Embed Size (px)
Citation preview

Full Terms & Conditions of access and use can be found athttps://www.tandfonline.com/action/journalInformation?journalCode=infd20
Infectious Diseases
ISSN: 2374-4235 (Print) 2374-4243 (Online) Journal homepage: https://www.tandfonline.com/loi/infd20
Management of BK-virus infection – Swedishrecommendations
Tina Dalianis, Britt-Marie Eriksson, Marie Felldin, Vanda Friman, Anna-LenaHammarin, Maria Herthelius, Per Ljungman, Johan Mölne, Lars Wennberg &Lisa Swartling
To cite this article: Tina Dalianis, Britt-Marie Eriksson, Marie Felldin, Vanda Friman, Anna-Lena Hammarin, Maria Herthelius, Per Ljungman, Johan Mölne, Lars Wennberg & Lisa Swartling(2019) Management of BK-virus infection – Swedish recommendations, Infectious Diseases, 51:7,479-484, DOI: 10.1080/23744235.2019.1595130
To link to this article: https://doi.org/10.1080/23744235.2019.1595130
© 2019 The Author(s). Published by InformaUK Limited, trading as Taylor & FrancisGroup.
Published online: 23 Apr 2019.
Submit your article to this journal
Article views: 873
View related articles
View Crossmark data

INFECTIOUS DISEASES,2019; VOL. 51,NO. 7, 479–484
https://doi.org/10.1080/23744235.2019.1595130
REVIEW ARTICLE
Management of BK-virus infection – Swedishrecommendations
Tina Dalianisa, Britt-Marie Erikssonb, Marie Felldinc, Vanda Frimand, Anna-Lena Hammarine, MariaHertheliusf, Per Ljungmang, Johan M€olneh, Lars Wennbergi,j and Lisa Swartlingk
aDepartment of Oncology-Pathology, Karolinska Institutet, Stockholm, Sweden; bDepartment of Medical Science, Section ofInfectious Diseases, Uppsala University, Uppsala, Sweden; cTransplant Institute, Sahlgrenska University Hospital, Gothenburg,Sweden; dDepartment of Infectious Diseases, Sahlgrenska University Hospital, Gothenburg, Sweden; eUnit for LaboratoryDevelopment and Technology Transfer, The Public Health Agency of Sweden, Stockholm, Sweden; fPaediatric Nephrology, TheChildren’s and Women’s Health Theme, Karolinska University Hospital, Stockholm, Sweden; gDepartment of Cellular Therapy andAllogeneic Stem Cell Transplantation, Karolinska University Hospital, Stockholm, Sweden; hDepartment of Pathology andGenetics, Sahlgrenska Academy, University of Gothenburg, Gothenburg, Sweden; iDepartment of Clinical Science, Interventionand Technology, Karolinska Institutet, Stockholm, Sweden; jDepartment of Transplantation Surgery, Karolinska UniversityHospital, Stockholm, Sweden; kDepartment of Infectious Diseases, Karolinska University Hospital, Stockholm, Sweden
ABSTRACTBK-virus (BKV) associated nephropathy (BKVAN) and BKV associated haemorrhagic cystitis (HC) are complications of BKVinfection/reactivation in renal and allogeneic haematopoietic stem cell transplantation (HSCT) patients, respectively. Thetask of how to manage these diseases was given to the chair by the Swedish Reference Group for Antiviral Therapy (RAV).After individual contributions by members of the working group, consensus discussions were held in a meeting on 23January 2018 arranged by RAV. Thereafter, the recommendations were published in Swedish on November 2018. The cur-rent translation to English has been approved by all co-authors. High BKV serum levels suggest an increased risk forBKVAN and potential graft failure. For detection of BKVAN, careful monitoring of BKV DNA levels in serum or plasma is rec-ommended the first year after renal transplantation and when increased creatinine serum levels of unknown cause areobserved. Notably, a renal biopsy is mandatory for diagnosis. To reduce the risk for progression of BKVAN, there is no spe-cific treatment, and tailored individual decrease of immunosuppression is recommended. For BKV-HC, BKV monitoring isnot recommended, since BK-viruria frequently occurs in HSCT patients and the predictive value of BKV in plasma/serumhas not been determined. However, the risk for BKV-HC is higher for patients undergoing myeloablative conditioning, hav-ing an unrelated, HLA-mismatched, or a cord blood donor, and awareness of the increased risk and early intervention maybenefit the patients. Also for BKV-HC, no specific therapy is available. Symptomatic treatment, e.g. forced diuresis and anal-gesics could be of use.
KEYWORDSBKVtransplantationimmunosuppressionhaemorrhagic cystitisBKVANmanagement
ARTICLE HISTORYReceived 7 March 2019Accepted 8 March 2019
CONTACTTina Dalianis
[email protected] of Oncology-Pathology, Karolinska
Institutet, Bioclinicum J6:20, Karolinska UniversityHospital, 171 74 Stockholm, Sweden
� 2019 The Author(s). Published by Informa UK Limited, trading as Taylor & Francis Group.This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial-NoDerivatives License (http://creativecommons.org/licenses/by-nc-nd/4.0/),which permits non-commercial re-use, distribution, and reproduction in any medium, provided the original work is properly cited, and is not altered, transformed, or built upon inany way.

Background
Infections with BK-virus (BKV) are common and >80% ofall adults have antibodies against BKV as a result of aprevious infection [1–4]. It is assumed that BKV transmis-sion occurs through the respiratory tract or by faecal-oral transmission. BKV is transmitted through solid organtransplantation, usually in the context of a renalorgan transplant.
After an asymptomatic primary infection, generallyoccurring in early childhood, the virus establisheslatency, especially in the tubular cells of the kidney.Upon immunosuppression, BKV is frequently activatedthereby causing inflammation of the urinary tract andthe kidneys in particular. In rare situations, other organsmay also be affected. Clinical manifestations of BKV areprimarily observed in patients previously undergoingrenal, or allogeneic haematopoietic stem cell transplant-ation (HSCT) [3,4].
BKV infection in organ transplant patients
In renal transplant patients, both primary BKV infectionand reactivation of latent BKV infection may lead to thedevelopment of BKV-associated nephropathy (BKVAN),which in turn may result in progressive dysfunction ofthe graft, and ultimately, the loss of the renal transplant[4]. BKVAN is rare in other solid organ transplantedpatients, but it has been described, and the sameaccounts for BKV-associated haemorrhagic cystitis (HC),ureteral stenosis, pneumonia, encephalitis and retin-itis [3,4].
Reactivation of BKV and the detection of BKV DNA inthe urine and blood are frequently reported after renaltransplantation. BK-viruria is found in 30–40% of thepatients, and BK-viraemia in up to 29% of all renal trans-planted patients, with the highest incidence of viraemia3–6 months after transplantation [5–7]. BK-viraemia andBKVAN may occur late after transplantation and shouldbe considered upon renal dysfunction.
BK-virus-associated nephropathy
It has been reported that 5–10% of all renal transplantedpatients develop BKVAN, with the highest incidencebetween 5 and 13 months after transplantation, andwith 95% of all cases occurring within 2 years aftertransplantation [5–7]. The variation in frequency of viru-ria, viraemia and BKVAN in different reports is mostlikely due to differences in the immunosuppressive treat-ment of the patients, how the patients are monitoredand which PCR method is used. BKVAN does generallynot result in early symptoms, although an increase inserum creatinine may be the first indication. Withoutdecreasing immunosuppression more than 90% of thepatients with BKVAN will develop a decrease in theirrenal function, with a loss of the graft in half the cases.
The most important risk factor for BKVAN is theimmunosuppressive regimen, in which the total intensityof immunosuppression, but also the individual drugs areof importance. Other possible risk factors for BKVAN areBKV incompatibility (e.g. the combination of a BKV sero-positive donor and a BKV seronegative recipient), anon-going BK-viraemia in the donor, an elderly donor
Table 1. Facts: evidence- and recommendation gradinga.Quality grading of evidence
1a Systematic analysis of randomized controlled studies with homogeneity1b At least one large randomized controlled study.1c ‘All or nothing’ is ascertained when all patients died before treatment was avail-
able, but some survived after treatment, or – some survived after treatment, butafter treatment all survive.
2a Systematic analysis of cohort studies with homogeneity2b Individual cohort studies, including randomized controlled studies with low evi-
dence value (poor quality, wide confidence intervals, low inclusion of some sub-groups in a study, etc.).
2c ‘Outcome Research’3a Systematic analysis of case-control studies with homogeneity3b Individual case-control studies4 Case series with case-control studies and cohort studies with low quality5 Expert opinions without critical analysis or without being based on physiological
findings, etc.Grading of recommendationsA Based on quality grading of evidence 1a, b or cB Based on quality grading of evidence 2a, b or c, 3a or bC Based on quality grading of evidence 4D Based on quality grading of evidence 5
aAccording to the Oxford Centre for Evidence-based Medicine – Levels of Evidence (March 2009; https://www.cebm.net/2009/06/oxford-centre-evidence-based-medicine-levels-evidence-march-2009/).
480 T. DALIANIS ET AL.

(>65 years of age), a male recipient, and a high degreeof HLA mismatching [8].
Monitoring and microbiological diagnostics
For early detection of BK-viraemia, before BKVAN hasdeveloped, monitoring of BKV in plasma or serum dur-ing the first 1–2 years after renal transplantation is rec-ommended (recommendation grade B) (Table 1). Inaddition, BKV should also be monitored in plasma orserum when an increased serum creatinine level cannotclearly be explained by other causes. Also patients thatare treated for an acute graft rejection (and have there-fore received intensified immunosuppression) should becarefully monitored for a potential BKV infection/reactivation.
Schedules for monitoring of BKV infection:
� The standard patient: Monitor the presence of BKV inplasma or serum 3, 6, 9 and 12 months aftertransplantation.
� Patients with intensified immunosuppression (e.g.anti-lymphocyte globulin, rejection treatment orincreased general immunosuppression): Earlier, aswell as more frequent and prolonged monitoring of
BKV in plasma or serum than for the standard patientshould be considered.
In addition, analysis of BKV DNA in serum/plasmashould always be considered upon an increase of serumcreatinine, that does not have any other obvious explan-ation, irrespective of time after transplantation. The riskto develop BKVAN is high when >10,000 BKV DNA cop-ies/mL are observed in serum or plasma. However,BKVAN can occur (and can never be excluded) inpatients with lower BKV levels (1000–10,000 BKV DNAcopies/mL in serum/plasma) [5,9]. Of note, the levels ofBKV DNA can vary between different sample material(plasma, serum) and between different laboratories.
Morphological diagnostics
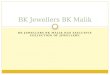
A renal biopsy is mandatory to verify the diagnosis ofBKVAN and should be performed upon increasingserum-creatinine levels and/or the finding of >10,000BKV DNA copies/mL in serum/plasma. The morpho-logical findings of BKVAN in the kidney vary dependingon when after transplantation the infection is diagnosed.The diagnosis is based on immunohistochemistryusing antibodies directed against SV40 (which in turn
Figure 1. Histological slides stained by haematoxylin–eosin (a and c) as well as immunohistochemical staining for SV-40 T antigen, thatdetect virus infected cells in the renal tubule (b and d). Pictures a and b show a biopsy from a transplanted kidney with minimal inflamma-tion (a) and no convincing morphological pictures of a BKV infection. The immune staining in (b) shows small groups of positive cell nucleiin the tubules epithelium indicating infection with BKV in the renal parenchyma. Pictures c and d show a more strongly affected renal tis-sue, with a rich infiltration of lymphocytes (c) and some oedema and fibrosis in the tissue. The findings strongly indicate the presence ofBKV, which is demonstrated by immune staining (d). G: glomerulus.
INFECTIOUS DISEASES 481

cross-react with BKV) (Figure 1). BKVAN is graded intoclasses 1–3, depending on the grade of fibrosis and thenumbers of infected cells [10]. In biopsies, it may be dif-ficult to distinguish between BKVAN in the absence vs.the presence of acute rejection. The morphology mayactually be quite similar. The presence of inflammationin arteries (endarteritis) and/or microvascular inflamma-tion suggests the presence of an acute rejectiontogether with BKVAN.
Management/treatment of BKVAN
Today, there is no specific antiviral therapy against BKVinfection, and the primary treatment strategy is todecrease immunosuppression (recommendationgrade B).
At serum/plasma levels of 1000–10,000 BKV DNA cop-ies/mL, a decrease of immunosuppression can be con-sidered (recommendation grade D) (Table 1), but therisk for rejection should always be considered.
If serum/plasma-levels are >10,000 BKV DNA copies/mL, or having a confirmed BKVAN, immunosuppressionshould be reduced (recommendation grade B). There isno generally accepted regimen for reduction ofimmunosuppression, which therefore needs to be donein collaboration with a transplantation specialist clinic,and decreasing immunosuppression should be tailoredfor each patient according to the clinical situation.
Possible alternatives:
� Lower the dose of tacrolimus, with the aim to lowerits concentration by 25–50%.
� Lower the dose of glucocorticoids.� Lower the dose of mycophenolate mofetil usually
by 50%.
Upon an insufficient effect on the levels of BKV DNA inserum/plasma, the doses of tacrolimus or mycophenolatemofetil can be reduced even more, with the possiblecomplete discontinuation of mycophenolate mofetil andglucocorticoid treatment. Immunosuppression withmTOR-inhibitor has in some studies been associated withlower rates of BKV [11], and changing mycophenolatemofetil to an mTOR-inhibitor can also be considered.
If treatment instead includes cyclosporine A or aza-thioprine, the doses of these agents can be reducedcorrespondingly.
The levels of BKV DNA usually decrease slowly, andviral levels can be analysed with 2–4-week intervals.Upon no change or increased levels of BKV DNA, an
additional decrease of immunosuppression in line withthe above should be considered. The duration of BKVDNA level monitoring is decided individually, anddepends mainly on the dynamics of viral level changes,the effects on renal function, and immunological risk.Some patients can have a low BKV DNA level in serum/plasma during long periods without affecting therenal function.
As always, when immunosuppression is reduced,there is an increased risk for a rejection of the graft. Theincreased risk of graft rejection following reducedimmunosuppression necessitates a close follow-up ofrenal function and consideration/determination of druglevels. A new renal biopsy should be considered if theserum-creatinine level goes up during the adjustment ofthe patient’s immunosuppression.
Medical treatment of BKVAN
There is no strong evidence for antiviral treatment ofBKV. Several agents have been tried, although not in thecontext of controlled studies. When a decrease ofimmunosuppression has no effect, or is not possible dueto a concomitant acute graft rejection, alternative treat-ment needs to be considered. This should always bedone in collaboration with an experienced trans-plant physician.
� Cidofovir has in some cases been reported todecrease the risk of renal dysfunction and graft rejec-tion in the context of BKVAN [12–14]. However,randomized controlled studies do not seem to exist.Based on existing data, treatment with cidofovir can-not be recommended, but neither can its usefulnessbe excluded (recommendation grade C) (Table 1).
� Brincidofovir is a prodrug of cidofovir. It results inhigher concentrations of cidofovir, but less renal tox-icity [15]. There are a few case reports where brinci-dofovir has been used for BKVAN. Brincidofovirhowever, has not been licensed in Sweden, and iscurrently not available for ‘compassionate use’ for theindication BKVAN.
� Leflunomide has immunosuppressive qualities andhas been studied as an alternative to mycophenolatemofetil for inhibiting immune responsiveness duringorgan transplantation [16]. Leflunomide also has anantiviral effect in vitro against BKV, and some studieshave reported the stabilization of renal function upontreatment of BKVAN with leflunomide. On the otherhand, it has not been possible to show that
482 T. DALIANIS ET AL.

leflunomide has any additional effect other thandecreasing immunosuppression [17]. Leflunomide isused in clinical practice at some transplantationcentres, but due to lack of scientific documentation itcannot be recommended.
� Quinolones have activity in vitro against BKV. In twocontrolled studies of renal transplant patients, whengiving quinolone as a prophylactic drug, no effectwas observed [18,19]. This was later confirmed with ameta-analysis of eight studies, where there was noprophylactic effect of quinolones on BKVAN [20].Quinolones can therefore not be recommended fortreatment or prophylaxis against BKV infection (rec-ommendation grade B).
� Intravenous immunoglobulin (IVIG) administration:commercial IVIG contains antibodies to BKV. Studieson IVIG have shown conflicting results and thereforeno recommendation can be given.
BKV infection in association to allogeneichematopoietic stem cells transplantation
BKV may induce HC in patients that have undergone anallogeneic HSCT. HC occurs in 2–66% of HSCT patients,depending on type of HSCT, conditioning and thepatient’s age. Early HC occurs <1 week after HSCT andis considered being caused by a toxic effect of the con-ditioning regimen. Late HC occurs >1 week after HSCT,and in general at the time of engraftment, and isregarded to be due to viral infection, most commonlydue to BKV reactivation/infection (but can also be dueto adenovirus infection and in rare cases infections withherpes simplex virus, cytomegalovirus or JC virus). BKVassociated HC (BKV-HC) usually occurs 2–8 weeks (1week to 6 months) after HSCT. The highest risk for BKV-HC is observed after HSCT with myeloablative condition-ing, with an unrelated or HLA mismatched donor, and inHSCT using cord blood donors [21–23].
Clinical manifestations
Clinical manifestations of BKV-HC do not differ fromthose of other HC, and may include dysuria, low abdom-inal pain, and a variable degree of haematuria. The paincan be severe and haematuria can be extensive resultingin anaemia requiring blood transfusions. Blood clottingmay also occur and result in urinary tract obstruction,which in turn can lead to secondary renal failure. Thedegree of haematuria is graded as: Grade 1: microscopichaematuria; grade 2: macroscopic haematuria; grade 3:
macroscopic haematuria with blood clots; and grade 4:renal failure due to urinary tract obstruction. The symp-toms usually decrease after 3–5 weeks.
Diagnosis
The probability of BKV-HC increases when a triad of clin-ical symptoms together with haematuria grades II–IV,and the presence BKV in the urine >7 log10 copies/mLis found (and with the exclusion of another probablecause of HC). High BKV levels are not specific for BKV-HC, since >80% of HSCT patients secrete BKV in theirurines, while only 5–20% develop BKV-HC. However, ifBKV is not found in the urine, the negative predictivevalue is very high. The predictive value of BKV inplasma/serum for BKV-HC is still under debate [17].
Treatment
The treatment is primarily symptomatic with forced diur-esis and analgesics. In severe cases, irrigation of theurinary bladder is performed. Upon extended bleedingand anaemia, erythrocyte and thrombocyte transfusionsare given. Surgery can be necessary upon obstruction ofthe urinary tract (recommendation grade B). Dependingon the risk for graft versus host disease (GVHD), theimmunosuppression of each patient should beindividualized.
Similar to BKVAN, there is a lack of controlled studiesof specific treatment directed against BKV infections andtherefore no recommendations can be given.
Acknowledgements
We thank Jan Albert and Linnea Haeggblom for valuable sugges-tions, which improved the manuscript.
Disclosure statement
The authors have no conflicts of interest.
References
[1] Knowles WA. Discovery and epidemiology of the humanpolyomaviruses BK virus (BKV) and JC virus (JCV). Adv ExpMed Biol. 2006;577:19–45.
[2] Bofill-Mas S, Pina S, Girones R. Documenting the epidemio-logic patterns of polyomaviruses in human populations bystudying their presence in urban sewage. Appl EnvironMicrobiol. 2000;66:238–245.
[3] Chesters PM, Heritage J, McCance DJ. Persistence of DNAsequences of BK virus and JC virus in normal human tis-sues and in diseased tissues. J Infect Dis. 1983;147:676–684.
INFECTIOUS DISEASES 483

[4] Rinaldo CH, Tylden GD, Sharma BN. The human polyomavi-rus BK (BKPyV): virological background and clinical implica-tions. APMIS. 2013;121:728–745.
[5] Hirsch HH, Knowles W, Dickenmann M, et al. Prospectivestudy of polyomavirus type BK replication and nephropathyin renal-transplant recipients. N Engl J Med. 2002;347:488–496.
[6] Hirsch HH, Vincenti F, Friman S, et al. Polyomavirus BK rep-lication in de novo kidney transplant patients receivingtacrolimus or cyclosporine: a prospective, randomized, mul-ticenter study. Am J Transplant. 2013;13:136–145.
[7] Schwarz A, Linnenweber-Held S, Heim A, et al. Viral origin,clinical course, and renal outcomes in patients with BKvirus infection after living-donor renal transplantation.Transplantation. 2016;100:844–853.
[8] Sawinski D, Goral S. BK virus infection: an update on diag-nosis and treatment. Nephrol Dial Transplant. 2015;30:209–217.
[9] Randhawa P, Ho A, Shapiro R, et al. Correlates of quantita-tive measurement of BK polyomavirus (BKV) DNA with clin-ical course of BKV infection in renal transplant patients. JClin Microbiol. 2004;42:1176–1180.
[10] Nickeleit V, Singh HK, Randhawa P, et al. The Banff workinggroup classification of definitive polyomavirus nephrop-athy: morphologic definitions and clinical correlations.JASN. 2018;29:680–693.
[11] Bowman LJ, Brueckner AJ, Doligalski CT. The role of mTORinhibitors in the management of viral infections: a reviewof current literature. Transplantation. 2018;102:S50–S59.
[12] Kuypers DR, Vandooren AK, Lerut E, et al. Adjuvant low-dose cidofovir therapy for BK polyomavirus interstitialnephritis in renal transplant recipients. Am J Transplant.2005;5:1997–2004.
[13] Kuypers DR, Bammens B, Claes K, et al. A single-centrestudy of adjuvant cidofovir therapy for BK virus interstitialnephritis (BKVIN) in renal allograft recipients. J AntimicrobChemother. 2008;63:417–419.
[14] Kuten SA, Patel SJ, Knight RJ, et al. Observations on theuse of cidofovir for BK virus infection in renal transplant-ation. Transpl Infect Dis. 2014;16:975–983.
[15] Reisman L, Habib S, McClure GB, et al. Treatment of BKvirus-associated nephropathy with CMX001 after kidneytransplantation in a young child. Pediatr Transplantation.2014;18:E227–E231[InsertedFromOnline.
[16] Leca N. Leflunomide use in renal transplantation. Curr OpinOrgan Transplant. 2009;14:370–374.
[17] Johnston O, Jaswal D, Gill JS, et al. Treatment of polyoma-virus infection in kidney transplant recipients: a systematicreview. Transplantation. 2010;89:1057–1070.
[18] Knoll GA, Humar A, Fergusson D, et al. Levofloxacin for BKvirus prophylaxis following kidney transplantation: arandomized clinical trial. JAMA. 2014;312:2106–2114.
[19] Lee BT, Gabardi S, Grafals M, et al. Efficacy of levofloxacinin the treatment of BK viremia: a multicenter, double-blinded, randomized, placebo-controlled trial. Clin J AmSoc Nephrol. 2014;9:583–589.
[20] Song TR, Rao ZS, Qiu Y, et al. Fluoroquinolone prophylaxisin preventing BK polyomavirus infection after renal trans-plant: a systematic review and meta-analysis. Kaohsiung JMed Sci. 2016;32:152–159.
[21] Giraud G, Priftakis P, Bogdanovic G, et al. BK-viruria andhemorrhagic cystitis are more frequent in allogeneic haem-atopoietic stem cell transplant patients receiving full condi-tioning and unrelated-HLA-mismatched grafts. BoneMarrow Transplant. 2008;41:737–742.
[22] Dalianis T, Ljungman P. Full myeloablative conditioningand an unrelated HLA mismatched donor increase the riskfor BK virus-positive hemorrhagic cystitis in allogeneichematopoietic stem cell transplanted patients. AnticancerRes. 2011;31:939–944.
[23] Cesaro S, Dalianis T, Hanssen Rinaldo C, et al. ECIL guide-lines for the prevention, diagnosis and treatment of BK pol-yomavirus-associated haemorrhagic cystitis inhaematopoietic stem cell transplant recipients. JAntimicrob Chemother. 2018;73:12–21.
484 T. DALIANIS ET AL.






![Further study of Advanced MIMO receiverpeng/MIMO-Receiver.pdf · b k [b1 b2 bk 1 bk 1 bN],bk [b1 b2 bk 1 1 bk 1 bN] and bk [b1 b2 bk 1 1 bk 1 bN] Problem: the number of combinations](https://img.dokumen.tips/doc/110x75/5fe7675492953575f353f746/further-study-of-advanced-mimo-receiver-pengmimo-b-k-b1-b2-bk-1-bk-1-bnbk.jpg)