Embed Size (px)
Citation preview

MALIGNANT POLYPS DURING THE FIRST THREE SCREENING ROUNDS (2005-2011) FOR COLON-RECTAL CANCER (CRC) IN A NORTH-EASTERN SANITARY
DISTRICT (ULSS-1 VENETO). 1Lucas G. Cavallaro, 1Pierenrico Lecis, 1Ermenegildo Galliani, 1Elisabetta Dal Pont, 2Paolo Iuzzolino, 3Fabio Soppelsa, 3Rosanna Mel, 3Sabrina Di Camillo, 1Bastianello Germanà 1Gastroenterology Unit, 2Pathology Unit, 3Public Health Service, San Martino Hospital, Belluno.
BackgroundThe malignant polyp is defined as a colonic adenoma invading the submucosal layer and it has a risk of both local and lympho-haematogenic diffusion. This lesion represents a very small group (about 6%) of CRC detected during standard colonscopies. A malignant polyp with very low risk of both local and systemic diffusion, according to both endoscopical and pathological criteria, can be treated only by endoscopic resection.
AimTo analyse both incidence and characteristics of malignant polyps during the first three consecutive CRC screening rounds.
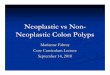
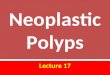
MethodsThe ULSS-1 sanitary district consists of a part of Belluno Province (in the north of Veneto region). The screening programme included all the residents aged between 50 and 69 years. The first round was performed from 2005 to 2007; the second one from 2007-2009; the third one from January 2009 to January 2011. All the inhabitants enrolled, were invited, by mail, to collect, every two years, a 1-day faecal specimen. The positive subjects were invited to undergo colonoscopy. We addressed to surgery all the malignant polyps if they were considered at high risk according to the presence of at least one either pathological or endoscopical adverse criterion. Conversely, we managed low risk malignant polyps by only an endoscopical approach. A follow-up by both an abdomen CT (computerized tomography) and endoscopy was performed after one year of detection of low risk malignant polyps. Results 1We performed 994, 721 and 719 colonoscopies during the first, second and third round respectively. Malignant polyps were detected in 14 out of 56 (25%), 9 out of 36 (25%), and 8 out of 30 (26%) in first, second and third round respectively. Among all the malignant polyps, the low risk ones were: 36% (n=5), 22% (n=2) and 25% (n=2) in the first, second and third round respectively. These low risk lesions were only managed by an endoscopic approach. Currently the patients with these lesions did not showed any local or systemic recurrence.
Risk factor for lymph nodes metastasis:
GradeG1 / G2 (low) G3/G4 (high)
Limphatic or vascular invasions
Haggitt levels (stalked lesions)
-from 1 (invasion of submucosa limited to head of polyp) to 4 (invasion of submucosa beyond the stalk)
Japanese classification (sessile/non polypoid lesion)
-Dept invasion: SM1, SM2, SM3 -Lateral invasion: SM1a, SM1b, SM1c (high grade: SM2, SM3, SMc)
Measure of the depth of invasion in the submucosa in micrometers from the lower part of the muscularis mucosae
(high grade: > 1000 m)Budding
(cluster of cells in the stroma) n: 0-9 groups: low grade 10 groups: high grades
Incomplete endoscopic removal (piece-meal)
Margin of endoscopic resection involvedASGE 2005 GISCoR 2005 Kikuchi 1995 Ueno 2004 Lambert 2009
ConclusionsDuring the three rounds, the detection rate of malignant polyps is steady higher than that obtained during colonoscopies performed to symptomatic patients. An effective endoscopic en-bloc resection, has a crucial role for both staging and treatment of these lesions.
25 2526
0
20
40
Malignant polyps %
I roundII roundIII round
36
2225
0
20
40
60
80
Low risk malignant polyps %
I roundII roundIII round
Only managed by endoscopic approach NO RECURRENCE








![Prolapsed Ano-Rectal Neoplastic Polyps in Elderly Patients ...A].pdf · over 65 years of age with prolapsed anorectal polyps which we treated by transanal excision. Patients who underwent](https://img.dokumen.tips/doc/110x75/608a7dd07ab5bf3eba4c0539/prolapsed-ano-rectal-neoplastic-polyps-in-elderly-patients-apdf-over-65.jpg)


![Transanal endoscopic microsurgery for radical resection of ...Transanal endoscopic microsurgery in sigmoid cancer 1451 JBUON 2019; 24(4): 1451 large rectal polyps by TEM [11]. However,](https://img.dokumen.tips/doc/110x75/60f7e35c60455642d5494ef7/transanal-endoscopic-microsurgery-for-radical-resection-of-transanal-endoscopic.jpg)