Embed Size (px)
DESCRIPTION
Last Lecture. Maps Plasticity of maps Retinotopic map. Today’s Outline. More: Retinotopic Map Parallel Visual Pathways Blindsight. Visual world onto the retina. RVF Left Temporal retina Right Nasal retina. LVF Left Nasal retina Right Temporal retina. Retinotopic Map. - PowerPoint PPT Presentation
Citation preview

• Maps• Plasticity of maps• Retinotopic map
Last Lecture
• More: Retinotopic Map• Parallel Visual Pathways• Blindsight
Today’s Outline

Visual world onto the retina
LVFLeft Nasal retina Right Temporal retina
RVFLeft Temporal retinaRight Nasal retina
Retinotopic Map

Left Eye’s View
Retinotopic Map

Right Eye’s view
Retinotopic Map

Perimetric testing to Diagnose field defects
View from above
Retinotopic Map

Each eye’s field of View (visual field) is mapped out
Can light be detected throughout the visual field?
Retinotopic Map

Left
Right
VF Left Eye VF Right Eye
Combined Visual Field
Retinotopic Map

Left
Right
VF Left Eye VF Right Eye
Combined Visual Field
Retinotopic Map

Function: Perimetric Map shows blindness in lower right quadrant of…
Left Eye Right Eye
Where is the damage?Retinotopic Map

On the retinae?
Retinotopic Map

From Retina to Brain
Geniculo-Striate Pathway Optic nerve carries
signals from retina.• Decussation at optic
chiasm (optic tract)• Synapse at Thalamus:
Lateral Geniculate Nucleus (LGN)
• Optic radiations to• AREA 17; Striate
Cortex, Primary visual cortex
Retinotopic Map

Visual World Mapped onto Cortex (via the retina) >> retinotopic map
Retinotopic Map
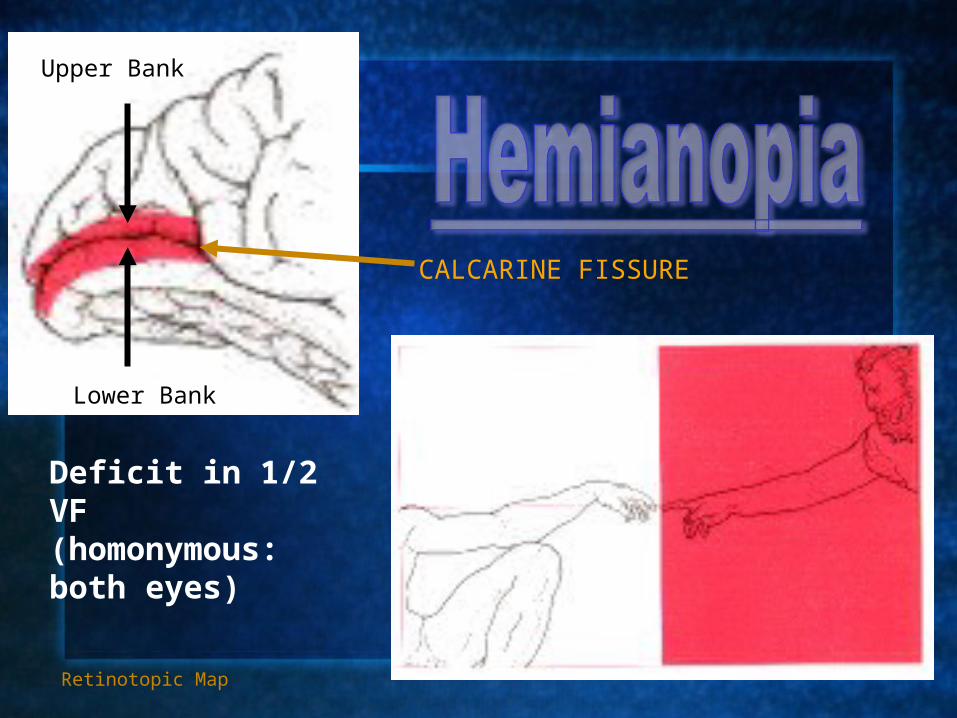
Deficit in 1/2 VF (homonymous: both eyes)
Retinotopic Map
CALCARINE FISSURE
Upper Bank
Lower Bank

Function: Perimetric Map shows blindness in lower right quadrant of…
Left Eye Right Eye
Where is the damage?Retinotopic Map
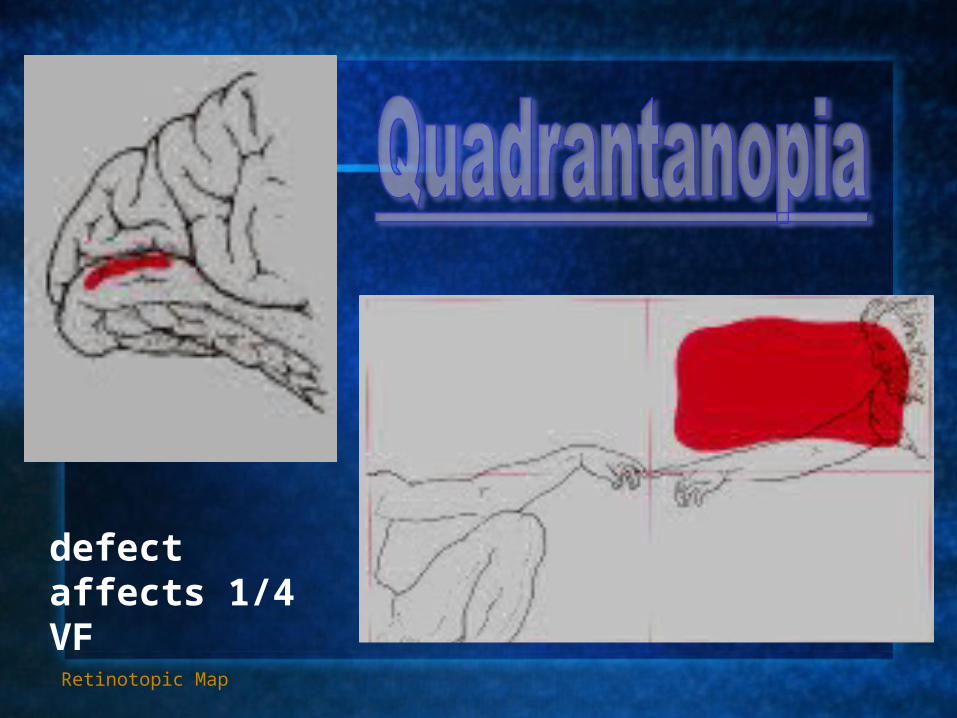
defect affects 1/4 VF
Retinotopic Map

An area of visual loss surrounded by relatively well-preserved vision. Size and shape vary.
Retinotopic Map

Gordon Holmes (1919)Correlated Visual Field Defects with lesion locus to identify theRetinotopic map.
Retinotopic Map
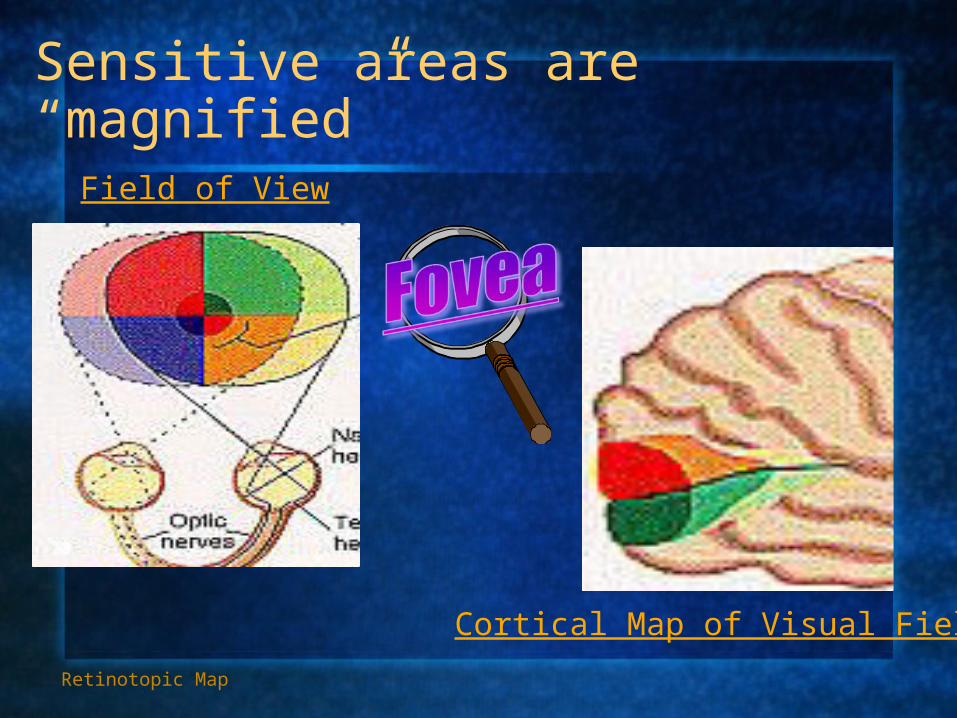
Sensitive areas are “magnified”
Field of View
Cortical Map of Visual Field
Retinotopic Map

Equi-visibility chart
Objects in the periphery must be
Physically larger in order to beas visible as objects falling on fovea
Fovea is more sensitive
Cortical Magnification
AnstisRetinotopic Map

Fovea is a small portion of retina
Retinotopic Map

Cortical Magnification
• Area 17 neurons have receptive fields in the retina
• More neurons have foveal receptive fields
Retinotopic Map

Retinotopic map: Summary
Crossed organization Left 17 --> RVF Right 17 --> LVF
Inverted organization Lower calcarine > Upper VF Upper calcarine > Lower VF
Fovea: Disproportional representation cortical magnification
NOTE: Each visual cortex represents a visual field NOT an eye.
Retinotopic Map

VF Left Eye VF Right Eye
Combined Visual Field
Left
Right
Nasal
Retinotopic Map

Left
Right
Nasal
VF Left Eye VF Right Eye
Combined Visual Field
Retinotopic Map

Left
Right
Nasal
VF Left Eye VF Right Eye
Combined Visual Field
Retinotopic Map

For your review: the connections
Left EyeNasal hemiretina- LVF- projects
to right hemisphereTemporal hemiretina- RVF-
projects to left hemisphere
To cross at optic chiasm
uncrossed uncrossed
Right EyeNasal hemiretina- RVF- projects to left hemisphereTemporal hemiretina- LVF- projects to right hemisphere
nasal
LVF input to Rhem. RVF input to LHem
LEFT EYE’s RETINA
RIGHT EYE’s RETINA

• The Retinotopic Map• Parallel Visual Pathways• Blindsight
Outline

Parallel Pathways
From Retina
To primary visual cortex
To superior colliculus
Parallel Pathways
Path to SC

LGN StriateextraStriate
LORE of neurology until the early 70's...
Vision requires Area 17…or maybe not?
Reports of residual vision in Animals with striate lesions (hamsters; monkeys): Recovery after experimental field defects (cortical ablations)
spared light/dark discrimination spared localization abilities
Implication: Other pathways can compensate for some geniculo-striate function.
Can this also be true in humans??
Parallel Pathways





























