Embed Size (px)
Citation preview

Balanced information for better care
Managing pain without overusing opioidsImplementing safe, effective, and less risky analgesic strategies

2 Managing pain without overusing opioids
Opioids in America: increasing use, increasing complications• Pain is the most common reason for physician visits.1
• Over 100 million Americans suffer from some form of chronic pain.2
• In the 1990s, concern about under-treatment of pain and the introduction of new opioid products were followed by a surge in the use of prescribed opioids.
FIGURE 1. Opioid pain medication use increased sharply, as did deaths caused by prescription pain medications and admissions for the treatment or abuse of these products.3
Prescribed opioid deaths/100,000
Treatment admissions/10,000
Prescribed opioid sales kg/10,000
1999 2001 2003 2005 2007 2009
Year
8
7
6
5
4
3
2
1
0
Rat
e
The increase in dependence, morbidity, and mortality caused by opioid analgesics has prompted a reassessment of the appropriate role of these medications in managing both acute and chronic pain.
* Age-adjusted rates per 100,000 population for prescribed opioid deaths, crude rates per 10,000 population for treatment admissions related to prescribed opioid abuse, and crude rates per 10,000 population for kilograms of prescribed opioid sold.

Alosa Foundation | Balanced information for better care 3
Limit the quantity and duration of opioids in acute painMost acute pain is self-limited.
Initial management of acute pain should include:
• non-pharmacologic options (R.I.C.E.—Rest, Ice, Compression, Elevation)
• pharmacologic options (acetaminophen or non-steroidal anti-inflammatory (NSAIDs))
Only the small minority of patients with severe pain will require an opioid.
Principles for prescribing opioids for acute pain:
• Use a low dose.
• Use an immediate release formulation.
• For those who need opioids, 2-3 days of treatment will usually suffice.
Leftover opioids become an opportunity for diversion or other misuse.
• In one state study, 20.8% of the population received an opioid prescription in a year. Over half the patients with unused medications kept them.5
• Over half of people using prescription opioids for non-medical purposes got the drug from friends or family.6
FIGURE 2. In a recent study of patients prescribed opioids after outpatient orthopedic surgery, almost half of patients used less than 5 pills from the average of 30 dispensed.4
0
% S
ub
ject
s
Number of pills used
50
40
30
20
10
0-5 6-10 11-15 16-20 21-25 26-30 ≥31
On average, 19 pills
per patient were unused.

4 Managing pain without overusing opioids
Higher doses = higher risk
The risk of complications from opioids rises with doses over 100 mg morphine-equivalent dose daily.
Or use dose calculator online: http://agencymeddirectors.wa.gov/mobile.html
Increases noted above are for patients taking >100mg morphine-equivalent dose per day (see below).
• misuse, abuse, addiction7
• chronic constipation8
• intentional or accidental overdose9
• falls and fractures (especially in the elderly) at initiation and dose increase10
• low testosterone11
!Risks of opioid use include:
6.1%
40-50%
1.8%
4.7%
19.3%
100 mg morphine-equivalent dose =
fentanyl (mcg/hr)
>37hydrocodone
100 mgoxycodone
65 mghydromorphone
25 mg

Alosa Foundation | Balanced information for better care 5
Opioids for chronic pain:
Little evidence of efficacy, considerable evidence for harm
All randomized trials of opioids in chronic pain lasted for only 16 weeks or less; average trial lasted for 5 weeks.12
FIGURE 3. Weighing the risks and benefits of chronic opioid use
TABLE 1. Among studies that do exist, opioids, especially strong opioids, can reduce pain scores, but a reduction in pain does not translate to functional gain.12
Opioids v placebo -0.6 (-0.69, -0.50) -0.31 (-0.41, -0.22)
Opioids v NSAIDs or TCAs -0.05 (-0.32, 0.21) 0.16 (0.03, 0.30)
Strong opioids v NSAIDs or TCAs (e.g. morphine, oxycodone) -0.34 (-0.67, -0.01) 0.0 (-0.35, 0.35)
AVERAGE EFFECTPain (95% CI) Function (95% CI)
1. Negative results favor opioids; positive results favor the comparator.
2. Over 30% of patients dropped out of the studies, due to side effects and/or inadequate pain relief in the opioid group.
High rate of adverse effects
Little evidence of long-term benefit

6 Managing pain without overusing opioids
Initial management of chronic painR
EASSESS REGULARLY REASSESS REGULAR
LY
For example:• participation in physical therapy• sleeping in a bed, instead of a chair
Orient treatment around functional goals.
Y N
Increase, add, or change therapy.
Continue or taper therapy.
Is the patient meeting functional goals?
Select one or more treatment options.
Non-Pharmacologic
• exercise
• weight training
• yoga
• massage
• Tai Chi
• relaxation
• cognitive behavior therapy
Pharmacologic
Match to cause of pain:
• SNRIs
• antiepileptics
• tricyclic antidepressants (TCAs)
• lidocaine patches

Alosa Foundation | Balanced information for better care 7
Initial management of chronic pain
N
Y Start opioid therapy:
• Start low and go slow.
• No opioid is more effective than another.
• No benefit from using a long-acting or extended release product.14
Are opioids an option, with increased monitoring?
• Explore or revisit previous treatments.
• Consider other non-opioid treatment options.
• Refer to pain specialist.
• Alcohol use
• Benzodiazepines and other drug use
• Clearance and metabolism of the drug
• Delirium, dementia, and falls risk
• Psychiatric comorbidities
• Query the prescription monitoring program
• Respiratory insufficiency and sleep apnea
• Safe driving, work, storage, and disposal
Complete ABCDPQRS opioid risk assessment:13
Does pain still impede functional improvement despite optimizing therapy?
Evaluate whether opioid therapy may be required.
Is the patient at high risk of opioid-induced problems?
NY
Continue to reassess progress towards functional goals.

8 Managing pain without overusing opioids
Implement a system for opioid monitoringIf patients require ongoing use of opioid medications, a monitoring system can help guide progress and identify problems.
Determine if patient is progressing toward functional goals.Activity
Evaluate the patient to determine response to treatment.Analgesia
A dverse effects
If you suspect abuse:
1. Use a screening tool like the Opioid Risk Tool (ORT).
2. Discuss concern with the patient.
3. Review expectations from pain management plan.
4. Increase monitoring: urine screens, pill counts, reviewing the patient’s profile in the prescription monitoring program.
Abuse
• constipation
• nausea or vomiting
• sedation
• pruritus
• hallucination or dysphoria
• sexual dysfunction
FIGURE 4. Example of a monitoring approach
Resources for patients with substance abuse:
• Substance abuse treatment in your office: Screening, Brief Intervention, and Referral to Treatment (SBIRT) Materials and training available at: integration.samhsa.gov/clinical-practice/SBIRT
• SAMHSA’s Behavioral Health Treatment Locator—findtreatment.samhsa.gov Helpline at 1-800-662-HELP (1-800-662-4357)

Alosa Foundation | Balanced information for better care 9
Improving the safety of opioid use
Use prescription monitoring programs to enhance safety and improve communication.
Prescribers can review a patient’s prescription opioid-use history:
• provides a platform for discussion with patient about pain medication use
• enhances coordination of care between providers
• identifies combinations of medications that may be problematic or put patient at risk of overdose
Challenges:
• Federal programs do not report to state prescription monitoring programs (Veterans Affairs, Department of Defense, Indian Health Services).
• Data is not yet real time.
Identify and reduce risk of opioid overdose.
Educate patient and family on signs of opioid overdose.
1. Emphasize the need to take as prescribed.
2. Keep track of how frequently as needed medications are taken.
Consider prescribing the opioid antagonist naloxone (Narcan) for:
• anyone on >50mg morphine equivalents daily
• patients on opioids with:
— renal dysfunction or hepatic disease
— concurrent benzodiazepine or antidepressant use
• patients or caregivers, upon request
Be sure to instruct patients on how to administer naloxone (Narcan).
10 Managing pain without overusing opioids
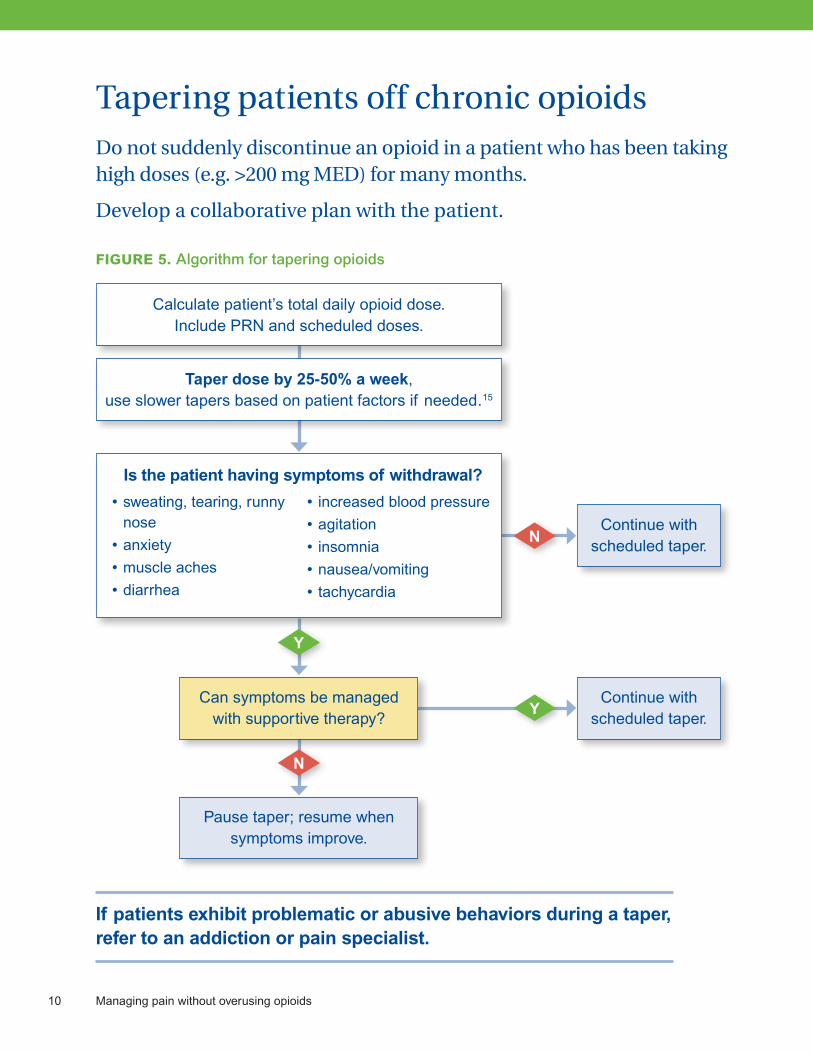
Tapering patients off chronic opioidsDo not suddenly discontinue an opioid in a patient who has been taking high doses (e.g. >200 mg MED) for many months.
Develop a collaborative plan with the patient.
FIGURE 5. Algorithm for tapering opioids
Y
N
N
Y
Pause taper; resume when symptoms improve.
Calculate patient’s total daily opioid dose. Include PRN and scheduled doses.
Taper dose by 25-50% a week, use slower tapers based on patient factors if needed.15
• sweating, tearing, runny nose
• anxiety
• muscle aches
• diarrhea
• increased blood pressure
• agitation
• insomnia
• nausea/vomiting
• tachycardia
Is the patient having symptoms of withdrawal?
Can symptoms be managed with supportive therapy?
Continue with scheduled taper.
Continue with scheduled taper.
If patients exhibit problematic or abusive behaviors during a taper, refer to an addiction or pain specialist.

Alosa Foundation | Balanced information for better care 11
SummaryAcute pain:
• Acute pain usually responds well to non-pharmacologic approaches, NSAIDs, and acetaminophen. Use opioids only when acute pain is severe, and prescribe limited amounts of opioids, for short durations.
Chronic non-cancer pain:
• First, optimize pharmacologic and non-pharmacologic alternatives to opioids; resort to chronic opioid therapy only for severe pain when other alternatives are inadequate.
• Screen patients for risk of abuse or misuse before writing an opioid prescription. Periodically re-screen during treatment. Counsel patients about opioid side effects, safe storage, and disposal.
• If opioids are prescribed, set clear functional goals and realistic expectations as part of a comprehensive pain management plan. Opioids will generally not return the patient to normal function, and may even reduce functional status.
• Taper and discontinue opioids whenever possible, and particularly in patients who have significant side effects or exhibit problematic behavior.
• Refer patients to a chronic pain or addiction specialist for advice if the patient does not achieve functional goals or shows signs of problematic behavior.
References:(1) Fox CD, Berger D, Fine P, et al. Pain assessment and treatment in the managed care environment: a position statement from the American Pain Society. Glenview, IL: American Pain Society; 2000. (2) Institute of Medicine. Relieving pain in American: a blueprint for transforming prevention, care, education, and research. June 2011. (3) Centers for Disease Control & Prevention. Vital signs: overdoses of prescription opioid pain relievers—United States, 1999-2008. MMWR. Morbidity and mortality weekly report. 2011;60(43):1487-1492. (4) Rodgers J, Cunningham K, Fitzgerald K, Finnerty E. Opioid consumption following outpatient upper extremity surgery. The Journal of hand surgery. 2012;37(4):645-650. (5) Centers for Disease Control & Prevention. Adult use of prescription opioid pain medications—Utah, 2008. MMWR. Morbidity and mortality weekly report. 2010;59(6):153-157. (6) McCabe SE, West BT, Boyd CJ. Leftover prescription opioids and nonmedical use among high school seniors: a multi-cohort national study. The Journal of adolescent health: official publication of the Society for Adolescent Medicine. 2013;52(4):480-485. (7) Edlund MJ, Martin BC, Russo JE, DeVries A, Braden JB, Sullivan MD. The role of opioid prescription in incident opioid abuse and dependence among individuals with chronic noncancer pain: the role of opioid prescription. The Clinical Journal of Pain. 2014;30(7):557-564. (8) Coyne KS, LoCasale RJ, Datto CJ, Sexton CC, Yeomans K, Tack J. Opioid-induced constipation in patients with chronic noncancer pain in the USA, Canada, Germany, and the UK: descriptive analysis of baseline patient-reported outcomes and retrospective chart review. ClinicoEconomics and outcomes research: CEOR. 2014;6:269-281. (9) Dunn KM, Saunders KW, Rutter CM, et al. Opioid prescriptions for chronic pain and overdose: a cohort study. Annals of internal medicine. 2010;152(2):85-92. (10) Miller M, Sturmer T, Azrael D, Levin R, Solomon DH. Opioid analgesics and the risk of fractures in older adults with arthritis. Journal of the American Geriatrics Society. 2011;59(3):430-438. (11) Deyo RA, Smith DH, Johnson ES, et al. Prescription opioids for back pain and use of medications for erectile dysfunction. Spine. 2013;38(11):909-915. (12) Furlan AD, Sandoval JA, Mailis-Gagnon A, Tunks E. Opioids for chronic noncancer pain: a meta-analysis of effectiveness and side effects. CMAJ. 2006;174(11):1589-1594. (13) Thorson D, Biewen P, Bonte B, Epstein H, Haake B, Hansen C, Hooten M, Hora J, Johnson C, Keeling F, Kokayeff A, Krebs E, Myers C, Nelson B, Noonan MP, Reznikoff C, Thiel M, Trujillo A, Van Pelt S, Wainio J. Institute for Clinical Systems Improvement. Acute Pain Assessment and Opioid Prescribing Protocol. Published January 2014. (14) Pedersen L, et al. A randomized, double-blind, double-dummy comparison of short- and long-acting dihydrocodeine in chronic non-malignant pain. Pain. 2014;155(5):881-8. (15) Chou R, Fanciullo GJ, Fine PG, et al. Clinical guidelines for the use of chronic opioid therapy in chronic noncancer pain. J Pain. 2009;10(2):113-130.

Copyright 2015 by the Alosa Foundation. All rights reserved.
These are general recommendations only; specific clinical decisions should be made by the treating physician based on an individual patient’s clinical condition. More detailed information on this topic is provided in a longer evidence document at alosafoundation.org.
About this publication
The Independent Drug Information Service (IDIS) is supported by the Massachusetts Department of Public Health and the PACE Program of the Department of Aging of the Commonwealth of Pennsylvania.
This material is provided by the Alosa Foundation, a nonprofit organization which is not affiliated with any pharmaceutical company. IDIS is a program of the Alosa Foundation.
This material was produced by Brian Bateman, M.D., M.Sc., Assistant Professor of Anesthesia, Jerry Avorn, M.D., Professor of Medicine, Michael A. Fischer, M.D., M.S., Associate Professor of Medicine, Niteesh K. Choudhry, M.D., Ph.D., Associate Professor of Medicine, all at Harvard Medical School; Eimir Hurley, BSc (Pharm), MBiostat, Program Director, Ellen Dancel, PharmD, MPH, Director of Clinical Material Development, both at the Alosa Foundation. Drs. Avorn, Bateman, Choudhry, and Fischer are all physicians at the Brigham and Women’s Hospital in Boston. None of the authors accepts any personal compensation from any drug company.
Medical writer: Stephen Braun.