Embed Size (px)
Citation preview

Mass Casualty Management
for the Doctor, Nurse & Paramedic
-Formerly ATLS Mass Casualty Management
By Dr S. T. Boyd,BSc(Hons), MBChB, DA(SA), FCEM(SA),
Dip.PEC(SA)

Mass Casualty Management
• Goal: To apply trauma triage principles in multiple patient scenarios
• Objectives:– Brief local / international history with mass
casualties– Define triage– Understand and identify factors– Apply principles of triage with scenarios– Conclude with an example which is still today
RSA’s biggest train accident
• You've carefully thought out all the angles.
• You've done it a thousand times before.
• It comes naturally to you.
• You know what you're doing, its what you've been trained to do your whole life.
• Nothing could possibly go wrong, right ?

Natal & Durban Floods September 1987
Largest floods in living memory, Cyclone Demonia
1986 excluded

Durban Umlaas Canal - EMPTY

Similar to September 1987
Problems created in Sept 1987?Loss of road, rail & almost all air communications (Durban International under water & Virginia nearly so)
Loss of telephone & radio comms
Washaways in informal settlement areas (>400 people washed away when rivers came down in flood)
Mudslides with entrapments

Pietermaritzburg Floods
25/12/1995

Durban Floods Nov 1999

Minibus Accidents

Total number = 4 dead & 40 injured

DC3 - Crash landed in the surf line
M.V. Oceanos off the Transkei Coast

A plan was needed to go from this……..

Bus bombers - the sequel

To this…..

Mass casualties - why train accidents in India have so many injured

Mass Casualty Management
Interactive scenario session

Disaster Management- Triage
• French = “to sort or select” (“Sorting of differing grades of wool & later coffee beans”)
• Napoleon’s surgeon Baron Larrey, applied the principle to the assessment & treatment of the injured
• To sort into categories based on an assessment of:– A B C D E’s– Resources available
RSA System: Red (P1), Yellow (P2), Green (P3) & Blue (P4)

TRIAGE
CATEGORIES:
• RED (P1) = 1-5%
• YELLOW (P2) = 5-10%
• GREEN (P3) = 80%
• BLUE (P4) = 1-5%

Triage• "RED CODE" (“P1”) = The horizontal &
groaning / gurgling patient (ABCD) seriously affected / malfunctional:– A life threatening condition requiring
immediate treatment : Airway obstruction Inadequate ventilation / tension pneumothorax Active bleeding Shock

Triage• "YELLOW CODE" (“P2”) = The
horizontal but ABC intact patient who is demanding: – An injury which requires complex care but
is not an immediate threat to life : Fracture of a long bone Spinal lesion Abdominal injuries without shock Vascular injuries Large burns 20-60% BSA
Triage• "GREEN CODE" (“P3”) = The walking
talking but very demanding in terms of resources: – Patients with minor injuries requiring first
aid or outpatient treatment : Small lacerations Burns <20% BSA Musculoskeletal injuries without shock

Triage• "BLUE CODE" (“P4”) = The gasping /
agonal or obviously dead: (sometimes called black or grey codes):– Patients who are obviously dead or who
have apparently mortal injuries.
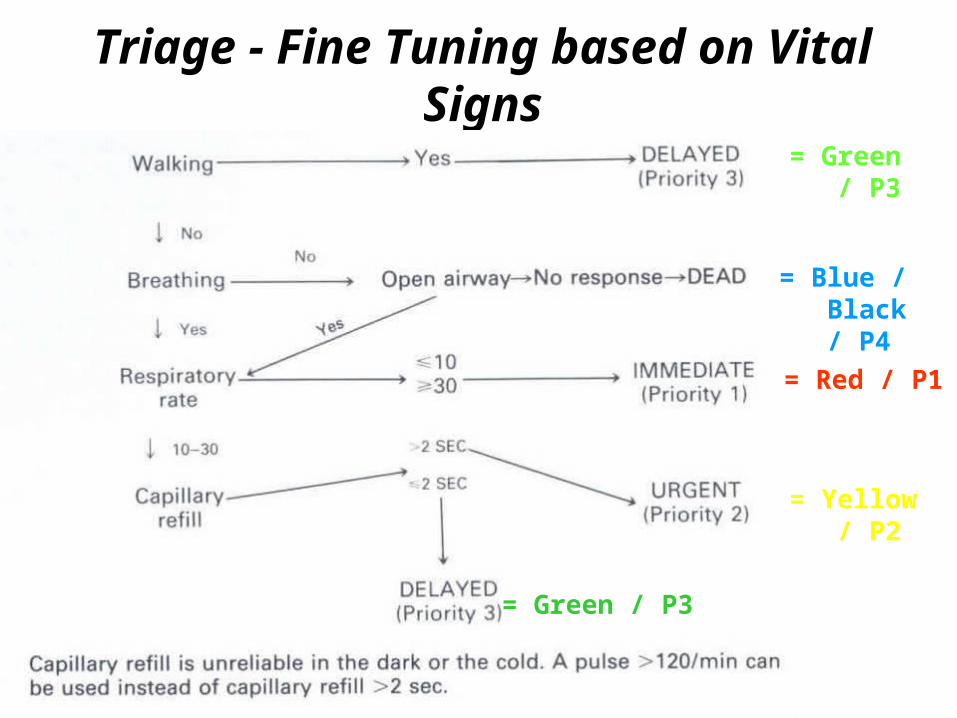
Triage - Fine Tuning based on Vital Signs
= Green / P3
= Blue / Black / P4
= Red / P1
= Yellow / P2
= Green / P3

Triage - Reality Check - KISS!!!!
• To summarise - Keep it simple stupid!! :– remove the walking ABCD intact green codes = +/-
80%– the +/-20% left behind are all horizontal -
• horizontal and gurgling with ABCD compromised = red codes = 1st priority
• horizontal with intact ABC so are able to cry for help = yellow codes = 2nd priority
• and the horizontal with ABCD foo-baa and dead or dying = blue codes = leave alone

Disaster Management
Triage tags applied to patients,
make one’s task of
sorting much easier
USA MILTAGS
Front Back

Disaster Management
Triage tags come in all shapes &
sizes

P1UrgentA B C
P2Semi-Urgent
D
P3Walkingwounded
P4Dead orDying
Name___________Dept__________Time____:____ Date___/__/____BP___/___P________R________IV____@__:____________________________________________
Triage Tag - fold to show
appropriate colour on outside
Triage
• Note Triage is on going / repeated:– T1 on scene – T2 at CCS/FAP– T3 on route / at hospital– T4 in the trauma unit

Scenario I-Bank Hold-up• Customer involved in a bank hold-up.
• 5 shot - 3 bank patrons & 2 bank employees.
• Robbers hold you & 12 individuals in the bank as hostages while they negotiate with the police negotiators.

Scenario I-Bank Hold-up• You are allowed to examine the victims
and evacuate them one at a time, to an ambulance in exchange for cool-drinks, food, beers, whisky & sodas, etc (wheels & firearms are not permitted) .
• The shootings occurred at noon - it is now 14:00
• The five injured are:

Scenario I-Bank Hold-up– A - 45yr man with 2xGSW - 1st entered below
the right nipple & exited through the right scapula while 2nd is a thro’ & thro’ injury to the palm of the right hand. Awake & alert. The hand & chest is wrapped with a torn shirt. Neither wound is bleeding. VS: P=90, RR=25
– B - 68yr diabetic man with a thro’ & thro’ GSW injury to the left thigh. C/O left leg & foot pain. A very large haematoma of the left thigh is noted & the distal foot is cool & pulseless. VS: P=110, RR=30

Scenario I-Bank Hold-up– C - 50yr obese woman with a GSW to the
right buttock - entry wound visible but no exit. She is lethargic, but responds to verbal stimuli. Her skin is cool & moist to the touch. VS: P=120, RR=35
– D - 25yr man with a thro’ & thro’ GSW to the left chest - entry wound 4th ICS midaxillary line & exited at the xiphoid. He is awake & alert, & C/O abdominal & chest pain. There is no obvious bleeding. VS: P=140, RR=25

Scenario I-Bank Hold-up– E - 22yr woman was standing near a window
& showered with glass from ricocheting bullets. She sustained multiple lacerations of the face & arms, including the right eyelid & globe. VS: P=90, RR=25
Who goes 1st, 2nd, 3rd, 4th & 5th in terms of evacuation - A, B, C, D, or E? (press right arrow for answer)
Answer: Evacuate patients in the followingorder C, D, A, B & E.

Scenario I-Bank Hold-up• How to triage:
1.ABCDE - boring, boring, boring but it works
2.MOI = Mechanism Of Injury - whose is the more severe
3.Who has the more deranged vital signs!
• SIMPLE STUFF ESPECIALLY IF THE CROCODILES ARE BITING
Scenario II-CarCrash• You are the only doc on a rural scene of a
motor vehicle accident - MOI = rollover with ejections
• You have available to assist you one paramedic student and AEA of 2 years standing
• You have 5 patients who were occupants of the car travelling at 96kph before it crashed
• The injured patients are:

Scenario II-CarCrash• A- 45yr unrestrained male driver who was
thrown against the windscreen. On arrival, he was in severe respiratory distress. Injuries include severe maxillofacial trauma with bleeding from the mouth & nose, an angulated deformity of the left forearm & multiple abrasions over the anterior chest - VS: BP= 150/80, HR= 120, RR= 40, GCS= 8

Scenario II-CarCrash• B- 38yr woman front seat passenger who
was thrown from the car & found 9meters from the car. On arrival she is awake, alert & C/O abdominal & chest pain. On palpating her hips, she complains of pain & fracture related crepitus is felt. - VS: BP= 110/90, HR= 140, RR= 25.

Scenario II-CarCrash• C- 48yr male passenger was found under
the car. He is confused & responds slowly to verbal stimuli. Injuries - multiple abrasions to his face, chest & abdomen. Breath sounds are absent on the left & abdomen is tender on palpation - VS: BP= 90/50, HR= 140, RR= 35, GCS= 10.

Scenario II-CarCrash• D- 25yr hysterical woman extricated from
the back seat of the vehicle. She informs you that she is 6/12 pregnant & C/O abdominal pain. Injuries include multiple abrasions to face & anterior abdominal wall - abdomen is tender to palpation & she is in active labour - VS: BP= 120/80, HR= 100, RR= 25.

Scenario II-CarCrash• E- 6yr boy extricated from floor of rear
seat who prior to your arrival was alert & talking. He now responds to painful stimuli by only crying out. Injuries include multiple abrasions & an an angulated deformity of right lower leg. There is dry blood around his nose & mouth - VS: BP= 110/70, HR= 180, RR= 35.

Scenario II-CarCrash• Triage these patients as to who you
would treat first, second, third, fourth & fifth (press right arrow for answer)
Answer: A, C, B, E & D

Scenario III-Disaster Planning
• It is 14:00hrs on a Sunday afternoon - “snooze time”. You are in charge of a 100 bed rural community hospital.
• Your available staff in the casualty include an ER physician, 2 nurses & four paramedics who are on clinical rotation as part of their clinical training.
• Your rural hospital has three ground ambulances & availability of a helicopter from the EMS. Surgical services are also available at your facility on a callout basis afterhours.

Scenario III-Disaster Planning
• The nearest definitive care center is 160km away
• A trucker calling on his radio, notifies the hospital that an overloaded minibus has run off the highway & rolled over.
• He states the minibus has approximately 25 passengers, some of whom are children who are in various degrees of panic & injury.
• The incident is approximately 10 minutes away from the hospital by ground ambulance.

Scenario III-Disaster Planning
• What calls need to be made & who should make them?
• What areas in the hospital need to be designated or set up for this condition?
• Who should go to scene?• What equipment & agencies should be
deployed to scene?

Scenario III-Disaster Planning
• What categories of triage should you anticipate using, & how should they be employed?
• What communications would you have available at the: – Scene?– Hospital?

Scenario III-Disaster Planning
• How would you manage the following:– Crowd control?– News media?– Ground ambulances?– Helicopter?– Traffic?– Patient indentification?

Scenario III-Disaster Planning
• Having considered all of the above:– Are you involved in disaster planning at your
hospital?– Is the plan adequate for the hospital?– Is the plan adequate for the community?– What are the key elements to the successful
management of a disaster plan?

Concepts in Mass Casualty Management – Pre-Hospital
FCPIC
OC
FAPCCS
Incident
CHA: Toys
Wheels/WingsPeople
Access route Egress route
COMMS
MetroControl
Primary & SecondaryHospitals
Principles:•FCP•IC / OC•FAP•CCS•CHA•Access•Egress•Comms•Hospitals

Marionhill Train Accident
8th March 1994• Emergency Medical Services Disaster
Management of the Scene - Summary:
• >380 injured
• >68 dead

Marionhill Train Accident• Early morning commuter train / rural Durban
bound railway line• ? Train speeding excessively & the passenger
coaches jumped the railway line while negotiating a curve near Marionhill station.
• Accident occurred @ 05:00hrs
• Driver went into the tunnel & contacted Spoornet Control & then ESCAPED the crowds wrath by going through the tunnel

Marionhill Train Accident• First emergency units arrived 10 - 15min later • Info relayed to Metro Control & additional units
dispatched• 05:30hrs - FCP created and attempts at creating
a CCS for red and yellow code patients was already in progress.
• Initially, great difficulty was experienced in clearing the highly emotional crowd of spectators away from the designated CCS

Marionhill Train Accident• The CCS was eventually achieved utilising
"reverse psychology" + local chief, who requested his community to assist in acting as stretcher bearers – this dissipated the not unexpected, high emotion present when EMS first arrived on scene.
• Often this emotion is unreasonable & directed at anyone representing some authority - use the emotion wisely - give people something to do!

Aerial view into the valley : 11 coaches involved, 2 separated & 9 derailed
Tunnel + 2x coaches200m away
Durban bound

Note effectiveness of cordons in keeping spectators back

Marionhill Train Accident• Acute shortages of stretchers in the early
phase of the response, required that patients brought to the CCS were moved off the stretcher or board onto the ground, so that the stretcher could be reused for another patient
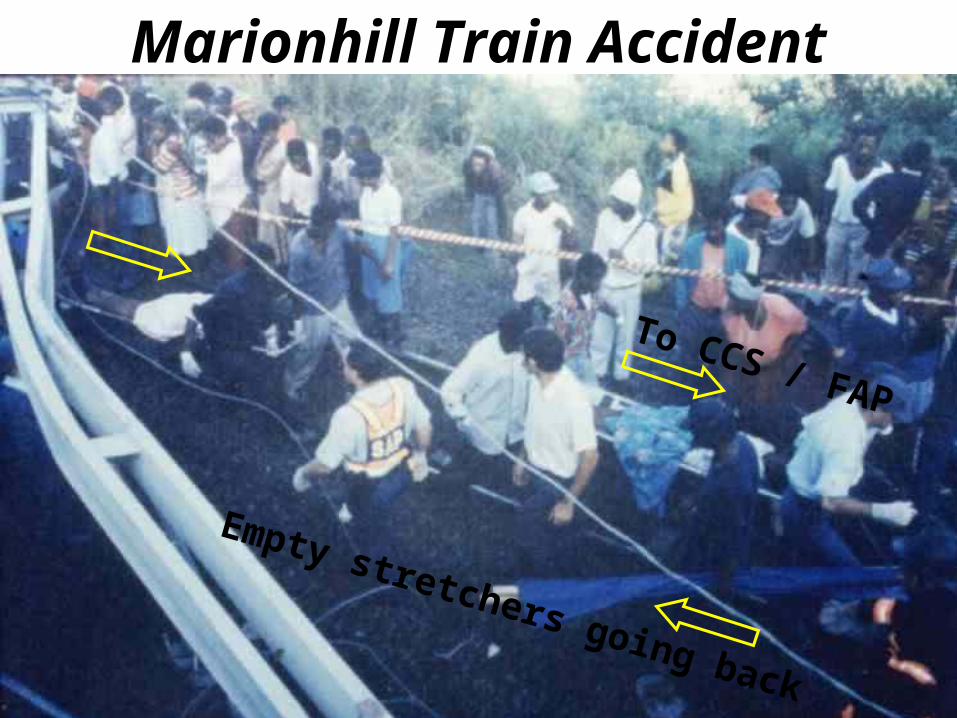
Marionhill Train Accident
To CCS / FAP
Empty stretchers going back

Marionhill Train Accident• At this point & despite every effort, it had
become obvious that the small dirt track winding down to the railway line, was completely blocked by numerous vehicles preventing ambulances shuttling patients up to the top of the hill.
• Other options had to be explored: – hand carrying the stretchers up the hill – SAAF 15 Sqdrn heli assets airlift ????

Marionhill Train Accident• SAAF Oryx helicopters arrived overhead ->
circled & the first came in hovering under the high tension Eskom power lines to land -> unloaded sorely needed 20 fold up stretchers -> before loading 7 - 8 red code patients on the floor of the aircraft + 1x paramedic
• Additionally a pilot joined the FCP with a ground-to-air radio to act as a local ATC & relay designated hospitals to the aircraft

Overview of Marionhill Accident Site
Tunnel & Durban
FCP
CCS
Yellow CodeCCS + Buses+ Bulk Supply
Green codeFAP + Buses
Communications unit placed on hill top
H2OFood
Railway linein valley floor
HeliLZ2
Eskom HTpower linesacross the
valley
Egress routeto Durban
Footpath throughvalley Heli
LZ3
Main tarred roadon hilltop
2
1
3
Heli LZ1

Marionhill Train Accident• By 09:00hrs (4 hours after the accident), >380
patients moved by ambulance, disaster bus & helicopter (>60) to 12 different hospitals
• The patient loads were determined by the capabilities of the respective hospitals e.g. Marianhill Hospital accepted 50 green codes
• No hospital was sent more than 50 patients to prevent hospital overload
IT AINT FINISHED UNTIL THE FAT LADY SINGS! So true!5/2/2002 Charlottedale Station near Stanger - Dead = 26 (>16 children) & Injured = 100


Concepts in Mass Casualty Management - In-Hospital
FCPIC
OC
FAPCCS
Incident
CHA: Toys
Wheels/WingsPeople
Access route Egress route
COMMS
MetroControl
Primary & SecondaryHospitals
Principles:•FCP•IC / OC•FAP•CCS•CHA•Access•Egress•Comms•Hospitals

Triage- Comrades Marathon Medical Tent - A Planned Annual Disaster
Medical Tent
Triage Tent
First Aid Tent
Entry

Triage- Comrades Marathon Medical Tent - A Planned Disaster for 14,000 masochistic
runners
1. Dr John Godlington2. Dr Jeremy Bolton3. ?Where are the articles??
Mobile walking talking FCP

Iraq 2003/4

Simple & cleanable
Burn pack
Thomas bag ALS
Spine broad
Bulk stretchers
Bulk C’ collars

Triage
ER Resus
OR/OT Wards
ICU
<- Power
Sewerage
Heli access
Road access
Water
Lab / blood bank
Containerised bulk supplies
Wings + wheels egress
Access into & Egress route out of
FCP +Comms
Staff accomadation
Security cordon
FAP
Air Con Units
Pharmacy

ER Triage / Resus Area - Waiting for the choppers – tents are
sealed positive pressure units in case of biochem warfare

1
42 3
6
5
10
87
11
9
15
14
16
1312
20
19 18
17
1. OP entrance 2. Expat Dr Room 3. National Dr Room 4. Dental Room 5. Pharmacy 6. OP waiting area 7. Admin 8. Holding room 9. Tea Room 10. Toilet 11. Toilet 12. Lab 13. X-Ray 14. Shower 15. Janitor 16. Receiving / Triage Area 17. Foyer 18. ER Holding 19. Scrub 20. ER
Original Point A Clinic floor plan
(Not to Scale)

1
42 3
6
5
10
87
11
15
14
16
1312
17
1. OP entrance 2. Expat Dr Room 3. National Dr Room 4. Dental Room 5. Pharmacy 6. OP waiting area 7. Admin 8. Holding room 10. Toilet 11. Toilet 12. Lab 13. X-Ray 14. Shower 15. Janitor 16. Receiving / Triage Area 17. Foyer
New Point A Clinic floor plan
(Not to Scale)
ER / TreatmentRoom

1
42 3 5
10
7
11
15
14
16
1312
Triage Area
Communications Centre
KE
EP
CL
EA
R• RADIO - BASE STATION
• RADIO H/HELD
• PHONE
• FAX
• H/PHONE
Links: • ERC / APO• Security• Jakarta Medical• Medan / Sing Evac• Aviation• SLS / NSO• Ambulances

1
42 3
6
5
10
87
11
15
14
16
1312
Triage AreaAccess
Clear outpatients and non-essential personnel
Egress
On notification of Incident
Ambulance
Holding
Area
A
Establish Cordon
SECURITY OFFICER
ER / TreatmentRoom
•Open disaster stock
•Check communications
• Assemble & brief staff including all & additional ambulance drivers• Check all ambulance radios communicating with base station
•Put out trestles & NATO stretchers for overflow
•Open pharmacy

1
42 3
6
5
10
87
11
15
14
16
1312
Triage AreaAccess
Clear outpatients and non-essential personnel
Egress
Arrival of Casualties
Ambulance
Holding
Area
A
Establish Cordon
SECURITY OFFICER
ER / TreatmentRoom
•Monitor communications
• Place staff appropriately • Monitor ambulance radios for ETA
•Assess triage on trestles & NATO stretchers
•Pharmacy to assist with supplies

Admin
Lab
15
X-ray
Triage Area
KE
EP
CL
EA
R
RADIO
DESIGNATED HOLDING AREA
HOLDING AREAS (MASS STOCKS)GREEN CODE PATIENTS
YELLOW CODE PATIENTS
COMMUNICATIONS
RED CODE PATIENTS BLUE CODE PATIENTS
Clinic – Mass Casualty Plan
ACCESS
EGRESS
Resuscitation Area
Mortuary Area +
Security
Security
Security

Access (& forced egress) route is totally inadequate for ambulances & buses all arriving & crowding in at once. Instead this requires a drive through capability after off-loading patients. Also ensure disaster bus
configurations are taken into account – height & length. Currently there is not even enough turning
circle therefore. Currently even ambulances get hemmed in, blocking access (as during our visit),
never mind buses.
Ngwelezane Hospital Disaster Ideas

Triage Area as big as possible
Extend cover
The area provided for ambulances is totally inadequate – a basic principle of disaster management is the avoidance of vehicle turn
around or cross-over. There should be a clear access & egress routes which do not cross over otherwise there will be an ambulance
blockage at the ER entrance causing delays & unnecessary chaos (there is usually enough chaos anyway – lets not add to it – it becomes a medico-legal hazard). Similarly, green codes going to MOPD by foot
or wheelchair, should not cross over other coded patient paths.
The triage area should be as large as possible to cover all eventualities considering a single bus accident will engender a minimum of 60
patients if not overloaded. A train accident will be even worse.
Helipad to be developed
Ideally direct drive through after patient off-load cf. Kentucky
Fried Chicken!
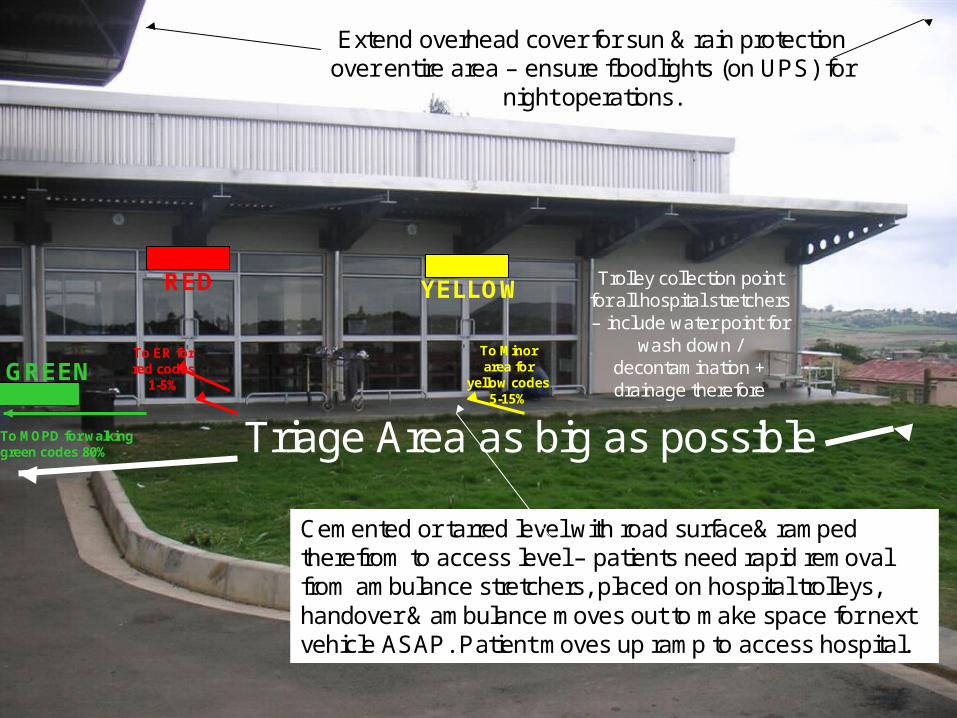
Cemented or tarred level with road surface& ramped therefrom to access level – patients need rapid removal from ambulance stretchers, placed on hospital trolleys, handover & ambulance moves out to make space for next vehicle ASAP. Patient moves up ramp to access hospital.
Extend overhead cover for sun & rain protectionover entire area – ensure floodlights (on UPS) for
night operations.
To MOPD for walking green codes 80%
To ER for red codes
1-5%
To Minor area for
yellow codes 5-15%
Trolley collection point for all hospital stretchers – include water point for
wash down / decontamination + drainage therefore
Triage Area as big as possible
RED YELLOW
GREEN

Replace / modify with painted red, yellow & green stripes on the floor for
uneducated / uninformed staff / volunteers to move patients within hospital – e.g. “follow the red line”
ERMOPDMinor Area

The Extreme Disaster - The Turkish Earthquake
04:45hrs 17 August 1999

45 sec earthquake7.4 Richter scale17,000 dead,>50,000 injured,some estimating>70,000.
Widespreaddestruction to housing, water,sanitation, power,communications,road & rail links
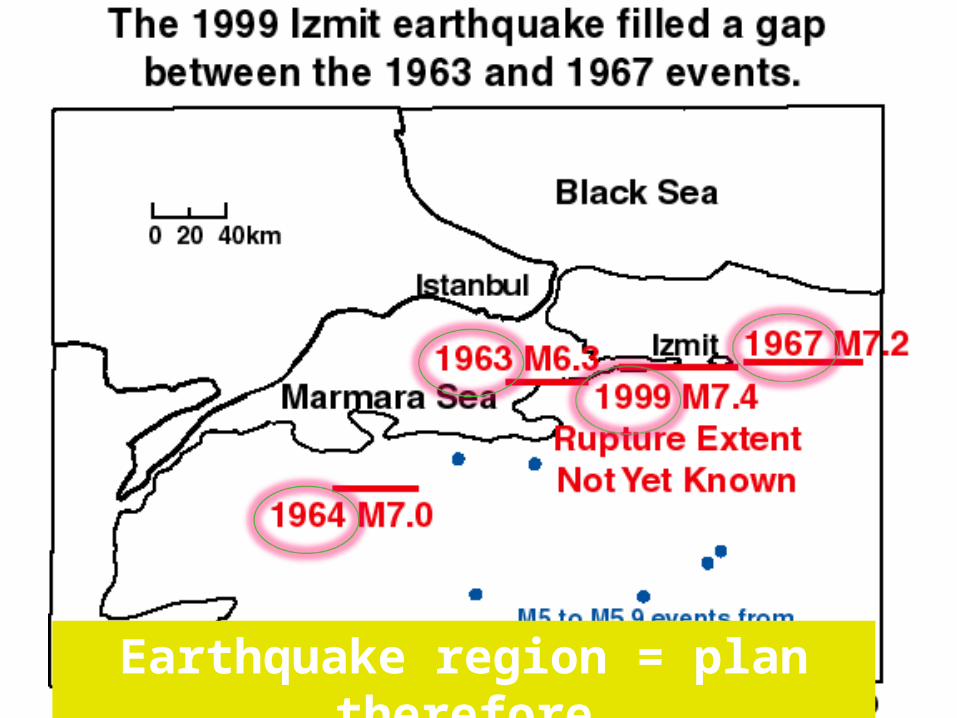
Earthquake region = plan therefore

Have SOMEONE engage politicians & media when they arrive, otherwise you
will be chowed!

No cordon = chaos = Gauteng petrol tanker rollover 2008 – KISS for the idiots of this world

WHEN YOU ARE UP TO YOUR EARS IN CROCODILES - REMEMBER THE FACE!!
I
FCPIC
OC
FAPCCS
CHA: Toys
WheelsPeople
Access route Egress route
COMMS
MetroControl
Primary & SecondaryHospitals
THANKYOU
With acknowledgementto Mr Alan White, FRCS
& J.P.Keenan, FRCS,Chief AEMS 1981-1986 & 1986-
91 respectively