Embed Size (px)
Citation preview

Management of Hyperlipidemia
Clinical Management Course
1/30/06
James M. May, M.D.
Department of Medicine
Vanderbilt University School of Medicine

GOALS :
• Rationale for treatment
• NCEP guidelines
• Diet therapy
• Drug therapy

-20
-26
5
-31-33
-22-25
-35
8
-34
-42
-30
-20
-28
5
-24
-19
-8
-45
-40
-35
-30
-25
-20
-15
-10
-5
0
5
10
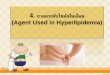
WOSCOPS (N=6,595) 4S (N=4,444) CARE (N=4,159)
N = number enrolled.
TC LDL-C
HDL-C
1o prevention 2o prevention 2o prevention
Summary of Effects of Lipid Lowering on Coronary Events in Recent Statin Trials
Nonfatal MI/CHD death
CHD death
All-cause mortality
%+

Risk of increased LDL and CHD: 30% change in = 30% change in CHD
Grundy, SM et al. . Circulation. 110:227-239, 2004.

Event Reduction and LDL: At What LDL Level Does Risk Go to Zero?
Primary Prevention Secondary Prevention
O’Keefe, JH, et al. Am. J. Cardiol. 43:2142-2146, 2004.

PI=placebo; Rx=treatment
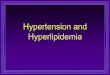
Shepherd J et al. N Engl J Med. 1995;333:1301-1307.4S Study Group. Lancet. 1995;345:1274-1275.Sacks FM et al. N Engl J Med. 1996;335:1001-1009.Downs JR et al. JAMA. 1998;279:1615-1622.Tonkin A. Presented at AHA Scientific Sessions, 1997.
Mean LDL-C level at follow-up (mg/dL)
Relation Between CHD Events and LDL-C in Recent Statin Trials
0
5
10
15
20
25
30
90 110 130 150 170 190 210
% withCHD event CARE-Rx
LIPID-Rx
4S-Rx
CARE-PILIPID-PI
4S-PI
2° Prevention
1° Prevention
WOSCOPS-PI
WOSCOPS-RxAFCAPS/TexCAPS-Rx
AFCAPS/TexCAPS-PI

New Features of NCEP Guidelines: ATP III
• LDL remains primary treatment goal
• Diabetes: CHD risk equivalent
• Framingham projections of 10-year CHD risk
– Identify certain patients with multiple risk factors for more intensive treatment
• HDL cholesterol <40 mg/dL
– Raised from <35 mg/dL
• Multiple metabolic risk factors (metabolic syndrome)

Central obesityGlucose intolerance
AtherosclerosisHypertension
Polycystic ovary syndrome
Clinical Manifestations
Lipid:Carbohydrate:
Biochemical Abnormalities
Fibrinolysis:Insulin resistanceHyperinsulinemia
High TGLow HDL-C
Small, dense LDL particles
Increased PAI-1
The Insulin Resistance Syndrome

Laboratory: Fasting Lipid Profile
• 12-h fast
• Draw total cholesterol, HDL and triglycerides
• Calculate LDL = TC – HDL – TG/5
(accurate up to TG of 400 mg/dl)
• If TG > 400, measure LDL directly following ultracentrifugation.

Causes of Secondary Dyslipidemia
• Diabetes
• Hypothyroidism
• Obstructive liver disease
• Chronic renal failure
• Drugs: Raise TG, LDL and lower HDL: progestins anabolic steroids
thiazides beta-blockers corticosteroids

LDL Cholesterol Goals and Levels for Therapeutic Lifestyle Changes (TLC) and Drug Therapy
Risk CategoryLDL Level for
TLC
(mg/dL)
LDL Level for Drug Therapy
(mg/dL)
LDL Goal (mg/dL)
0–1 Risk Factor 160190
(160–189: drug optional)
<160
2+ Risk Factors (10-year risk 20%) 130
130(10-year risk 10–20%)
160(10-year risk <10%)
<130
CHD or CHD Risk Equivalents
(10-year risk >20%)100
130 (100–129: drug
optional)
<100(<70 if very high
risk patient)

Therapeutic Lifestyle Changes• TLC Diet
– Previous Step II Diet)• Saturated fats <7% of total calories• Dietary cholesterol <200 mg per day
– LDL-lowering therapeutic options• Plant stanols/sterols (2 g/day)• Viscous (soluble) fiber (10–25 g/day)
• Weight reduction • Increased physical activity

0 1000 2000 3000 40000
20
30
40
50
60
70
1 mg/dl increase = 450 Caloriesr = 0.987, p < 0.001
HD
L (m
g/dl
)
Exercise Calories/Week

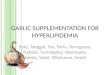
Effects of Drug Therapy and Diet on Lipids
* 84% reached NCEP LDL target (<130 mg/dL)† 63% reached NCEP LDL-C target (<100 mg/dL)
Barnard RJ, et al. Exerpta Medica Brief Reports. 1997;1112-1114.
100
125
150
175
200
225
250
275
300
325 Pre-drugDrug
Drug + diet
TC (mg/dL) * †
P<0.01
1° Prevention (n=40) 2° Prevention (n=53)

Mechanism of action of Lipid-Lowering Agents on Lipoproteins
Agents LDL-C HDL-C VLDL-C
Resins 15-40% (modest ) secretion
Niacin 10-15% 30-40% 30-40%
Fibric acids (small ) 10-15% 50%
Statins 25-50% 5-8% 20-50%
Ezetimibe 18-20% 5-8% 15-20%

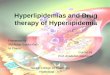
* Significantly less than atorvastatin 10 mg (P<0.02).† Significantly less than atorvastatin 20 mg (P<0.01).‡ Significantly greater than mg-equivalent dose of comparative agents (P0.01).Jones P et al. Am J Cardiol. 1998;81:582-587.
-60
-50
-40
-30
-20
-10
0
0 10 20 30 40 50 60 70 80 90
Atorvastatin
Fluvastatin
Lovastatin
Pravastatin
Simvastatin
Dose range (mg)
Mean% LDL-Creduction
*
**
*
** *
†
† †‡
‡
‡
The CURVES Trial: A Comparison of LDL-C Lowering Among Statins

-70
-60
-50
-40
-30
-20
-10
0
Baseline Week 2 Week 4 Last DB visit
Mean % in LDL-C
P<0.05.DB=double blind.
Nawrocki JW et al. Arterioscler Thromb Vasc Biol. 1995;15:678-682.
10 mg20 mg
40 mg
80 mg
Atorvastatin Dose-Response Relationship in Primary Hypercholesterolemia

Drug Therapy in Primary Prevention
If LDL goal not achieved, intensifyLDL-lowering therapy
Increase statin or add ezetimibe (or a bile acid sequestrant)
6 wks
Rx: statin, or if severe LDL increase, statin + ezetimibe
Initiate LDL-lowering drug therapy
6 wks
If LDL goal not achieved, intensify drug therapy or refer to a lipid specialist
Monitor response and adherence to therapy
If LDL goal achieved, treat other lipid risk factors
Q 4-6 mos

SUMMARY and CONCLUSIONS:
• LDL Lowering remains primary
• Stress: HDL, diabetes, & diet/exercise
• AHA step II is standard diet
• Statins as primary therapy
• Treat triglycerides, low HDL, especially if part of the “metabolic syndrome”