Embed Size (px)
Citation preview
AddingtonAddington HospitalHospital
Managing Clinical Adverse EventsPresented by:
Dr J Hurst – Hospital ManagerMrs M Chinniah – Nursing & Quality Manager
19 January 2005WHO World Alliance for Patients Safety Meeting
Durban
ADDINGTON HOSPITALVISION
To achieve a quality health service through innovative and dynamic healthcare leadership.
MISSION STATEMENT
Addington Hospital is committed to providing a safe, legal, ethical, quality patient focusseddistrict and regional health service through the integration of the Batho Pele, Good Governance and Accreditation programmes, supported by information technology to achieve:
optimal, cost-effective clinical outcomes for patients within the available resources and current provincial health policy;
attraction and retention of talented staff by providing an exceptional work environment conducive to staff well being, participation, development, learning and research;
enhanced customer satisfaction ensuring the dignity and rights of patients, staff and other customers;
sound financial management;
improved co-ordination and communication with stakeholders including the promotion of partnerships with the Community and the eThekwini District Health Office.
HOSPITAL MANAGER
CORE VALUES
INTEGRITY
TRUSTWORTHY
CO-OPERATIVE GOVERNANCE
SELF AWARENESS
TEAM WORK
COMPASSIONATE CARING
ACCOUNTABILITY
DEDICATION
ENTHUSIASM
APPROACHABILITY
Some Background InformationSome Background Information
Situated on Durban’s famous Golden MileBuilt on present site in 1897 and has undergone many additions to the original complexKwaZulu Natal Public Sector Hospital

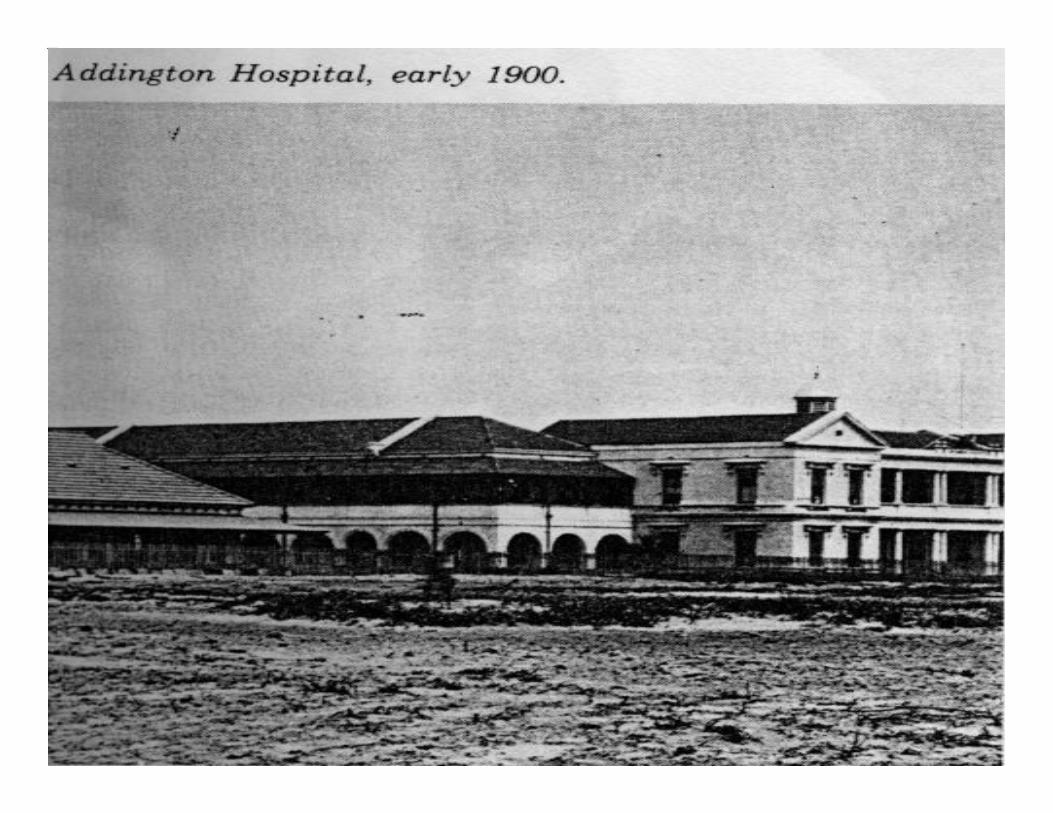
1861
First Government Hospital
Durban - Bayside

2004Hospital Beds – 512Average Occupancy Rate – 94%Admissions p.a. – 31,630Outpatients p.a. – 350,083Staff - 2500
Some Background InformationSome Background InformationContCont……....

Some Background InformationSome Background InformationContCont……....
Services offered by the Hospital:Obs/Gynae, Paediatrics, DentalGeneral Surgery, Orthopaedics, Ophthalmology, ENT, Urology,Radiotherapy and Oncology, Critical Care ServicesRehabilitative Services: Physiotherapy, Occupational Therapy, Speech TherapySupport Services: Radiology, Nuclear Medicine, Pharmacy, Anaesthetic, Laboratory, Social Work, DieteticsSpecial programmes: Prevention of Mother to Child Transmission, Voluntary Counselling and Testing, Antiretroviral rollout programme, HIV/AIDS Resource Centre, Advice Desk for Abused,Crisis Centre (Post Exposure Prophylaxis)

First Phase

Path Through Adverse EventsPath Through Adverse EventsFirst PhaseFirst Phase
Incident Reporting but on adhoc/crises intervention basis
No structured, formalised process of collation, analysis and monitoring of trends for remediation
Not integrated into Quality and Risk Management
No “Buy-in “ – Casemix/Abstracting Module

Second Phase

Path Through Adverse EventsPath Through Adverse EventsSecond PhaseSecond Phase
Re-entry into Accreditation Programme
Quality Steering Committee
In-house Risk Manager
Case Manager
Literature search for a model for Adverse Event Reporting and Monitoring
Path through Adverse Events
The Changing approach
Third Phase
Towards a Culture of Safety

Path Through Adverse EventsPath Through Adverse EventsThird PhaseThird Phase
Adapted and Adopted Adverse Event reporting and Monitoring Model
Policies and Procedures:
Quality Management and Improvement Strategy and Programme
Risk Management Strategy and Programme
Adverse Event Reporting and Monitoring
Policy Statement:Policy Statement:Quality Management and improvement Quality Management and improvement strategy and strategy and ProgrammeProgramme –– July 2003July 2003
PURPOSE: The provision of a framework for the Hospital and
the leaders to provide Patient Care in a well managed environment.
Prioritised focus for Clinical areas: Clinical audit including Adverse Events reporting and monitoring
QUALITYSAFE

Policy Statement:Policy Statement:Risk Management Strategy and Risk Management Strategy and
ProgrammeProgramme –– Jan 2004Jan 2004
1. PURPOSE: The provision of a framework to Identify, Analyse and Evaluate risks so as to reduce the frequency, severity and impact of all incidents, accidents and injuries.
2. Definition of Risk: Risk is the presence of uncertainty and it is measured as the deviation from the expected outcome of a given situation or event.
3. Definition of Risk Management: A planned Programme to prevent loss and control liability.
4. Implementation of Integrated Clinical Risk Management Model.

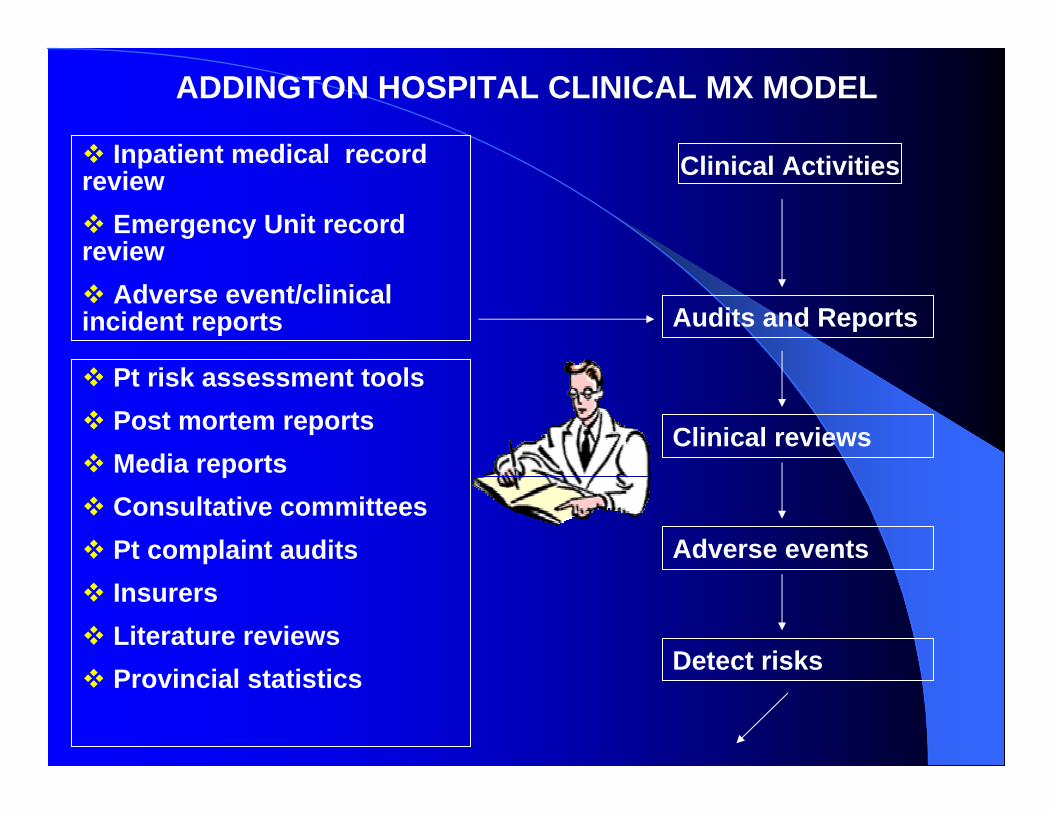
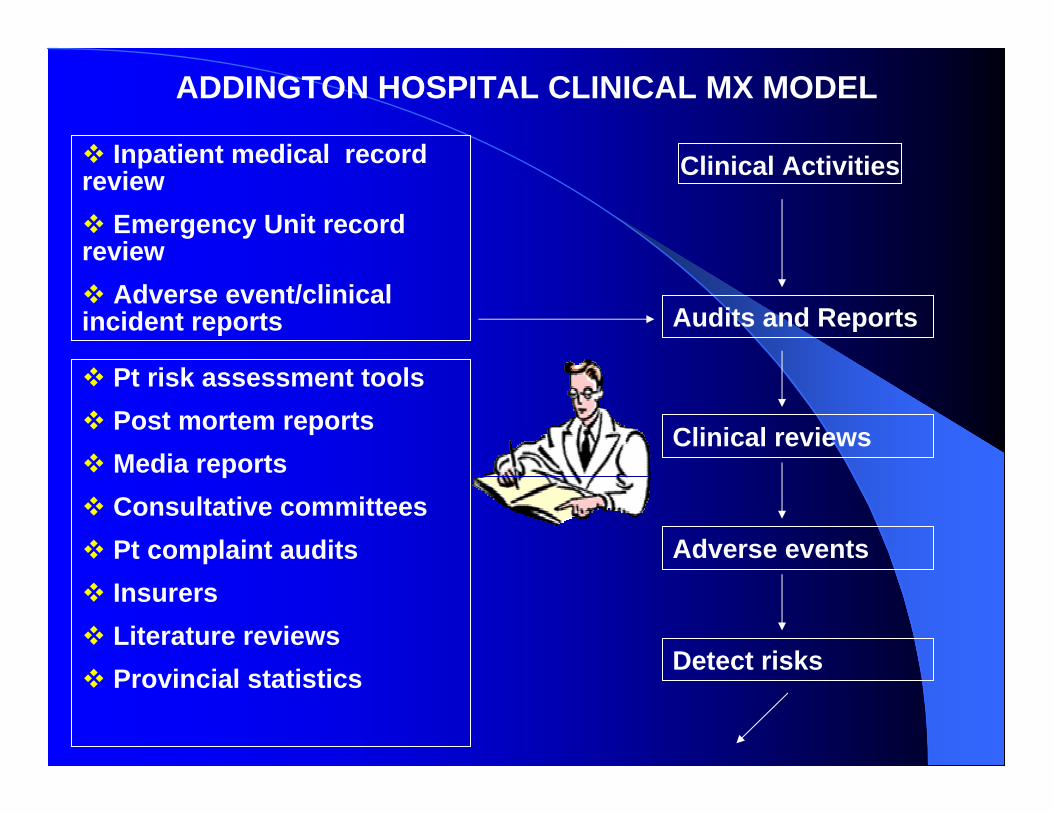
ADDINGTON HOSPITAL CLINICAL MX MODEL
Inpatient medical record review
Emergency Unit record review
Adverse event/clinical incident reports
Clinical Activities
Audits and Reports
Pt risk assessment tools Post mortem reportsMedia reports Consultative committees Pt complaint audits InsurersLiterature reviewsProvincial statistics
Clinical reviews
Adverse events
Detect risks
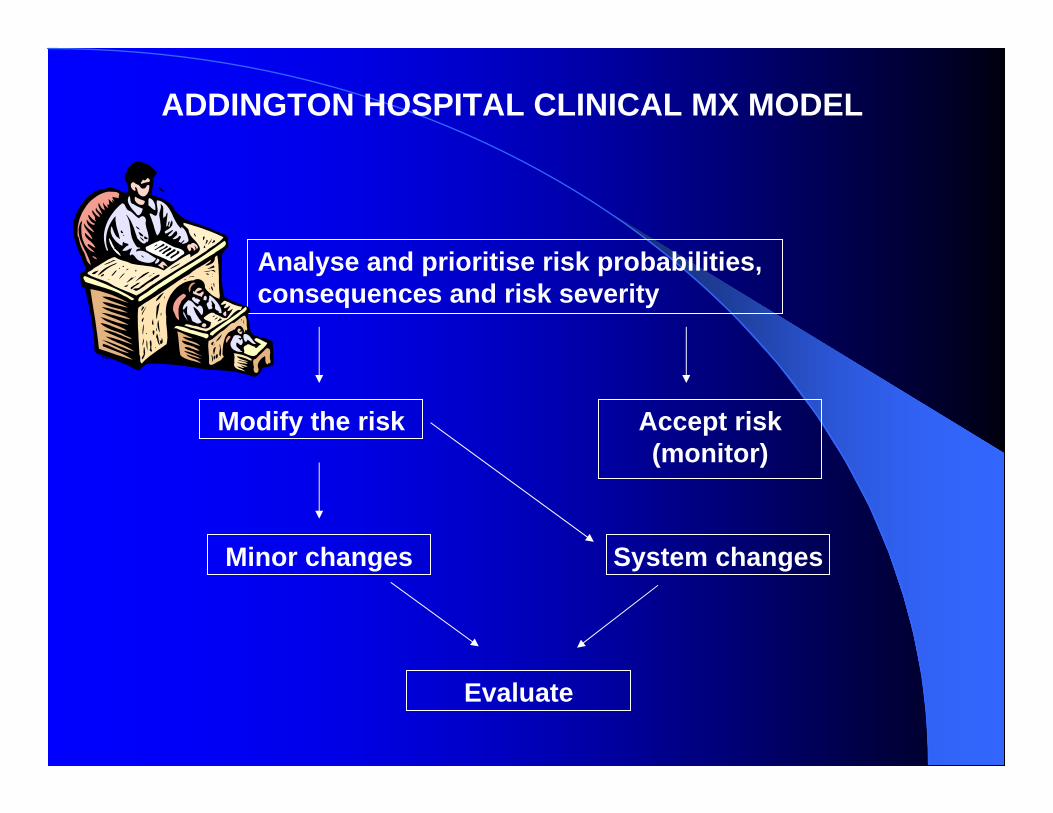
ADDINGTON HOSPITAL CLINICAL MX MODEL
Analyse and prioritise risk probabilities, consequences and risk severity
Modify the risk Accept risk(monitor)
System changesMinor changes
Evaluate
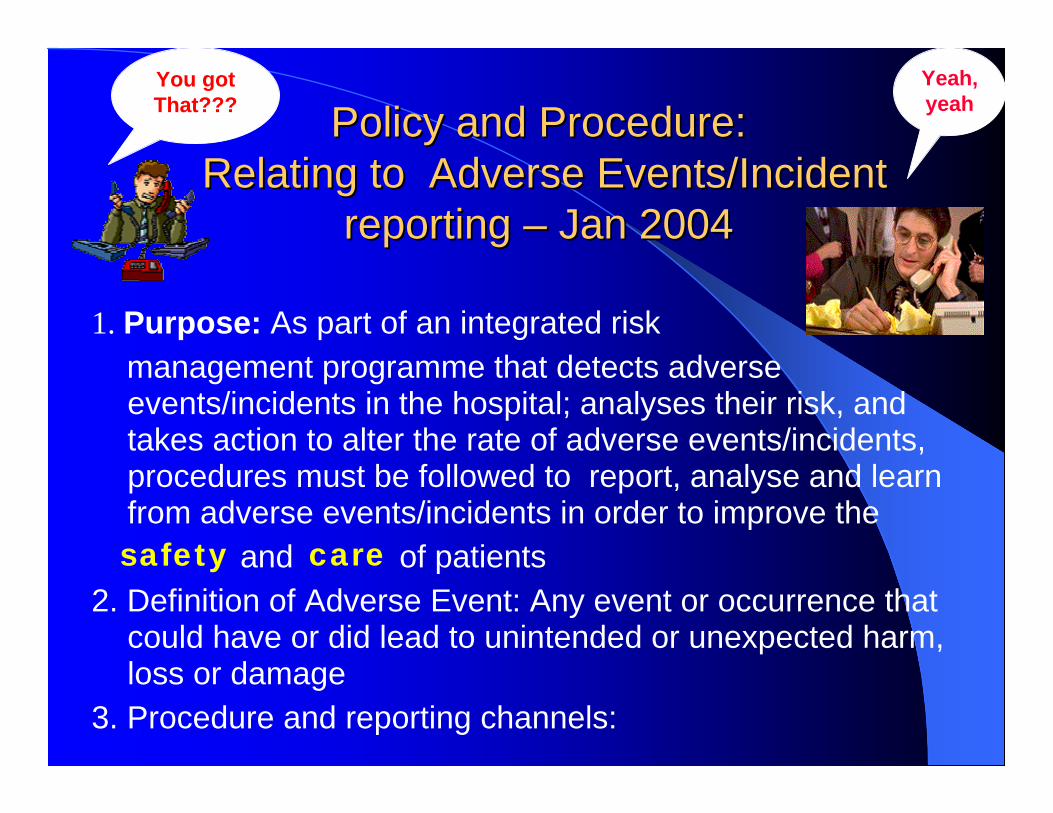
Policy and Procedure:Policy and Procedure:Relating to Adverse Events/Incident Relating to Adverse Events/Incident
reporting reporting –– Jan 2004Jan 2004
1. Purpose: As part of an integrated risk management programme that detects adverse events/incidents in the hospital; analyses their risk, and takes action to alter the rate of adverse events/incidents, procedures must be followed to report, analyse and learn from adverse events/incidents in order to improve the
and of patients2. Definition of Adverse Event: Any event or occurrence that
could have or did lead to unintended or unexpected harm, loss or damage
3. Procedure and reporting channels:
safety care
You got That???
Yeah,yeah

NOTIFICATION OF AN INCIDENT
(To be completed within 3 hours of occurrence)
Ward/department: _______________________
Date of incident: ________________________ Time of incident: ___________________________
Name of patient: __________________________________________________________________
File number: ___________________________
Diagnosis: _______________________________________________________________________
Brief description of incident:
________________________________________________________________________________
________________________________________________________________________________
________________________________________________________________________________
________________________________________________________________________________
Doctor notified (if applicable) Yes No
Persons involved:________________________________________________________________________________
________________________________________________________________________________
________________________________________________________________________________
Notified by: ______________________________ Date: ______________________
Please forward the notification to the office of the Hospital Manager during working hours, or to the office of the Duty Matron after hours.

INCIDENT REPORTInstructions:1. To be completed within one week of notification of the incident.2. Attach the duplicate notification of the incident to this form.3. Forward to the office of the Nursing Manager.
Diagnosis:Type of Incident:Date of Incident: Time of Incident:Hospital: Ward/Department:
Report:
Comments:
Signature – Reporter: Date:Signature – Doctor if applicable:Signature – Unit Manager:Signature – Nursing Manager:Signature – Hospital Manager: Date:
Date of incident : ____________________________________________________________
Type of incident : ____________________________________________________________
Hospital : ____________________________________________________________
Intervention :____________________________________________________________________________
____________________________________________________________________________
____________________________________________________________________________
____________________________________________________________________________
____________________________________________________________________________
____________________________________________________________________________
____________________________________________________________________________
__ _________________________________________________________________________ Is adverse event/clinical incident risk assessment tool completed? Yes No ____________________________________________________________________________
Signature – Nursing Manager: __________________________ Date:______________
Evaluation of Intervention:_____________________________________________________________________________
_____________________________________________________________________________
_____________________________________________________________________________
INCIDENT INTERVENTION
Signature – Nursing Manager: __________________________ Date: _____________
Hospital Manager: Date: --------------------

HELP……
Help
√
√
√√
√
√√
√
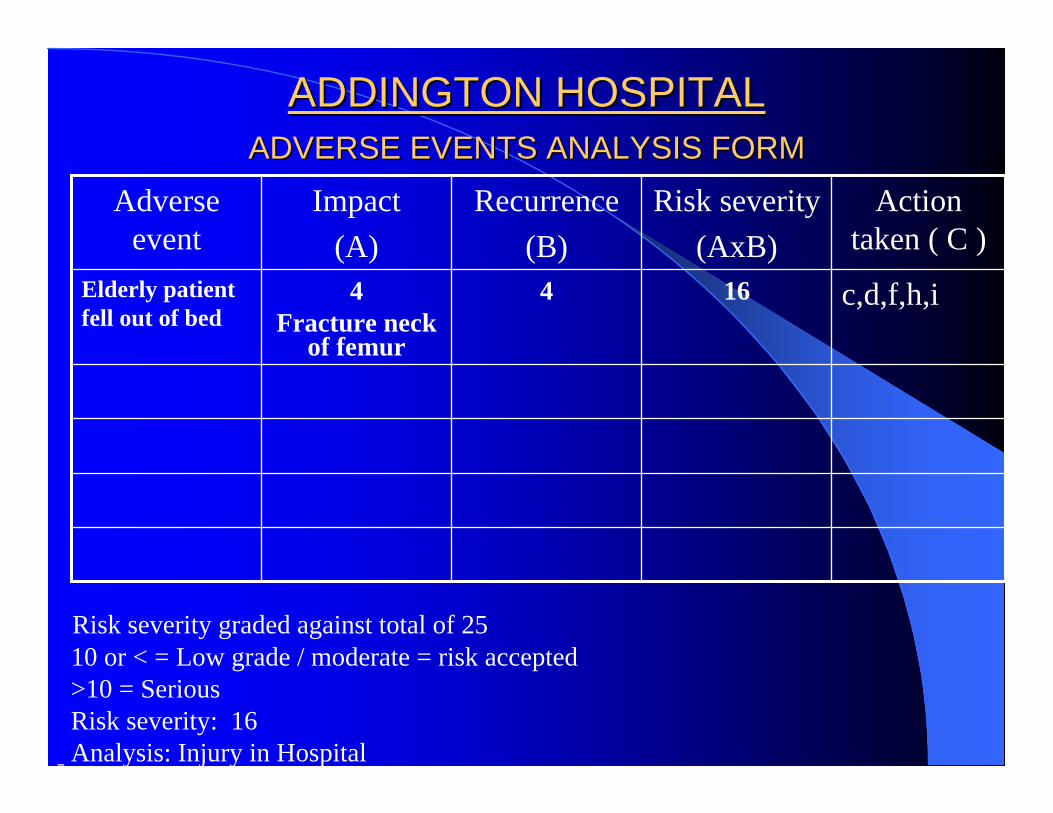
ADDINGTON HOSPITALADDINGTON HOSPITALADVERSE EVENTS ANALYSIS FORMADVERSE EVENTS ANALYSIS FORM
Action taken ( C )
Risk severity(AxB)
Recurrence(B)
Impact(A)
Adverse event
c,d,f,h,i1644Fracture neck
of femur
Elderly patient fell out of bed
Risk severity graded against total of 2510 or < = Low grade / moderate = risk accepted>10 = SeriousRisk severity: 16Analysis: Injury in Hospital

ADDINGTON HOSPITALADDINGTON HOSPITALADVERSE EVENTS ANALYSIS FORMADVERSE EVENTS ANALYSIS FORM
ContCont…………..
10 or < 10
Accepted and will bemonitored
>10
Recommended relevant Action
1.Recircularisation & Education of P&P – cot side
2.Counselling of junior staff & supervisor for non-adherence to P&P
Risk Manager:__xx______ Date:___xx_______ Signature:_xx____
Forwarded to: 1. Quality Steering Committee √2. Health and Safety Committee √3. Unit Manager √4.

No of Adverse Events No of Adverse Events April April –– Nov 2004Nov 2004
5568TOTAL25Nov56Oct1010Sept912Aug39July79June1010May97April
ADMINCLINICALMONTH
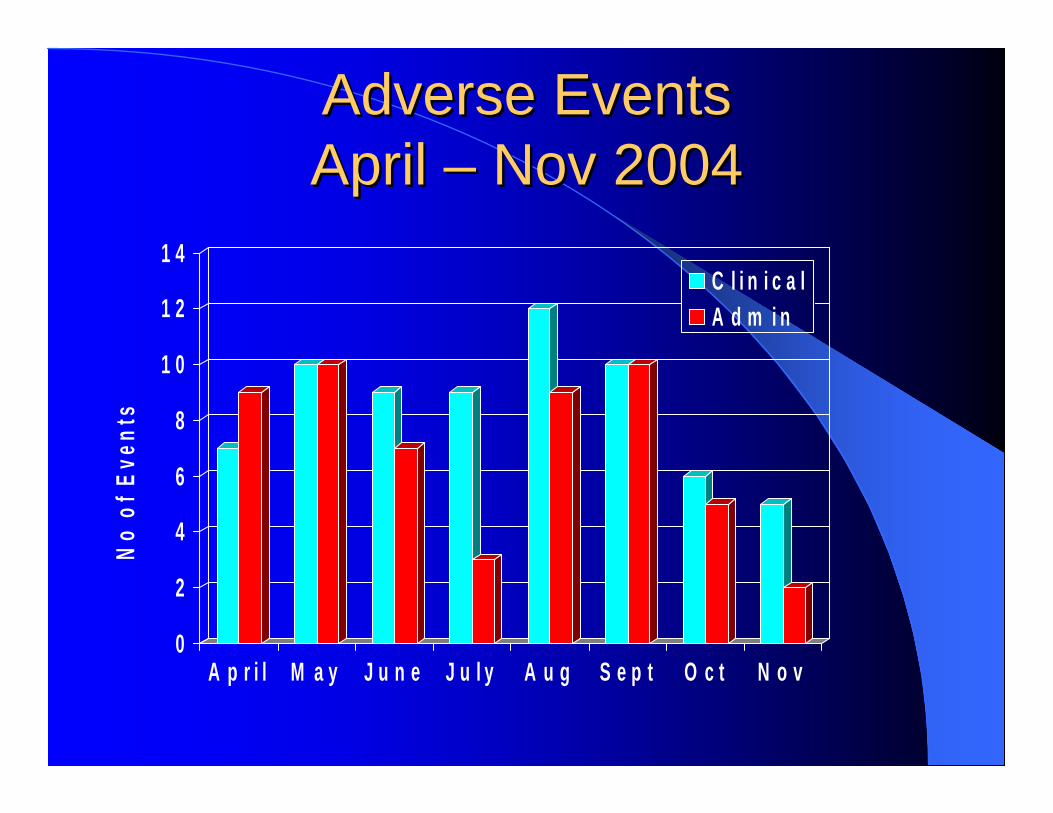
Adverse Events Adverse Events April April –– Nov 2004Nov 2004
0
2
4
6
8
1 0
1 2
1 4
No
of E
vent
s
A p r i l M a y J u n e J u l y A u g S e p t O c t N o v
C l i n i c a lA d m i n
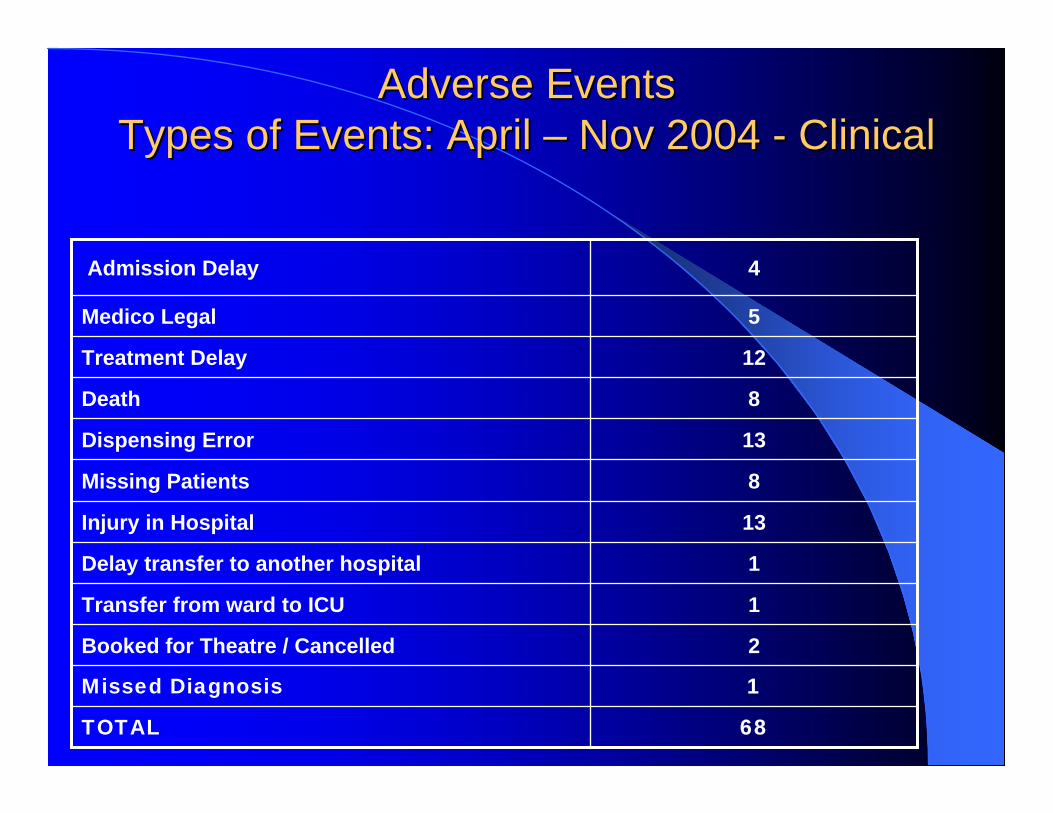
Adverse EventsAdverse EventsTypes of Events: April Types of Events: April –– Nov 2004 Nov 2004 -- ClinicalClinical
68TOTAL
1Missed Diagnosis
2Booked for Theatre / Cancelled
1Transfer from ward to ICU
1Delay transfer to another hospital
13Injury in Hospital
8Missing Patients
13Dispensing Error
8Death
12Treatment Delay
5Medico Legal
4Admission Delay

0
2
4
6
8
10
12
14
16
No
of E
vent
s
Adm Delay Med Legal Rx Delay Death Disp Error Missing Pts Inj in Hosp T/F to ICU Theatrecancelled
T/F to otherhospital
Md
Clinical
Adverse EventsAdverse EventsTypes of Events: April Types of Events: April –– Nov 2004Nov 2004

Adverse EventsAdverse EventsTypes of Events: April Types of Events: April –– Nov 2004Nov 2004
AdministrativeAdministrative
32TOTAL
3Invalid Consent
3Lack of Security
11Service Failure
8Misconduct
7Theft/Loss

Adverse EventsAdverse EventsTypes of Events: April Types of Events: April –– Nov 2004Nov 2004
02468
1 01 21 41 6
No
of E
vent
s
T h e f t / L o s s M i sc o n d u c t
S e r v i c eF a i l u r e
L a c k o fS e c u r i t y
I n v a l i dC o n s e n t
A d m in

1
3
9
1 8
2
7 7
1 1
3 3
1 2
1
6
2
6
0
8
01
02
01 1
02468
1 01 21 41 61 82 0
No
of In
cide
nts
1 2 3 4 5 6 8 9 1 0 1 2 1 5 1 6 2 0 2 5G r a d in g / S e v e r i t y
C l i n i c a lA d m i n
Adverse EventsAdverse EventsGrading/Severity: April Grading/Severity: April –– Nov 2004Nov 2004
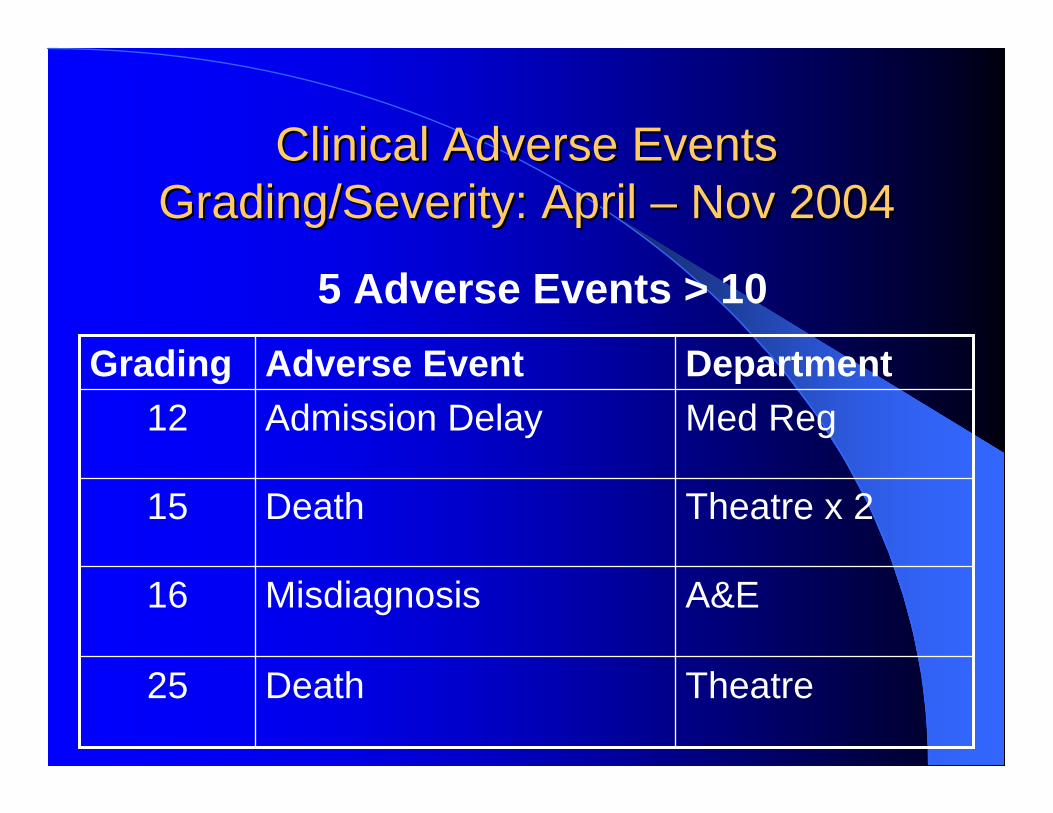
Clinical Adverse EventsClinical Adverse EventsGrading/Severity: April Grading/Severity: April –– Nov 2004Nov 2004
TheatreDeath25
A&EMisdiagnosis16
Theatre x 2Death15
Med RegAdmission Delay12DepartmentAdverse EventGrading
5 Adverse Events > 10
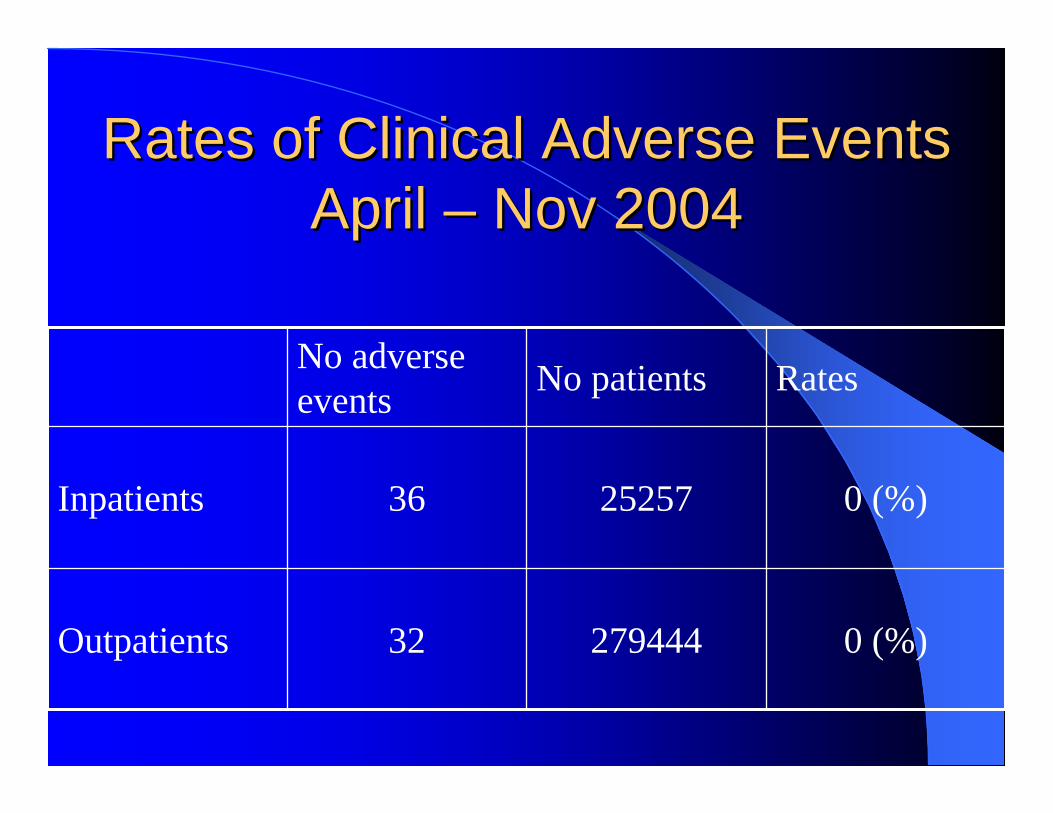
Rates of Clinical Adverse Events Rates of Clinical Adverse Events April April –– Nov 2004Nov 2004
0 (%)27944432Outpatients
0 (%)2525736Inpatients
RatesNo patientsNo adverse events

First Phase
Second phase
Third PhaseWay Forward

The adverse clinical incident ratings The adverse clinical incident ratings and risk severities are only done for and risk severities are only done for the adverse clinical incidents the adverse clinical incidents reporting, therefore does not reflect reporting, therefore does not reflect the total adverse clinical incidents.the total adverse clinical incidents.
We need to apply incidence ratings We need to apply incidence ratings and risk severities to our other and risk severities to our other methods of clinical adverse events methods of clinical adverse events detection.detection.
ADDINGTON HOSPITAL CLINICAL MX MODEL
Inpatient medical record review
Emergency Unit record review
Adverse event/clinical incident reports
Clinical Activities
Audits and Reports
Pt risk assessment tools Post mortem reportsMedia reports Consultative committees Pt complaint audits InsurersLiterature reviewsProvincial statistics
Clinical reviews
Adverse events
Detect risks
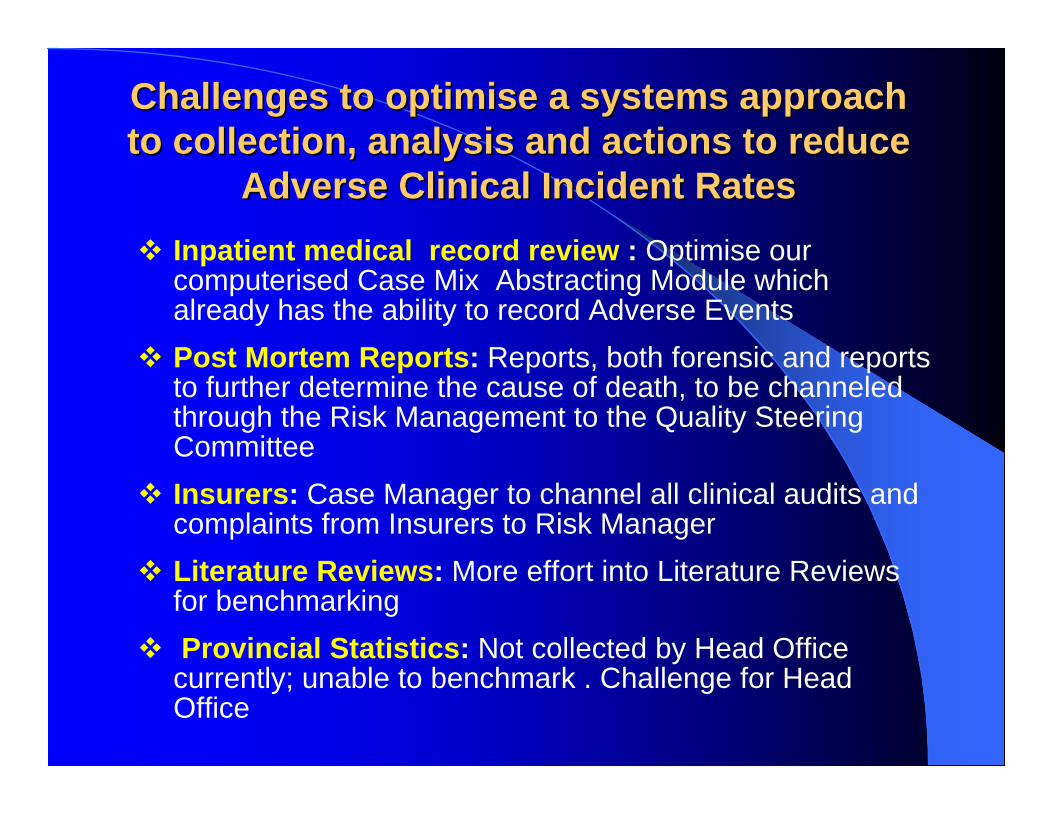
Challenges to Challenges to optimiseoptimise a systems approach a systems approach to collection, analysis and actions to reduce to collection, analysis and actions to reduce
Adverse Clinical Incident RatesAdverse Clinical Incident RatesInpatient medical record review : Optimise our computerised Case Mix Abstracting Module which already has the ability to record Adverse EventsPost Mortem Reports: Reports, both forensic and reports to further determine the cause of death, to be channeled through the Risk Management to the Quality Steering CommitteeInsurers: Case Manager to channel all clinical audits and complaints from Insurers to Risk ManagerLiterature Reviews: More effort into Literature Reviews for benchmarkingProvincial Statistics: Not collected by Head Office currently; unable to benchmark . Challenge for Head Office

Challenges to Challenges to optimiseoptimise a systems a systems approach to collection, analysis approach to collection, analysis and actions to reduce Adverse and actions to reduce Adverse
Clinical Incident RatesClinical Incident RatesOngoing in-servicing of staff on utilisation of Clinical Adverse Events reportingOrganisation wide feedback on Adverse Events, as at this moment it is only to involved unitsCloser liaison between Risk Manager,Quality Manager, Case Manager,Infection Control Manager and Public Relation Officer to integrate data collection for analysis 6 Monthly comparative data evaluation to plot trends and patterns for remediation
ACKNOWLEDGEMENTSACKNOWLEDGEMENTS
Detecting and reducing Hospital Adverse Events: Outcomes of the Wimmera Clinical Risk Programme. MJA 2001; 174:621-625Alan M WolffJo BourkeIan A CampbellDavid W Leembruggen
Appreciation to:Addington Hospital: Informatics Team

![Managing performance in the era of adverse action and ... · An employer must not take adverse action ... to unlawful discrimination claim – Dare v Hurley [2005] ... of adverse](https://img.dokumen.tips/doc/110x75/5b93809f09d3f280378d7429/managing-performance-in-the-era-of-adverse-action-and-an-employer-must-not.jpg)



























