Embed Size (px)
Citation preview
Maryland Regulatoryand
Legislative Update: Past and Present
Michelle Hayes Duell, CRNA, DNPMANA spring meeting
March 2015
1

ObjectivesObjectives
Awareness of Nurse Anesthesia regulations in Maryland
Appreciate the history and changes of the regulations
Acknowledge past & present legislation impacting Nurse Anesthesia regulations
Compare current Maryland regulations to those regulations in other states
2

OverviewOverview
CRNA Regulations History Changes Collaboration Agreement
Advanced Practice Nursing Initiatives
“The Future of Nursing” 2010 IOM Report
Recent Legislative History Anesthesiology Assistant Bill Physician Assistant Bill Nurse Practitioner Bill
3

RegulationsRegulations
Advanced Practice Nurses in Maryland
CRNAs (730) Advanced Practice Registered
Nurse/Psychiatric Mental Health ( APRN/PMH)
Certified Nurse midwives (243) Nurse Practitioners (5,200) (New) CNS - October 2014
4

RegulationsRegulations
In 2002, an Advanced Practice Nurse was placed on Maryland Board of Nursing
Specialty Changes
CRNAs were first (John Bing)
APRN/PMH (Susan Krause)
Midwife is up next…
5

CRNA RegulationsCRNA Regulations
HistoryEstablished December 1, 1979COMAR (Title 10 Chapter 06) of the
Maryland Nurse Practice ActRegulations Available Online
Regulate our practiceCollaboration Agreement Required
Now referred to as an “Attestation”
6

CRNA RegulationsCRNA Regulations
Three changes documented 2000 terminology was changed which
allowed for scope of practice to be listed separately
2006 agreement not necessary before obtaining license
2007 Master’s degree requirement and grandfathering of CRNAs prior to January 1, 2008
7

Maryland CRNA RegulationsMaryland CRNA Regulations
8
Regulation“A CRNA may not practice in this state
until the CRNA has notified the Board of the name and license number of the collaborating physician or dentist.”
27.06.02 (c) p. 1592

Maryland CRNA RegulationsMaryland CRNA Regulations
9
Collaboration“The development and implementation
of an agreement between a nurse anesthetist and an anesthesiologist, licensed physician, or dentist concerning the practice of nurse anesthesia.”
27.06.02 (c) p. 1592

CRNA RegulationsCRNA Regulations
Collaboration Agreement issue .02 Certification.
A. An applicant for certification as a CRNA shall..
B. If the applicant's nurse anesthetist program was completed after January 1, 2008…program with a master's degree or higher.
C. A CRNA may not practice in this State until the CRNA has notified the Board of the name and license number of the collaborating physician or dentist.
D. The Board shall forward the name and license number of the collaborating physician or dentist to the appropriate regulatory board.
10

Old Agreement Old Agreement
11

NEW NotificationNEW Notification
12

Attestation Attestation UPDATED NOTIFICATION OF COLLABORATION
The Code of Maryland Regulations (COMAR) 10.27.06.02 C. requires that Certified Registered Nurse Anesthetists (CRNAs) provide the Maryland Board of Nursing (MBON) a notification of collaboration. The notification shall include the name of ONE collaborating physician or dentist. Additional notices for specific work sites are not required.
Collaborator most recently named will be the physician or dentist collaborator of record.
If you currently have more than one collaborator on file, please notify the board as soon as possible to indicate which ONE collaborator of record you wish to maintain. Please call (410) 585-1926 or email [email protected]
13
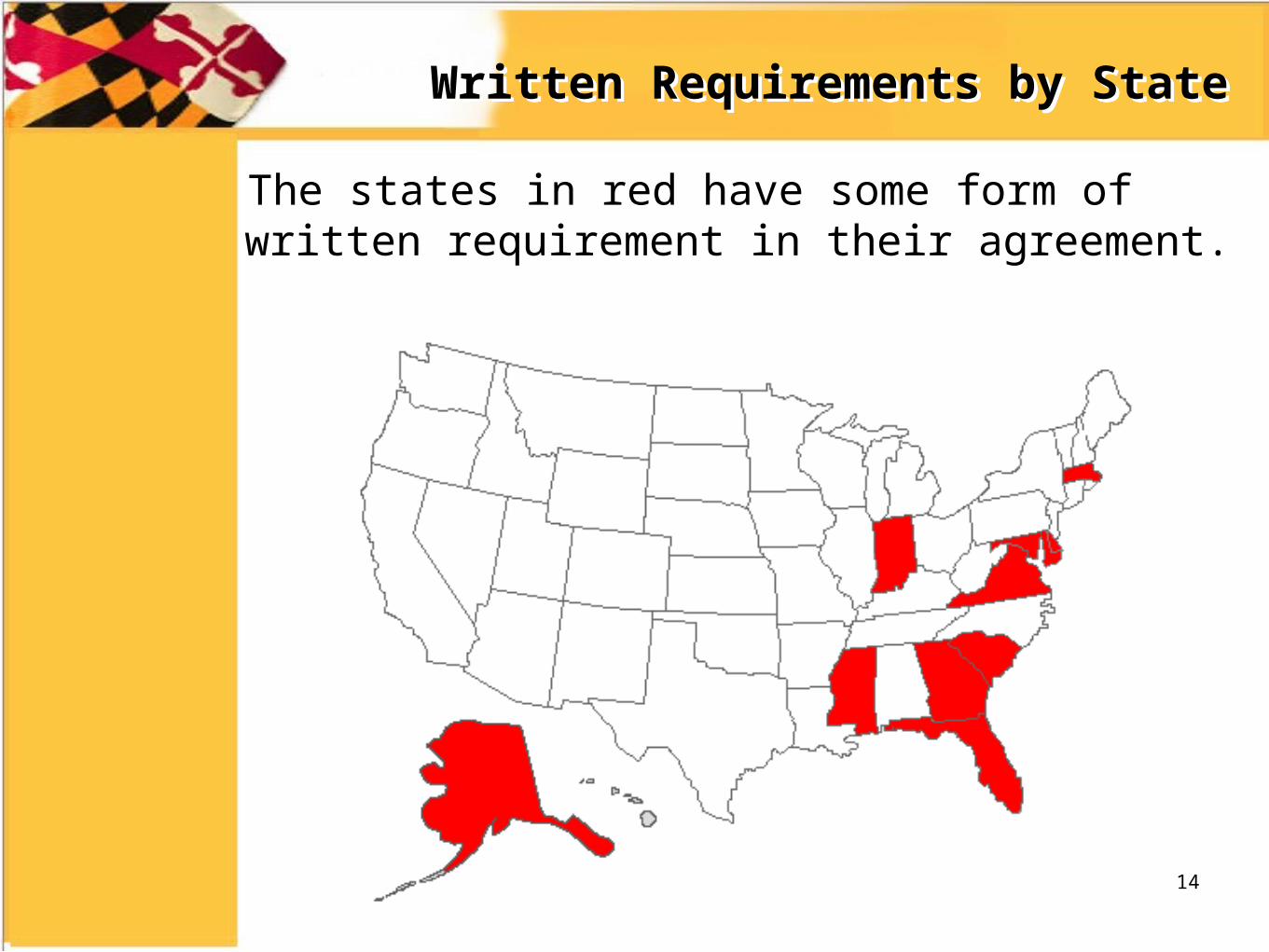
Written Requirements by StateWritten Requirements by State
The states in red have some form of written requirement in their agreement.
14
CRNA RegulationsCRNA Regulations
Take C and D away under certification? .02 Certification…
C. A CRNA may not practice in this State until the CRNA has notified the Board of the name and license number of the collaborating physician or dentist.
D. The Board shall forward the name and license number of the collaborating physician or dentist to the appropriate regulatory board.
Clarify definition of collaboration? Add Podiatrists
15

CRNA RegulationsCRNA Regulations
Peer Advisory Committee CRNA members
08 CRNA Peer Review/Advisory Committee.
A. The Board shall appoint at least four CRNAs to act as the Board's advisory committee.
B. The Committee shall:
(1) Meet at least four times a year;
(2) Report at least annually on its overall activities; and
(3) Function at the Board's direction and provide the Board with expert advice related to the practice of nurse anesthesia.
C. Members of the Committee shall be appointed for a 4-year term and may be reappointed for one additional 4-year term.
16

The Instituteof
MedicineReport
2010
17
18
The 2010 IOM ReportThe 2010 IOM Report
1. Remove scope of practice barriers2. Expand opportunities for nurses to lead in
collaborative efforts3. Implement nurse residency pro4. Increase the proportion of nurses with a
baccalaureate degree to 80% by 20205. Double the number of nurses with a
doctorate by 20206. Ensure that nurses engage in lifelong
learning7. Prepare and enable nurses to lead change
to advance health8. Build an infrastructure for the collection
and analysis of inter-professional health care workforce data

The 2010 IOM ReportThe 2010 IOM Report
Remove Scope of Practice Barriers Conform to National Council of State Boards
of Nursing (NCSBN) Model Nursing Practice Act
Fee for Service and reimbursement Arrangements
Hospital participation requirements
Restrictive state regulations should be amended
19

20
Legislative History

Anesthesiologist Assistant Legislation
Anesthesiologist Assistant Legislation
We hear “through the grapevine”, Johns Hopkins Hospital may put forth legislation for AA’s to practice.
Early fall 2008 this “talk” starts
MANA begins preparing for legislation to be filed in the upcoming session.
Fall fundraisers are attended.
MANA holds a fundraiser for HGO Chair Pete Hammen
21
Anesthesiologist Assistant Legislation
Anesthesiologist Assistant Legislation
Johns Hopkins Hospital chief anesthesiologist is spearheading the legislative effort.
MANA lobbyist requests a meeting with him in December to discuss this proposed idea one-on-one.
Meeting December 16, 2008
22

Anesthesiologist Assistant Legislation
Anesthesiologist Assistant Legislation
JHH sited decreased manpower as the reason for initiating an AA program.
MANA supported a study to be done to evaluate the staffing shortages
University of Maryland SON NAP offers site specific students to alleviate “shortage”
Waited…and waited…and waited…
23

Anesthesiologist Assistant Legislation
Anesthesiologist Assistant Legislation
A company that specializes in grassroots was hired to put together letters and packets to be mailed to CRNAS
A automated phone service was initiated prompting CRNAs to call their legislators
Groups of CRNAs were organized for multiple days each week to make visits to both house and senate
These CRNAs were educated on what needed to be said
Buy in from influential parties was attempted: MNA, MBON, BOM
Those CRNAs that would speak for all CRNAs in Maryland during the hearing were selected
Recruiting as many CRNAs as possible to be present during the hearing to show support
24

Anesthesiologist Assistant Legislation
Anesthesiologist Assistant Legislation
Senate bill was introduced first by Senator Conway (SB 798)
Remind you that Senator Andy Harris sat on the Senate committee this bill was assigned to.
Lobbying and grassroots efforts began
25

Anesthesiologist Assistant Legislation
Anesthesiologist Assistant Legislation
Senate Hearing-March 13, 2009
Large support presence from CRNAs
Met resistance from Senator Harris
AA’s testified about their practice
Maryland PA/AA stayed completely neutral
BOM testified they could not regulate another group of providers
26

Anesthesiologist Assistant Legislation
Anesthesiologist Assistant Legislation
Senate Chair stated that discussion was required for the bill and that it would be sent to summer study.
Within a hour of Senate hearing finishing, Chair of the House committee called MANA lobbyist and informed him that the sponsor of the HGO bill had respectfully pulled his bill!
27
Physician Assistant LegislationPhysician Assistant Legislation
PA legislation surfaced in the 2010 legislative session
This is an example of a bill that inadvertently has consequences not planned.
28
Physician AssistantPhysician Assistant
Overall, I feel this legislation was a “lose” situation for CRNAs
However, the best case scenario was obtained
29

Physician AssistantPhysician Assistant
10.32.03.06
.06 Delegation Agreements — Approval.
B. Core Duties.(1) Upon receipt of a delegation agreement at the Board of Physicians,
a physician may delegate and a physician assistant may perform delegated core medical acts.
(2) The Board shall notify the primary supervising physician and the physician assistant of the Board’s receipt of the delegation agreement.
C. General Anesthesia and Neuroaxial Anesthesia.(1) Regardless of setting or other factors, a supervising physician
may not delegate and a physician assistant may not perform general anesthesia or neuroaxial anesthesia before the Board has approved the delegation.
(2) The Board shall provide written notification of approval or disapproval of the delegation under §C(1) of this regulation.
30

Certified Nurse MidwivesCertified Nurse Midwives
Collaborative plan was eliminated September 2014
31
NP LegislationNP Legislation
2010 NP Bill Practice authority under Board of
Nursing only Attestation verses multiple page
agreement Regulation, but also statute
2015 proposed legislation Remove attestation requirement HB999 and SB723
32

33
Questions?





























