Embed Size (px)
Citation preview

Managing the Unusual Airway:Case Studies in Complexity
Difficult airways are by definition complex to manage.
But some of these cases are more challenging
than others. We asked several clinicians to give
us examples of their more memorable airway cases.
61� Anesthesiology�news�guide � to�A irwAy�MAnAgeMent� 2010
Printer-Friendly�Version�At�Anesthesiologynews.CoM
62� trauma�and�tracheal�intubationJ. Antonio Aldrete, MD
63� Accessing�the�nasal�AirwayJeff E. Mandel, MD
64� Clearing�luminal�occlusionsThomas C. Mort, MD F. Luke Aldo, DO George W. Kopp, RRT
66� Videographic�evidence�of�regurgitation�And�Aspiration�despite�Cricoid�PressureRichard M. Cooper, BSc, MSc, MD, FRCPC
67� hypopharyngeal�stenosis�related�to�radiation�Masquerading�as�the�larynxAllan P. Reed, MD Elizabeth A.M. Frost, MD
68� Video�laryngoscopy�and�the�Pathologic�Airway�in�a�Pediatric�PatientCheryl K. Gooden, MD

Case�1
Trauma and Tracheal Intubation
J. Antonio Aldrete, Md Professor Emeritus
Department of Anesthesiology University of Alabama at Birmingham
Birmingham, Alabama
Dr. Aldrete has nothing to disclose.
Large trauma hospitals often receive challenging cases in which staff from anesthesiology, the trauma team, or emergency medicine—and sometimes all three—may be called to secure the airway and intubate patients with unusual foreign bodies in their faces.
These objects may impede the adaptation of a mask to the face and/or the insertion of a laryngoscope into the mouth. The gentle and gradual passing of an endo-tracheal tube while listening to the respiratory sounds was a technique mastered by N.A. Gillespie who sup-posedly always had a tube in his back pocket and sel-dom used a laryngoscope.1
More recently, a young male involved in an argu-ment ended up with a pocket knife stabbed into his left orbit.2 When he arrived at the emergency depart-ment, the knife was still in place (Figure 1). The weapon had been inserted at an acute angle so that the applica-tion of a mask was impossible. However, the right nos-tril remained accessible.
X-rays taken of the lateral view showed the tip of the knife located against the C1 vertebra (Figure 2). As a result, extending or flexing the neck might have pro-duced further injury.
With the head immobilized, after insufflating oxygen beside the patient’s face, benzocaine was sprayed into the right nostril. Two minutes later, a 6-mm nasotracheal tube was inserted through the nostril and advanced gradually, by the “Gillespie method” of listening to the breathing sounds transmitted through the tube as the tip approached the larynx.
At onset of inspiration, the tube was advanced promptly through the larynx, and 250 mg of propofol was administered. The tube cuff then was inflated and manual ventilation begun.
Although various endoscopic devices are available, procuring and preparing equipment takes time. With a knife blade in the eye, manipulation of an intubating
bronchoscope, which frequently requires 4 hands, could have proven difficult and damaging to the patient. Guid-ing the endotracheal tube by ear is a potentially lifesav-ing maneuver that clinicians should preserve.
referencesGillespie NA. Blind nasotracheal intubation. 1. Curr Res Anesth Analg. 1950:29(4):217-222.
Aldrete JA. Nasotracheal intubation. S2. urg Clin North Am. 1969;49(6):1209-1215.
Figure�1.�Patient�with�a�pocket�knife�in�the�left�eye.
Figure�2.�lateral�radiograph�of�patient�with�knife�in�face.
indePendently �deVeloPed�by �MCMAhon�Publ ishing62

Case�2
Accessing the Nasal AirwayJeff e. MAndel, Md
Clinical Associate of Anesthesiology and Critical Care Attending Anesthesiologist
Hospital of the University of Pennsylvania Clinical Associate in Anesthesiology and Critical Care,
University of Pennsylvania School of Medicine Philadelphia, Pennsylvania
Dr. Mandel has nothing to disclose.
A 25-year-old homeless man presented with an ulcerated fungating mass of his lower lip. On biopsy the mass, which had been growing over the previous 9 months, was identified as a squamous cell carcinoma invading the mandible.
Radical resection of the mandible with a free flap from the scapula was considered the best course of manage-ment. A tracheostomy was planned because postoper-ative airway compromise was likely. The patient spoke little English and was judged to be a poor candidate for awake tracheostomy or awake fiber-optic intubation.
As the tracheostomy was the initial procedure, on discussion with the surgical team, we proposed tra-cheostomy facilitated by placement of an LMA (LMA North America). Following topical anesthesia of the left nares, a 34 Fr Robertazzi airway was placed and the connector from an 8-mm endotracheal tube inserted to permit connection to the anesthesia circuit.
An inhalational induction was performed with 8% sevoflurane administered with a fresh gas flow of 12 L per minute. Mandibular advancement was performed to manage obstruction (Figure 1).
After 5 minutes, the patient was judged adequately anesthetized and a No. 5 LMA was placed. With the patient deeply anesthetized, a tracheostomy was per-formed. Fiber-optic confirmation of tracheal entry was performed, and a 6-mm wire-reinforced endotracheal tube was placed and sutured in position (Figure 2).
The patient then underwent the planned proce-dure, which was completed in 22 hours. The patient achieved lip occlusion and a normal facial contour, and his tracheostomy was decannulated uneventfully. How-ever, the patient was lost to follow-up as a result of his nomadic lifestyle.
Figure�1.�squamous�cell�carcinoma�invasive�to�jaw.
Figure�2.�inhalational�induction�via�nasal�airway.
� Anesthesiology�news�guide � to�A irwAy�MAnAgeMent� 2010 63

Case�3
Clearing Luminal OcclusionsthoMAs C. Mort, Md
Senior Associate in Anesthesiology Associate Director of the Surgical Intensive Care Unit
Associate Professor of Anesthesiology and Surgery University of Connecticut School of Medicine
Farmington, Connecticut
f. luke Aldo, do Resident in Anesthesiology
University of Connecticut School of Medicine, Farmington, Connecticut
GeorGe W. kopp, rrt Surgical Coordinator
Hartford Hospital Hartford, Connecticut
The authors have nothing to disclose.
Biofilm in the luminal wall and adherence of secre-tions within the endotracheal tube have been impli-cated in the development of ventilator-associated pneumonia, increased work of breathing, delay in extu-bation, and worse. Total or near-total luminal occlusion can present a situation requiring urgent or emergent airway control.
A 63-year-old, morbidly obese man was admitted to the intensive care unit with multifocal ischemic strokes. The patient had a history of obstructive sleep apnea and difficult mask ventilation and intubation. Of note, the patient had bitten his tongue, which caused bleed-ing that required frequent oropharyngeal suctioning.
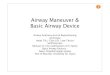
The patient was weaned off mechanical ventilation uneventfully over the next 4 days, at the end of which he underwent a trial with continuous positive airway pressure (CPAP). The patient immediately decompen-sated with hypertension, tachycardia, marked agita-tion, desaturation, and “gasping” respiration. Return to pressure-controlled mechanical ventilation revealed reduced tidal volumes (from 800 to 400 mL). Min-imal secretions were removed by suctioning of the tube, yet some resistance was noted on passing the suction catheter. Fiber-optic bronchoscopy revealed significant luminal narrowing resulting from accumula-tion of biofilm; brown tenacious secretions in the dis-tal lower lumen caused partial obstruction at various levels ( Figure 1).
Because of potential difficulty in exchanging the tube, a CAM Rescue Cath (Omneotech) was passed
Figure�1.�bronchoscopic�view�of�ett�lumen.�this�was�present�at�various�levels�in�the�distal�two-thirds�of�the�ett.�
ett, endotracheal tube
Figure�2.�secretion�specimen�removed�following�first�pass�of�CAM�rescue�Cath.
indePendently �deVeloPed�by �MCMAhon�Publ ishing64

twice to clear the obstructing secretions from the tube lumen (Figures 2 and 3). The procedure took less than 90 seconds, after which tidal volumes returned to the original 800 mL range and a subsequent trial with CPAP was uneventful.
A similar episode of severe agitation and “gasp-ing” respiration occurred 34 hours later during a trial of CPAP. Bronchoscopy revealed reaccumulation of biofilm and obstructing secretions in a different pat-tern ( Figure 4). Because the CAM Rescue Cath was not available, bronchoscopy was used to clear the biofilm. During the 30-minute procedure, secretion manipu-lation led to 2 episodes of complete occlusion of the tube, as well as brief desaturation and multiple high-pressure alarms.
Build-up of biofilm and thick secretions obstruct-ing a tracheostomy or endotracheal tube can dramati-cally decrease tidal volumes, increase airway resistance, and lead to catastrophic blockage. Incorporating tradi-tional suction catheters may be ineffective, and bron-choscopy, extubation, tube exchange, and reintubation carry significant costs and hazards for patients.
Figure�4.�reaccumulation�of�obstructing�biofilm�and�secretions.
Figure�3.�luminal�patency:�single-pass�improvement�with�CAM�rescue�Cath.�
Proper luminal hygiene is a patient safety concept that has received little attention yet may lead to cata-strophic consequences if ignored. Technology such as the CAM Rescue Cath for improved luminal hygiene is a step in the right direction toward tackling the impor-tant clinical problem of excessive accumulation of bio-film and secretions.
referencesKapadia FN. Factors associated with blocked tracheal tubes. 1. Intensive Care Med. 2001;27(10):1679-1681.
Boqué MC, Gualis B, Sandiumenge A, Rello J. Endotracheal tube 2. intraluminal diameter narrowing after mechanical ventilation: use of acoustic reflectometry. Intensive Care Med. 2004;30(12):2204-2209.
Kirton OC, DeHaven CB, Morgan JP, Windsor J, Civetta JM. 3. Elevated imposed work of breathing, masquerading as ventilator weaning intolerance. Chest. 1995;108(4):1021-1025.
Leiman BC, Katz J, Stanley TH, Butler BD. Removal of tracheal 4. secretions in anesthetized dogs: balloon catheters versus suction. Anesth Analg. 1987;66(6):529-532.
Shah C, Kollef MH. Endotracheal tube intraluminal volume loss 5. among mechanically ventilated patients. Crit Care Med. 2004; 32(1): 120-125.
� Anesthes iology�news�guide � to�A irwAy�MAnAgeMent� 2010 65

Case�4
Videographic Evidence of Regurgitation and Aspiration
Despite Cricoid PressureriChArd M. Cooper, BsC, MsC, Md, frCpC
Professor of Anesthesia, University of Toronto Director, University Health Network, Anesthesia Airway
Fellowship, Toronto General Hospital Toronto, Canada
Dr. Cooper is an unpaid consultant to Verathon Medical.
An elderly woman presented to the operating room with progressive abdominal pain and marked disten-sion. She had been admitted to the hospital and was found to have a small bowel obstruction that failed con-servative management. A nasogastric tube was drain-ing bile-stained gastric fluid. Intravenous and arterial catheters were placed, in addition to the standard monitors. The nasogastric tube was aspirated and sub-sequently allowed to drain freely. The staff anesthesi-ologist located the cricoid cartilage and an assistant’s fingers were positioned appropriately.
Pre-oxygenation was continued for approximately 3 minutes, followed by the cautious administration of fen-tanyl, propofol, and rocuronium (1 mg/kg); during this time, progressive force was applied to the cricoid car-tilage. As the oxygen saturation began to fall, gentle bag mask ventilation was provided while cricoid pres-sure (CP) was maintained. An anesthesia resident with experience in using the GlideScope video laryngoscope (Verathon Medical) performed laryngoscopy. This pro-vided a good laryngeal view; however, gastric contents that pooled in the oropharynx were suctioned with a Yankauer device, but quickly recurred. Eventually, endo-tracheal intubation was attempted, but the resident encountered minor difficulties when introducing and advancing the endotracheal tube.
A gastric volvulus was identified but resection was not required. Postoperatively, ventilation was continued for 2 hours to ensure that the patient’s condition did not deteriorate further. She was then extubated with-out complications.
Sellick was not the first to advocate CP, but since his published paper of 1961,1 the technique has been the cornerstone of “rapid sequence induction/intuba-tion,” despite being based on relatively poor science. The amount of pressure required has been variously described as firm, painful, and 20 to 44 newtons. Most
practitioners have no idea whether they are applying insufficient or excessive pressure, and the procedure is both difficult to teach and monitor. CP may provoke retching, relaxation of the lower esophageal sphinc-ter, interference with insertion of the laryngoscope, or impairment of the laryngeal view, and may even obstruct the airway.2
Several fundamental faults of the practice can be identified, including the possibility that the cricoid car-tilage may be insufficiently rigid to achieve esophageal occlusion3 and that it may not predictably overlie the esophagus.4
There is a growing body of literature questioning the efficacy of CP.2,5-7 However, it is unlikely that a con-trolled study would be sanctioned by a research ethics board. Effective or not, CP is likely to remain a standard of practice because we cannot completely disprove its value and there may not be a better option.
Assuming that CP will be performed, what is the safest way to proceed with endotracheal intubation when managing a patient with an indwelling nasogastric tube? The presence of a nasogastric tube in the esoph-agus may breach the integrity of the lower esophageal sphincter, and by acting as a capillary tube, encour-age regurgitation. This is particularly likely if there is an upper gastrointestinal obstruction and associated raised intragastric pressure. It also may interfere with the application of an occlusive force to the esophagus.
If the tube is functioning, should it be suctioned and removed, attached to continuous suction, left in situ but open to vent increased intra-abdominal pres-sure? Should the patient be positioned head down to reduce the risk for aspiration, or head up to reduce the risk for regurgitation? If CP interferes with insertion of
Figure.�GlideScope image showing presence of gastric con-tents welling up in the hypopharynx despite the application of cricoid pressure and a properly posi-tioned, free-draining nasogastric tube. (The continuous stream of regurgitation is more apparent in the video footage.)
indePendently �deVeloPed�by �MCMAhon�Publ ishing66

the laryngoscope or the laryngeal view, should it be released? If intubation cannot be achieved and inser-tion of a supraglottic airway device is required, should the CP be released to facilitate placement and reap-plied—with the risk for dislodging the airway? If gas-tric contents are viewed in the oropharynx, should this be suctioned, thereby delaying intubation? Should the endotracheal tube cuff be inflated with saline rather than air to achieve a more complete seal?
In this case, we used a GlideScope, which provided an excellent laryngeal view and allowed the image to be captured. Although it was not our intention, this enabled us to document the ineffectiveness of CP (which was apparently applied appropriately). Unfor-tunately, the difficulty that the resident encountered in delivering and advancing the endotracheal tube may have contributed to the magnitude of the aspira-tion. This case raises several interesting questions that, hopefully, will stimulate thought about how to best manage such a patient.
A video of this case can be viewed at www.AnesthesiologyNews.com.
referencesSellick BA. Cricoid pressure to control regurgitation of stomach 1. contents during induction of anaesthesia. Lancet. 1961; 2(7199): 404-406.
Ovassapian A, Salem MR. Sellick’s maneuver: to do or not do. 2. Anesth Analg. 2009; 109(5):1360-1362.
Palmer JHM, Ball DR. The effect of cricoid pressure on the cricoid 3. cartilage and vocal cords: an endoscopic study in anaesthetised patients. Anaesthesia. 2000;55(3):263-268.
Smith KJ, Dobranowski J, Yip G, Dauphin A, Choi PT. Cricoid 4. pressure displaces the esophagus: an observational study using magnetic resonance imaging. Anesthesiology. 2003;99(1):60-64.
Lerman J. Is cricoid pressure necessary? 5. Paediatr Anaesth. 2002; 12(7): 655.
Maltby JR, Beriault MT. Science, pseudoscience and Sellick. 6. Can J Anesth. 2002;49(5):443-447.
Neilipovitz DT, Crosby ET. No evidence for decreased incidence 7. of aspiration after rapid sequence induction. Can J Anesth. 2007; 54(9): 748-764.
Case�5
Hypopharyngeal Stenosis Related to Radiation
Masquerading as the LarynxAllAn p. reed, Md
elizABeth A.M. frost, MdDepartment of Anesthesiology
Mount Sinai School of Medicine New York, New York
The authors have nothing to disclose.
A 66-year-old man presented for direct suspension laryngoscopy and laser excision of diagnosed hypo-pharyngeal stenosis. He complained of mild difficulty swallowing and dysphonia. The patient had undergone chemotherapy and cervical radiation for laryngeal can-cer. The airway examination was within normal limits for all parameters.
After preoxygenation and induction, the ability to perform bag-mask ventilation was confirmed. Laryn-goscopy was performed using a Macintosh 3 blade, revealing an aperture within midline pink tissue, and an anterosuperior tissue flap suggesting an edematous
larynx and epiglottis. Because of concerns regarding the anatomic appearance, a tracheal tube was not passed. Bag-mask ventilation was re-initiated, followed by flexi-ble fiber-optic laryngoscopy. An aperture was identified and the fiberscope was passed through this opening. Immediately after, a well-defined larynx was visualized and intubation successfully achieved.
Figure.�Postradiation�hypopharyn-geal�stenosis�masquerading�as�the�larynx.�A tracheal tube with its pilot balloon tube traverses the stenosis. A tissue flap above the tracheal tube resembles the epiglottis. Lateral and posterior tissues resemble edematous laryngeal mucosa.
� Anesthes iology�news�guide � to�A irwAy�MAnAgeMent� 2010 67

The first choice of a 4.5 cuffed tube was too large; a size 3.5 cuffed tube ultimately was used and was sutured in place by the surgeon. Extubation of the tra-chea occurred the following day under the guidance of the anesthesia team.
The extremely challenging nature of this airway resulted from the small mouth opening, micrognathia, and limited area of the oropharynx secondary to the encroaching soft tissue. From the perspectives of both the anesthesiologist and the surgeon, a greater appreci-ation of this patient’s airway was obtained through the use of video laryngoscopy.
Figure�2.�hypoplasia�of�the�mandible.
(Image courtesy of Peter J. Taub, MD, Mount Sinai Medical Center, New York, NY).
Case�6
Video Laryngoscopy and The Pathologic Airway
In a Pediatric PatientCheryl k. Gooden, Md
Associate Professor of Anesthesiology & Pediatrics Mount Sinai School of Medicine
New York, New York
Dr. Gooden has received equipment support from Verathon Medical.
A 4-year-old, 12-kg female patient with Pierre Robin Sequence presented for mandible reconstruction with distraction. Past medical and surgical history was sig-nificant for airway obstruction requiring an emergent tracheostomy on her first day of life. A gastrostomy tube was placed when the child was 1 week old. At 10 months, she underwent mandible reconstruction but remains severely micrognathic. Approximately 2 years ago, she was decannulated and the tracheostomy site was closed. Subsequently, she was scheduled for fur-ther mandible surgery but unsuccessful attempts at intubation at another institution required cancellation of the proposed procedure.
Examination revealed a Mallampati class IV airway with a mouth opening of less than 1 cm. A difficult air-way was anticipated based on clinical features and past anesthesia history. The rest of her physical examination was unremarkable.
Preparation of the operating room included stocking various sizes of endotracheal tubes, airway devices, and equipment in the event they were needed. A tracheos-tomy set also was made available for use.
When the patient arrived in the operating room, standard monitors were placed, followed by insertion of an IV catheter and the administration of glycopyrro-late. Anesthesia was induced with 70% nitrous oxide in oxygen and 8% sevoflurane through a face mask. The patient was able to breathe spontaneously.
Once an adequate depth of anesthesia was obtained, the small mouth opening was appreciated. Direct laryn-goscopy was attempted but produced no view of the airway. The next choice of airway device was a Glide-Scope (Verathon Medical) with the Cobalt blade No. 2. Advancing the blade revealed a narrow oropharynx sur-rounded by redundant soft tissue and tonsils. Visualiza-tion of the vocal cords proved challenging and required external laryngeal manipulation. The trachea was devi-ated to the left side.
Figure�1.��Four-year-old�girl�with�micrognathia.�
indePendently �deVeloPed�by �MCMAhon�Publ ishing68