Embed Size (px)
Citation preview


Malaria
• Malaria has long been recognized as an important parasitic disease of humans, having been described by the early Egyptians in the third millennium B.C.,
• Despite the introduction of control programs in many parts of the world over the past few decades, the impact of malaria on human populations continues to increase. Recent estimates suggest,
(1) that 1.5 billion persons live in areas of the world where malaria is an endemic disease,
(2) that the number of infected humans exceeds 500,000,000, and,
(3) that 1-3 million persons die each year, including about 1 million children under 5 years old (3,000 per day).
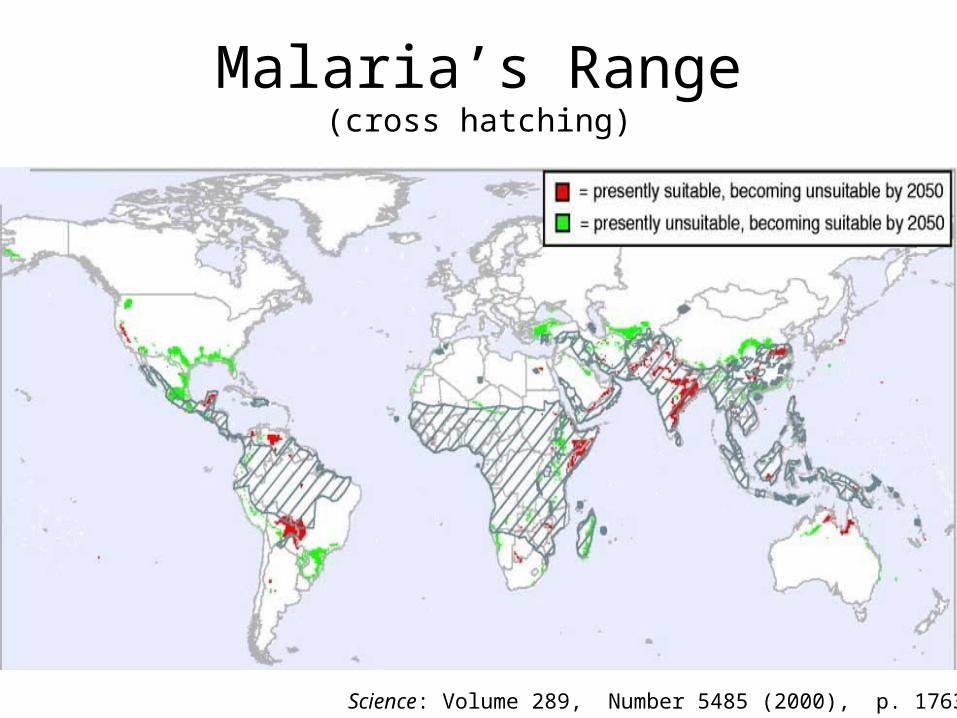
Malaria’s Range(cross hatching)
Science: Volume 289, Number 5485 (2000), p. 1763

LINKS BETWEEN MALARIA AND POVERTY
• Poverty affects malaria. Communities with low incomes, limited education and poor access to health care are least able to engage in malaria control activities.
• Malaria affects poverty. In poor households, a greater proportion of income is likely to be spent on malaria treatment than in affluent households,
– malaria illness causes absenteeism from work and school, poor scholastic performance, lack of labor for cultivation, and a decline in child care, etc.
• Hence, a negative spiral can develop with malaria causing and deepening poverty which, in turn, exacerbates inequalities in societies.

General Malaria Pathology…more later.
• Host (human) inflammatory response resulting in severe chills and fever,
– paroxysms,
• Anemia due to loss of red blood cells,
• Recurrence of paroxysms at periodic intervals.

• These single celled eukaryotes have heteroxenous life cycles with both vertebrate and invertebrate hosts,
– Humans,– Mosquitos.
• Macro- and micro- gametes develop independently and the resultant zygote is motile and is called the Ookinete.
Causative Agent: Plasmodium sp.
(Protozoa: Haemosporina)

Malarial Plasmodium
There are four important species that infect humans, causing malaria;
* P. vivax - benign tertian malaria - accounts for ~43% of cases
* P. falciparum - malignant tertian malaria accounts for ~50% cases
* P. malariae - quartan malaria - accounts for ~7% of cases
* P. ovale - mild tertian malaria - accounts for < 1% of cases.

P. vivax - benign tertian malaria
• The disease gets its name from the time between paroxysms, which occur every 48 hours,
– from the Roman custom to call the first day of the event day 1 and therefore 48 hours later would be day 3,
• Tertian malaria accounts for 43% of all cases of malaria.
• This species is mainly found in Asia and recrudescence has been known to occur up to 8 years after. The first infection due to the presence of a dormant exoerythrocytic stage, also known as hypnozoites.
• P. vivax are only capable of infecting red blood cells via genetically determined receptor sites. Only people exhibiting these antigenic sites are susceptible to the disease.
P. ovale - mild tertian malaria: similar

Duffy Blood Group
• Human populations express two dominant alleles, signified as Fya and Fyb,
– the expressed glycoproteins are recognized by their respective antigens on the erythocyte cell membranes,
• A third allele Fy has no antigen associated with it.
• The Fy/Fy genotype appears in about 40% of the African population as opposed to less than 0.1% in European populations.
• Individuals with Fya/_ and Fyb/_ genotypes therefore express the antigen on the surface of the red cell to which the plasmodium can bind, allowing infection.

Tertian Malaria• The paroxysms commence with the patient having a feeling of intense
cold (15 min - 1 hour),
– this is due to a rapid rise in body temperature to 104-106o F, – accompanied with violent shivering, – often with nausea and vomiting.
• Followed by the hot phase, which includes headache and often delirium (2 - 6 hours).
• The fever breaks with the copious production of perspiration. The body temperature drops back to normal after 2 - 4 hours. The patient may sleep for 8-12 hours and feel well until the next paroxysm.

P. falciparum - malignant tertian malaria
• The time between the onset of paroxysms is 48 hours, but the period of fever is prolonged, lasting from 24-36 hours,
• The course of this disease is very rapid and it is not uncommon to see more than 60% of a patient's red blood cells infected.
• When the number of infected cells rises above 25% the disease is usually fatal, in spite of treatment.
“knobs”
Knobs promote cell clumping… clogging veins and arteries.

Falciparum Malaria
• In Falciparum malaria the paroxysms last longer 20-36 hours and so the patient does not recover before the onset of the next bout.
• In 10% of P. falciparum cases patients develop cerebral malaria, 80% of which result in death.
– characterized by headaches followed by the patient falling into a coma, often with convulsions.
• This is particularly common in children.
• Ultimately death ensues with the patients temperature reaching up to 108 F.

P. malariae - quartan malaria
• This species of malaria has a 72 hour cycle of paroxysms and is found in both the New and Old World.
• Recrudescence has been reported up to 53 years after the first infection.
• It is the principal cause of malaria episodes as a result of blood transfusion.

Anopheline Mosquitoes
• Anopheline mosquitoes are the only vector (except blood transfusions, and unprotected sex)
• Out of the 380 species of Anopheline mosquitoes, 60 can transmit malaria.
• Only female mosquitoes are involved as the males do not feed on blood.

Malaria Cycle Three Main (Human) Stages
• Stage I : Upon infection by the mosquito, the malaria parasites move rapidly into the liver (within ~30 minutes ),
– and reproduce rapidly (mitosis) for 5 days or more, depending on the species ( P. falciparum or P. vivax) ,
• Stage II : The malaria parasite exits the liver, enters the bloodstream, and within minutes invade red blood cells, where they grow and divide,
– every 48-72 hours (time differences depend on the species) the red blood cells rupture, – dispersing more parasites along with waste products/toxins into the blood stream,– this step causes fever, chills and anemia in the victim,– the released parasites then invade other red blood cells, beginning the cycle again.
• Stage III: Some parasites invade red blood cells and develop into sexual forms,
– may be ingested by uninfected biting mosquitoes, – inside the mosquito they mate and begin to reproduce,– the zygotes (ookinetes) make their way to the salivary glands of the mosquito, ready to move on to
another victim when the mosquito takes its next blood meal.

Plasmodia/Mesquito/Human Life Cycle
1. Sporozoite / liver,
2-5. Mitosis, liver cell lysis,
6. Trophozoite / red blood cell,
• 7-11: (mitosis),
12. Gametocytes (via meiosis),
13,14. Gametes via mitosis (midgut),
15,16. Ookinetes, zygotes via conjugation,
• cross the midgut epithilium,
17. Oocysts, mitosis,
18-20. Cross salivary epithelium.


Fighting Malaria• Insecticides (mosquitoes develop resistance quickly),
– most effective (DDT) banned,
• Bed nets (often coated with insecticides),
• Post infection drugs, even the best (chloroquine and sulfadoxine-pyrimethamine) generally lose effectiveness over time.
“New” Chinese remedy: Qinghaosu plant, used in fever remedies for 2,000 years,
• Artemisia annua, known as sweet wormwood or Chinese wormwood, grows wild, even in the United States.
• Incredibly effective, although long term effectiveness and side effects are not known.


Plasmodium: Mosquito Life
Cycle
Sporozoites cross the salivary gland epithelium,
This is thought to be receptor mediated.
Ookinetes cross the midgut epithelium,
This is thought to be receptor mediated.

Receptor Mediated Transfer
Ross CellMosquito epithelium
Ookinete
Ross CellMosquito epithelium
Ookinete
normal/infection no infection
Ookinete binds open receptor.
enters cell
Molecules bind receptor sites, block Ookinete
transfer.

The Experiment
• Try to find a transgene that produces a peptide that will effectively block the receptor mediated transfer of ookinetes,
– a “transgene” is an introduced gene.

Preliminary Work

Phage Display
T7 phage
…insert a DNA sequence into phage gIII gene sequence.
…recombinant phage express the sequence as part of the gIII protein.

Recombinatorial LibraryInsert DNA coding for dodecapeptides (XCX8CX) into T7 genome.
Allow recombinant DNAs to replicate and repackage themselves.
Run T7 phage over the receptor.

Procedure• 109 different phages
in the population,
– XCX8CX yields ~2010
different possible peptides…,
• Mosquitoes were injected with ~ 1011 phages.

SM1
• PCQRAIFQSICN: protein sequence bound both salivary gland and midgut epithelia,
• Injection of the peptide into the mosquitos body cavity inhibited oocyst formation by roughly 90%.
PCQRAIFQSICNXCXXXXXXXXCX XCX8CX

SM1 Injected into Mosquitoes
A mouse model system has been established in order to provide a clinical vertebrate host.

Delivery
• We can’t hope to hand-inject every mosquito in the world,
– or, even feed them all SM1 peptide,
• How can we deliver the 12 amino acid peptide into the correct cells in mosquitoes?

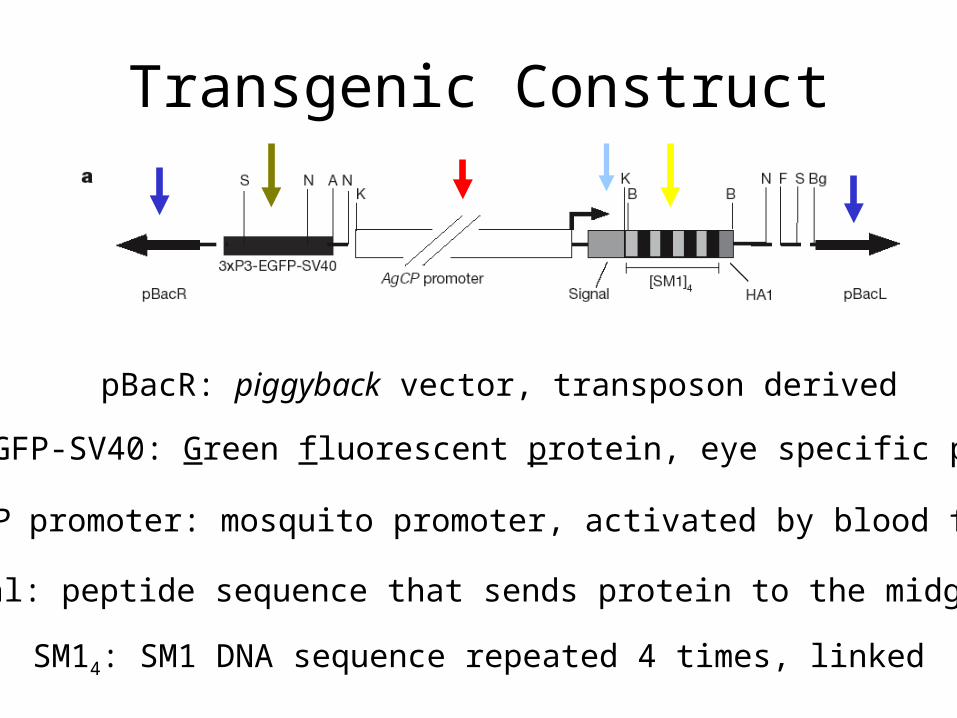
Transgenic Construct
pBacR: piggyback vector, transposon derived
3xP3-EGFP-SV40: Green fluorescent protein, eye specific promoter
AgCP promoter: mosquito promoter, activated by blood feast.
SM14: SM1 DNA sequence repeated 4 times, linked
Signal: peptide sequence that sends protein to the midgut.

Transformation
• Embryos are injected with the transgene/vector construct, and a “helper” plasmid,
• Surviving embryos are raised and crossed with virgin wt mosquitos,
– Subsequent offspring are scored for GFP eyes.

wt (top)
wt (front)
trans (top)
trans (front)
trans (bottom)
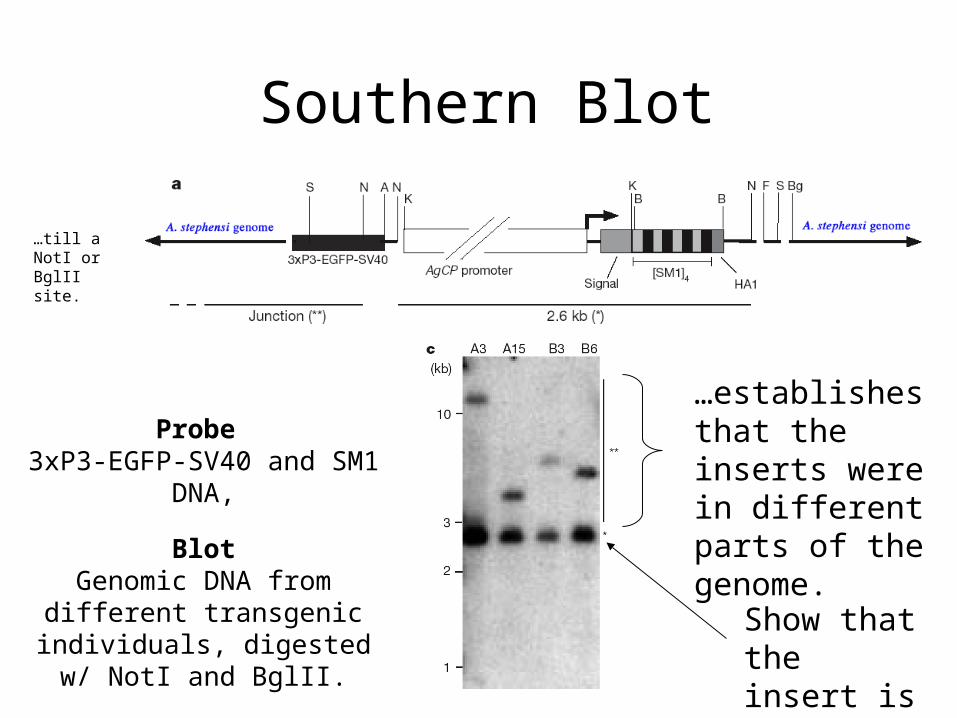
Southern Blot
…establishes that the inserts were in different parts of the genome.
…till a NotI or BglII site.
Probe 3xP3-EGFP-SV40 and SM1
DNA,
BlotGenomic DNA from different
transgenic individuals, digested w/ NotI and BglII.
Show that the insert is present.

Northern Blot
mt rRNA Control: constant expression gene, shows total RNA level was similar in all lanes.
Why no male expression?
SM1 expression…after a blood meal.
Probes: SM1 DNA (mt rRNA for control)

Transgenic SM1 Results

Other Controls
• wt Phage infection; no anti-ookinete function,
• GFP transgene only; no anti-ookinete function,
• Transposons; ditto,
• Other peptides; ditto.
Further: SM1 was inserted into 4 different genomic regions, all had the same phenotype,
This suggests that the anti-ookinete function wasn’t due to a disrupted gene.


Epitope Tagging
• Fluorescent antibodies are available for a portion of a virus protein influenza hemagglutin (HA1)...
When in a transgene, and subsequently translated, the location of transgene expression in the organism can be assayed.

Trangenic
Wt
Midguts
in situ, “Western”
Western:protein target,antibody probe.

Does SM1 Stop New Infections?
• Transgenic and wt mosquitoes are fed blood meals on malaria infected mice,
• Then are placed with uninfected mice,
– These mice are then assayed for malaria.

And it’s Only a Heterozygote
• The authors conjecture that the possibility exists that homozygous SM1 expressing mosquitoes might display stronger anti-ookinete function.

But(t)
• SM1 transgenic mosquitoes don’t seem to stop/kill all plasmodium, thus, the plasmodium may be able to mutate and maybe find a way around the SM1-blocked receptor,
• SM1 transgenic mosquitoes:
– healthy?
– how do you replace natural populations?
– are there unknown environmental consequences of the transgene?• how do you test for this?
– are all of the anopholines similar?• maybe the receptor differs between species?

Genetics…in the news.
paper (pdf)

To Know
• Understand the basic life cycle of Plasmodium,
• Understand the Figures and Tables in this experiment,
• Understand the general rational of the experiment.

Wednesday
• Assigned Questions: 6.8, 6.13, 6.18, 6.19, 10.6, 10.7, 10.9, 10.11,
• Chapter 7: (7.1 - 7.5) for quiz,
• Start Bacterial Genetics.
![Characterising malaria connectivity using malaria ......Arucial and legitimate concern of malaria control pro-grammes is the threat of malaria importation˜[1].It has long been acknowledged](https://img.dokumen.tips/doc/110x75/5f64a26f577ec557b52b4778/characterising-malaria-connectivity-using-malaria-arucial-and-legitimate.jpg)




























