Embed Size (px)
Citation preview
Mapping the Policy Environment for Family Health
Rowena Cabigon, Rhodora Tiongson, Carlo Panelo, and Orville Solon, editors

by Rowena Cabigon
Rhodora Tiongson, Carlo Panelo, Orville Solon, editors
Mapping the Policy Enviroment for Family Health
Published by the UPecon-Health Policy Development Program (HPDP), Encarnacion Hall, University of the Philippines Campus, Diliman, Quezon City, Philippines. Telephone: +632 927-9686 loc 322. E-mail: [email protected]. April 2012.
products does not imply that they are endorsed or recommended by the publisher in preference over others of a similar nature. Articles may
permission, provided credit is given to HPDP and/or the individual authors for original pieces. A copy of the reprinted or adapted version will be appreciated.
Suggested Citation:
R. Cabigon. Mapping the Policy Environment for Family Health. Quezon City: UPecon-Health Policy Development Program, 2011.
This volume was made possible with the support of the American people through the U.S. Agency for International Development (USAID) to the UPecon-Health Policy Development Program under the terms of Cooperative Agreement No. 492-A-00-06-00031. The contents of this volume are the sole responsibility of the authors and do not
the Department of Health (DOH).
Style editing: Wystan de la Peña
Cover design and lay-out: Giselle de la Peña and Judith Camille Rosette
Cover photos courtesy of Maria Gracia Alcantara
Table of Contents
8
9
10
14
INTRODUCTION 16
PURPOSE AND SCOPE 17
1 ELIMINATING UNMET NEED FOR FAMILY PLANNING
Contraceptive Self-Reliance StrategyLocal Government Response to CSRGrowing Involvement of the Private Sector
Gaps, Challenges and Opportunities
Persistent Need for Better Contraceptive Information and Accessibility
the Poor and Hard-To-Reach Population Sectors
Lack of LGU Capacity to Manage and Implement CSRLimited Private Sector Participation in FP Service Delivery and Supply of CommoditiesCost Issues and Funds Availability
20
21
23
23242828
29
29
30
31
3132
Department of Health (DOH)Local Government Units (LGUs)PhilHealthFaith-based Organizations
34
35404142
2 IMPROVING MATERNAL AND CHILD HEALTH
Trends in Maternal, Neonatal and Child Health
Broad-based legislative support for child healthRecent Shift from “Risk Approach” to an “Emergency Obstetric and Neonatal Approach”Opportunities for Service Quality Upgrading through Capacity BuildingInnovative Service Strategies, and Facility Expansion / Upgrading for MNCH Service Delivery
Gaps, Challenges and Opportunities
Geographic and Socioeconomic Disparities in MNCHLimited Quality, Accessibility and Sustainab ility of MNCH ServicesLow Utilization of MNCHN Services and Continued Preference for Home-based Deliveries (Villa & Villegas, 2008)Inadequate Financing Mechanisms
43
44
46
46
47
49
49
51
51
52
5253
54
3 ACHIEVING PUBLIC HEALTH CONTROL OF TUBERCULOSIS
56
57
58
60
TB ControlQuality AssurancePublic-Private Partnerships Financing Package
Local Variations in TB ControlInadequate LGU Capacity and OwnershipInadequate Expansion and Monitoring of DOTS CoverageHealth-Seeking Behavior, Knowledge and Attitudes on TBLimited Private Sector Participation in DOTS Need for Sustained and Coordinated Financing
65
6667676768
69
697071717273
77
4 PREVENTING A LARGER EPIDEMIC OF HIV/AIDS
Strong Framework for HIV/AIDS Policy and ImplementationEarly Establishment of Active and Passive Surveillance Systems Multi-Sectoral Response to Service Needs
Persistent Risks and Vulnerabilities Among High-Risk GroupsHigh-Risk Behaviors Among the YouthLow Level of HIV/AIDS Knowledge and Awareness
the Role of PNAC
Need for Sustained Financing
79
81
82
82
8385
86
868787
888889
90
5 ACCELERATING HEALTH IMPROVEMENTS IN THE AUTONOMOUS REGION IN MUSLIM MINDANAO (ARMM)
Region With The Poorest Health and Development Indicators
Lack of Competent Health Professionals
Limited Financing for Health and Challenges to NHIPUnique Politico-Administrative Setup of ARMM
Assessing CSR Response In ARMM
CSR in ARMMUnmet Need and Contraceptive Prevalence RateKey Policy Recommendations for CSR in ARMM
Scaling Up Malaria Control in ARMM
Challenges for Malaria Control in ARMMKey Policy Recommendations for Malaria Control in ARMM
Securing Critical Health Human Resources for ARMM
Plantilla VacanciesMisuse of Plantilla ItemsLack of Appropriate Skills Among Current Personnel
Alternative Planning Strategies for Planning and Response Mechanisms in ARMM
Need for Accurate Health Information in the Planning Process
91
92
93
93939495
96
969797
98
99100
101
102103104105
106
108108109
110

6 LOCAL F1 IMPLEMENTATION AND OTHER
FAMILY HEALTH
Utility of the Province-Wide Investment Plan for Health (PIPH),
Accomplishments and Shortcoming of the PhilHealth Indigent
Access to Health Care
the Private and Public Sectors
113
114
118
123
130
134
7 POLICY ENVIRONMENT FOR FAMILY HEALTH: SUMMARY AND HIGHLIGHTS 141
144
About the Author and Editors 154

8
List of Tables
Table 1Prevalence and Mortality in the Philippines: 1990-2005
57
Table 2
in USG-supported areas
61
Table 3 64
Table 4 75
Table 5 80
Table 6and their Descriptions
115
Table 7and Needed Professional Competencies
131
9
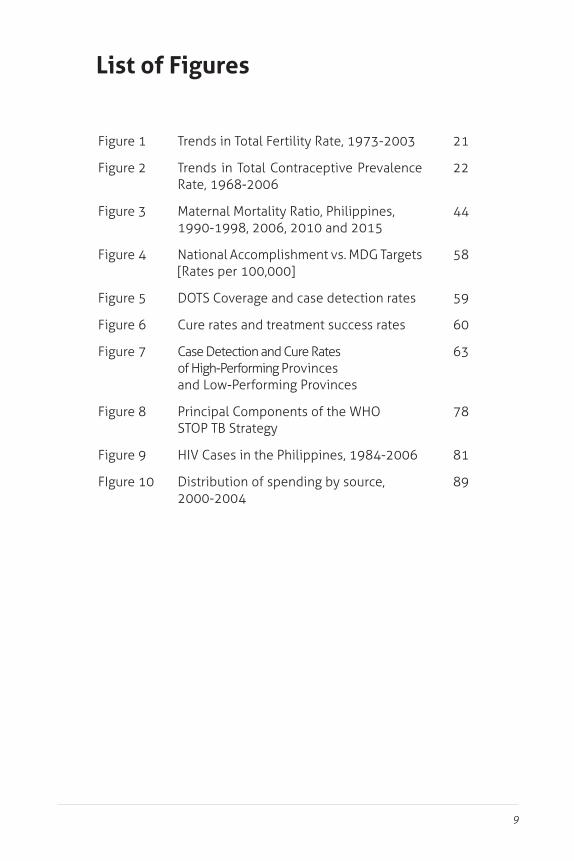
List of Figures
21
Trends in Total Contraceptive Prevalence Rate, 1968-2006
22
Maternal Mortality Ratio, Philippines, 1990-1998, 2006, 2010 and 2015
44
National Accomplishment vs. MDG Targets [Rates per 100,000]
58
DOTS Coverage and case detection rates 59
Cure rates and treatment success rates 60
Case Detection and Cure Rates of High-Performing Provinces and Low-Performing Provinces
63
Principal Components of the WHO 78
81
Distribution of spending by source, 2000-2004
89

10
AIPHAOAOPARGARMM
ASHI
CCMCDCCDLMIS
CDRCEmONC
CHDChild 21
CHOCOCPRCRCSCSOCSRCUPDepEd
DOHDOH-ARMM
ARMM-wide Investment Plan for HealthAdministrative OrderAnnual Operation PlanAutonomous Regional GovernmentAutonomous Region in Muslim MindanaoAnti-retroviral ARMM Strategy for Health Improvement
Information SystemCountry Coordinating MechanismCenter for Disease ControlContraceptive Distribution Logistics and Management Information SystemCase Detection RateComprehensive Emergency Obstetric and Neonatal CareCenter for Health Development
Plan Development for Children, 2000-2025
Capital OutlayContraceptive Prevalence RateCure RateChild SurvivalCivil Society OrganizationContraceptive Self-Reliance
Department of Education
Department of HealthDepartment of Health – Autonomous Region in Muslim Mindanao
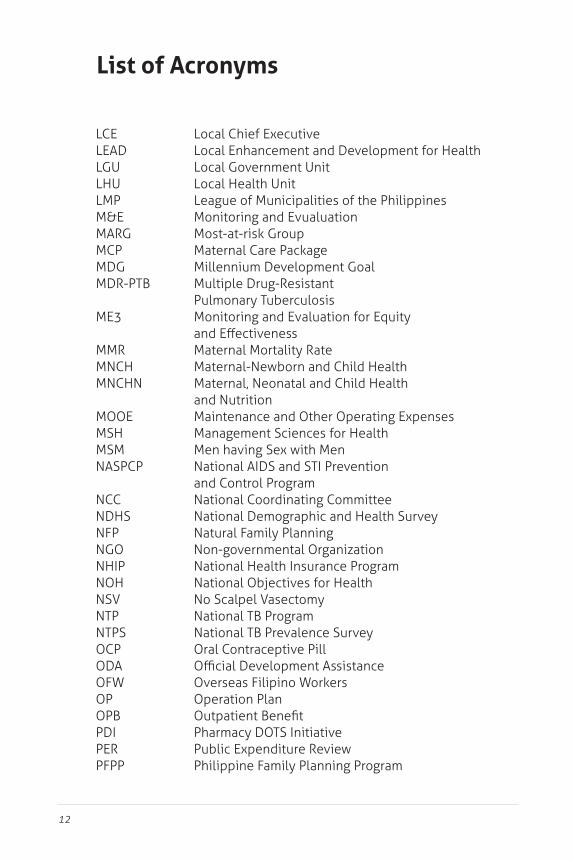
List of Acronyms

11
DOLEDOTS
DSSM
ECCECCD
EO
HACTHARHHRHPDPHRGHSSICICSIDUIECILHZIPGIPHOIRAITNIUDJACKfWLAC
Department of Labor and EmploymentDirectly Observed Treatment Short CourseDirect Sputum Smear Microscopy
Early Childhood Care and Development Program
Human Health ResourcesHealth Policy Development Program
Injectable ContraceptiveIntegrated Communication StrategyInjecting Drug UserInformation Education CommunicationInter-Local Health ZoneInvestment Plan Goal
Internal Revenue Allotment
Intrauterine DeviceJoint Appraisal CommitteeKreditanstalt fur WiederaufbauLocal AIDS Council
12
LCELEADLGULHULMPM&EMARGMCPMDG
ME3
MMRMNCHMNCHN
MOOEMSHMSMNASPCP
NCCNDHS
NGONHIPNOH
NTPNTPSOCPODA
OP
PDIPER
Local Enhancement and Development for HealthLocal Government UnitLocal Health UnitLeague of Municipalities of the PhilippinesMonitoring and Evualuation
Millennium Development GoalMultiple Drug-Resistant Pulmonary TuberculosisMonitoring and Evaluation for Equity
Maternal Mortality RateMaternal-Newborn and Child HealthMaternal, Neonatal and Child Health and Nutrition
Management Sciences for Health
National AIDS and STI Prevention and Control ProgramNational Coordinating CommitteeNational Demographic and Health Survey
Non-governmental OrganizationNational Health Insurance ProgramNational Objectives for Health
Oral Contraceptive Pill
Operation Plan
Pharmacy DOTS Initiative
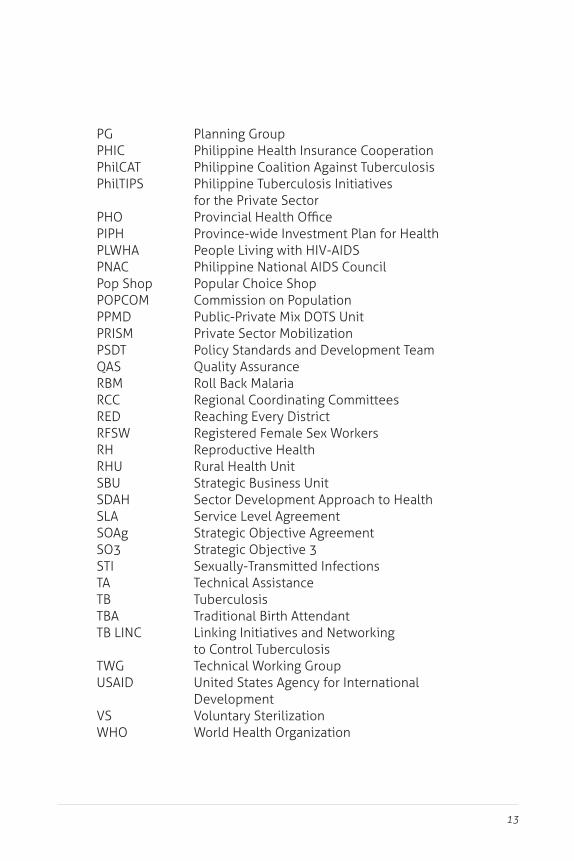
List of Acronyms
13
PGPHICPhilCATPhilTIPS
PHOPIPHPLWHAPNACPop ShopPOPCOMPPMDPRISMPSDTQAS
RCCRED
RHRHU
SDAHSLASOAgSO3STITA
TWGUSAID
WHO
Planning GroupPhilippine Health Insurance CooperationPhilippine Coalition Against TuberculosisPhilippine Tuberculosis Initiatives for the Private Sector
Province-wide Investment Plan for Health
Philippine National AIDS CouncilPopular Choice ShopCommission on Population
Private Sector MobilizationPolicy Standards and Development TeamQuality Assurance
Regional Coordinating CommitteesReaching Every District
Reproductive HealthRural Health Unit
Sector Development Approach to HealthService Level AgreementStrategic Objective AgreementStrategic Objective 3
Technical AssistanceTuberculosis
to Control Tuberculosis
United States Agency for International Development
World Health Organization

14 Mapping the Policy Environment for Family Health
EDITORIAL OVERVIEW:
Mapping the Policy Enviroment for Family Health
The Health Policy Development Program (HPDP) through
scans to assess the policy environment on family health as they relate to the USAID Strategic Objective 31 (SO3) and the National Objectives for Health.
policy recommendations drawn from the 29 policy scans that
family health:
1 On September 27, 2006, the United States Agency for International Development (USAID) and the DOH entered into a Strategic Objective Agreement
Achieved”. Under the agreement, the USAID shall provide grants to support the
health sector reforms in the Philippines for the medium term covering 2005 to 2010. The HPDP, as a USAID partner agency, shall assist in “instituting supportive policies or guidelines both at the national and local levels required to achieve SO3 (Intermediate Result 4)”.
15
The scans aimed to provide a brief assessment of the development or implementation of priority health policy reforms, both at the national and local levels, to guide not only the HPDP but the Department of Health (DOH) and development partners in determining the appropriate actions for improving the policy environment especially on family health.
These policy scans presented long-term or emerging policy issues or trends that impact on the health sector and provided policy-
term health policy amendments and reforms.
the whole process of conducting, reviewing and disseminating the policy scans. It engaged team leaders who guided individual
Space Knowledge Management fora) to assist policy scanners in gathering and validating information for their reports – and in the
the thematic area reports separately developed by the team leaders.
Scan results and policy recommendations from the nine thematic
16 Mapping the Policy Environment for Family Health
“Accelerating Health Improvements in ARMM”
equitable health in the Philippines.
Introduction
entails hurdling challenges brought about by relatively high rates in fertility, morbidity and mortality, a large population, and low socio-economic status. A WHO report (WHO, 2007a) sums up these challenges as follows:
the minimal involvement of the private sector in the delivery
service delivery system, where there is excessive reliance on the use of high-end hospital services rather than primary
health programmes and inadequate resources for public health. “The current workforce is inadequate to meet population health needs, and is inequitably distributed. Migration from rural to urban areas, poor salaries/ wages and lack of incentives, and poor working environments, including shortages of basic medical equipment and supplies, contribute to the worsening of the health worker shortage in rural areas, where health needs are greatest. At the same time, out-migration of health workers, including physicians, nurses and midwives, is a serious problem.”

17
equity of the health system (Department of Health [DOH], 2005c).
national and local levels. There is a need to carry out a careful analysis of these policy gaps and institute measures to will address them (USAID, 2004).
Purpose and Scope
In support of an enhanced health policy development process that will contribute to the sustainable achievement of improved family
Policy Development Program (HPDP) commissioned, from May 2006 to January 2008, a broad and comprehensive scan of the Philippine policy landscape. The policy scans contained an inventory and analysis of policies, laws, guidelines, regulations and issuances on a particular topic or issue relevant to family health.
This volume consolidates the
and other relevant documents to provide an overview of the policy environment for family health.
DEFINITIONS
The health status of the family as a unit including the impact of the health of one member of the family on the family as a unit and on individual family members (Online Medical Dictionary, 1997-2007).
The state of complete physical, mental and social well-being and not merely the absence of disease or
Box 1. and “Health”

18 Mapping the Policy Environment for Family Health
1.
2. Identify policy strengths and enabling factors, gaps and
3.
This volume also intends to provide the DOH and its development partners with a snapshot of the policy circumstances that primarily promote and facilitate the improvement of health care provision
approach. The content of this volume is limited, considering the
the DOH and USAID in their strategic objective agreement.
1. Family planning (FP). The section on family planning presents
An important intervention for improving maternal and child health, and the overall well-being of entire families is to enable individuals and couples to decide freely and responsibly the
International, 2007).
2. Maternal and Neonatal Health. This section introduces
child health and nutrition (MNCHN) consisting of clinical
and governance mechanisms for improving the wellbeing of mothers and children. The aim is the improvement of the health of mothers and newborns and an accelerated reduction in maternal and neonatal deaths.

19
3. Tuberculosis (TB) and HIV/AIDS program. This section
well-being of the family and the community as well.Policies
programs are assessed to identify issues and gaps, and the corresponding recommendations are presented
4. ARMM Health Policy Issues. As the ARMM has consistently
unique administrative and operational challenges this separate chapter on health policy issues in the Autonomous
and presents alternatives for addressing them.
5. F1 Implementation. The last section on cross-cutting issues presents several policy issues related to the implementation
care system, as well as human resources for health, and
that can be addressed feasibly in the medium-term. The reader is encouraged to refer to the individual policy scans for a more

20
1 Eliminating Unmet Need for Family Planning
An important intervention for improving maternal and child health, and the overall well-being of entire families is enabling individuals and couples to decide freely and responsibly on the number, spacing, and timing of their children (Family Health International, 2007). Healthy timing and spacing of pregnancies improve the outcomes of pregnancy and childbirth for both mothers and their children. Harmful outcomes can be avoided if a woman waits at least two years after the birth of a child before becoming pregnant again (Extending Service Delivery Project, 2007). Yet in 2006, the
currently married women who does not want any more children or wants to wait some time before having another child, is not using

Eliminating Unmet Need for Family Planning 21
Trends in Family Planning
from 6 children per woman in the 1970s to 3.5 children per woman
target), coincided with the low contraceptive prevalence rate
the National Objectives for Health (NOH) 2010 CPR target of 80%
6.0
5.2 5.1 4.4
4.1 3.7
3.5
0
1
2
3
4
5
6
7
1973 1978 1983 1986 1993 1998 2003
Chi
ldre
n pe
r wom
an
Years
Figure 1. Trends in Total Fertility Rate, 1973-2003

22 Mapping the Policy Environment for Family Health
every 100 married women used modern family planning methods.2 The pill remained the most preferred method of contraception (16.6%), followed by ligation or female sterilization (10.4%), withdrawal (7.3%), calendar method (7%), and intrauterine
which include mucus/billing/ovulation, Lactational Amenorrhea
2.9 10.7
17.2
18.9
21.6
24.9
28.2 33.4 35.8
12.5 6.7
21.3
13.1
14.5
15.1
18.3
15.5
14.8
0
10
20
30
40
50
60
1968 NDHS
1978 NDS
1978 RPFS
1983 NDS
1988 NDS
1993 NDS
1998 NDHS
2003 NDHS
2006 FPS
Perc
ent
Years
and
Sources
Traditional Methods Modern Methods
Figure 2. Trends in Total Contraceptive Prevalence Rate, 1968-2006Source: NDS, RPFS & NDHS, Philippines, 1968-2003, 2006 FPS
Eliminating Unmet Need for Family Planning 23
(58.6%), Southern Mindanao (57.2%), and Northern Mindanao
ARMM had the lowest proportions of users.
standing. Contraceptive use in 2006 was highest among married women aged 35 to 39 years (58.2%), and lowest among those aged 15 to 19 years (23.3%). Married women with some
with higher level of education. Those with no education were the
poor households (52.4%was higher than among those belonging to poor households (47.3 %) (NSO, 2007).
CURRENT POLICY INITIATIVES: Enabling and Supporting Factors
Contraceptive Self-Reliance Strategy
being a demographically-driven program in the 1970s to one that
planning, thereby enabling couples to achieve their desired number and spacing of children (Taguiwalo, 2007). Historically, the program has been highly dependent on donated
in securing contraceptive supplies for the country (L. Alcantara, 2007). This weaning from dependence on donor agencies for contraceptives is in response to the phase-down of contraceptive donations. Donated condoms were gradually phased out during

24 Mapping the Policy Environment for Family Health
the years 2003-2007. Injectable donations, gradually reduced in 2005, were completely phased out in 2008. Meanwhile, IUD donations ended between 2007 and 2008.
In preparation for the imminent phase-out of foreign-donated contraceptive commodities, the DOH issued Administrative Order 158 to guide local governments in implementing a Contraceptive Self-Reliance (CSR) strategy. The CSR strategy is “a set of
to be provided for increasing numbers of current and potential
directions (L. Alcantara, 2007):
1. Assure no disruption in the provision of contraceptive
2. procurement through a variety of options (PhilHealth,
3.
supplies through self-help community-based distribution, non-governmental organization (NGO) outlets, private and
Local Government Response to CSR 3
Administrative Order (AO) 158 encourages local governments to provide the poor with priority access to subsidized contraceptives,
contraceptives. In a country where half the population subsists on less than US $2 a day and amidst scarce government resources,

Eliminating Unmet Need for Family Planning 25
subsidies to the poorest.
Complementing this public sector strategy, commercial suppliers,
incentive to promote a broader range of products to capture
address the contraceptive phase-down, LGUs are encouraged to:
1. Develop contraceptive distribution guidelines to cover their catchment cities, municipalities and devolved
2. Conduct campaigns to inform their catchment areas of
3. Provide resources for the delivery of contraceptives to
4. contraceptives through:
(i) contraceptives for free distribution.
(ii) Sale of contraceptives at cost recovery basis or at margins above cost.
(iii) Authorization of consigned supplies from social
made available to clients in LGU outlets.
Some LGUs, especially those involved in the Management
Health (MSH LEAD) project, responded to the situation by passing a resolution supporting the National Directorate Resolution No. 009-2004 of the League of Municipalities of the Philippines (LMP). The resolution pushed for the implementation of the
municipalities to do the same.

26 Mapping the Policy Environment for Family Health
the “Kung Maliit ang Pamilya, Kayang-Kaya” (KMPKK) campaign during its National General Assembly in December 2004. It started as an advocacy on CSR that eventually turned into a full-blown program distributing low-cost, quality commodities to selected poor municipalities. The program was launched in 12 LMP
of 14 Chapters, Southern Cotabato and Eastern Samar were also
responses were:
Seven out of ten non-ARMM LGUs in the MSH LEAD project were in various stages of CSR+4 implementation by April 2006.
5
allowed 17 of 29 provinces engaged by LEAD to acquire a signed or approved CSR policy logistics guidelines and have trainers for the revised Contraceptive Distribution Logistics and Management Information System (CDLMIS). As of June 29, 2006,
Technical assistance (TA) was provided through a series of
of contraceptive self-reliance.

Eliminating Unmet Need for Family Planning 27
Other enabling factors that can help facilitate CSR implementation in the country are found in the table below:
Other Enabling Factors for CSR Implementation
Templates for guidelines, modules, and
These were developed in projects, that may be adopted for CSR such as the CSR logistics
an improved CDLMIS, cost-recovery and client-referral systems, training modules on forecasting
and service delivery options
Advocacy groups for CSR
These should be operating at national and local
Commercial or private sector initiatives
model of DKT 6
the revenues are used to buy more products – an

28 Mapping the Policy Environment for Family Health
Growing Involvement of the Private Sector
condoms from the public to the private sector. More women acquired OCPs from the private sector in 2006 (56.6%) than in 2005 (46.5) .Eight out of ten women accessed condoms from the private sector in 2005, compared to seven out of ten the previous year (NSO, 2007).
collaboration. Increased private sector participation is noted
with DKT for the supply of pills to its health facilities. Latest sales
an increase in sales of various brands of OCPs and injectables.
grew 38,4% and sales increased by 26.7% (L. Alcantara, 2007).
A 2005 assessment found substantial recent and ongoing male involvement activities in family planning, which encompassed research, policy guidelines, information education communication
are supported by an enabling DOH policy, which recognizes that involvement of men as critical to the success of reproductive health programs. Such policy is embodied in the DOH AO No. 2006-0035:
involvement in reproductive health (DOH, 2006a).
Eliminating Unmet Need for Family Planning 29
POLICY ISSUES: Gaps, Challenges and Opportunities
Persistent Need for Better Contraceptive Information and Accessibility
one contraceptive method (NSO, 2003a). However, this nearly
by a relatively low CPR. Contributing factors may include barriers
information or misinformation, and poor service quality. One study
distant location of family planning services, and cost. Three out of four women with unmet need for family planning have
pregnancy or when to use contraceptives. Such responses highlight the need for better education and counseling on contraceptives,
informed about the advantages of the methods and their potential
(Commission on Population, 2000).
There is also a need to address the full range of unmet demand for
have been fully supportive of informed choice primarily because it
other methods, availability of supplies at service delivery points has
voluntarily and without coercion, the method most appropriate for them from a range of choices that include both natural and
to clients. Most methods included in the menu usually did not
30 Mapping the Policy Environment for Family Health
long-term permanent methods (voluntary surgical sterilization
the local CSR response (Raterta, 2008b).
Higher Unmet Need for Family Planning Among the Poor and Hard-to-Reach Population Sectors
Poor women, on the average, have more unintended pregnancies
the Philippines, the poor have around two more children than they want, according to the 2003 National Demographic Health Survey (NDHS) (NSO, 2003a). In 2006, married women in the poor sector had a greater unmet need for family planning (20.3%), compared to their non-poor married counterparts. Without increasing access to modern contraception among the poor, intergenerational cycles of poverty will continue (Allen, 2007).
private sector in four out of ten cases. (NSO, 2006)
AO 158 encourages LGUs to adopt a segmentation strategy to
the poor from the non-poor (L. Alcantara, 2007).
Eliminating Unmet Need for Family Planning 31
Lack of LGU Capacity to Manage and Implement CSR
of the LGUs to operationalize it in their respective localities. In a
varied as the number of LGUs, and have largely been dictated by ongoing or past foreign-funded projects.” This is not surprising
of the CSR process (Raterta, 2008b). This is compounded by the
To date, there are still a number of LGUs that need to be oriented on
strengthen LGU capacity, the DOH still needs to provide technical assistance, especially in procurement, warehousing, resource mobilization, forecasting, collection, and fund management. The DOH also needs to standardize all operational policies,
timely and adequate information on CSR implementation by LGUs.
Limited Private Sector Participation in FP Service Delivery and Supply of Commodities
The public sector continues to dominate the family planning
and NGO sector participation, if only to increase the choices available to users who used to receive free public sector services
requirements, LGUs should increase private sector participation

32 Mapping the Policy Environment for Family Health
However, one survey (Hartigan-Go 2007) has shown that the private commercial sector had very low awareness of CSR and
Oral and injectable contraceptives (OCs and ICs), two of the essential commodities supplied by the drug industry, are not
Philippines is estimated to be worth only P 50 million (0.5% of total pharmaceutical sales), these drugs are not being promoted among doctors with the same same degree of aggressiveness as other medicinal products (Hartigan-Go, 2007). In addition,
aggressively pursue hormonal contraceptive sales (Raterta, 2008b).
Evidence suggests that the private sector has an important role to play in producing and delivering contraceptives and condoms
LGUs must, however, put in place necessary enabling policies and regulatory conditions to spur private sector participation in
sector is to demonstrate that the LGU is committed to provide the
their products and services (Raterta, 2008b).
Cost Issues and Funds Availability
According to the 2000 State of the Philippine Population Report, unmet need of women stems largely from high costs associated
system. These costs deter women from availing themselves of family planning methods. This argument is validated in the scan
2008b) The report cited the cost of accessing health care as a

Eliminating Unmet Need for Family Planning 33
need. Another reason is productivity cost, or the possible loss of
Aside from the passage of a resolution, only a few LGUs have
supply reduction brought about by the phase out. The Commission on Population (POPCOM) estimates that between 30% to 35% of LGUs have so far allocated a budget line item to purchase modern contraceptives. Many of the LGUs, which are committed
that they need more funding from the national government, which is generally unavailable. Most, therefore, depend heavily on their two main sources of revenue – the internal revenue
to 90% of local income (L. Alcantara, 2007).
The IRA is a major source of revenue for most LGUs with an approved budget. In an interview with the Philippine Center for Investigative Journalism (2007), Senator Aquilino Pimentel said
from the phase out. Hence, some LGUs have resorted to various resource-generating activities such as the following:
Equal sharing between the city government and barangay of the 20% social development fund from the IRA (Laoag City)
Use of capitation fund by PhilHealth-accredited
Establishment of popshops, which are franchises that sell various contraceptive products, in health facilities
Mangaldan, Pangasinan).

34 Mapping the Policy Environment for Family Health
fewer tap them. Loan funds provided by the German government through Kreditanstalt fur Wiederaufbau (KfW), for instance, are
Alcantara, 2007). PhilHealth reported a very low utilization rate by LGUs of the capitation fund: only 3% of the 997-million peso
POLICY OPTIONS AND RECOMMENDATIONS
manageable household size, family members get a bigger share of resources to meet individual socio-economic needs, thus contributing to better nutrition, education and health, and fewer maternal and child deaths, and a healthier and more productive population – the engine that spurs economic growth. Given its socio-economic implications, it is critical to address previously
This paper presents the following policy options and recommendations for the DOH, LGUs and other partners to attain
Eliminating Unmet Need for Family Planning 35
DEPARTMENT OF HEALTHFP
PO
LIC
Y T
HR
UST
AN
D IS
SUA
NC
ES
1. Standardization of Operational Policies, Procedures and Guidelines
The DOH needs to standardize all operational policies,
components of the CSR strategy and disseminate the same
2. Strong DOH leadership in FP promotion
FIN
AN
CIN
G
1. Development of Access and Utilization Guidelines
program and its budgetary appropriations from being used for other purposes.
There should be methodology used for assessing LGU implementation of the CSR.
36 Mapping the Policy Environment for Family Health
DEPARTMENT OF HEALTH
FIN
AN
CIN
G
Cooperation with PhilHealth should be solicited in the
There should be advocacy for continued coverage of
Information dissemination should be done for the utilization of PhilHealth services.
3. Appropriate categorization of LGUs and Criteria Set for FP Assistance
The DOH should categorize its LGUs into poor and non-poor,
The criteria must not pose restrictions to access by LGUs
Programs.
realize desired family size of their constituents.
The DOH and other partners should provide support in terms of:
(1) (2) (3)
(4) revision of the present IRA formula to include minimum
(5) media advocacy for the inclusion of population issues in the priority public agenda.

Eliminating Unmet Need for Family Planning 37
DEPARTMENT OF HEALTHFI
NA
NC
ING
5. Consolidation of public sector procurement of FP commodities and supplies.
This entails pooling orders (possibly at provincial level) to avail of big volume discounts. At the national level, the DOH
ensure that concerned foreign funded projects provide
the contraceptive phase down plan. It may serve as the focal unit for disseminating information on available health funding sources for LGUs.
FP S
ERV
ICE
UTI
LIZA
TIO
N A
ND
PRO
VIS
ION
1. Demand for reproducting health care through public education.
The DOH and partners should create demand for reproductive health care through public education. The promotion of RH education, possibly in coordination with the Department of Education (DepEd), would raise RH awareness and enhance demand for RH services.
However, this remains a challenge especially since DepEd has made it clear during the Strategic Planning of Philippine
was not its priority.
2. Rethinking Family Planning Methods
under the NDHS. The needs of the young and those nearing

38 Mapping the Policy Environment for Family Health
DEPARTMENT OF HEALTH
FP S
ERV
ICE
UTI
LIZA
TIO
N A
ND
PRO
VIS
ION
3. Training of FP service providers
a monitoring and evaluation (M&E) system for the provision of
4. Mapping of FP service providers
sector) is needed to determine their appropriate roles and
(a)
(b)
(c)
deliberate displacement of NGOs and other competitors
to entice service providers to prescribe a particular contraceptive brand, should be discouraged).
Eliminating Unmet Need for Family Planning 39
DEPARTMENT OF HEALTHFP
SER
VIC
E U
TILI
ZATI
ON
AN
D P
ROV
ISIO
N
5. Creation of a positive policy environment for the commercial sector
The DOH should provide a policy environment conducive to
comprehensive and acceptable CSR approach with government agencies.
dialogues between public and private sectors, including donors, to clarify their strategic roles in CSR.
equally important to clarify the roles of international donors
sector programs.
6. Targetting the poor and hard-to-reach population sectors
The DOH and partners should continue to target the poor and hard-to-reach population. Guidelines in identifying the poor, encouraging the provision of quality services to the underserved population, and allowing for cost recovery without prejudice to the poor should continue to be implemented and enhanced.
40 Mapping the Policy Environment for Family Health
LOCAL GOVERNMENT UNITS (LGUs)
FIN
AN
CIN
G
1. Financial and Technical Assistance
strategies and implementation. (ARMM is dependent on
2. Activities for Unmet FP Need
LGUs should introduce a range of activities to holistically
Activities may:
(1) involve the private sector as partner in planning, policy-
(2)
(3) allow private-sector promotion and distribution of
(4)
(5)

Eliminating Unmet Need for Family Planning 41
LOCAL GOVERNMENT UNITS (LGUs)FP
SER
VIC
E U
TILI
ZATI
ON
AN
D P
ROV
ISIO
N
corresponding to the needs of their constituents. LGUs must
and marginalized.
for those who wish to limit their families.
PHILHEALTH
NAT
ION
AL
HEA
LTH
INSU
RA
NC
E PR
OG
RA
M (N
HIP
)
Increased NHIP funding for FP
Intervention is required to clarify misconceptions on the use of capitation funds.
Performance-based budgeting should be introduced, whereby budget releases to LGUs will be based on results
42 Mapping the Policy Environment for Family Health
PHILHEALTH
FIN
AN
CIN
G
There should be advocacy for continued coverage of indigents
Information dissemination should be done for the utilization of PhilHealth services.
FP S
ERV
ICE
UTI
LIZA
TIO
N A
ND
PRO
VIS
ION
Information and advocacy activities.
activities (as in the case of ARMM) and initiatives. This strategy usually results in buy-in and LCE support for the
using contraceptives.

43
2 Improving Maternal and Child Health
before the 1990s. Yet too many mothers and children still die or
health care (WHO, 2005). This is especially true in the Philippines where approximately 4,000 mothers die each year due to pregnancy complications (DOH, 2008b), and almost 8,000 newborns die annually (BASICS II, 2004).
The Philippines has committed itself to improving maternal health through the reduction of its the maternal mortality ratio (MMR) by
(Villaverde et al., 2005).
44 Mapping the Policy Environment for Family Health
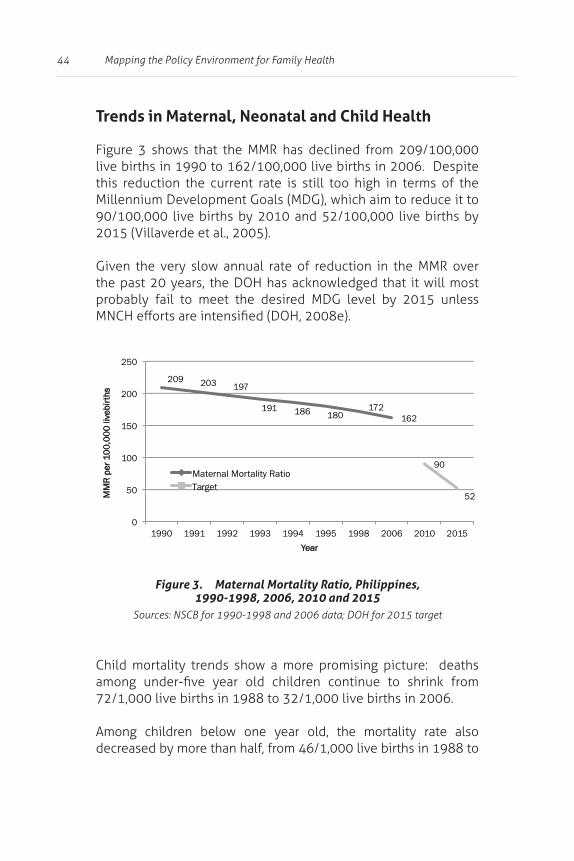
Trends in Maternal, Neonatal and Child Health
live births in 1990 to 162/100,000 live births in 2006. Despite this reduction the current rate is still too high in terms of the Millennium Development Goals (MDG), which aim to reduce it to 90/100,000 live births by 2010 and 52/100,000 live births by
Given the very slow annual rate of reduction in the MMR over
probably fail to meet the desired MDG level by 2015 unless
Child mortality trends show a more promising picture: deaths
72/1,000 live births in 1988 to 32/1,000 live births in 2006.
Among children below one year old, the mortality rate also decreased by more than half, from 46/1,000 live births in 1988 to
Figure 3. Maternal Mortality Ratio, Philippines, 1990-1998, 2006, 2010 and 2015
209 203 197
191 186 180 172
162
90
52
0
50
100
150
200
250
1990 1991 1992 1993 1994 1995 1998 2006 2010 2015
MM
R pe
r 10
0,00
0 liv
e birt
hs
Year
Maternal Mortality Ratio Target
Improving Maternal and Child Health 45
24/1,000 live births in 2006. Given this rate of decline, achieving
probable. However, the pace of reduction has slowed down in the
very slow decline in neonatal and post-neonatal deaths (DOH,
Geographic disparities in maternal-newborn and child health
and sub-regional levels. The best- and worst-performing provinces vary according to the health indicator used (DOH, 2008b). Data also show that maternal, newborn and child health
and socioeconomic characteristics. Childhood death rates are higher among male children and among mothers who gave birth at age below 20 and 40 years old and older, and among children with birth orders fourth and up.
Children born less than 2 years apart are almost twice as
between one to four years old born to poorest mothers are 21
who are one to 11 months old (post neonates) born to poorest
counterparts. (NSO, 2003a).

46 Mapping the Policy Environment for Family Health
CURRENT POLICY INITIATIVES: Enabling and Supporting Factors
Broad-based legislative support for child health
in place. Among these is the Early Childhood Development Act of 2000, which mandates the provision of overall care and
Order (EO) 286 directs all national government agencies and other partner institutions to actively support and implement programs for children aged zero to 17 years, and initially cover 100 nutritionally-depressed municipalities in the country.
Development and Protection of Children Act, was passed to defend the right of children to assistance, including proper care and
and other conditions prejudicial to their development. It mandates every barangay to institute a day care center with a program that includes immunization, growth and nutritional monitoring, care of
Other notable forms of legislative support relevant to child
Development for Children, 2000-2025 (Child 21), Early Childhood
A relatively mature Child Survival (CS) strategy is also in place. It pursues 5 directions7 to meet MDG 4 (Reduce child mortality) by

Improving Maternal and Child Health 47
2015. The strategy centers on upgrading the capacities of health
interventions8
population. It aims to move LGUs forward to be truly accountable to their mandate in delivering basic services, step up community
Recent Shift from “Risk Approach” to an “Emergency Obstetric and Neonatal Approach”
Among the direct causes of maternal deaths are severe bleeding (hemorrhage), infection (sepsis), unsafe abortion, pregnancy-induced hypertension (eclampsia) and obstructed labor. Most of maternal deaths occur during or within 24 hours after childbirth. In particular, complications such as hemorrhage, hypertension and obstructed labor cannot be predicted or prevented.
Majority of neonatal deaths are due to prematurity, sepsis,
from obstetric emergencies. Half of neonatal deaths occur during
supply and sanitary toilets, personal and domestic hygiene in areas with least access to sanitation facilities

48 Mapping the Policy Environment for Family Health
an “emergency obstetric and neonatal approach” in pregnancy
and Safe Motherhood Project (WHSMP2), considers all pregnant
in pregnancy, including delivery by a midwife, nurse or doctor, as well as emergency treatment for all complications during pregnancy, delivery and after birth, postpartum family planning,
and calls for the following:
1. Provision and use of integrated MNCHN services consisting of clinical interventions that address the direct causes of mortality, and public health services
2. Enforcement of regulatory measures and guidelines on
the establishment and operations of health facilities and
3. available instruments through DOH and LGU budgets,
4. Establishment of governance mechanisms that secure
2008e).
Improving Maternal and Child Health 49
Opportunities for Service Quality Upgrading through Capacity Building
Competencies of service providers on MNCH service delivery should be continuously developed and enhanced through the provision of guides, standards, protocols and training on MNCH. These materials include, among others, the following (G. Alcantara et al., 2008).
Enhanced Clinic Practice Guides Community Maternal Newborn Clinical Practice GuidelinesMaternal Death Review Guide
Innovative Service Strategies and Facility Expansion /Upgrading for MNCH Service Delivery
Adoption of the following innovative service strategies and approaches has improved coverage and reach of MNCH interventions:
(1) adoption of the Reaching Every District (RED) strategy,
malls, and schools which improved access and utilization
(3) encouragement of active involvement of the private

50 Mapping the Policy Environment for Family Health
Other accomplishments towards improved coverage of MNCH
increasing the number of lying-in and birthing homes/clinics being put up and accredited for the Maternal
accreditation of several health facilities under Sentrong
authorization of hospitals as centers of mother-baby
9 (Marilyn Noval-Gorra, 2007b)
services, including prenatal care, normal delivery, postpartum care and family planning counseling. Instead of the usual itemized payment of services rendered, the MCP uses a case-based
(e.g. midwives or physicians) should have PhilHealth accreditation for their patients to be able to avail of the MCP.
strategy should ideally lead to a greater number of women going for professionally-attended delivery. Complemented with the PhilHealth
9 This section draws heavily from the policy scan by Noval-Gorra (2007b)

Improving Maternal and Child Health 51
POLICY ISSUES: Gaps, Challenges and Opportunities
Geographic and Socioeconomic Disparities in MNCH
One of the factors that may have contributed to wide variations in maternal and child health indicators across the country is the
the political will and commitment to support it.
of maternal and newborn health, there is generally poor
(a) (b) (c) poor coordination among agencies involved
(d) (e) (f) (g) non-translation of MNCH laws into local
resolutions or ordinances
Wide variations across regions and socio-economic groups mean that rapid mortality reduction through a prescriptive
neonatal health interventions must then be focused on areas/
priority areas/groups will require especially-tailored health messages and approaches. LGUs must be given the necessary technical assistance to support the implementation of MNCHN interventions. National standards in increasing the demand for quality MNCHN services can be set to guide local adaptations

52 Mapping the Policy Environment for Family Health
Limited Quality, Accessibility and Sustainability of MNCH Services
address the direct causes and intermediate precursors of maternal-newborn and child deaths, their scope and coverage remain low. Mothers and neonates have limited access to emergency obstetric and neonatal care during delivery, as there are few health facilities
In addition, while lying-in/birthing homes continue to sprout all
for MCP) and to guide rationalization of their location, coverage
Low Utilization of MNCHN Services and Continued Preference for Home-based Deliveries 10
Key program indicators point to low utilization of MNCHN services: only seven out of ten pregnant women had at least three or four prenatal care visits, compared to the 2010 target of nine out of
and only 69.8% of children are fully immunized compared with the program target of 95%.
The health of mothers and children is negated by three delays: (1) (2) delay in reaching appropriate care, and (3) delay in receiving care. These are mainly due to
health care, psychological and social concerns and fears, limited
geographical/physical barriers to accessing health care.

Improving Maternal and Child Health 53
Most women prefer to deliver at home because it allows family
the hospital when women are often left on their own. It also gives
home childbirth still lets them watch over their other children. Moreover, delivering at home does not subject them to the
Inadequate Financing Mechanisms
to cover the cost of maternity care, which is currently estimated
and technologies for maternity care. The addition of the P
are now way below the true cost of service delivery and provision (Noval-Gorra, 2007).
following elements:
free access to the health system through several means (e.g., minimal-to-zero copayment, cash transfer for
incentives for institutional and individual providers, both in the public and private sectors (e.g., PhilHealth
54 Mapping the Policy Environment for Family Health
reimbursement share, performance-based incentives, shares in user fees for paying clients, and facility
incentives for local government participation (e.g. PhilHealth capitation fund, DOH grants).
POLICY OPTIONS AND RECOMMENDATIONS
health. Data further suggest a correlation a high maternal
need to integrate maternal and child health services and allow
Ensuring universal access of mothers and their neonates to the
equitable life-saving services for mothers and children in a catchment population. Each service area should be customized to the needs of the locality, and there must be adequate personnel to deliver
supplemented with a localized, targeted communication tool to
and accessible” and empower mothers to routinely choose the best facility for delivery.

Improving Maternal and Child Health 55
Due to inadequate resources, targeting low-performing areas can be prioritized. Instituting a performance-based grant
ensure quality outcomes, considering that the health system
also recommended. A performance-based grant mechanism may
system.
deserve national attention. Questions on the quantity and quality

56
3 Achieving Public Health Control of Tuberculosis
Tuberculosis (TB) is a disease that spreads across all age groups (Grimard & Harling, 2004), and impacts not only the health of the
(NSO, 2008). It was also the 6th leading cause of morbidity with 169.9 cases per 100,000 population in 2006 (Department of Health, 2006b). Globally, the Philippines ranks ninth among 22
estimated number of new TB cases (all forms) arising worldwide each year (WHO, 2007b).
Achieving Public Health Control of Tuberculosis 57
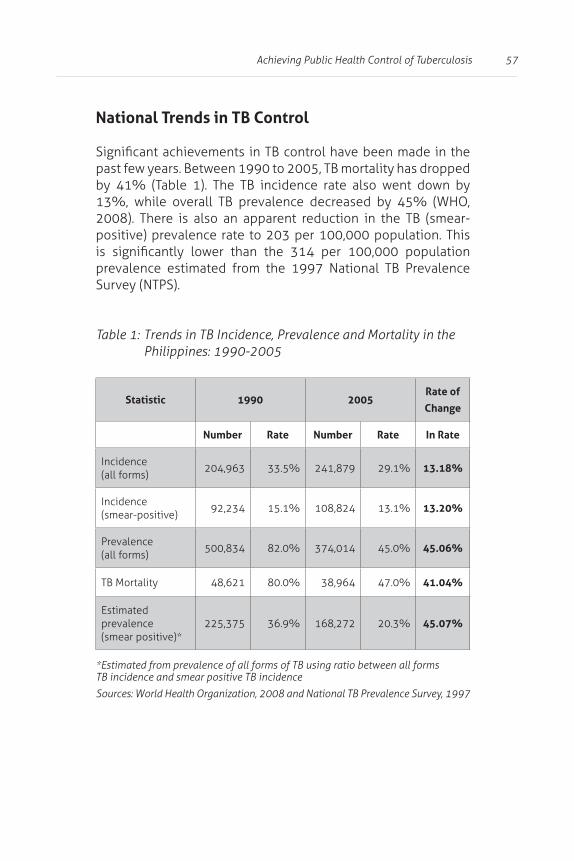
National Trends in TB Control
positive) prevalence rate to 203 per 100,000 population. This
Survey (NTPS).
Trends in TB Incidence, Prevalence and Mortality in the
Statistic 1990 2005Rate of
Change
Number Rate Number Rate In Rate
Incidence (all forms)
204,963 33.5% 241,879 29.1% 13.18%
Incidence (smear-positive)
92,234 15.1% 108,824 13.1% 13.20%
Prevalence (all forms)
500,834 82.0% 374,014 45.0% 45.06%
48,621 80.0% 38,964 47.0% 41.04%
Estimated prevalence (smear positive)*
225,375 36.9% 168,272 20.3% 45.07%
*Estimated from prevalence of all forms of TB using ratio between all forms TB incidence and smear positive TB incidence
58 Mapping the Policy Environment for Family Health
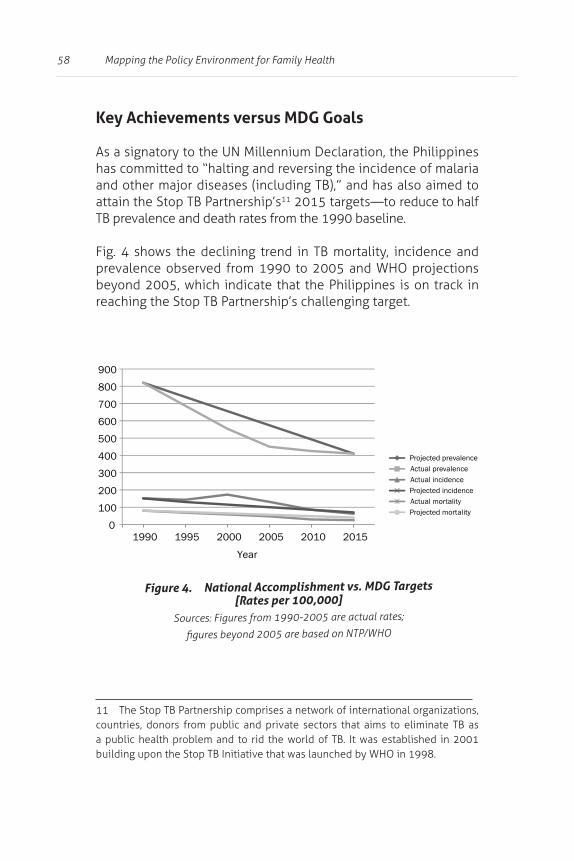
Key Achievements versus MDG Goals
As a signatory to the UN Millennium Declaration, the Philippines has committed to “halting and reversing the incidence of malaria
11
prevalence observed from 1990 to 2005 and WHO projections
Figure 4. National Accomplishment vs. MDG Targets [Rates per 100,000]
Projected prevalence Actual prevalence Actual incidence Projected incidence Actual mortality
Projected mortality
0
100
200
300
400
500
600
700
800
900
1990 1995 2000 2005 2010 2015
Year
Achieving Public Health Control of Tuberculosis 59
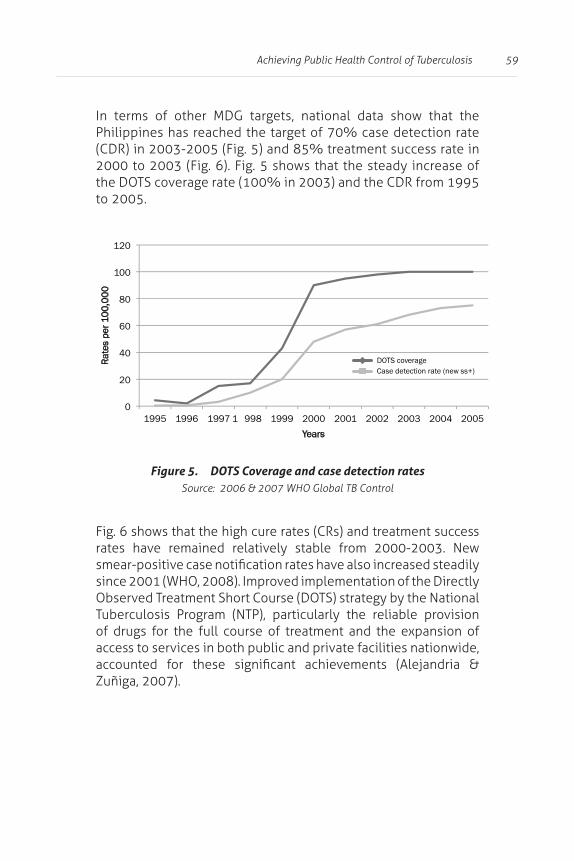
In terms of other MDG targets, national data show that the Philippines has reached the target of 70% case detection rate
the DOTS coverage rate (100% in 2003) and the CDR from 1995 to 2005.
rates have remained relatively stable from 2000-2003. New
since 2001 (WHO, 2008). Improved implementation of the Directly Observed Treatment Short Course (DOTS) strategy by the National Tuberculosis Program (NTP), particularly the reliable provision
access to services in both public and private facilities nationwide,
Zuñiga, 2007).
Figure 5. DOTS Coverage and case detection rates
0
20
40
60
80
100
120
1995 1996 1997 1 998 1999 2000 2001 2002 2003 2004 2005
Rate
s
per 10
0 ,0 0
0
Years
DOTS coverage Case detection rate (new ss+)

60 Mapping the Policy Environment for Family Health
are quite impressive, there is a need to determine whether these
levels. Data collected for the operational plan (OP) indicators show
cases across regions and provinces (see Table 2).
Figure 6. Cure rates and treatment success rates
73 75 77 81
88 88 88 88
0 10
20 30 40 50 60 70 80 90
100
2000 2001
2002 2003
Perc
ent
Years
Cure Rate Treatment Success Rate
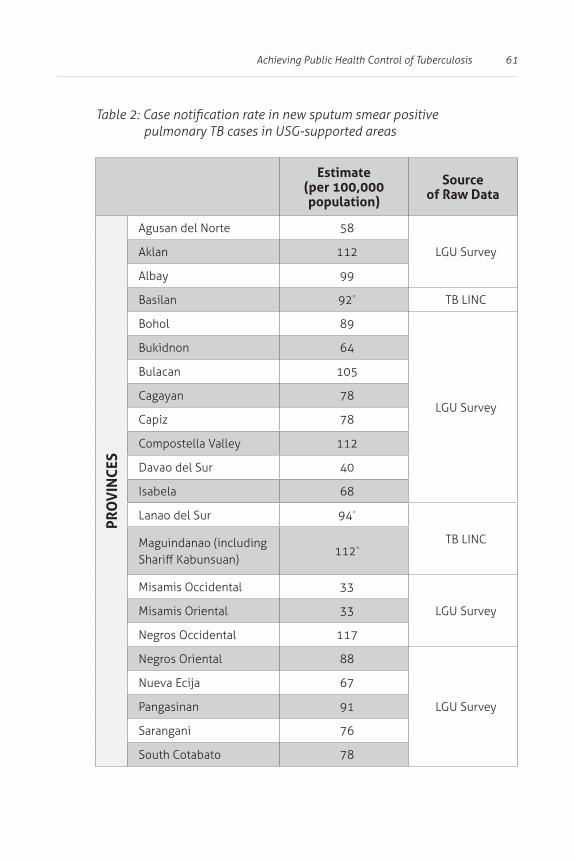
Achieving Public Health Control of Tuberculosis 61
pulmonary TB cases in USG-supported areas
Estimate(per 100,000 population)
Source of Raw Data
PRO
VIN
CES
Agusan del Norte 58
LGU Survey112
Albay 99
92*
89
LGU Survey
64
105
Cagayan 78
Capiz 78
112
Davao del Sur 40
Isabela 68
Lanao del Sur 94*
Maguindanao (including 112*
Misamis Occidental 33
LGU SurveyMisamis Oriental 33
Negros Occidental 117
Negros Oriental 88
LGU Survey
Nueva Ecija 67
Pangasinan 91
Sarangani 76
South Cotabato 78

62 Mapping the Policy Environment for Family Health
Estimate(per 100,000 population)
Source of Raw Data
PRO
VIN
CES
Sulu 82*
Tarlac 47 LGU Survey
Tawi-tawi 99*
Zamboanga del Norte 76
LGU SurveyZamboanga del Sur 74
Zamboanga Sibugay 20
CIT
IES Quezon City 79
LGU SurveyZamboanga City 86
Shaded cells can be used as baseline estimates. *Estimates provided by TB LINC12
case detection rate and cure rate using 2006 NTP data. Provinces
while those with low CDR and low CR are categorized as “low performers”. There are also provinces with high CDR and low CR, or low CDR and high CR. Each of the four groups poses unique
public and private sectors.

Achieving Public Health Control of Tuberculosis 63
Figure 7. Case Detection and Cure Rates of High-Performing Provinces and Low-Performing Provinces

64 Mapping the Policy Environment for Family Health
age groups 35 to 64 years old. The unequal distribution among
investigation and possibly targeting of interventions to reach
Age group and
Gender0–14 15–24 25–34 35–44 45–54 55–64 65+
Male (cases)
482 7,358 11,275 13,253 12,531 7,646 4,279
Male (rate per 100,000
3 86 170 273 370 379 299
374 3,710 5,268 5,565 4,603 3,274 2,029
(rate per 100,000
3 45 81 115 132 157 113
856 11,068 16,543 18,818 17,134 10,920 6,308
(rate per 100,000
3 66 126 194 249 266 196
Achieving Public Health Control of Tuberculosis 65
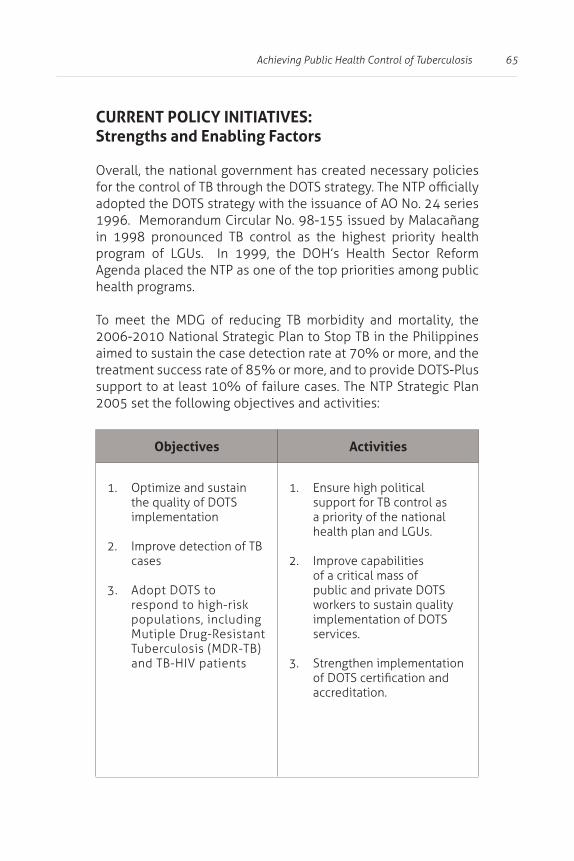
CURRENT POLICY INITIATIVES: Strengths and Enabling Factors
Overall, the national government has created necessary policies
adopted the DOTS strategy with the issuance of AO No. 24 series 1996. Memorandum Circular No. 98-155 issued by Malacañang
Agenda placed the NTP as one of the top priorities among public health programs.
aimed to sustain the case detection rate at 70% or more, and the treatment success rate of 85% or more, and to provide DOTS-Plus support to at least 10% of failure cases. The NTP Strategic Plan 2005 set the following objectives and activities:
Objectives Activities
1. Optimize and sustain the quality of DOTS implementation
2. cases
3. Adopt DOTS to
populations, including Mutiple Drug-Resistant
1. Ensure high political
a priority of the national health plan and LGUs.
2. Improve capabilities of a critical mass of public and private DOTS
implementation of DOTS services.
3. Strengthen implementation
accreditation.

66 Mapping the Policy Environment for Family Health
Objectives Activities
4. management functions, particularly monitoring and evaluation of NTP-DOTS implementation.
5. Intensify and enhance
(PPMDs) in strategic sites.
6. Strengthen collaboration between public hospitals and health centers to increase access to, and improve
7. (+) initiatives and institutionalize these in the public sector.
8. Strengthen integration of
In March 2003, the government released EO 187, which announced the partnership between the DOH and the Philippine
Developed by the DOH and PhilCAT, together with other government agencies and the private sector, the CUP adopted
the enabling environment for public-private partnership in this endeavour (Alejandria and Zuniga 2007).
Achieving Public Health Control of Tuberculosis 67
TB Control
In response to EO 187, the Department of Labor and Employment (DOLE) issued Department Order No. 73-05 (“Guidelines for the Implementation of Policy and Program on Tuberculosis Prevention
his family to either a public or a private DOTS unit. Appropriate
(ECC), Social Security System (SSS) and PhilHealth should be given (Alejandria & Zuniga, 2007).
Quality Assurance
In April 2007, AO No. 2007-0019 (Guidelines for the Implementation of the Quality Assurance System for Direct Sputum Smear Microscopy) was issued to:
1. guidelines on direct sputum smear microscopy (DSSM),
2. broaden the coverage of QAS to include private laboratories (DOH, 2007).
Public-Private Partnerships
Department Circular No. 104 s. 2004 (on the Adoption of the
68 Mapping the Policy Environment for Family Health
DOH AO No. 154 s. 2004 facilitated the creation of the National
Composed of the DOH, PhilCAT, PHilHealth and PPMD Technical
of the PPMD strategy (Alejandria & Zuniga, 2007).
Financing Package
PhilHealth Circular No.17 s. 2003 provided for the accreditation
to facilitate processing of claims applications for the Outpatient
Circulars No. 19 of May 11, 2003 and No. 36 of October 10, 2003.
payments to the accredited DOTS unit. This fee covers diagnostic
(Alejandria & Zuniga, 2007).

Achieving Public Health Control of Tuberculosis 69
POLICY ISSUES: Gaps, Challenges and Opportunities
Local Variations in TB Control
localities. Some areas get the services they need more than the
challenged to innovate in their implementation strategies (Punsalan, 2007). Local innovations, however, are limited by their
epidemiology does not limit itself to geographic boundaries and political jurisdictions (Solon et al., 2005).
public health control requires a comprehensive understanding
areas sharing the common health threat. This assessment of the
investments to reach the desired level of public health control in the medium term.
In the process of developing investment plans for health,
assistance can come in terms of grants, loans and preferential access to central transfers.
program, a DOH requirement for LGU access to support.
However, there is no clear indication for a locally-customized
of Capiz and Pangasinan. A localized strategy is critical for the development and use of appropriate policies, standards and tools
70 Mapping the Policy Environment for Family Health
locality (Health Policy Development Program, 2007).
(Dagupan City is a chartered city located in Pangasinan).
Inadequate LGU Capacity and Ownership
capacity of some LGUs to come up with an appropriate implementation strategy that factors in coordinated use of
capability of most LGUs to partner and negotiate with other
LGU support, coupled with proactive regional coordinating
other hand, regions with poor performance are those where
equity (Alejandria & Zuniga, 2007).
Achieving Public Health Control of Tuberculosis 71
Inadequate Expansion and Monitoring of DOTS Coverage
While the NTP has achieved 100% coverage, it does not mean it is accessible to all. DOTS may be present in almost all the 3,500 local health centers, but there are centers in many remote areas that are very inaccessible.
The basis for claiming 100% DOTS coverage is questionable since the measure of DOTS coverage is based on readiness of public sector facilities, not accessibility by a catchment population. DOTS readiness in public facilities is mostly limited to the training
facilities. These enhancements, however, may not translate into
because there is a large government sector where health services are also available. This includes the devolved, regional and national hospitals, DepEd, LGUs and the armed forces, among others. Many of them are non-DOTS compliant. In 2005, the CUP attempted to standardize the use of DOTS in this sector despite
Health-Seeking Behavior, Knowledge and Attitudes on TB
public health facilities is also often perceived to be poor and patients anticipate a shortage of drugs and supplies. General
72 Mapping the Policy Environment for Family Health
Limited Private Sector Participation in DOTS13
Philippines has a large private sector composed of private-for-
fragmented and unregulated, the role of the private health sector
Surveys and interviews conducted before the adoption of the
and with great variability in the treatment regimens prescribed by
In the DOH nationwide baseline survey for the national objectives for health, less than half of the private providers were aware of
Dispensing of drugs is largely unregulated, and small retail drug stores and large chains abound in the country. Pharmacists also tend to recommend medications to the consumer. CDRs and CRs
NTP (Alejandria & Zuniga, 2007).
In recognizing the private sector gap in the NTP , several initiatives were designed primarily through the PhilCAT, in coordination with the DOH. These initiatives centered mainly on setting up public-private partnerships through grants from the Center for Disease Control (CDC), USAID-PhilTIPS (Philippine Tuberculosis Initiatives
13 This section draws heavily from the policy scan report by Alejandria and
Achieving Public Health Control of Tuberculosis 73
were piloted and evaluated in the country (private hospital-based, HMO-based, local coalition-, corporate social responsibility- and multi-specialty clinic-based, faith-based, and stand-alone
Despite these improvements, barriers to improving private sector participation still need to be addressed:
(1)
(2)
(3)
(4)
(5)
(6) and
(7) Quality Assurance system of the DOH.
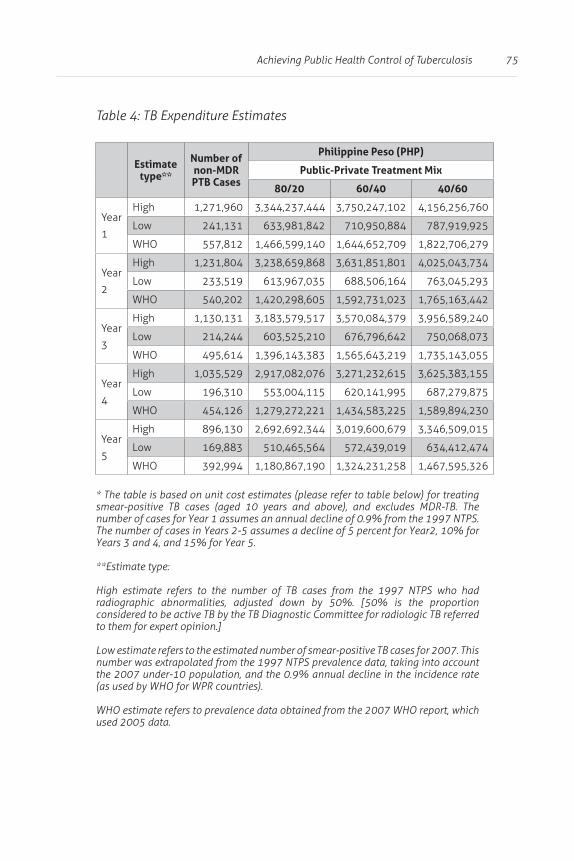
Need for Sustained and Coordinated Financing
Available funding may only reach to a third of what is required by the regular program (refer to Table 4). The cost estimate for drugs, laboratory and DOTS service is around 3.34 billion pesos for non-
Assuming an optimistic decline of 5-15% (using more than 70% CDR and 85% CR), the cost estimate will decrease to 2.69 billion
74 Mapping the Policy Environment for Family Health
the cost estimate for drugs, laboratory and DOTS service is around 1.47 billion pesos.. With the same assumed rates of decline as
Given the decentralized local public health systems, the
(central, local and social health insurance funds) and the
promoting stronger government leadership (Dantes & Llamido-Mortera, 2007).
Tuberculosis, being a public health problem of national
particularly drugs. Drugs constitute the most critical aspect of
economies are actually derived from the centralized government
service level agreements that leverage continued supply as well as corresponding technical assistance with performance in local
Achieving Public Health Control of Tuberculosis 75
TB Expenditure Estimates
Estimate type**
Number of non-MDR PTB Cases
Philippine Peso (PHP)
Public-Private Treatment Mix
80/20 60/40 40/60
1
High 1,271,960 3,344,237,444 3,750,247,102 4,156,256,760
Low 241,131 633,981,842 710,950,884 787,919,925
WHO 557,812 1,466,599,140 1,644,652,709 1,822,706,279
2
High 1,231,804 3,238,659,868 3,631,851,801 4,025,043,734
Low 233,519 613,967,035 688,506,164 763,045,293
WHO 540,202 1,420,298,605 1,592,731,023 1,765,163,442
3
High 1,130,131 3,183,579,517 3,570,084,379 3,956,589,240
Low 214,244 603,525,210 676,796,642 750,068,073
WHO 495,614 1,396,143,383 1,565,643,219 1,735,143,055
4
High 1,035,529 2,917,082,076 3,271,232,615 3,625,383,155
Low 196,310 553,004,115 620,141,995 687,279,875
WHO 454,126 1,279,272,221 1,434,583,225 1,589,894,230
5
High 896,130 2,692,692,344 3,019,600,679 3,346,509,015
Low 169,883 510,465,564 572,439,019 634,412,474
WHO 392,994 1,180,867,190 1,324,231,258 1,467,595,326
* The table is based on unit cost estimates (please refer to table below) for treating smear-positive TB cases (aged 10 years and above), and excludes MDR-TB. The
High estimate refers to the number of TB cases from the 1997 NTPS who had
considered to be active TB by the TB Diagnostic Committee for radiologic TB referred to them for expert opinion.]
Low estimate refers to the estimated number of smear-positive TB cases for 2007. This number was extrapolated from the 1997 NTPS prevalence data, taking into account
(as used by WHO for WPR countries).
WHO estimate refers to prevalence data obtained from the 2007 WHO report, which used 2005 data.
76 Mapping the Policy Environment for Family Health
has the potential to contribute greatly toward addressing
intervention:
1.
2. increase PHIC membership specially among the
3. create a complementary policy environment that favors sustained implementation made feasible by
4.
through better, easier and more patient- as well as provider-friendly mechanisms.
These are critical for PHIC to perform its mandate to provide a
Achieving Public Health Control of Tuberculosis 77
POLICY OPTIONS AND RECOMMENDATIONS
initiatives will not be attained simply by repeating previous
local level. Customized province/city-wide models of NTP implementation, which integrate all elements of the CUP into a
used as the main mechanism for a nationwide NTP implementation over the medium- to long-term period until public health control
following essential elements:
(1)
(2)
(3)
(4) Additional enhancement of treatment programs
(5)
(6) Advocacy, Communication and Social Mobilization (ACSM)/reporting and monitoring.
developing and moving local-area models from implementation
city-wide models and then determine the current stage each province or city is in. The national strategy should aim to move all at least to Stage 1, move those at Stage 1 to Stage 2, and sustain all
to facilitate attainment of these objectives (G. Alcantara et al.,
78 Mapping the Policy Environment for Family Health
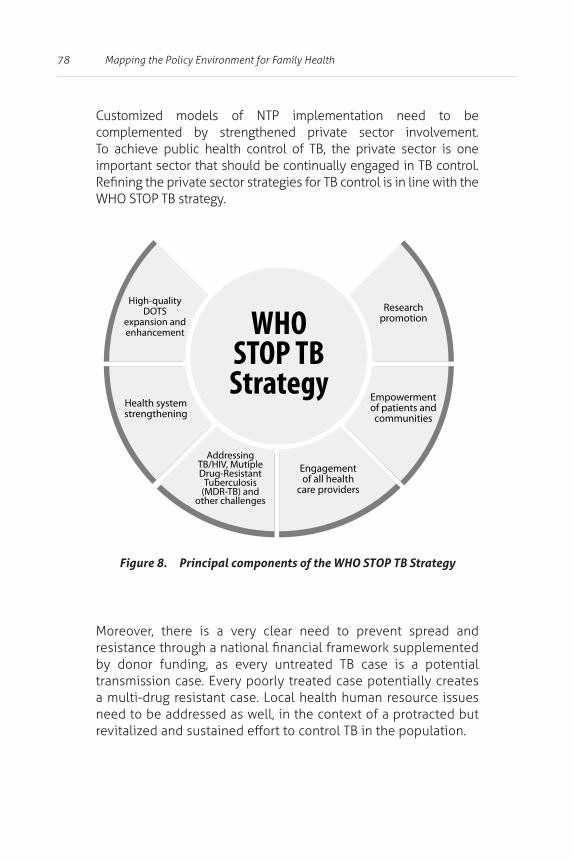
Customized models of NTP implementation need to be complemented by strengthened private sector involvement.
Moreover, there is a very clear need to prevent spread and
transmission case. Every poorly treated case potentially creates a multi-drug resistant case. Local health human resource issues
Figure 8. Principal components of the WHO STOP TB Strategy
79
4 Preventing a Larger Epidemic of HIV/AIDS
“Just as the virus depletes the human body of its natural defenses, it can also deplete families and communities of the assets and social structures necessary for successful prevention and provision of care and treatment for persons living with HIV/ AIDS. The impact of HIV/ AIDS extends beyond those living with the virus, as each infection
and communities surrounding an infected person.”
(Lyons, The Impact of HIV and AIDS on Children, Families and
Epidemic, 1998)
80 Mapping the Policy Environment for Family Health
problem, with an estimated 11,168 cases in the Philippines
four has progressed to full-blown AIDS, while the rest remain asymptomatic (DOH, 2008f). The average cumulative annual
AIDS Council [PNAC], 2005).
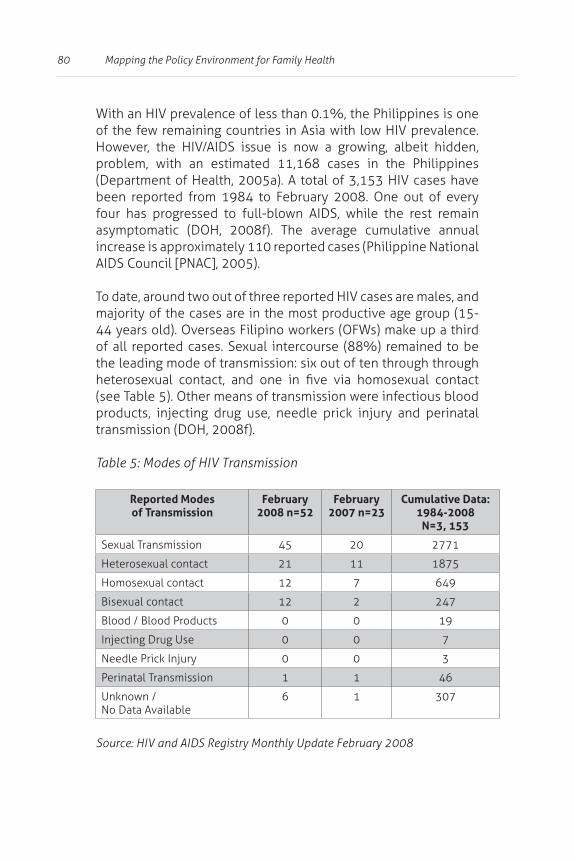
majority of the cases are in the most productive age group (15-
(see Table 5). Other means of transmission were infectious blood
transmission (DOH, 2008f).
Modes of HIV Transmission
Reported Modes of Transmission
February 2008 n=52
February 2007 n=23
Cumulative Data: 1984-2008
N=3, 153
45 20 2771
21 11 1875
12 7 649
12 2 247
0 0 19
Injecting Drug Use 0 0 7
0 0 3
Perinatal Transmission 1 1 46
No Data Available6 1 307
81Preventing a Larger Epidemic of HIV/AIDS
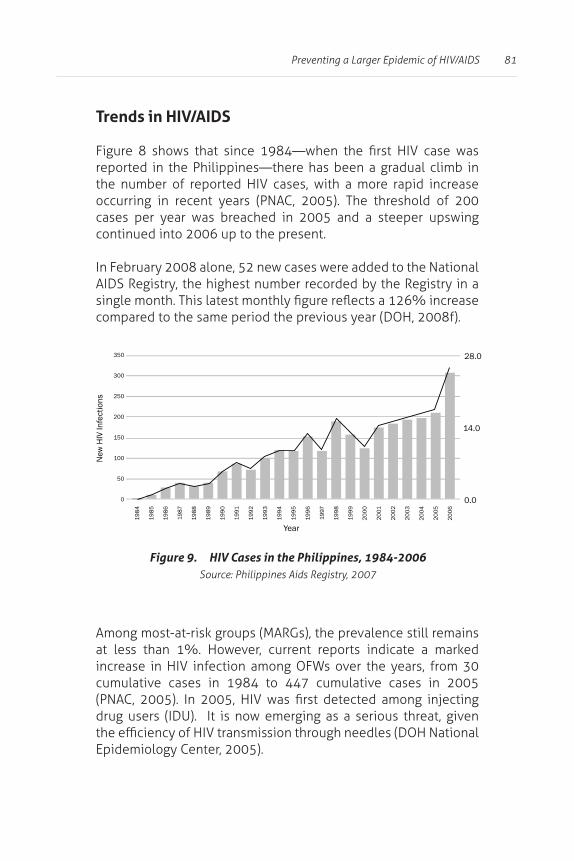
Trends in HIV/AIDS
occurring in recent years (PNAC, 2005). The threshold of 200 cases per year was breached in 2005 and a steeper upswing continued into 2006 up to the present.
AIDS Registry, the highest number recorded by the Registry in a
compared to the same period the previous year (DOH, 2008f).
cumulative cases in 1984 to 447 cumulative cases in 2005
drug users (IDU). It is now emerging as a serious threat, given
Epidemiology Center, 2005).
Figure 9. HIV Cases in the Philippines, 1984-2006
82 Mapping the Policy Environment for Family Health
CURRENT POLICY INITIATIVES: Enabling and Supporting Factors
Strong Framework for HIV/AIDS Policy and Implementation
The Philippines created the National AIDS and STI Prevention and Control Program (NASPCP) in 1988 within the DOH in response
other reproductive tract infections and mitigation of their impact (DOH NASPCP, 2008).
an advisory body to the President. It is a multi-sectoral body
and several NGOs. PNAC was envisioned to provide a strong
National AIDS Council, 2006).
The AIDS Law (RA 8504, or the Philippine AIDS Prevention and Control Act of 1998) was enacted to mandate promulgation of
and control, the institutionalization of a nationwide information and educational program, establishment of a comprehensive monitoring system, and strengthening of PNAC (PNAC, 2005).
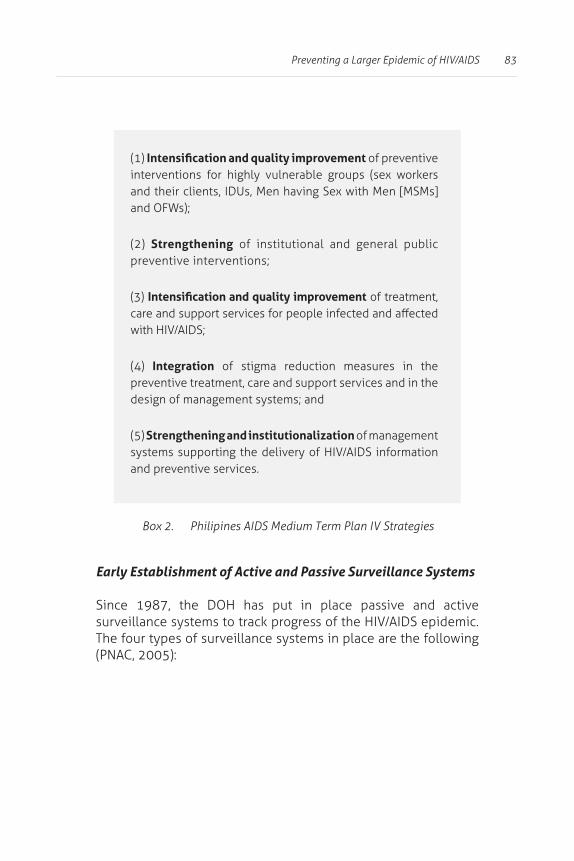
of the disease on individuals, families and communities. It adopts
83Preventing a Larger Epidemic of HIV/AIDS
Early Establishment of Active and Passive Surveillance Systems
Since 1987, the DOH has put in place passive and active
The four types of surveillance systems in place are the following (PNAC, 2005):
(1) of preventive
(2) Strengthening of institutional and general public
(3) of treatment,
(4) Integration of stigma reduction measures in the preventive treatment, care and support services and in the
(5) Strengthening and institutionalization of management
and preventive services.
Box 2. Philipines AIDS Medium Term Plan IV Strategies

84 Mapping the Policy Environment for Family Health
HIV/AIDS Registry (HAR)
A passive surveillance system established
accredited hospitals, laboratories, blood
HIV Serologic Surveillance (HSS)
Started in 1993 to serve as early warning
consistently monitored what it considered as
Behavioral Sentinel Surveillance (BSS)
Established in 10 HSS sentinel sites to
increasing the number of surveillance sites
monitored but research teams were allowed to include other special groups considered at
Sentinel STI Etiologic Surveillance System (SSESS)
Set up in December 2001 and made
prevent transmission.

85Preventing a Larger Epidemic of HIV/AIDS
Multi-Sectoral Response to Service Needs
Several initiatives have contributed to the sustained low prevalence
multiple sectors, include the following (PNAC, 2006):
(1) strategies, comprehensive treatment and distribution of
through Social Hygiene Clinics of LGUs.
(2) Piloted community-based interventions, ranging from information dissemination to behavior change strategies
(3) quality prevention, care and support services, and the
in government-retained hospitals and NGOs based in the community.
(4) Creation of Local AIDS Councils (LACs) in some cities, thereby institutionalizing partnership of LGUs and NGO at the city
(5)
training of trainers on the use of these modules.
(6) the DOLE. A tripartite committee was formed to ensure full implementation of this policy. Involvement of the business sector and trade unions facilitated the establishment of
(7)

86 Mapping the Policy Environment for Family Health
POLICY ISSUES: Gaps, Challenges and Opportunities
Despite the presence of an enabling policy environment, the “low
Philippines in the past has relegated the issue at the bottom of the development agenda. This is evident in fewer resources allotted
implementation of guidelines and protocols, as well as unsustained but promising pilot interventions (PNAC, 2006).
Persistent Risks and Vulnerabilities Among High-Risk Groups
Consistent condom use was generally low (<30%) among the
of STI among vulnerable groups remained uninterrupted, and only the MSM group posted some improvement from 2002 to
patterns of STI among selected groups, signifying inadequacies in both the quantity and quality of interventions for HRGs, probably
Observed STI patterns were:
Syphilis rates Among HRGs, the rate ranged from 1% to 4%, the
Female sex workers
often than MSMs.
Injecting Drug Users (IDU)
There was a 50% increase of IDUs reporting signs and symptoms of STI in 2003, compared to 2002.
87Preventing a Larger Epidemic of HIV/AIDS
High-Risk Behaviors Among the Youth
The vulnerability of young people is emerging as a major concern
More men (70%) than women (68%) engaged in unprotected
remained low. The prevalence of STI among young females and males is also quite high compared to the general population.
These trends among the respondents, coupled with their low
epidemic will not be undermined (PNAC, 2005).
Low Level of HIV/AIDS Knowledge and Awareness
Among the general population, the 2003 National Demographic
to one uninfected partner).
2005). This situation presents a huge challenge for information
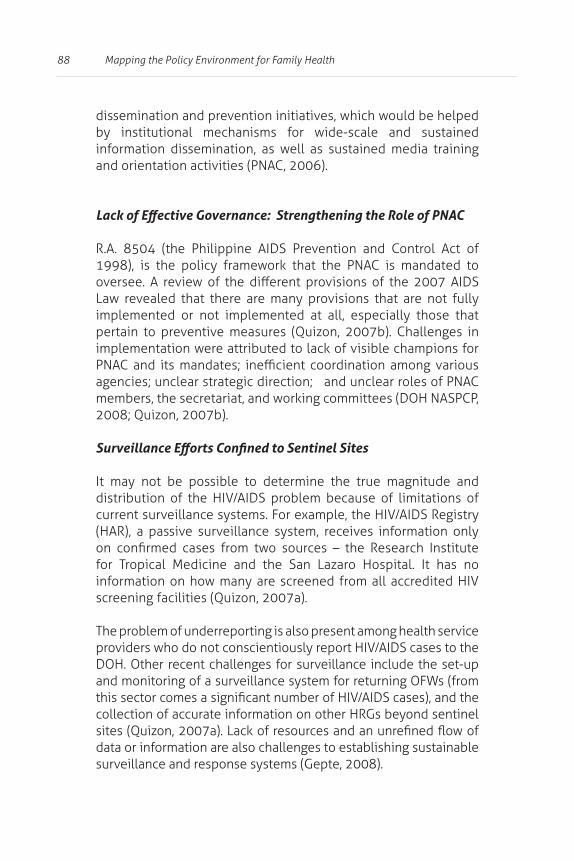
88 Mapping the Policy Environment for Family Health
dissemination and prevention initiatives, which would be helped by institutional mechanisms for wide-scale and sustained information dissemination, as well as sustained media training and orientation activities (PNAC, 2006).
R.A. 8504 (the Philippine AIDS Prevention and Control Act of
Law revealed that there are many provisions that are not fully implemented or not implemented at all, especially those that pertain to preventive measures (Quizon, 2007b). Challenges in
It may not be possible to determine the true magnitude and
(HAR), a passive surveillance system, receives information only
for Tropical Medicine and the San Lazaro Hospital. It has no
screening facilities (Quizon, 2007a).
The problem of underreporting is also present among health service
DOH. Other recent challenges for surveillance include the set-up
collection of accurate information on other HRGs beyond sentinel
data or information are also challenges to establishing sustainable surveillance and response systems (Gepte, 2008).
89Preventing a Larger Epidemic of HIV/AIDS
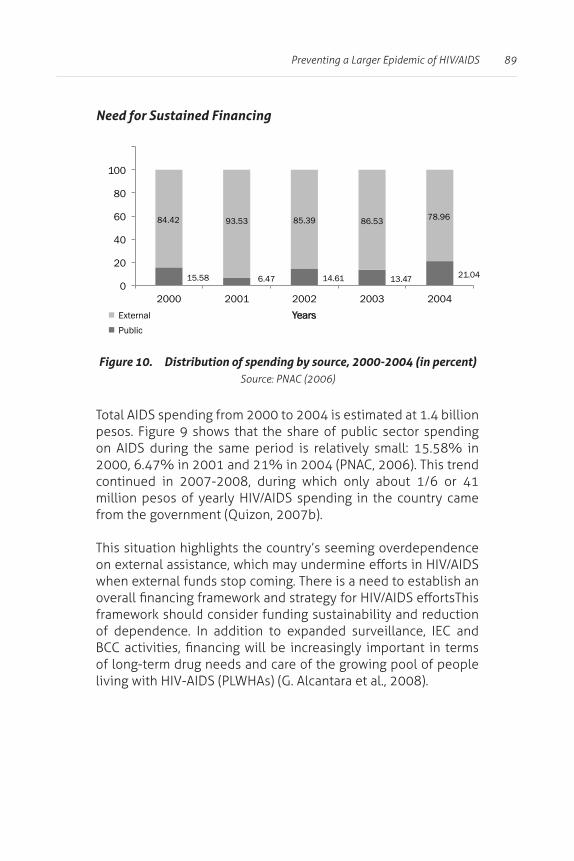
Need for Sustained Financing
Total AIDS spending from 2000 to 2004 is estimated at 1.4 billion
on AIDS during the same period is relatively small: 15.58% in 2000, 6.47% in 2001 and 21% in 2004 (PNAC, 2006). This trend continued in 2007-2008, during which only about 1/6 or 41
from the government (Quizon, 2007b).
of long-term drug needs and care of the growing pool of people
Figure 10.
15.58 6.47
14.61 13.47 21.04
84.42 93.53 85.39 86.53 78.96
0
20
40
60
80
100
2000 2001
2002 2003 2004 Years
External
Public
90 Mapping the Policy Environment for Family Health
POLICY OPTIONS AND RECOMMENDATIONS
With these outcomes in mind, there is a need to implement
retrovirals and condoms), and the provision of care and support for PLWHAs. As part of the care and support for PLWHAs, the
described in the DOH AO 2008-0022 (“Policies and Guidelines in
[DOH, 2008a]), should be promoted to address concerns not only
be established to allow widespread and sustained information dissemination and education campaigns. Surveillance also needs
reporting systems, as well as by strengthening LGU capacity to
terms of the long-term drug needs and care of the growing pool of PLHA. In this light, the possible usefulness of RA No. 9502, or
A functional national leadership and management mechanisms
the ultimately accountable agency. The Secretary of Health
enjoin other agencies to recognize and discharge their roles and
91
5 Accelerating Health Improvements in the Autonomous Region in Muslim Mindanao (ARMM)
Established in 1990, the Autonomous Region in Muslim Mindanao (ARMM) has received assistance both from national and international entities for almost two decades but remains one of the most underdeveloped regions in the country. Created on August 1, 1989 by R.A. 6734 (“An Organic Act for the ARMM”), the ARMM expanded its original composition of provinces (Maguindanao, Lanao del Sur, Sulu and Tawi-Tawi) to include Basilan and the city of Marawi through an amending law, passed in September 2001, R.A. 9054 (“An Act to Strengthen and Expand the Organic Act for the ARMM”). The latter
and governance, with the Autonomous Regional Government (ARG) getting a fairly wide range of powers. The structure of the ARG is generally patterned after the national government. ARMM is politically subdivided into nine congressional districts, 113 municipalities and

92 Mapping the Policy Environment for Family Health
The region is located in the southern part of Mindanao. Mainland provinces include Lanao del Sur and Maguindanao, while Sulu and Tawi-Tawi comprise the traditional island centers of Muslim economic, political and cultural activities. The island provinces
Adding to the uniqueness of this region, two cities, Cotabato and Isabela, are politically under Regions XII and IX, respectively.
Zamboanga City. Neither, however, forms part of ARMM (Cristobal,
Region with the Poorest Health and Development Indicators
literacy rate is 61.2%, way below the country average of 83.3% (DOH-ARMM, 2007a). Over half of the population lives below the
Report, 2007).
ARMM is characterized as having the poorest health and
It has the highest maternal mortality rates, second to CARAGA
rates and the highest percentage of women with unmet family planning needs.
Even as a predominantly Islamic region where contraceptive use is acceptable, it has the lowest rate of contraceptive use (18.7%), and eight out of ten women with unmet need for family planning (80%) do not intend to use contraceptives (National Statistics

93Accelerating Health Improvements
in the Autonomous Region in Muslim Mindanao (ARMM)
In the 2005 ARMM Health Summit, the ARMM Strategy for Health
the national rate. Infant mortality was at 41 out of 1000 live births.
The Philippine Human Development Report shows that in 2003, the infant mortality rate in the ARMM was as high as 72 deaths
Development Report, 2005). ARMM also has the highest malaria morbidity rate and the number of malaria cases reported by DOH-ARMM increased from 2005 to 2006. (DOH -ARMM, 2007b).
POLICY ISSUES: Gaps, Challenges and Opportunities
Lack of Competent Health Professionals
long in service. This may be attributed to the low level of health
Another factor that aggravates the poor health situation in ARMM
clashes and military-versus-Muslim secessionists, to banditry. All these have displaced residents.
94 Mapping the Policy Environment for Family Health
displacements have occurred in Maguindanao, Marawi City, and
term peace has made people reluctant to invest in developmental
employment, leading to further insecurity and contributing to the continuous cycle of violence.
Limited Financing for Health and Challenges to NHIP
the national government IRA. The DOH-ARMM budget for health in 2007 was 498 million pesos (DOH-ARMM, 2007). Personnel services
well-equipped health facilities that can deliver quality health care services. Although it was envisioned that reliance on the national budget would decrease as the region improved its income-generating capacity, this is yet to be seen.
In 2005, per capita gross regional domestic product was 75.8%
2007). Almost three-fourths of the total ARMM population live
commodities and services.
The prospects for the NHIP seemed promising, particularly after the 2004 elections, when indigency cards were distributed in many areas in ARMM. However, health facilities were not ready for the increased demand, as most have yet to be licensed and

95Accelerating Health Improvements
in the Autonomous Region in Muslim Mindanao (ARMM)
that could yield immediate return of investment. Since the system was not devolved, LCEs did not see delivery of health services as a joint responsibility with DOH-ARMM. The absence of guidelines in using capitation fund also allowed its utilization for non-health related activities (Serdoncillo, 2007).
Unique Politico-Administrative Setup of ARMM
in the country. Complications arise with the devolved setup in
in non-devolved areas. These may become progressively independent from the LGU because they are answerable only to the autonomous regional government (ARG).
This can lead to serious problems in direct supervision and monitoring activities, especially of areas far from the Regional
LCE when instituting health service reforms. In the devolved
managers and politicians can be a problem (Cristobal, 2007).
The national government should consider this uniqueness when crafting policies for nationwide implementation. The ARG has to be able to adapt to national policies and be able to customize these to their autonomous setting. Governance, service delivery,
arrangements between the ARG and component ARMM LGUs will

96 Mapping the Policy Environment for Family Health
To strengthen health care collaboration between the ARG and component LGUs, the DOH-ARMM formulated an ARMM-wide Investment Plan to advance improvement of health care. It has
accessible, available and acceptable basic and essential
functional and responsive health management structures
quality health facilities, services, products, devices in compliance with National and WHO Standards (health
improved and sustained investments in health for an equitable, wider coverage and improved health outcomes
Assessing CSR Response In ARMM14
CSR in ARMM
Over the last two decades, ARMM has relied on the national government, NGOs and donor agencies for contraceptive commodity support. R.A,. 9054, however, is not clear on which local government – the the Autonomous Regional Government or the Autonomous Region in Muslim Mindanao – is responsible for the actual provision of services and commodities. This poses a problem because DOH support includes only technical assistance.
services and commodities, still rests on the LGUs.
14 This section draws heavily from the policy scan of Serdoncillo (2007), which
97Accelerating Health Improvements
in the Autonomous Region in Muslim Mindanao (ARMM)
The regional leadership has voiced out support for the DOH-ARMM to scale up the CSR strategy, which is however, is still awaiting review and endorsement. The DOH-ARMM has health personnel
Choice Shops) has been introduced and so far has been accepted
hampers the implementation of CSR strategies.
Unmet Need and Contraceptive Prevalence Rate
The 2003 National Demographic and Health Survey (NDHS) reported a 27.4% unmet need with a Contraceptive Prevalence Rate of 18.7%. Although still not comparable to the rest of the
15)
supply of these services and commodities due to the gradual
Considering the above situation and the earlier-described
a region with indicators consistently at the bottom compared to the rest of the country in terms of performance, and always on
policies should be addressed.
Key Policy Recommendations for CSR in ARMM
change should be developed. This should be addressed not only to
15 A legal pronouncement in Islam.

98 Mapping the Policy Environment for Family Health
The private sector should also be tapped to provide resources
Training and capacity building on Contraceptive Distribution Logistics and Management Information System (CDLMIS) and
establish a delivery and monitoring system unique to ARMM. Similarly, operationalization of the Regional Project Management
always consider the unique politico-administrative setup in ARMM to ensure parallel development.
Scaling Up Malaria Control In ARMM16
Malaria is no longer a leading cause of mortality in the country, but remains as the eighth leading cause of morbidity (DOH, 2005b). According to the WHO, malaria burden of disease rests disproportionately on poor and marginalized communities. ARMM has the highest malaria morbidity rate in the country
limited access to and/or unavailability of basic health services
99Accelerating Health Improvements
in the Autonomous Region in Muslim Mindanao (ARMM)
in the region. Geographical constraints and the long history of
international and national malaria control programs, such as the
strategy categorizes areas in the country in terms of burden and
priority areas for intervention. Donor agencies, to date, continue to provide resources for malaria control in ARMM provinces
Challenges for Malaria Control in ARMM
Aside from persistent problems with access to and availability of health services, ARMM faces other challenges in malaria control. Surveys done both by the government and its development partners show that there is still low level of awareness about malaria and malaria prevention in many communities, even in areas where support has been available for the past several
malaria control and prevention measures at the household level (DOH-ARMM, 2007b).
Another problem in ARMM concerns the quality of available anti-malaria health services.Treatment and control are not guaranteed, owing to various limitations in the current malaria control program
access to related services and their low awareness level on the illness, misdiagnosis and underreporting are prevalent in the region. The region might be inadequately prepared to cope with the continuing challenge posed by malaria in communities where
100 Mapping the Policy Environment for Family Health
DOH-ARMM also has problems with data collection and surveillance, partly due to gaps in the quantity and quality of
underreporting, problems with data collection and surveillance
malaria control programs.
Although it is good that there are several donor agencies interested in malaria control, separate malaria organizations are not sustainable entities, and they tend to pull away resources and
Key Policy Recommendations for Malaria Control in ARMM
DOH-ARMM and donor organizations should head towards more creative, localized community-based and household-based approaches to stimulate interest within target communities.
promotion and education, particularly on convincing people
preparation and practicing prevention with the use of Insecticide-
signs and symptoms of uncomplicated and complicated malaria, but also to refer patients to appropriate hospitals as well.
Capacities of health personnel at the regional and provincial levels must also be strengthened. Training of regional and provincial malaria coordinators can focus on achieving basic competency on the management of the malaria control program. Meanwhile, training of hospital and RHU personnel can focus on improving capacities for diagnosis, cure, prevention, and surveillance.
Development and implementation of quality assurance standards based on local conditions and limitations may help develop and maintain reliable microscopy for carrying out malaria diagnosis.
101Accelerating Health Improvements
in the Autonomous Region in Muslim Mindanao (ARMM)
where malaria is endemic. This will be crucial in the provision of appropriate anti-malarial therapy and the generation of accurate
resource allocation.
There may also be a need to involve the private health sector
should be updated on the latest standards and tools for malaria control to ensure their cooperation in implementing standard protocols for diagnosis, treatment, recording and reporting of
malaria control in the region.They need to strengthen their mechanism for donor coordination, emphasizing transparency and accountability. A mechanism similar to the Country Coordinating
provincial, municipal, and even barangay levels.
in the DOH-ARMM budget. This should be supported with corresponding LGU allocations for malaria. PhilHealth also needs
the DOH-ARMM has to upgrade facilities to comply with PhilHealth accreditation requirements. All these would ensure sustainability even after phase-out of development programs in the region.
Securing Critical Health Human Resources for ARMM17
The current health situation in ARMM is largely due to its
17 This section draws heavily from the policy scan of Cristobal (2007), which

102 Mapping the Policy Environment for Family Health
of securing health personnel. HHR problems can be grouped
the management of HHR. In turn, HHR problems can be further
of surrounding regions, CHD-ARMM or the DOH-ARMM would
consideration, as many as 76 items would be necessary to accelerate desired improvements.
nurses and midwives) in community and provincial posts. If computed based on DOH standards, ARMM needs additional 92 physicians, 60 nurses, 202 midwives, 40 dentists and 41 sanitation
a midwife or a nurse -- for every two adjacent barangays.
of budget for hospital personal services. Hence, an increase in the number of plantilla items proportionate to the needs of ARMM should be advocated not only at the regional but at the the national government level as well.
departments, agencies, bureaus, commissions, state universities and colleges and other instrumentalities of the national
103Accelerating Health Improvements
in the Autonomous Region in Muslim Mindanao (ARMM)
government in status quo pending the approval of Rationalization Plans. Applicability of this policy to DOH-ARMM should be
Another policy obstacle impeding the creation of additional plantilla positions is R.A. 6734, which states that authority over the health sector in ARMM is to be devolved to the regional government, while the national government provides the budget
while the ARG is in charge of human resources, plantilla items come from the national government. This ambivalence creates an administrative dichotomy in HHR management.
To provide the legal basis for appropriate HHR complementation
for the formulation of the ARMM Health Code and its adoption by the regional leadership. It should also conduct studies on health facilities and assess human resource needs to generate needed evidence to
Plantilla Vacancies
Even with the current number of plantilla items, there are communities and provincial posts with physician vacancies. Of the 176 physician items in ARMM, 12 are vacant, most of which are located in Sulu and Tawi-tawi. Among the reasons cited were: poor facilities and living conditions, unstable security and political
seen in many areas of the Philippines. In one study, massive health
as a combination of low salaries for health professionals in the Philippines and the tremendous demand for health professionals
The DOH-ARMM and the ARG, with the help of the LGUs, should
sources to encourage employment and deployment despite

104 Mapping the Policy Environment for Family Health
budget, particularly for areas that are not IRA-dependent. This
Memorandum No. 53 states that IRA funds can be used for the
professionals can be immediately assigned to the neediest areas in ARMM. Meanwhile, scholarships provided by the Pinoy MD Program can be used to strengthen capacities of health personnel. Partnerships with local medical schools may also be established to provide additional scholarships that would require graduates to serve in communities as part of their contractual obligation. Region IX has entered into a similar arrangement with the Ateneo de Zamboanga School of Medicine. This partnershiphas increased the number of physicians deployed in the region.
health services. This is similar to the nurse practitioner program in Canada. The health referral system in doctor-less areas can also be strengthened to ensure the best possible care for the community.
Misuse of Plantilla Items
Another HHR problem in ARMM is the misuse of plantilla
personnel are falsely entered in the government payroll, thereby depleting already limited resources for health. This usually occurs in poorly-monitored areas.
or review health personnel hiring.
105Accelerating Health Improvements
in the Autonomous Region in Muslim Mindanao (ARMM)
of the Ateneo de Zamboanga School of Medicine, some personnel rarely or never report to their area of assignment. They stay in the
plantilla items and continuously collect their salaries. In some instances, an individual will be hired for a community post but
or be detailed elsewhere through internal arrangements. Reasons
posts, security issues and the limited LGU budget for Travel
personal resources to carry out their duties, discouraging them to regularly report to their designated posts.
provisions for promotion and disciplinary schemes. This should
a database of personnel should be created and review conducted to determine whether personnel meet core competencies required by their current posts.
Lack of Appropriate Skills Among Current Personnel
This may be due to the hiring of fresh graduates for management posts, which has been a consequence of the high turnover rate of human resources. Without proper orientation, the new recruits
Some LGUs do not allow their employees to attend training
for personnel travel and training.
There is also a huge gap in information management. Health Information and Surveillance Systems were not taught to ARMM employees. Despite the obvious need to hire epidemiology and management information systems specialists, the region is

106 Mapping the Policy Environment for Family Health
information system, and data collection – if being done at all – is carried out haphazardly.
There is therefore a need to develop an HHR development plan that focuses on building and strengthening management and technical competencies. The plan should identify critical HHR
be part of this development plan.
Guidelines and tools to assess the training needs of employees based on their current positions and responsibilities should also be developed. These can be used to determine who and how many need to be trained. A Memorandum Order for the utilization of these guidelines and tools may be issued. It may specify the
Alternative Planning Strategies for Planning and Response Mechanisms in ARMM18
ARMM to determine planning and response mechanisms in
functions of the DOH-ARMM were fully transferred to the ARG,

107Accelerating Health Improvements
in the Autonomous Region in Muslim Mindanao (ARMM)
and administrative control and supervision of the Department is
This is in contrast to the rest of the country, where the LGU is primarily held accountable for the health of its constituents. This poses two main questions: (1) How do LGUs factor in the health service provision in ARMM when the ARG and the DOH-ARMM are
centralized and devolved areas?
The Secretary is the head of the DOH-ARMM and is co-terminus with the Governor. He is supported by a team of technical and
of Marawi City.
The DOH-ARMM, which leads the planning process, consults with
This traditional planning is conducted annually with minimal
While the DOH-ARMM generally follows national guidelines and
Marawi City further complicates planning and response. Health
by the LGUs, limiting the role of the DOH-ARMM to mere provision of technical assistance.
need and leveraged for performance needs to be established. Setting up reasonably attainable performance criteria can help
among national agencies to accelerate assistance to the region.

108 Mapping the Policy Environment for Family Health
Operational arrangements with the newly integrated LGUs in
must support national and regional health goals. Until issues about health systems integration are addressed, the DOH-ARMM, with the support of the ARG, should be responsible for health
responsibilities to ARMM LGUs, particularly in the sharing of the IRA. Although this may initially be limited to advocacy, the development of a binding regional legislation should be a long-term goal.
Need for Accurate Health Information in the Planning Process
Developing an appropriate response to health problems in ARMM requires an in-depth analysis of its health situation. This,
in epidemiology, personnel, health monitoring and evaluation, undermines the functionality of the health information system in ARMM.
Training on epidemiological monitoring and surveillance should be given attention. Use of data and related information in health development planning, investment programming and program management should be promoted to underscore the importance and implications of generating accurate and timely data on the ground.
Some of the technical assistance (TA) provided by development partners to ARMM get implemented with minimal coordination (if any, at all) with the ARG and the DOH-ARMM. This means that the DOH-ARMM still has to strengthen its capacity to provide technical oversight and guidance in coordinating and harmonizing all health and related interventions of development partners in the region.

109Accelerating Health Improvements
in the Autonomous Region in Muslim Mindanao (ARMM)
promoting collaboration among development partners, the DOH-ARMM should also develop plans to sustain various interventions initiated in the region.
promote accountability and transparency in the ARG and the DOH-ARMM. It will help the region determine its health strategies and priorities, provide corresponding investments, and identify
ARMM-wide investment plan for health.
The persistence of man-made emergencies due to armed
epidemics due to poor health service delivery further strains already overstretched health budgets. Health responses – be they emergency needs in evacuation centers or routine health care in Rural Health Centers – are usually inadequate to address health
District Hospitals to create alternative funding sources, mostly
not been adopted for the whole heath care setup.
increases with the change in regional priorities accompanying
medium-term investment plan.
Health emergency response mechanisms, particularly for man-
may be adopted to ensure health service delivery in those areas.

110 Mapping the Policy Environment for Family Health
Recognition of indigenous methods in health care provision can
formal protocols that respect the sensibilities of various parties
SUMMARY OF POLICY OPTIONS AND RECOMMENDATIONS
the region to implement national issuances and policies often formulated for LGUs in a more devolved setup. The national
that the poor health performance of ARMM partly stems from this
allocations for ARMM. This will allow it to adequately respond to
be developed to foster collaboration among various government agencies and development partners in accelerating assistance to ARMM.
Health reforms should start with the approval of either the ARMM Health Code or the ARMM Administrative Code to provide a legal basis for appropriate human resource complementation
politicization of decisions on critical health concerns. Localization
concerning the mandate, authority and responsibility on health are not clear.
While the Local Government Code transferred from the national government to LGUs the responsibility for the delivery of basic
primarily responsible for the implementation of programs and

111Accelerating Health Improvements
in the Autonomous Region in Muslim Mindanao (ARMM)
projects, including those on health. The latter has led some ARMM LGUs to assume that they can start deprioritizing health, since the responsibility on the implementation of health programs rests
remains unresolved, the ARG and the DOH ARMM may advocate
Partnership among the DOH-ARMM, ARMM LGUs, and PhilHealth should be strengthened. PhilHealth enrolment, however, should
revenuegenerating instrument. PhilHealth should monitor use of it s capitation fund to ensure that it is mainly used for health systems development and service delivery improvement.
the private sector, NGOs, civil society organizations (CSO) and POs in dialogues/fora and programs that promote community involvement. Opportunities in capacity building and grant
for engaging CSOs and NGOs in in community mobilization and health promotion should be developed.
The DOH-ARMM should pursue the ARMM-wide investment plan for health (AIPH) as an instrument for identifying health problems
management-related issues and concerns in the ARMM to promote
AIPH goals should be attainable, and its interventions doable in the medium term. The goals and interventions should be accompanied by an HHR development plan, which may include creative solutions for addressing health personnel shortage,

112 Mapping the Policy Environment for Family Health
services. The HHR development plan should also contain strategies for addressing service delivery gaps and for promoting the acceptability and utilization of health programs and activities
emergency situations that deprive people of basic services,
peace and security problem is a crucial step towards achieving
113
6 Local F1 Implementation and Other Cross-Cutting Issues
the health care system during the past few years. F1 serves as the framework for implementing the Health Sector Reform Agenda. Its
Ensure access to and availability of essential and basic health
Improve health system performance. This section, in looking at how the F1 strategy has been incorporated into the health care system, intends to distill lessons from which future initiatives may be built. Financing initiatives through PhilHealth are also reviewed to assess their contribution to the
access to health services. Emerging issues in HHR and health facility rationalization are also presented.

114 Mapping the Policy Environment for Family Health
Assessing F1 Implementation19
documents such as AOs that spell out objectives, possible structures, strategies, and mechanisms meant to facilitate its implementationHowever, there appears to be large variance in
a broader integrated communication strategy (ICS) campaign.20
organizational structure and policy process. The establishment of the Sectoral Coordination Management and of Policy and Standards Development teams (PSDTs) has created focused
organizational structure does not provide the focus required to prioritize issues related to the achievement of sustainable family health (e.g. achieving desired family size, improving maternal and child health, controlling tuberculosis and preventing the rapid
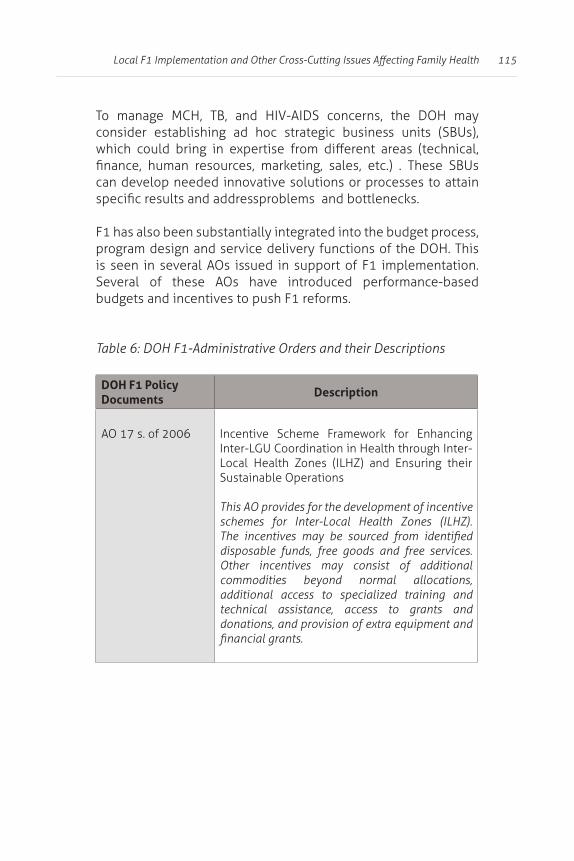
115
can develop needed innovative solutions or processes to attain
program design and service delivery functions of the DOH. This
Several of these AOs have introduced performance-based
DOH F1-Administrative Orders and their Descriptions
DOH F1 Policy Documents
Description
AO 17 s. of 2006Inter-LGU Coordination in Health through Inter-Local Health Zones (ILHZ) and Ensuring their Sustainable Operations
This AO provides for the development of incentive schemes for Inter-Local Health Zones (ILHZ).
disposable funds, free goods and free services. Other incentives may consist of additional commodities beyond normal allocations, additional access to specialized training and technical assistance, access to grants and donations, and provision of extra equipment and

116 Mapping the Policy Environment for Family Health
AO 23 s. of 2006
This AO clearly lays down the F1 budget framework as oriented towards rational and performance-based incentives, like allocation of public health goods, and the development of service packages for each level of facility. It also spells out LGU public health service performance guidelines.
The DOH is expected to fast track automation and harmonization of its regulatory processes, and institutionalization of its quality seals. It is also mandated to work on securing income retention
Province-Wide Investment Plan for Health (PIPH) and the LGU Health Scorecard to help LGU-level health systems. Finally, it has to upgrade the
procurement, logistics and information, and internal audit management capacities of CHDs.
AO 22 s. of 2006Public Health
This AO details the F1 budget framework set by AO 23 (2006). The F1 budget is envisioned for use in a multi-pronged approach for attainment of desired
a.
HIV-AIDS, and emerging infections) and the
b.
c.
d. address lifestyle-related and water and sanitation-related illnesses.
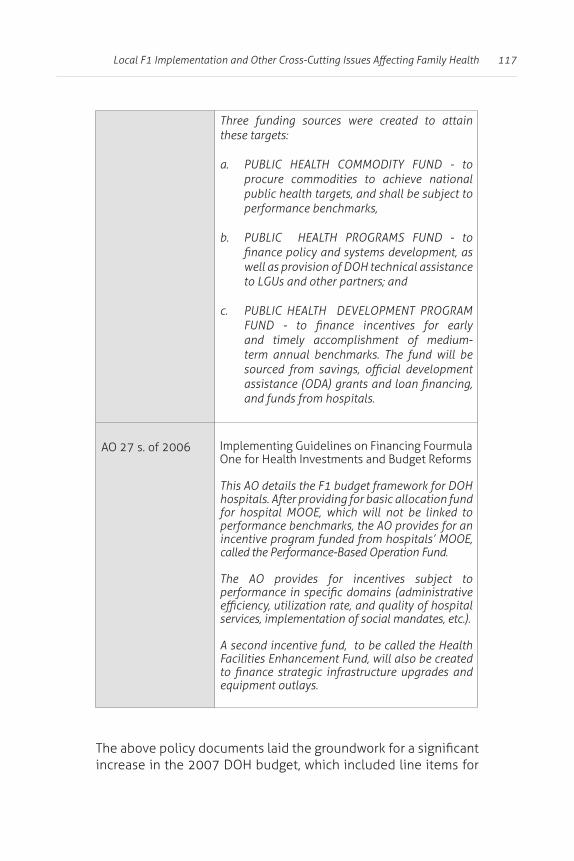
117
Three funding sources were created to attain
a. PUBLIC HEALTH COMMODITY FUND - to procure commodities to achieve national public health targets, and shall be subject to performance benchmarks,
b. PUBLIC HEALTH PROGRAMS FUND - to
well as provision of DOH technical assistance
c. PUBLIC HEALTH DEVELOPMENT PROGRAM
and timely accomplishment of medium-term annual benchmarks. The fund will be
and funds from hospitals.
AO 27 s. of 2006
This AO details the F1 budget framework for DOH hospitals. After providing for basic allocation fund for hospital MOOE, which will not be linked to performance benchmarks, the AO provides for an
called the Performance-Based Operation Fund.
The AO provides for incentives subject to
services, implementation of social mandates, etc.).
A second incentive fund, to be called the Health Facilities Enhancement Fund, will also be created
equipment outlays.
increase in the 2007 DOH budget, which included line items for

118 Mapping the Policy Environment for Family Health
to fully convert its whole budget into a performance-based
legislative mandate to secure income retention functions for regulatory agencies and increased management autonomy for DOH hospitals. The DOH should also focus on necessary policy actions in tandem with policy changes it is implementing with its
being applied as a guide, or strategy in health program planning, design and management. These policies include
of DOH hospital licensing, installation of hospital governing boards and the introduction of consumer participation in health
for capacities, processes, and instruments are still needed for full
Utility of the Province-wide Investment Plan for Health (PIPH), Its Process and Tools to Establish F1-oriented Partnerships21
instrument for establishing partnerships with LGUs and other
better health outcomes, more responsive health system, and
As a whole, the PIPH process, guidelines and tools are fairly successful and useful. Hence, the provinces are able to produce their own situational analyses (SAs) and provincial plans,

119
of Strategic Objective No. 3 (i.e. achieving sustainable family
investments geared towards Maternal and Child Health (MCH),
and reproductive health, Contraceptive Self-Reliance plans and
Most provincial investment plans are complete with health
management and organizational structures for implementation spelled out. However, there is a greater bias for service delivery
well prioritized in most provinces. One possible reason for this leaning towards service delivery, and the lower priority for other
Most of the PIPH activities can be easily integrated into the usual LGU budget planning systems. The greater challenge is to elicit and enforce resource commitments of participating LGUs, and to impose sanctions on those who failed on their promises.
contributions in the total investment for health. However, aggregate funds commitments of some LGUs for the PIPH are
increments in their health budgets could challenge the absorptive capacity of the local health sector, and may lead to unnecessary

120 Mapping the Policy Environment for Family Health
LGU scorecard, and the Service Level Agreement (SLA) instrument. Additional innovations for DOH to consider are the following:
1. Expansion of the scope and substance of the SLAs.
public health sector there. A mapping and analysis of the private sector should guide investors in identifying complementary services that should be upgraded in the public sector so that local residents, especially the poor with PhilHealth coverage, should have a full array of available service in the province.
2. Strengthening the DOH Bureau of Local Health
to review the PIPH, and of CHDs to supervise and monitor the progress of the entire PIPH process.
(a) introduction of other objective or quantitative indicators or parameters to assess PIPH documents, and (b) evaluation of investments by at least two persons, one of whom is preferably
3. Development of legal instruments for service level agreements.
health goals).
There is no need to reduce the 12 steps in developing the PIPH,
out simultaneously. What needs to be done, however, is to require the holding of properly-documented public consultations
Appraisal Committee (JAC).
121
Among the things the JAC may require is a set of “criteria” similar
with more direct impact on the poor or have greater strategic
in PhilHealth so they can access health services and at the same
4. Simplification of guidelines and their dissemination to LGUs on a timely basis.
study those reference materials.
The guidelines should present models or templates on
approach to establish correlation, if not causation, between
types, amounts and timing of interventions.
made available to LGUs to teach them PER, or at least
and methodologies.
122 Mapping the Policy Environment for Family Health
5. Expansion of the composition of the TWG/PG and require conduct of public consultations and stakeholders’ meetings.
These meetings are meant to validate SAs and investment plans. Additional members may include private sector representatives
The new members should be able to bring in concerns, ideas, perspectives, resources and support to the whole PIPH process. They should also insist on the complete documentation of the composition of the TWG/PG and all of their activities.
The PIPH process, guidelines and tools may be localized to the level of cities/municipalities in the case of provinces that have
TWG/PG.
problems among adjacent LGUs. Shared health problems could be spread of disease epidemics, disease contagion brought about by environmental factors or population.
The PIPH should also prioritize interventions to solve shared health problems (brought about by outside factors).
Another consideration in the choice of investments would be the possible economies of scale, or scope in the provision of certain services to a group of health services. Since the cities/municipalities are involved right in the beginning of the PIPH process, they should be willing to provide their own counterpart
guidelines and materials may be needed.

123
In the case of provinces that have already completed their PIPH, the challenge is how to convince the component cities/municipalities to buy in to the proposed investment plans. The planned advocacy activities should help set the tone for negotiation between the province (that spearheaded the PIPH) and its component cities
city/municipality will get from participation and what it will not get should it decline. However, the province should be prepared
local plans and programs.
The province could also leverage its own fund commitments to elicit participation from cities and municipalities.In some cases, the DOH and development partners may have to craft proposed SLAs to involve both the province and the city/municipality. In
monitor and contract an enforcer to facilitate and implement inter-LGU agreements. Technical Assistance to develop, pilot and implement this facility may be necessary.
Accomplishments and Shortcoming of the Philhealth
Ensuring the Poor’s Access to Health Care22
health insurance coverage to the poorest among of the population who are least able to pay the premium. This was made possible through a scheme where both the national and local governments
government. Enrolled indigents and their families are entitled to

124 Mapping the Policy Environment for Family Health
PhilHealth Circular No. 40 S-2000 introduced (“Implementing
under the Medicare Para sa Masa Program”) a special outpatient
(1) encourage LGU participation and integration of community, private sector and other government initiatives
(2) minimize over-utilization of hospital facilities,
(4) help LGUs upgrade health facilities and services through
(5) encourage integration of local health systems through
subsidy through capitation payments.
visual acetic screening for cervical cancer).
PhilHealth capitation fund is to be created as the repository of these payments, to be managed through the appropriate LGU health boards, and spent for supplies, referral fees as well as administrative costs.
The number of enrolled families in the SP grew to 4.6 million (or about 36.3% of total PhilHealth membership) in 2006 from 2,904 in 1997. The number of enrolled families reached some 6.2

125
of some of the contracts in 2005. This led to OPlan 2.5 million,
enroll 2.5 million families.
The number of enrolled families in 2006 was about 105% of the estimated number of poor families, an upturn from the 58% increment in 2005, but meager compared to the 148% growth in
was successfully covering the poor. However, some enrolled families may not be poor, and some poor families may not be enrolled.
This may have resulted from problems in identifying the poor
estimating the total number of the poor. There are wide variations in the ratio of actively enrolled families to estimated number of total poor families in the provinces. About half of the provinces reached ratios of actively enrolled families to total poor families below 129%.
payments has been tied to the type of sponsor (regular vs. OPlan 2.5). Regular program indigents, which include LGU-sponsored families, are those whose “LGU shares” of the premium contributions – shouldered by the respective LGU, national government agencies, legislators and private sponsors – are part
include those enrolled as part of OPlan 2.5 million, whose premiums are entirely shouldered by the national government.
receive partial capitation payments, or none at all for these families.

126 Mapping the Policy Environment for Family Health
to type of enrollment. What should have been done: provide the
Nearly half of the total RHUs in the country are now accredited
with a relatively low number of accredited RHUs. The trend in accreditation of RHUs largely followed the increase in
members comprise about a little over a third (36%) of PhilHealth
Schneider and Racelis (2004) found that a lower percentage
have many families enrolled in the SP program, whether LGU-sponsored or not.
This somehow indicates that capitation payments were being
high-enrollment areas in terms of average percentage of RHUs with
How have capitation funds been utilized and managed, particularly with regard to improving access and utilization of quality services? Information on the allocation and disposition of PhilHealth capitation funds was not readily available, nor included in the forms submitted for release of those funds. There is also unevenness in the requirements, since some PhilHealth
while some do not.

127
In a 2003 survey of RHUs, Schneider and Racelis (2004) found that capitation payments were used for drugs (62%), honoraria of personnel (8-16%), equipment and supplies (13-26%).The survey
received and how it had spent it. and where this However, average
to be higher in high-enrollment areas than in low-enrollment onesThis can be a partial indication that capitation funds were utilized to supplement spending for drugs and supplies.
with enrollment levels. Thus, it would seem that the PhilHealth capitation funds are mainly spent for maintenance and operating
municipalities, the RHU budget is reduced by the amount of the capitation funds received. No new funds are made available to improve care. LGUs are able to get away with this because utilization remains low. However, the ability to deliver better
inquiry into this matter is needed.
utilization and quality of services. As long as capitation funds are seen as a premium rebate, PhilHealth will consider its duty done once the fund is released. Once the capitation fund is considered
capitation funds are being spent.
discrimination between regular members and those under OPlan 2.5, and give PhilHealth the right to demand value for money.
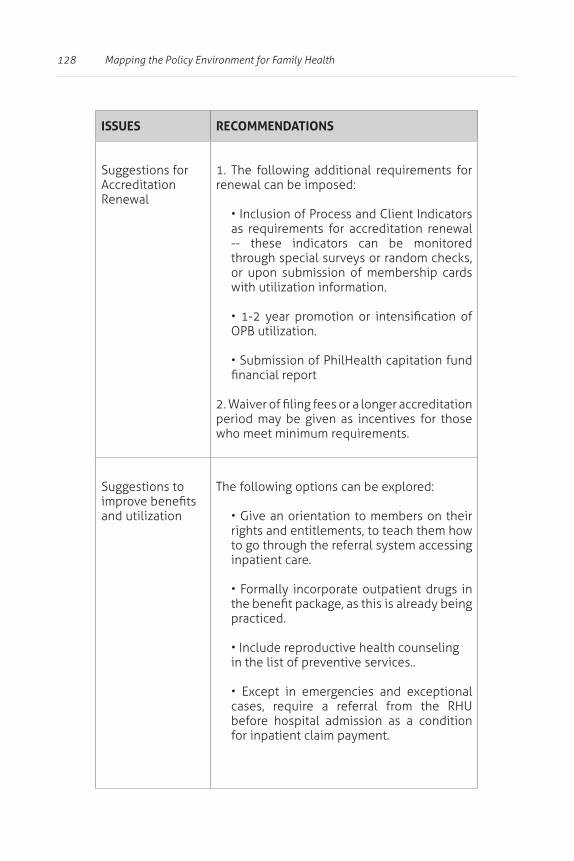
128 Mapping the Policy Environment for Family Health
ISSUES RECOMMENDATIONS
Suggestions for Accreditation Renewal
1. The following additional requirements for renewal can be imposed:
as requirements for accreditation renewal -- these indicators can be monitored
or upon submission of membership cards with utilization information.
period may be given as incentives for those who meet minimum requirements.
Suggestions to
and utilizationrights and entitlements, to teach them how to go through the referral system accessing inpatient care.
practiced.
in the list of preventive services..
cases, require a referral from the RHU before hospital admission as a condition for inpatient claim payment.

129
ISSUES RECOMMENDATIONS
gate-keeping functions, the “emergencies” and “exceptional cases” should be
humanitarian and practical terms.
The membership booklet should contain
of family members and a client satisfaction form. The booklet, to be surrendered to PhilHealth upon membership renewal, can provide data and information for
Incentives to increase utilization of PhilHealth
1. Consider advanced payment (semestral instead of quarterly) for increased utilization
2. Consider the release of 20% of the capitation amount, or whatever be the equal to administrative costs, conditioned on a minimum provision for education and preventive health services. This minimum can be increased and stipulated in the MOA between the LGU and PhilHealth.
3. Seriously monitor the utilization of the capitation fund -- either directly through
through increases in quality of care.
patient-reported satisfaction and quality of care are necessary to monitor the impact of
130 Mapping the Policy Environment for Family Health
Securing Critical Health Human Resource to Implement F123
HHR should guarantee the delivery of three other components:
HHR organization and management, both at the national and local levels.
implementation at the national and local levels (see Table 7).
This produced a list of competencies comparable to those prescribed for each type of health professionals.
perform these roles and responsibilities were also determined. The list, while not comprehensive, serves as basis for comparing
to health care delivery. Unfortunately, these are not the competencies of the current crop of local health professionals..
coverage of areas deemed important for the non-health service

131
to program management, program development, health care
governance, quality assurance and continuing quality improvement, among others.
List of Responsibilities by F1 Area and Needed Professional Competencies
Responsibilities Needed Professional Competencies
sources
and national health spending
to priority programs
health insurance program
Health Insurance
Health Program ManagementHealth Problem AnalysisProject and Proposal
Development
Social MobilizationProgram Evaluation
Health Communications
REGULATION
accreditation and Quality Assurance
and policiesQuality Assurance ToolsContinuing Quality Improvement
Organizational Development
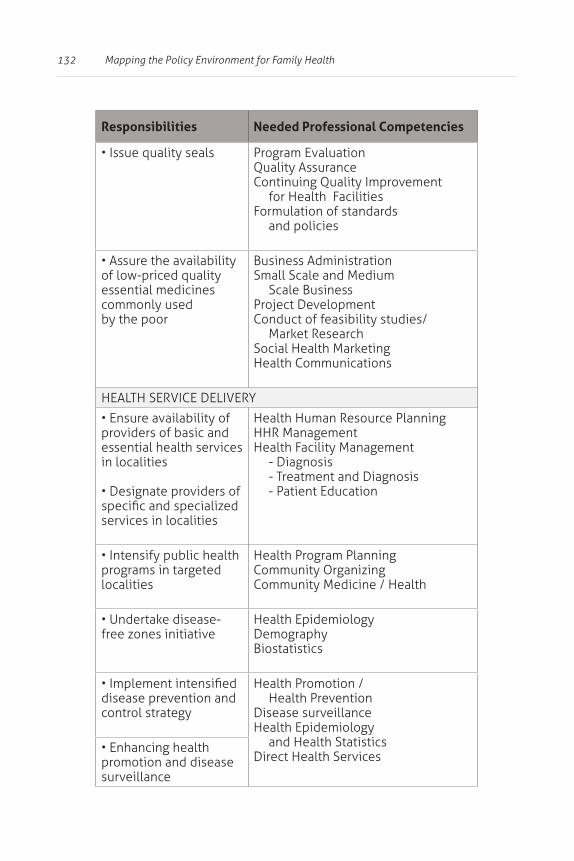
132 Mapping the Policy Environment for Family Health
Responsibilities Needed Professional Competencies
Program EvaluationQuality AssuranceContinuing Quality Improvement
and policies
of low-priced quality essential medicines commonly used by the poor
Small Scale and Medium
Project DevelopmentConduct of feasibility studies/
Health Communications
providers of basic and essential health services in localities
services in localities
Health Human Resource PlanningHHR Management
- Diagnosis- Treatment and Diagnosis- Patient Education
programs in targeted localities
Health Program PlanningCommunity OrganizingCommunity Medicine / Health
free zones initiativeHealth EpidemiologyDemography
disease prevention and control strategy
Health Promotion / Health Prevention
Disease surveillanceHealth Epidemiology
and Health StatisticsDirect Health Servicespromotion and disease
surveillance
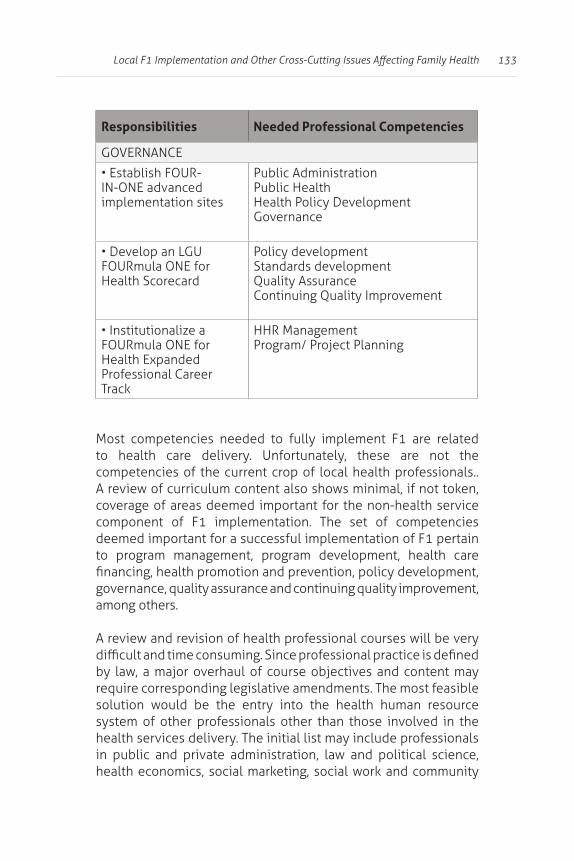
133
Responsibilities Needed Professional Competencies
IN-ONE advanced implementation sites
Public AdministrationPublic Health Health Policy DevelopmentGovernance
Health Scorecard
Policy developmentStandards developmentQuality AssuranceContinuing Quality Improvement
Professional Career
HHR ManagementProgram/ Project Planning
to health care delivery. Unfortunately, these are not the competencies of the current crop of local health professionals..
coverage of areas deemed important for the non-health service
to program management, program development, health care
governance, quality assurance and continuing quality improvement, among others.
A review and revision of health professional courses will be very
by law, a major overhaul of course objectives and content may require corresponding legislative amendments. The most feasible solution would be the entry into the health human resource system of other professionals other than those involved in the health services delivery. The initial list may include professionals in public and private administration, law and political science,

134 Mapping the Policy Environment for Family Health
development, organizational development, industrial psychology and enterprise development.
To address the current HHR situation and its limitations, the
as required competencies for health professionals who will be
is a need to augment current academic training programs with
for health facilities and not use only delivery of certain health
should be included in determining critical HR requirement, both at the DOH and at the local level.
Feasibility of Implementing Health Facility Rationalization in the Private and Public Sectors24
for health care, the need for rational health facility investment
those groups with limited or no access to health services, the poor and the marginalized population–.
With the right combination of program and policy support,
of a set of incentives and enablers that will secure adequate
Implementing a health facility rationalization policy will entail

135
in protocols, methods and processes, and an increased level of public education, advocacy and lobbying for increased resource support for health. It will also require in-house improvements in
associated with the successful implementation of a health facility rationalization policy.
accreditation and regulation of health facilities and services.
criteria should be developed. This will set the stage for
facility assessors. Only those who have successfully completed the training and passed the evaluation and testing criteria are
be renewable every three years, subject to refresher training
on a review of management protocols, operating manuals, and service delivery policies adopted by the assessed health facility for quality assurance or continuing quality improvement. The third level of assessment will be based on a review of the assessed

136 Mapping the Policy Environment for Family Health
for each level of assessment that the health facility hurdles. A newly established health facility will be initially assessed
each corresponding assessment level, a health facility will have corresponding tiered access to social health insurance payment mechanism or public subsidy. Thus, health facilities that pass all three levels of assessment may access higher levels of social health insurance payments or higher levels of budget support
It may be more practical and acceptable if a revised accreditation
incorporates all the requirements from the DOH, PhilHealth, LGUs and related agencies. This will minimize red tape, which causes inconvenience and increases cost for providers.
A national policy should declare all public health facilities
respective local governments. They may enjoy possible increases from the national government through the DOH, subject to agreed performance standards and adoption of essential public
programs and services shall be determined based on standards for per capita funding allocations commensurate with the prevailing
The DOH shall establish the desired level of per capita budget support for public health programs in each locality, based on demographic, epidemiologic, and socio-economic analysis. Initially, international standards set per capita spending for public health at US$ 12.50 (around PhP 525) in low-income localities and US$21.50 (around PhP 900) for middle and upper income localities may be adopted, but shall be subject to review and analysis for local adoption or adaptation.
Social health insurance will need to be re-designed as the principal second-peso payment mechanism for personal health

137
care that are catastrophic or are potentially catastrophic in nature. User fees for personal health care should be limited to reasonable
to review and updating every three years. This will have the
thus encourage households to set aside savings for emergency health care.
contributions to health care through sponsorship of indigents
partnership with the local governments where the sponsored member resides. Special incentive programs may also be
and collection/remittance of monthly social health insurance premiums for the self-employed. Incentives may be in the form of semi-annual or annual rebates on premiums paid, which could be deducted from future premiums.
Public hospitals operated and administered by the DOH or LGUs should be encouraged to upgrade their services and recover all of their MOOE costs from proceeds of social health insurance and user fee deductibles or co-payments from paying patients. Patients
eligible to zero or very minimal co-payment after investigation of capacity to pay. Zero co-payment may also be conditioned on the
The DOH will need to establish guidelines and initiate the
health zones. It will need to determine gaps in health facilities investments, and generate a health priority investment list to be shared with LGUs and prospective private investors. Grants for feasibility studies and design of health facilities may be made
intent to invest in health facilities development.
138 Mapping the Policy Environment for Family Health
CHDs can lead in customization, or local translation of the
in collaboration with LGUs and private entities or NGOs in their areasCHDs shall also be responsible for giving professional health facilities assessors the capacity to oversee and review development plans and proposals from prospective investors.
The DOH needs to mobilize funds from domestic or international sources to support the establishment of health facilities in
sector investors, or used to match grants for local governments who wish to invest in health facilities development. Awarding of grants or loans may be subject to feasibility assessment, acceptance of performance conditions and/or adherence to policies on operations.
As needed, the DOH may commission the services of professional technical assistance providers to facilitate the formulation of a national health facilities investment priority plan, and monitor
years. During this period, monitoring and evaluation protocols and guidelines shall be developed and tested through consultative
planning, monitoring and evaluation shall be developed through mentoring, training, and testing.
(1) uneven nationwide implementation that may largely be due
The uneven response of LGUs may have largely contributed to these discrepancies. Some LGUs have accorded top priority to
139
strategic health plans and implement them further compound the problem. Moreover, local variations in health indices are pervasive
A.O. No. 2006-0029 on Guidelines for Rationalizing the Health
on the Creation of National Steering Committee for Health, and (3) A.O. No. 2007-0038 on Adopting the Sector Development
Nonetheless, even the most straightforward of these, A.O. No. 2007-0037 -- which designates the Secretary of the Department
National Steering Committee for Health (with the DOH Secretary as Chair) -- advocates at most the “strengthen(ed) partnership
Health A.O. No. 2007-0037 )
Whether these cooperation-enhancing yet technically non-binding policies will enable and facilitate further LGU commitments in health remains to be seen. Their actual impact on community health outcomes presents another area of interest.
In view of the reality that there are limited capacities in certain areas
incapable of providing even basic health services to the concerned communities, formulate customized approaches for these priority
health programs in these areas.
140 Mapping the Policy Environment for Family Health
In addition, current restrictions at the LGU level demonstrate the limitation of “devolution” in ensuring community-responsive health delivery. This should serve as a signal to the DOH for the need for
restrictions, which is the Local Government Code of 1991.
to coverage and accessibility of health programs. The need to augment health manpower should be addressed. HHR issues are not only limited to the number of available health professionals
As pointed out in previous sections, the DOH requires a “new
to get involved in legislative initiatives to amend the Medical Act,

141
7 Policy Environment for Family Health:
Summary and Highlights
and child health, tuberculosis, HIV/AIDS and ARMM. Admittedly, the topical arrangement emphasizes the vertical nature of program administration, and veers away from the generally-recommended adoption of an integrated, locally-customized approach.
This was done deliberately as current systems are still in transition from a vertical to a much more integrated and area-based approach.
appreciation of the family health policy climate in the Philippines
and emphasizing opportunities for action that will impact across

142 Mapping the Policy Environment for Family Health
Another policy issue prevalent across all health programs is the need for sustainable
performance-based incentives
of the main mechanisms for
in the provision of essential health services.
While an attractive proposition, “underperforming” units may
cannot be adequately overcome
better performing units may have simply learned to “play” the system by focusing only on measured areas of performance.
Thus, other than a purely rewards-based system, a regular assessment of the prevailing
points and levels of the health
A graduated system may be utilized, in which least capable units are given a predetermined set of resources and, thereby, all the means to develop capacities. Incentives are provided subsequently, with steeper requirements at higher levels of development.
FOOD FOR THOUGHT
There seems to have been great
control, and a policy regime that has encouraged a widespread
apparently the linchpin of this
Two aspects of this section deserve further reassessment.
utilized in other areas? Secondly, what other initiatives can properly sustain if not improve on the prevailing positive trend? In
bears mentioning that, while there is a relatively substantial private
the DOH has not relinquished its leadership role. Such a decisive stance remains to be made in the Reproductive Health arena.
may be less contentious than, say, providing contraceptives, and may not generate the same degree of private sector cooperation. The prevailing incentive structure may seem to be still marginally
Arriving at the commensurate incentive level for maternal care may help improve service delivery in the latter area.

143 SUMMARY AND HIGHLIGHTS
increased PhilHealth coverage deemed necessary for many of the recommended programs may further draw the fund into the gray area delineating personal health care and public health services.
primarily directed to meet personal, and potentially catastrophic,
some LGUs, without corresponding improvements in delivery, highlights the inherent hazard in such arrangements.
Improving family health, a subject beyond the purview of this report, entails addressing, at the very least, policy gaps in the main cross-cutting issues presented here. It also warrants a more
social and public infrastructure policies that ameliorate poverty and other factors associated with health inequalities. After all,
circumstances. The role of development, although well beyond the scope of this volume, cannot be over-emphasized, and should be given due attention in the crafting and implementation of enhanced health policies.
144
References
Alcantara, G., Castillo, M., Lachica, J., Libre, S., Molato, R.,
Development Program.
Planning: Assessing CSR Response by LGUs. Unpublished Policy Scan Report. Health Policy Development Program and
Inc.
for the Advancement of Clinical Epidemiology, Inc.
Allen, R. H. (2007). The role of family planning in poverty reduction. Obstet Gynecol, 110(5), 999-1002.
Auer, C., Sarol, J., Jr., Tanner, M., & Weiss, M. (2000). Health
Patients in Manila, Philippines. Trop Med Int Health, 5(9), 648-656.
Analysis. Retrieved August 30, 2008, from http://www.basics.
Approach. Paper presented at the DOH Policy and Standards Development Team (PSDT) and Sectoral Management and
in ARMM. Unpublished Policy Scan Report. Health Policy
of Clinical Epidemiology, Inc.

145
Commission on Population. (2000). State of the Philippine Population Report 2000. Retrieved March 22, 2008. from http://www.popcom.gov.ph/sppr/sppr01/sppr/contents.htm.
Policy Scan Report. Health Policy and Development Program and
to the National Tuberculosis Program (NTP). Unpublished Policy Scan Report. Health Policy Development Program and
Department of Health. (2004). Administrative Order 158 series 2004: Guidelines on the Management of Donated Commodities under the Contraceptive Self-Reliance Strategy. Retrieved
Estimate in the Philippines. Manila: Department of Health.
Health.
146
Department of Health. (2006a). Administrative Order No. 2006-
Involvement in Reproductive Health. Retrieved November 17,
order/2006.
Department of Health. (2007). Administrative Order No. 2007-0019: Guidelines for the Implementation of the Quality Assurance System for Direct Sputum Smear Microscopy. Retrieved June 15, 2008. from http://www.doh.gov.ph/node/1873/print.
Department of Health. (2008a). DOH Administrative Order 2008-0022: Policies and Guidelines in the Collaborative Approach
Department of Health. (2008b). Health Policy Note: Accelerate
Department of Health.
Department of Health. (2008c). Health Policy Note: Combat the
of Health.
Maternal, Neonatal, Child Health and Nutrition (MNCHN) for Rapid Reduction of Maternal and Neonatal Mortality (Draft Administrative Order). Department of Health.
Department of Health. (2008e). National Health Sector Meeting
Transcending the Continuum of the Life-Cycle Stage: Department of Health.
147
2008). Manila: Department of Health.
and Health & Development of Older Persons. Powerpoint Presentation. Manila: Department of Health.
DOH NASPCP. (2008). National AIDS/STI Prevention & Control Program (NASPCP). Powerpoint Presentation at the DOH Program Implementation Review. Department of Health.
DOH National Epidemiology Center. (2005). 2005 Integrated
Department of Health.
Practitioners, Program Managers, and Community Leaders. Washington, DC: ESD Project.
Advancement of Clinical Epidemiology.
Unpublished Policy Scan Report. Health Policy Development
Epidemiology, Inc.
Cordero, S., Lopez, C., et al. (2008). Integrating Women and Child Health Services. Unpublished Policy Scan Report. Health Policy
Clinical Epidemiology.
148
Advancement of Clinical Epidemiology, Inc.
response in ARMM. Unpublished Policy Scan Report. Health
Advancement of Clinical Epidemiology, Inc.
Gepte, A. T. D. (2008). A Review and Assessment of Policy Issues on Strengthening Philippine Surveillance Systems for Infectious
Policy Scan Report. Health Policy Development Program and
on Economic Growth. Retrieved April 8, 2008, from http://
Hartigan-Go, K. (2007). Assessing Contraceptive Self-Reliance (CSR) Response in the Private Sector. Unpublished Policy Scan
for the Advancement of Clinical Epidemiology, Inc.
Control in the Philippines: A Review of Achievements, Emerging Issues and Possible Threats (Draft Discussion Paper).
AIDSreg2008.pdf
Advancement of Clinical Epidemiology, Inc.
149
Clinical Epidemiology, Inc.
Initiatives for the Private Sector.
Demographic Health Survey 2003. Manila.
Three Persons per Minute (Results from the 2000 Census of Population and Housing, NSO). Retrieved July 25, 2008, from
for Modern Methods Unchanged at 36 Percent (Results from
2008, from http://www.census.gov.ph/data/pressrelease/2007/
Number and Percent Distribution of Deaths by Top 10 Causes: 2004. Retrieved March 6, 2008, from http://www.census.gov.ph/data/sectordata/2004/ds0404.htm
Unpublished Policy Scan Report. Health Policy Development
Epidemiology, Inc.
Unpublished Policy Scan Report. Health Policy Development
Epidemiology, Inc.

150
Panelo, C. I. A. (2007). Achieving Public Health Control of
Advancement of Clinical Epidemiology, Inc.
Philippine Center for Investigative Journalism. (2007) Interview with Senator Aquilino Pimentel Jr. Retrieved January 31, 2007
interview.pdf
Philippine Human Development Report. (2005). Retrieved July
Philippine National AIDS Council. (2005). Country Report of the Philippines: January 2003 to November 2005. Manila.
Philippine National AIDS Council. (2006). Scaling Up Towards
AIDS Prevention, Treatment, Care and Support. Manila.
Portero, J. L., & Rubio, M. (2003). Private Practitioners and Tuberculosis Control in the Philippines: Strangers When They Meet? Trop Med Int Health, 8(4), 329-335.
Punsalan, J. (2007). Assessing Interlocal Implementation
Clinical Epidemiology, Inc.
Unpublished Policy Scan Report. Health Policy Development
Epidemiology, Inc.
Quizon, M. C. (2007b). Strengthening the Role of the PNAC. Unpublished Policy Scan Report. Health Policy Development
Epidemiology, Inc.

151
Schneider, P. and R. Racelis. (2004). The impact of PhilHealth
facilities in the Philippines. Partners for Health Reforms, Abt Associates, Maryland, USA.
Methods. Unpublished Policy Scan Report. Health Policy
Clinical Epidemiology, Inc.
Epidemiology, Inc.
Roa, C. J. C., & Llamido-Mortera, L. (2008). Special Philhealth
Advancement of Clinical Epidemiology, Inc.
migration in the Philippines : a case study and policy direction.
Resources for Health. Retrieved July 25, 2008, from Http://www.aaahrh.org/reviewal/philippines%20-%20draft.pdf
Serdoncillo, M. (2007). Assessing CSR Response in ARMM. Unpublished Policy Scan Report. Health Policy and
Clinical Epidemiology, Inc.
Theobald, S. J. (2007). The Malawi National Tuberculosis Programme: an equity analysis. International Journal for Equity in Health, 6(24).
152
(2006). Unintended Pregnancy And Induced Abortion In the
Institute.
Solon, O. J., Taguiwalo, M., Guanzon, M. R., Panelo, C. I. A., Castillo-
Strategy for the Prevention and Control of Tuberculosis in
Initiatives for the Private Sector/LEAD.
Self-Reliance (Powerpoint Presentation). USAID-PRISM.
Tuberculosis: Implications for Control. Int J Tuberc Lung Dis, 4(12), 1126-1132.
Retrieved August 30, 2008, from http://philippines.usaid.gov/
USAID. (2006). Technical Notes: Local Enhancement And
Paper. Paper presented at the DOH-PSDT/SMCO Program Implementation Review.
Into the Maternal-Newborn-Child Health and Nutrition Program - Input Document to: MNCHN Strategic Plan, MNCHN Implementing Guide and MNCHN Technical Assistance Plan. Health Policy Development Program.
153
National Objectives for Health Philippines, 2005-2010. Manila: Department of Health.
docs/104890.pdf
World Health Organization. Preamble to the Constitution of the World Health Organization as adopted by the International
of the World Health Organization, no. 2, p. 100) and entered into force on 7 April 1948. Retrieved November 18, 2008
World Health Organization. (1999). The world health report 1999:
World Health Organization. (2005). The World Health Report
Health Organization.
World Health Organization. (2007b). WHO Report 2007 Global Tuberculosis Control. Geneva: World Health Organization.
World Health Organization. (2008). Global Tuberculosis Database. Retrieved March 6, 2008, from http://www.who.int/globalatlas/DataQuery/default.asp
Development Program.

154
About the Author and Editors
Carlo PANELO is Deputy Chief of Party at UPecon-HPDP.