-
8/10/2019 Maximizing Auditory Slides
1/18
Maximizing Auditoryand Speech Potential for
Deaf and Hard-of-Hearing
Children
-
8/10/2019 Maximizing Auditory Slides
2/18
Course Objectives
Today well cover a lot of territory about hearing loss in
children.You may be surprised to know that congenital hearing
lossaffects between 1 to 3 per 1,000 live births, making it the
mostcommon anomaly in newborns.
Well discuss the profound impact of hearing loss on the childs
life,
as well as review the wide range of interventions now
available.
Perhaps most important, well talk about the communicationoptions
available to deaf and hard-of-hearing children, and how tomaximize
a deaf or hard-of-hearing childs ability to listen and speak.
Many parents and professionals have assumed that the only
optionis sign language, and do not know that almost all deaf and
hard-of-hearing children can learn to listen and to speak through
oral deafeducation, which gives them many advantages in a hearing
world.It is important to note that 90 percent of deaf children are
born tohearing parents.
Maximizing Auditory and Speech Potentialfor Deaf and
Hard-of-Hearing Children
Good morning, and thank you for asking me here today to
talkabout maximizing auditory and speech potential for deaf
andhard-of-hearing children.
Slide 1
Slide 3
Early InterventionEarly identification and intervention are the
most importantfactors for maximizing auditory and speech potential
for deafand hard-of-hearing children.
As you will learn today, the first six months are crucial.
Childrenwhose hearing loss is identified by six months of age
developsignificantly better language skills than children
identified later.
They achieve more academically and they have an easier
timefunctioning in society. Many can manage their day-to-day
interactions independently, without the help of an
interpreter.
Slide 2
-
8/10/2019 Maximizing Auditory Slides
3/18
Facts: Risk Factors for Hearing Loss -Birth to 29 days
What causes hearing loss?
In about 50 percent of all cases, the cause of a childs hearing
loss isnot known or identifiable. Risk factors include:
Known genetic factors in 25 percent of cases. However,
mostgenetic deafness is recessive and 90 percent of deaf and
hard-of-hearing children are born to parents who have normal
hearing.
In utero infections such as cytomegalovirus can cause hearing
loss.
Other anomalies are associated with deafness, including
craniofaciaanomalies.
Birth weight under 3.3 lbs
Hyperbilirubinemia requiring exchange transfusion
Ototoxic medications
Apgar scores of 0-4 at 1 minute or 0-6 at 5 minutes
When any of these risk factors are present, the childs
hearingshould be screened immediately, and in the presence of
somefactors, tested at 6-month intervals until the child is 3 years
of age.
Of course, it is always recommended to test all newborns because
othe benefits of early intervention.
Facts: Hearing Loss Incidence
As I mentioned, hearing loss is the most common birth
anomaly.Occurring in 1 to 3 per 1,000 live births, its 20 times
more
common than phenylketonuria, for which newborns are
routinelyscreened. It is twice as common as
phenylketonuria,hypothyroidism, sickle cell disease, and
galactosemia combined.
Hearing loss also occurs after birth due to causes
includingautoimmune inner-ear disease, meningitis, maternal viral
infectionduring pregnancy, or ototoxic drugs given after birth.
Despite the frequency of hearing loss in children, many
pediatricprofessionals are unaware of the advances in hearing
testing,technology, and the many communication options available
todeaf and hard-of-hearing children.
A survey conducted last year found that while half of
pediatricianshad heard of oral deaf education, only 30 percent were
aware ofprograms in their community. More than 90 percent believed
thatsign was the primary method used by deaf and
hard-of-hearingchildren to communicate.
Slide 4
Slide 5
-
8/10/2019 Maximizing Auditory Slides
4/18
The Case for Early Diagnosis and
InterventionSome of those consequences include damage to the
parent-childbond and behavioral problems, as well as delays and
problems withlanguage acquisition.
Lets look at these in more detail.
Facts: Diagnosis and Intervention Lag
Although hearing loss is the most common birth anomaly,universal
screening has only recently begun in some states. As aresult,
babies are often 1, 2, 3, or even 4 years old before they
arediagnosedon average 13-22 months of age, depending on
theseverity of the loss.
Parental concern is a very important clinical indicator that
there isa problem, and should be taken as seriously as any other
risk factor.
Often there is a lag of several months after parents bring
theirconcern to a physician before the physician tests the childs
hearing.
Physiological tests of hearing can identify and diagnose
infanthearing loss very early. No child is too young to have a
hearing test.
The lag in diagnosis and treatment can have serious
consequencesfor the child.
Slide 7
Slide 8
Facts: Risk Factors for Hearing Loss -29 days to 2 years
Parent/caregiver concern regarding hearing, speech,
language,and/or developmental delay
Bacterial meningitis and other infections associated
withsensorineural loss
Head trauma associated with loss of consciousness or skull
fracture
Stigmata or other findings associated with a syndrome known
toinclude hearing loss
Ototoxic medications
Recurrent or persistent otitis media with effusion for at least
6months
Family history of hearing loss
Slide 6
-
8/10/2019 Maximizing Auditory Slides
5/18
The Case for Early Diagnosis andIntervention
Early childhood is a critical time for language development,
butuntil recently we didnt realize HOW early and HOW critical. As
itturns out, the first 6 months are perhaps the most important.
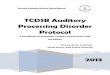
To determine whether early intervention with children with
hearing
loss made a difference in language development,
Yoshinaga-Itanoand colleagues from the University of Colorado
compared thereceptive and expressive language abilities in children
with hearingimpairment with those of children with no hearing
loss.
The study found that scores were significantly higher when
thechildren were diagnosed and intervention started before 6
monthsof age.
This is reflected in the Yoshinaga-Itano results charted
here.
The Case for Early Diagnosis and
InterventionA child with hearing loss does not respond in the
same way ashearing children do. For instance, he or she may not
turn towardpeople who are talking to him or her. When the hearing
loss hasnot been diagnosed, parents and other people often
interpret thisas an emotional problem instead of a physical
problem.
Parents may assume problems with the relationship, withtheir
parenting, or with the childs emotional style instead ofsuspecting
hearing loss.
A hard-of-hearing or deaf child may use hitting or aggression to
geta point across or gain attention, or out of frustration at
beingunable to communicate. Some children may withdraw as a
resultof a lack of communication skills.
If not diagnosed until the child is 2 or 3 years old, the
emotionaland social damage can be longstanding.
Ironically, the child most likely to be diagnosed and treated is
theprofoundly deaf child. Yet the child with mild to moderate
hearingloss may suffer the same issues and bonding problems.
Slide 9
Slide 10
-
8/10/2019 Maximizing Auditory Slides
6/18
Screening Protocols
Because hearing loss is the most common birth anomaly,
andbecause early intervention is so critical for language
developmentand socialization, every hospital should institute a
universal protocolto screen for hearing loss.
Universal screening can be conducted for less than $30 per
baby,including hardware cost, disposables, and the screeners time
to
conduct the test.
The Case for Early Diagnosis and
InterventionWhat was particularly striking in the
Yoshinaga-Itano study is thatin children with normal cognitive
abilities, the statistical difference
was independent of age, gender, ethnicity, communication
mode,degree of hearing loss, socioeconomic group, or the presence
orabsence of other disabilities. The only meaningful difference
wasthe age of diagnosis and intervention.
Those first 6 months give the child the chance to develop
languagenormally, instead of playing catch up.
Screening Protocols
Routine newborn screening is not the whole story,
however.Genetic hearing loss may not be present at birth, but may
developin the months after.
And as we discussed earlier, other causes, such as hearing loss
dueto ototoxic medications, can occur later. So there are other
times
when children should be tested.
Parental concern should be considered a valid factor that there
isa hearing loss, and a child should be tested immediately if
theparent suspects a hearing problem.
If there are risk factors such as family history or low Apgar
scores,the child should be tested even if there are no obvious
othersymptoms.
If there is a question about the results of initial testing,
additional
tests should be scheduled at 3- or 6-month intervals.
Slide 11
Slide 12
Slide 13
-
8/10/2019 Maximizing Auditory Slides
7/18
Auditory and Language Milestones
At 6 to 12 months, the child should be babbling,
repeatingsyllables like ma-ma-ma, and using pointing and facial
gesturesto communicate.
A 12-month old may only be speaking a few words, but shouldbe
playing with sounds to make adult-like speech patterns,
andtypically understands 50 words or so. The child should knowhis
or her own name, understand no, and understandsimple
directions.
Between 18 months and 36 months, most children experiencevery
rapid development of speech. By 3 years, a child will knowthousands
of words, make short sentences, and sing songs.
Children who miss these milestones should be tested again
for
hearing loss.
Auditory and Language Milestones
An infant who has tested normally, but who misses
majordevelopmental milestones should be tested again.
Newborns should startle to loud and sudden sounds.
By 2 to 3 months, the child should laugh, form sounds in the
backof the mouth, recognize familiar voices, and distinguish
changes intone of voice, for instance, a question or a happy
statement.
A child of 4 to 6 months ought to turn his or her head toward
asound to find the source. The child also should start
makingsyllable-type noises, putting vowels and consonants
together,and simply make noises of all types.
Slide 14
Slide 15
-
8/10/2019 Maximizing Auditory Slides
8/18
Audiology
The audiologist uses a range of tests, often over a period of
monthsor years, to pinpoint the exact type and severity of hearing
loss.Some of these are passive tests that can be administered
withoutactive participation on the childs part. Some tests must be
post-
poned until the child is old enough to respond actively.Severity
of hearing loss is classified as mild from 25-40 dB,moderate 41-70
dB, severe 71-90 dB, and profound is anythingmore than 90 dB. The
audiologist can also identify whichfrequencies are affected.
Profound loss does not mean total absence of hearing, which is
infact very rare.
Screening Protocols
Taking immediate action when you suspect a hearing loss is
important because every day missed is a day that
languageacquisition is affected.
As soon as a screening indicates a problem or you suspect a
problem,the childs hearing should be thoroughly checked by an
audiologist
with pediatric training. The audiologists pediatric experience
isessential, because testing children and infants is very different
fromtesting adults who are losing their hearing, and requires
specialtraining.
When hearing loss is identified, a medical work-up,
usuallyperformed by an otolaryngologist, should occur to
determinecause and possible treatment options.
Hearing aids can and should be prescribed and fitted as soon as
thehearing loss is diagnosed, even on tiny newborns. There is no
benefitto waiting. Hearing aids alone are not a quick fix. Parents
andprofessionals need to work closely with children to help
themmake sense of sound.
Parents also need time to mourn, adjust, learn, and
immersethemselves in the skills and knowledge theyll need. Some
periodof adjustment is to be expected. However, parents who
hesitate for
more than a month or two may need help to get moving,
becausetheir denial can have long-term consequences for the
child.
Slide 16
Slide 17
-
8/10/2019 Maximizing Auditory Slides
9/18
Audiology
The active tests of a childs hearing require special training
and skillon the part of the audiologist to interpret and understand
thechilds reactions.
In Behavioral Observational Audiometry (BOA), the
audiologistwatches the babys face and changes in behavior in
response to aseries of sounds.
In Visual Reinforcement Audiometry (VRA), the audiologistdirects
the child to a toy that lights up or moves when the childlooks at
it in response to a sound.
In Play Audiometry, the audiologist teaches the child to
respondwith a particular action when he or she hears a sound.
All of these tests are done with speech sounds and pure tones
atdifferent pitch and loudness levels to obtain the most
completemap possible of the range and severity of the childs
hearing loss.
Audiology
Passive tests are ideal for small children because they dont
requirecooperation. These tests can be conducted on children as
early asone or two days after birth.
Auditory Brainstem Response (ABR) uses electrodes to test
aninfants brain response to a series of sounds including
differentfrequencies and clicks. Babies older than 4 months may
needsedation, not because the test is painful, but to keep them
still.
ABR tests the entire auditory pathway.
The Otoacoustic Emission (OAE) test uses a probe to
measureechoes from the inner ear in response to sound. A normal
cochleacreates its own sound in response to sound entering the ear.
OAEtests this function of the cochlea.
Tympanometry measures the movement of the eardrum and theability
of the middle ear to conduct sound to the inner ear.
Acoustic reflex tests for a normal reflexive response to loud
noises.
Slide 18
Slide 19
-
8/10/2019 Maximizing Auditory Slides
10/18
Hearing Technology Today
Hearing technology has improved dramatically in the past 10
yearsand continues to become more powerful and sophisticated.
Even profoundly deaf children can benefit from hearing aids
today,whereas 20 or 30 years ago, the available aids often did not
provideenough amplification. In addition, todays aids can be tuned
to thechilds specific hearing profile.
The range of options for different children and different
situationsincludes hearing aids, FM systems and cochlear implants,
each of
which well review in greater detail.
The critical point to remember is that even though it is
powerfuland effective, the technology is not a solution by itself.
Hearing andspeech must be taughtthe technology does not make
hard-of-hearing and deaf children into normal-hearing children.
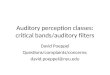
Audiology
This familiar sounds audiogram is designed to explain a
childshearing loss to families in terms that they can better
understand.It is used to show the frequencies affected and the
severity of theloss, as well as what the aided potential is with
hearing aids.
Slide 20
Slide 21
Slide 22
Hearing Techology TodayHearing aids work like tiny amplification
systems. They receivesound and amplify it at each frequency to make
the most of thechilds residual hearing.
-
8/10/2019 Maximizing Auditory Slides
11/18
Hearing Technology Today
There are three basic types of hearing aids and many
variationsamong them. There are benefits and drawbacks to each,
anddifferent aids may be appropriate for different children.
Analog aids can be made more powerful than digital aids, and
areoften the best choice for profoundly deaf children. However,
theymake some static noise even when its quiet, which can
bedistracting for children with mild hearing loss.
Programmable aids are easier to tailor to a childs hearing
profilethan conventional aids are.
Digital aids offer the most precise control, and are silent when
itsquiet, but they are not as powerful as analog aids, so they may
notbe ideal for children with the most profound loss.
The services of an experienced pediatric audiologist are
required torecommend the appropriate amplification device.
Hearing Technology Today
Fitting children with hearing aids is not a one-time event.It
takes time and patience.
Since the patients are generally pre-verbal, observation and
deductionwill be required. The audiologists observations at the
childsappointments are important, but time-limited. Therefore,
theparents ability to notice and discuss the childs response
isimportant in fitting aids. Encourage parents to take notes
andbring them to appointments.
Parents may need to work with several different types of aids
overtime to find the one that works best for their child. A daily,
weekly,
and monthly maintenance routine is important to ensure thatyoung
children are getting the benefit of the aid. Batteries go
bad,peanut butter gets in the amplifier, cords break, etc. At any
giventime, only half of small childrens aids are working.
Children may find aids distracting or try to take them out at
first.Parents may feel embarrassed or experience emotions and need
toprocess these normal feelings.
Slide 23
Slide 24
-
8/10/2019 Maximizing Auditory Slides
12/18
Cochlear Implants
Cochlear implants offer dramatic benefits to many children
whosehearing aids dont supply sufficient amplification to learn to
developspoken language efficiently. Different from hearing aids
that amplifysound to the middle and inner ear, cochlear implants
send electrical
signals directly to the inner ear and stimulate the auditory
nerve.This is accomplished by surgically implanting an electrode
arrayin the cochlea. The external component of the cochlear
implantconsists of a headpiece with a microphone and a speech
processor(usually body worn).
The speech processor converts acoustic information entering
themicrophone into electronic codes, which are then
transmittedthrough the skin to the implanted cochlear stimulator
and onto theelectrode array. The electrodes stimulate the nerve
endings withinthe cochlea, which send a stimulus to the brain and
is interpreted
as sound.
Hearing Technology Today
FM systems consist of a wireless microphone that is worn by
onepersonusually a parent or teacherthat transmits sound to
thechild, who wears a receiver. FM systems overcome problems
ofdifficult listening situations, such as a noisy environment ora
distance.
FM systems can work as a hearing aid, and also focus and
clarifythe sound of the speaker using the microphone
consistently.
FM systems can be very useful when a baby is little and
needsaccess to consistent sound to learn to use the sense of
hearing.
They are traditionally used in schools to overcome the
noisyclassroom environment.
Slide 25
Slide 26
-
8/10/2019 Maximizing Auditory Slides
13/18
Communication Options
Although American Sign Language has developed a high profileover
the past decade, there are other communication options forthe deaf
or hard-of-hearing child that parents and professionalsmust be made
aware of.
Today, deaf and hard-of-hearing children have options,
includinglearning to listen and speak.
Parents have the ultimate responsibility and the right to choose
thecommunication option that they feel is right for their child
andtheir family.
Cochlear Implants
Children may be candidates for cochlear implants if they have
abilateral severe to profound hearing loss, and have received
marginalbenefit from their amplification after at least six months
of use.
As we learn more from the success of the earliest implants,
cochlearimplants are becoming more common in younger children.
Cochlear implants are FDA-approved for children 12 months
andolder, although there are now many cases of children
receivingcochlear implants as early as 9 months of age.Slide 27
Slide 28
-
8/10/2019 Maximizing Auditory Slides
14/18
Communication Options
Cued speech is intended to help the deaf person by providing
visualcues from the speaker for the sounds they are producing as
theyspeak. These cues help to clarify what is being spoken. The
cuesare not sign language, and have no meaning without the
verbalcontext, but clarify the specific sound being made.
Communication Options
Auditory oral and auditory verbal are two slightly
differentmethodologies with the same basic goal: to enable deaf
orhard-of-hearing children to learn to listen and speak andfunction
independently in a hearing world. Both make use ofavailable
technologies to aid the childs ability to listen, always
inconjunction with a comprehensive education program that
isdevelopmentally appropriate for the child. Ill discuss them
todayusing the term, oral deaf.
Oral deaf education also focuses on the cognitive domain of
eachchild in order to promote thinking skills. All of these domains
will
greatly enhance the childs educational future. Studies have
shownthat spoken language acquisition has a positive effect on
literacy.
Oral deaf educators teach children listening, speaking, and
thinkingskills in addition to academic topics. They also teach
parents, family,and friends how to interact with the deaf or
hard-of-hearing childto support language development through
strategies that enhancelistening and speaking.
Slide 29
Communication Options
Total communication combines auditory training with SigningExact
English, or SEE. SEE is a manual code for English that hasthe same
vocabulary and syntax.
Total communication has a disadvantage in that most hearing
peopledo not understand the signs, so it may limit the childs
ability tocommunicate with the hearing world.
Slide 30
Slide 31
-
8/10/2019 Maximizing Auditory Slides
15/18
Communication Options
ASL is sound-free. It is its own language, with unique syntax
andgrammar, communicated by gesture and facial expression, and it
isnot English.
Some people advocate teaching ASL over spoken language becauseit
is more natural or easy for the deaf or hard-of-hearing infant
tolearn. There is a large pool of ASL speakers, including resources
atschools and universities.
ASL is not spoken or understood by most hearing people,
whichposes a challenge to the ASL speaker who wants to simply buy
ahamburger or ask directions.
In addition, because literacy is based on auditory, rather than
visualpathways, it is more challenging for speakers of ASL to learn
toread, and literacy among ASL speakers has historically been
low.
Slide 32
Slide 33
Oral Deaf Education: Team Approach
The success of oral deaf education depends on the skills and
cooperation of an extended team of professionals, family,and
friends.
The child and family are at the core, doing the daily work
ofimproving listening and verbal skills, and choosing andmanaging
the rest of the team.
The pediatrician and ENT specialist have roles in monitoring
thechilds auditory health in addition to other health issues of
childhood.
Audiologists and speech pathologists provide specialized
technicalexpertise in diagnosing and treating the hearing loss, and
working
with the child and his or her parents to develop listening
skills.
Oral deaf educators use specialized teaching techniques to
teachlanguage skills along with academic subject matter.
-
8/10/2019 Maximizing Auditory Slides
16/18
Oral Deaf Education
Social interaction is the motivation every child has to learn
and grow.
All family and friends should be invited and taught the skills
theyneed to communicate with the deaf or hard-of-hearing child.
Siblings can be excellent motivators and teachers.
Grandparentsmay have time and patience to share.
Involving the entire family not only is good for the child, but
alsogives the parents a much-needed break.Slide 34
Slide 35
Oral Deaf Education
Though many pediatricians have deaf or hard-of-hearing
patients,few know the options for children with hearing loss. A
recent studyfound that 90 percent of pediatricians believe that the
primarymodality is ASL. Only about 1 in 3 knows of oral deaf
resources intheir community.
Its important to have those resources ready, because parents
will
turn to you for referrals.
The ENT specialist is essential in the diagnostic
process,determining cause and possible treatment options and
working
with the pediatric audiologist to provide the
appropriateamplification device to maximize the childs listening
potential.
-
8/10/2019 Maximizing Auditory Slides
17/18
Oral Deaf Education
The pediatric audiologist is the testing and hearing
technologyexpert. As we discussed, audiologists can pinpoint the
degree ofhearing loss and the frequencies that are affected.
Audiologists
work with families to find the right hearing aids and to
fine-tunethem to the childs needs.
The speech and language pathologist teaches the child the skills
heor she will need to listen, attach meaning to sound, and
developspeech skills. These professionals also work with parents
and familyto teach effective communication skills for use with the
child.
Slide 36
Slide 37
Oral Deaf Educators
Oral deaf educators teach the whole child at each
developmentallevel, while supporting speech, listening, and
language acquisitionand preparing the child for regular education.
When appropriate,oral deaf educators teach all academic subjects
and prepare childrento move into mainstream schooling.
Oral deaf educators are often one of the best networking
resourcesfor parents.
Slide 38
Conclusion: Remember These Key Points
As pediatricians, what do you need to remember?
Hearing loss is the most common birth anomaly by far, andhas
enormous consequences for the child. Advocate foruniversal testing
at your facilities.
Children can be tested in the first days after birth, and
hearingaids fitted immediately. Research shows that there is
anenormous benefit to intervention before 6 months of age.
Technology does not fix hearing. Technology gives the child
thebest opportunity to listen and develop spoken communication,
which must be supported with the right education over time.
Even children with profound hearing loss can learn to listenand
speak and communicate with hearing family members,friends, and
peers.
-
8/10/2019 Maximizing Auditory Slides
18/18
Conclusion (For physician audience)
You may be the parents first or only source of information
aboutoral deaf education. Make a point to keep a file on resources
suchas pediatric audiologists, oral deaf educators, and speech
therapistsso that you can help your patients achieve all they
can.
Slide 39
Conclusion (Alternate slide fornon-physician audience)
You may be the parents first or only source of information
aboutoral deaf education. Make a point to keep a file on resources
suchas pediatric audiologists, oral deaf educators, and speech
therapistsso that you can help your patients achieve all they
can.
Slide 40