 NMS Policy Document Standards and Sub-Standards Fully Met by AHS (italics) 2010 NMS Policy Document (Alberta Health & Wellness, dated March 2010) 123
2.4 AHS must develop an emergency preparedness plan and maintain delivery of NMS Program services during emergencies and infectious disease events.
Procedure and Operational Policies
3. Procedures and operational policies related to program activity must be developed, implemented provincially and maintained to reflect current AHW policy.
3.1 Operational policies, procedures, plans, and training and informational materials related to NMS Program delivery must be submitted to AHW on request and AHW may request modifications to these documents.
3.2 AHW must be notified of any significant operational changes to the NMS Program in a timely manner.
Access 4. Newborn Metabolic Screening is part
of the health care services provided to infants born in Alberta.
4.1 AHS must make all reasonable efforts to screen all infants born in Alberta.
4.2 AHS must provide training to staff registering newborns in the Person Directory application, obtaining the screening samples and accessing the NMS Application.
4.3 AHS must register infants born in Alberta in the Person Directory application through the "add newborn" function within 24 hours of birth.
5. Newborn metabolic screening is part of the standard of care that every baby born in Alberta receives. Parents/guardians must be informed about the nature and purpose of newborn metabolic screening.
5.1 The health professional taking the sample for screening or the primary care provider who is requisitioning the sample must inform the parent of the reason for the screen and provide information about the program before the sample is collected.
Refusals 6. If parents/ guardians decline to have
the newborn screen sample collected it is important that they are informed of the purpose of the test and the possible implications of refusing the screen.
6.1 Parents/guardians who decline the screening must be informed by the health professional arranging sample collection or the primary care provider who is treating the infant about the possible implications of the infant not being screened. Refusal of screening must be adequately documented by the health professional in accordance with direction from AHS' legal counsel.
7. NMS screening applies to all disorders in the screening list; there is no option for selective screening.
7.1 Parents/guardians who do not wish their child to be screened for all the disorders are therefore refusing the screen and must be immediately referred, by the health professional providing care, to their physician for follow up and the parents' decision must be documented.
7.2 Parents/guardians who accept screening and request additional testing for disorders not on the list should have the newborn's sample collected as per protocol and referred to their physician for any additional screening.
8. Screening will not be provided in cases where a physician advises that screening should not be done for a clinical reason.
8.1 It is the responsibility of AHS to obtain legal advice on how to respond to a physician who advises against screening and to document physician refusal of screening.
Sample Collection and Delivery 9. If infant is born in Alberta, AHS is
responsible for obtaining the sample for newborn metabolic screening and for transporting samples to the NMS lab within the specified timeframe.
9.1 AHS must collect initial samples from infants between 24 hours and 72 hours of age and as close to the 24 hours as reasonably possible.
9.2 AHS must collect a repeat screen between three and six weeks of age for all infants who are in the neonatal intensive care unit (NICU) for three weeks or longer.
9.3 Samples must be taken according to the instructions provided by the NMS laboratory.
9.4 The health professional taking the sample must fill out the NMS requisition completely and accurately.
9.5 AHS shall create, monitor and manage a province-wide system to deliver samples to the NMS lab.
9.6 AHS must deliver samples to the NMS lab within three days of sample collection.

NEWBORN METABOLIC SCREENING INITIATIVE: ACTION PLAN REPORT, NOVEMBER 30, 2010 (FINAL)
Page 15 of 71
Table 2: 2010 NMS Policy Document Standards and Sub-Standards Fully Met by AHS (italics) 2010 NMS Policy Document (Alberta Health & Wellness, dated March 2010) 123
Alert Management 10. AHS is responsible for monitoring
alerts in the NMS Application and ensuring appropriate actions are preformed in accordance with AHW policies and standards.
10.1 NMS contacts must check the NMS Application for alerts and perform activities related to alert management every business day.
10.2 When an alert is posted, AHS must collect and submit a sample within 4 days of the alert posting (except for increased tyrosine).
10.3 In the case of increased tyrosine, AHS must collect and submit a sample between 30 and 42 days of age.
10.4 AHS must implement a process for contacting families for screening and efforts to contact the family must be documented in the NMS Application.
10.5 AHS must implement a process for determining when it is appropriate to manually close alerts in the NMS Application (when efforts to collect the sample have been unsuccessful) and explanations for closing alerts must be documented in the NMS Application.
10.6 If the newborn has moved out of province, AHS shall notify a person responsible for NMS in the jurisdiction where the infant resides of the status of screening and document notification in the NMS Application.
Sample Testing
11. AHS must designate a single laboratory as the provincial NMS laboratory.
11.1 The NMS laboratory is responsible for timely testing of all initial and repeated screens.
11.2 The NMS laboratory must be fully operational on all business days. It must not be closed for more than two consecutive days.
11.3 The NMS laboratory must accurately record the date and time when a sample arrives in the NMS laboratory.
11.4 The NMS laboratory must enter a sample in the laboratory information system whenever possible on the day received and in any event within two days of arrival.
11.5 The NMS laboratory must analyze samples whenever possible on the day received and in any event within two days of arrival.
11.6 The NMS laboratory must check the NMS Application for alerts and perform activities related to alert management every business day.
11.7 Laboratory polices related to retention, security, access to, quality assurance and reporting of NMS samples must be submitted to AHW on request and AHW may request modifications to these documents.
12. AHS must designate a single laboratory as the NMS Molecular Diagnostic Laboratory.
12.1 The Molecular Diagnostic Laboratory is responsible for the DNA testing component of CF screening.
Research 13. The sample is collected only for the
purpose of NMS screening for the newborn.
13.1 All research requests regarding access to NMS samples must be made in accordance with the requirements of the Health Information Act.
Reporting of Results
14. NMS lab results must be reported to the: • Primary care provider as documented on the requisition, • The birth facility, • The NMS Application, and the Electronic Health Record (EHR).
14.1 The NMS lab must issue an alert or have test results posted within four days of receipt of the sample (except for DNA testing for CF).
14.2 The molecular diagnostic lab must report CF DNA results on referred specimens to the NMS lab. The NMS lab must issue an alert or have test results posted for CF DNA results within 21 days of receipt of the sample.
14.3 AHS must report NMS laboratory data electronically to the NMS Application in a format acceptable to AHW, and the delivery of the electronic messages must be monitored and any interruption to delivery identified, reported to AHW and resolved in a timely manner.
15. All children with abnormal screen results must receive timely and
15.1 AHS must establish protocols for referral and follow up for each of the disorders screened for in consultation with specialty clinics and AHW.
NEWBORN METABOLIC SCREENING INITIATIVE: ACTION PLAN REPORT, NOVEMBER 30, 2010 (FINAL)
Page 16 of 71
Table 2: 2010 NMS Policy Document Standards and Sub-Standards Fully Met by AHS (italics) 2010 NMS Policy Document (Alberta Health & Wellness, dated March 2010) 123
appropriate referral for follow up and treatment.
15.2 The NMS lab must report abnormal test results to primary care providers and specialty clinics in accordance with the AHS protocols for referral and follow up.
Diagnosis and Treatment 16. It is the responsibility of primary
care providers and specialty clinics to follow up with families and provide timely assessment, diagnosis and treatment.
16.1 Primary care providers receiving notification of abnormal test results must follow up with the family and/or specialty clinic as appropriate or immediately notify the NMS lab if unable to contact the family.
16.2 Specialty clinics must contact the family upon notification by the NMS lab that there is no primary care provider, or one cannot be contacted, or upon the request of the primary care provider.
16.3 Specialty clinics and physicians must provide diagnostic results (when available) to the NMS lab for quality assurance purposes.
17. The reporting and investigation of incidents must identify potential risks, actions required to prevent similar occurrences and opportunities for quality improvement.
17.1 Any individual who knows or suspects of an incident must report the incident to the Alberta Health and Wellness NMS Program contact in a timely manner.
17.2 On request from AHW, the designated AHS senior executive responsible for NMS program delivery must investigate incidents promptly and report outcome, recommendations and steps taken to AHW.
17.3 AHW may perform its own investigation of incidents at its discretion. (Applicable to AHW)
Following the assessment of how AHS was meeting the 2010 NMS Policy Document standards and sub-standards, each Working Group developed and validated ‘actions’ to address identified gaps in meeting the standards and sub-standards. The actions were themed by the HPDIP NMS Core Planning Group as Staff Training and Resources; Parent Resources; Program Communication; Partnership and Collaboration; Policies, Procedures, Standards and Guidelines; Infrastructure; and Information Technology and shared with the Integration and Steering Committees. Working Group action items, along with action items from content specialists in evaluation, emergency and disaster management, process improvement, patient safety, clinical policy, and information technology, were further reviewed and synthesized into the Action Plan by the HPDIP NMS Core Planning Group with support from Strategic Planning, and presented to the Integration and Steering Committees for validation.

NEWBORN METABOLIC SCREENING INITIATIVE: ACTION PLAN REPORT, NOVEMBER 30, 2010 (FINAL)
Page 17 of 71
OPERATIONAL MODEL NMS PROGRAM QUALITY MANAGEMENT FRAMEWORK A Quality Management (QM) Framework and a Governance Structure comprise the recommended Operational Model for the NMS Program. A NMS Program QM Framework will support continued development of high quality screening services and integrated AHS enterprise-wide processes in order to ensure quality care.
Within the NMS Program QM Framework, Action Plan indicators and ongoing performance measures will be used to monitor how well the Program is performing. NMS Program performance will be measured against the 2010 NMS Policy Document standards and sub-standards. A process improvement focus will guide all current and future improvements to the NMS Program. The purpose of the NMS Program QM Framework will be to maximize screening opportunities and reduce the risk of missing a newborn, screen, result, and/or follow-up.
The components of the QM Framework selected for the NMS Program (as illustrated in Figure 3) are adapted from the AHS Calgary Stroke Program Model which uses an integrated approach to managing care across the continuum.
Figure 3: Components of the Quality Management Framework2
24
The NMS Program QM Framework shown in Figure 4 is recommended to address areas of concern and the need for regular performance measurement as identified in both the 2009 NMS Audit and the 2010 NMS Policy Document standards and sub-standards assessment.
Care that we provide
How we support care
M aking it better where we can /
should
M easuring how well we are doing

NEWBORN METABOLIC SCREENING INITIATIVE: ACTION PLAN REPORT, NOVEMBER 30, 2010 (FINAL)
Page 18 of 71
Figure 4: NMS Program Quality Management Framework25
Primary Care Provider
Engagement
Program Planning
Program Communication
NMS Screening Processes
Supporting Process ResultsInternal
External
AHS StaffEngagement
Parent Engagement
Collaborative Partnerships
Emergency/Disaster
Management Information Technology
SupportingProcesses
Analysis and Reporting
Newborn Metabolic Screening Processes
ProcessImprovement and Design
PerformanceMeasurement
and EvaluationProgram and Project Evaluation
Benchmarking
Work-up and Follow-up
Patient Safety
Knowledge Management
Sample Collection and Transportation
Newborn Registration
Alert Management
NMS Program Quality Management Framework
The NMS Program QM Framework includes:26
Newborn Metabolic Screening Processes: Services and care that are provided at the right time, by the right care provider (e.g., policies, procedures, standards, and guidelines; staffing models; pathways and care maps).
Supporting Processes: Ensuring supports are in place for care providers to provide care to clients, patients, and families (e.g., learning and development; staff, parent and provider engagement; program communication and planning).
Performance Measurement and Evaluation: Measuring how screening services and support processes are performing.
Process Improvement and Design: Utilizing systematic techniques to improve how the NMS Program provides and supports screening care.
ACTION PLAN GOVERNANCE STRUCTURE The Action Plan Governance Structure in Figure 5 is proposed as the second component of the recommended Operational Model for the NMS Program to support Action Plan Implementation. An integrated, comprehensive project management approach will be used throughout the Implementation Phase.

NEWBORN METABOLIC SCREENING INITIATIVE: ACTION PLAN REPORT, NOVEMBER 30, 2010 (FINAL)
Page 19 of 71
Figure 5: Action Plan Governance Structure
The Action Plan Governance Structure includes a Steering Committee, an Action Plan Implementation Committee, and Interdisciplinary Project Teams to implement the NMS Action Plan projects with support from the HPDIP NMS Program Provincial Team. The responsibilities within each group include:
NMS Steering Committee Purpose: To work collaboratively across AHS portfolios to oversee, direct, and ensure an integrated, AHS enterprise-wide approach is taken to implement the NMS Action Plan.
Responsibilities: Oversee the implementation of the NMS Action Plan within a Quality Management
Framework Refine and apply the Action Plan Governance Structure Identify and respond to the overall AHS enterprise-wide impact of the 2010 NMS Policy
Document Engage senior executives, medical leaders, and key stakeholders in providing strategic
direction and make recommendations for planning, implementing and sustaining NMS service delivery requirements
Anticipate problems and take or recommend corrective action; escalate issues and problems as necessary
Review and approve the annual NMS report prior to submission to AHW
NMS Action Plan Implementation Committee Purpose: To work collaboratively to support the implementation of the NMS Action Plan within a Quality Management Framework.
Responsibilities: Support the implementation of the NMS Action Plan within a Quality Management
Framework

NEWBORN METABOLIC SCREENING INITIATIVE: ACTION PLAN REPORT, NOVEMBER 30, 2010 (FINAL)
Page 20 of 71
Develop a plan to guide process change Identify circumstances that would necessitate program review or reorientation Monitor the progress of the Interdisciplinary Project Teams Review interim and final reports from the NMS Interdisciplinary Project Teams Consult with clinical experts and consultants as appropriate Identify performance measures, evaluation structures, and process improvement
projects Develop the evaluation framework and logic model in consultation with the evaluation
specialist Review annual reports for AHW and other program partners Monitor implementation timelines, report potential delays and issues to the Steering
Committee promptly
NMS Interdisciplinary Project Teams Purpose: To implement NMS Action Plan projects within a Quality Management Framework.
Responsibilities: Implement NMS Action Plan projects and activities using a Quality Management
Framework Develop project work plans and ensure alignment with the NMS Action Plan Identify roles and responsibilities within the project team Complete project within the assigned timeframe Bring issues forward to the NMS Action Plan Implementation Team Complete interim and final project reports for the NMS Action Plan Implementation Team
HPDIP NMS Program Provincial Team Purpose: To coordinate the implementation of the Action Plan within the NMS Program Quality Management Framework and the Action Plan Governance Structure. Responsibilities: Provide a co-chair to coordinate the NMS Program Steering Committee, NMS Action
Plan Implementation Team, and each NMS Interdisciplinary Project Team Provide administration support to the NMS Program committees, teams, and projects Provide an AHS central point of contact for AHW for the NMS Program Develop overall Action Plan implementation work plans, timelines, and other project
management tools Identify roles and responsibilities within the provincial team Bring issues forward to the NMS Project Teams, Action Plan Implementation Team,
NMS Steering Committee as appropriate Prepare performance measurement reports, process improvement recommendations,
progress reports, and annual reports for AHW and other program partners

NEWBORN METABOLIC SCREENING INITIATIVE: ACTION PLAN REPORT, NOVEMBER 30, 2010 (FINAL)
Page 21 of 71
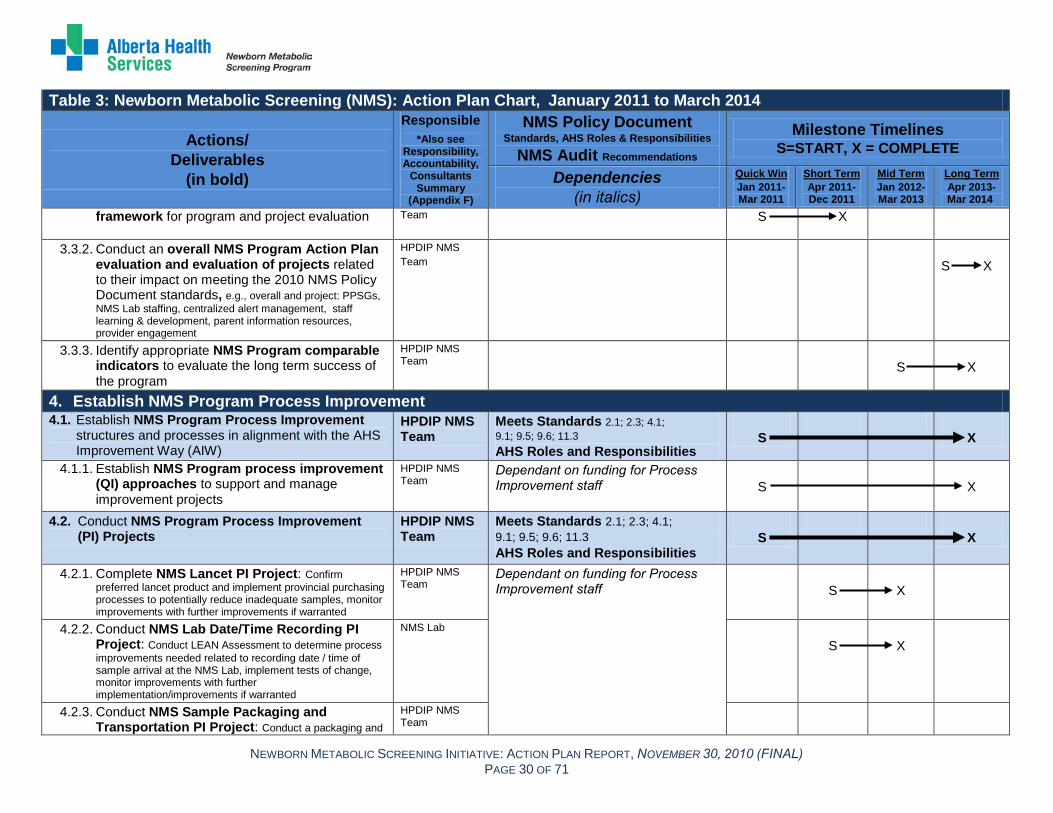
ACTION PLAN OVERVIEW OF ACTIONS The Action Plan detailed in Table 3 outlines the recommended actions and timelines within AHS to achieve the 2010 NMS Policy Document standards and sub-standards. The roles and responsibilities of AHS, and the 2009 NMS Audit concerns are also addressed. The actions included in the Action Plan have been endorsed by the five Working Groups, the HPDIP NMS Core Planning Group, the Integration Committee, and the NMS Steering Committee.
In order to deliver an effective NMS Program that meets the 2010 NMS Policy Document standards and sub-standards, it is essential to ensure coordination and integration along the Newborn Metabolic Screening Pathway (i.e., registration, sample collection, transportation, analysis, follow-up and work-up). A successful NMS Program is also dependent on supporting processes such as learning and development opportunities for staff and primary care providers, information for parents/guardians, program communication, program evaluation, and process improvements. Establishing effective partnerships with primary care providers, families, and staff across AHS is integral to developing the program.27
The Action Plan outlines the recommended actions to improve and establish the four components of the NMS Program Quality Management Framework:
The intent of the Action Plan is to identify actions needed to improve NMS Program infrastructure, processes, outputs, and outcomes. The Action Plan addresses these components and is the foundation for the further development of a comprehensive NMS Program.
Newborn Metabolic Screening Processes
NMS Program Supporting Processes
NMS Program Performance Measurement and Evaluation
NMS Program Process Improvement
The milestone timelines are defined as the following:
Quick Win: January 2011-March 2011
Short Term: April 2011-December 2011
Mid Term: January 2012-March 2013
Long Term: April 2013-March 2014
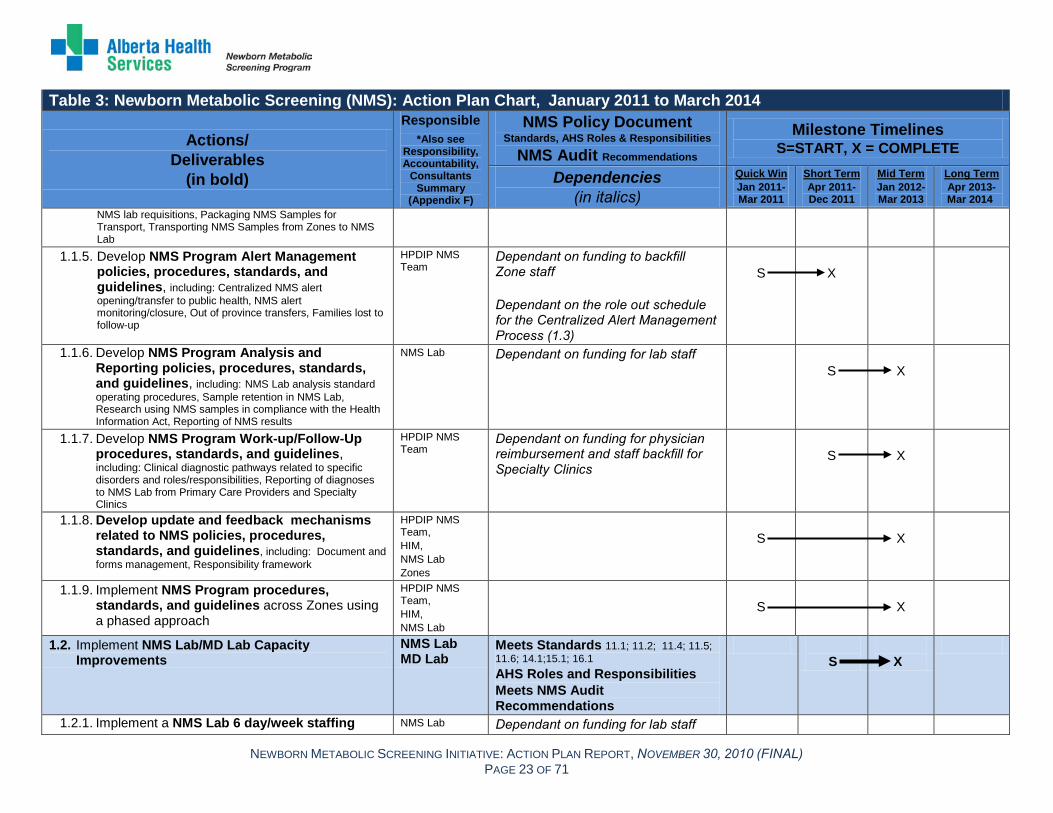
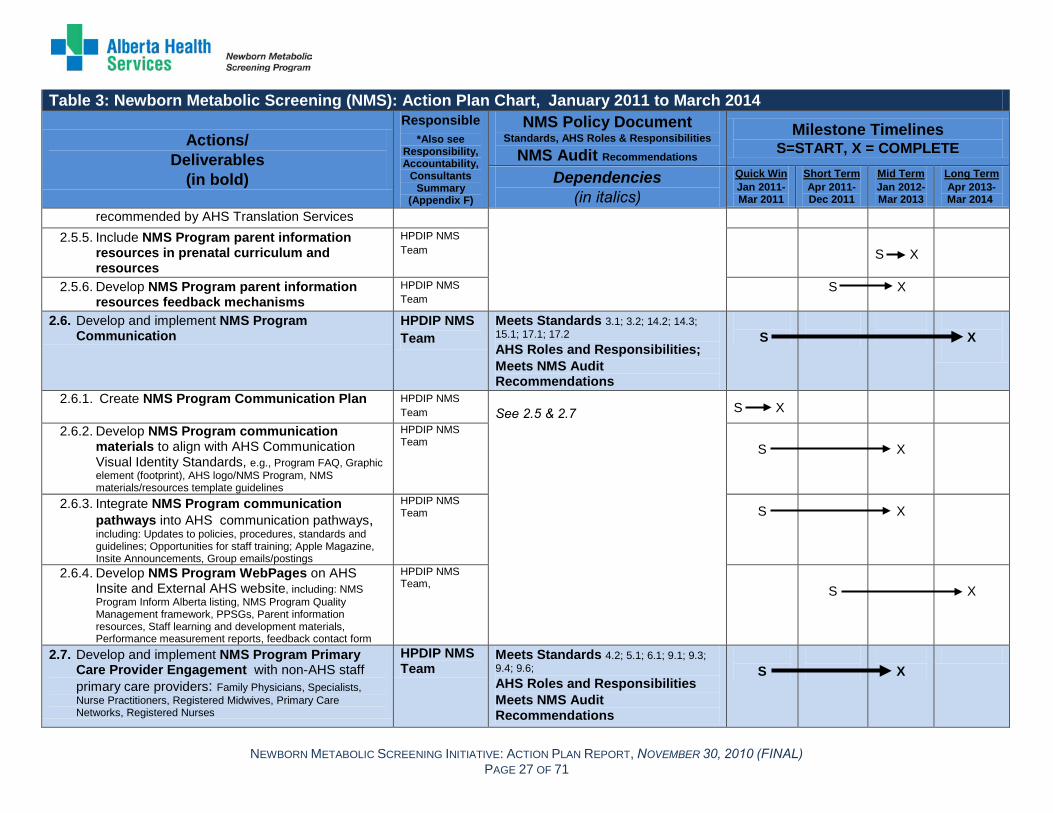
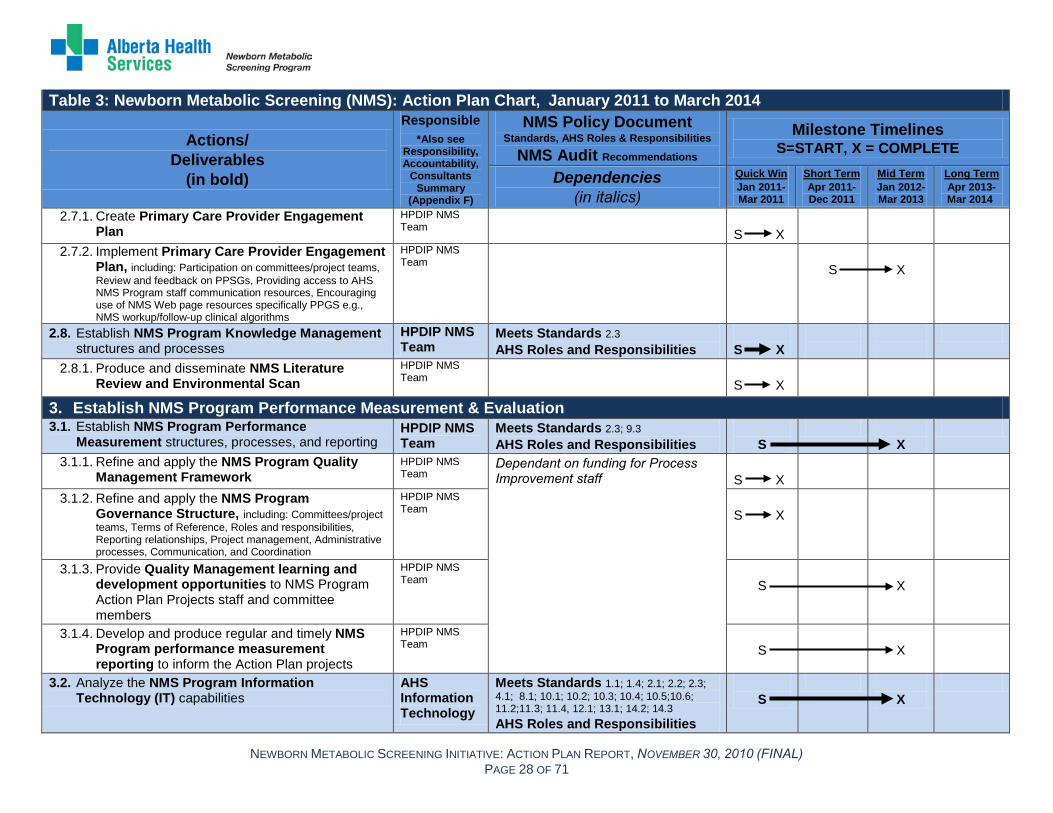
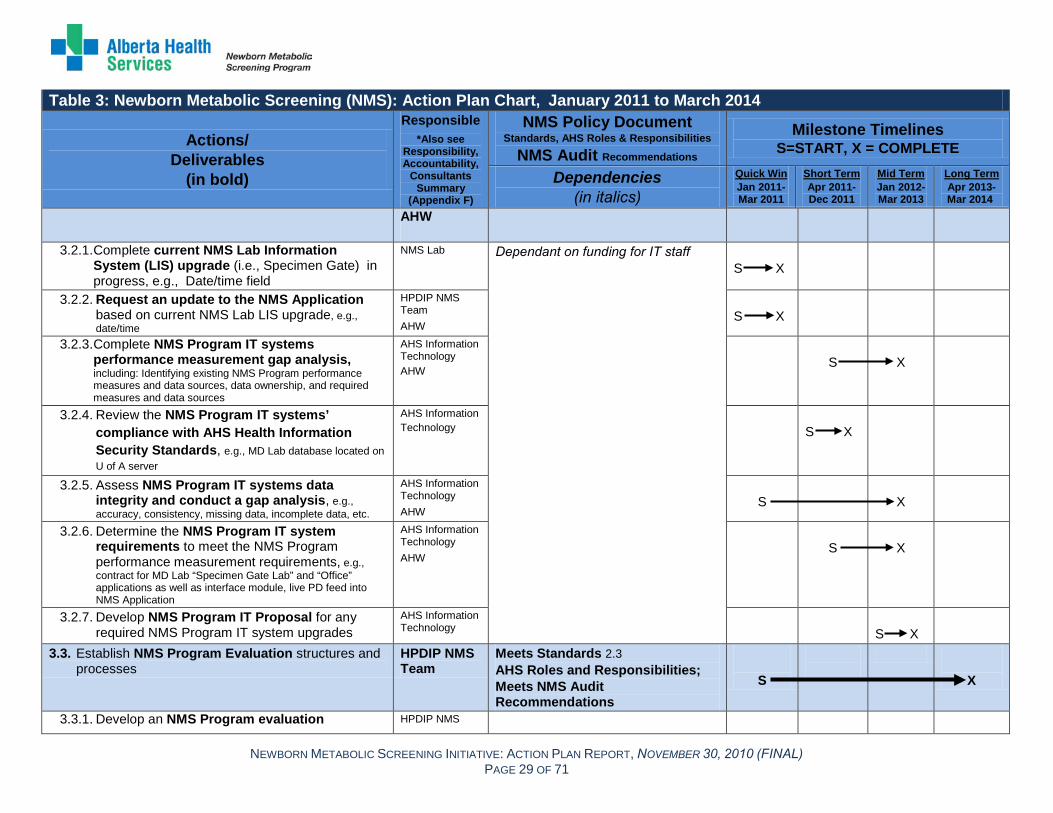
Refer to Table 3 for the NMS Action Plan Chart. Deliverables within the NMS Action Plan Chart are in bold font in the ‘Action’ column. The accountability for each deliverable is identified, as are the standards and sub-standards each action will address. Timelines and dependencies are also identified for each step of the plan. Appendix E summarizes the actions as they relate to the 2010 NMS Policy Document standards and sub-standards. Appendix F presents the Action Plan Responsibility, Accountability, and Consultants Summary.

NEWBORN METABOLIC SCREENING INITIATIVE: ACTION PLAN REPORT, NOVEMBER 30, 2010 (FINAL) PAGE 22 OF 71
Table 3: Newborn Metabolic Screening (NMS): Action Plan Chart, January 2011 to March 2014
Actions/ Deliverables
(in bold)
Responsible *Also see
Responsibility, Accountability,
Consultants Summary
(Appendix F)
NMS Policy Document Standards, AHS Roles & Responsibilities
NMS Audit Recommendations Milestone Timelines
S=START, X = COMPLETE
Dependencies (in italics)
Quick Win Jan 2011-Mar 2011
Short Term Apr 2011-Dec 2011
Mid Term Jan 2012-Mar 2013
Long Term Apr 2013-Mar 2014
1. Improve Newborn Metabolic Screening Processes 1.1. Develop and implement NMS clinical policies,
procedures, standards, and guidelines in alignment with Alberta Health Services (AHS) Strategic Governance Document Framework (2009)
Health Promotion Disease & Injury Prevention (HPDIP) NMS Team
Meets Standards 2.1; 2.2; 2.3; 3.1; 4.1; 4.2; 4.3; 5.1; 6.1; 7.1; 7.2; 9.1; 9.2; 9.3, 9.4; 9.6; 10.1; 10.2; 10.3; 10.4; 10.5; 10.6; 11.1; 11.3; 11.4; 11.5; 11.6; 11.7; 13.1; 14.1; 14.2; 15.1; 15.2; 16.2; 16.3; 17 Meets AHS Roles & Responsibilities Meets NMS Audit Recommendations
S
X
1.1.1. Develop an overarching AHS NMS Program clinical policy related to the NMS program directive
HPDIP NMS Team
S
X
1.1.2. Develop general NMS Program policies, procedures, standards, and guidelines, including: NMS Documentation, Appropriate use of telephone/fax/email/texting to contact, Reasonable number of attempts to contact/collect/recollect sample
HPDIP NMS Team
S
X
1.1.3. Develop NMS Program Newborn Registration policies, procedures, standards, and guidelines, including: Access to Person Directory (PD), Creating newborn Unique Lifetime Identifiers (ULIs) in PD, Updating PD upon an infant death, Updating PD when an infant is transferred to another facility, Off-site registration in rural areas, Midwife newborn registration processes
HPDIP NMS Team, Health Information Management (HIM)
S
X
1.1.4. Develop NMS Program Sample Collection and Transportation policies, procedures, standards, and guidelines, including: Collecting NMS samples on infants > 24 hours of age in acute care prior to discharge, Collecting NMS sample on infants < 24 hours of age who live in rural remote areas or with complex family situations prior to discharge from acute care, NICU/SCN collections, Informed refusal / informed consent including documentation, Sample collection clinical process, Parents requesting partial screens, Parents requesting additional screens, Review, procurement, and distribution of
HPDIP NMS Team
Dependant on funding to backfill Zone staff Dependant on Process Improvement projects (LEAN assessment NMS Lab; Packaging and Transportation Time study. See 4.1)
S
X
NEWBORN METABOLIC SCREENING INITIATIVE: ACTION PLAN REPORT, NOVEMBER 30, 2010 (FINAL) PAGE 23 OF 71
Table 3: Newborn Metabolic Screening (NMS): Action Plan Chart, January 2011 to March 2014
Actions/ Deliverables
(in bold)
Responsible *Also see
Responsibility, Accountability,
Consultants Summary
(Appendix F)
NMS Policy Document Standards, AHS Roles & Responsibilities
NMS Audit Recommendations Milestone Timelines
S=START, X = COMPLETE
Dependencies (in italics)
Quick Win Jan 2011-Mar 2011
Short Term Apr 2011-Dec 2011
Mid Term Jan 2012-Mar 2013
Long Term Apr 2013-Mar 2014
NMS lab requisitions, Packaging NMS Samples for Transport, Transporting NMS Samples from Zones to NMS Lab
1.1.5. Develop NMS Program Alert Management policies, procedures, standards, and guidelines, including: Centralized NMS alert opening/transfer to public health, NMS alert monitoring/closure, Out of province transfers, Families lost to follow-up
HPDIP NMS Team
Dependant on funding to backfill Zone staff Dependant on the role out schedule for the Centralized Alert Management Process (1.3)
S
X
1.1.6. Develop NMS Program Analysis and Reporting policies, procedures, standards, and guidelines, including: NMS Lab analysis standard operating procedures, Sample retention in NMS Lab, Research using NMS samples in compliance with the Health Information Act, Reporting of NMS results
NMS Lab
Dependant on funding for lab staff S
X
1.1.7. Develop NMS Program Work-up/Follow-Up procedures, standards, and guidelines, including: Clinical diagnostic pathways related to specific disorders and roles/responsibilities, Reporting of diagnoses to NMS Lab from Primary Care Providers and Specialty Clinics
HPDIP NMS Team
Dependant on funding for physician reimbursement and staff backfill for Specialty Clinics
S
X
1.1.8. Develop update and feedback mechanisms related to NMS policies, procedures, standards, and guidelines, including: Document and forms management, Responsibility framework
HPDIP NMS Team, HIM, NMS Lab Zones
S
X
1.1.9. Implement NMS Program procedures, standards, and guidelines across Zones using a phased approach
HPDIP NMS Team, HIM, NMS Lab
S
X
1.2. Implement NMS Lab/MD Lab Capacity Improvements
NMS Lab MD Lab
Meets Standards 11.1; 11.2; 11.4; 11.5; 11.6; 14.1;15.1; 16.1 AHS Roles and Responsibilities Meets NMS Audit Recommendations
S
X
1.2.1. Implement a NMS Lab 6 day/week staffing NMS Lab Dependant on funding for lab staff

NEWBORN METABOLIC SCREENING INITIATIVE: ACTION PLAN REPORT, NOVEMBER 30, 2010 (FINAL) PAGE 24 OF 71
Table 3: Newborn Metabolic Screening (NMS): Action Plan Chart, January 2011 to March 2014
Actions/ Deliverables
(in bold)
Responsible *Also see
Responsibility, Accountability,
Consultants Summary
(Appendix F)
NMS Policy Document Standards, AHS Roles & Responsibilities
NMS Audit Recommendations Milestone Timelines
S=START, X = COMPLETE
Dependencies (in italics)
Quick Win Jan 2011-Mar 2011
Short Term Apr 2011-Dec 2011
Mid Term Jan 2012-Mar 2013
Long Term Apr 2013-Mar 2014
model using a phased approach: initially long weekend, followed by 6 day/week operations
S X
1.2.2. Implement NMS Lab staff and MD Lab staffing coverage improvements
NMS Lab MD Lab
Dependant on funding for lab staff
S
X
1.3. Develop and implement NMS Program Centralized Alert Management Process
HPDIP NMS Team
Meets Standards 1.4; 10.1; 10.2; 10.3; 10.4; 10.5; 10.6 AHS Roles and Responsibilities
S
X
1.3.1. Develop draft NMS Program centralized alert management (CAM) process
HPDIP NMS Team
S X
1.3.2. Conduct NMS Program centralized alert management (CAM) Information technology (IT) fit gap analysis
AHS Information Technology
S X
1.3.3. Conduct NMS Program centralized alert management (CAM) transition tests between NMS Program Provincial Team, NMS Lab, and Zones Public Health (see also 1.1.5)
HPDIP NMS Team
S
X
1.3.4. Roll out a NMS Program centralized alert management (CAM) process phased launch between NMS Program Provincial Team, NMS Lab, and Zones Public Health
HPDIP NMS Team
Dependant on funding to support alert management activities at the Zone level Dependant on funding for centralized clerical staff
S X
2. Improve NMS Program Supporting Processes 2.1. Define and maintain NMS Program Collaborative
Partnerships HPDIP AHS Roles and Responsibilities
Meets NMS Audit Recommendations
S
X
2.1.1. Establish AHS NMS Program Point of Contact with Alberta Health & Wellness (AHW), including: Identifying an AHS NMS Program point person, developing regular contact and reporting processes between AHS and AHW, clarifying NMS Program reporting requirements and frequency, communication pathways
HPDIP S X
2.1.2. Create Annual AHS NMS Program Report for HPDIP NMS Team
S X

NEWBORN METABOLIC SCREENING INITIATIVE: ACTION PLAN REPORT, NOVEMBER 30, 2010 (FINAL) PAGE 25 OF 71
Table 3: Newborn Metabolic Screening (NMS): Action Plan Chart, January 2011 to March 2014
Actions/ Deliverables
(in bold)
Responsible *Also see
Responsibility, Accountability,
Consultants Summary
(Appendix F)
NMS Policy Document Standards, AHS Roles & Responsibilities
NMS Audit Recommendations Milestone Timelines
S=START, X = COMPLETE
Dependencies (in italics)
Quick Win Jan 2011-Mar 2011
Short Term Apr 2011-Dec 2011
Mid Term Jan 2012-Mar 2013
Long Term Apr 2013-Mar 2014
AHW and other program partners 2.1.3. Create and execute AHS NMS Program
Memorandum of Understanding (MOU) with Health Canada – First Nations Inuit Health (FNIH) Alberta branch, including: NMS Program PPSGs, Document management, Transfer of care between AHS and FNIH, Ownership and sharing of parent information, Ownership and sharing of staff learning and development resources and materials, Communication pathways
HPDIP, HPDIP NMS Team, FNIH
Dependant on relationship with Health Canada - FNIH
S
X
2.2. Develop and implement NMS Program AHS Staff Engagement Strategy
HPDIP NMS Team
Meets Standard 4.2 AHS Roles & Responsibilities Meets NMS Audit Recommendations
S
X
2.2.1. Create NMS Program AHS Staff Engagement Plan
HPDIP NMS Team
Dependant on funding for project staff Dependant on funding to backfill Zone staff
S
X
2.2.2. Develop and test NMS Program AHS staff learning and development materials and resources, e.g., e-learning modules, skill development kits, webinars
HPDIP NMS Team
As above S
X
2.2.3. Implement NMS Program AHS staff learning and development opportunities across related AHS areas, including: Health information management, Public Health, Acute Care, Lab, NMS Lab, MD Lab, Specialty Clinics
HPDIP NMS Team
As above
S
X
2.2.4. Develop NMS Program AHS staff engagement ongoing feedback and review mechanisms
HPDIP NMS Team
As above S
X
2.3. Monitor and report on NMS Program Patient Safety utilizing AHS Reporting and Learning System (RLS) for Patient Safety (2010)
HPDIP NMS Team
Meets Standard 17 AHS Roles & Responsibilities
S
X
2.3.1. Develop and test NMS Program Patient Safety Reporting processes, including: Reporting of
HPDIP NMS Team
Dependent on AHS wide roll out of RLS and patient safety culture
S
X

NEWBORN METABOLIC SCREENING INITIATIVE: ACTION PLAN REPORT, NOVEMBER 30, 2010 (FINAL) PAGE 26 OF 71
Table 3: Newborn Metabolic Screening (NMS): Action Plan Chart, January 2011 to March 2014
Actions/ Deliverables
(in bold)
Responsible *Also see
Responsibility, Accountability,
Consultants Summary
(Appendix F)
NMS Policy Document Standards, AHS Roles & Responsibilities
NMS Audit Recommendations Milestone Timelines
S=START, X = COMPLETE
Dependencies (in italics)
Quick Win Jan 2011-Mar 2011
Short Term Apr 2011-Dec 2011
Mid Term Jan 2012-Mar 2013
Long Term Apr 2013-Mar 2014
adverse events, Close calls and/or hazards 2.3.2. Produce regular and timely NMS Program
Patient Safety reports HPDIP NMS Team
S
X
2.4. Develop NMS Program Emergency/Disaster Management Plans in alignment with AHS Emergency/Disaster Management and Business Continuity processes
AHS Emergency / Disaster Management
Meets Standard 2.4 AHS Roles & Responsibilities
S
X
2.4.1. Develop NMS Lab and MD Lab Business Continuity Plans, including review and update mechanisms
AHS Emergency / Disaster Management
Dependant on funding for Business Continuity Specialist
S
X
2.4.2. Develop Business Continuity Plans for remaining NMS Program components, including review and update mechanisms
AHS Emergency / Disaster Management
S
X
2.5. Develop and implement NMS Program Parent Engagement
HPDIP NMS Team
Meets Standards 5.1; 6.1 AHS Roles and Responsibilities Meets NMS Audit Recommendations
S
X
2.5.1. Create NMS Program Parent Engagement Plan
HPDIP NMS Team
Dependant on funding
S X
2.5.2. Revise, develop, and focus test NMS Program parent information resources, including: Plain language resources and interpretation services e.g., information for parents on: newborn metabolic screening, re-considering declining screening, infants who screen positive, preparing for a potential positive diagnoses, etc.
HPDIP NMS Team
S
X
2.5.3. Develop and implement NMS Program parent information resources distribution mechanisms
HPDIP NMS Team
S
X
2.5.4. Develop translated NMS Program parent information resources (6 major languages) as
HPDIP NMS Team
S X
NEWBORN METABOLIC SCREENING INITIATIVE: ACTION PLAN REPORT, NOVEMBER 30, 2010 (FINAL) PAGE 27 OF 71
Table 3: Newborn Metabolic Screening (NMS): Action Plan Chart, January 2011 to March 2014
Actions/ Deliverables
(in bold)
Responsible *Also see
Responsibility, Accountability,
Consultants Summary
(Appendix F)
NMS Policy Document Standards, AHS Roles & Responsibilities
NMS Audit Recommendations Milestone Timelines
S=START, X = COMPLETE
Dependencies (in italics)
Quick Win Jan 2011-Mar 2011
Short Term Apr 2011-Dec 2011
Mid Term Jan 2012-Mar 2013
Long Term Apr 2013-Mar 2014
recommended by AHS Translation Services 2.5.5. Include NMS Program parent information
resources in prenatal curriculum and resources
HPDIP NMS Team
S X
2.5.6. Develop NMS Program parent information resources feedback mechanisms
HPDIP NMS Team
S X
2.6. Develop and implement NMS Program Communication
HPDIP NMS Team
Meets Standards 3.1; 3.2; 14.2; 14.3; 15.1; 17.1; 17.2 AHS Roles and Responsibilities; Meets NMS Audit Recommendations
S
X
2.6.1. Create NMS Program Communication Plan
HPDIP NMS Team
See 2.5 & 2.7
S X
2.6.2. Develop NMS Program communication materials to align with AHS Communication Visual Identity Standards, e.g., Program FAQ, Graphic element (footprint), AHS logo/NMS Program, NMS materials/resources template guidelines
HPDIP NMS Team
S
X
2.6.3. Integrate NMS Program communication pathways into AHS communication pathways, including: Updates to policies, procedures, standards and guidelines; Opportunities for staff training; Apple Magazine, Insite Announcements, Group emails/postings
HPDIP NMS Team
S
X
2.6.4. Develop NMS Program WebPages on AHS Insite and External AHS website, including: NMS Program Inform Alberta listing, NMS Program Quality Management framework, PPSGs, Parent information resources, Staff learning and development materials, Performance measurement reports, feedback contact form
HPDIP NMS Team,
S
X
2.7. Develop and implement NMS Program Primary Care Provider Engagement with non-AHS staff primary care providers: Family Physicians, Specialists, Nurse Practitioners, Registered Midwives, Primary Care Networks, Registered Nurses
HPDIP NMS Team
Meets Standards 4.2; 5.1; 6.1; 9.1; 9.3; 9.4; 9.6; AHS Roles and Responsibilities Meets NMS Audit Recommendations
S
X
NEWBORN METABOLIC SCREENING INITIATIVE: ACTION PLAN REPORT, NOVEMBER 30, 2010 (FINAL) PAGE 28 OF 71
Table 3: Newborn Metabolic Screening (NMS): Action Plan Chart, January 2011 to March 2014
Actions/ Deliverables
(in bold)
Responsible *Also see
Responsibility, Accountability,
Consultants Summary
(Appendix F)
NMS Policy Document Standards, AHS Roles & Responsibilities
NMS Audit Recommendations Milestone Timelines
S=START, X = COMPLETE
Dependencies (in italics)
Quick Win Jan 2011-Mar 2011
Short Term Apr 2011-Dec 2011
Mid Term Jan 2012-Mar 2013
Long Term Apr 2013-Mar 2014
2.7.1. Create Primary Care Provider Engagement Plan
HPDIP NMS Team
S X
2.7.2. Implement Primary Care Provider Engagement Plan, including: Participation on committees/project teams, Review and feedback on PPSGs, Providing access to AHS NMS Program staff communication resources, Encouraging use of NMS Web page resources specifically PPGS e.g., NMS workup/follow-up clinical algorithms
HPDIP NMS Team
S
X
2.8. Establish NMS Program Knowledge Management structures and processes
HPDIP NMS Team
Meets Standards 2.3 AHS Roles and Responsibilities
S X
2.8.1. Produce and disseminate NMS Literature Review and Environmental Scan
HPDIP NMS Team
S X
3. Establish NMS Program Performance Measurement & Evaluation 3.1. Establish NMS Program Performance
Measurement structures, processes, and reporting HPDIP NMS Team
Meets Standards 2.3; 9.3 AHS Roles and Responsibilities
S
X
3.1.1. Refine and apply the NMS Program Quality Management Framework
HPDIP NMS Team
Dependant on funding for Process Improvement staff
S X
3.1.2. Refine and apply the NMS Program Governance Structure, including: Committees/project teams, Terms of Reference, Roles and responsibilities, Reporting relationships, Project management, Administrative processes, Communication, and Coordination
HPDIP NMS Team
S X
3.1.3. Provide Quality Management learning and development opportunities to NMS Program Action Plan Projects staff and committee members
HPDIP NMS Team
S
X
3.1.4. Develop and produce regular and timely NMS Program performance measurement reporting to inform the Action Plan projects
HPDIP NMS Team
S
X
3.2. Analyze the NMS Program Information Technology (IT) capabilities
AHS Information Technology
Meets Standards 1.1; 1.4; 2.1; 2.2; 2.3; 4.1; 8.1; 10.1; 10.2; 10.3; 10.4; 10.5;10.6; 11.2;11.3; 11.4, 12.1; 13.1; 14.2; 14.3 AHS Roles and Responsibilities
S
X
NEWBORN METABOLIC SCREENING INITIATIVE: ACTION PLAN REPORT, NOVEMBER 30, 2010 (FINAL) PAGE 29 OF 71
Table 3: Newborn Metabolic Screening (NMS): Action Plan Chart, January 2011 to March 2014
Actions/ Deliverables
(in bold)
Responsible *Also see
Responsibility, Accountability,
Consultants Summary
(Appendix F)
NMS Policy Document Standards, AHS Roles & Responsibilities
NMS Audit Recommendations Milestone Timelines
S=START, X = COMPLETE
Dependencies (in italics)
Quick Win Jan 2011-Mar 2011
Short Term Apr 2011-Dec 2011
Mid Term Jan 2012-Mar 2013
Long Term Apr 2013-Mar 2014
AHW
3.2.1. Complete current NMS Lab Information System (LIS) upgrade (i.e., Specimen Gate) in progress, e.g., Date/time field
NMS Lab Dependant on funding for IT staff
S X
3.2.2. Request an update to the NMS Application based on current NMS Lab LIS upgrade, e.g., date/time
HPDIP NMS Team AHW
S X
3.2.3. Complete NMS Program IT systems performance measurement gap analysis, including: Identifying existing NMS Program performance measures and data sources, data ownership, and required measures and data sources
AHS Information Technology AHW
S
X
3.2.4. Review the NMS Program IT systems’ compliance with AHS Health Information Security Standards, e.g., MD Lab database located on U of A server
AHS Information Technology
S X
3.2.5. Assess NMS Program IT systems data integrity and conduct a gap analysis, e.g., accuracy, consistency, missing data, incomplete data, etc.
AHS Information Technology AHW
S
X
3.2.6. Determine the NMS Program IT system requirements to meet the NMS Program performance measurement requirements, e.g., contract for MD Lab “Specimen Gate Lab” and “Office” applications as well as interface module, live PD feed into NMS Application
AHS Information Technology AHW
S
X
3.2.7. Develop NMS Program IT Proposal for any required NMS Program IT system upgrades
AHS Information Technology
S X
3.3. Establish NMS Program Evaluation structures and processes
HPDIP NMS Team
Meets Standards 2.3 AHS Roles and Responsibilities; Meets NMS Audit Recommendations
S
X
3.3.1. Develop an NMS Program evaluation HPDIP NMS
NEWBORN METABOLIC SCREENING INITIATIVE: ACTION PLAN REPORT, NOVEMBER 30, 2010 (FINAL) PAGE 30 OF 71
Table 3: Newborn Metabolic Screening (NMS): Action Plan Chart, January 2011 to March 2014
Actions/ Deliverables
(in bold)
Responsible *Also see
Responsibility, Accountability,
Consultants Summary
(Appendix F)
NMS Policy Document Standards, AHS Roles & Responsibilities
NMS Audit Recommendations Milestone Timelines
S=START, X = COMPLETE
Dependencies (in italics)
Quick Win Jan 2011-Mar 2011
Short Term Apr 2011-Dec 2011
Mid Term Jan 2012-Mar 2013
Long Term Apr 2013-Mar 2014
framework for program and project evaluation Team
S X
3.3.2. Conduct an overall NMS Program Action Plan evaluation and evaluation of projects related to their impact on meeting the 2010 NMS Policy Document standards, e.g., overall and project: PPSGs, NMS Lab staffing, centralized alert management, staff learning & development, parent information resources, provider engagement
HPDIP NMS Team
S X
3.3.3. Identify appropriate NMS Program comparable indicators to evaluate the long term success of the program
HPDIP NMS Team
S
X
4. Establish NMS Program Process Improvement 4.1. Establish NMS Program Process Improvement
structures and processes in alignment with the AHS Improvement Way (AIW)
HPDIP NMS Team
Meets Standards 2.1; 2.3; 4.1; 9.1; 9.5; 9.6; 11.3 AHS Roles and Responsibilities
S
X
4.1.1. Establish NMS Program process improvement (QI) approaches to support and manage improvement projects
HPDIP NMS Team
Dependant on funding for Process Improvement staff
S
X
4.2. Conduct NMS Program Process Improvement (PI) Projects
HPDIP NMS Team
Meets Standards 2.1; 2.3; 4.1; 9.1; 9.5; 9.6; 11.3 AHS Roles and Responsibilities
S
X
4.2.1. Complete NMS Lancet PI Project: Confirm preferred lancet product and implement provincial purchasing processes to potentially reduce inadequate samples, monitor improvements with further improvements if warranted
HPDIP NMS Team
Dependant on funding for Process Improvement staff
S
X
4.2.2. Conduct NMS Lab Date/Time Recording PI Project: Conduct LEAN Assessment to determine process improvements needed related to recording date / time of sample arrival at the NMS Lab, implement tests of change, monitor improvements with further implementation/improvements if warranted
NMS Lab S
X
4.2.3. Conduct NMS Sample Packaging and Transportation PI Project: Conduct a packaging and
HPDIP NMS Team

NEWBORN METABOLIC SCREENING INITIATIVE: ACTION PLAN REPORT, NOVEMBER 30, 2010 (FINAL) PAGE 31 OF 71
Table 3: Newborn Metabolic Screening (NMS): Action Plan Chart, January 2011 to March 2014
Actions/ Deliverables
(in bold)
Responsible *Also see
Responsibility, Accountability,
Consultants Summary
(Appendix F)
NMS Policy Document Standards, AHS Roles & Responsibilities
NMS Audit Recommendations Milestone Timelines
S=START, X = COMPLETE
Dependencies (in italics)
Quick Win Jan 2011-Mar 2011
Short Term Apr 2011-Dec 2011
Mid Term Jan 2012-Mar 2013
Long Term Apr 2013-Mar 2014
transportation point in time study to assess any current gaps, issues in sample transport processes, implement tests of change, monitor improvements through periodic point in time studies with further implementation/improvements if warranted
S X
4.2.4. Conduct NMS Community/Out- Patient Lab Collections Feasibility PI Project: Explore the feasibility and impact of alternate NMS collection models (i.e., collection occurs primarily within community/out-patient labs, including using NMS out-patient order sets), develop improvement projects if warranted
HPDIP NMS Team
S X
4.2.5. Conduct NMS Collections “Discharge Lounge” Concept Feasibility PI Project: Assess the feasibility of a “discharge lounge” concept for rural-remote families to wait in hospital until NMS sample can be obtained at 24 hours of age, develop improvement projects if warranted
HPDIP NMS Team
S X
4.2.6. Conduct RN/LPN After Hours NMS Collections PI Project: Assess the feasibility of educating LPNs/RNs in acute care to collect NMS samples after-hours, when lab collectors are not on shift, develop improvement projects if warranted
HPDIP NMS Team
S X

NEWBORN METABOLIC SCREENING INITIATIVE: ACTION PLAN REPORT, NOVEMBER 30, 2010 (FINAL)
Page 32 of 71
IMPLEMENTATION IMPLEMENTATION EXEMPLARS Two implementation exemplars outline how the actions items in the Action Plan will support AHS in meeting the 2010 NMS Policy Document standards and sub-standards, as well as address the roles and responsibilities of AHS, and the 2009 NMS Audit concerns. The exemplars also illustrate the necessity of working within a quality management framework across program areas in an integrated, coordinated manner in order to deliver an effective and efficient NMS Program.
1. The development and implementation of an overarching AHS NMS Program clinical policy related to the 2010 NMS Policy Document will be completed by April 2012. Twenty-six policies, procedures, standards or guidelines (PPSGs) are to be developed and aligned with the overarching AHS policy. One of the policies to be developed relates to collecting NMS samples on all infants greater than or equal to 24 hours of age prior to discharge from acute care. This policy will allow AHS to maximize screening opportunities and reduce the risk of missing a newborn, screen, result, and/or follow-up. Further, it will assist with meeting standards and sub-standards related to timely NMS collection, transportation, sample analysis, and reporting. Additionally, the policy should reduce the number of public health nursing visits specific to newborn metabolic screening, thereby increasing the capacity of public health nurses to enhance client care in other areas (e.g., breastfeeding support, sleep safety, etc.).
2. The development and implementation of a NMS Program Centralized Alert Management (NMS CAM) process will address several standards and sub-standards in the 2010 NMS Policy Document. The NMS CAM process will provide a central point of contact for AHS staff and AHW related to NMS alert management, ensure daily monitoring of alerts, streamline alert processes and management across Zones, facilitate recollection within the prescribed timeframe, facilitate timely identification of infants with an abnormal screen, and provide data for NMS Program quality assurance.
STAGED APPROACH TO IMPLEMENTATION A staged approach will be used to implement the Action Plan. Action items are staged as ‘Quick Win,’ ‘Short Term,’ ‘Mid Term,’ and ‘Long Term,’ based on priorities, interdependencies with other action items, the length of time required to implement the action, the funding and infrastructure required to implement the action, and timely recruitment of qualified staff to successfully implement the plan.
Implementing the NMS Program Quality Management Framework and Action Plan Governance Structure will be a top priority as these are foundational to supporting quality care and an integrated approach to managing the NMS Program. The development of an overarching AHS NMS Program clinical policy related to the 2010 NMS Policy Document will be initiated within the ‘Quick Win’ time frame. Other actions to be completed within the first three months of Implementation include incorporating the ‘date and time specimen is received’ field into the NMS Lab Information System; completing a number of clinical policies, procedures, standards,

NEWBORN METABOLIC SCREENING INITIATIVE: ACTION PLAN REPORT, NOVEMBER 30, 2010 (FINAL)
Page 33 of 71
and guidelines related to registration, sample collection, and alert management; developing a NMS Program communication plan; creating an engagement plan for primary care providers (including family physicians, specialists, nurse practitioners, registered midwives, primary care networks, and registered nurses); developing a NMS Program Centralized Alert Management process; establishing communication processes with AHW; and completing the NMS literature review and environmental scan.
Action items staged as ‘Short Term,’ ‘‘Mid Term,’ and ‘Long Term’ are contingent on the completion of an earlier action item and /or require funding to purchase equipment and recruit staff. For example, the NMS and Molecular Diagnostic Lab will require information technology (IT) and equipment upgrades and additional staff to meet many of the standards and sub-standards related to sample analysis in the 2010 NMS Policy Document. As these action items are funding dependent, this work will likely begin in April 2011, once budget has been secured for additional staff and equipment.
Staging action items also builds in time for the changes resulting from implementation to be realized throughout AHS, and for the impact to be evaluated, before introducing another major change. For example, statistics show there are likely to be significant gains achieved by collecting the NMS sample on all infants who remain in hospital after 24 hours of age. This action should be implemented and evaluated prior to moving forward with a feasibility study related to collecting the majority of NMS samples within community and out-patient labs. If significant gains can be made with collecting the sample prior to discharge from acute care, an alternate lab-based service delivery model may not be indicated.
A number of other action items will begin in January 2011 but will not be fully implemented until a later stage. Many of the procedures, standards, and guidelines related to sample collection and transportation fall into this category. For example, the procedures, standards, and guidelines related to packaging the sample for transport cannot be written until after the ‘Mid Term’ process improvement project on packaging has been completed.
The Action Plan will be implemented over three years and is sequenced based on priorities, funding requirements, and timely recruitment of qualified staff. Many of these actions are interdependent and will require extensive coordination by the NMS Action Plan Implementation Team and the NMS Interdisciplinary Project Teams under the umbrella of the Steering Committee. Success will be measured by the number of deliverables completed on time, projects coming in on budget, the number of standards and sub-standards achieved, and the integration of the NMS Program Quality Management Framework and Action Plan Governance Structure in all aspects of the NMS Program.

NEWBORN METABOLIC SCREENING INITIATIVE: ACTION PLAN REPORT, NOVEMBER 30, 2010 (FINAL)
Page 34 of 71
FUTURE STATE The overarching goal of the Newborn Metabolic Screening Initiative is to build a comprehensive, enterprise-wide NMS Program to achieve the standards and sub-standards set forth in the 2010 NMS Policy Document. In Phase One, key stakeholders worked collectively to understand the current state of the newborn metabolic screening within AHS. The gaps identified in the action planning process were addressed by developing an integrated Action Plan to improve NMS Program service delivery and program coordination to meet the 2010 NMS Policy Document standards and sub-standards. The Action Plan is the foundation for the development of a comprehensive NMS Program over time.
Achieving Action Plan deliverables will require a collaborative effort across AHS and will bring new AHS partners into the Action Plan Governance Structure. Within Action Plan Implementation, new and current partners will work together to support the infrastructure required to implement the proposed Operational Model within a NMS Program Quality Management Framework. New or expanded partners within AHS include:
Information Technology Services Clinical Policy Quality Performance and Service Improvement Emergency/Disaster Management Patient Safety Communications Alberta Health Link
Achieving Action Plan deliverables will also require strong partnerships with AHW, FNIH physicians, registered midwives, nurse practitioners, and parents/guardians. The Future State Map can be found in Appendix G.
NEWBORN METABOLIC SCREENING INITIATIVE: ACTION PLAN REPORT, NOVEMBER 30, 2010 (FINAL)
Page 35 of 71
EVALUATION PLAN CURRENT PERFORMANCE MEASUREMENT AND EVALUATION During the Action Plan Phase, AHS Population and Public Health (PPH) evaluation specialists identified data sources related to the 2010 NMS Policy Document standards and sub-standards. Performance indicators, data sources, and further data needs were also highlighted. A process evaluation of the Action Plan Phase was developed and will be completed during the Implementation Phase.
FUTURE PERFORMANCE MEASUREMENT AND EVALUATION During Action Plan implementation, a NMS Program Logic Model will be created which will form the basis of an overall NMS Program Evaluation Framework. Baseline performance information will be gathered as new data sources are identified. AHS Information Technology Services (IT) and AHW will be consulted to address current data needs and the data limitations identified above in order to produce accurate performance measurement related to the 2010 NMS Policy Document standards and sub-standards. As the NMS Interdisciplinary Project Teams begin to set priorities and plan projects around the action items, the evaluation specialists will consult with the teams to identify goals and objectives for these projects (e.g., staff learning and development, parent information resources). Guidance will be provided to the teams to develop evaluation questions and to undertake the evaluation for their specific projects.
Evaluation will be embedded throughout the implementation of the Action Plan and a report on overall NMS Program evaluation will be completed at the end of the Implementation Phase. Following implementation, the Program Maintenance Phase will involve the evaluation specialists, with guidance from the NMS Steering Committee, potentially collaborating with NMS representatives from health ministries across Canada to develop long term NMS Program success indicators and ongoing monitoring practices.
REPORTING TO ALBERTA HEALTH AND WELLNESS Reporting to AHW will occur on an annual basis. The annual report will be submitted to the Assistant Deputy Minister of Community and Population Health on June 30th each year and will be a synthesis of the year in review. The report will detail the progress made in achieving the deliverables of the Action Plan, speak to the performance measures for the period, and report on any other relevant program events including a summary of significant incidents.

NEWBORN METABOLIC SCREENING INITIATIVE: ACTION PLAN REPORT, NOVEMBER 30, 2010 (FINAL)
Page 36 of 71
BUDGET ESTIMATE HIGH LEVEL BUDGET ESTIMATE The estimated costs associated with implementing the Action Plan are provided in Table 4. Table 5 provides further breakdown of Year 1 and 2 estimated costs by action item. Current State costs, estimated incremental costs related to Action Plan Implementation, and incremental costs associated with Future State are shown in Table 6. A detailed breakdown of costs is available from the HPDIP NMS team upon request.
In Year 1 (2011-2012), incremental costs associated with Action Plan Implementation are estimated to be $2,498,000. This figure includes approximately $1,518,700 of one-time project costs and $979,200 recurring costs. In Year 2* (2012-2013), the estimated cost of implementing the Action Plan drops to $1,482,090 as many project costs associated with Year 1 will not carry over to the second year. The annualized on-going cost of the Action Plan is estimated to be $1,331,300 for year 3 and beyond. Staff salaries and ongoing equipment costs account for this recurring cost.
* Additional resources may be required depending on the outcomes of the feasibility projects (see Table 3 Action Plan).
Table 5: Year 1 and Year 2 Budget Estimate for Action Plan Actions Year 1 Year 2 Staffing Resources
Services One Time Recurring One Time Recurring 1.1. Develop and implement NMS
Screening Processes including policies, procedures, standards and guidelines
$58,625 $0 $0 $0
Zones Public Health/RN backfill time HPDIP staff in kind NMS Lab staff in kind HIM staff in kind
1.2. Implement NMS Lab/MD Lab Capacity Improvements
$96,400 $525,879 $0 $525,879
NMS and MD Labs staffing
NMS and MD Labs equipment and IT upgrades
1.3. Develop and implement NMS Program Centralized Alert Management Process
$75,265 $281,765 $14,941 $281,765
Zones Public Health backfill time HPDIP NMS team Support for Zones local
alert management Equipment HPDIP staff in kind NMS Lab staff in kind
2.1. Define and maintain NMS Program Collaborative Partnerships $89,900 $1000 $0 $1000
Graphic design Statistician HPDIP staff in kind
Table 4: Summary of Budget Estimate for Action Plan Yr 1
(2011-2012) Yr 2*
(2012-2013) Yr 3 and Beyond
(2013 and Beyond) Incremental one-time cost $ 1,518,733 $ 150,777 $ 0 Incremental recurring cost $ 979,212 $ 352,101 $ 0 Recurring cost from Yr 1 $ 0 $ 979,212 $ 979,212 Recurring cost from Yr 2 $ 0 $ 0 $ 352,101 Total $ 2,497,945 $ 1,482,090 $ 1,331,313

NEWBORN METABOLIC SCREENING INITIATIVE: ACTION PLAN REPORT, NOVEMBER 30, 2010 (FINAL)
Page 37 of 71
Table 5: Year 1 and Year 2 Budget Estimate for Action Plan Actions Year 1 Year 2 Staffing Resources
Services One Time Recurring One Time Recurring 2.2. Develop and implement NMS
Program AHS Staff Engagement Strategy
$126,710 $20,000 $0 $20,000
Zones Public Health/RN backfill time Resources/ materials HPDIP NMS team HPDIP staff in kind Zone staff in kind
2.3. Monitor and report on NMS Program Patient Safety utilizing AHS Reporting and Learning System (RLS) for Patient Safety $0 $0 $0 $0
HPDIP staff in kind
2.4. Develop NMS Program Emergency/ Disaster Management Plans $9,000 $89,900 $0 $89,900
Business Continuity staffing
2.5. Develop and implement NMS Program Parent Engagement
$123,680 $5000 $0 $5000
Resources/materials Translations HPDIP NMS team HPDIP staff in kind
2.6. Develop and implement NMS Program Communication $0 $2000 $0 $2000
Resources/ materials HPDIP staff in kind
2.7. Develop and implement NMS Program Primary Care Provider Engagement $5000 $0 $0 $0
Advertising HPDIP staff in kind
2.8. Establish NMS Program Knowledge Management Structures and Processes $0 $0 $0 $0
HPDIP staff in kind
3.1. Establish NMS Program Performance Measurement Structures and Processes $0 $0 $0 $0
HPDIP staff in kind
3.2. Analyze the NMS Program Performance Measurement and IT Capabilities
$834,003 $0 $113,361 $352,101
IT staffing/contracted services NMS Lab staff in kind MD Lab staff in kind HPDIP staff in kind
3.3. Establish NMS Program Evaluation Structures and Processes $0 $0 $0 $0
HPDIP staff in kind
4.1. Establish NMS Program Process Improvement Structures and Processes
$100,150 $53,668 $22,475 $53,668
Process improvement staffing HPDIP NMS team Supplies HPDIP staff in kind
Subtotals $1,518,733 $979,212 $150,777 $1,331,313
Table 6: Newborn Metabolic Screening Costs (in 1,000s) Future State Cost over 2 Year Period $ 8,460 Current State Cost (2009/10) $ 5,358 Incremental $ 3,102 Incremental cost related to Action Plan: Annualized cost $ 1,331 One time cost (Year 1 and Year 2) $ 1,670 Incremental cost in Future State (related to lab reagent cost)
$ 101
$ 3,102

NEWBORN METABOLIC SCREENING INITIATIVE: ACTION PLAN REPORT, NOVEMBER 30, 2010 (FINAL)
Page 38 of 71
CONCLUSION In order to successfully deliver the Action Plan on time, on target, and on budget, the following conditions must be met:
The Action Plan is approved.
There is continued senior AHS executive support.
There is adequate funding and resources approved and received.
There is continued stakeholder support.
There is continued involvement of internal staff and external primary care providers.
Timelines and deliverables are feasible and achievable.
The recruitment of staff occurs with support from Finance and Human Resources.
The NMS Information Technology systems requirements proposal is defined, funded, and implemented to provide identified infrastructure for the NMS Program.
The actions support patient safety and reduce risk and liability.
The actions are implemented using available evidence and evidence-informed practices.
The recommended Action Plan has the potential to improve NMS Program quality and performance through collaborative actions within AHS in partnership with AHW, FNIH, physicians, registered midwives, nurse practitioners, and parents/guardians. Support for the Action Plan will build a strong foundation for the NMS Program. Most importantly, the actions outlined in the Action Plan will maximize newborn metabolic screening opportunities, thereby contributing to the healthy development of infants and children.

NEWBORN METABOLIC SCREENING INITIATIVE: ACTION PLAN REPORT, NOVEMBER 30, 2010 (FINAL)
Page 39 of 71
REFERENCES 1 Government of Alberta. (March 2010). Alberta Newborn Metabolic Screening Program Policy Document. 2 Government of Alberta. (March 2010). Alberta Newborn Metabolic Screening Program Policy Document. 3 Government of Alberta. (March 2010). Alberta Newborn Metabolic Screening Program Policy Document. 4 Archer, S. (September 2010). Newborn Metabolic Screening Statistics. Presented at the NMS Steering Committee Meeting, September 10, 2010.
5 Alberta Health and Wellness. (November 2006). Newborn Metabolic Screening in Alberta 2002 – 2005. 6 Government of Alberta. (March 2010). Alberta Newborn Metabolic Screening Program Policy Document. 7 Government of Alberta. (March 2010). Alberta Newborn Metabolic Screening Program Policy Document. 8 Alberta Health Services. (2009). Summary of 2009 Audit Results.
9 Government of Alberta. (March 2010). Alberta Newborn Metabolic Screening Program Policy Document. 10 Government of Alberta. (2008). Alberta Newborn Metabolic Screening Program Policies, Standards and Guidelines.
11 Alberta Health Services. (2010). Action Planning Tools. Available from S. Philley, HPDIP. 12 Alberta Health Services. (2010). Specimen Gate Application Data Report, January 1, 2009 – December 31, 2009. [Specimen Gate Application]. Available from S. Archer, NMS Laboratory.
13 Alberta Health Services. (2010). Specimen Gate Application Data Report, January 1, 2009 – December 31, 2009. [Specimen Gate Application]. Available from S. Archer, NMS Laboratory.
14 Alberta Health and Wellness. (2009). Newborn Metabolic Screening Performance Report, January 1, 2009 – December 31, 2009. [NMS Application]. Available from Alberta Health and Wellness Application Portal site, http://portal2.albertawellnet.org/ (login required).
15 Alberta Health and Wellness. (2010). Newborn Metabolic Screening Performance Report, April 1, 2010 – September 1, 2010. [NMS Application]. Available from Alberta Health and Wellness Application Portal site, http://portal2.albertawellnet.org/ (login required).
16 Alberta Health Services. (2010). Births in Alberta Hospitals by Birth Hospital, Length of Stay, April 2009-March 2010. Available from Decision, Integration, Measurement and Reporting Unit.

NEWBORN METABOLIC SCREENING INITIATIVE: ACTION PLAN REPORT, NOVEMBER 30, 2010 (FINAL)
Page 40 of 71
17 Alberta Health Services. (2010). Births in Alberta Hospitals by Birth Hospital, Length of Stay, April 2009-March 2010. Available from Decision, Integration, Measurement and Reporting Unit.
18 Alberta Health Services. (2010). Custom Specimen Gate Application Data Report, January 1, 2009 – December 31, 2009. [Specimen Gate Application]. Available from PerkinElmer.
19 Alberta Health Services. (2010). Number of Newborn Metabolic Screens completed by Calgary Zone Public Health Nurses, April, 1, 2009 – March 31, 2010. [PHANTIM Database]. Available from Population Health Surveillance and Community Data Management.
20 Calgary Laboratory Services. (2010). Calgary Laboratory Services Inpatient and Outpatient Newborn Metabolic Screening Statistics, March 2010 – August 2010. Available from Calgary Laboratory Services.
21 Alberta Health Services. (2010). Custom Specimen Gate Application Data Report, January 1, 2009 – December 31, 2009. [Specimen Gate Application]. Available from PerkinElmer.
22 Alberta Health Services. (2010). Births in Alberta Hospitals by Birth Hospital, Length of Stay, April 2009-March 2010. Available from Decision, Integration, Measurement and Reporting Unit.
23 Government of Alberta. (March 2010). Alberta Newborn Metabolic Screening Program Policy Document
24 Suddes, M. (2010). Evaluation of Health Services Performance: Quality and Safety Programs, Quality Indicators. Presentation http://iweb.calgaryhealthregion.ca/programs/stroke/qualitymanagement.htm 25 Note. From Calgary Stroke Program Quality Management Framework by Alberta Health Services 2009. Adapted with permission.
26 Suddes, M. (2010). Evaluation of Health Services Performance: Quality and Safety Programs, Quality Indicators. Presentation http://iweb.calgaryhealthregion.ca/programs/stroke/qualitymanagement.htm 27 Schultz, LA. (In press). Newborn Metabolic Screening: Evidence for the Benefit of Health Promotion Program Development.

NEWBORN METABOLIC SCREENING INITIATIVE: ACTION PLAN REPORT, NOVEMBER 30, 2010 (FINAL) Page 41 of 71
APPENDICES
APPENDIX A: AHW NMS PROGRAM DIRECTIVE TO AHS (APRIL 30, 2010)
APPENDIX B: COMMITTEE MEMBERS, CONSULTANTS, AND CONTRIBUTORS
APPENDIX C: WORKING GROUP ACTION PLANNING TOOLS
APPENDIX D: NMS PROCESSES: CURRENT STATE MAP
APPENDIX E: ACTIONS TO MEET 2010 NMS POLICY DOCUMENT STANDARDS
APPENDIX F: ACTION PLAN RESPONSIBILITY, ACCOUNTABILITY &
CONSULTANTS SUMMARY
APPENDIX G: NMS PROCESSES: FUTURE STATE MAP
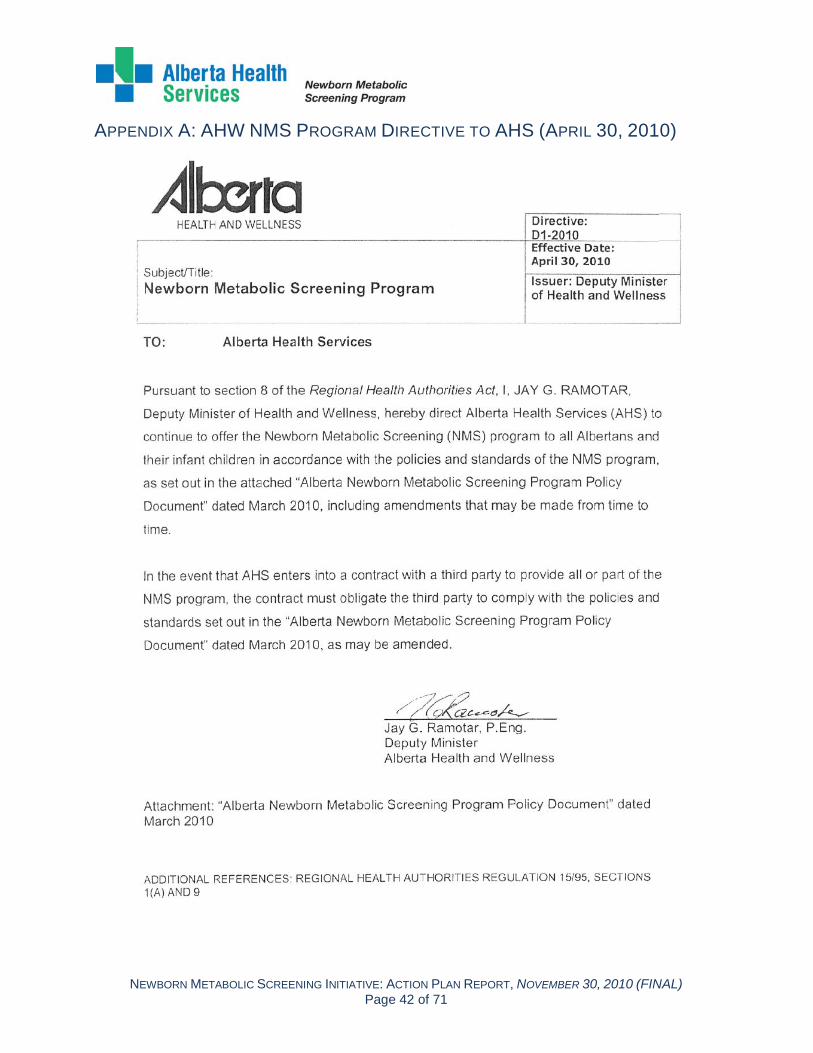
NEWBORN METABOLIC SCREENING INITIATIVE: ACTION PLAN REPORT, NOVEMBER 30, 2010 (FINAL)Page 42 of 71
APPENDIX A: AHW NMS PROGRAM DIRECTIVE TO AHS (APRIL 30, 2010)

NEWBORN METABOLIC SCREENING INITIATIVE: ACTION PLAN REPORT, NOVEMBER 30, 2010 (FINAL) Page 43 of 71
APPENDIX B: COMMITTEE MEMBERS, CONSULTANTS, AND CONTRIBUTORS * = HPDIP NMS Core Planning Group member
Newborn Metabolic Screening Steering Committee *Shelly Philley Director, Reproductive Health, Healthy Child and
Youth Development, Health Promotion, Disease and Injury Prevention, Population and Public Health
Co-Chair
Tammy Hofer Vice President, Laboratory Services Co-Chair
*Alison Nelson Manager, Screening Programs, Health Promotion, Disease and Injury Prevention, Population and Public Health
Member
Barbara Smith Project Manager (Alberta Health and Wellness) Member
Brent Windwick Legal Counsel, Legal and Privacy Member
Cheryl Bourassa Executive Director, Emergency and Disaster Management, Population and Public Health
Member
Christine Westerlund Site Director, Stollery Children’s Hospital, Edmonton Zone
Member
Debbie Mcniel Director, Public Health Innovation and Decision Support, Population and Public Health
Member
Donna Koch Executive Director, Public Health, Primary Care and Chronic Disease Management, North Zone
Member
*Donna Rose Senior Strategic and Integrated Service Planner, North Team
Member
Dr. Fiona Bamforth Director of Newborn Screening Lab, Professor and Chair, Medical Biochemist, Laboratory Medicine and Pathology
Member
Dr. Gloria Keays Associate Medical Officer of Health, Edmonton Zone Member
Elizabeth Kyplain Nursing Practice Consultant, Community Health Nursing (Health Canada-First Nations Inuit Health, Alberta)
Member
Heather Crosland Director, Women's Health Grey Nuns and Misericordia Hospital (Covenant Health)
Member
Janice Blair Director, Public Health, South Zone Member
Jennifer Currie Executive Director, Public Health, Primary Care, and Chronic Disease Management, Central Zone
Member
Laurie Blahitka Executive Director, Public Health, Primary Care, Chronic Disease, and Allied Health, Calgary Zone
Member
Leah Feist Program Manager, Maternal Child Health Program, Edmonton Zone
Member
*Maureen Devolin Manager, Sexual and Reproductive Health, Health Promotion, Disease and Injury Prevention, Population and Public Health
Member
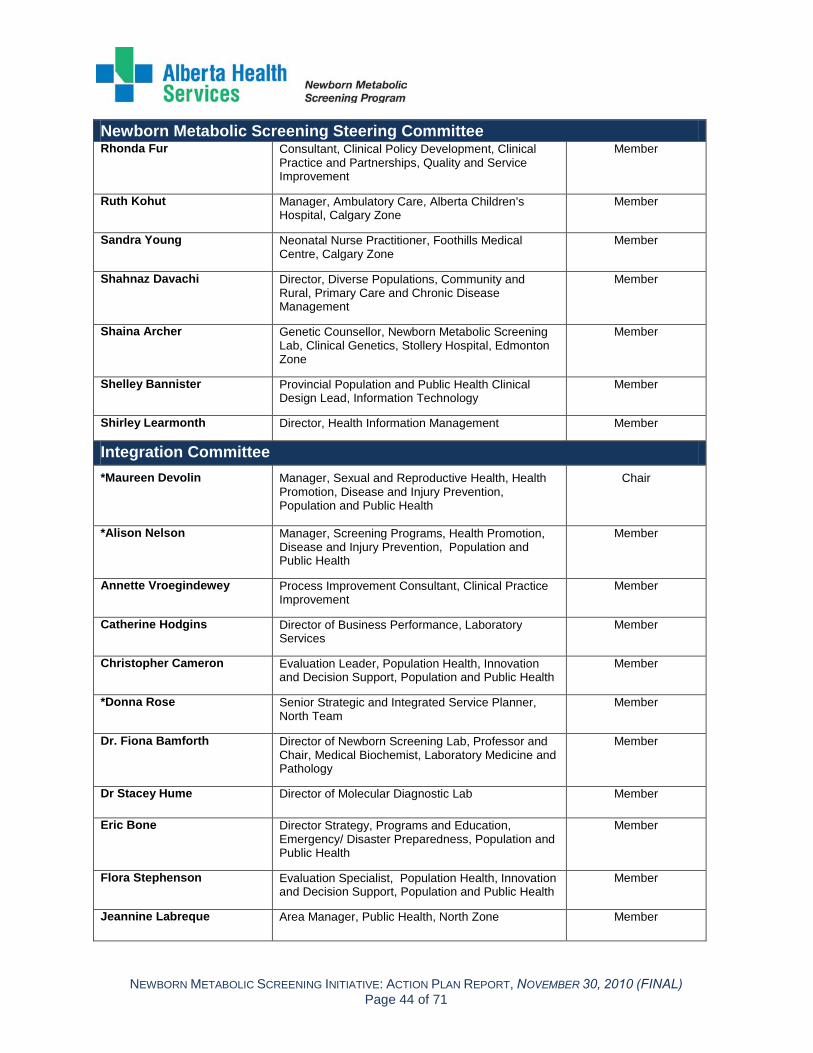
NEWBORN METABOLIC SCREENING INITIATIVE: ACTION PLAN REPORT, NOVEMBER 30, 2010 (FINAL) Page 44 of 71
Newborn Metabolic Screening Steering Committee Rhonda Fur Consultant, Clinical Policy Development, Clinical
Practice and Partnerships, Quality and Service Improvement
Member
Ruth Kohut Manager, Ambulatory Care, Alberta Children’s Hospital, Calgary Zone
Member
Sandra Young Neonatal Nurse Practitioner, Foothills Medical Centre, Calgary Zone
Member
Shahnaz Davachi Director, Diverse Populations, Community and Rural, Primary Care and Chronic Disease Management
Member
Shaina Archer Genetic Counsellor, Newborn Metabolic Screening Lab, Clinical Genetics, Stollery Hospital, Edmonton Zone
Member
Shelley Bannister Provincial Population and Public Health Clinical Design Lead, Information Technology
Member
Shirley Learmonth Director, Health Information Management Member
Integration Committee *Maureen Devolin Manager, Sexual and Reproductive Health, Health
Promotion, Disease and Injury Prevention, Population and Public Health
Chair
*Alison Nelson Manager, Screening Programs, Health Promotion, Disease and Injury Prevention, Population and Public Health
Member
Annette Vroegindewey Process Improvement Consultant, Clinical Practice Improvement
Member
Catherine Hodgins Director of Business Performance, Laboratory Services
Member
Christopher Cameron Evaluation Leader, Population Health, Innovation and Decision Support, Population and Public Health
Member
*Donna Rose Senior Strategic and Integrated Service Planner, North Team
Member
Dr. Fiona Bamforth Director of Newborn Screening Lab, Professor and Chair, Medical Biochemist, Laboratory Medicine and Pathology
Member
Dr Stacey Hume Director of Molecular Diagnostic Lab Member
Eric Bone Director Strategy, Programs and Education, Emergency/ Disaster Preparedness, Population and Public Health
Member
Flora Stephenson Evaluation Specialist, Population Health, Innovation and Decision Support, Population and Public Health
Member
Jeannine Labreque Area Manager, Public Health, North Zone Member

NEWBORN METABOLIC SCREENING INITIATIVE: ACTION PLAN REPORT, NOVEMBER 30, 2010 (FINAL) Page 45 of 71
Integration Committee Mary John Manager, Women’s Health Services, Calgary Zone Member
*Maryann Kusmirski Research Project Coordinator, Sexual and Reproductive Health, Health Promotion, Disease and Injury Prevention, Population and Public Health
Member
Michael Essex Enterprise Architect for Public Health, Information Technology
Member
Michael Sambir Director, Clinical Policy, Implementation and Evaluation, Quality and Service Improvement
Member
Mikie Mork Director, Patient Safety, Quality and Service Improvement
Ad hoc
Reanne Mason Registered Midwife (Calgary) Member
Rhonda Fur Consultant, Clinical Policy Development, Clinical Practice and Partnerships, Quality and Service Improvement
Member
Ruth Kohut Manager, Ambulatory Care, Alberta Children’s Hospital, Calgary Zone
Member
Shelley Bannister Provincial, Population and Public Health Clinical Design Lead, Information Technology
Member
Shirley Learmonth Director, Health Information Management Member
*Stephanie Patterson Health Promotion Specialist, Screening Programs, Health Promotion, Disease and Injury Prevention, Population and Public Health
Member
Registration Working Group Shirley Learmonth Director, Health Information Management Co-Chair
*Maryann Kusmirski Research Project Coordinator, Sexual and Reproductive Health, Health Promotion, Disease and Injury Prevention, Population and Public Health
Co-Chair
Cheryl Parkes Manager, Obstetrics, Royal Alexandra Hospital, Edmonton Zone
Member
Christy Groves Coordinator, Patient Registration, Edmonton Zone Member
Gail Hachey Health Information Management Supervisor, North Zone
Member
Grace Bole-Campbell Lead, Registration Systems Management, Clinical Transformation, Information Technology
Ad Hoc
Marilyn Ritchie Supervisor Registration, Patient Information and Business Office, Rockyview General Hospital, Calgary Zone
Member
Michael Essex Enterprise Architect for Public Health, Information Technology
Member

NEWBORN METABOLIC SCREENING INITIATIVE: ACTION PLAN REPORT, NOVEMBER 30, 2010 (FINAL) Page 46 of 71
Registration Working Group Nicole Delaney Health Information Management Administrative
Supervisor , Patient Registration, Switchboard and Information, Edmonton Zone
Member
Patti O'Neill Health Information Management Supervisor, Central Zone
Member
Peggy Colborne Manager, Registration, Switchboard and Patient Information.
Member
Shirley Martin Health Information Management Supervisor, Patient Information and Switchboard, Medicine Hat and Area, South Zone
Member
Tracey Pavlick Health Information Management Supervisor, Registration, Central Zone
Member
Sample Collections Working Group Jeannine Labrecque Area Manager, Public Health, North Zone Co-Chair
Mary John Manager, Women’s Health Services, Calgary Zone Co-Chair
*Maryann Kusmirski Research Project Coordinator, Sexual and Reproductive Health, Health Promotion, Disease and Injury Prevention, Population and Public Health
Co-Chair
Anna Marshall Maternal Child Coordinator (West), South Zone Member
Annette Vroegindewey Process Improvement Consultant, Clinical Practice Improvement
Member
Barbara Romansky Lab Technologist III, Royal Alexandra Hospital, Edmonton Zone
Member
Christina Beck Clinical Supervisor, Alberta Children’s Hospital (Calgary Lab Services)
Member
Elizabeth Kyplain Nursing Practice Consultant, Community Health Nursing (Health Canada-First Nations Inuit Health, Alberta)
Member
Jocelyn Churchill Lead, Perinatal and Postpartum Community Services, Calgary Zone
Member
Karen Pelletier Unit Supervisor, Northern Alberta Neonatal Intensive Care Program, Royal Alexandra Hospital, Edmonton Zone
Member
Leslie Doan Public Health Manager, Central Zone Member
Linda Johnston Manager, Public Health Nursing (East), South Zone Member
Marilyn Young Manager, Postpartum Community Services, Calgary Zone
Member
Reanne Mason Registered Midwife (Calgary)
Member

NEWBORN METABOLIC SCREENING INITIATIVE: ACTION PLAN REPORT, NOVEMBER 30, 2010 (FINAL) Page 47 of 71
Sample Collections Working Group Stacey Newton Manager, Healthy Beginnings, Public Health,
Edmonton Zone Member
Teri Langlois Senior Practice Consultant, Interprofessional Practice, Health Profession Strategy and Practice
Member
Transportation Working Group Catherine Hodgins Director, Business Performance, Laboratory
Services Co-Chair
*Alison Nelson Manager, Screening Programs, Health Promotion, Disease and Injury Prevention, Population and Public Health
Co-Chair
Brynn Rasmussen Laboratory Assistant II, Newborn Metabolic Screening Laboratory, University of Alberta Hospital, Edmonton and Area, Laboratory Services
Member
Carol Stirling Area Manager, Public Health, North Zone Member
Christine Lemaire Acting Manager, Operational Services (Calgary Lab Services)
Member
Cynthia Gaudry Lab Supervisor, Central Alberta, Laboratory Services
Member
Donna Macklin Community Health Nurse, South Zone Member
Holly Calliou Maskwacis Community Health Services, Hobbema, Treaty 6 (Health Canada - First Nations Inuit Health)
Member
Julie Nordstrom Nurse In Charge, Atikameg Health Centre, Atikameg, Treaty 8 (Health Canada - First Nations Inuit Health)
Member
Kathy Sokol Director, Logistics Supply Management, Contracting, Procurement and Supply Management
Member
Layol McRae Lab Supervisor, Medicine Hat Lab, Laboratory Services
Member
Lynn Kelly Manager, Transportation, Diagnostic Laboratory Services (DynaLife DX)
Member
Michelle Brown Manager, Specimen Logistics, Provincial Laboratory for Public Health
Member
Monica Chabot Lab Technologist III, Grande Prairie Lab, Laboratory Services
Member
Sandy Phillips Public Health Manager, Rural Airdrie, Didsbury, Strathmore and Thornhill, Calgary Zone
Member
Stacey Newton Healthy Beginnings Consultant, Public Health, Edmonton Zone
Member
Theresa Barrett Registered Midwife (Calgary) Member

NEWBORN METABOLIC SCREENING INITIATIVE: ACTION PLAN REPORT, NOVEMBER 30, 2010 (FINAL) Page 48 of 71
Sample Analysis Working Group Dr. Fiona Bamforth Director, Newborn Screening Lab, Professor and
Chair, Medical Biochemist, Laboratory Medicine and Pathology
Co-chair
Dr. Stacey Hume Director, Molecular Diagnostics Lab Co-chair
*Maryann Kusmirski Research Project Coordinator, Sexual and Reproductive Health, Health Promotion, Disease and Injury Prevention, Population and Public Health
Co-chair
Jolene Yuen-Jung Laboratory Technologist, Newborn Metabolic Screening Lab, University of Alberta Hospital, Edmonton and Area, Laboratory Services
Member
Lucille Journault Manager of University Hospital, Edmonton and Area, Laboratory Services
Member
Mark Hicks Senior Clinical Molecular Technologist, Molecular Diagnostic Lab
Member
Ruth Nadeau Lab Technologist, Newborn Metabolic Screening Lab, University of Alberta Hospital, Edmonton and Area, Laboratory Services
Member
Transfer of Care Working Group Ruth Kohut Manager, Ambulatory Care, Alberta Children's
Hospital, Calgary Zone Co-chair
*Alison Nelson Manager, Screening Programs, Health Promotion, Disease and Injury Prevention, Population and Public Health
Co-chair
Catherine Hill Manager, Specialty Clinics, Stollery Children’s Hospital, Edmonton Zone
Member
Dr. Alicia Chan Physician, Molecular Disorders/Genetics, Lab, Edmonton
Member
Dr. David Roseman Community Pediatrician (Edmonton) Member
Dr. Floyd Snyder Director, Biochemical Genetics Lab, Calgary Member
Dr. Gloria Keays Associate Medical Officer of Health, Edmonton Zone Member
Dr. Jill Boulton Neonatologist, Calgary Consultant
Dr. John Van Aerde Neonatologist, Edmonton Consultant
Dr. Jonathan Dawrant Pediatric Endocrinologist, Alberta Children’s Hospital, Calgary Zone
Member
Dr. Leslie Cunning Medical Director (Calgary Rural Primary Care Network)
Member
Dr. Mark Montgomery Physician, Cystic Fibrosis Clinic, Alberta Children’s Hospital, Calgary Zone
Member

NEWBORN METABOLIC SCREENING INITIATIVE: ACTION PLAN REPORT, NOVEMBER 30, 2010 (FINAL) Page 49 of 71
Transfer of Care Working Group Dr. Peter Zuberbuhler Physician, Cystic Fibrosis Clinic, Stollery Children’s
Hospital, Edmonton Zone Consultant
Dr. Robin Casey Physician Director, Inherited Metabolic Disorders Program, Alberta Children’s Hospital, Calgary Zone
Member
Dr. Seth Marks Physician, General Endocrinology and Diabetes Clinics, Edmonton Zone
Member
Gloria Letendre Public Health Nurse (Health Canada – First Nations Inuit Health)
Member
Janet Kiist Manager, Public Health, Central Zone Member
Margaret Lilley Genetic Counsellor, Molecular Diagnostic Lab, Clinical Genetics, Stollery Hospital, Edmonton Zone
Member
Shaina Archer Genetic Counsellor, Newborn Metabolic Screening Lab, Clinical Genetics, Stollery Hospital, Edmonton Zone
Member
Sheena Clifford Primary Care Coordinator, Calgary Zone Consultant
Tracy M. Smith Area Manager, Public Health, North Zone Member
Consultants / Contributors Amanda Wilson Administration Assistant, Chronic Disease Prevention and Oral Health, Health
Promotion, Disease and Injury Prevention, Population and Public Health
*Angel Mercier Administrative Assistant, Reproductive Health, Healthy Child and Youth Development, Health Promotion, Disease and Injury Prevention, Population and Public Health
Anne Marie McInnis Community Development Coordinator, Child and Youth Development, Health Promotion, Disease and Injury Prevention, Population and Public Health
Bretta Maloff Executive Director, Health Promotion, Disease and Injury Prevention, Population and Public Health
Carol Gray Vice President, Population and Public Health
Cecille Quinto-Ireland Senior Business Analyst, Business Advisory Services
Christine Couturier Public Health Manager, Central Zone
Claire McCrank Vice President, Rural and Primary Care IT Services, Information Technology
Claudia Doyle Manager, Data Reporting and Processes, Information Technology
Claye Hopkins Business Advisory Services Manager, Laboratory and Diagnostic Imaging Services
Connie Holland Secretary III, Injury Prevention, Health Promotion, Disease and Injury Prevention, Population and Public Health
NEWBORN METABOLIC SCREENING INITIATIVE: ACTION PLAN REPORT, NOVEMBER 30, 2010 (FINAL) Page 50 of 71
Consultants / Contributors Dawn Friesen Senior Manager (Alberta Health and Wellness)
*Debbie Charteris Secretary III, Health Promotion, Disease and Injury Prevention, Population and Public Health
Deb Shera IT Clinical Transformation, Information Technology
Eileen Mercer Manager, Quality Improvement, Screening Programs, Health Promotion, Disease and Injury Prevention, Population and Public Health
Ellen Moffat Health Promotion Coordinator, Child and Youth Development, Health Promotion, Disease and Injury Prevention,
Fiona Murray-Galbraith Director, Public Health, North Zone
Glenn McRae Executive Director, Patient Safety, Quality and Service Improvement
Heather Sereda Business Analyst (Calgary Lab Services)
James Shrimpton Lead (Helix Design Communications)
Jennifer Scott -Munoz Outreach Worker, Sexual and Reproductive Health, Health Promotion, Disease and Injury Prevention, Population and Public Health
Joan Silzer Research Project Coordinator, Sexual and Reproductive Health, Health Promotion, Disease and Injury Prevention, Population and Public Health
Julie Whitney IT Lead, Clinical Transformation Deployment, Information Technology
Kathy Ervin Director, Lab Information System and Millennium System (Calgary Lab Services)
Kim Gall Coordinator (Newborn Screening Ontario)
Leslie Barker Research Project Coordinator, Early Childhood, Health Promotion, Disease and Injury Prevention, Population and Public Health
Lori Anne Schultz Research Project Coordinator, Sexual and Reproductive Health, Health Promotion, Disease and Injury Prevention, Population and Public Health
Louise Holub Program Assistant, Public Health, North Zone
Louise Maurik Area Manager, Public Health, North Zone
Margo Kirkwood CIS Data Lead, Health Services Management, Public Health, Data Integration, Measurement and Reporting
Mark Dixon Director (Acting), Marketing and Creative Services, Communications
Mark Helmak Director, Rural and Community Operations, Information Technology
*Mary Wandzura Secretary III, Sexual and Reproductive Health, Health Promotion, Disease and Injury Prevention, Population and Public Health
Michael Suddes Manager, Calgary Stroke Program, Foothills Medical Centre, Calgary Zone

NEWBORN METABOLIC SCREENING INITIATIVE: ACTION PLAN REPORT, NOVEMBER 30, 2010 (FINAL) Page 51 of 71
Consultants / Contributors Ray Harrison Community Development Coordinator, Sexual and Reproductive Health,
Health Promotion, Disease and Injury Prevention, Population and Public Health
Rhonda Patton Manager, Healthy Child and Youth Development, Health Promotion, Disease and Injury Prevention, Population and Public Health
Sandra Whittleton Secretary III, Reducing Disparities, Health Promotion, Disease and Injury Prevention, Population and Public Health
Robert Septou Applications Consultant, Central Zone, Information Technology
Ruth Griffeth Health Information Analyst, Data Integration, Measurement and Reporting
Shaunne Letourneau Director, Health Link Alberta
Tara Duhaney Health Promotion Coordinator, Sexual and Reproductive Health, Health Promotion, Disease and Injury Prevention, Population and Public Health
Todd Schnirer Director, Analytical Support, Budgeting and Financial Planning
Tracy Smith Area Manager, Public Health, North Zone
Vera E. Hill Program Assistant, Public Health, North Zone
Wendy Farrance Health Promotion Coordinator, Child and Youth Development, Health Promotion, Disease and Injury Prevention, Population and Public Health
Wendy MacGregor Secretary III, Screening Programs, Health Promotion, Disease and Injury Prevention, Population and Public Health
Wes Schreiber Manager, Information Management, Screening Programs, Health Promotion, Disease and Injury Prevention, Population and Public Health

NEWBORN METABOLIC SCREENING INITIATIVE: ACTION PLAN REPORT, NOVEMBER 30, 2010 (FINAL)Page 52 of 71
APPENDIX C: WORKING GROUP ACTION PLANNING TOOLS
Working Group Process Map (SAMPLE)
NMS Standards Assessment Tool (SAMPLE)
SAMPLE
SAMPLE

NEWBORN METABOLIC SCREENING INITIATIVE: ACTION PLAN REPORT, NOVEMBER 30, 2010 (FINAL)Page 53 of 71
Working Group Action Planning Tool (SAMPLE)SAMPLE

NEWBORN METABOLIC SCREENING INITIATIVE: ACTION PLAN REPORT, NOVEMBER 30, 2010 (FINAL)Page 54 of 71
APPENDIX D: NMS PROCESSES: CURRENT STATE MAP

NEWBORN METABOLIC SCREENING INITIATIVE: ACTION PLAN REPORT, NOVEMBER 30, 2010 (FINAL) Page 55 of 71
APPENDIX E: ACTIONS TO MEET 2010 NMS POLICY DOCUMENT STANDARDS Actions To Meet 2010 NMS Policy Document Standards NMS Actions 2010 NMS Policy Document (Alberta Health & Wellness, dated March 2010) Accountability Action 3.2
1. Clear accountability and lines of responsibility are a requirement for effective program delivery.
1.1 AHS must implement and deliver the NMS program.
Standard met √ 1.2 The CEO of AHS shall be accountable for whether the NMS Program operates in accordance with current AHW policy and standards.
Standard met √ 1.3 AHS must designate a senior executive with responsibility for the NMS program delivery plan and adherence to current AHW policy and standards.
Actions 1.3; 3.2 1.4
AHS must designate NMS managers and NMS contacts with responsibility for monitoring and reporting on the NMS program, in sufficient numbers to operate the program in adherence to current AHW policy and standards.
Program Delivery Timeline
Actions 1.1; 3.2; 4.1
2. The goal of the program is that all babies have an initial screen reported on or before the 10th day of age (except for DNA testing of CF results).
2.1 The expectation is that AHS will align its processes so that initial screens are reported wherever reasonably possible on or before the 10th day of age.
Actions 1.1; 3.2 2.2 Guidelines provided within this document are benchmarks for processes in the screening process and shall not supersede the overall reporting standard of 10 days.
Actions 1.1; 2.8; 3.1; 3.2; 3.3; 4.1 2.3
AHS must evaluate all aspects of program delivery and whenever possible reduce delays and strive to minimize the period of time between birth and reporting of screening results.
Action 2.4 2.4 AHS must develop an emergency preparedness plan and maintain delivery of NMS program services during emergencies and infectious disease events.
Procedure and Operational Policies
Actions 1.1; 2.6 3. Procedures and
operational policies related to program activity must be developed, implemented provincially and maintained to reflect current AHW policy.
3.1
Operational policies, procedures, plans, and training and informational materials related to NMS program delivery must be submitted to AHW on request and AHW may request modifications to these documents.
Action 2.6 3.2 AHW must be notified of any significant operational changes to the NMS Program in a timely manner.
Access
Actions 1.1; 3.2 4. Newborn Metabolic
Screening is part of the health care services provided to infants born in Alberta.
4.1 AHS must make all reasonable efforts to screen all infants born in Alberta.
Actions 1.1; 2.2; 2.7 4.2 AHS must provide training to staff registering newborns in the Person Directory application, obtaining the screening samples and accessing the NMS Application.
Action 1.1 4.3 AHS must register infants born in Alberta in the Person Directory application through the "add newborn" function within 24 hours of birth.
Actions 1.1; 2.5; 2.7
5. Newborn metabolic screening is part of the standard of care that every baby born in Alberta receives. Parents/ guardians must be informed about the nature and purpose of newborn metabolic screening.
5.1
The health professional taking the sample for screening or the primary care provider who is requisitioning the sample must inform the parent of the reason for the screen and provide information about the program before the sample is collected.
Refusals
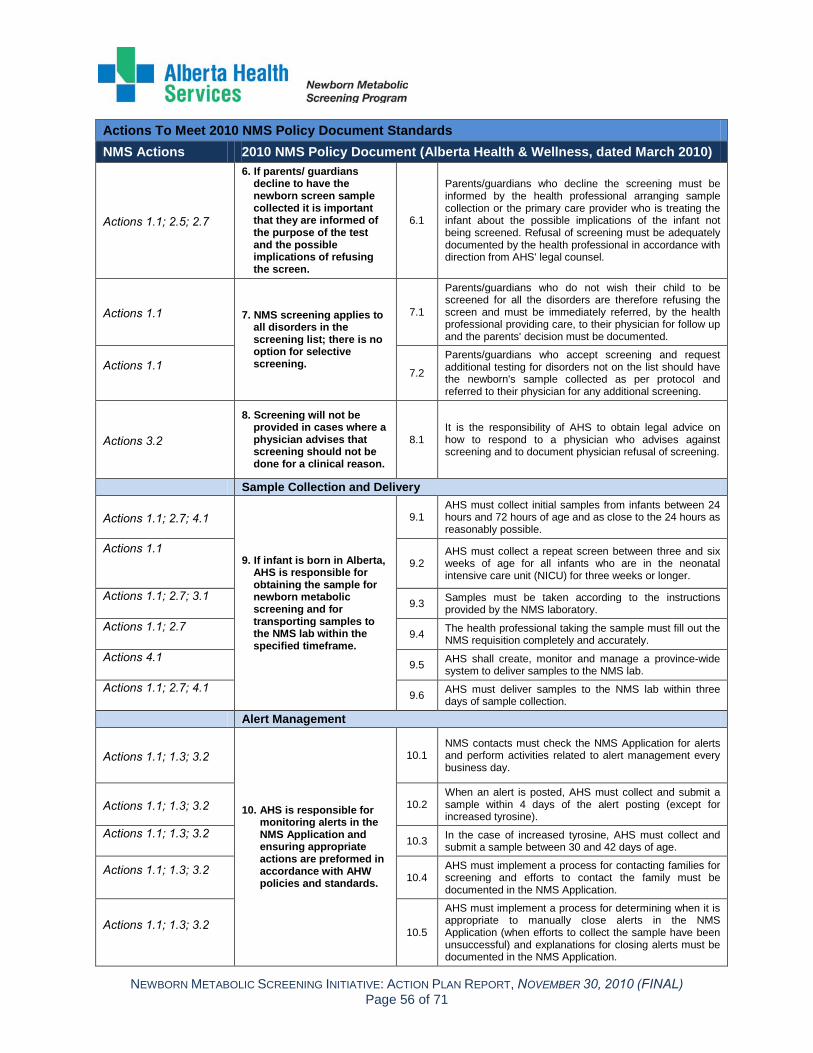
NEWBORN METABOLIC SCREENING INITIATIVE: ACTION PLAN REPORT, NOVEMBER 30, 2010 (FINAL) Page 56 of 71
Actions To Meet 2010 NMS Policy Document Standards NMS Actions 2010 NMS Policy Document (Alberta Health & Wellness, dated March 2010)
Actions 1.1; 2.5; 2.7
6. If parents/ guardians decline to have the newborn screen sample collected it is important that they are informed of the purpose of the test and the possible implications of refusing the screen.
6.1
Parents/guardians who decline the screening must be informed by the health professional arranging sample collection or the primary care provider who is treating the infant about the possible implications of the infant not being screened. Refusal of screening must be adequately documented by the health professional in accordance with direction from AHS' legal counsel.
Actions 1.1 7. NMS screening applies to all disorders in the screening list; there is no option for selective screening.
7.1
Parents/guardians who do not wish their child to be screened for all the disorders are therefore refusing the screen and must be immediately referred, by the health professional providing care, to their physician for follow up and the parents' decision must be documented.
Actions 1.1 7.2
Parents/guardians who accept screening and request additional testing for disorders not on the list should have the newborn's sample collected as per protocol and referred to their physician for any additional screening.
Actions 3.2
8. Screening will not be provided in cases where a physician advises that screening should not be done for a clinical reason.
8.1 It is the responsibility of AHS to obtain legal advice on how to respond to a physician who advises against screening and to document physician refusal of screening.
Sample Collection and Delivery
Actions 1.1; 2.7; 4.1
9. If infant is born in Alberta, AHS is responsible for obtaining the sample for newborn metabolic screening and for transporting samples to the NMS lab within the specified timeframe.
9.1 AHS must collect initial samples from infants between 24 hours and 72 hours of age and as close to the 24 hours as reasonably possible.
Actions 1.1 9.2
AHS must collect a repeat screen between three and six weeks of age for all infants who are in the neonatal intensive care unit (NICU) for three weeks or longer.
Actions 1.1; 2.7; 3.1 9.3 Samples must be taken according to the instructions
provided by the NMS laboratory. Actions 1.1; 2.7
9.4 The health professional taking the sample must fill out the NMS requisition completely and accurately.
Actions 4.1 9.5 AHS shall create, monitor and manage a province-wide
system to deliver samples to the NMS lab. Actions 1.1; 2.7; 4.1
9.6 AHS must deliver samples to the NMS lab within three days of sample collection.
Alert Management
Actions 1.1; 1.3; 3.2
10. AHS is responsible for monitoring alerts in the NMS Application and ensuring appropriate actions are preformed in accordance with AHW policies and standards.
10.1 NMS contacts must check the NMS Application for alerts and perform activities related to alert management every business day.
Actions 1.1; 1.3; 3.2 10.2 When an alert is posted, AHS must collect and submit a sample within 4 days of the alert posting (except for increased tyrosine).
Actions 1.1; 1.3; 3.2 10.3 In the case of increased tyrosine, AHS must collect and
submit a sample between 30 and 42 days of age.
Actions 1.1; 1.3; 3.2 10.4
AHS must implement a process for contacting families for screening and efforts to contact the family must be documented in the NMS Application.
Actions 1.1; 1.3; 3.2 10.5
AHS must implement a process for determining when it is appropriate to manually close alerts in the NMS Application (when efforts to collect the sample have been unsuccessful) and explanations for closing alerts must be documented in the NMS Application.

NEWBORN METABOLIC SCREENING INITIATIVE: ACTION PLAN REPORT, NOVEMBER 30, 2010 (FINAL) Page 57 of 71
Actions To Meet 2010 NMS Policy Document Standards NMS Actions 2010 NMS Policy Document (Alberta Health & Wellness, dated March 2010)
Actions 1.1; 1.3; 3.2 10.6
If the newborn has moved out of province, AHS shall notify a person responsible for NMS in the jurisdiction where the infant resides of the status of screening and document notification in the NMS Application.
Sample Testing
Actions 1.1; 1.2
11. AHS must designate a single laboratory as the provincial NMS laboratory.
11.1 The NMS laboratory is responsible for timely testing of all initial and repeated screens.
Actions 1.2; 3.2 11.2
The NMS lab must be fully operational on all business days. It must not be closed for more than two consecutive days.
Actions 1.1; 3.2; 4.1 11.3 The NMS laboratory must accurately record the date and
time when a sample arrives in the NMS laboratory.
Actions 1.1; 1.2; 3.2 11.4
The NMS laboratory must enter a sample in the laboratory information system whenever possible on the day received and in any event within two days of arrival.
Actions 1.1; 1.2 11.5
The NMS laboratory must analyze samples whenever possible on the day received and in any event within two days of arrival.
Actions 1.1; 1.2 11.6
The NMS laboratory must check the NMS Application for alerts and perform activities related to alert management every business day.
Actions 1.1 11.7
Laboratory polices related to retention, security, access to, quality assurance and reporting of NMS samples must be submitted to AHW on request and AHW may request modifications to these documents.
Actions 3.2
12. AHS must designate a single laboratory as the NMS Molecular Diagnostic Laboratory.
12.1 The Molecular Diagnostic Laboratory is responsible for the DNA testing component of CF screening.
Research
Actions 1.1; 3.2 13. The sample is collected
only for the purpose of NMS screening for the newborn.
13.1 All research requests regarding access to NMS samples must be made in accordance with the requirements of the Health Information Act.
Reporting of Results
Actions 1.1; 1.2 14. NMS lab results must be
reported to the: • Primary care provider as documented on the requisition, • The birth facility, • The NMS Application, and the Electronic Health Record (EHR).
14.1 The NMS lab must issue an alert or have test results posted within four days of receipt of the sample (except for DNA testing for CF).
Actions 1.1; 2.6; 3.2 14.2
The molecular diagnostic lab must report CF DNA results on referred specimens to the NMS lab. The NMS lab must issue an alert or have test results posted for CF DNA results within 21 days of receipt of the sample.
Actions 2.6; 3.2 14.3
AHS must report NMS laboratory data electronically to the NMS Application in a format acceptable to AHW, and the delivery of the electronic messages must be monitored and any interruption to delivery identified, reported to AHW and resolved in a timely manner.
Actions 1.1; 1.2; 2.6 15. All children with abnormal screen results must receive timely and appropriate referral for follow up and treatment.
15.1 AHS must establish protocols for referral and follow up for each of the disorders screened for in consultation with specialty clinics and AHW.
Actions 1.1 15.2
The NMS lab must report abnormal test results to primary care providers and specialty clinics in accordance with the AHS protocols for referral and follow up.
Diagnosis and Treatment

NEWBORN METABOLIC SCREENING INITIATIVE: ACTION PLAN REPORT, NOVEMBER 30, 2010 (FINAL) Page 58 of 71
Actions To Meet 2010 NMS Policy Document Standards NMS Actions 2010 NMS Policy Document (Alberta Health & Wellness, dated March 2010)
Actions 1.2
16. It is the responsibility of primary care providers and specialty clinics to follow up with families and provide timely assessment, diagnosis and treatment.
16.1
Primary care providers receiving notification of abnormal test results must follow up with the family and/or specialty clinic as appropriate or immediately notify the NMS lab if unable to contact the family.
Actions 1.1 16.2
Specialty clinics must contact the family upon notification by the NMS lab that there is no primary care provider, or one cannot be contacted, or upon the request of the primary care provider.
Actions 1.1 16.3
Specialty clinics and physicians must provide diagnostic results (when available) to the NMS lab for quality assurance purposes.
Actions 1.1; 2.3; 2.6 17. The reporting and investigation of incidents must identify potential risks, actions required to prevent similar occurrences and opportunities for quality improvement.
17.1 Any individual who knows or suspects of an incident must report the incident to the Alberta Health and Wellness NMS program contact in a timely manner.
Actions 2.6 17.2
On request from AHW, the designated AHS senior executive responsible for NMS program delivery must investigate incidents promptly and report outcome, recommendations and steps taken to AHW.
N/A 17.3
AHW may perform its own investigation of incidents at its discretion.
Actions 1.1; 1.2; 1.3; 2.1.; 2.2; 2.3; 2.4; 2.5; 2.6; 2.7; 2.8; 3.1; 3.2; 3.3; 4.1
Meets AHS Roles and Responsibilities
Actions 1.1; 1.2; 2.1; 2.2; 2.5; 2.6; 2.7; 3.3
Meets NMS Audit Recommendations

NEWBORN METABOLIC SCREENING INITIATIVE: ACTION PLAN REPORT, NOVEMBER 30, 2010 (FINAL) Page 59 of 71
APPENDIX F: ACTION PLAN RESPONSIBILITY, ACCOUNTABILITY & CONSULTANTS SUMMARY Action Plan Responsibility, Accountability & Consultants Summary (DRAFT) LEGEND: Alberta Health and Wellness (AHW) AHS Children’s Hospitals Specialty Clinics (Specialty
Clinics) AHS Clinical Policy (Clinical Policy) AHS Clinical Practice Improvement (Clinical Practice
Improvement) AHS Contract Procurement Supply Management
(CPSM) AHS Data Integration Measurement and Reporting
(DIMR) AHS Emergency/Disaster Management (Emergency
/Disaster Management)
AHS Health Information Management (HIM) AHS Health Promotion, Disease and Injury Prevention
(HPDIP ) AHS HPDIP NMS Program Provincial Team (HPDIP
NMS Team) AHS Human Resources (HR) AHS Information & Privacy (Information & Privacy) AHS Information Technology (IT) AHS Laboratory Services (Lab Services) AHS Legal Services (Legal Services) AHS Molecular Diagnostic Lab (MDL) AHS Newborn Metabolic Screening Lab (NMS Lab)
AHS Patient Concerns (Patient Concerns) AHS Patient Safety (Patient Safety) AHS Population Health Innovation Decision Support
(PHIDS) AHS Quality & Service Improvement (Quality & Service
Improvement) AHS Senior Executive Committee (Senior Exec) AHS Specialty Diagnostic Labs (Specialty Diagnostic
Labs) AHS Translation Services AHS Zones – Public Health (Zones - Public Health)
Health Canada -First Nations Inuit Health (FNIH) Primary Care Networks (PCNs) Primary Care Providers (PCPs) Registered Midwives (Midwives) AHS Zones – Acute Care (Zones – Acute Care) AHS Zones– Community Labs (Zones – Community Labs)
Actions/ Deliverables (in bold) Responsible Accountability Consultants
1. Improve Newborn Metabolic Screening Processes 1.1. Develop and implement NMS clinical policies,
procedures, standards, and guidelines in alignment with Alberta Health Services (AHS) Strategic Governance Document Framework (2009)
HPDIP NMS Team
Legal Services Information & Privacy IT Clinical Policy Clinical Practice
Improvement Emergency/Disaster
Management HIM MDL NMS Lab
Patient Concerns PHIIDS Quality & Service Improvement Senior Executive Committee Specialty Clinics Zones – Acute Care Zones– Community Labs Zones – Public Health
AHW FNIH Midwives PCPs PCNs
1.1.1. Develop an overarching AHS NMS Program clinical policy related to the NMS program directive
HPDIP NMS Team Clinical Policy
Senior Executive Committee
1.1.2. Develop general NMS Program policies, procedures, standards, and guidelines
HPDIP NMS Team Legal Services Information and Privacy
Clinical Policy Senior Executive Committee Zones – Public Health
1.1.3. Develop NMS Program Newborn Registration policies, procedures, standards, and guidelines
HPDIP NMS Team Clinical Policy HIM
Zones– Acute Care
AHW FNIH Midwives

NEWBORN METABOLIC SCREENING INITIATIVE: ACTION PLAN REPORT, NOVEMBER 30, 2010 (FINAL) Page 60 of 71
Action Plan Responsibility, Accountability & Consultants Summary (DRAFT) LEGEND: Alberta Health and Wellness (AHW) AHS Children’s Hospitals Specialty Clinics (Specialty
Clinics) AHS Clinical Policy (Clinical Policy) AHS Clinical Practice Improvement (Clinical Practice
Improvement) AHS Contract Procurement Supply Management
(CPSM) AHS Data Integration Measurement and Reporting
(DIMR) AHS Emergency/Disaster Management (Emergency
/Disaster Management)
AHS Health Information Management (HIM) AHS Health Promotion, Disease and Injury Prevention
(HPDIP ) AHS HPDIP NMS Program Provincial Team (HPDIP
NMS Team) AHS Human Resources (HR) AHS Information & Privacy (Information & Privacy) AHS Information Technology (IT) AHS Laboratory Services (Lab Services) AHS Legal Services (Legal Services) AHS Molecular Diagnostic Lab (MDL) AHS Newborn Metabolic Screening Lab (NMS Lab)
AHS Patient Concerns (Patient Concerns) AHS Patient Safety (Patient Safety) AHS Population Health Innovation Decision Support
(PHIDS) AHS Quality & Service Improvement (Quality & Service
Improvement) AHS Senior Executive Committee (Senior Exec) AHS Specialty Diagnostic Labs (Specialty Diagnostic
Labs) AHS Translation Services AHS Zones – Public Health (Zones - Public Health)
Health Canada -First Nations Inuit Health (FNIH) Primary Care Networks (PCNs) Primary Care Providers (PCPs) Registered Midwives (Midwives) AHS Zones – Acute Care (Zones – Acute Care) AHS Zones– Community Labs (Zones – Community Labs)
Actions/ Deliverables (in bold) Responsible Accountability Consultants
1.1.4. Develop NMS Program Sample Collection and Transportation policies, procedures, standards, and guidelines
HPDIP NMS Team Legal Services Clinical Policy Clinical Practice Improvement MDL
NMS Lab Zones – Acute Care Zones – Community Lab Zones – Public Health
AHW FNIH Midwives PCP PCNs
1.1.5. Develop NMS Program Alert Management policies, procedures, standards, and guidelines
HPDIP NMS Team Legal Services Information and Privacy Clinical Policy
Clinical Practice Improvement NMS Lab Zones – Public Health
AHW FNIH
1.1.6. Develop NMS Program Analysis and Reporting policies, procedures, standards, and guidelines
NMS Lab
IT Legal Services Information and Privacy Clinical Policy Clinical Practice Improvement
Emergency/Disaster Management HPDIP NMS PHIDS MDL NMS Lab Specialty Clinics
AHW FNIH
1.1.7. Develop NMS Program Work-up/Follow-Up procedures, standards, and guidelines
HPDIP NMS Team Clinical Policy NMS Lab
Specialty Clinics
FNIH Midwives PCP PCN
1.1.8. Develop update and feedback mechanisms related to NMS Program policies, procedures, standards, and guidelines
HPDIP NMS Team Legal Services Information and Privacy IT Clinical Policy Clinical Practice Improvement Emergency/Disaster
Management HIM Senior Executive Committee
NMS Lab MDL Patient Concerns PHIDS Quality & Service Specialty Clinics Zones – Acute Care Zones– Community Labs Zones– Public Health
AHW FNIH Midwives PCP PCN

NEWBORN METABOLIC SCREENING INITIATIVE: ACTION PLAN REPORT, NOVEMBER 30, 2010 (FINAL) Page 61 of 71
Action Plan Responsibility, Accountability & Consultants Summary (DRAFT) LEGEND: Alberta Health and Wellness (AHW) AHS Children’s Hospitals Specialty Clinics (Specialty
Clinics) AHS Clinical Policy (Clinical Policy) AHS Clinical Practice Improvement (Clinical Practice
Improvement) AHS Contract Procurement Supply Management
(CPSM) AHS Data Integration Measurement and Reporting
(DIMR) AHS Emergency/Disaster Management (Emergency
/Disaster Management)
AHS Health Information Management (HIM) AHS Health Promotion, Disease and Injury Prevention
(HPDIP ) AHS HPDIP NMS Program Provincial Team (HPDIP
NMS Team) AHS Human Resources (HR) AHS Information & Privacy (Information & Privacy) AHS Information Technology (IT) AHS Laboratory Services (Lab Services) AHS Legal Services (Legal Services) AHS Molecular Diagnostic Lab (MDL) AHS Newborn Metabolic Screening Lab (NMS Lab)
AHS Patient Concerns (Patient Concerns) AHS Patient Safety (Patient Safety) AHS Population Health Innovation Decision Support
(PHIDS) AHS Quality & Service Improvement (Quality & Service
Improvement) AHS Senior Executive Committee (Senior Exec) AHS Specialty Diagnostic Labs (Specialty Diagnostic
Labs) AHS Translation Services AHS Zones – Public Health (Zones - Public Health)
Health Canada -First Nations Inuit Health (FNIH) Primary Care Networks (PCNs) Primary Care Providers (PCPs) Registered Midwives (Midwives) AHS Zones – Acute Care (Zones – Acute Care) AHS Zones– Community Labs (Zones – Community Labs)
Actions/ Deliverables (in bold) Responsible Accountability Consultants
1.1.9. Implement NMS Program procedures, standards, and guidelines across Zones using a phased approach
HPDIP NMS Team
Legal Services Information & Privacy IT HIM NMS Lab Clinical Policy Clinical Practice Improvement Emergency/Disaster
Management HIM
NMS Lab MDL Patient Concerns PHIDS Quality & Service Improvements Senior Executive Committee Specialty Clinics Zones – Acute Care Zones– Community Labs Zones– Public Health
AHW FNIH PCP PCN Midwives
1.2. Implement NMS Lab/MD Lab Capacity Improvements
NMS Lab MD Lab
Information & Privacy IT Clinical Practice
Improvement
HR HPDIP NMS
1.2.1. Implement a NMS Lab 6 day/week staffing model
NMS Lab AHS Information Technology Clinical Practice Improvement
1.2.2. Implement NMS Lab staff and MD Lab staffing coverage improvements
NMS Lab MDL
AHS Information Technology Clinical Practice Improvement
Human Resources
1.3. Develop and implement NMS Program Centralized Alert Management Process
HPDIP NMS Team Legal Services Information & Privacy IT Clinical Practice Improvement
NMS Lab Zones – Public Health
AHW FNIH
1.3.1. Develop draft NMS Program centralized alert management (CAM) system
HPDIP NMS Team Legal Services Information & Privacy Clinical Practice Improvement
NMS Lab Zones – Public Health
AHW
1.3.2. Conduct NMS Program centralized alert management (CAM) Information technology
HPDIP NMS Team IT
Zones – Public Health

NEWBORN METABOLIC SCREENING INITIATIVE: ACTION PLAN REPORT, NOVEMBER 30, 2010 (FINAL) Page 62 of 71
Action Plan Responsibility, Accountability & Consultants Summary (DRAFT) LEGEND: Alberta Health and Wellness (AHW) AHS Children’s Hospitals Specialty Clinics (Specialty
Clinics) AHS Clinical Policy (Clinical Policy) AHS Clinical Practice Improvement (Clinical Practice
Improvement) AHS Contract Procurement Supply Management
(CPSM) AHS Data Integration Measurement and Reporting
(DIMR) AHS Emergency/Disaster Management (Emergency
/Disaster Management)
AHS Health Information Management (HIM) AHS Health Promotion, Disease and Injury Prevention
(HPDIP ) AHS HPDIP NMS Program Provincial Team (HPDIP
NMS Team) AHS Human Resources (HR) AHS Information & Privacy (Information & Privacy) AHS Information Technology (IT) AHS Laboratory Services (Lab Services) AHS Legal Services (Legal Services) AHS Molecular Diagnostic Lab (MDL) AHS Newborn Metabolic Screening Lab (NMS Lab)
AHS Patient Concerns (Patient Concerns) AHS Patient Safety (Patient Safety) AHS Population Health Innovation Decision Support
(PHIDS) AHS Quality & Service Improvement (Quality & Service
Improvement) AHS Senior Executive Committee (Senior Exec) AHS Specialty Diagnostic Labs (Specialty Diagnostic
Labs) AHS Translation Services AHS Zones – Public Health (Zones - Public Health)
Health Canada -First Nations Inuit Health (FNIH) Primary Care Networks (PCNs) Primary Care Providers (PCPs) Registered Midwives (Midwives) AHS Zones – Acute Care (Zones – Acute Care) AHS Zones– Community Labs (Zones – Community Labs)
Actions/ Deliverables (in bold) Responsible Accountability Consultants
(IT) fit gap analysis 1.3.3. Conduct NMS Program centralized alert
management (CAM) transition tests between HPDIP NMS Program Provincial Team, NMS Lab, and Zones Public Health (see also 1.1.5)
HPDIP NMS Team Legal Services Information & Privacy Clinical Policy Clinical Practice Improvement
NMS Lab Zones – Public Health
AHW
1.3.4. Roll out a NMS Program centralized alert management (CAM) system phased launch between HPDIP NMS Program Provincial Team, NMS Lab, and Zones Public Health
HPDIP NMS Team Legal Services Information & Privacy IT Clinical Practice Improvement
NMS Lab Zones – Public Health
AHW
2. Improve NMS Program Supporting Processes 2.1. Define and maintain NMS Program Collaborative
Partnerships HPDIP Legal Services
Information and Privacy HPDIP NMS AHW
FNIH
2.1.1. Establish AHS NMS Program Point of Contact with Alberta Health & Wellness
HPDIP NMS Team HPDIP NMS Team AHW
2.1.2. Create Annual AHS NMS Program Report for AHW and other program partners
HPDIP NMS Team AHW FNIH
2.1.3. Create and execute AHS NMS Program Memorandum of Understanding (MOU) with Health Canada – First Nations Inuit Health (FNIH)
HPDIP NMS Team Information & Privacy Legal Services
AHW FNIH
2.2. Develop and implement NMS Program AHS Staff Engagement Strategy
HPDIP NMS Team Communications

NEWBORN METABOLIC SCREENING INITIATIVE: ACTION PLAN REPORT, NOVEMBER 30, 2010 (FINAL) Page 63 of 71
Action Plan Responsibility, Accountability & Consultants Summary (DRAFT) LEGEND: Alberta Health and Wellness (AHW) AHS Children’s Hospitals Specialty Clinics (Specialty
Clinics) AHS Clinical Policy (Clinical Policy) AHS Clinical Practice Improvement (Clinical Practice
Improvement) AHS Contract Procurement Supply Management
(CPSM) AHS Data Integration Measurement and Reporting
(DIMR) AHS Emergency/Disaster Management (Emergency
/Disaster Management)
AHS Health Information Management (HIM) AHS Health Promotion, Disease and Injury Prevention
(HPDIP ) AHS HPDIP NMS Program Provincial Team (HPDIP
NMS Team) AHS Human Resources (HR) AHS Information & Privacy (Information & Privacy) AHS Information Technology (IT) AHS Laboratory Services (Lab Services) AHS Legal Services (Legal Services) AHS Molecular Diagnostic Lab (MDL) AHS Newborn Metabolic Screening Lab (NMS Lab)
AHS Patient Concerns (Patient Concerns) AHS Patient Safety (Patient Safety) AHS Population Health Innovation Decision Support
(PHIDS) AHS Quality & Service Improvement (Quality & Service
Improvement) AHS Senior Executive Committee (Senior Exec) AHS Specialty Diagnostic Labs (Specialty Diagnostic
Labs) AHS Translation Services AHS Zones – Public Health (Zones - Public Health)
Health Canada -First Nations Inuit Health (FNIH) Primary Care Networks (PCNs) Primary Care Providers (PCPs) Registered Midwives (Midwives) AHS Zones – Acute Care (Zones – Acute Care) AHS Zones– Community Labs (Zones – Community Labs)
Actions/ Deliverables (in bold) Responsible Accountability Consultants
2.2.1. Create NMS Program AHS Staff Engagement Plan
HPDIP NMS Team Communications
2.2.2. Develop and test NMS Program AHS staff learning and development materials and resources
HPDIP NMS Team Communications
2.2.3. Implement NMS Program AHS staff learning and development opportunities
HPDIP NMS Team Communications Legal Services Information & Privacy
Clinical Policy Clinical Practice Improvement Emergency/Disaster
Management HIM
MDL NMS Lab PHIDS Quality & Service Improvements Specialty Clinics Zones – Acute Care Zones– Community Labs Zones– Public Health
2.2.4. Develop NMS Program AHS staff engagement ongoing feedback and review mechanisms
HPDIP NMS Communications
2.3. Monitor and report on NMS Program Patient Safety utilizing AHS Reporting and Learning System (RLS) for Patient Safety (2010)
HPDIP NMS Quality & Service Improvements AHW
2.3.1. Develop and test NMS Program Patient Safety Reporting processes, including: Reporting of adverse events, Close calls and/or hazards
HPDIP NMS Quality & Service Improvements
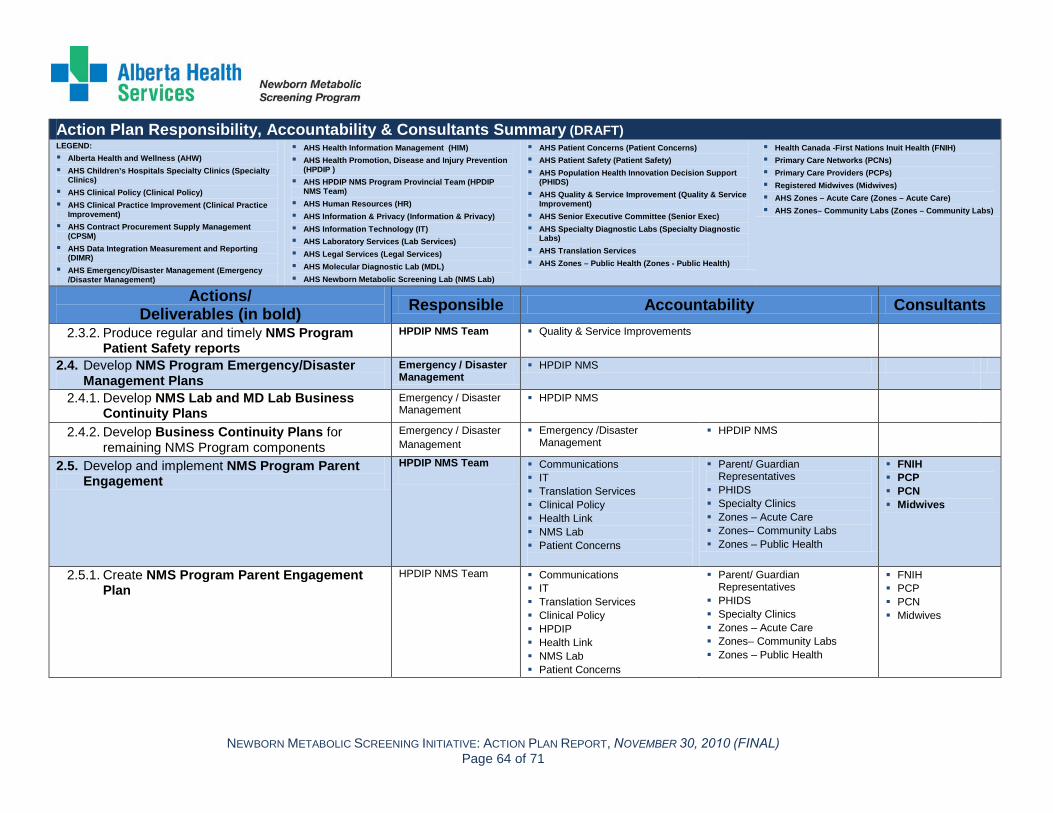
NEWBORN METABOLIC SCREENING INITIATIVE: ACTION PLAN REPORT, NOVEMBER 30, 2010 (FINAL) Page 64 of 71
Action Plan Responsibility, Accountability & Consultants Summary (DRAFT) LEGEND: Alberta Health and Wellness (AHW) AHS Children’s Hospitals Specialty Clinics (Specialty
Clinics) AHS Clinical Policy (Clinical Policy) AHS Clinical Practice Improvement (Clinical Practice
Improvement) AHS Contract Procurement Supply Management
(CPSM) AHS Data Integration Measurement and Reporting
(DIMR) AHS Emergency/Disaster Management (Emergency
/Disaster Management)
AHS Health Information Management (HIM) AHS Health Promotion, Disease and Injury Prevention
(HPDIP ) AHS HPDIP NMS Program Provincial Team (HPDIP
NMS Team) AHS Human Resources (HR) AHS Information & Privacy (Information & Privacy) AHS Information Technology (IT) AHS Laboratory Services (Lab Services) AHS Legal Services (Legal Services) AHS Molecular Diagnostic Lab (MDL) AHS Newborn Metabolic Screening Lab (NMS Lab)
AHS Patient Concerns (Patient Concerns) AHS Patient Safety (Patient Safety) AHS Population Health Innovation Decision Support
(PHIDS) AHS Quality & Service Improvement (Quality & Service
Improvement) AHS Senior Executive Committee (Senior Exec) AHS Specialty Diagnostic Labs (Specialty Diagnostic
Labs) AHS Translation Services AHS Zones – Public Health (Zones - Public Health)
Health Canada -First Nations Inuit Health (FNIH) Primary Care Networks (PCNs) Primary Care Providers (PCPs) Registered Midwives (Midwives) AHS Zones – Acute Care (Zones – Acute Care) AHS Zones– Community Labs (Zones – Community Labs)
Actions/ Deliverables (in bold) Responsible Accountability Consultants
2.3.2. Produce regular and timely NMS Program Patient Safety reports
HPDIP NMS Team
Quality & Service Improvements
2.4. Develop NMS Program Emergency/Disaster Management Plans
Emergency / Disaster Management
HPDIP NMS
2.4.1. Develop NMS Lab and MD Lab Business Continuity Plans
Emergency / Disaster Management
HPDIP NMS
2.4.2. Develop Business Continuity Plans for remaining NMS Program components
Emergency / Disaster Management
Emergency /Disaster Management
HPDIP NMS
2.5. Develop and implement NMS Program Parent Engagement
HPDIP NMS Team Communications IT Translation Services Clinical Policy Health Link NMS Lab Patient Concerns
Parent/ Guardian Representatives
PHIDS Specialty Clinics Zones – Acute Care Zones– Community Labs Zones – Public Health
FNIH PCP PCN Midwives
2.5.1. Create NMS Program Parent Engagement Plan
HPDIP NMS Team Communications IT Translation Services Clinical Policy HPDIP Health Link NMS Lab Patient Concerns
Parent/ Guardian Representatives
PHIDS Specialty Clinics Zones – Acute Care Zones– Community Labs Zones – Public Health
FNIH PCP PCN Midwives

NEWBORN METABOLIC SCREENING INITIATIVE: ACTION PLAN REPORT, NOVEMBER 30, 2010 (FINAL) Page 65 of 71
Action Plan Responsibility, Accountability & Consultants Summary (DRAFT) LEGEND: Alberta Health and Wellness (AHW) AHS Children’s Hospitals Specialty Clinics (Specialty
Clinics) AHS Clinical Policy (Clinical Policy) AHS Clinical Practice Improvement (Clinical Practice
Improvement) AHS Contract Procurement Supply Management
(CPSM) AHS Data Integration Measurement and Reporting
(DIMR) AHS Emergency/Disaster Management (Emergency
/Disaster Management)
AHS Health Information Management (HIM) AHS Health Promotion, Disease and Injury Prevention
(HPDIP ) AHS HPDIP NMS Program Provincial Team (HPDIP
NMS Team) AHS Human Resources (HR) AHS Information & Privacy (Information & Privacy) AHS Information Technology (IT) AHS Laboratory Services (Lab Services) AHS Legal Services (Legal Services) AHS Molecular Diagnostic Lab (MDL) AHS Newborn Metabolic Screening Lab (NMS Lab)
AHS Patient Concerns (Patient Concerns) AHS Patient Safety (Patient Safety) AHS Population Health Innovation Decision Support
(PHIDS) AHS Quality & Service Improvement (Quality & Service
Improvement) AHS Senior Executive Committee (Senior Exec) AHS Specialty Diagnostic Labs (Specialty Diagnostic
Labs) AHS Translation Services AHS Zones – Public Health (Zones - Public Health)
Health Canada -First Nations Inuit Health (FNIH) Primary Care Networks (PCNs) Primary Care Providers (PCPs) Registered Midwives (Midwives) AHS Zones – Acute Care (Zones – Acute Care) AHS Zones– Community Labs (Zones – Community Labs)
Actions/ Deliverables (in bold) Responsible Accountability Consultants
2.5.2. Revise, develop, and focus test NMS Program parent information resources
HPDIP NMS Team
Communications IT Translation Services Clinical Policy FNIH Health Link NMS Lab
Patient Concerns Parent/ Guardian
Representatives PHIDS Specialty Clinics Zones – Acute Care Zones– Community Labs Zones – Public Health
FNIH PCP PCN Midwives
2.5.3. Develop and implement NMS Program parent information resources distribution mechanisms
HPDIP NMS Team Communications IT Translation Service Health Link NMS Lab Patient Experience
Parent/ Guardian Representatives
Specialty Clinics Zones – Acute Care Zones– Community Labs Zones – Public Health
FNIH PCP PCN Midwives
2.5.4. Develop translated NMS Program parent information resources
HPDIP NMS Team Communications Translation Services
Health Link
2.5.5. Include NMS Program parent information resources in prenatal curriculum and resources
HPDIP NMS Team Communications Translation Services
Health Link Zones – Acute Care Zones – Public Health
FNIH \Midwives
2.5.6. Develop NMS Program parent information resources feedback mechanisms
HPDIP NMS Team Communications
Health Link Patient Concerns
2.6. Develop and implement NMS Program Communication
HPDIP NMS Team Communications Legal Services Information & Privacy IT Clinical Policy
MDL NMS Lab Patient Concerns PHIDS Quality & Service
AHW FNIH PCP PCN Midwives

NEWBORN METABOLIC SCREENING INITIATIVE: ACTION PLAN REPORT, NOVEMBER 30, 2010 (FINAL) Page 66 of 71
Action Plan Responsibility, Accountability & Consultants Summary (DRAFT) LEGEND: Alberta Health and Wellness (AHW) AHS Children’s Hospitals Specialty Clinics (Specialty
Clinics) AHS Clinical Policy (Clinical Policy) AHS Clinical Practice Improvement (Clinical Practice
Improvement) AHS Contract Procurement Supply Management
(CPSM) AHS Data Integration Measurement and Reporting
(DIMR) AHS Emergency/Disaster Management (Emergency
/Disaster Management)
AHS Health Information Management (HIM) AHS Health Promotion, Disease and Injury Prevention
(HPDIP ) AHS HPDIP NMS Program Provincial Team (HPDIP
NMS Team) AHS Human Resources (HR) AHS Information & Privacy (Information & Privacy) AHS Information Technology (IT) AHS Laboratory Services (Lab Services) AHS Legal Services (Legal Services) AHS Molecular Diagnostic Lab (MDL) AHS Newborn Metabolic Screening Lab (NMS Lab)
AHS Patient Concerns (Patient Concerns) AHS Patient Safety (Patient Safety) AHS Population Health Innovation Decision Support
(PHIDS) AHS Quality & Service Improvement (Quality & Service
Improvement) AHS Senior Executive Committee (Senior Exec) AHS Specialty Diagnostic Labs (Specialty Diagnostic
Labs) AHS Translation Services AHS Zones – Public Health (Zones - Public Health)
Health Canada -First Nations Inuit Health (FNIH) Primary Care Networks (PCNs) Primary Care Providers (PCPs) Registered Midwives (Midwives) AHS Zones – Acute Care (Zones – Acute Care) AHS Zones– Community Labs (Zones – Community Labs)
Actions/ Deliverables (in bold) Responsible Accountability Consultants
Clinical Practice Improvement Emergency/Disaster
Management HIM
Improvements Specialty Clinics Zones – Acute Care Zones– Community Labs Zones – Public Health
2.6.1. Create NMS Program Communication Plan
HPDIP NMS Team AHS Communications AHS Information Technology Health Information Management
(HIM) Health Promotion, Disease and
Injury Prevention (HPDIP ) MDL NMS Lab
Patient Experience PHIDS Quality & Service Improvements Specialty Clinics Zones – Acute Care Zones– Community Labs Zones – Public Health
AHW FNIH PCP PCN Midwives
2.6.2. Develop NMS Program communication materials to align with AHS Communication Visual Identity Standards
HPDIP NMS Team Communications
2.6.3. Integrate NMS Program communication pathways into AHS communication pathways
HPDIP NMS Team Communications IT
Health Link Patient Concerns Patient Safety
AHW FNIH PCP PCN Midwives
2.6.4. Develop NMS Program WebPages on AHS Insite and External AHS website
HPDIP NMS Team Communications IT
Health Link AHW
2.7. Develop and implement NMS Program Primary Care Provider Engagement with non-AHS staff
HPDIP NMS Team Communications IT NMS Lab Specialty Clinics
Zones – Acute Care Zones– Community Labs Zones – Public Health
FNIH PCP PCN Midwives
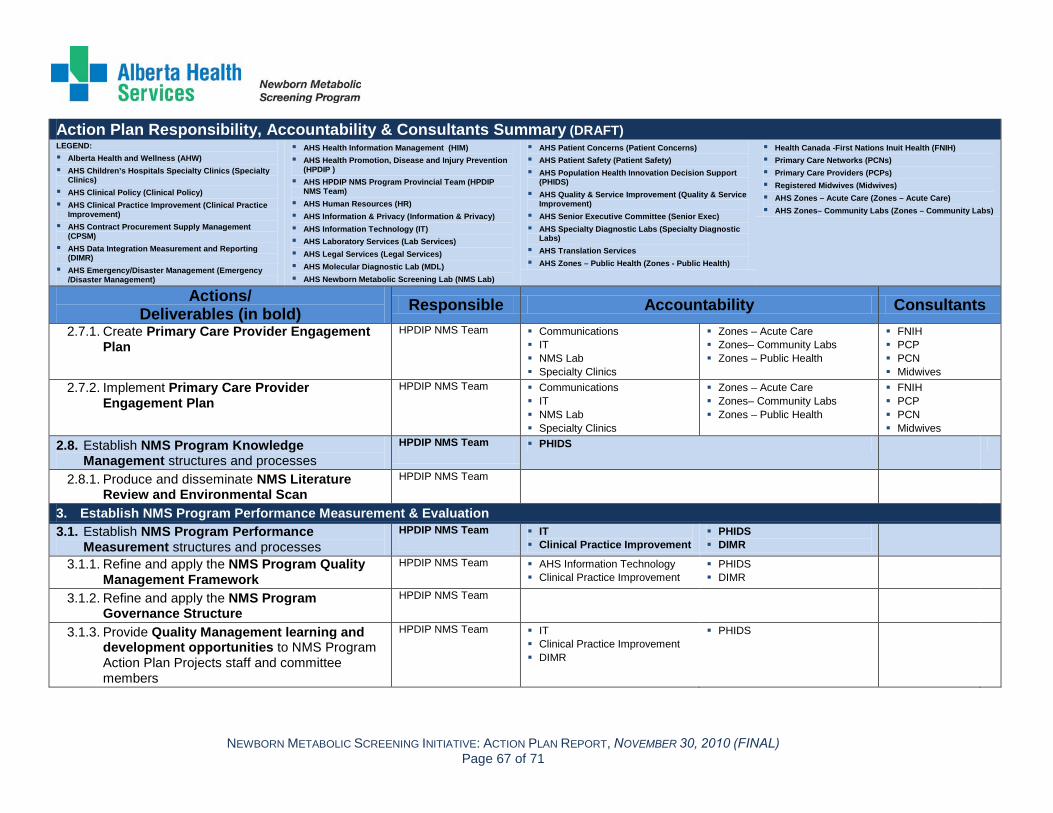
NEWBORN METABOLIC SCREENING INITIATIVE: ACTION PLAN REPORT, NOVEMBER 30, 2010 (FINAL) Page 67 of 71
Action Plan Responsibility, Accountability & Consultants Summary (DRAFT) LEGEND: Alberta Health and Wellness (AHW) AHS Children’s Hospitals Specialty Clinics (Specialty
Clinics) AHS Clinical Policy (Clinical Policy) AHS Clinical Practice Improvement (Clinical Practice
Improvement) AHS Contract Procurement Supply Management
(CPSM) AHS Data Integration Measurement and Reporting
(DIMR) AHS Emergency/Disaster Management (Emergency
/Disaster Management)
AHS Health Information Management (HIM) AHS Health Promotion, Disease and Injury Prevention
(HPDIP ) AHS HPDIP NMS Program Provincial Team (HPDIP
NMS Team) AHS Human Resources (HR) AHS Information & Privacy (Information & Privacy) AHS Information Technology (IT) AHS Laboratory Services (Lab Services) AHS Legal Services (Legal Services) AHS Molecular Diagnostic Lab (MDL) AHS Newborn Metabolic Screening Lab (NMS Lab)
AHS Patient Concerns (Patient Concerns) AHS Patient Safety (Patient Safety) AHS Population Health Innovation Decision Support
(PHIDS) AHS Quality & Service Improvement (Quality & Service
Improvement) AHS Senior Executive Committee (Senior Exec) AHS Specialty Diagnostic Labs (Specialty Diagnostic
Labs) AHS Translation Services AHS Zones – Public Health (Zones - Public Health)
Health Canada -First Nations Inuit Health (FNIH) Primary Care Networks (PCNs) Primary Care Providers (PCPs) Registered Midwives (Midwives) AHS Zones – Acute Care (Zones – Acute Care) AHS Zones– Community Labs (Zones – Community Labs)
Actions/ Deliverables (in bold) Responsible Accountability Consultants
2.7.1. Create Primary Care Provider Engagement Plan
HPDIP NMS Team Communications IT NMS Lab Specialty Clinics
Zones – Acute Care Zones– Community Labs Zones – Public Health
FNIH PCP PCN Midwives
2.7.2. Implement Primary Care Provider Engagement Plan
HPDIP NMS Team Communications IT NMS Lab Specialty Clinics
Zones – Acute Care Zones– Community Labs Zones – Public Health
FNIH PCP PCN Midwives
2.8. Establish NMS Program Knowledge Management structures and processes
HPDIP NMS Team PHIDS
2.8.1. Produce and disseminate NMS Literature Review and Environmental Scan
HPDIP NMS Team
3. Establish NMS Program Performance Measurement & Evaluation 3.1. Establish NMS Program Performance
Measurement structures and processes HPDIP NMS Team IT
Clinical Practice Improvement PHIDS DIMR
3.1.1. Refine and apply the NMS Program Quality Management Framework
HPDIP NMS Team AHS Information Technology Clinical Practice Improvement
PHIDS DIMR
3.1.2. Refine and apply the NMS Program Governance Structure
HPDIP NMS Team
3.1.3. Provide Quality Management learning and development opportunities to NMS Program Action Plan Projects staff and committee members
HPDIP NMS Team IT Clinical Practice Improvement DIMR
PHIDS

NEWBORN METABOLIC SCREENING INITIATIVE: ACTION PLAN REPORT, NOVEMBER 30, 2010 (FINAL) Page 68 of 71
Action Plan Responsibility, Accountability & Consultants Summary (DRAFT) LEGEND: Alberta Health and Wellness (AHW) AHS Children’s Hospitals Specialty Clinics (Specialty
Clinics) AHS Clinical Policy (Clinical Policy) AHS Clinical Practice Improvement (Clinical Practice
Improvement) AHS Contract Procurement Supply Management
(CPSM) AHS Data Integration Measurement and Reporting
(DIMR) AHS Emergency/Disaster Management (Emergency
/Disaster Management)
AHS Health Information Management (HIM) AHS Health Promotion, Disease and Injury Prevention
(HPDIP ) AHS HPDIP NMS Program Provincial Team (HPDIP
NMS Team) AHS Human Resources (HR) AHS Information & Privacy (Information & Privacy) AHS Information Technology (IT) AHS Laboratory Services (Lab Services) AHS Legal Services (Legal Services) AHS Molecular Diagnostic Lab (MDL) AHS Newborn Metabolic Screening Lab (NMS Lab)
AHS Patient Concerns (Patient Concerns) AHS Patient Safety (Patient Safety) AHS Population Health Innovation Decision Support
(PHIDS) AHS Quality & Service Improvement (Quality & Service
Improvement) AHS Senior Executive Committee (Senior Exec) AHS Specialty Diagnostic Labs (Specialty Diagnostic
Labs) AHS Translation Services AHS Zones – Public Health (Zones - Public Health)
Health Canada -First Nations Inuit Health (FNIH) Primary Care Networks (PCNs) Primary Care Providers (PCPs) Registered Midwives (Midwives) AHS Zones – Acute Care (Zones – Acute Care) AHS Zones– Community Labs (Zones – Community Labs)
Actions/ Deliverables (in bold) Responsible Accountability Consultants
3.1.4. Develop and produce regular and timely NMS Program performance measurement reporting to inform the Action Plan projects
HPDIP NMS Team IT DIMR
PHIDS
3.2. Analyze the NMS Program Performance Measurement and Information Technology (IT) capabilities
HPDIP NMS Team IT Clinical Practice Improvement
DIMR PHIDS
AHW
3.2.1. Complete current NMS Lab Information System (LIS) upgrade (i.e., Specimen Gate) in progress
NMS Lab IT NMS Lab
3.2.2. Request an update to the NMS Application based on current NMS Lab LIS upgrade
HPDIP NMS Team IT NMS Lab AHW
3.2.3. Complete NMS Program IT systems performance measurement gap analysis
HPDIP NMS Team IT Legal Services Clinical Practice Improvement
NMS Lab PHIDS DIMR
AHW
3.2.4. Review the NMS Program IT systems’ compliance with AHS Health Information Security Standards,
HPDIP NMS Team IT Legal Services
Privacy & Information
3.2.5. Assess NMS Program IT systems data integrity and conduct a gap analysis,
HPDIP NMS Team IT Clinical Practice Improvement
PHIDS DIMR
AHW
3.2.6. Determine the NMS Program IT system requirements to meet the NMS Program performance measurement requirements
HPDIP NMS Team IT Clinical Practice Improvement DIMR
NMS Lab PHIDS
AHW
3.2.7. Develop NMS Program IT Proposal for any required NMS Program IT system upgrades
HPDIP NMS Team IT

NEWBORN METABOLIC SCREENING INITIATIVE: ACTION PLAN REPORT, NOVEMBER 30, 2010 (FINAL) Page 69 of 71
Action Plan Responsibility, Accountability & Consultants Summary (DRAFT) LEGEND: Alberta Health and Wellness (AHW) AHS Children’s Hospitals Specialty Clinics (Specialty
Clinics) AHS Clinical Policy (Clinical Policy) AHS Clinical Practice Improvement (Clinical Practice
Improvement) AHS Contract Procurement Supply Management
(CPSM) AHS Data Integration Measurement and Reporting
(DIMR) AHS Emergency/Disaster Management (Emergency
/Disaster Management)
AHS Health Information Management (HIM) AHS Health Promotion, Disease and Injury Prevention
(HPDIP ) AHS HPDIP NMS Program Provincial Team (HPDIP
NMS Team) AHS Human Resources (HR) AHS Information & Privacy (Information & Privacy) AHS Information Technology (IT) AHS Laboratory Services (Lab Services) AHS Legal Services (Legal Services) AHS Molecular Diagnostic Lab (MDL) AHS Newborn Metabolic Screening Lab (NMS Lab)
AHS Patient Concerns (Patient Concerns) AHS Patient Safety (Patient Safety) AHS Population Health Innovation Decision Support
(PHIDS) AHS Quality & Service Improvement (Quality & Service
Improvement) AHS Senior Executive Committee (Senior Exec) AHS Specialty Diagnostic Labs (Specialty Diagnostic
Labs) AHS Translation Services AHS Zones – Public Health (Zones - Public Health)
Health Canada -First Nations Inuit Health (FNIH) Primary Care Networks (PCNs) Primary Care Providers (PCPs) Registered Midwives (Midwives) AHS Zones – Acute Care (Zones – Acute Care) AHS Zones– Community Labs (Zones – Community Labs)
Actions/ Deliverables (in bold) Responsible Accountability Consultants
3.3. Establish NMS Program Evaluation structures and processes
HPDIP NMS Team Clinical Practice Improvement DIMR
PHIDS AHW
3.3.1. Develop an NMS Program evaluation framework for program and project evaluation
HPDIP NMS Team Clinical Practice Improvement DIMR
PHIDS
3.3.2. Conduct an overall NMS Program Action Plan evaluation and evaluation of projects related to their impact on meeting the 2010 NMS Policy Document standards
HPDIP NMS Team Clinical Practice Improvement DIMR
PHIDS
AHW
3.3.3. Identify appropriate NMS Program comparable indicators to evaluate the long term success of the program
HPDIP NMS Team Clinical Practice Improvement DIMR
PHIDS AHW
4. Establish NMS Program Process Improvement 4.1. Establish NMS Program Process Improvement
structures and processes HPDIP NMS Team Clinical Practice Improvement
Quality & Service Improvements
PHIDS DIMR
4.1.1. Establish NMS Program process improvement (PI) approaches to support and manage improvement projects aligned with the AHS Improvement Way (AIW)
HPDIP NMS Team Clinical Practice Improvement DIMR
PHIDS
4.2. Conduct NMS Program Process Improvement (PI) Projects
HPDIP NMS Team Quality & Service Improvements DIMR
PHIDS
4.2.1. Complete NMS Lancet PI Project HPDIP NMS Team Clinical Practice Improvement Contract Procurement Supply
Management
NMS Lab PHIDS

NEWBORN METABOLIC SCREENING INITIATIVE: ACTION PLAN REPORT, NOVEMBER 30, 2010 (FINAL) Page 70 of 71
Action Plan Responsibility, Accountability & Consultants Summary (DRAFT) LEGEND: Alberta Health and Wellness (AHW) AHS Children’s Hospitals Specialty Clinics (Specialty
Clinics) AHS Clinical Policy (Clinical Policy) AHS Clinical Practice Improvement (Clinical Practice
Improvement) AHS Contract Procurement Supply Management
(CPSM) AHS Data Integration Measurement and Reporting
(DIMR) AHS Emergency/Disaster Management (Emergency
/Disaster Management)
AHS Health Information Management (HIM) AHS Health Promotion, Disease and Injury Prevention
(HPDIP ) AHS HPDIP NMS Program Provincial Team (HPDIP
NMS Team) AHS Human Resources (HR) AHS Information & Privacy (Information & Privacy) AHS Information Technology (IT) AHS Laboratory Services (Lab Services) AHS Legal Services (Legal Services) AHS Molecular Diagnostic Lab (MDL) AHS Newborn Metabolic Screening Lab (NMS Lab)
AHS Patient Concerns (Patient Concerns) AHS Patient Safety (Patient Safety) AHS Population Health Innovation Decision Support
(PHIDS) AHS Quality & Service Improvement (Quality & Service
Improvement) AHS Senior Executive Committee (Senior Exec) AHS Specialty Diagnostic Labs (Specialty Diagnostic
Labs) AHS Translation Services AHS Zones – Public Health (Zones - Public Health)
Health Canada -First Nations Inuit Health (FNIH) Primary Care Networks (PCNs) Primary Care Providers (PCPs) Registered Midwives (Midwives) AHS Zones – Acute Care (Zones – Acute Care) AHS Zones– Community Labs (Zones – Community Labs)
Actions/ Deliverables (in bold) Responsible Accountability Consultants
4.2.2. Conduct NMS Lab Date/Time Recording PI Project
NMS Lab Clinical Practice Improvement NMS Lab PHIDS
4.2.3. Conduct NMS Sample Packaging and Transportation PI Project
HPDIP NMS Team Clinical Practice Improvement HPDIP NMS Lab
PHIDS Zones – Community Labs Zones - Public Health
4.2.4. Conduct NMS Community/Out- Patient Lab Collections Feasibility PI Project
HPDIP NMS Team Clinical Practice Improvement NMS Lab
PHIDS Zones – Community Labs Zones - Public Health
4.2.5. Conduct NMS Collections “Discharge Lounge” Concept Feasibility PI Project
HPDIP NMS Team Clinical Practice Improvement
PHIDS Zones – Acute Care
4.2.6. Conduct RN/LPN After Hours NMS Collections PI Project
HPDIP NMS Team Clinical Practice Improvement
PHIDS Zones – Acute Care
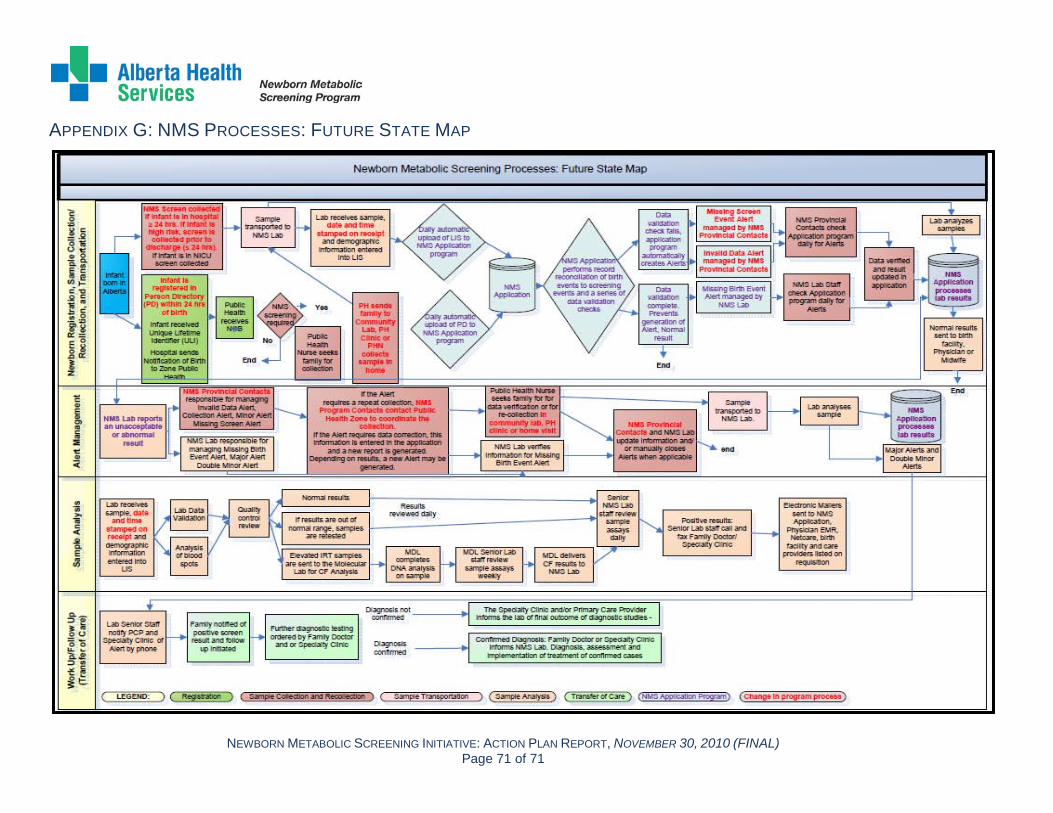
NEWBORN METABOLIC SCREENING INITIATIVE: ACTION PLAN REPORT, NOVEMBER 30, 2010 (FINAL)Page 71 of 71
APPENDIX G: NMS PROCESSES: FUTURE STATE MAP





























