Embed Size (px)
Citation preview

MANAGERIAL ACCOUNTING TOOLS USED IN PUBLIC
INSTITUTIONS IN THE ROMANIAN HEALTH SYSTEM
PhD Thesis Abstract
Scientific adviser,
PhD Professor GEORGESCU Iuliana Eugenia
PhD Candidate,
GHEONEA Victoria
IAŞI
- 2012 -

1
Content of PhD Thesis Abstract
Key words........................................................................................................................................1
Structure of PhD Thesis...................................................................................................................2
Motivation and importance of research ...........................................................................................4
Synthetic presentation of thesis chapters.........................................................................................5
Conclusions, contributions and future research directions............................................................17
Selected references ........................................................................................................................23
Key words
Managerial accounting, health management, public sector, hospital services, health
system, cost, calculation methods, budget, Balanced Scorecard, Diagnosis Related Groups,
performance indicators

2
Structure of PhD Thesis
INTRODUCTION
Motivation and importance of research
The purpose and objectives of the research
State of knowledge in the use of management accounting tools in public sector
Research methodology
Chapter I. MANAGERIAL ACCOUNTING, A NECESSITY FOR THE SUCCESS OF ORGANIZATION
1.1. The relationship between management accounting and financial accounting
1.2. Objectives of management accounting and its role in management of organizations
1.3. Managerial accounting, information resource for management of health institutions
Chapter II. PARTICULARITIES OF HEALTH SYSTEM IN ROMANIA
2.1. Analysis of the Romanian healthcare system
2.1.1. Romanian health system analysis in European and global context
2.1.2. SWOT analysis of the health services in Romania
2.2. Financial management in the healthcare system
2.3. Analysis of performance indicators of public hospital management
2.4. Financing of health services
2.4.1. Models of health insurance financing used internationally
2.4.1.1. The British system - Beveridge
2.4.1.2. German system - Bismarck
2.4.1.3. Private insurance-based system used in the U.S.
2.4.2. Financing of hospital services in Romania
Chapter III. COSTS IN DECISION MAKING IN THE PUBLIC HEALTH SECTOR
3.1. Strategic Cost Management
3.2. The cost of healthcare quality
3.3. Models of cost-based decisions in the public sector
3.3.1. General considerations on cost-based decisions
3.3.2. "Produce or buy" decision. Outsourcing costs
3.3.3. Decision under limited resources. Opportunity cost
3.4. Methods of cost calculation of hospital services
3.4.1. Features of the calculation cost in terms of classical methods
3.4.2. Activity-based cost method
3.4.3. Comparative study on cost calculation in a public hospital: global method and activity based costing method
3
Chapter IV. MANAGEMENT TOOLS OF PERFORMANCE IN ROMANIAN HEALTH INSTITUTIONS
4.1. Planning and budgetary management
4.1.1. The budget, a tool for assessing the performance of public sector
4.1.1.1. Budgeting methods in the public sector
4.1.1.2. Programming the public budget
4.1.2. Control through budgets
4.2. Balanced Scorecard – strategic management tool of performance in public institutions
4.2.1. General considerations on Balanced Scorecard
4.2.2. The perspectives of Balanced Scorecard
4.2.2.1. Financial perspective
4.2.2.2. Customer perspective
4.2.2.3. Internal processes perspective
4.2.2.4. Learning & Growth perspective
4.2.3. Balanced Scorecard in Romania
4.2.4. Implementation of Balanced Scorecard in a public hospital
Chapter V. EMPIRICAL STUDY ON THE COSTING IN HEALTHCARE USING DIAGNOSIS RELATED GROUPS SYSTEM
5.1. Presentation of Diagnosis Related Groups System
5.1.1. DRG-based hospital financing system
5.1.2. SWOT analysis of DRG
5.2. Diagnosis Related Groups System, specific management tool to cost estimation of hospital services
5.2.1. Case study on example of "Gheorghe Buzoianu" Targu Bujor Hospital
5.2.2. Statistical analysis of hospitalized morbidity indicators according to diagnostic groups
5.2.2.1. Factorial analysis
5.2.2.2. Analysis of "cluster"
5.2.2.3. Conclusions statistical analysis
CONCLUSIONS, CONTRIBUTIONS AND FUTURE DIRECTIONS FOR RESEARCH
REFERENCES
ANNEXES

4
Motivation and importance of research
The thesis falls into a very current context: reforming the management of health units,
respectively the answer of managers to reform expectations. In this context, our research
approach is the extent to which managers succeed by applying and implementing new methods
and modern forms of management of accounts information, to obtain improved performance
health units, and develop advantages in the competition health market. In light of current trends,
especially future trends, of development of public sector in general, and the health system in
particular, it can be said that reform radical measures are needed.
Managerial accounting is often used, but the concept still arouses the interest of
researchers and practitioners in this field, they trying to highlight its delineation of management
accounting through advanced managerial accounting tools and complex information that it can
provide (Gupta & Gunasekaran, 2005; Kaplan & Atkinson, 1998; Roslender & Hart, 2003).
Decision making has become very complex and diverse due to various situations that
may occur in the activity of any organization, and therefore management accounting is a prime
source of information for managers, assisting them in making decisions, planning and control, a
context which confirms the topicality of investigated theme.
The main motivation for choosing the theme is the fact that, both in research and in
practice, study and use of management accounting are mainly in the private sector, public sector
management accounting tools are rarely addressed. Management of an organization is based on
the decisions that were taken from a good knowledge of internal and external factors which
could impact the organization activity. Complexity of the activity in a hospital needs usefulness
of managerial accounting tools, because the accurate determination of costs and their
implications in achieving the proposed performance is a constant imperative of decision making.
Thus, the scientific approach pursued, becomes a novelty and utility at the same time, both for
public sector accountants as well as academic, scientific novelty of the thesis is determined by
the goal and objectives of the research.
Through our approach, we aim to study and deepen the implementation of management
accounting tools in the public sector, the primary aim of our research.
5
Synthetic presentation of thesis chapters
In the introduction we defined the theoretical and methodological research, presenting the
theme, motivation and importance of research purpose and research objectives, level of
knowledge in the use of public sector management accounting tools and research methodology.
The first chapter entitled "Managerial accounting, a necessity for the success of
organization" we analyzed the role and objectives of management accounting, mainly in the
public sector in order to identify the information needs of the public manager from managerial
accounting and how it becomes the main tool in decision making process of the public
institution.
Managerial accounting is the most important source of information for planning and
control of resources and decision-making accordingly. Management accounting in public
institutions of the Romanian health system aims mainly to obtain information necessary for the
health unit management to base decisions. This information relates mainly to:
� financing mechanisms;
� costs of hospital services;
� performance of public hospitals, namely their monitoring by identifying
difficulties, irregularities and possible alternatives, in assessing the efficiency
ratio allocation / consumption and the development of strategies and plans.
On health care financing, management accounting provides valuable information, which
determines the viability of the financial institution and outlines the scope of services provided
action and size, quantifying financial resources being a key determinant for the organization.
This information relates to attracting and balanced managing of funds with a good foundation of
funding. A hospital is a public institution financed wholly from own revenues based on medical
service contracts with health insurance houses. Depending on the achievements and addressing
hospital patients, it can encounter two common situations in practice:
� The hospital performed more than the contracted amount (number of patients
treated is greater than the number of cases contracted with the house health); case there is a very
high addressability and the hospital is required to treat all patients who come to hospital. The
difference is a loss because the hospital treats patients either from its own resources saved, either
by reducing the quality of care for all patients. This situation is most common in hospitals in
Romania.
� Hospital achieved less than the contracted amount and the number of patients
treated is much smaller than the number of cases contracted. In this case, the house of health
adjusted the contract value to patients treated, and the hospital does not record deficit. Appear,
6
however, shortcomings in current and future planning: operational strategy is affected, it creates
a precedent unfavorable hospital for the next few years, which will affect the amounts to be
incurred in the future and are threatened the conditions of continuity of hospital activity, i.e. it
does not can continue operation and cannot meet its obligations for the foreseeable future.
In such cases, the information provided by managerial accounting support the manager by
warning and adjustment tools (e.g., determining beneficial activities and departments
"locomotive" of the hospital - which types of patients / diagnostic with benefit).
On the costs of hospital services, managerial accounting helps management of health
institutions to substantiate fair prices and tariffs, and precise control of centers of consumption
expenditure on activities or projects, thus helping to rigorous documentation of decisions
making. Information received in this case, are extremely useful in calculating costs of hospital
services to the level of procedure, patient and diagnostic group. They determine the real costs of
hospitalization knowledge, assessing their efficiency and financial decision making informed,
and manager having thus provided both clinical data and cost data at the patient level.
Managerial accounting can answer therefore to the question "how much costs this type of patient
/ diagnosis?"
The second chapter, "Particularities of the health system in Romania", aims to identify
and describe the current state of the Romanian health system performance, establishing precisely
the areas where managerial accounting can intervene and improve healthcare processes and
activities. Thus, we obtained an overview of the Romanian health system by which we identified
its particularities in financial terms by comparison with international financing patterns of
hospital care, by presenting the advantages and disadvantages of the current system, describing
resources and performances in relation to allocated resources, and description of existing
financial model.
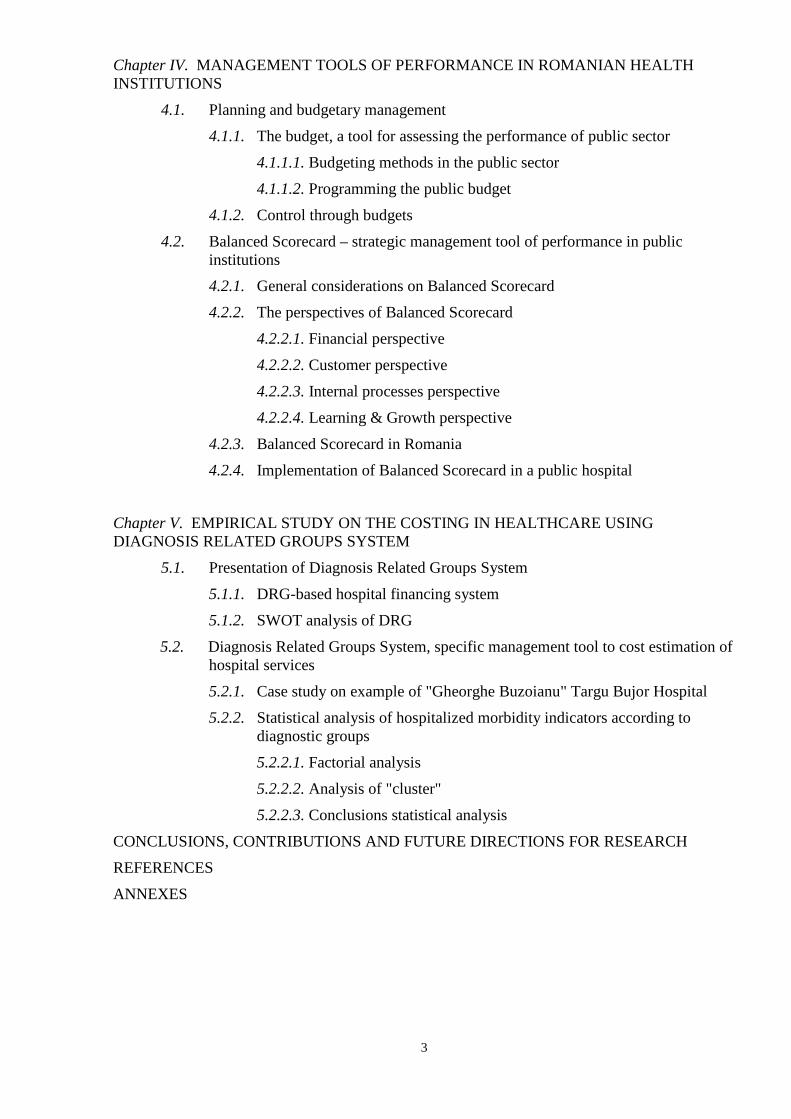
Romanian health budget has decreased by over 40% in the last three years. It is obvious
that the public health system in Romania is really underfunded, given occidental standards
(where over 10% of GDP allocated to health) and that our health indicators look much worse
than those of other European countries, not only European Union.

7
Figure 1 Ranking of Euro Health Consumer Index for 2012
(Source: own achievement by Euro Health Consumer Index 2012 Report)
According to the Euro Health Consumer Index for 20121, the annual comparative
research of health systems in Europe relegated Romania ranked 32 (!) with 489 points, out of 34
European countries (Figure 1). Rank points out that states in top (Netherlands, Denmark,
Iceland) begin to use information about health and choice, to involve patients in decision
making, building bottom-up process to improve performance. At the end of the standings is a
group of countries (Romania, Bulgaria, and Serbia) stuck in the old health system, hierarchized
and lacking in transparency. This difference poses a challenge to the principles of equity and
solidarity of the European Union.
Recent data centralized by the National Health Insurance House2 (NHIH) shows that after
Romania joined the EU, 45% of the total NHIH's budget reaches to hospitals (Figure 2).
Figure 2 Composition of the National Unique Health Insurance Fund budget after EU accession
(Source: own achievement data by NHIH)
1 *** Euro Health Consumer Index 2012 Report, available at http://www.healthpowerhouse.com/files/Report-EHCI-2012.pdf (accessed 16 August 2012) 2 *** The National Health Insurance House (NHIH), The National Unique Health Insurance Fund Evolution, available at http://www.cnas.ro/informatii-publice/bugetul-fnuass/evolutia-fnuass (accessed 7 March 2012)

8
In addition to underfunding, we can talk about arbitrary use of resources: allocation of
resources between different regions, between different types of health services, between different
health institutions is inefficient and inequitable. Analyzing data from the Ministry of Health3, It
can be notice the inequitable of resource allocation by counties. Thus, in Figure 3 we notice that
28 counties (67% of all counties) receive less than 2% of the budget and 9 counties (21%)
receive between 2-3%. "Favorites" ranks are occupied by 4 counties (Cluj - 6% of the budget,
Iaşi 5%, Mureş and Timişoara 4%), in the top being Bucharest with funding over 23% of the
budget.
Figure 3 Hospitals financing by counties in 2010, in % of total budget
(Source: own achievement by the Ministry of Health)
Therefore, differences between regions and counties are too large to not suspect the
presence of unfair inequalities in resource allocation. Even if in our analysis we observed that in
some counties high level is determined by a certain factor that acts locally and regionally (the
concentration of a large number of medical institutions specialized in these areas where the entire
population migrates), which result in a sharp contrast with the low level of other districts, this
factor should be the subject of health policy interventions that aim to reduce unfair differences
found in the analysis.
The third chapter, entitled "Costs in decision making in the public health sector",
shows how hospital care in Romania can be modeled and improved based on actual cost data.
Thus, Chapter III focuses on the study of the relationship between costs and public sector
decision making through concrete analysis, comparisons between different decision models and
costing methods and an overview of managerial accounting tools currently used in the public
sector to identify their advantages and limitations. 3 *** Ministry of Health, Hospitals Financial Situation. 2010, available at http://www.ms.ro/?pag=210 (accessed 10 March 2012)
9
Strategic decision "to produce or buy” certain products or services is mandated to assess
and establish realistic, exactly, that alternative is more advantageous to the final economic
results of the organization. The criteria for analysis are not only economic, must be taken into
account certain technical reasons, organizational and even social: "produce" if we gets low cost
or if there is wrong suppliers or if used thus the surplus of staff and benefit increases, or to
obtain a desired quality; "buy" if there is more than one supplier or if there is no technical skills,
managerial and adequate capacities to produce, or if fast and costly technological changes occur.
Opportunity cost is the sacrifice that supports an economic subject when choosing
between several possible solutions. Opportunity cost is used only for limited resources, because
in these conditions, the sacrifice may occur in favor of other more efficient alternatives. The
public sector has always faced the problem of limited resources. Act of choice, especially in the
public sector, appears like a need for limiting resources. Resources are limited, especially in
public sector, which makes their use to compete: when you want to satisfy in a higher degree of
certain need (ensuring staff salaries, for example), must be accepted to satisfy other needs in a
lesser extent (investment in equipment). Limitation of resources forces the manager to be
effective in restoring public priorities. No matter how limited it is an action of a public
institution, it exerts an influence on resource allocation, because itself, inevitably involves
consumption of resources and so long as resources are limited, it involves an opportunity cost.
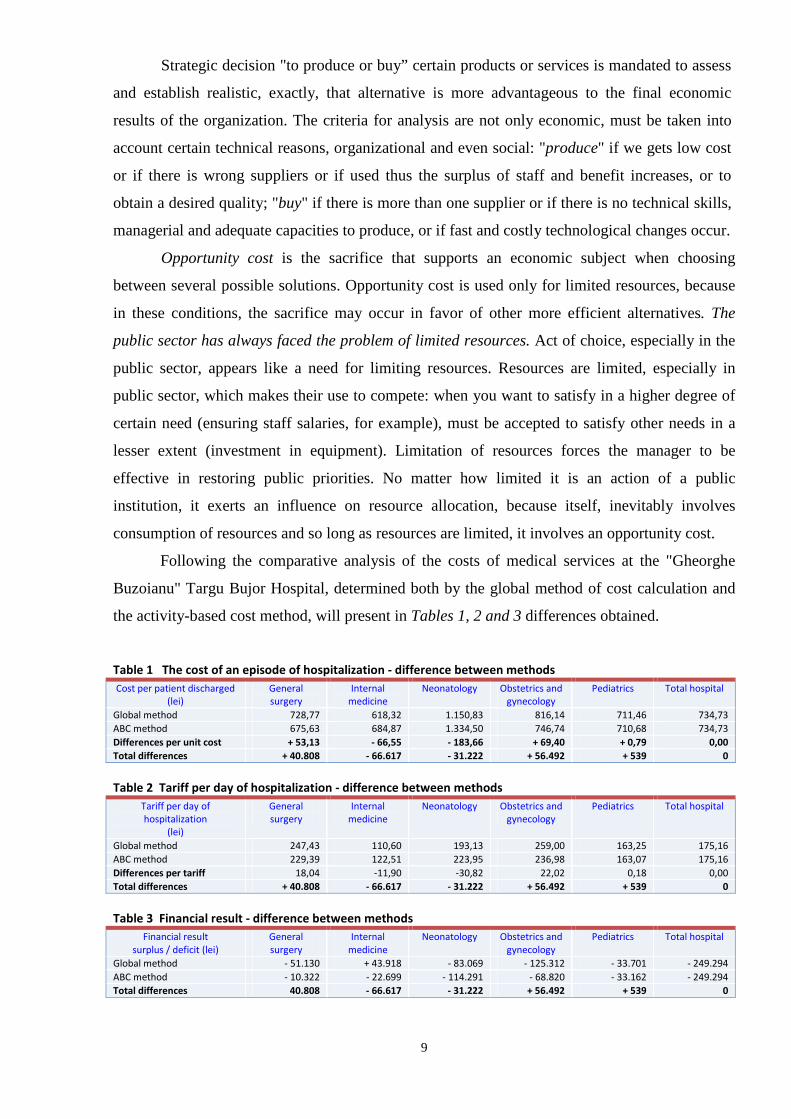
Following the comparative analysis of the costs of medical services at the "Gheorghe
Buzoianu" Targu Bujor Hospital, determined both by the global method of cost calculation and
the activity-based cost method, will present in Tables 1, 2 and 3 differences obtained.
Table 1 The cost of an episode of hospitalization - difference between methods
Cost per patient discharged
(lei)
General
surgery
Internal
medicine
Neonatology Obstetrics and
gynecology
Pediatrics Total hospital
Global method 728,77 618,32 1.150,83 816,14 711,46 734,73
ABC method 675,63 684,87 1.334,50 746,74 710,68 734,73
Differences per unit cost + 53,13 - 66,55 - 183,66 + 69,40 + 0,79 0,00
Total differences + 40.808 - 66.617 - 31.222 + 56.492 + 539 0
Table 2 Tariff per day of hospitalization - difference between methods
Tariff per day of
hospitalization
(lei)
General
surgery
Internal
medicine
Neonatology Obstetrics and
gynecology
Pediatrics Total hospital
Global method 247,43 110,60 193,13 259,00 163,25 175,16
ABC method 229,39 122,51 223,95 236,98 163,07 175,16
Differences per tariff 18,04 -11,90 -30,82 22,02 0,18 0,00
Total differences + 40.808 - 66.617 - 31.222 + 56.492 + 539 0
Table 3 Financial result - difference between methods
Financial result
surplus / deficit (lei)
General
surgery
Internal
medicine
Neonatology Obstetrics and
gynecology
Pediatrics Total hospital
Global method - 51.130 + 43.918 - 83.069 - 125.312 - 33.701 - 249.294
ABC method - 10.322 - 22.699 - 114.291 - 68.820 - 33.162 - 249.294
Total differences 40.808 - 66.617 - 31.222 + 56.492 + 539 0

10
It can notice from the three summary tables, that there is a significant difference between
the results obtained by the two methods of calculation, representing nearly 4% of total health
care costs. The explanation for the large differences reflected by ABC is the high complexity
diagnoses and long duration of hospitalization both specific to neonatology and internal
medicine departments. On the other hand, internal medicine department has the largest medical
addressability by nature of diseases treated, hospitalizing almost 30% of all patients in the
hospital. Also, these medical departments, through the specific diagnoses have the longest period
of hospitalization, per an episode of admission (about 6 days in one patient).
All these costs were not captured by the classical method, which calculated against ABC
a complete cost per patient and a charge per day of hospitalization by 11% lower in the
department of internal medicine, respectively 16% in neonatology. This lack of precision leads to
a considerable error of 97,839 lei: hospitalization in internal medicine is more expensive by
66,617 lei, and neonatology department with 31,222 lei. The sum of 97,839 lei is allocated
incorrectly by classical method to the costs of surgery and obstetrics-gynecology departments.
The only department where the two methods have achieved a similar result is pediatrics.
We appreciate the usefulness of ABC method, especially in a hospital where "final
product" - healthcare - can be decomposed into activities, which in turn can be quantified in
costs. In this sense, medical clinical protocols and guidelines are extremely useful, all medical
maneuvers and medical behavior takes place according to clear and detailed criteria, as they are
developed by international guidelines based on evidence of clinical effectiveness and at the same
time, economic and adapted to specialty and hospital competence. Using multiple cost drivers
and less arbitrary, ABC method led to obtaining a real cost and therefore produced a relevant
cost, identifying the exact origins of costs and factors that triggered the consumption of resources
on each medical department.
Given the conclusions of the previous chapters, in the following chapters we realized
empirical studies on the application of managerial accounting tools in public health sector and
the benefits they provide. Thus, in the fourth chapter we presented "Management tools of
performance in Romanian health institutions".
In a public institution, and not only, it is very important to ensure continuity of the
strategic process. Consequently, the budgeting process should not be isolated from the initial
stage (at start of year), but a continuous and ongoing process, trend in global strategic
management being "sliding forecasting". From this perspective, budgets must be able to adapt,
be flexible. Flexible budget is a budget designed to be modified according to the level of activity
achieved. It is known as variable budget or sliding scale budget4 or continuous budget5.
4 Vijayakumar, T., Accounting for Management, Tata McGraw Hill, New Delhi, 2010, p. 20.7

11
Sliding budgeting ensures that if the different achievements of planning, budget figures
be able to correct, of course after following certain rules. Sliding budgeting is to establish a
baseline budget version, from a year, and in its periodic update (recommended quarterly)
depending on achievements of the past period. Changing projections depending on the
circumstances, and thus using in the sliding budget the latest information on the development
and updating quarterly forecasts, it is an advantage of this budget. Sliding budgeting involves
quarterly review of the budget, and this means a higher volume of work and costs. But this
disadvantage is canceled by the fact that the sliding budget is designed for a long time (ideally to
be developed in the medium term of 3 years) and is updated constantly on the go, at
predetermined intervals on the achievements of past time periods and requirements of
foreseeable future. Premises and assumptions are continuously reviewed, as management learns
from experience. In this way, the latest information is included continuously in budgeting
process.
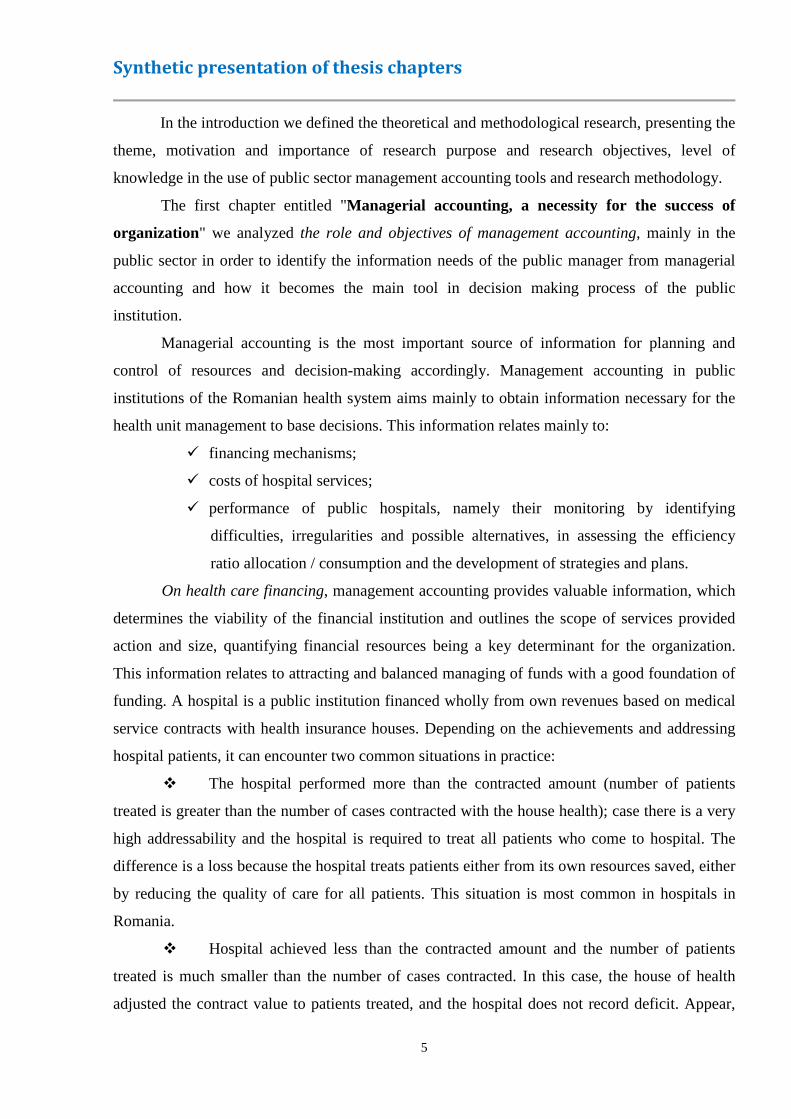
Some authors6 consider that the Balanced Scorecard was originally conceived as a
concept addressed to the need for performance measurement in the private sector and not fully
meet the needs of the public sector in this regard. Costs are high and lack of specialists
constitutes a real obstacle in implementing BSC in public institutions. BSC implementation in a
public hospital could lead to very valuable results. Basically, the Balanced Scorecard scheme for
a hospital is presented in Figure 4.
Figure 4 Balanced Scorecard scheme for hospital
(Source: own achievement after Albu & Albu, 2005, p. 221)
In the fifth chapter of the thesis, we developed an Empirical study on the costing in
healthcare using Diagnosis Related Groups System (DRG). As long as DRG System is used
in real mode with actual data from hospitals, it is really a management tool to estimate and
control costs of hospital services. In practice of the Romanian health sector, DRG system is used
only as a method of funding hospitals because it uses standard data, required by law, obviously
5 Ştefănescu, A., Ţurlea, E., Tănase, G.L., Meanings and controversies on economic entities budgets, in Review of Financial Audit, year X, no. 91, July 2012, p. 19, available at http://www.cafr.ro/uploads/AF%207%202012%20-%20Site-d6af.pdf (accessed 1 September 2012) 6 Wisniewski, M., Olafsson, S., Developing balanced scorecards în local authorities: a comparison of experience, in International Journal of Productivity and Performance Management, vol. 53, no. 7(2004), pp. 602-610
12
for reasons of the Romanian imperative - saving all extremely limited resources with serious
consequences on the Romanian health system, widely publicized and well known.
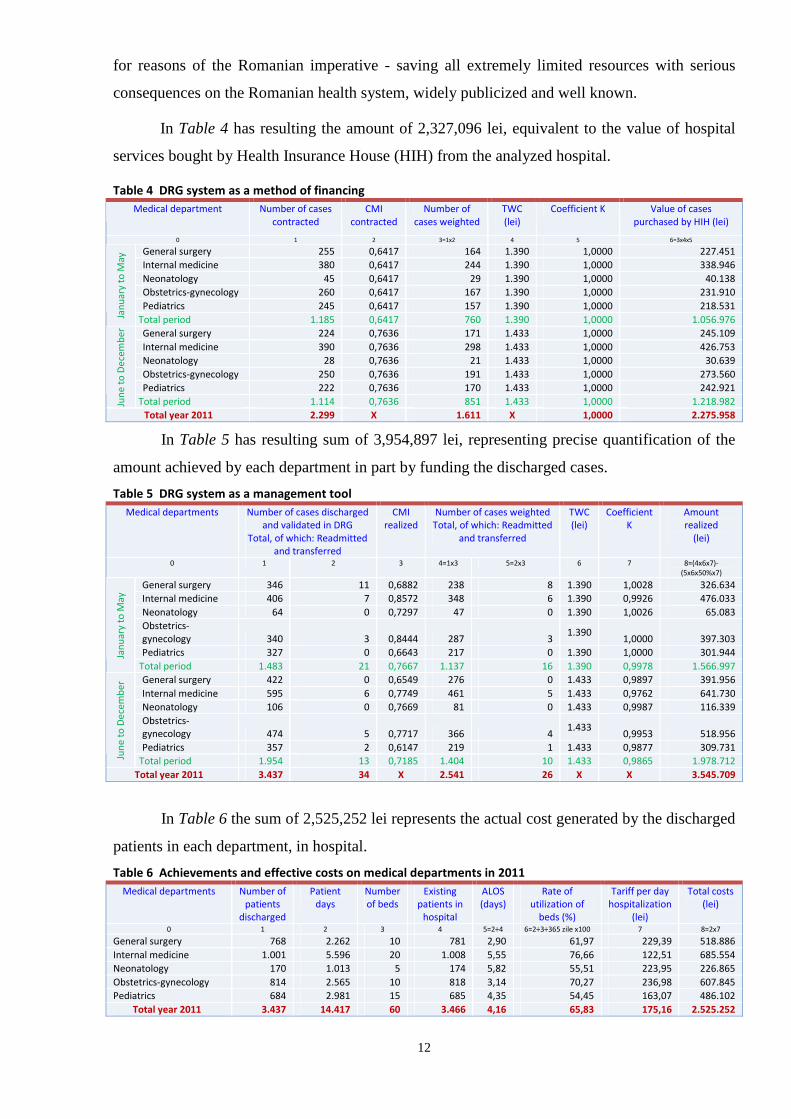
In Table 4 has resulting the amount of 2,327,096 lei, equivalent to the value of hospital
services bought by Health Insurance House (HIH) from the analyzed hospital.
Table 4 DRG system as a method of financing
Medical department Number of cases
contracted
CMI
contracted
Number of
cases weighted
TWC
(lei)
Coefficient K Value of cases
purchased by HIH (lei)
0 1 2 3=1x2 4 5 6=3x4x5
General surgery 255 0,6417 164 1.390 1,0000 227.451
Internal medicine 380 0,6417 244 1.390 1,0000 338.946
Neonatology 45 0,6417 29 1.390 1,0000 40.138
Obstetrics-gynecology 260 0,6417 167 1.390 1,0000 231.910
Pediatrics 245 0,6417 157 1.390 1,0000 218.531
Jan
ua
ry t
o M
ay
Total period 1.185 0,6417 760 1.390 1,0000 1.056.976
General surgery 224 0,7636 171 1.433 1,0000 245.109
Internal medicine 390 0,7636 298 1.433 1,0000 426.753
Neonatology 28 0,7636 21 1.433 1,0000 30.639
Obstetrics-gynecology 250 0,7636 191 1.433 1,0000 273.560
Pediatrics 222 0,7636 170 1.433 1,0000 242.921
Jun
e t
o D
ece
mb
er
Total period 1.114 0,7636 851 1.433 1,0000 1.218.982
Total year 2011 2.299 X 1.611 X 1,0000 2.275.958
In Table 5 has resulting sum of 3,954,897 lei, representing precise quantification of the
amount achieved by each department in part by funding the discharged cases.
Table 5 DRG system as a management tool
Medical departments Number of cases discharged
and validated in DRG
Total, of which: Readmitted
and transferred
CMI
realized
Number of cases weighted
Total, of which: Readmitted
and transferred
TWC
(lei)
Coefficient
K
Amount
realized
(lei)
0 1 2 3 4=1x3 5=2x3 6 7 8=(4x6x7)-
(5x6x50%x7)
General surgery 346 11 0,6882 238 8 1.390 1,0028 326.634
Internal medicine 406 7 0,8572 348 6 1.390 0,9926 476.033
Neonatology 64 0 0,7297 47 0 1.390 1,0026 65.083
Obstetrics-
gynecology 340 3 0,8444 287 3 1.390
1,0000 397.303
Pediatrics 327 0 0,6643 217 0 1.390 1,0000 301.944 Jan
ua
ry t
o M
ay
Total period 1.483 21 0,7667 1.137 16 1.390 0,9978 1.566.997
General surgery 422 0 0,6549 276 0 1.433 0,9897 391.956
Internal medicine 595 6 0,7749 461 5 1.433 0,9762 641.730
Neonatology 106 0 0,7669 81 0 1.433 0,9987 116.339
Obstetrics-
gynecology 474 5 0,7717 366 4 1.433
0,9953 518.956
Pediatrics 357 2 0,6147 219 1 1.433 0,9877 309.731
Jun
e t
o D
ece
mb
er
Total period 1.954 13 0,7185 1.404 10 1.433 0,9865 1.978.712
Total year 2011 3.437 34 X 2.541 26 X X 3.545.709
In Table 6 the sum of 2,525,252 lei represents the actual cost generated by the discharged
patients in each department, in hospital.
Table 6 Achievements and effective costs on medical departments in 2011
Medical departments Number of
patients
discharged
Patient
days
Number
of beds
Existing
patients in
hospital
ALOS
(days)
Rate of
utilization of
beds (%)
Tariff per day
hospitalization
(lei)
Total costs
(lei)
0 1 2 3 4 5=2÷4 6=2÷3÷365 zile x100 7 8=2x7
General surgery 768 2.262 10 781 2,90 61,97 229,39 518.886
Internal medicine 1.001 5.596 20 1.008 5,55 76,66 122,51 685.554
Neonatology 170 1.013 5 174 5,82 55,51 223,95 226.865
Obstetrics-gynecology 814 2.565 10 818 3,14 70,27 236,98 607.845
Pediatrics 684 2.981 15 685 4,35 54,45 163,07 486.102
Total year 2011 3.437 14.417 60 3.466 4,16 65,83 175,16 2.525.252

13
The difference between the amount realized theoretically and the amount contracted with
HIH is clearly positive (+1,269,751 lei) and represents the amount that the hospital would be
required to collect in addition to the contracted budget, because, regardless of the resources
consumed by patients discharged, the amount of 3,545,709 lei reflect actual funding for
discharged cases, according to DRG mechanism. By comparing the actual value of cases
discharged (3,545,709 lei) with costs to treat patients (2,525,252 lei) results a surplus of
1,020,457 lei - savings that could be kept in the hospital for investment.
The difference between the contracted budget (2,275,958 lei) and costs incurred to
resolve all cases (2,525,252 lei) is negative (– 249,294 lei), representing a deficit resulting from
the fact that the hospital has treated a total of 3,466 patients and received only the equivalent of
2,299 cases. In concrete terms, although the hospital activity is profitable, so economically
efficient, performing with 50.76% more, the hospital receive 9.87% less than spent and 35.81%
less than realized. The situation is almost unrealistic unfair, as follows: hospital has treated 3,466
patients of whom only 3,437 cases was DRG validated and HIH has paid only 2,299 cases (!)
Therefore, it results a number of 1167 cases discharged from hospital, for which there was no
"leu" returned from the National Unique Health Insurance Fund (NUHIF), patients being treated
from the hospital savings.
If the HIH, as a customer of the hospital, would have bought all medical services
performed by the hospital, we can say with conviction that healthcare, led by a management
team well prepared, is a very profitable activity: the value of all cases discharged and validated
in 2011 i.e. 3,437 cases, mean revenues totaling 3,545,709 lei, plus the 29 cases invalidated by
DRG (3,466 realized cases minus 3,437 validated).
To obtain at least fictional this revenue, the hospital performed the actual expenditures
2,525,252 lei, resulting in a surplus of 1,020,457 lei, amount absolute sufficient to purchase
modern medical equipment, for example, a chapter that most hospitals in Romania are very
poorly. In fact, although the hospital has spent 2,525,252 lei for 3,437 discharged cases, the
revenue from HIH, under contract, were 2,275,958 lei cashed for only 2,299 cases.
Extrapolating, if the hospital would be treated only 2,299 patients (cases reimbursed by
HIH), according to Table 7, the costs were worth 1,689,042 lei, and the surplus would have been
586,916 lei (2,275,958 lei received for the 2,299 patients minus 1,689,042 lei spent on the same
2,299 patients). Instead, the hospital not only achieved a surplus of 586,916 lei, but more, it
spent extra 836,211 lei for unsettled patients (difference between effective expenditures of
2,525,252 lei and HIH reimbursed expenditures for patients of 1,689,042 lei).
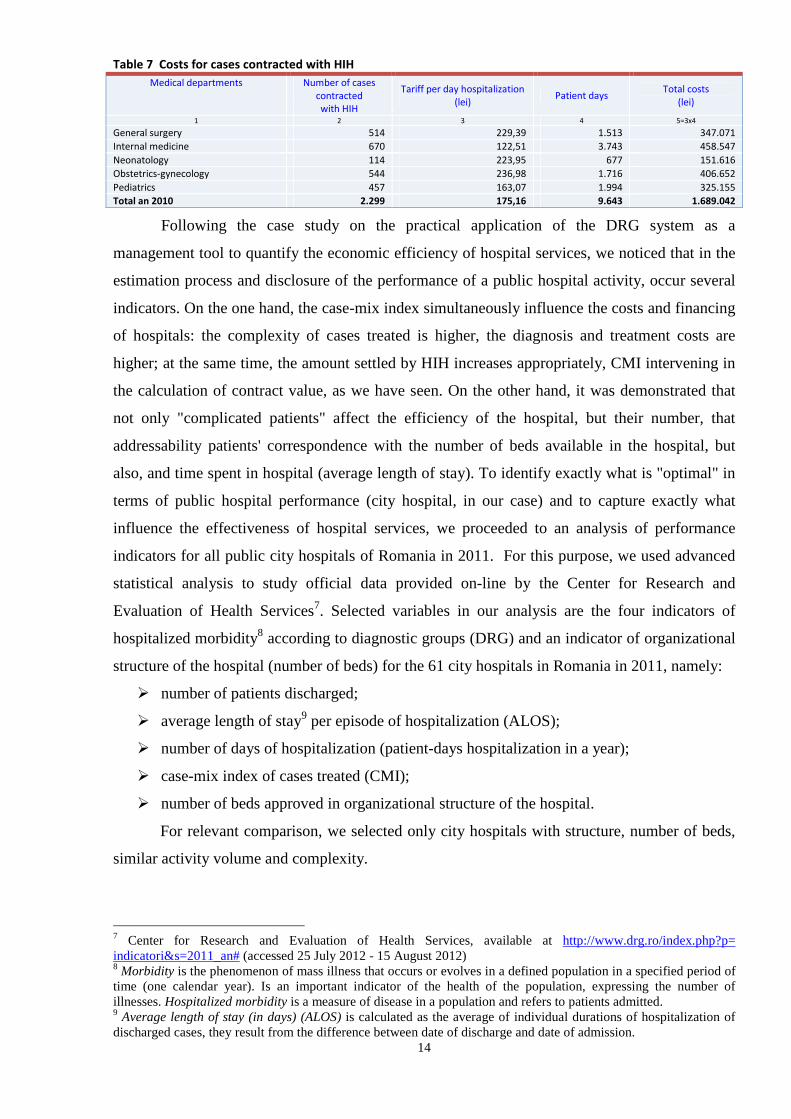
14
Table 7 Costs for cases contracted with HIH
Medical departments Number of cases
contracted
with HIH
Tariff per day hospitalization
(lei) Patient days
Total costs
(lei)
1 2 3 4 5=3x4
General surgery 514 229,39 1.513 347.071
Internal medicine 670 122,51 3.743 458.547
Neonatology 114 223,95 677 151.616
Obstetrics-gynecology 544 236,98 1.716 406.652
Pediatrics 457 163,07 1.994 325.155
Total an 2010 2.299 175,16 9.643 1.689.042
Following the case study on the practical application of the DRG system as a
management tool to quantify the economic efficiency of hospital services, we noticed that in the
estimation process and disclosure of the performance of a public hospital activity, occur several
indicators. On the one hand, the case-mix index simultaneously influence the costs and financing
of hospitals: the complexity of cases treated is higher, the diagnosis and treatment costs are
higher; at the same time, the amount settled by HIH increases appropriately, CMI intervening in
the calculation of contract value, as we have seen. On the other hand, it was demonstrated that
not only "complicated patients" affect the efficiency of the hospital, but their number, that
addressability patients' correspondence with the number of beds available in the hospital, but
also, and time spent in hospital (average length of stay). To identify exactly what is "optimal" in
terms of public hospital performance (city hospital, in our case) and to capture exactly what
influence the effectiveness of hospital services, we proceeded to an analysis of performance
indicators for all public city hospitals of Romania in 2011. For this purpose, we used advanced
statistical analysis to study official data provided on-line by the Center for Research and
Evaluation of Health Services7. Selected variables in our analysis are the four indicators of
hospitalized morbidity8 according to diagnostic groups (DRG) and an indicator of organizational
structure of the hospital (number of beds) for the 61 city hospitals in Romania in 2011, namely:
� number of patients discharged;
� average length of stay9 per episode of hospitalization (ALOS);
� number of days of hospitalization (patient-days hospitalization in a year);
� case-mix index of cases treated (CMI);
� number of beds approved in organizational structure of the hospital.
For relevant comparison, we selected only city hospitals with structure, number of beds,
similar activity volume and complexity.
7 Center for Research and Evaluation of Health Services, available at http://www.drg.ro/index.php?p= indicatori&s=2011_an# (accessed 25 July 2012 - 15 August 2012) 8 Morbidity is the phenomenon of mass illness that occurs or evolves in a defined population in a specified period of time (one calendar year). Is an important indicator of the health of the population, expressing the number of illnesses. Hospitalized morbidity is a measure of disease in a population and refers to patients admitted. 9 Average length of stay (in days) (ALOS) is calculated as the average of individual durations of hospitalization of discharged cases, they result from the difference between date of discharge and date of admission.
15
In order to get a more precise classification of city hospitals in Romania in terms of
efficiency, in our approach we use factor analysis and cluster analysis. Following the analysis,
we observed that the five individual variables are characterized by high levels of volatility, but
some are highly correlated with each other (as was the case indicators "Number of patients
discharged" and "Number of hospitalization days"), which means that in addition to the intrinsic
information content of each variable, there is a significant amount of information directly
dissipated in unobserved connections between variables. In this context, principal components
analysis has proven to be a useful tool to study because managed both synthesizing information
and information redundancy elimination.
Applying principal components method on our data set, we obtained two components
which summarizes approximately 77.880% of the information contained in the original data.
Thus, halving variables was performed under conditions of minimal information loss of 22.12%.
Therefore, we concluded that the indicator "Number of patients discharged" is not really
necessary in a city hospital efficiency analysis as long as the indicator "Number of
hospitalization days" provides more relevant information. Depending on the complexity and
pathology of disease, an episode of hospitalization may take 2-3 until 10-15 days for acute
patients or even up to 40-50 days (or more) for patients with chronic diseases. Thus, there may
be 10 patients who accumulate 20 days of hospitalization and only one admitted for 20 days and
the costs, at least hotelier ones (food, utilities, clothes, personal hygiene products, cleaning) are
identical for a patient or 10 patients. The first component can be analyzed in terms of morbidity
hospitalized at the admission capacity, because we noticed that there is a strong correlation
between the total number of patients discharged in a year, patient-days hospitalization per year
and the number of hospital beds. A second component can be analyzed in terms of the
complexity of cases treated or hospitalization period, statistical analysis capturing well close
correlation between the two indicators. We see therefore that there is no determining factor
between the complexity of the disease and greater or smaller number of patients discharged, but
obviously hospital beds are constantly crowded (day hospitalization) due to high turnover on a
bed (discharged patients).
In terms of hospital performance, it is difficult to assess which hospital is economically
efficient: a hospital with more patients (indicator "Number of patients discharged" is high) or a
hospital with patients "complicated" (indicator "Case-mix index" is high), a hospital with patients
"complicated" due to prolonged hospitalization (indicator "Average length of stay" is high) or an
increased complexity of diagnosis etc. Statistical analysis reached its intended purpose and was
able to clarify these issues: information redundancies were eliminated (Targu Carbunesti
Hospital is atypical for our analysis), we obtained a homogeneous mass of most city hospitals
(class 2) and we identified a benchmark of economic efficiency (Costesti Hospital). "Performing

16
supplier" recorded the best values of efficiency indicators. Although CMI increased, compared
with other providers, the hospital was able to make adequate values, which led placing first in
ranking. In other words, the optimum efficiency is the obvious, that hospital that manages to
quickly treat a number of patients appropriate for hospital capacity, but at the same time with a
high complexity of diagnostics. Accordingly, such a hospital will receive funding from HIH
sufficient to cover the costs of medical services provided and will be able to use resources in an
economical manner.
At the other extreme are the hospitals which forces length of stay, artificial - to get more
funding or wrongly - because there are doctors that hospitalized those patients who are not
suitable for continuous hospitalization (many hospitals still treating patients in continuous
hospitalization, even if the diseases can be treated in one day hospitalization). These ways of
increasing the length of stay determines implicitly equally artificial increase of the complexity of
cases treated, but much less than the costs involved, fact reflected in insufficient funding to cover
high costs, not always justified.
Statistical analysis performed identified thus some correlation between hospital
performance indicators. Thus, at the level of correlation between the number of cases discharged
and complexity index, we see that increasing the number of patients treated implicitly determines
an increase in costs, and in this respect we believe that increasing complexity index of cases
(DRG's complexity) must ensure an optimal level of hospital resources, in accordance with
treated patients. Statistical analysis performed reinforces the idea that, in time, at the level of
hospitals has formed a gap increasing in terms of funding. Thus, given that theoretically, the cost
of a weighted case is the same, we consider that, in terms of required resources, should not
register significant differences between healthcare providers.
17
Conclusions, contributions and future research directions
Managing a public hospital has a special place, because involves management of
complex activities with a high consumption of resources, so that leads to health services of high
quality. These activities begin with the treatment provided to patients (clinical activity) and
continue with hotel services (accommodation and food), effective stock management (medicines,
medical supplies, laboratory reagents, etc.) and extremely limited financial resources, but also
strategies to improve the quality of medical care (training, investment in medical equipment
performance, quality management standards). For this reason, a hospital management is based on
decisions from knowledge of all the factors that could influence activity and strategic objectives.
In this regard, accurate determination of costs and their implications in achieving established
performance is a constant imperative in decision making. There is no doubt that in a public
institution, a well established managerial accounting and dynamic, flexible, is a powerful tool
available to managers as a valuable source of information in decision-making relevant to
planning, financing costs and strategies. But it is absolutely necessary to establish and develop a
new mentality among managers about cost strategy and the importance of its use.
We observed in our approach, also studying current trends in research, that the
organizations themselves, private and especially public, and normalizers and professional
accountants, show no interest and seem not to understand the importance of managerial
accounting. Managers and even accountants identifies managerial accounting with simple cost
calculation, ignoring modern and advanced methods that can enhance value and improve
organization performance and its internal processes. Also, the lack of methodological rigor of
normalizers, who are not concerned with the development of more specific and severe
regulations on managerial accounting, and also the lack of a specialized professional body, leads
practitioners not be concerned with this area, known the fact that they are turning their attention
rather to what is highly regulated, standardized and obligatory (financial accounting, taxation,
financial statements). Precisely for these reasons, also observed in practice, we join the experts
who believe that academic environment understand the importance and need for managerial
accounting and advanced cost calculation, having the power to facilitate the process of
knowledge through its experts, demonstrated by research concerns more frequent and more
advanced in this field in recent years.
Making parallels between financial and managerial accounting, between classical and
modern methods of budgeting, costing methods, analyzing the particularities of the health system
in Romania, we can formulate the following conclusions and proposals regarding the application
of modern tools of management accounting in the public sector, namely the public health system.
18
Financial accounting has its well-defined role in an organization, but its information is
intended for external environment. Managerial accounting uses some of this information, but
with the help of advanced tools and with increased and informed interest from the management,
with concern and dedication of the professionals, with the cooperation and effective
communication between all hierarchical levels in the organization, can create a strong system of
information necessary for the future of the organization, an adviser to management decision
making. Managerial accounting has evolved from a system of financial information to a set of
tools oriented outwards, towards strategy and future, by changing over time, the orientation of
the calculation and identifies problems, to reduce waste and using the resources for value
creation and support for act of management and decision.
Specialists and many healthcare organizations have attempted to provide a valid response
to those who wonder to what extent the health system is better than another. Each national health
system has a number of objectives. Essentially, any healthcare system aims to provide a high
level of health and equitable distribution of health services. Meanwhile, a healthcare system has
to comply with people's expectations, which implies respect for the individual (autonomy and
confidentiality) and client orientation (prompt service and quality medical act). The conclusion
after analyzing the Romanian healthcare system in the European and international context is that
all these objectives should be related to the absolute level of responsiveness to the demands of
patients and the distribution of health care, and the health system reform has to take into account
the national specificities and must be based on a solid knowledge of system problems, on
available resources and clearly defined goals.
Our analysis at national level surprised that although the hospital financing system takes
into account the principle of "money follows the patient", in reality this applies only partially,
and transfers of funds are not made on the basis of clearly defined criteria. In this respect, it is
necessary to separate the funding system unlike system health care providers to ensure those who
pay greater autonomy in spending and unequivocal adoption of the idea that the health sector
resources should be directed to the patient needs (e.g. DRG codes).
Cost data can be used mainly in strategic decisions, because at the time when information
is presented to the management, production processes were consumed, and interventions that
occur are late. This is why the best cost for the organization is not necessarily the lowest, but one
that occurs in the place and at the right time and gives to user (the manager) the desired
precision. If costs involved are not taken into account, a decision is made difficult because the
main objective of the organization is to achieve performance, a goal that can be achieved only
under conditions of correlation decisions with costs.
Strategic cost management is articulated with managerial accounting rather it is an
integral part of it. In essence, the role of strategic cost management is "the establishment of
19
budgets, standard costs and actual costs of operations, processes, activities or products and
employees analysis, profitability on the use of funds" (Lucey, 2002), representing a
"cornerstone" for accounting information system in an organization.
By testing practical example of a public hospital of the ABC method compared to the
classical method allocation of costs, we identified a competitive tool that offers more relevant
costs to management. ABC method is the most used approach, recognized and appreciated
internationally to improve system cost, since it is based on understanding how resources are
consumed to create value. We have noticed that in the public sector the situation becomes more
complicated, as the management of costs is much affected by budgetary constraints. Therefore,
cost allocation based on resource consuming activities is the most accurate method of
quantifying the indirect costs of a hospital. Given the complexity of hospital care, which
involves many types of resources and services provided, the percentage of indirect costs is very
high and thus causes inaccurate estimates costing (cost per episode of hospitalization or
discharged patient, tariff per day of hospitalization, etc). In this respect, the ABC method is a
solution to identify activities inefficient and resource consuming activities in terms of cost /
benefit, thereby facilitating their effective costs control. Also, the cost information obtained by
the ABC method, i.e. activity costs, allowing to the hospital management to better and more
accurately estimate future costs with the same type of patient or diagnosis, and compare medical
costs with the level of funding. Relevance of the information provided by the ABC method
allows the hospital to identify and expand profitable services or to reorganize and restrict
inefficient activities.
In the public sector, especially for public institutions financed from own revenues (such
as public hospitals), it is imperative a more flexible mechanism of the budgetary process based
on procedures and rules focused on evaluation, results, efficiency, performance. Availability of
flexible budgets means for a manager the ability to handle information and resources and lead
the change. Ideally, a flexible budget should be built based on several scenarios depending on the
overall context of the internal and external environment of public institution, and its ability to
adapt: pessimistic, realistic (balanced) or optimistic, in conjunction with what happens in its field
and at the macroeconomic level, but with the real possibilities of public institution. Both the Law
no. 95/2006 on healthcare reform and the project of new health law, in the "Hospitals funding"
section, the first article reads: "Hospitals are organized as public institutions fully financed from
own revenues, and operates on the principle of financial autonomy". Under article 16, paragraph
(1) of Law no. 273/2006 on local public finance, the principle of financial autonomy means that
"administrative-territorial units are entitled to sufficient financial resources...". As such, hospitals
need flexible budgets, funded by achievements and not depending on the HIH budget, or local
councils and directorates of public finance restrictions.

20
A public hospital, works only if produces services: receives funds from HIH if it treating
patients, unlike public institutions financed from the state budget (such as the ministries,
National House of Pension, National Health Insurance House, National Agency for
Employment), which regardless of achievements receive funds. For this reason, the hospital
needs a sliding budget to enable comparisons between the reality of budget execution and initial
budgetary projections, based on patient addressability size - i.e., what has received from HIH and
what actually performed (as we presented empirical study on DRG system). With a flexible
budget, fixed costs should remain constant and variable costs should be modified according to
sales (HIH settled patients) if they were higher or less than were projected. Flexible budget is
then compared with reality, and the differences between planned and realized are calculated and
designed to be favorable or unfavorable (surplus or deficit). Health institution prepare flexible
budget taking account of changing consumption according to their achievements, this
representing a dynamic basis for comparing actual results with budget indicators. A flexible
budget is a detailed plan implemented in order to control indirect costs and which is available for
a significant period. It helps to control certain expenditure for which consumptions are not easy
to standardized, because they are not in each final product (such as laboratory investigations, for
example, which are not found in all medical services provided). It is required where possible
(and in a public hospital is possible) that budgets must be flexible, meaning adjustable, adaptable
so that their contents may change as the activity is changing and should be reviewed taking into
account the changes in the organization. Sliding budget proposed by us, obliges the financial
manager to set achievable goals and identify the key factor or limiting factor that will impose
constraints on current and future activities of the institution. This is because a budget that
includes unrealized indicators is totally ineffective.
We identified in our approach a strategic tool for measurement and performance
management, which helps the entity to accommodate long-term strategies with short-term
actions, using both financial indicators and non-financial: Balanced Scorecard. Performance
measurement, the main function of the BSC, divided these indicators of outcome indicators that
indicate past efforts and pilot indicators that indicate future performance, intervening to identify
opportunities and prevent errors. These indicators help finally to building the organization's
performance through the balance and interaction of the four forces (financial, customer
satisfaction by pursuing their perceived value, the efficiency of internal processes and its
capacity for growth and development). Balanced Scorecard is a tool designed to align actions
and strategic plans into a coherent control system. Since the BSC philosophy is to learn from its
actions, teamwork and follow-up strategy, this tool puts a strong emphasis on clear
communication of objectives and priorities. In short, being a flexible and dynamic instrument,
the BSC shows what needs to be done. According to its authors, Kaplan and Norton Balanced
21
Scorecard is a management system that translates strategy into action (The Balanced Scorecard:
Translating Strategy into Action, 1996). If a strategy for success has never been an easy task,
surely its practical application is crucial. Kaplan and Norton summarized this very well: "The
formulation of great strategies is an art, and it will always remain so. But the description of
strategy should not be an art. If people can describe strategy in a more disciplined way, they will
increase the likelihood of its successful implementation"10. Specifically, the Balanced Scorecard
approach helps public managers in the implementation of the ideas contained in the management
plans and development strategy. In the Balanced Scorecard the indicators of the four perspectives
(financial, customer, internal processes and learning & growth) are derived from vision and
strategy of organization. Developing the prospective board (balanced scorecard) implies that for
each of these perspectives to establish in a first stage: targets (what we aim), priorities (what
trying to achieve) and strategic objectives (what key elements should rectify to achieve the
objectives). Subsequently, for each key objective it will identify the sources of information and
performance indicators related to objectives (how do we measure), which are disaggregated by
organizational levels, responsible persons, optimum values and possibly on terms. And finally,
we set up measures to achieve the objectives (how do we know if we got to where we plan), BSC
placing great emphasis on performance measurement feedback. Of course, the Balanced
Scorecard is accompanied by an implementation plan on how the objectives will be achieved.
In Romania, where organizational climate is quite precarious, there is every chance that
such a system may be regarded only as an additional form of control of staff, so be sabotaged by
employees. On the other hand, the interest of managers of public institutions not often goes to
performance, at least not in the terms set by the Balanced Scorecard. Too few public institutions
are concerned with customer satisfaction of accountability to citizens, and efficiency (Şandor &
Raboca, 2004). We ensure that academic environment, for which performance is a real concern,
will also be able to guide organizational climate to these concerns essential to success of
organization, we appreciate.
The results of our research revealed many shortcomings of the current system of
financing and costing of public sector health and showed how it could be modeled and improved
by advanced methods of modern managerial accounting based on actual costs hospital care in
Romania. By recourse to the particularities of the health system in Romania, we presented a
model costing hospital services based on classification diagnosis-related groups system (DRGs).
The study, based on practical experience, is an element of novelty and utility, as we consider that
case-mix board made through the Diagnosis-Related Group provides hospital management
10 Kaplan, R.S., Norton, D.P., Having Trouble with Your Strategy? Then Map it, in Harvard Business Review, September-October 2000, pp. 167-176, available at http://www.bscol.se/_wcm/documents/Having%20trouble% 20with%20your%20stategy%20then%20map%20it%20%282%29.pdf (accessed 7 June 2012)

22
information on effectiveness of the financial mechanism, and at the same time, is a management
tool to estimate and control costs of hospital services.
From the idea that "you'll get only what you pay", using this funding mechanism based on
complexity of diagnoses treated, stimulates the hospital to treat patients more quickly and in the
best conditions. This is because the amount received from HIH depends on the types of patients
treated (volume and complexity of diagnosis), and not arbitrary factors such as structure and
hospital capacity (number of beds, number of medical departments, or degree of medical
equipment) or other process indicators (number of days of hospitalization, average length of stay
per type of departments). In this way resource allocation to hospitals becomes more objective,
transparent and fair: a hospital with a small number of patients, or patients with less severe
diseases will have lower financing.
In the DRG-based financing mechanism, were developed rates per weighted case, ie
"standard" cases, adjusted by complexity pathology. Using this mechanism manifests differently
in terms advantage / disadvantage to its three beneficiaries. Thus, on the one hand, hospitals
know exactly how much they receive from HIH for a patient, but do not know the cost to the
patient concerned. On the other hand, health insurance houses know what types of patients
contracted services with hospitals, but do not know the package of medical services actually
provided to patients, covered by amount. Third, patients know (or should know) what medical
services are entitled as insured persons, but in reality they do not know what services they will
actually receive from public health system (Haraga & Ţurlea, 2009). ICM-DRG board allows
clear and consistent measure of the types of patients treated, control costs incurred by them and
therefore efficient use of resources and disclosure of medical performance achieved by each
department individually. For these reasons, our study demonstrated how the DRG system
stimulates the calculation and control of hospital costs at department level and at the patient
level, helping to reduce patient costs and on DRG, and average length of stay on groups of
diseases or medical specialties, especially at DRG's which "allows" these things. In addition,
following the application mechanism DRG, the hospital has developed a highly complex
database that can provide useful information to hospital management. In fact, data DRG helps
the management team to know better the hospital, with its weaknesses and strengths, and act
accordingly, based on the evidence in the process of increasing the quality and efficiency of
services.
Finally, we consider that our research has achieved its purpose and meet the information
needs of academics, specialists and practitioners in particular, giving them more modern and
efficient methods of managerial accounting, solutions and proposals which they can apply in
practice of public healthcare institutions.
23
Selected references
Specialized books
1. Albu, N., Albu, C. - Instrumente de management al performanţei. Contabilitate de gestiune, Volumul I , Editura Economică, Bucureşti, 2003
2. Albu, N., Albu, C. - Instrumente de management al performanţei. Control de gestiune, Volumul II, Editura Economică, Bucureşti, 2003
3. Albu, N., Albu, C. - Soluţii practice de eficientizare a activităţilor şi de creştere a peformanţei organizaţionale. Gestiunea dezvoltării durabile prin Balanced Scorecard, Editura CECCAR, Bucureşti, 2005
4. Andrei, T., Matei, A., Stancu I., Andrei C. L.
- Socioperformanţa reformei sistemului public de sănătate, Editura Economică, Bucureşti, 2009
5. Androniceanu, A. - Management public - Studii de caz din instituţii şi autorităţi ale administraţiei publice, Editura Universitară, Bucureşti, 2008
6. Anica - Popa L.E. - Conducerea întreprinderii prin costuri. Recursul la modelele contabilităţii manageriale, Editura Economică, Bucureşti, 2005
7. Bouquin, H. - Contabilitate de gestiune, traducere Prof. dr. Tabără N., Editura TipoMoldova, Iaşi, 2004
8. Braga, V.F. - Contabilitate managerială, Editura Fundaţiei România de Mâine, Bucureşti, 2009
9. Briciu, S. - Contabilitatea managerială. Aspecte teoretice şi practice, Editura Economică, Bucureşti, 2006
10. Briciu, S., Căpuşneanu, S., Rof, M.L., Topor, D.
- Contabilitatea şi controlul de gestiune, instrumente pentru evaluarea performanţei entităţii, Editura Aeternitas, Alba Iulia, 2010, p. 12
11. Budugan, D., Georgescu, I., Berheci, I., Beţianu, L.
- Contabilitate de gestiune, Editura CECCAR, Bucureşti, 2007
12. Butuc, C., Dragomirişteanu, A., Fărcăşanu, A.
- Managementul serviciilor de sănătate, Editura C.N.I. Coresi, Bucureşti, 2000
13. Cardoş, I. R. - Contabilitate managerială şi calculaţia costurilor. Trecut, prezent şi viitor, Editura Alma Mater, Cluj-Napoca, 2010
14. Călin, O. (coord.), Man, M., Nedelcu, M.V.
- Contabilitate managerială, Editura Didactică şi Pedagogică, Bucureşti, 2008
15. Călin, O., Călin, C. - Contabilitate managerială, Editura Tribuna Economică, Bucureşti, 2007
16. Căpuşneanu, S. - Elemente de management al costurilor, Editura Economică, Bucureşti, 2008
17. Chadwick, L. - The Essence of Management Accounting, traducere Criste D., Contabilitate de gestiune, Editura Teora, Bucureşti, 1998
18. Diaconu, P. - Contabilitate managerială & Planuri de afaceri, Editura Economică, Bucureşti, 2006
19. Diaconu, P., Albu, N., Mihai S., Albu, C., Guinea F.
- Contabilitate managerială aprofundată, Editura Economică, Bucureşti, 2003
20. Dragomirişteanu A., Radu P., Mihăescu C., Brutu C.
- Economie sanitară şi management sanitar, Editura Rao, Bucureşti, 2003
21. Dumitru, M., Calu, D.A.
- Contabilitatea de gestiune şi calculaţia costurilor, Editura Contaplus, Ploieşti, 2008
22. Farkas, E. - Elemente de sănătate publică şi management sanitar, Editura University Press, Târgu-Mureş, 2006
23. Fătăcean, G. - Contabilitate managerială, Editura Alma Mater, Cluj-Napoca, 2005
24. Garrison, R., Noreen, E., Brewer, P.
- Managerial Accounting, McGraw-Hill Irwin, New York, 2008
25. Gisberto-Chiţu, A., Tudorache, S., Pitulice, C.
- Contabilitatea şi gestiunea instituţiilor publice, Editura CECCAR, Bucureşti, 2003
26. Glynn J.J., Murphy M., Perrin J., Abraham A.
- Accounting for Managers, Third Edition, Thompson Learning, 2003
27. Gray, S.J., Salter S.B., Radebaugh L.H.
- Global Accounting and Control. A managerial Emphasis, John Wiley & Sons, New York, 2001
28. Ham, C. - Health Policy in Britain, 5th edition, Palgrave McMillan, Hampshire, 2004
29. Heisinger, K. - Essentials of Managerial Accounting, South-Western Cengage Learning Publisher, USA, 2010
30. Hoffmeyer, U.,K., McCarthy T., R.
- Financing Health Care, vol. I, Kluwer Academic Publishers, Dordrecht, 1994
31. Hopwood, A.G., Chapman, C.S.
- Handbook of Management Accounting Research, vol. 3, Elsevier Ltd., Oxford, 2009
32. Horngren, C.T., Srikant, M.D., Foster, G.
- Contabilitatea costurilor, o abordare managerială, traducere Leviţchi, R., Leviţchi, V., Stanciu, D., Ediţia a XI-a, Editura Arc Chişinău, 2008
24
33. Horngren, C.T., Sundem, G.L., Stratton, W.O.
- Introduction to Management Accounting, 14th edition, Prentice Hall International Press, Upper Saddle River, 2005
34. Iacob C., Firescu V., Băluţă A., Popescu L., Mihai D. , Marinică D.
- Costurile: calculaţie, contabilizare, previziune, Editura Fundaţiei România de Mâine, Bucureşti, 2002
35. Ionescu, L. - Reforma bugetului public şi a contabilităţii publice în România, Editura Economică, Bucuresti, 2005
36. Ionescu, L. (coord.), Diaconu, E., Şuiu, I.
- Contabilitate publică, Editura Fundaţiei România de Mâine, Bucureşti, 2008
37. Johnson, H.T., Kaplan, R.S.
- Relevance Lost: The Rise and Fall of Management Accounting, Harvard Business Press, Business & Economics, 1991
38. Kaplan, R.S., Atkinson, A.A.
- Advanced Management Acconting, Third Edition, Prentice Hall International Press, 1998
39. Kaplan, R.S., Norton, D.P.
- The Strategy-Focused Organization: How BalancedScorecard Companies Thrive in the New Business Environment, Harvard Business School Press, Boston, 2001
40. Kumar, R., Goel, S.L. - Hospital Administration And Management: Theory And Practice, Deep & Deep Publications Ltd, New Delhi, 2007
41. Lock, D. (coord.) - Manualul Gower de Management, Editura Codecs, Bucureşti, 2001
42. Lucey, T. - Costing, 6th edition, Thomson Learning, Continuum, Londra, 2002
43. Mincă, D. - Sănătate publică şi management sanitar, Editura Universitară Carol Davila, Bucureşti, 2005
44. Muţiu, A., Mureşan, M. - Contabilitate managerială, Editura Risoprint, Cluj-Napoca, 2006
45. Nicolescu, O., Verboncu, I.
- Metodologii manageriale, Editura Universitară, Bucureşti, 2008
46. Nistor, C.S. - Trecut, prezent şi perspective în contabilitatea publică românească, Editura Casa Cărţii de Ştiinţă, Cluj Napoca, 2009
47. Niven, P.R. - Balanced Scorecard Step-by-step for Government and Nonprofit Agencies, 2nd Edition, John Wiley & Sons, New Jersey, 2008
48. Nowicki, M. - The Financial Management of Hospitals and Healthcare Organizations, Health Administration Press, Chicago, 2008
49. Olteanu, M. (coord.) - Renaşterea sistemului sanitar printr-o reformă bazată pe dovezi, I.D. International Technoprint, Bucureşti, 2005
50. Opincaru., C., Imbri, E., Gălăţescu, E.
- Managementul calităţii serviciilor în unităţile sanitare, Editura C.N.I. Coresi, Bucureşti, 2004
51. Oprea, C., Man, M., Nedelcu, M.V.
- Contabilitate managerială, Editura Didactică şi Pedagogică, Bucureşti, 2008
52. Pârvu, F. - Costuri şi fundamentarea deciziilor, Editura Economică, Bucureşti, 1999
53. Păunescu, M. (coord.) - Management public în România, Editura Polirom, Iaşi, 2008
54. Proctor, R. - Managerial Accounting for Business Decisions, 2nd Edition, Pearson Education Ltd., Edinburgh, 2006
55. Rampersad, H.K. - Total Performance Scorecard: Fundamente, traducere Turmac C., Editura Didactică şi Pedagogică, Bucureşti, 2005
56. Sarant, P.C. - Zero Base Budgeting in the Public Sector: A Pragmatic Approach, Addison - Westley Publishing, Massachusetts, 1978
57. Simionescu, A., Buşe, F., Bud, N., Purcaru Stamin, I.
- Control Managerial, Editura Economică, Bucureşti, 2006
58. Tabără, N. - Contabilitate şi control de gestiune. Studii şi cercetări , Editura Tipo Moldova, Iaşi, 2004
59. Tabără, N. - Modernizarea contabilităţii şi controlului de gestiune, Editura Tipo Moldova, Iaşi, 2006
60. Tabără, N. - Control de gestiune, Editura TipoMoldova, Iaşi, 2009
61. Tabără, N., Briciu, S. (coord.)
- Cercetări privind modernizarea în contabilitate şi control de gestiune, Editura Tipo Moldova, Iaşi, 2011
62. Tănăsescu, P. - Managementul financiar al activităţii sanitare, Editura Tribuna Economică, Bucureşti, 2001
63. Tănăsescu, P. - Economia sanitară şi management financiar, Editura Rao, Bucureşti, 2003
64. Tiron Tudor, A., Gherasim, I.
- Contabilitatea instituţiilor publice, Editura Dacia, 2002, Cluj Napoca
65. Vijayakumar, T. - Accounting for Management, Tata McGraw Hill, New Delhi, 2010
66. Vlădescu, C. - Managementul serviciilor de sănătate, Editura Expert, Bucureşti, 2000
67. Vlădescu, C. (coord.) - Sănătate publică şi management sanitar. Sisteme de sănătate, Editura Cartea Universitară, Bucureşti, 2004
68. Warren, C.S., Reeve, J.M., Duchac, J.
- Financial and Managerial Accounting, South-Western Cengage Learning Publisher, USA, 2009
69. Webster, W. - Accounting for managers, McGraw-Hill Irwin, 2004
70. Weygandt, J.J., Kimmel, P.D., Kieso, D.E.
- Managerial Accounting: Tools for Business Decision Making, 5th Edition, John Wiley & Sons, New Jersey, 2010
71. Young, D.W. - Management Accounting in Health Care Organizations, Jossey-Bass Publisher, San Francisco, 2003
72. *** - Şcoala Naţională de Sănătate Publică şi Management Sanitar, Managementul spitalului, Editura Public H Press, Bucureşti, 2006

25
Scientific articles published in journals or volume of national and international conferences
73. Abernethy, M.A., Chua, W.F., Luckett, P.F., Selto, F.H.
- Research in managerial accounting: Learning from others’ experiences, în Accounting and Finance, no. 39(1999), pp. 1-27
74. Albu, C., Albu, N. - Bugetele - între tradiţie şi reformă: o tipologie a funcţiilor şi formelor procesului bugetar, în Contabilitatea, Expetiza şi Auditul Afacerilor, nr.11/2006, pp. 48-53
75. Albu, N. - O investigaţie asupra naturii şi întinderii atribuţiilor de contabilitate managerială în România, la Congresul al XVI-lea al profesiei contabile din România, Bucureşti, 15-16 septembrie 2006, pp. 27-48
76. Albu, N., Albu, C. - Fenomenul de convergenţă în contabilitatea managerială: între discurs şi realitate, în Expertiza şi Auditul Afacerilor, nr. 3 (2008), pp. 44-49
77. Aldea, A. - Ghid privind efectuarea analizei diagnostic în unităţile sanitare, în Revista Administraţie şi Management Public, nr. 3 (2004), Editura ASE Bucureşti
78. Armean, P. - Analiza sistemelor de sănătate din perspectiva calităţii, în Revista Management în Sănătate, nr. 3 (2002)
79. Bârliba, I., Siniţchi, G. - Sisteme de sănătate europene, în Revista Practica Medicală, Empire Publishing, vol. 3/2008, nr. 3(11), pp. 116-121
80. Berheci, I., Budugan, D.
- Contabilitatea şi exigenţele manageriale în contextul economiei de piaţă, în Buletinul Ştiinţific al Universităţii George Bacovia Bacău, 1998, pp. 47-48
81. Bigliardi, B., Alberto Ivo Dormio, Galati, F.
- Balanced Scorecard for the Public Administration: Issues from a Case Study, în International Journal of Business, Management and Social Sciences, vol. 2, no. 5, 2011, pp. 1-16, disponibil la http://www.ijbmss-ng.com/ijbmss-ng-vol2-no5-pp1-16.pdf (accesat 30 aprilie 2012)
82. Briciu, S., Căpuşneanu, S.
- Aspecte ale normalizării contabilităţii manageriale din România la nivel microeconomic, în Revista Economie Teoretică şi Aplicată, vol. XVIII (2011), nr. 3 (556), pp. 57-68, disponibil la http://store.ectap.ro/articole/573_ro.pdf (accesat 3 septembrie 2011)
83. Briciu, S., Teiuşan, S.C.
- Sistemul informaţional al contabilităţii de gestiune, în Revista Annales Universitatis Apulensis Series Oeconomica, Universitatea 1 Decembrie 1918 Alba Iulia, nr. 8/2006, vol. 1, pp. 17-23, disponibil la http://oeconomica.uab.ro/upload/lucrari/820061/3.pdf (accesat12 iunie 2011)
84. Budugan, D., Georgescu, I.
- Decizii pe bază de costuri în condiţii de incertitudine, în Analele Ştiinţifice ale Universităţii Alexandru Ioan Cuza Iaşi, Seria Ştiinţe Economice, Tom LII/LIII, 2005/2006, pp. 9-13, disponibil la http://anale.feaa.uaic.ro/anale/resurse/01_Budugan_D,_Georgescu_I_-_Decizii_pe_baza_de_costuri_in_conditii_de_incertitudine.pdf (accesat 11 iunie 2011)
85. Budugan, D., Georgescu, I., Creţu, L.
- Relaţia cost-valoare în contabilitatea managerială, la Congresul al XVIII-a al profesiei contabile din România: «Pentru o nouă cultură în profesia contabilă», 3-4 septembrie 2010, Bucureşti, Editura CECCAR, 2010, pp. 55-72
86. Capps, C., Dranove, D., Lindrooth, R.C.
- Hospital closure and economic efficiency, în Journal of Health Economics, vol. 29 (2010), pp. 87-109, disponibil la http://www.sciencedirect.com/ (accesat 19 iulie 2012)
87. Cardinaels, E., Roodhooft, F., van Herck, G.
- Drivers of cost system development in hospitals: results of a survey, în Health Policy, vol. 69 (2004), pp. 239-252, disponibil la http://www.sciencedirect.com/ (accesat 19 iulie 2012)
88. Căpuşneanu. S. - Metoda ABC (Activity-Based Costing). Principiile gestiunii pe activităţi, în Revista Economie Teoretică şi Aplicată, nr. 432/2005
89. Căpuşneanu. S., Martinescu, D.M.
- Convergenţa principiilor ABC şi ABM - garanţia unui management performant, în Revista Economie Teoretică şi Aplicată, vol. XVII (2010), nr. 10 (551), pp. 51-61, disponibil la http://store.ectap.ro/articole/180.pdf (accesat 18 septembrie 2011)
90. Cokins, G., Căpuşneanu, S.
- Menţinerea în funcţiune a unui sistem eficient ABC/ABM, în Revista Economie Teoretică şi Aplicată, Vo.l XVIII (2011), nr. 2 (555), pp. 46-57, diponibil la http://store.ectap.ro/articole/555_ro.pdf (accesat 14 august 2011)
91. Constantin, C., Gănescu, R.
- Sistemul de sănătate: concept şi importanţă, în Jurnalul Cercetării Doctorale în Ştiinţe Economice, vol. I, nr. 3, Editura ASE Bucureşti, 2009
92. Dascălu, C., Caraiani, C., Dumitrana, M.
- Bugetarea şi controlul bugetar - o provocare pentru economia românească, în Analele Universităţii Orade, Seria Ştiinţe Economice, tom XV, vol. 2, 2006, pp. 468-472, disponibil la http://steconomice.uoradea.ro/anale/vol./2006/finante-contabilitate-si-banci/21.pdf (accesat 4 iunie 2011)
93. Daum, J.H. - Beyond Budgeting: A Model for Performance Management and Controlling in the 21st Century?, în Controlling & Finance, July 2002 issue, pp. 1-3, disponibil la http://www.juergendaum.de/articles/beyond_budgeting.en.pdf (accesat 2 septembrie 2012)
94. Dirsmith, M.W., Jablonsky, S.F., Luzi, A.D.
- Planning and Control in the US Federal Government: a Critical Analysis of PPB, MBO and ZBB, în Strategic Management Journal, vol. I, no. 4, 1980, publicat on-line 17 august 2006, pp. 303-329, disponibil la http://onlinelibrary.wiley.com/doi/10.1002/smj.4250010403/abstract (accesat 8 mai 2010)
95. Doboş, C. - Finanţarea sistemelor de sănătate în ţările Uniunii Europene. România în context european, în Revista Calitatea Vieţii , vol. XIX, nr. 1-2, Editura Academiei Române, 2008, pp. 107-123, disponibil la http://www.revistacalitateavietii.ro/2008/CV-1-2-2008/06.pdf (accesat 26 august 2010)
96. Donaldson, C., Magnussen, J.
- DRGs: the road to hospital efficiency, în Health Policy, vol. 21(1), May 1992, pp. 47-64, disponibil la http://www.sciencedirect.com/ (accesat 19 iulie 2012)
97. Dothan, M.U., Thompson, F.
- A Better Budget Rule, în Journal of Policy Analysis and Management, vol. 28, no. 3 (2009), pp. 463-478, disponibil la http://papers.ssrn.com/sol3/papers.cfm?abstract_id=1077555 (accesat 2 septembrie 2012)
98. Drăgoi, C.M., Ionescu, E., Iamandi, I.E., Chiciudean, A., Constantin, L.G.
- An economic analysis of the romanian healthcare system based on an european comparative approach, în WSEAS Transactions on Business and Economics, vol. 5, issue 6, June 2008, pp. 330-340, disponibil la adresa: http://www.wseas.us/e-library/transactions/economics/2008/27-578.pdf (accesat 30 aprilie 2011)
99. Florea, G. - Consideraţii privind obiectivele informaţiei contabile în sectorul public, în Analele Universităţii din Oradea, Fascicula Ştiinţe Economice, tom XV, vol. II, 2006, pp. 643-646

26
100. Fragidis, L., Chatzis, V. - Modeling Hospital Expenses for a Patient Accounting System, în International Scientific Conference Computer Science, vol. 2 (2008), pp. 449-455, disponibil la http://csconf.org/vol.2/page449.pdf (accesat 12 septembrie 2011)
101. Gheorghiţă, M. - Posibilităţi de implementare a managementului strategic în unităţile sanitare, în Revista Management în Sănătate, nr. 3/2006, pp. 7-10
102. Guinea, F. - Ingerinţe culturale în contabilitatea managerială, în Revista de Economie Teoretică şi Aplicată, nr. 6/2006(501), pp. 69-72, disponibil la http://store.ectap.ro/articole/113.pdf (accesat 10 iunie 2011)
103. Gumbus, W., Bellhouse, D.E., Lyons, B.
- A three-year journey to organizational and financial health using the balanced scorecard: A case study at a Yale New Haven health system hospital, în Journal of Business & Economic Studies, vol. 9, issue 2(2003), pp. 54-64
104. Gupta, K., Gunasekaran, A.
- Costing in New Enterprise Environment: Challenge for Managerial Accounting Researchers and Practitioners, în Managerial Auditing Journal, vol. 20, no. 4 (2005), pp. 337-353, disponibil la http://www.emeraldinsight.com/journals.htm?articleid=1463718&show=html (accesat 30 august 2011)
105. Haraga, S., Ţurlea, E. - Alocarea resurselor catre spitale pe baza costurilor standard pe grupe de diagnostic, în Revista Management în Sănătate, nr. 1/2009, pp. 11-14
106. Haslam, C., Lehman, G.
- Accounting for healthcare: Reform and outcomes, în Accounting Forum, vol. 30 (2006), pp. 319-323, disponibil la http://www.sciencedirect.com/ (accesat 19 iulie 2012)
107. Healy, J., McKee, M. - Implementing hospital reform in central and eastern Europe, în Health Policy, vol. 61, issue 1 (2002), pp. 1-19, disponibil la http://www.sciencedirect.com/ (accesat 19 iulie 2012)
108. Inamdar, N., Kaplan R.S., Bower, M., Reynolds, K.
- Applying the Balanced Scorecard in Healthcare Provider Organizations, în Journal of Healthcare Management, vol. 47, issue 3, May/June 2002, pp. 179-195, disponibil la http://www.ncbi.nlm.nih.gov/pubmed/12055900 (accesat 10 iunie 2011)
109. Johnsen, A. - Balanced scorecard: theoretical perspectives and public management implications, în Managerial Auditing Journal, vol. 16, issue 6 (2001), pp. 319-330
110. Kaplan, R.S. - The Balanced Scorecard and Nonprofit Organizations, în Balanced Scorecard Report, Harvard Business Publishing Newsletters, November-December 2002, pp. 1-4, disponibil la http://hbr.org/product/balanced-scorecard-and-nonprofit-organizations/an/B0211A-PDF-ENG (accesat 21 august 2011)
111. Kaplan, R.S., Norton, D.P.
- Using the Balanced Scorecard as a Strategic Management System, în Harvard Business Review, January-February 1996, pp. 75-85
112. Lee, M.T., Su, Z.Y., Hou, Y.H., Liao, H.C., Lian, J.D.
- A decision support system for diagnosis related groups coding, în Expert Systems with Applications, vol. 38 (2011), pp. 3626-3631, disponibil la http://www.sciencedirect.com/ (accesat 19 iulie 2012)
113. Lehtonen, T. - DRG-based prospective pricing and case-mix accounting - Exploring the mechanisms of successful implementation, în Management Accounting Research, vol. 18 (2007), pp. 367-395
114. Leister, J.E., Stausberg, J.
- Comparison of cost accounting methods from different DRG systems and their effect on health care quality, în Health Policy, vol. 74 (2004), pp. 46-55, disponibil la http://www.sciencedirect.com/ (accesat 19 iulie 2012)
115. Leyenaar, H. - Management accounting for hospitals, în South African Medical Journal, vol. 87, no. 10(1997), pp. 1349-1351, disponibil la http://archive.samj.org.za/ (accesat 15 septembrie 2011)
116. Maiga, A.S., Jacobs, F.A.
- Balanced Scorecard, Activity-Based Costing and Company Performance: An Empirical Analysis, în Journal of Management Issues, vol. 15 (3), 2003, pp. 283-301
117. McClintock Roe, A., Liberman, A.
- A Comparative Analzsis of the United Kingdom and the United States Healthcare Systems, în The Health Care Manager, vol. 23, no. 3 (2007), pp. 190-212, disponibil la http://www.slideshare.net/abbiemc/A-Comparative-Analysis-of-the-UK-and-US-Health-Care-Systems (accesat 2 februarie 2012)
118. Mihăescu-Pinţia, C. - Metodologie de calculare a costurilor spitaliceşti la nivel de pacient, în Revista Management în Sănătate, Anul VIII, nr. 4, Decembrie 2005
119. Mitu, N.E., Nanu, R.M., Mitu, I.E.
- Tipuri de abordare a bugetului operaţional, în Revista Tribuna Economică, vol. 18, nr. 7 (2007), pp. 84-86
120. Moldovan, B.A., Pavel, A., Hogye, M.
- Deficite bugetare şi datoria publică, în Revista Transilvană de Ştiinţe Administrative, vol. 2 (26)/2010, pp. 55-66, disponibil la http://www.rtsa.ro/files/TRAS-26Special-2010-5Moldovan-Pavel-Mihaly.pdf (accesat 20 februarie 2012)
121. Olteanu, M. - Metode de creştere a eficienţei utilizării resurselor în sănătate, în Revista Medica Academica, Martie 2011, disponibil la http://medicaacademica.ro/2011/03/17/metode-de-crestere-a-eficientei-%E2%80%A8utilizarii-resurselor-in-sanatate/ (accesat 6 august 2011)
122. Or, Z., Renaud, T., Com-Ruelle, L.
- One price for all? Sources of cost variations between public and private hospitals, Institute for Research and Information in Health Economics, Working paper, no. 25, May 2009, disponibil la http://www.irdes.fr/EspaceRecherche/DocumentsDeTravail/DT25EcartsCoutHospitaliers.pdf (accesat 2 martie 2011)
123. Palmer, G., Reid, B. - Evaluation of the performance of diagnosis-related groups and similar casemix systems: methodologies and issues, în Health Services Management Research, vol. 14, issue 2(2001), pp. 71-81
124. Paraschivescu, M.D., Fotache, G.
- Contabilitatea managerială în procesul informaţional decizional, în Buletin Ştiinţific Universitatea George Bacovia Bacău, Anul IX, nr. 1 (2006), pp. 56-61, Editura SedCom Libris, Iaşi, disponibil la http://www.ugb.ro/etc/issues/issueno1-2006.pdf#page=56 (accesat 25 iunie 2011)
125. Patel, B., Chaussalet, T., Millard, P.
- Balancing the NHS balanced scorecard!, în European Journal of Operational Research, vol. 185, issue 3(2008), pp. 905-914, disponibil la http://www.sciencedirect.com/science/article/pii/S0377221706005698 (accesat 15 iunie 2011)
126. Pete, Şt., Cardoş, I.R. - Sarcinile şi atribuţiile profesionistului contabilităţii manageriale în era globalizării şi tehnologizării, în Studia Universitatis Vasile Goldiş Arad - Seria Ştiinţe Economice, nr. 5(2), 2011, pp. 544-553, disponibil http://www.uvvg.ro/studiaeconomia/images/2001/v1/63.%20SARCINILE%20SI%20ATRIBUTIILE%20PROFESIONISTULUI.pdf (accesat 21 ianuarie 2012)

27
127. Pettersen, I.J. - Implementing management accounting reforms in the public sector: the difficult journey from intentions to effects, în European Accounting Review, vol. 10, issue 3 (2001), pp. 561-581
128. Pina, V., Torres, L. - Reshaping public sector accounting: An international comparative view, în Canadian Journal of Administrative Science, vol. 20/2003, no. 4, pp. 334-350
129. Plumb, I. - Serviciile de sănătate şi asigurările sociale de sănătate în Revista Administraţie şi Management Public, nr. 1/2003, pp. 20-29, disponibil la http://ramp.ase.ro/_data/files/articole/1_02.pdf (accesat 22 iulie 2010)
130. Plumb, I., Zamfir, A. - Realităţi şi tendinţe ale managementului serviciilor publice de sănătate, în Revista Administraţie şi Management Public, nr. 3/2004, Editura ASE Bucureşti
131. Popa, L.A. - Recursul la contabilitatea managerială, o problemă de actualitate, în Revista Amfiteatru Economic, nr. 16, Septembrie 2004, Editura ASE Bucureşti, pp. 75-79, disponibil la http://www.amfiteatru economic.ase.ro/arhiva/pdf/no16/articol_fulltext_pag75.pdf (accesat 16 decembrie 2011)
132. Pyhrr, A.P. - Zero Base Budgeting, în Harvard Business Review, vol. 48, issue 6, Nov-Dec 1970, pp. 111-121
133. Reid, B., Sutch, S. - Comparing diagnosis-related group systems to identify design improvements, în Health Policy, vol. 87 (2008), pp. 82-91, disponibil la http://www.sciencedirect.com/ (accesat 19 iulie 2012)
134. Ristea, A.L., Stegăroiu, I., Ioan-Franc, V., Dinu, V.
- Reactivitatea sistemelor de sănătate: barometru al calităţii serviciilor medicale, în Revista Amfiteatru Economic, vol. XI, nr. 26, Editura ASE Bucureşti, 2009, pp. 277-287
135. Roslender, R. & Hart, S.J.
- In search of strategic management accounting: theoretical and field study perspectives, în Management Accounting Research, vol. 14, no. 3 (2003), pp. 255-279, disponibil la http://igup-urfu.ru/docs/Bank%20English_Transleted%20Articles/English/Strategic%20Management/In%20search%20of%20strategic%20management%20accounting.pdf (accesat 7 februarie 2012)
136. Ruffner, M., Wehner, J., Witt, M.
- Budgeting in Romania, în OECD Journal on Budgeting, vol. 4, no. 4 (2005), pp. 27-54, disponibil la http://www.oecd-ilibrary.org/governance/budgeting-in-romania_budget-v4-art20-en şi http://www2. gtz.de/dokumente/bib/06-0572.pdf (accesat 4 aprilie 2010)
137. Russell, K., Siegel, G., Kulesza, B.
- Counting More, Counting Less: Transformations in the Management Accounting Profession, în Strategic Finance Magazine, Institute of Management Accountants Publisher, vol. 81, issue 3, September 1999, pp. 39-44, disponibil la http://www.allbusiness.com/accounting/316010-1.html (accesat august 2011)
138. Ruud Hansen, T.W. - Changes in the utilization of diagnostic codes in neonatology following the introduction of activity- based financing, în Health Policy, vol. 74 (2005), pp. 218-223, disponibil la http://www.sciencedirect.com/ (accesat 19 iulie 2012)
139. Schaefer, C. - Descrierea reformei managementului financiar public - despre greşeala comună de a supraestima reforma ca remediu universal şi cum să eviţi acest lucru, în Revista Administraţie şi Management Public, nr. 6/2006, pp. 8-12
140. Scheller-Kreinsen, D., Quentin, W., Busse, R.
- DRG-Based Hospital Payment Systems and Technological Innovation in 12 European Countries, în Value in Health, vol. 14(2011), pp. 1166-1172, disponibil la http://www.sciencedirect.com/ (accesat 19 iulie 2012)
141. Schreyögg, J., Stargardt, T., Tiemann, O., Busse, R.
- Methods to determine reimbursement rates for diagnosis related groups (DRG): A comparison of nine European countries, în Health Care Management Science Journal, vol. 9, no. 3, august 2006, Springer Netherlands, pp. 215-223
142. Scorţe, C. - Calculaţia costurilor pe activităţi, în Analele Universităţii Oradea, Seria Ştiinţe Economice, tom XV, vol. 2, 2006, pp. 297-303, disponibil la http://steconomice.uoradea.ro/anale/vol./2006/finante-contabilitate-si-banci/48.pdf (accesat 19 iunie 2011)
143. Scorţe, C., Farcaş, M., Bogdan, V., Balaciu, D.
- Modernizarea contabilităţii de gestiune prin metoda ABC, în Analele Universităţii din Oradea. Ştiinţe Economice, tom XIV, 2005, pp. 454-457, diponibil la http://steconomice.uoradea.ro/ anale/vol./2005/finante-contabilitate-banci/45.pdf (accesat 10 iulie 2011)
144. Sharma, B., Gadenne, D.
- Balanced Scorecard Implementation in a Local Government Authority: Issues and Challenges, în Australian Journal of Public Administration, vol. 70, issue 2, June 2011, pp. 167-184, disponibil la http://onlinelibrary.wiley.com/doi/10.1111/j.1467-8500.2011.00718.x/full (accesat 28 martie 2012)
145. Sherlekar, V.S., Dean, B.V.
- An Evaluation of the Initial Year of Zero-Base Budgeting in the Federal Government, în Management Science Journal, vol. 26, no. 8, August 1980, pp. 750-772, disponibil la http://mansci.journal.informs.org/content/26/8/750.abstract (accesat 14 mai 2010)
146. Shields, M.D. - Management accounting practices in Europe: A view from the States, în Management Accounting Research, vol. 9, no. 4(1998), pp. 501-513
147. Shutt, J. - Balancing the Health Care Scorecard, în Managed Care Magazine, September 2003, pp. 42-46, disponibil la http://www.managedcaremag.com/archives/0309/0309.peer_balanced.pdf (accesat 14 octombrie 2011)
148. Siciliani, L., Hafsteinsdóttir, E.J.G.
- DRG prospective payment system: refine or not refine?, Discussion Papers in Economics The University of York Management School, no. 28, 2008
149. Soderlund, N., Milne, R., Gray, A., Raferty, J.
- Differences in hospital casemix, and the relationship between casemix and hospital costs, în Journal of Public Health Medicine, vol. 17, issue 1 (1995), pp. 25-32
150. Stamatian, F., Ciortea, C., Sauciuc, D.G., Dehelean, C.
- Managementul informaţiei în spital - o provocare pentru spitalele din România, în Revista Transilvană de Ştiinţe Administrative, vol. 1 (25)/2010, pp. 215-224, disponibil la http://www.rtsa.ro/ files/RTSA%2025%20-%2010%20-%20STAMATIAN,%20CIORTEA,%20SAUCIUC, %20DEHELEAN.pdf (accesat 20 februarie 2012)
151. Stănescu, S. - Exigenţe privind managementul calităţii. Studiu de caz: unităţi sanitare, la Lucrările Olimpiadei Naţionale a Studenţilor Economişti, Secţiunea Management, 26-28 Octombrie 2007, Editura Universităţii Petru Maior, Târgu Mureş, 2008, disponibil la http://www.upm.ro/ facultati_departamente/ ea/onm2007/SECTIUNEA%202/Stanescu_Suzana.pdf (accesat 10 aprilie 2012)
152. Şandor, S.D., Raboca, H.
- Măsurarea performanţelor în administraţie publică, în Revista Transilvană de Ştiinţe Administrative, nr. 3 (12), 2004, pp. 150-157

28
153. Ştefănescu, A., Dobrin, C., Calu, D.A., Ţurlea, E.
- Controverse privind măsurarea performanţei entităţilor administraţiei publice din România, în Revista Transilvană de Ştiinţe Administrative, nr. 1 (25), 2010, pp. 225-242, diponibil la adresa http://www.rtsa.ro/files/RTSA%2025%20-%2011%20-%20STEFANESCU,%20DOBRIN,%20CALU ,%20TURLEA.pdf (accesat 9 iulie 2011)
154. Tiron Tudor, A., Muţiu A.
- Balanced scorecard - A modern instrument in management, în Revista de Management şi Inginerie Economică, vol. 5, no. 3(19), 2006, pp. 95-105
155. Ţânţă, A.E. - Contabilitatea managerială între realitate şi oportunitate, în Analele Universităţii Oradea, Seria Ştiinţe Economice, vol. 2, tom XV, 2006, pp. 466-470, disponibil la http://steconomice .uoradea.ro/anale/vol./2006/finante-contabilitate-si-banci/78.pdf (accesat 12 octombrie 2011)
156. Ţurlea, E. - Auditul performanţei, element esenţial al perfecţionării managementului organizaţiilor sectorului public, în Revista Annales Universitatis Apulensis Series Oeconomica, Universitatea 1 Decembrie 1918 Alba Iulia, vol. 1, nr. 8 (2006), disponibil la http://oeconomica.uab.ro/upload/lucrari/820061/44.pdf (accesat 25 septembrie 2011)
157. Van de Vijsel, A.R., Engelfriet, P.M.,Westert, G.P.
- Rendering hospital budgets volume based and open ended to reduce waiting lists: Does it work?, în Health Policy, vol. 100 (2011), pp. 60-70, disponibil la http://www.sciencedirect.com/ (accesat 19 iulie 2012)
158. Vasilache, S., Prejmerean, M.C.
- Estimarea eficienţei spitalelor din România în relaţie cu competiţia de pe piaţa serviciilor de sănătate, în Revista Management şi Marketing, vol. 3/2009, nr. 3, Editura Economică, Bucureşti, pp. 97-106
159. Verboncu, I., Gănescu, R.
- Performanţa spitalelor, o componentă-cheie a procesului de reformare a sistemului de sănătate din România, în Revista Administraţie şi Management Public, nr. 14/2010, Editura ASE Bucureşti, pp. 10-23
160. Vitikainen, K., Street, A., Linna, M.
- Estimation of hospital efficiency - Do different definitions and casemix measures for hospital output affect the results?, în Health Policy, vol. 89 (2009), pp. 149-159, disponibil la http://www.sciencedirect.com/ (accesat 19 iulie 2012)
161. Vlădescu, C., Astărăstoae, V.
- Integrarea serviciilor de sănătate în politica de reformă sanitară din România, în Revista Română de Bioetică, vol. 10, nr. 2, Aprilie-Iunie 2012, disponibil la http://www.bioetica.ro/atdoc/RRBv10n2_2012_Vladescu_RO.pdf (accesat 30 iulie 2012)
162. Vlădescu, C., Astărăstoae, V., Scîntee, S.G.
- Un sistem sanitar centrat pe nevoile cetăţeanului. România. Serviciile spitaliceşti, asistenţa primară şi resursele umane. Soluţii (III), în Revista Română de Bioetică, vol. 8, nr. 4, Octombrie-Decembrie 2010, disponibil la http://www.bioetica.ro/atdoc/RRBv8n4_2010_Vladescu_RO.pdf (accesat 30 iulie 2012)
163. Vlădescu, C., Scîntee, G., Olsavszky, V.
- Romania: Health system review, în European Observatory on Health Care Systems and Policies, Health Systems in Transition, vol. 10, no. 3(2008), disponibil la http://www.euro.who.int/__data/assets/pdf_file/0008/95165/E91689.pdf (accesat 15 aprilie 2011)
164. Voinea, L., Pamfilie, R. - Consideraţii privind îmbunătăţirea performanţei serviciilor furnizate de spitalele din România prin implementarea unui sistem de management integrat, în Revista Amfiteatru Aconomic, nr. 26/2009, Editura ASE Bucureşti, pp. 339-345
165. Volkán, I.R., Tiron Tudor, A., Pete, Şt., Cardoş V.
- Is Balanced Scorecard and Strategy a Successful Couple in Organization's Every Day Activity?, în International Journal of Business Strategy, no. 9(1), 2009, pp. 173-182
166. Vos, L., Dückers, M.L.A., Wagner, C., van Merode, G.G.
- Does case-mix based reimbursement stimulate the development of process-oriented care delivery?, în Health Policy, vol. 98 (2010), pp. 74-80, disponibil la http://www.sciencedirect.com/ (accesat 19 iulie 2012)
167. Walker, K.B., Dunn, L.M.
- Improving hospital performance and productivity with the balanced scorecard, în Academy of Health Care Management Journal, vol. 2(2006), pp. 85-110
168. Wilson, C., Hagarty, D., Gauthier, J.
- Results using the balanced scorecard in the public sector, în Journal of Corporate Real Estate, vol. 6, issue 1(2004), pp. 53-64
169. Witcher, B.J., Chau, V.S.
- Contrasting uses of balanced scorecards: case studies at two UK companies, în Strategic Change, Wiley InterScience, no. 17 (2008), pp. 101-114, disponibil la http://www.uea.ac.uk/~mg597/downloads/ papers/2008d.pdf (accesat 9 februarie 2012)
170. Zelman, W.N., Pink, G.H., Matthias, C.B.
- Use of the balanced scorecard in health care, în Journal of Health Care Finance, vol. 29, no. 4 (2003), pp. 1-16
Other sources (studies, reports, PhD thesis, websites, legislation)
171. Allen, R., Tommasi, D. - Managing Public Expenditures: A Reference Book for Transition Countries, traducere Waldman F., OECD, 2001, disponibil la http://www.sigmaweb.org/dataoecd/5/61/39367679.pdf (accesat 3 decembrie 2011)
172. Albu, C.N. - O analiză a valorizării învăţării organizaţionale prin intermediul instrumentelor contabilităţii manageriale, Teză de doctorat, conducător ştiinţific Prof. univ. dr. Niculae Feleagă, ASE Bucureşti, 2005
173. Albu, N. - O abordare contingentă a utilizării instrumentelor contabilităţii manageriale strategice, Teză de doctorat, conducător ştiinţific Prof. univ. dr. Niculae Feleagă, ASE Bucureşti, 2005
174. Boyle, S. - United Kingdom (England): Health system review, European Observatory on Health Care Systems and Policies, în Health Systems in Transition, vol. 13, no. 1 (2011), disponibil la http://www.euro.who.int/__data/assets/pdf_file/0004/135148/e94836.pdf (accesat 28 aprilie 2012)
175. Brăescu, M. - Controllingul costurilor şi conducerea profitabilă a întreprinderii, Teză de doctorat, conducător ştiinţific Prof. univ. dr. Marius D. Paraschivescu, ASE Bucureşti, 2007
176. Busse, R., Geissler, A., Quentin, W., Wiley, M.M. (editori)
- Diagnosis-Related Groups in Europe. Moving towards transparency, efficiency and quality in hospitals, în European Observatory on Health Care Systems and Policies, Open University Press, November 2011, pp. 115-129
177. Cardoş. I.R. - Calculaţia costurilor prin prisma teoriei şi practicii internaţionale, Teză de doctorat, conducător ştiinţific Prof. univ. dr. Dumitru Matiş, Universitatea Babeş-Bolyai Cluj Napoca, 2010
29
178. Cylus, J., Irwin, R. - The challenges of hospital payment systems, în Euro Observer - The Health Policy Bulletin of the European Observatory on Health Systems and Policies, vol. 12, no. 3(2010), disponibil la http://www.euro.who.int/__data/assets/pdf_file/0018/121743/EuroObserver_Autumn2010.pdf (accesat 25 martie 2012)
179. Davey Smith, G. - The UK national Health Service and the National Health: 1948-98, în Critical Public Health, vol. 9(1), 1999, pp. 69-74, disponibil la http://www.tandfonline.com/doi/abs/10.1080/09581599908409220 (accesat 23 februarie 2012)
180. Dragomirescu, S. - Controlul de gestiune în economia modernă, Teză de doctorat, conducător ştiinţific prof. univ. dr. Neculai Tabără, Universitatea Al. I. Cuza Iaşi, 2010
181. Geense, I.M. - Managerial Accounting, Delft University of Technology, disponibil la http://www.managerialaccounting.org/ (accesat 20 august 2011)
182. Gheorghe, A. - Gheorghe, A., Reforma spitalelor publice - Evidenţe din spaţiul european, în Observatorul Român de Sănătate, Policy Report 02/2012, Bucureşti, disponibil la http://www.ors.org.ro/ sites/default/files/Raport%20ORS%2001_2012%20-%20Reforma%20spitalelor%20publice_0.pdf (accesat 3 mai 2012)
183. Guinea, F.A. - Analiza comparativă a obiectivelor şi instrumentelor controlului de gestiune la nivel internaţional, modalitate de proiectare a unui program de reformă a contabilităţii manageriale în ţara noastră, Teză de doctorat, conducător ştiinţific Prof. dr. Niculae Feleagă, ASE Bucureşti, 2009
184. Haraga, S. - Alocarea resurselor către spitale pe baza costurilor standard pe grupe de diagnostic, Teză de doctorat, conducător ştiinţific Prof. univ. dr. Eugeniu Ţurlea, ASE Bucureşti, 2009
185. Hunter, A. - The Balanced Scorecard in Health Care: Evolution, Current State and Emerging Trends, PhD Thesis, Supervisor Gordon Hollis, Athabasca University, disponibil la http://dtpr.lib.athabascau.ca/action/viewdtrdesc.php?cpk=767&id=36113 (accesat 21 august 2011)
186. Jakab, M., Preker, A., Harding, A., Hawkins, L.
- The introduction of market forces in the public hospital sector: from new public sector management to organizational reform, în Health, Nutrition and Population, Discussion Paper, June, 2002, Washington, D.C., The World Bank, disponibil la http://siteresources.worldbank.org/ HEALTHNUTRITIONANDPOPULATION/Resources/281627-1095698140167/Jakab-TheIntroductionof-whole.pdf (accesat 10 aprilie 2012)
187. Niehaves, B., Algermissen, L.
- BASIS - Balanced Scorecards and Strategic Management Information Systems for Public Administrations, European Research Center for Information Systems, Germany, disponibil la http://udoo.uni-muenster.de/downloads/publications/1876.pdf (accesat 10 martie 2012)
188. Niven, P.R. - Using the Balanced Scorecard in the Public Sector, în The Senalosa Group paper, 2006, disponibil la http://senalosa.com/images/docs/Using_the_Balanced_Scorecard_in_the_Public_Sector.pdf (accesat 15 iunie 2011)
189. Sheppard, D., Hodgkin, D., Anthony, Y.
- Analysis of Hospital Cost: a Manual for Managers, World Health Organization, Geneva, 1998, disponibil la http://www.who.int/management/facility/hospital/en/index1.html (accesat 4 aprilie 2012)
190. Şerban, R. - Contabilitatea managerială, sursă de informaţii în trecerea de la sistemul public la parteneriatul public-privat, Teză de doctorat, conducător ştiinţific Prof. dr. Eugeniu Ţurlea, ASE Bucureşti, 2010
191. Woodward, G., Manuel, D., Goel, V.
- Developing a Balanced Scorecard for Public Health, Institute for Clinical Evaluative Sciences, Investigative Report, June 2004, Toronto, disponibil la http://www.ices.on.ca/file/ Scorecard_report_final.pdf (accesat 6 august 2011)
192. *** - Acumen Integrat, Balanced Scorecard în România 2010 - Raportul studiului, Cluj-Napoca, Mai 2011, disponibil la http://www.indicatorideperformanta.ro/premium/rapoarte/raportul-studiului-balanced-scorecard-in-romania-2010-8.html (accesat 17 iulie 2011)
193. *** - Development of the Health Care System in Germany, http://www.germanculture.com.ua/ library/facts/bl_health_care_develop.htm (accesat 28 aprilie 2011)
194. *** - NHS in England: history of the NHS, http://www.nhs.uk/NHSEngland/thenhs/nhshistory/ Pages/NHShistory1948.aspx (accesat 26 aprilie 2011)
195. *** - Societatea Academică din România, Intră sănătatea în comă?, în SAR Policy Brief, nr. 44, Noiembrie 2009, pp. 1-19, disponibil la http://www.sar.org.ro/files/412_Policy%20memo44.pdf (accesat 11 septembrie 2010)
196. *** - Legea nr. 95 din 14 aprilie 2006 privind reforma în domeniul sănătăţii, publicată în Monitorul Oficial al României nr. 372 din 28 aprilie 2006, cu modificările şi completările ulterioare
197. *** - Ordinul Ministerului Finanţelor Publice nr. 1826 din 22 decembrie 2003 pentru aprobarea precizărilor privind unele măsuri referitoare la organizarea şi conducerea contabilităţii de gestiune, publicat în Monitorul Oficial al României nr. 23 din 12 ianuarie 2001
198. *** - Ordinul Ministerului Sănătăţii nr. 1723 din 20 decembrie 2011 pentru aprobarea Normelor metodologice de aplicare în anul 2012 a Contractului-cadru privind condiţiile acordării asistenţei medicale în cadrul sistemului de asigurări sociale de sănătate pentru anii 2011-2012, publicat în Monitorul Oficial al României nr. 922 din 27 decembrie 2011
199. *** - Casa Naţională de Asigurări Sociale de Sănătate, http://www.cnas.ro/
200. *** - Centrul de Cercetare şi Evaluare a Serviciilor de Sănătate, http://www.drg.ro/
201. *** - Ministerul Sănătăţii, http://www.ms.ro/
202. *** - Şcoala Naţională de Sănătate Publică, Management şi Perfecţionare în Domeniul Sanitar, http://www.snspms.ro/
203. *** - World Health Organization, http://www.who.int/