Embed Size (px)
Citation preview

Management of Foreign body in Management of Foreign body in liver following penetrating injury liver following penetrating injury
Presented by Dr. Rana
ChowdhuryAsst. Registrar, Dept. of Surgery, unit - 1
AbstractAbstract
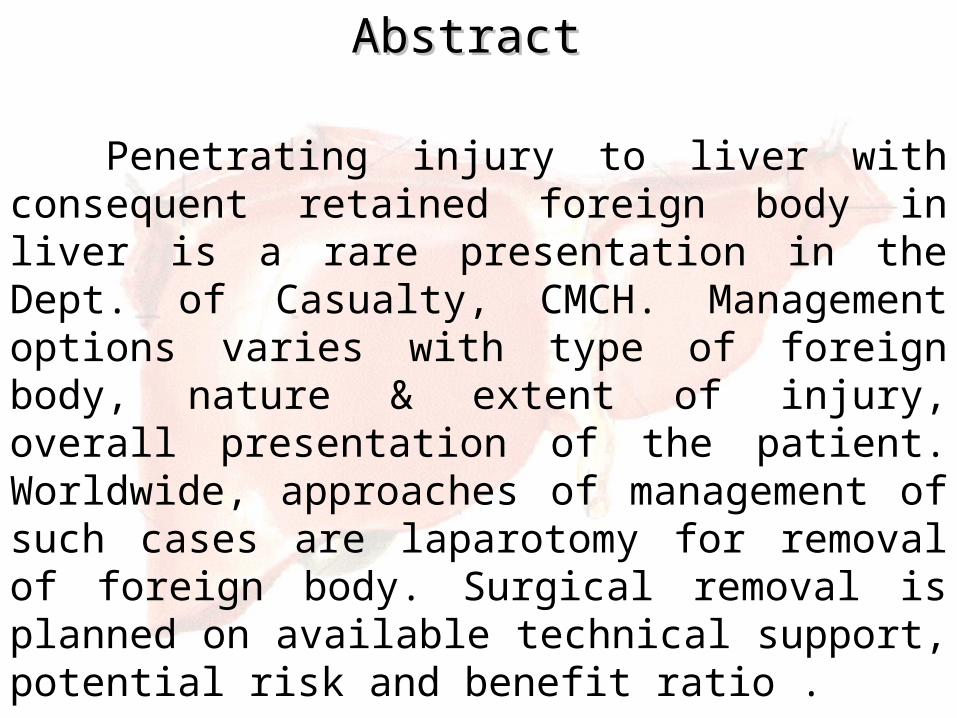
Penetrating injury to liver with consequent retained foreign body in liver is a rare presentation in the Dept. of Casualty, CMCH. Management options varies with type of foreign body, nature & extent of injury, overall presentation of the patient. Worldwide, approaches of management of such cases are laparotomy for removal of foreign body. Surgical removal is planned on available technical support, potential risk and benefit ratio .

Foreign body in liver Foreign body in liver
Foreign bodies may be introduced into the liver via penetrating trauma, surgical procedures or the ingestion of foreign bodies (which then migrate from the gut). Thus, they can be classified into the following three categories: penetrating, medical and migrated foreign bodies.

Migration of a swallowed toothpick into the liver
(a)Abdominal ultrasound demonstrates a hypoechoic
mass with heterogeneous reverberation and a linear
hyperechoic structure (whitearrow) in the medial segment
of the left lobe of the liver.
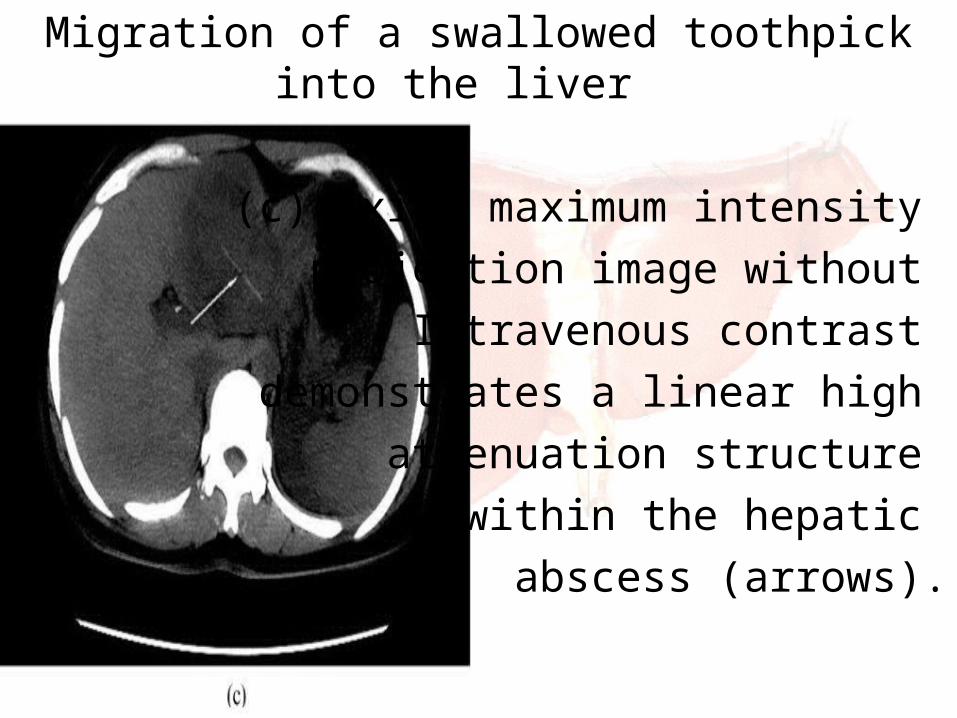
Migration of a swallowed toothpick into the liver
(c) Axial maximum intensity projection image without
Intravenous contrast demonstrates a linear high
attenuation structure within the hepatic
abscess (arrows).

Fish bone migration: an unusual cause of liver abscess A pyogenic liver abscess in a 45 year old
male was described who presented with a 10 day history of fever and abdominal pain.
A CT scan of the abdomen revealed a needle-like foreign body in the liver. At
operation a 2.5 cm fish bone was extracted from the liver. Subsequently, his feverish
symptoms disappeared, and he has remained well in the ensuing 3 month
postoperative period.

Foreign body retained in liver long after gauze packing
Foreign body retained in liver long after gauze packing
This case report describes a foreign body retained in the liver long after perihepatic gauze packing. A 64-year-old female patient had suffered a rib fracture and liver rupture during a traffic accident in 1973. She discovered a mass in her right hypochondrium. Her hepatic USG showed a round mass with fluid echogenicity in the right lobe of her liver, and a hepatic cystic-solid mass was identified in an abdominal CT scan. Several pieces of gauze were extracted, and brown pus from the hepatic mass was suctioned during her exploratory laparotomy. Histology documented gauze remnants with necrotic material inclusions and fibrotic capsules.

Foreign body granuloma mimicking liver metastasis.
The causative agent in foreign body granulomas may be suture
material, sponge used during Surgery or pieces of wood or
Glass introduced during trauma. Foreign body granulomas maycause diagnostic controversy
when they present withneoplasia-like imaging findings.

Foreign body in liver: Casualty ward, Chittagong Medical College Hospital.
case report: Mr. Kabir, 32 yrs old, S/O Mr. Moinuddin,
normotensive, non diabetic and non icteric, hailing from Vatiary, Chittagong, was admitted in our casualty ward at 11:00 AM on 02/07/13 with the complaints of •History of penetrating injury by broken tip of Rod cutting scissors over right lower chest 1 hour back. •Pain in the wound side since injury.

On general examination:
Anaemia: Absent Pulse: 84 bpmJaundice Absent BP: 130/ 80 mmHg Dehydration: Absent Resp rate: 22/ min Cyanosis: Absent Temp: 98.6 F

On Local examination: Inspection:
The wound measures about 0.5X0.3X4 cm. Mild swelling around the wound site. No active bleeding was present.
Palpation: Tenderness over the wound site. No sub cutaneous emphysema.
Auscultation: Breath sound are symmetrical in both side.

Examination of the Abdomen
Mild muscle guard in right hypochondriac region.
Abdomen was soft & non tender otherwise. Bowel sound was present.
Investigation: Chest X ray P/A view: Normal study.

Plain X ray Abdomen in erect posture A/P View
A linear radio opaque shadow was seen in the right
hypochondriac region.

Plain X ray Abdomen in erect posture right lateral view.
A linear radio opaque shadowwas seen in the peritoneal
cavity, probably in the liver.

CT scan of upper abdomen

CT scan of upper abdomen
There was a radio opaque foreign body of metallic density in the segment VI & VIII of right lobe of liver. It measured about 2.7 cm in length. Metallic artifacts are seen around the foreign body with no focal lesion within the liver.

Treatment given:
So far, patient has been treated conservatively with • Oxygen inhalation; • Resuscitation with I/V fluid; • Analgesic; • Broad spectrum antibiotic; • Anti ulcerants;

Current Status of the patient:
Now patient is haemodynamically stable, with all vital signs within normal limit; oral feeding started 2 days back (04-07-13) with no subsequent complication so far.
Next plan for treatment:
Laparotomy for removal of foreign body from the liver; after ensuring necessary technical support.

DiscussionDiscussion
• Foreign bodies may be introduced into the liver via penetrating trauma, surgical procedures or the ingestion of foreign bodies (which later migrate from the gut).
• Penetrating foreign bodies, such as bullets, shell fragments, glass and wood, can become lodged in the liver via gunshot or stab wounds.

DiscussionDiscussion
• An immediate assessment with ultrasound or CT after a blunt or penetrating abdominal injury remains the gold standard method for identifying bleeding and foreign bodies.
• Liver is the most commonly injured solid organ in blunt or penetrating abdominal or thoracic trauma, however, liver wounds associated with penetrating foreign bodies that are retained in the liver are rare.

DiscussionDiscussion
Treatment options: Hepatic penetrating foreign bodies are surgical emergencies that should prompt prophylactic extraction through laparotomy; however, the tissue injury caused by the penetrating liver trauma and not the penetrating foreign bodies themselves require surgery. Some penetrating foreign bodies, such as bullets, produce no clinical symptoms for many years.
DiscussionDiscussion Treatment options: Laparotomy remains the standard treatment for penetrating organ injuries with retained foreign bodies; however, non-operative management is preferred for stable patients, especially those with penetrating organ injuries without retained foreign bodies. Major complex surgical procedures, such as an anatomical resection, an irregular hepatotomy with direct suture and resectional debridement or artriocaval shunting, are thought to be indicated in the emergency setting in specialist units.

DiscussionDiscussion
Treatment options:
Fast and effective surgical damage control procedures (i.e., temporary gauze packing and mesh wrapping of the fragmented liver with absorbable mesh (mesh hepatorrhaphy) combined with ipsilateral ligation of the bleeding vessel) are safe and effective for treating severe liver injuries, especially in non-specialist centers or in remote, rural settings.
DiscussionDiscussion
Treatment options:
Interventional radiological techniques are becoming more widely used to more effectively manage severe liver injuries, particularly in patients who are managed non-operatively or have been stabilized using perihepatic packing.

DiscussionDiscussion
Complications if not removed: Intrahepatic haematoma; Liver abscess; Bile collection; Billiary fistula; Arteriovenous fistula; Arteriobilliary fistula. Hepatic Failure. Hepatic artery aneurism.

ConclusionConclusion
Laparotomy remains the standard treatment for penetrating organ injuries with retained foreign bodies; however, non-operative management is preferred for stable patients, especially those with penetrating organ injuries without retained foreign bodies.

ReferenceReference
Short Practice of Surgery: Bailey & Love. Hamilton Bailey’s Emergency Surgery. BMJ Case Reports 2012; doi:10.1136/bcr.09.2011.48381 of 4 World Journal of Gastroenterology: 7th June,
2013. The British Journal of Radiology, 78 (2005),
752–754. The British Journal of Radiology, 82 (2009),
e79–e81.