Embed Size (px)
Citation preview

Abdelmoumen E et al IJRD ISSUE 3, 2013
Downloaded from www.jrdindia.org - 129 -
Management of a Perforating
Internal Resorptive Defect with
Mineral Trioxide Aggregate:
A Case Report
Ehsen Abdelmoumen*, Sonia Zouiten Skhiri**, Abdelatif Boughzela# * Post graduate student, Department of Conservative Dentistry and Endodontics , Faculty of Dentistry of
Monastir, Tunisia ** Professor ,Department of Conservative Dentistry and Endodontics, EPS FarhatHached-
Sousse, Tunisia #Professor, chief department of dental medicine, EPS FarhatHached-Sousse, Tunisia.
Address for correspondence: EhsenAbdelmoumen, Faculty of dentistry of Monastir , department of conservative dentistry and endodontics, Street Avicenne 5000 Monastir Telephone No.: +21698383315 Email: [email protected] Abstract : Internal root resorption is a chronic inflammatory process initiated within the pulp space with the loss of dentin along the
middle and apical thirds of the canal walls as a result of clastic activities and is generally found in teeth with previous history of trauma. It
is important to diagnose this condition and institute treatment as early as possible to improve the prognosis of such teeth. The use of
biocompatible materials like mineral trioxide aggregate (MTA) may improve the prognosis of teeth with root perforation. This paper
reports a clinical case of perforating internal root resorption treated surgically with MTA.
Keywords: calcium hydroxide, internal resorption, mineral trioxide aggregate, root perforation, surgery.
INTRODUCTION
Internal root resorption is a relatively rare
resorption of dentin which starts in the
pulpal cavity or in the root canal and
destroys surrounding dental hard tissues.
The initiating factor in internal root
resorption is thought to be trauma or
chronic pulpal inflammation, but other
etiological factors have also been
suggested like caries, pulpitis, plup
capping with calcium hydroxide, cracked
tooth, excessive heat generated during
restorative procedures on vital teeth,
orthodontic treatment (3,2,1,6,11)The
progression of the resorption phenomena
can cause the perforation of the root and
the tooth structure been compromised.
(1,2, 3, 5, 6, 7).Clinically, internal root
resorption is usually asymptomatic and is
detected coincidentally through routine
radiographs or by the clinical sign of the
crown with pinkish color known as 'pink
spot' occurs late, when integrity of crow
has been compromised.(1, 2, 3, 5, 6, 7,9).
Radiographic examination usually reveals a
fairly rounded uniform radiolucent area. It
appears as an expansion of the pulp chamber
or canal and pulp chamber.(1,4,6,7)
The prognosis for treatment of small lesions
of internal resorption is good.
However, if the tooth structure is greatly
weakened and perforation has occurred, the
prognosis is poor and tooth extraction must
be considered.
After considering the differential diagnosis,
including external root resorption, treatment
ust aim at complete extirpation of the pulp
CASE REPORT
Abdelmoumen E et al
Downloaded from www.jrdindia.org
which stops the internal resorptio
in an attempt to prevent further l
tissue.
The mineral trioxide aggregate (
proposed by Torabinejad et al an
used in several applications. It's
as a favorable perforation repair
with its superior sealing ability,
biocompatibility, fibroblastic stim
and antimicrobial activity becom
weak.(3)
Histopathologically it is characte
osteoclastic activity and the pres
lacunae which may be filled in b
tissue, presence of multinucleate
or dentinoclasts. The pulp is usu
chnonicallyinflammed and meta
pulp may occur.(6)
Case report:
A 48 years- old female patient co
department of Conservative Den
Endodontics of University Hosp
FarhatHached -Sousse Tunisia w
complaint of a fistula related to t
The patient reported a history of
trauma at the age of 30 at the ant
and at that time tooth 11 and 21
crowned. The tooth was treated p
by another praticien.
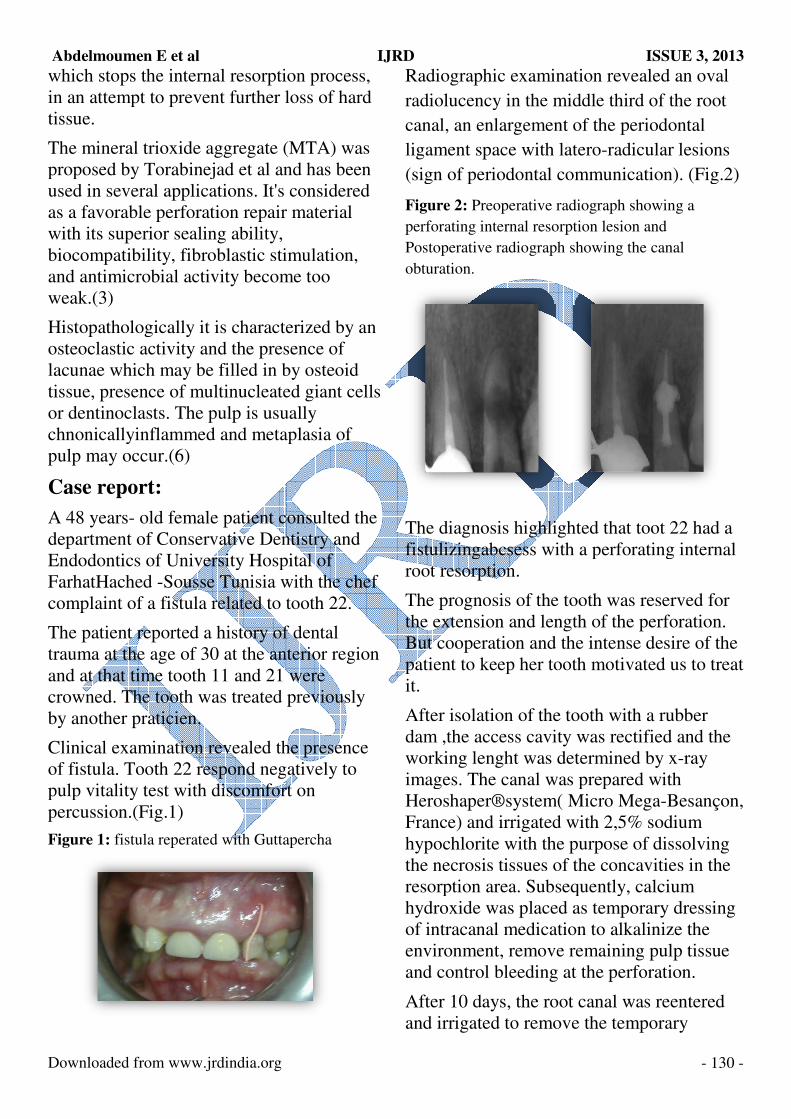
Clinical examination revealed th
of fistula. Tooth 22 respond nega
pulp vitality test with discomfort
percussion.(Fig.1)
Figure 1: fistula reperated with Gutta
IJRD
tion process,
r loss of hard
e (MTA) was
and has been
t's considered
ir material
y,
timulation,
ome too
cterized by an
resence of
by osteoid
ated giant cells
sually
taplasia of
t consulted the
entistry and
spital of
with the chef
o tooth 22.
of dental
anterior region
1 were
d previously
the presence
egatively to
ort on
ttapercha
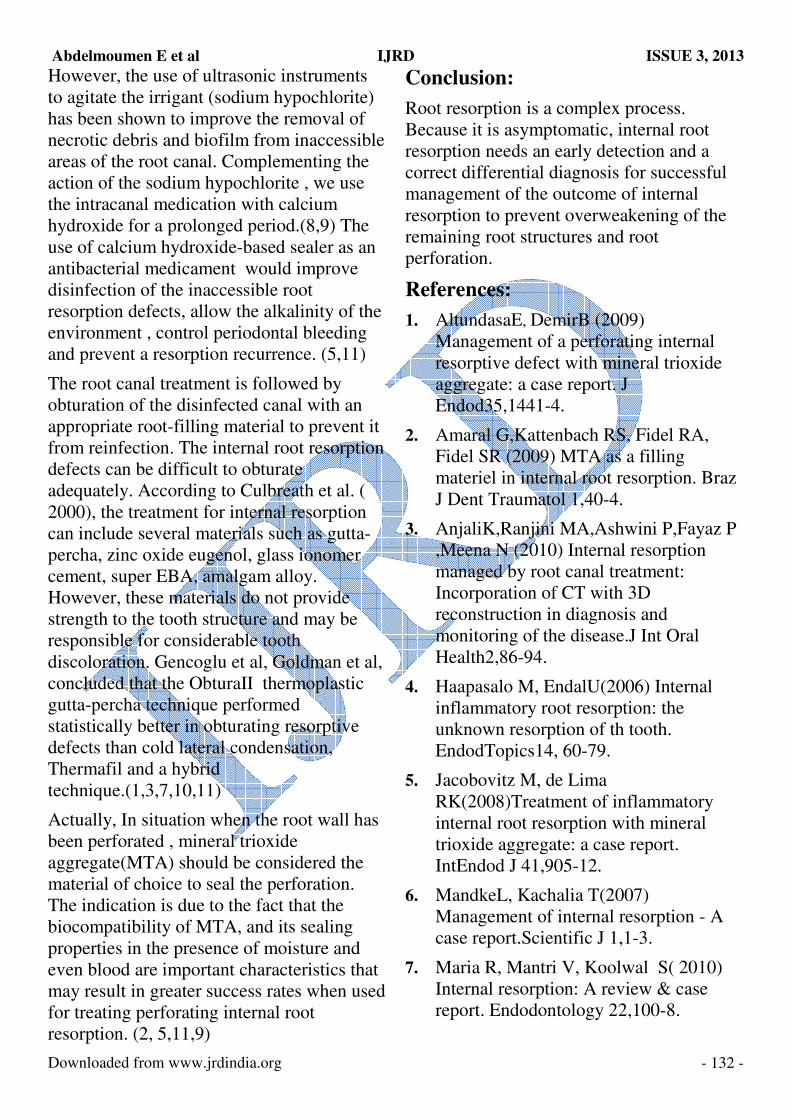
Radiographic examinat
radiolucency in the mid
canal, an enlargement o
ligament space with lat
(sign of periodontal co
Figure 2: Preoperative rad
perforating internal resorpt
Postoperative radiograph s
obturation.
The diagnosis highligh
fistulizingabcsess with
root resorption.
The prognosis of the to
the extension and lengt
But cooperation and th
patient to keep her toot
it.
After isolation of the to
dam ,the access cavity
working lenght was de
images. The canal was
Heroshaper®system( M
France) and irrigated w
hypochlorite with the p
the necrosis tissues of t
resorption area. Subseq
hydroxide was placed a
of intracanal medicatio
environment, remove r
and control bleeding at
After 10 days, the root
and irrigated to remove
ISSUE 3, 2013
- 130 -
nation revealed an oval
iddle third of the root
t of the periodontal
latero-radicular lesions
communication). (Fig.2)
adiograph showing a
rption lesion and
h showing the canal
ghted that toot 22 had a
ith a perforating internal
tooth was reserved for
gth of the perforation.
the intense desire of the
oth motivated us to treat
tooth with a rubber
ty was rectified and the
determined by x-ray
as prepared with
( Micro Mega-Besançon,
with 2,5% sodium
e purpose of dissolving
f the concavities in the
sequently, calcium
d as temporary dressing
tion to alkalinize the
e remaining pulp tissue
at the perforation.
ot canal was reentered
ve the temporary

Abdelmoumen E et al
Downloaded from www.jrdindia.org
dressing. After this, it was filled
thermoplasticized gutta-percha
technique(E&Q Wireless™, Me
co, Korea).(Fig.3)
Figure 3: Localization of the perforat
remove of the granulation tissue.
An excess filling material was re
the coronal pulp chamber, which
promptly sealed with a provision
An immediate postoperative radi
taken , showing satisfactory fillin
root canal with material extravas
perforation area due to the comm
between the internal root resorp
periodontal ligament.
Surgical treatment was necessar
the seat and extension of the per
A flap that exposed the granulati
and the perforation was elevated
granulation tissue and the excess
percha was removed. (Fig.4) . M
(Micro-Mega,Besançon, France)
and firmly condensed by using p
(Fig.5).
Finally, the flap was sutured. At
visit, the patient reported no pos
pain or discomfort.
IJRD
ed with
eta biomed
ration and
removed from
ich was
ional cement.
adiograph was
lling of the
asations in the
munication
rption and the
sary because of
perforation.
ation tissue
ed. The
ess of gutta-
MM-MTA®
ce) was placed
g plugger
At the next
ostoperative
A eight-month follow u
tooth clinically asympt
radiographic signs of h
Figure 5: Use of the MTA
repair the perforation.
Figure 6: Clinical and rad
showing satisfactory result
Discussion:
Internal inflammatory
insidious pathological
within the pulp space a
loss of dentine.
Because resorptive def
asymptomatic, they are
by routine radiograph.(
Once internal root reso
diagnosed, the clinician
decision on the progno
tooth is deemed restora
reasonable prognosis, r
must be considered, aim
cellular activity respon
resorptive activity.(Tro
The endodontic treatme
internal root resorption
the difficulty in removi
resorption cavity(8).
ISSUE 3, 2013
- 131 -
up demonstrated a
ptomatic with
f healing .(Fig.6)
A as a suitable material to
adiographic follow-up
ults.
y root resorption is an
al process, initiated
e and associated with
efects are often
are usually recognized
h.(4,10,11)
sorption has been
ian must make a
nosis of the tooth. If the
orable and has a
s, root canal treatment
aiming to arrest the
onsible for the
rope 2002)
ment of teeth with
on is complicated due to
oving the tissue of the
Abdelmoumen E et al IJRD ISSUE 3, 2013
Downloaded from www.jrdindia.org - 132 -
However, the use of ultrasonic instruments
to agitate the irrigant (sodium hypochlorite)
has been shown to improve the removal of
necrotic debris and biofilm from inaccessible
areas of the root canal. Complementing the
action of the sodium hypochlorite , we use
the intracanal medication with calcium
hydroxide for a prolonged period.(8,9) The
use of calcium hydroxide-based sealer as an
antibacterial medicament would improve
disinfection of the inaccessible root
resorption defects, allow the alkalinity of the
environment , control periodontal bleeding
and prevent a resorption recurrence. (5,11)
The root canal treatment is followed by
obturation of the disinfected canal with an
appropriate root-filling material to prevent it
from reinfection. The internal root resorption
defects can be difficult to obturate
adequately. According to Culbreath et al. (
2000), the treatment for internal resorption
can include several materials such as gutta-
percha, zinc oxide eugenol, glass ionomer
cement, super EBA, amalgam alloy.
However, these materials do not provide
strength to the tooth structure and may be
responsible for considerable tooth
discoloration. Gencoglu et al, Goldman et al,
concluded that the ObturaII thermoplastic
gutta-percha technique performed
statistically better in obturating resorptive
defects than cold lateral condensation,
Thermafil and a hybrid
technique.(1,3,7,10,11)
Actually, In situation when the root wall has
been perforated , mineral trioxide
aggregate(MTA) should be considered the
material of choice to seal the perforation.
The indication is due to the fact that the
biocompatibility of MTA, and its sealing
properties in the presence of moisture and
even blood are important characteristics that
may result in greater success rates when used
for treating perforating internal root
resorption. (2, 5,11,9)
Conclusion:
Root resorption is a complex process.
Because it is asymptomatic, internal root
resorption needs an early detection and a
correct differential diagnosis for successful
management of the outcome of internal
resorption to prevent overweakening of the
remaining root structures and root
perforation.
References:
1. AltundasaE, DemirB (2009)
Management of a perforating internal
resorptive defect with mineral trioxide
aggregate: a case report. J
Endod35,1441-4.
2. Amaral G,Kattenbach RS, Fidel RA,
Fidel SR (2009) MTA as a filling
materiel in internal root resorption. Braz
J Dent Traumatol 1,40-4.
3. AnjaliK,Ranjini MA,Ashwini P,Fayaz P
,Meena N (2010) Internal resorption
managed by root canal treatment:
Incorporation of CT with 3D
reconstruction in diagnosis and
monitoring of the disease.J Int Oral
Health2,86-94.
4. Haapasalo M, EndalU(2006) Internal
inflammatory root resorption: the
unknown resorption of th tooth.
EndodTopics14, 60-79.
5. Jacobovitz M, de Lima
RK(2008)Treatment of inflammatory
internal root resorption with mineral
trioxide aggregate: a case report.
IntEndod J 41,905-12.
6. MandkeL, Kachalia T(2007)
Management of internal resorption - A
case report.Scientific J 1,1-3.
7. Maria R, Mantri V, Koolwal S( 2010)
Internal resorption: A review & case
report. Endodontology 22,100-8.

Abdelmoumen E et al IJRD ISSUE 3, 2013
Downloaded from www.jrdindia.org - 133 -
8. Martos J, SilveiraLF,Vieira MM,Silveira
CF (2010) Internal root resorption in the
maxillary central incisor.South Braz
Dent J 7,239-4,.
9. Mente J,Hage N, Pfefferle T, et al
(2010)Treatment outcome of mineral
trioxide aggregate: repair of root
perforations. J Endod 36,208-13.
10. Milbauer S,Suda H(2008) Internal root
resorption. Endod 2,59-61.
11. Patel S, RicucciD, Durak C,TayF (2010)
Internal Root Resorption:A review. J
Endod 36, 1107-21.





























