Embed Size (px)
Citation preview
Malignant diseases of the breast
Michael G. HalaskaDept. of Obstetrics and Gynecology
2nd Medical Faculty, Charles University

I. The breast
reproducion - nutrition
secondary sexual sign - maturition of the women, important role in sexual life
S. Freud – the role of the breast in the satisfaction of oral libido

II. The structure of the gland
15-20 lobus, which is divided into 20-40 lobulus basic structure of the gland: terminal
ductolobular unit (TDLU) - consists of acini and terminal
intralobular duct - hormonally sensitive, estrogens - ductus,
progesteron, prolaktin - lobus - size 0,3-0,6 mm (10-100/lobulus)

II. Structure - TDLU

II. Structure - arterial supply
rr. perforantes from a. mammaria interna
(a. thoracica interna) a. mammaria externa
(a. thoracica lateralis) a. thoracoacromialis a. thoracica suprema
(a. axillaris)
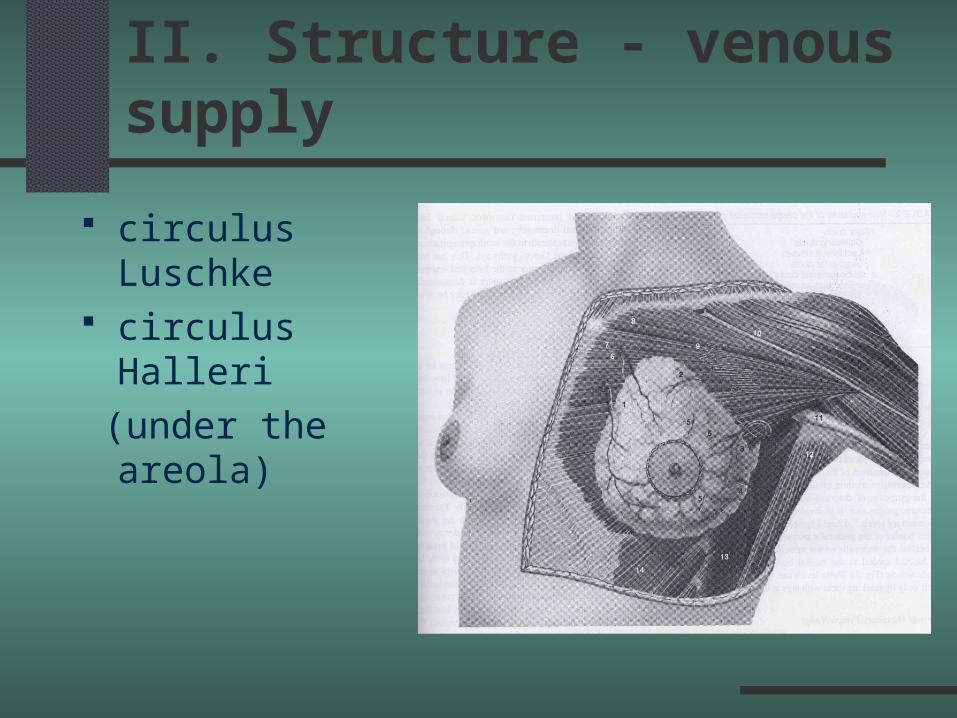
II. Structure - venous supply
circulus Luschke circulus Halleri
(under the areola)

II. Structure- lympahytic supply
lateral parts along a. thoracica lateralis into the axilla
upper parts to the apical axilla and subclavicular lymph n.
internal parts -
a. thoracica interna -
mediastinal lymph n.

III. Examination methods
self-examination (2-3 cm) physical exam – aspection, palpation (1-2cm) US - excellent differenciation between
solid and cystic structure- complementory to MG,young
women with higher density of the gland
- pregnant women MRI, CT, SPECT, PET ductography

III. Examination methods
cytology
a) secretory: from the nipple
b) punction (FNA)
- not by an suspition of malignity
- 15-20% false negativebenign malign

III. Examination methods
punctional biopsy – core-cut biopsy open biopsy
III. Examination methods
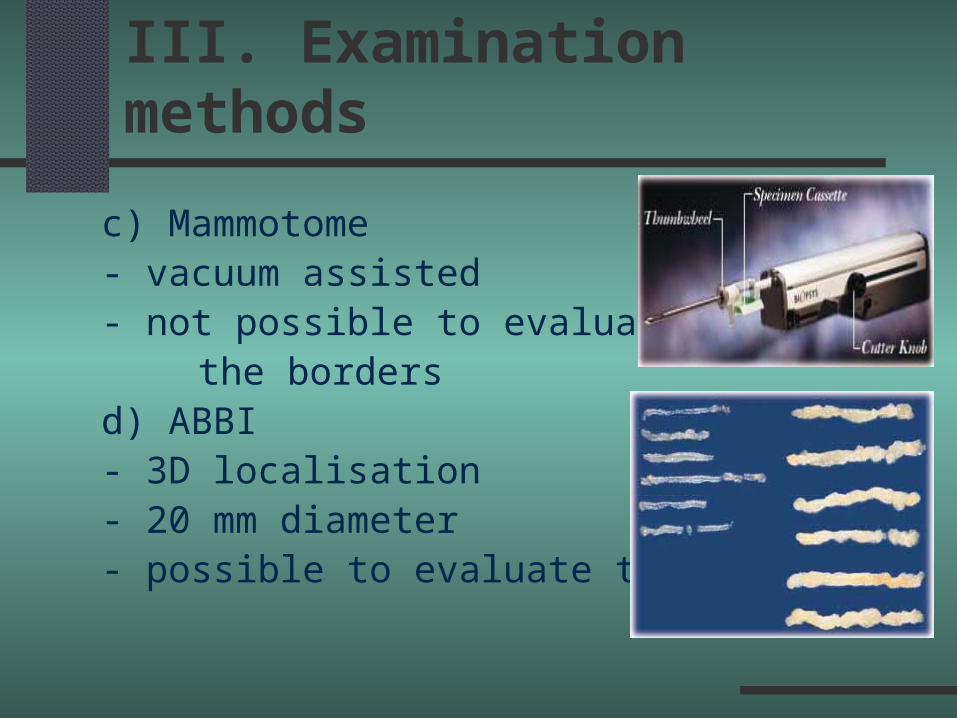
c) Mammotome- vacuum assisted- not possible to evaluate
the bordersd) ABBI - 3D localisation- 20 mm diameter- possible to evaluate the borders

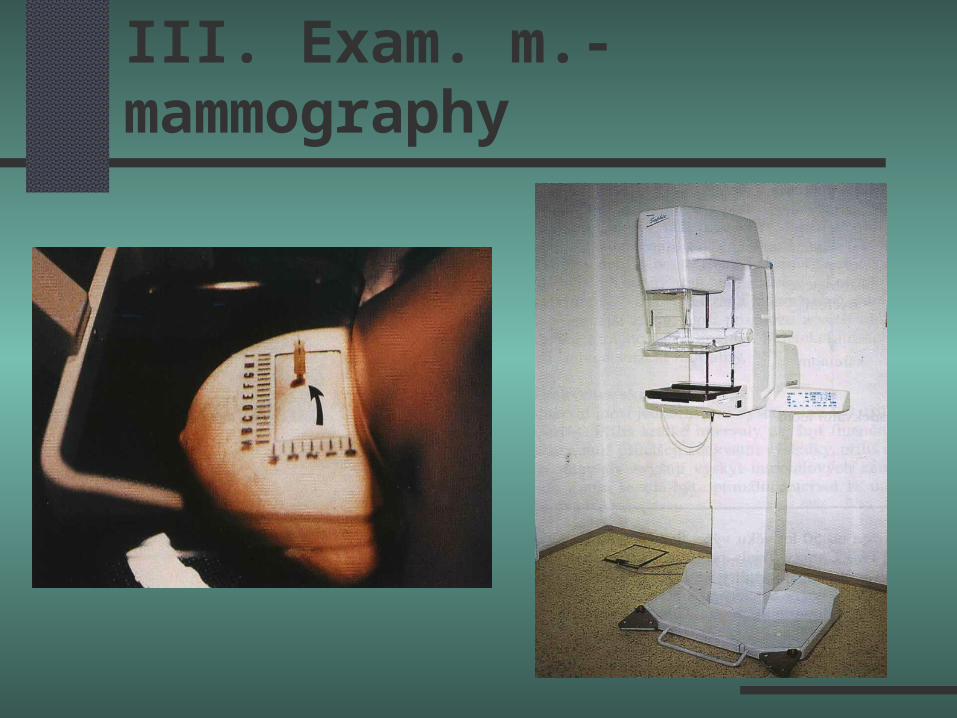
III. Exam. m.- mammography
over 35 y. detection ability: from 1-3 mm dose 0,1-0,2 rad
a) screening: 1. entry 35-40 y, 2. 40-50 y every 2 y.,3. over 50 y every 1 y (- 75 y.)
- mortality reduction 20-45%b) diagnostic
III. Exam. m.- mammography

III. Exam. m.- mammography

1a. Fibroadenoma
round, well circumscribed from lobulus proliferation of epithelial and stromal
components hormonally dependent a) pericanalicular b) intracanalicular

1b. Fibroadenoma
doesn´t increase the risk of breast cancer therapy:
- conservative: follow-up every 6 month
- radical: surgical extirpation italian study: extirpation leads to RR=2,0
(only follow-up) RR=0,97
2. Cysts
one of the most common changes from the lobular acini proliferation of the stromal component leads to an increased density of the gland therapy: conservative or punction of the
cyst

3a. Fibrocystic changes
present at 50-90% of women between 35-50 years of age, often asymptomatic
dysproportion of the involution - decrease of the amount of the stromal component (dominance of epithelial component)
histopathologic finding: fibrosis, cysts, adenosis, lymfoid infiltration, periductal inflammation
3b. Fibrocystic changes
intensity of „mastopatic“ changes which doesn´t correlate with the intensity of complaints
belongs to non-proliferative lesions of the breast zero proliferation indexes lead to worse mammographic lucidity therapy: conservative

4a. Papiloma
from the main ductus serose or bloody secretion from the nipple therapy: extirpation
4b. Juvenile papilomatosis
young women (under 20 years) solid, palpable formation (2-3cm) often upper outer quadrant multicystic
4c. Multifocal papilomatosis
from TDLU combination of epithelial and cystic
changes precancerosis therapy: extirpation, dispensarisation
5. Cystosarcoma phylloides
phyloides tumor proliferation of stromal component histologicaly commemorates intracanalicular
fibroadenoma often metaplasy: bone therapy: extirpation, often relaps

6. Rare tumours
lipoma adenolipoma myoepitelioma desmoidal tumour
7. Inflammation
juvenile hypertrophy - stromal hyperplasy duktektasis - dilatation of the large ductus
in perimenopausis or menopausis mechanical obstruction (deficiency of vit. A) cyklic mastodynie, palp. lesion, inflammation signs
therapy: symptomatic, ATB, excision
subareolar absces - chronic fistula therapy: incision, drainage, ATB
fat necrosis - trauma, radiotherapy, surgery

V. Carcinoma in situ
A) Ductal carcinoma in situ
– DCIS
B) Lobular carcinoma in situ
– LCIS
RR amplified 8-10x

A) Ductal carcinoma in situ
ductal epithelium has been replaced by carcinoma cells which doesn´t penetrate the basal membrane
often recidives in the place of biopsy microcalcifications often present therapy: extirpation + radioterapy or simple
mastectomy

B) Lobular carcinoma in situ
few clinical features no microcalcifications in 15-45% bilateral recidives bilateral LCIS – high risk

VI. Invasive breast carcinoma
1. Histologic type
2. Staging
3. Prognosis
4. Risk factors
5. Kancerogenesis
6. Characteristics of the tumour cell
7. Therapy

VI. Invasive breast carcinoma
1. Histologic type
2. Staging
3. Prognosis
4. Risk factors
5. Cancerogenesis
6. Characteristics of the tumour cell
7. Therapy

1a. Histologic type ductal carcinoma: 70-80% intraductal c.- type of DCIS lobular carcinoma - 10 % - difficult to detect by
mammography (no calcifications) medullar carcinoma - up to 5% - good
prognosis, doesn´t involve lymph nodes mucinous - coloid carcinoma - 3% - very slow
growth papilar carcinoma - 1% - bloody secretion

1b. Histologic type - special ca
inflammatory carcinoma – 1-4%, erythema, increased temperature, surgical treatment contraindicated,
primary treatment: radiotherapy Paget´s disease (carcinoma) – 4-5%, erosive
lesion of the nipple
VI. Invasive breast carcinoma
1. Histologic type
2. Staging
3. Prognosis
4. Risk factors
5. Cancerogenesis
6. Characteristics of the tumour cell
7. Therapy

2. Staging
T1 – tumour < 2 cm
T2 – tumour 2-5 cm
T3 – tumour over 5cm
T4 – penetration of the tumour into the chest
N1 – isolated metastasis, moveable l. nodes
N2 – isolated metastasis, fixated l. nodes
N3 – metastasis in internal mammary l. nodes
M1 – distant metastasis
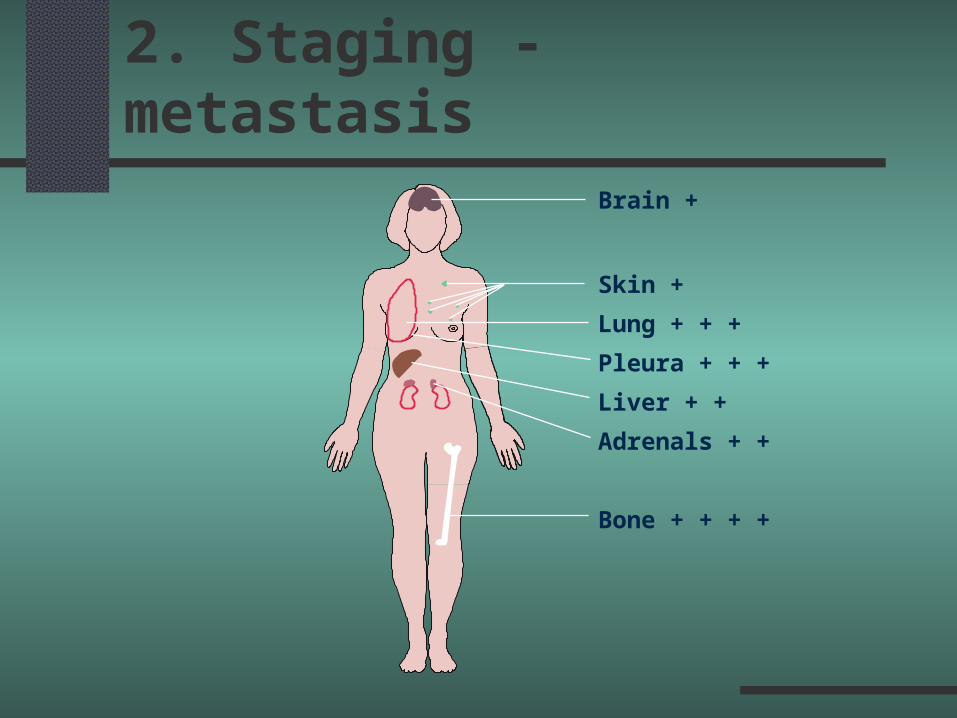
Brain +
Skin +
Lung + + +
Pleura + + +
Liver + +
Adrenals + +
Bone + + + +
2. Staging - metastasis
VI. Invasive breast carcinoma
1. Histologic type
2. Staging
3. Prognosis
4. Risk factors
5. Cancerogenesis
6. Characteristics of the tumour cell
7. Therapy

3. Prognosis
smaller than 1 cm: survival rate 90-95% tumor 2-3 cm: survival rate 65% involvement of 1-3 LN: survival rate 62% involvment of more than 4 LN: survival rate 32% positivity of estrogen/progesterone receptors EGF receptor – worse grade, lymfatic invasion
VI. Invasive breast carcinoma
1. Histologic type
2. Staging
3. Prognosis
4. Risk factors
5. Cancerogenesis
6. Characteristics of the tumour cell
7. Therapy
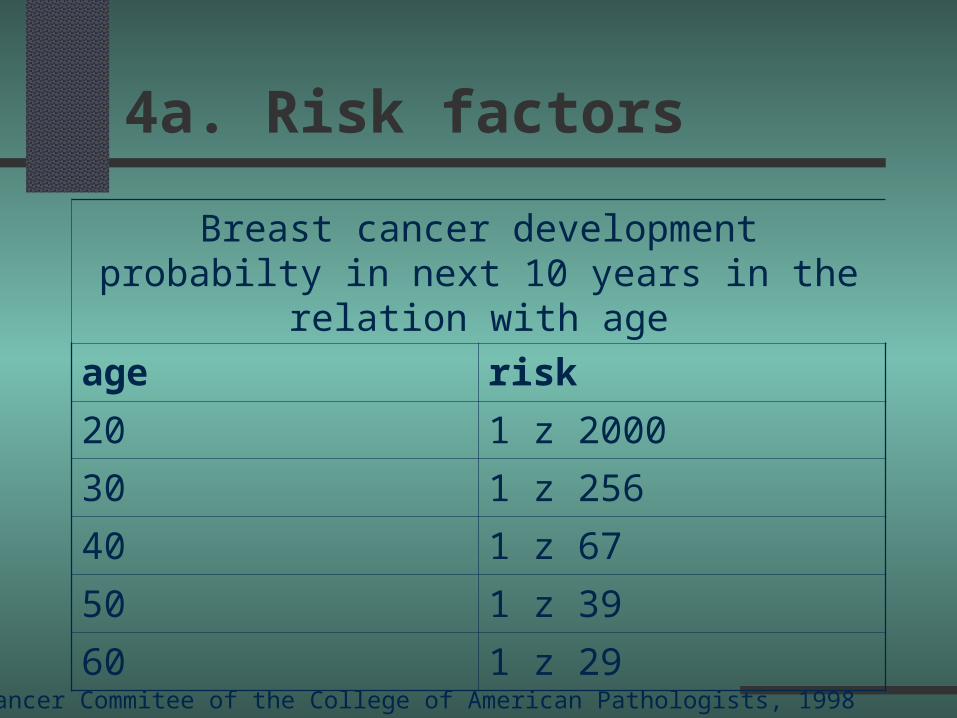
4a. Risk factors
Breast cancer development probabilty in next 10 years in the relation with age
age risk
20 1 z 2000
30 1 z 256
40 1 z 67
50 1 z 39
60 1 z 29
Cancer Commitee of the College of American Pathologists, 1998

4b. Risk factors
sex - frequency of ca female x male: 135 : 1 age - 65 years over 30 years: RR 17 absolute risk in 50 years: 7-10% menarche – early onset: RR 2 first delivery – delivery after 20. year: RR 2-3 menopausis – late menopausis: RR 2 breast feeding over 1 year reduces the risk by
20%

4c. Risk factors
FH - 1.line: RR 2 - 3
- 2.line: RR do 1,5 genetic carcinoma breast/ovary (BRCA 1,2)
- tumour supresor gen, AD heriditary
- absolute risk: 85% life style, body weight – alcohol, obesity
(BMI > 35), hyperinsulinemie
4d. Risk factors
environment – chemical cancerogens, genotoxic substances
society status: high socioeconomic standart, stress
radiation drugs- prolactine agonists HRT - slight elevation by the use over 10 years
(kontroversy)
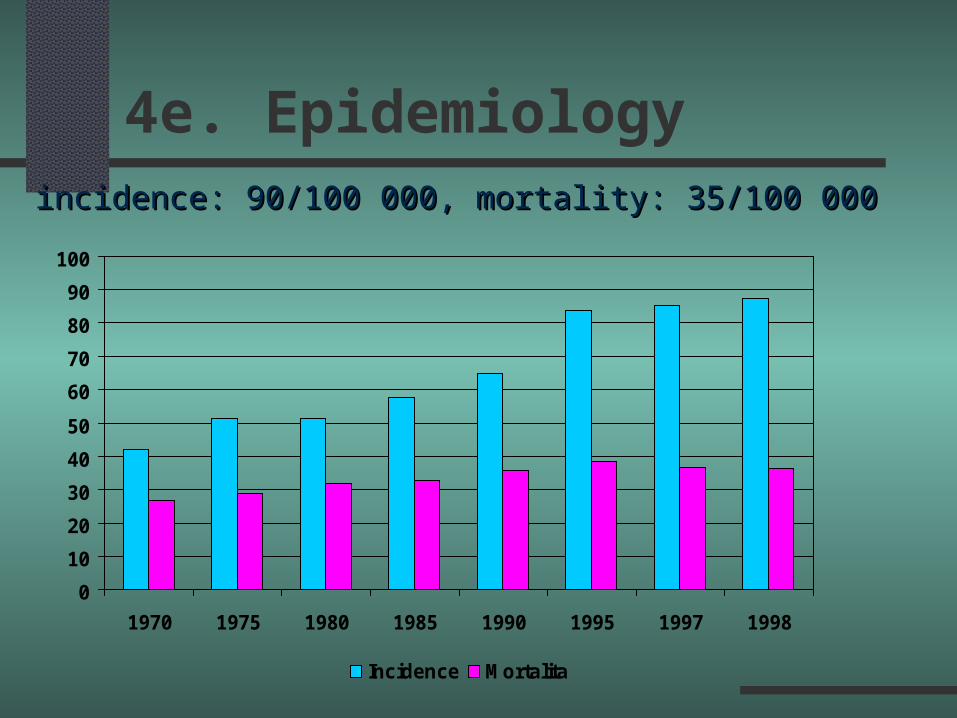
4e. Epidemiology
0
10
20
30
40
50
60
70
80
90
100
1970 1975 1980 1985 1990 1995 1997 1998
Incidence Mortalita
incidence: 90/100 000, mortality: 35/100 000incidence: 90/100 000, mortality: 35/100 000
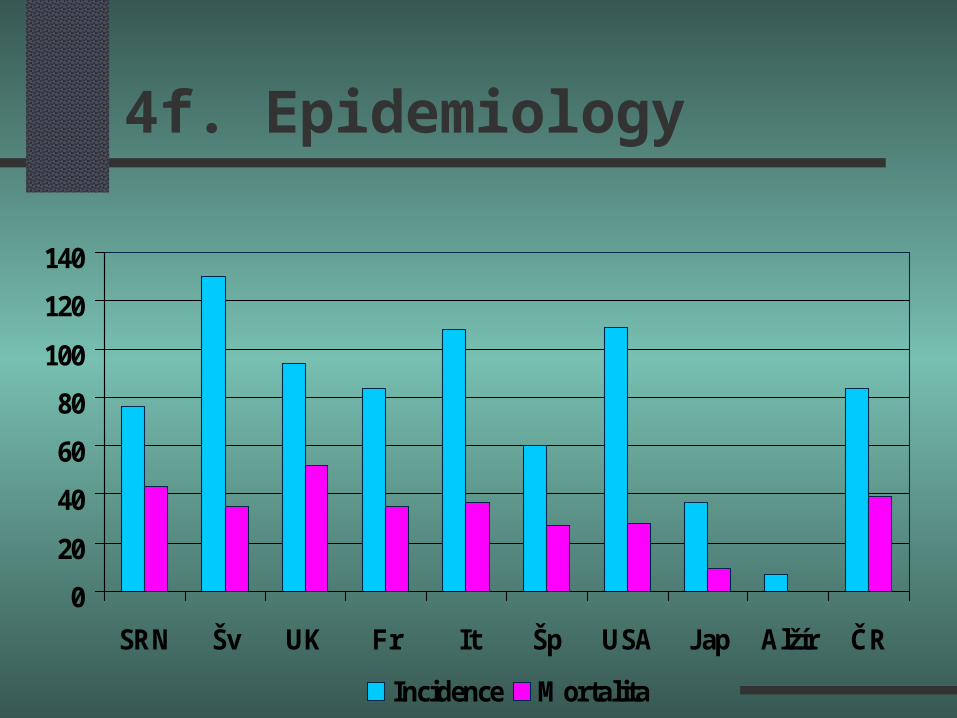
4f. Epidemiology
0
20
40
60
80
100
120
140
SRN Šv UK Fr It Šp USA Jap Alžír ČR
Incidence Mortalita
VI. Invasive breast carcinoma
1. Histologic type
2. Staging
3. Prognosis
4. Risk factors
5. Cancerogenesis
6. Characteristics of the tumour cell
7. Therapy
5. Cancerogenesis
oncogene activation genetics: genes BRCA 1,2, p53
1. Iniciation: during menarche - first delivery cancerogenes, radiation, nutrition, endogenous hormones2. Promotion: premenopausis (hormones)
postmenopausis - failure of apoptosis, failure of control of the cell cycle

5. Cancerogenesis
10 20 30 40 50
carcinomaBRCA BRCA
1. delivery 1. delivery lifestyle lifestyle
INDUCTIONINDUCTIONCancerogensCancerogensRadiationRadiationHormonesHormones
MenarcheMenarche
PROMOTIONPROMOTIONHormonesHormonesGrowth factorsGrowth factors
defekty apoptozy,defekty apoptozy, antioxydační ochrany,antioxydační ochrany, opravy DNAopravy DNA
accumultaion of defect DNAaccumultaion of defect DNA

VI. Invasive breast carcinoma
1. Histologic type
2. Staging
3. Prognosis
4. Risk factors
5. Cancerogenesis
6. Characteristics of the tumour cell
7. Therapy

6. Characteristics of tumour cell
no control of proliferation loss of intercell adhesion loss of epithelium-stromal interaction (loss of
contact inhibition of growth) loss of diferenciation elevated metabolic activity changes of HR, abnormal reaction to hormones

VI. Invasive breast carcinoma
1. Histologic type
2. Staging
3. Prognosis
4. Risk factors
5. Cancerogenesis
6. Characteristics of the tumour cell
7. Therapy

7a. Therapy
survival rate is given by the stage radiotherapy reduces the incidency of loco-regional metastasis
lymphadenectomy decreases the frequency of
local recidives in cases of negative lymph node negativity
lymphadenectomy is only staging

7b. Therapy - surgery
radical mastectomy
(Halstead) quadrantectomy segmentectomy tumorectomy/WLE modified radical mastectomy subcutaneous mastectomy plastic operations

7c. Therapy - surgery
primary surgery: tumors of stage I, II
(size < 5 cm) standard therapy: modified radical mastectomy
(mastectomy, ALND I, II) lymphatic mapping: sentinel lymph node axillary lymphadenectomy is being still
indicated by invasive breast cancer
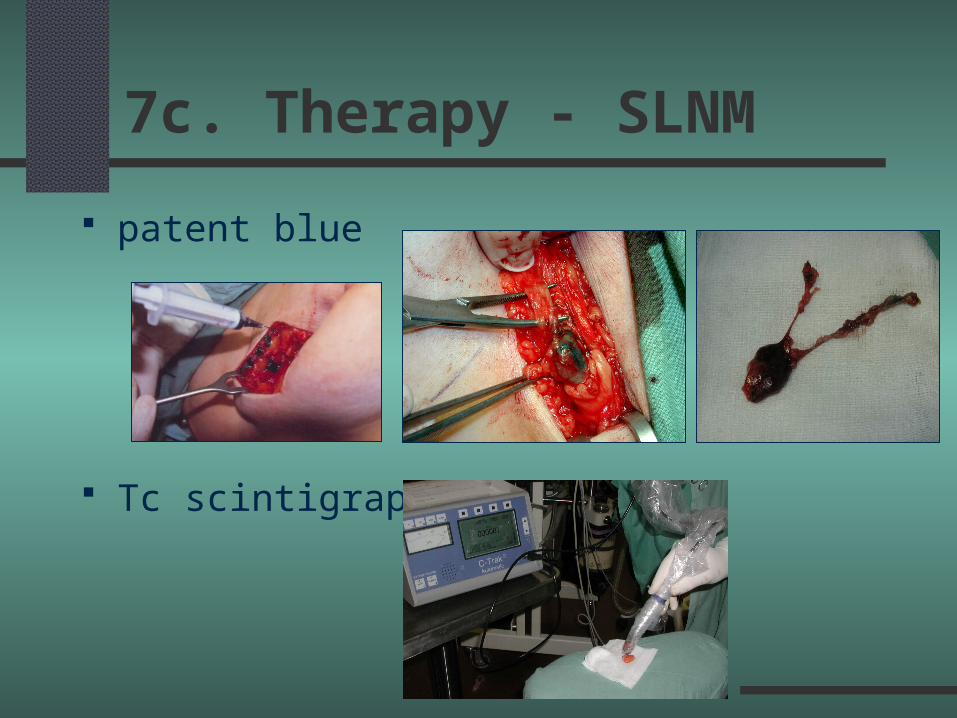
7c. Therapy - SLNM
patent blue
Tc scintigraphy

7d. Therapy - surgery
Breast conserving surgery: 1977 -
B. Fisher, J.L. Hayward, U.Veronesi condition:
- tumour size 3 – 4 cm
- tumour is not located in the breast center
- tumour is not multifocal
- radiotherapy must follow

7e. Therapy - plastic operations

7f. Therapy - plastic operations
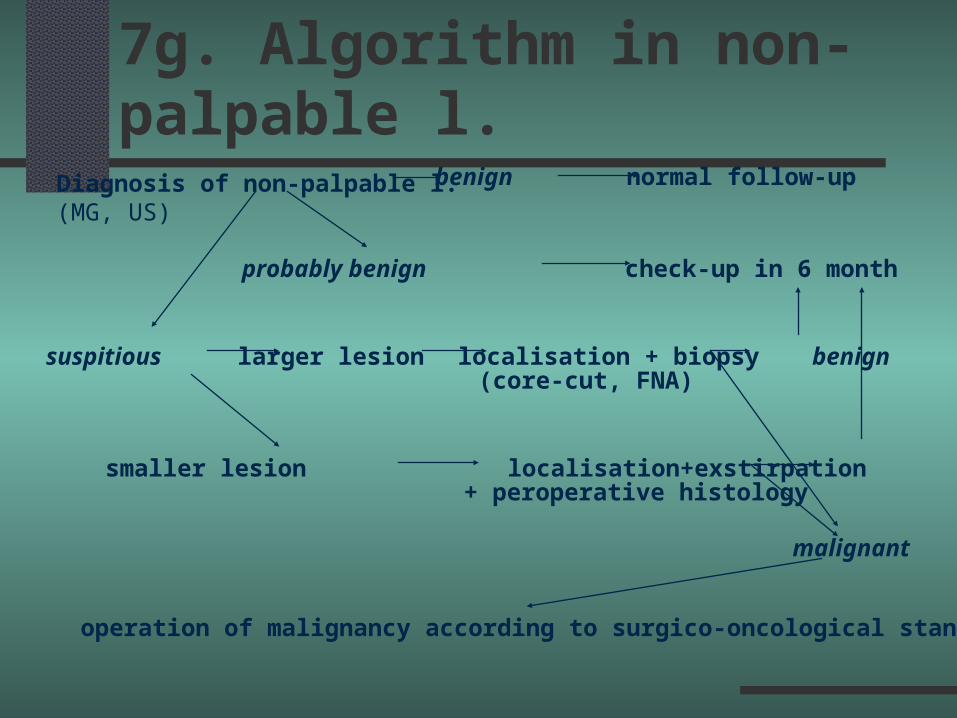
7g. Algorithm in non-palpable l.Diagnosis of non-palpable l. (MG, US)
benign normal follow-up
probably benign check-up in 6 month
suspitious larger lesion localisation + biopsy benign
smaller lesion localisation+exstirpation benign
(core-cut, FNA)
+ peroperative histology
malignant
operation of malignancy according to surgico-oncological standards

7h. Radiotherapy
I: T2, over 4 positive LN intensity of radiation: 4-6 MV - linear acc. after conservative surgery - dose of 50 Gy
(5 weeks + boost 10-15 Gy – Ir192) radiotherapy of the scar, axilla paliative radiotherapy of metastasis

7h. Radiotherapy

7i. System therapy - chemot.
only systemic therapy can improve prognosis combined chemotherapy
- neoadjuvant – before surgery
- adjuvant – after the surgery CMF, FAC, AT, ET cyklofosfamid, 5-fluoruracil, metotrexate,
doxorubicin, epidoxorubicin

7j.System therapy - hormonal t.
estrogen receptor blockage
- antiestrogens - tamoxifen, raloxifen synthesis blockage
- aromatase inhibitor - arimidex high dose progesterones - down regulation
of estrogen and progesterone receptors ovarian ablation
surgical/radiotherapeutical
7k. Prevention
proper nutrition and life style: age of the first delivery – breast feeding
reduction of environmental risk factors (ionisation radiation, cancerogenes, alcohol)
early diagnosis and adequate therapy (system) chemoprevention - antiestrogens: Tamoxifen
(USA,UK, Itálie)

7k. Phytoestrogens
isoflavonids (Genistein): soja, tofu, kari, beer, bourbon
flavonoids (Galanin): tea leafs lignands (Indol-3-Carbinol): spinach, broccoli monoterpens (limonen): lemon karotenoids: (lutein, lycopen): tomatoes
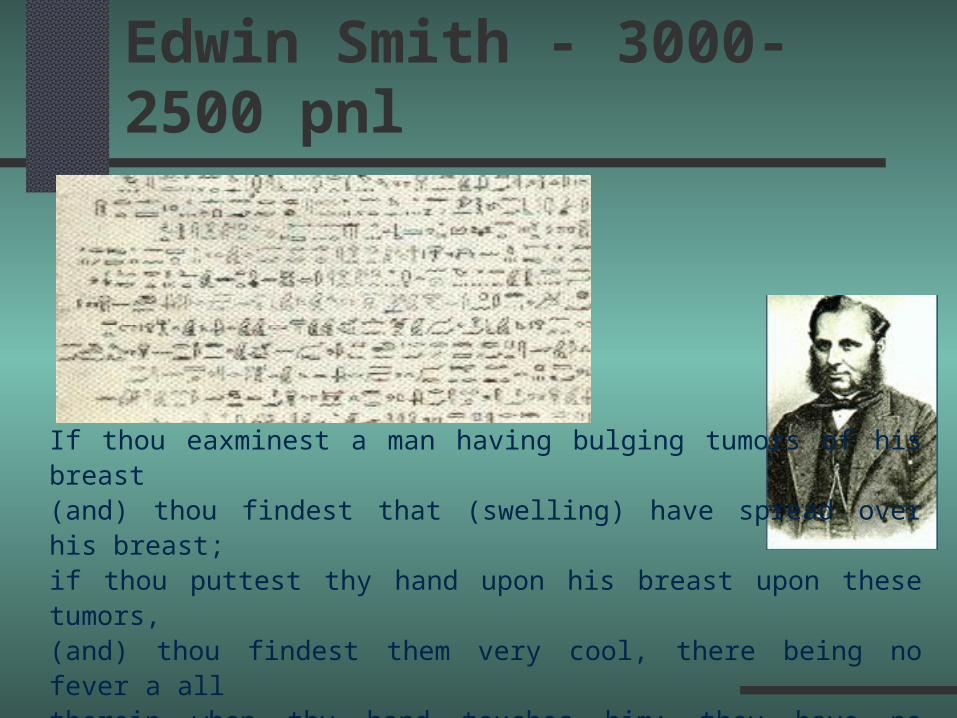
Edwin Smith - 3000-2500 pnl
If thou eaxminest a man having bulging tumors of his breast(and) thou findest that (swelling) have spread over his breast;if thou puttest thy hand upon his breast upon these tumors,(and) thou findest them very cool, there being no fever a alltherein when thy hand touches him: they have no granulation,they form no fluid, they do not generate secretion of fluid,and they are bulging to thy hand.There is no ( treatment).

Thank You for Your attention





























