-
Manifestation of Antiphospholipid Syndrome among Saudi patients
:examining the applicability of sapporo
Criteria
Farjah H AlGahtani Associate professor ,MD,MPH
Leukemia ,Lymphoma in adolescent ,Thromboembolic Disease
Oncology Center , King Saud University
-
OUTLINE :
• Historical Back ground of APS
• APS Morbidity
• Pathogenesis
• Sign and symptoms of APS
• Clinical criteria of APS
• APS in Saudia Arabia
-
1952-1963 Circulating anticoagulants in SLE are named lupus
anticoagulants ( LA) because they prolong the clotting
times in phospholipid dependent assays.LA believed to
cause clinical hemorrhagic disease
1963 LA are reported by Bowie et al to be associated with
thrombosis in SLE patients.
1983 LA are identified by Harris et al to be antibodies that
react with cardiolipin Lupus anticoagulants react with
purified cardiolipin and they are identified as
anticardiolipin
antibodies by RIA
-
1963 Edward John Walter Bowie, MD Mayo Medical School identified
APS as an acquired thrombophilia
1984 Graham Robert Vivian Hughes MD FRCP. St Thomas Hospital UK
identified APS as a generalized autoimmune disorder
hassouna
-
Hughes syndrome
-
background
who we are
what we do
overview
symptoms
diagnosis
treatment
research
prognosis
patient support
membership
publications
patient FAQs
research
conferences
your options
membership
fundraising
shop
activities
news
events
research
publicity
Hassouna February 2, 2010 8
javascript:this.close()http://www.hughes-syndrome.org/index.htmhttp://www.hughes-syndrome.org/donate.htmhttp://www.hughes-syndrome.org/sitemap.htmhttp://www.hughes-syndrome.org/links.htmhttp://www.hughes-syndrome.org/contact.htmhttp://www.hughes-syndrome.org/index.htmhttp://www.hughes-syndrome.org/donate.htmhttp://www.hughes-syndrome.org/sitemap.htmhttp://www.hughes-syndrome.org/links.htmhttp://www.hughes-syndrome.org/contact.htmhttp://www.hughes-syndrome.org/index.htm
-
Antiphospholipid antibodies the most significant target antigen
is the Beta 2 glycoprotein-1
In 1990 Monica Galli and her group in Bergamo, Italy reported
that the true antigenic targets of antiphospholipid antibodies are
not the phospholipids but a plasma protein beta 2 glycoprotein-1
bound to an anionic surface. Galli M,Comfurius P, Massen C et al.
Anticardiolipin antibodies (ACA) directed not to cardiolipin but to
a plasma protein co-factor. Lancet 1990;334: 1544-1547
-
APS morbidity
• APS is the most common cause of acquired thrombophilia.
• Prevalence in general population: 2-4%
• 15-20% of all DVT with or without PE.
• 1/3 of new strokes in patients < 50 years age.
• 10-15% women with recurrent pregnancy losses.
• APS: significant proportion of thromboembolic disease and
pregnancy loss in SLE.
• APL Abs present in 30-40% SLE. One third of those patients
have clinical manifestations of APS.
• aCL positivity may precede a more severe form of SLE.
-
PATHOGENESIS
-
Two mechanisms are identified in the induction of autoimmune
Antiphospholipid antibodies (a PL).
• Apoptotic phospholipid beta 2 glycoprotein-1 complexes.
• Phospholipids released from injured cells bound to beta 2
glycoprotein 1
• Infection related
antiphospholipid antibodies.
• From experiments in mice, antiphospholipid antibodies are
produced by binding of beta2-glycoprotein 1 to phospholipid viral
or bacterial proteins by molecular mimicry
-
“Listen to your patients , he is telling you the diagnosis”
-
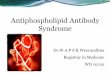
Multiple Strokes
in a Young Woman
(Brain MRI)
Occlusion of Right Middle Cerebral Artery
In a 3 Years Old Child with
Severe Headache and Hemiparesis
With aCL Antibodies +
-
Other recognized features of APS
Thrombocytopenia Haemolytic anaemia Livedo reticularis Cerebral
involvement
Epilepsy, cerebral infarction, chorea and migraine, transverse
myelopathy/myelitis mitral valve
Heart valve disease Hypertension Pulmonary hypertension Leg
ulcers
-
1000 patients with APS
• Deep vein thrombosis / PE 48%
• Pregnancy loss 35%
• Thrombocytopenia 30%
• Livedo reticularis 24%
• Stroke / TIA 20%
• Superficial thrombophlebitis 9%
• Hemolytic anemia 7%
Cervera et al. Arthritis Rheum 2002
-
Thrombotic events n = 1000 over 10 years
Baseline 10 years DVT 39% 4% Stroke/TIAs 31% 9% Pulmonary emboli
14% 4% Myocardial infarction 6% 2%
Cervera R et al Ann Rheum Dis 2015;74:1011
Antiphospholipid syndrome
-
Cervera R et al Ann Rheum Dis 2015;74:1011
Antiphospholipid syndrome
Obstetric manifestations n = 1000 over 10 years Baseline 10
years Pre-eclampsia 5% 6% Early pregnancy loss < 10 wks 35% 17%
Late pregnancy loss ≥ 10 wks 17% 5% Live birth with prematurity 11%
48% Live birth with IUGR 2% 26%
-
Clinical criteria for the diagnosis of APS
Thrombosis Venous
Arterial
Small vessel (e.g. thrombotic microangiopathy in
kidney)
Pregnancy
morbidity ≥3 consecutive miscarriages (
-
Diagnosis Of APS
• Anticardiolipin antibodies are measured using commercially
available enzyme-linked immunosorbent assay (ELISA) kits. Medium or
high titres of IgG or IgM are required.
• Firm diagnosis of APS requires two or more positive readings
for LA and/or aCL at least 6 -12weeks apart, plus at least one of
the clinical criteria listed before.
-
Background
Objectives
Method
Results Conclusion
• Antiphospholipid syndrome (APS) is a systematic autoimmune
disease featured with vascular thrombosis and pregnancy
morbidity.
• The revised Sapporo criteria are widely used classification
criteria for APS.
• This study aims to examine clinical and serological
manifestations of a cohort of Saudi APS patients.
• To examine the applicability of revised Sapporo criteria in
this cohort.
• This was a single center, retrospective study. • Data were
collected from the records of APS patients in King
Saud University Medical City. • The Sapporo criteria were
applied and divided patients into
definitive APS cases (fulfilled the criteria) and possible APS
cases (failed the criteria).
• Independent sample T-test was used to examine the difference
in clinical and laboratory manifestations and comorbidities between
the two group.
• Logistic regression was used to examine the association
between Sapporo criterial fulfillment and major clinical
manifestations.
• A total of 72 (90%) females were included. The mean (±SD) age
at diagnosis was 28.1 (± 8.7) years.
• 22 patients (27.5%) fulfilled the revised Sapporo criteria
(definitive APS).
• There was no significant difference in the clinical
manifestations or treatment between the two group (p>0.2).
• Most patients did not fulfill the revised Sapporo criteria. •
Our study identified a gap in applying these criteria in Saudi
patients. • Future studies of examining the diagnostic validity
of APS
laboratory manifestations are needed
Farjah Al-Qahtani1, Abdulrahman S. Arfaj2, Sayedah Asfar2 and
Mohammed A. Omair2 1 Division of Hematology, Department of
Medicine, King Saud University, Riyadh, Saudi Arabia 2 Division of
Rheumatology, Department of Medicine, King Saud University, Riyadh,
Saudi Arabia
Clinical and Laboratory Manifestations of Antiphospholipid
Syndrome Among Saudi Patients: Examining the Applicability of
Sapporo Criteria
Total (%, N=80)
Definitive APS (%, N=22)
Possible APS (%, N=58)
P value
Age at diagnosis, yr 28.5 (8.8) 29.7 (9.3) 28.1 (8.7) 0.46
Year at diagnosis 2002 (4) 2001 (4) 2002 (4) 0.6
Female 72 (90) 18 (81.8) 54 (93.1) 0.13
Nationality (Saudi) 71 (88.8) 18 (81.8) 53 (91.4) 0.23
Complications (Y/N) 10 (12.5) 6 (27.3) 4 (6.9) 0.014
Follow-up response
Remission without recurrent event 30 (37.5) 8 (36.4) 22
(37.9)
0.94 Recurrent event 14 (17.5) 4 (18.2) 10 (17.2)
Single visit 35 (43.8) 10 (45.5) 25 (43.1)
Died 1 (1.25) 0 (0) 1 (1.72)
Model 1 Model 2 Model 3
OR (95% CI) P value OR (95% CI) P value OR (95% CI) P value
Vascular thrombosis 1.87 (0.66, 5.25) 0.24 1.59 (0.55, 4.65)
0.39 1.61 (0.55, 4.71) 0.39
DVT or PE1 1.83 (0.68, 4.92) 0.23 1.54 (0.55, 4.32) 0.41 1.53
(0.55, 4.31) 0.42
Recurrent2 DVT or PE 0.65 (0.15, 2.79) 0.56 0.77 (0.14, 4.21)
0.77 0.67 (0.12, 3.81) 0.65
Pregnancy morbidity 0.53 (0.19, 1.46) 0.22 0.61 (0.21, 1.84)
0.39 0.63 (0.21, 1.92) 0.42
Serology Thrombosis2 Pregnancy morbidity3 Thrombocytopenia4
Asymptomatic Total
+ve5 aCL 7 (22.6) 12 (40) 3 (42.9) 6 (75) 28 (48.3)
+ve LA1 3 (9.7) 2 (6.7) 1 (14.3) 2 (25) 8 (13.8)
-ve 21 (67.7) 16 (53.3) 3 (42.9) - 40 (69.0)
Total 31 30 7 8
Table 1. Study population characteristics
Table 3. The association of Sapporo criteria fulfillment with
major clinical manifestations
Model 1: crude associations Model 2: adjusted for age at
diagnosis, gender, nationality Model 3: adjusted for covariates in
model 2 and follow-up response 1 DVT: deep vein thrombosis; PE:
pulmonary embolism 2 Analysis for recurrent DVT or PE was
restricted to 35 patients with previous DVT or PE event
Table 2. The serology results of the possible APS patients in
relation to their clinical manifestations (N=58)
Figure 1. The age distribution of definitive and possible APS
cases
-
Lessons learned
• Diagnosis is absolutely necessary for the proper clinical
management
• Lupus Anticoagulant is the “ identifier” or “ biomarker”
unique to the
Antiphospholipid syndrome and consider the
• Auto-antibodies that prolong clotting times in phospholipid
dependent
clotting assays are termed “lupus anticoagulant”
-
Special Coagulation Laboratory Recipe for APS diagnosis
• APTT clotting times must be prolonged at least twice control
plasma clotting times (correlates with high antibody titer)
• APTT prolonged clotting times does not correct in mixing
patient plasma with pooled normal plasma
• ELISA identifies beta2-glycoprotein 1 antigen and
auto-antibodies.
• Testing is repeated as indicated. • APS induced by viral or
bacterial proteins disappears after
infection is cured
-
SAUDI-APS RESEARCH GRUOP
-
AIMS of THE Saudi APS-Research Group :
• Describe outcomes of arterial venous and pregnancy
complications .
• Describe CAPS presentation in Saudi Population and the outcome
.
•Assess drug respond in APS . • assess quality of life /
depression in APS patients
• Role of genetics Factors of APS including familial and
sporadic cases
• Develop an APS registry and maybe guidelines under the
hematology society
• We need to manage getting different national /international
collaboration Centers onboard .
-
THANK YOU