Embed Size (px)
Citation preview

MALARIA Four Plasmodium species are
responsible for human malaria:
P. falciparum malignant tertian malaria
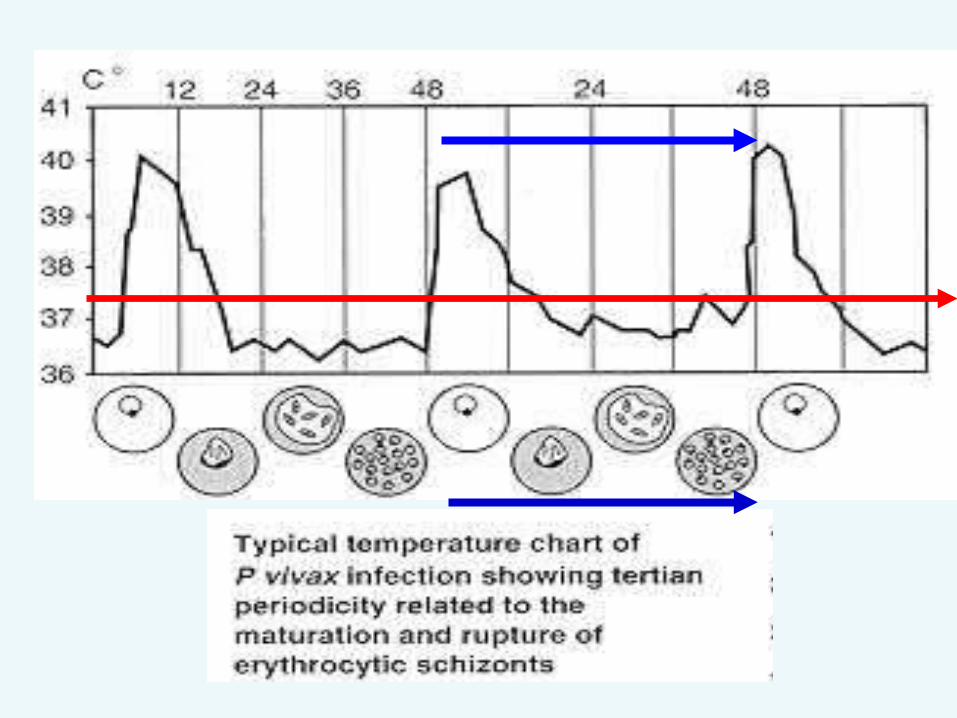
P. vivax, benign tertian malaria
P. ovale ovale tertian malaria P. malariae. quartan malaria
There are an estimated 200 million cases of malaria leading to mortality of more than one million people per year.
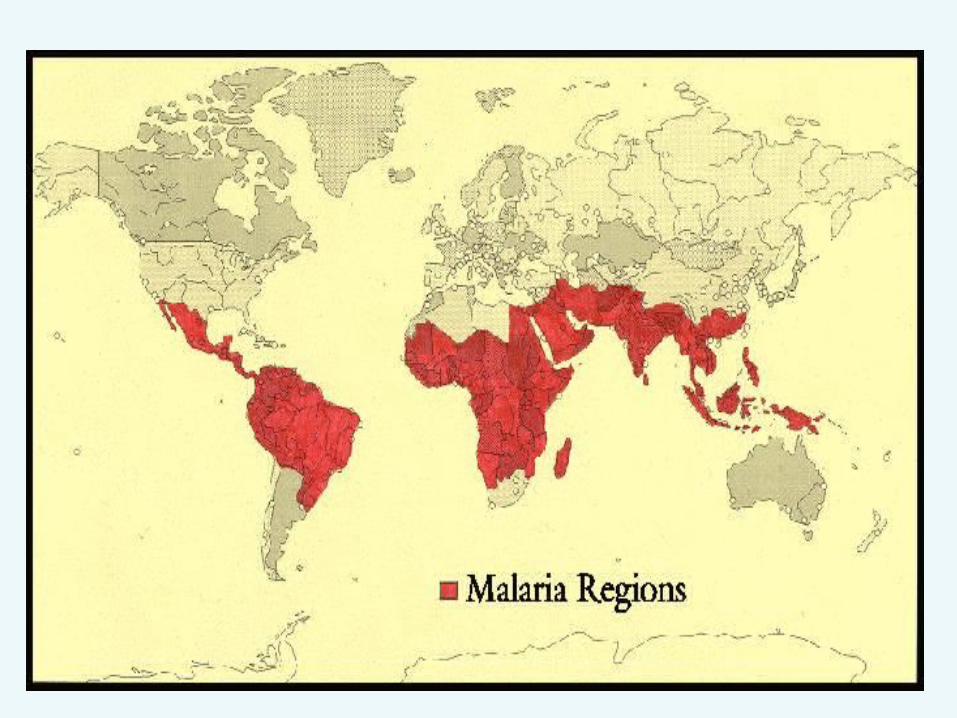
• P.falciparum and P.malariae are the most common species and are found in Asia and Africa.
•P. vivax predominates in Latin America, India and Pakistan.
•P. ovale is almost found in Africa.
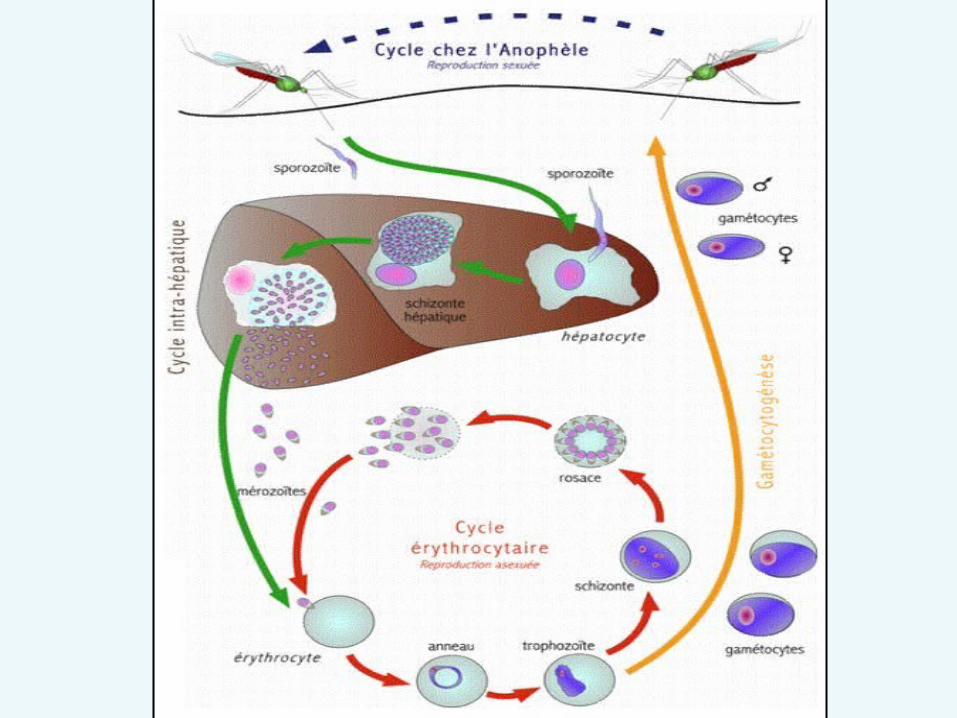
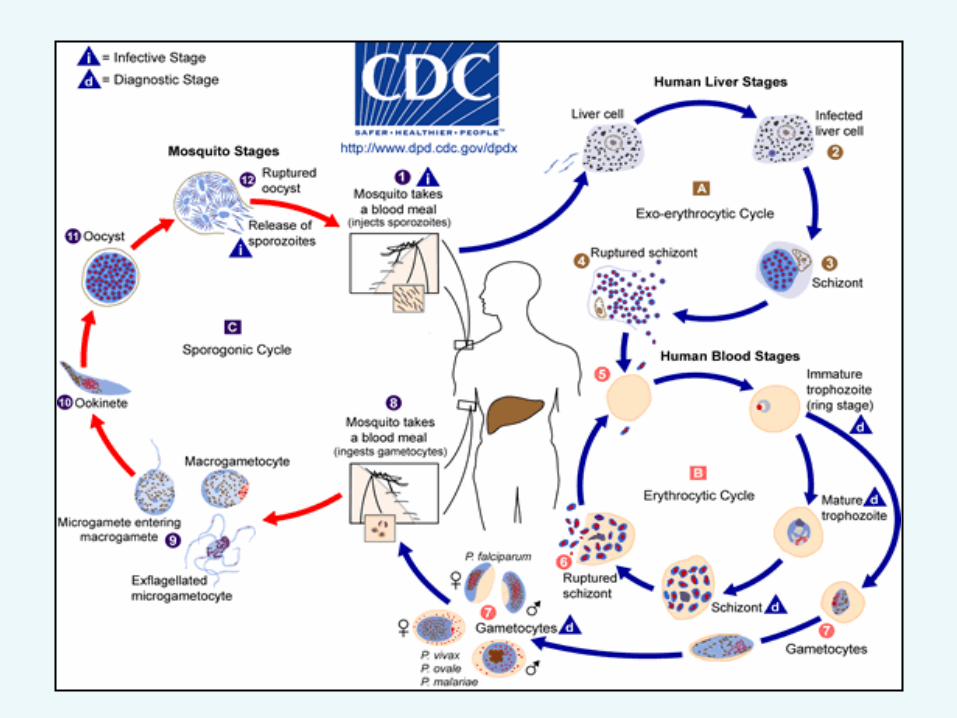
•Malarial parasites are transmitted by female anopheline mosquito which injects sporozoites present in the saliva of the insect.
• Sporozoites infect the liver parenchymal cells where they may remain dormant (hypnozoites) or undergo stages of schizogony to produce schizonts (merogony) to produce merozoites (meronts).
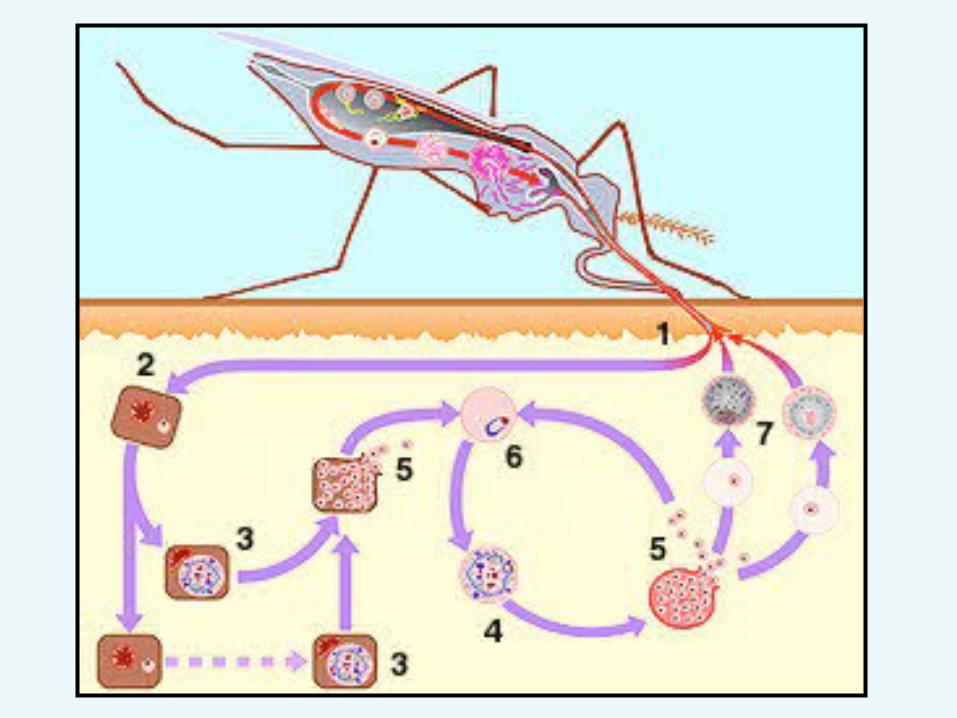
• When parenchymal cells rupture, thousands of meronts are released into blood and infect the red cells
• The liver cycle (extra-erythrocytic or pre- erythrocytic ) takes 5-15 days whereas the erythrocytic cycle takes 48 hours or 72 hours (P. malariae).
• Malaria can be transmitted by transfusion and transplacental.
• In red cells, the parasites mature into trophozoites. These trophozoites undergo schizogony (merogony) in red cells which burst and release merozoites.
• Some of the merozoites transform into male and female gametocytes while others enter red cells to continue the erythrocytic cycle.
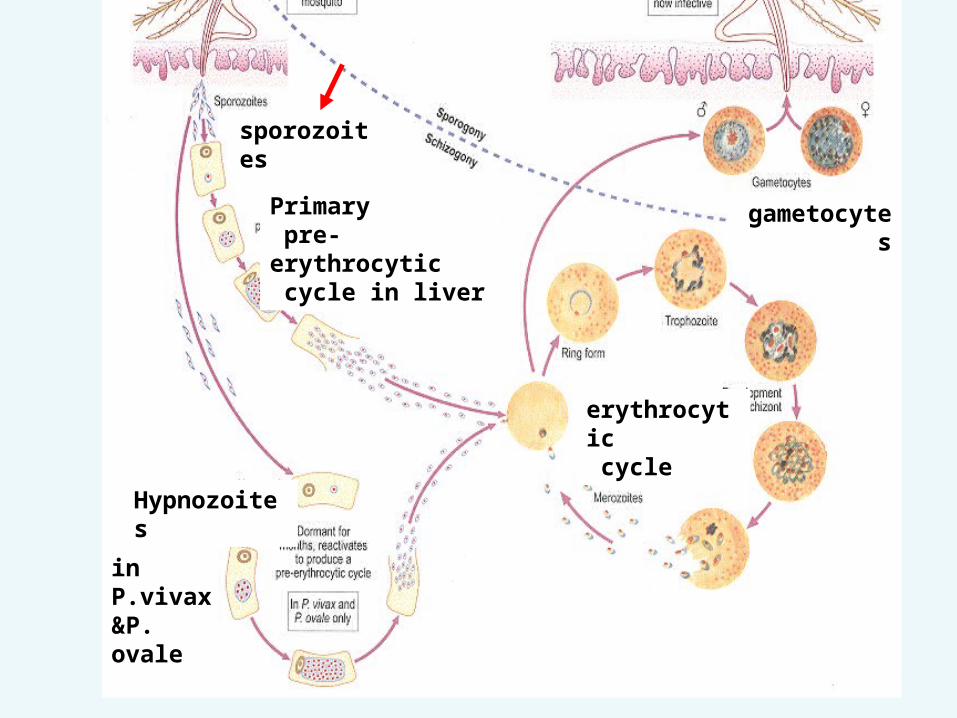
Primary pre-erythrocytic cycle in liver
sporozoites
gametocytes
Hypnozoites
in P.vivax&P. ovale
erythrocytic cycle
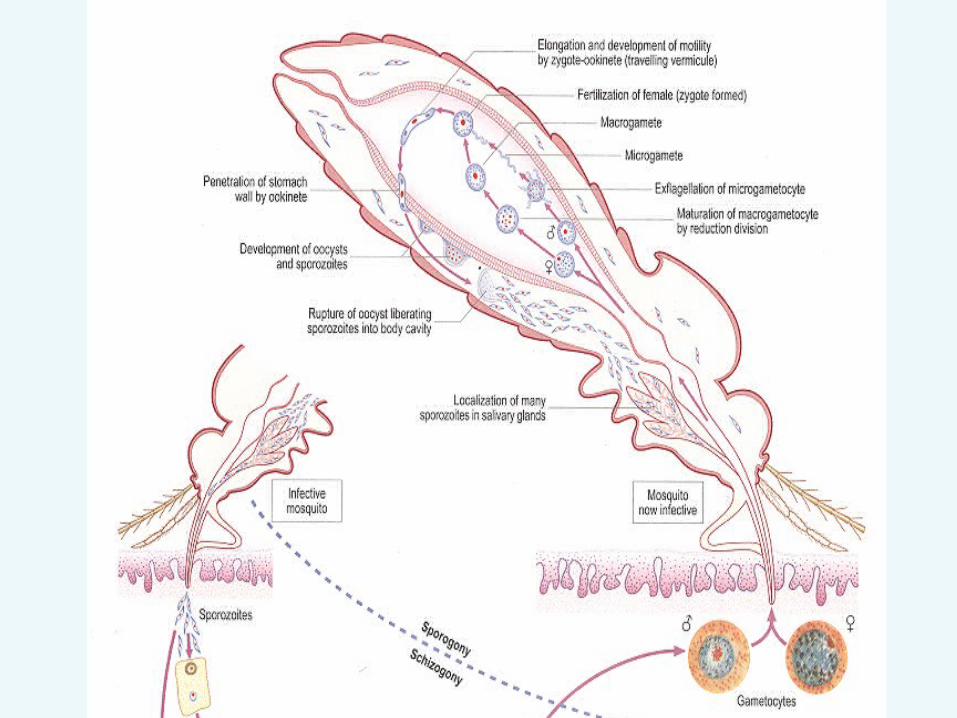
•The gametocytes taken by the female mosquito, the microgametes penetrate the macrogametes generating zygotes .
• The zygotes become motile ookinetes which invade the midgut wall of the mosquito where they develop into oocysts .
• The oocysts rupture, and release sporozoites , which go to the mosquito's salivary glands (sporogony)
• Inoculation of the sporozoites into a new human host inchoate the malaria life cycle. (Infective stage)
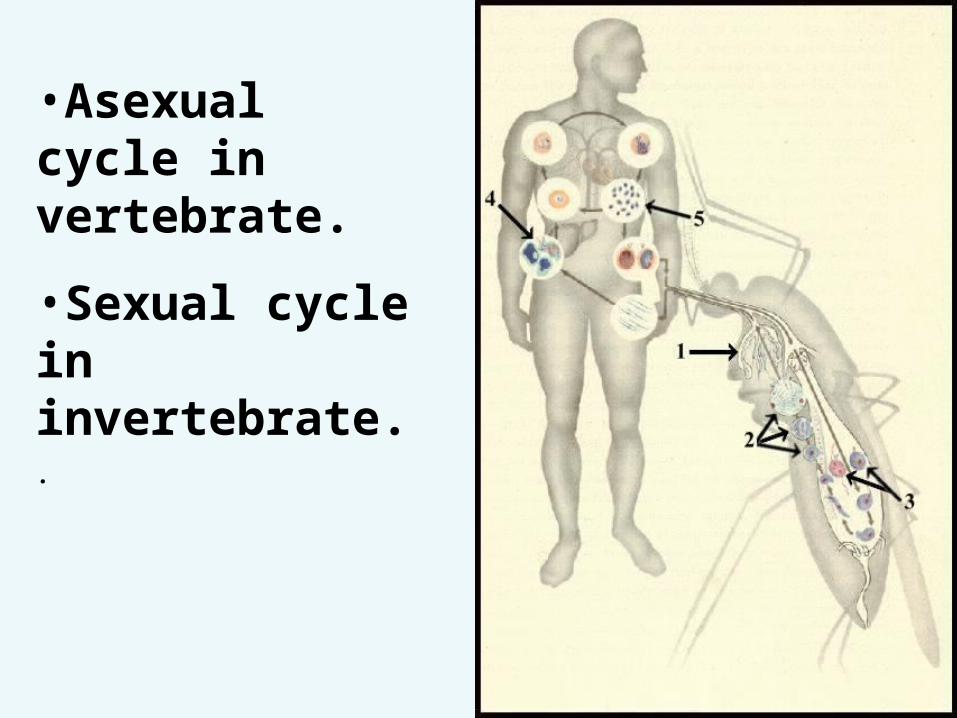
•Asexual cycle in vertebrate.
•Sexual cycle in invertebrate..
The malaria parasite life cycle involves two hosts
- Intermediate host
Vertebrate host Asexual cycle a-Exo-erythrocytic or pre-
erythrocytic schizogony (merogony)
b -Erythrocytic schizogony c -Gametogony- Definitive host Invertebrate host Sexual cycle sporogony
Clinical features (fever)•Cold stage: rigor (cold and shivers)
headache (half-1 hour)
•Fever (hot) stage:
temperature rises to maximum ,sever headache pain in back and joints vomiting and diarrhea (1-4 h)
•Sweating stage patient perspires temperature fall and patient relieved until the next rigor (1-4h).
• Cold- hot- sweating - normal
• Incubation period
•Primary attack
Malarial paroxysm cold -hot –sweating normal
•Repeated attack Relapse recrudescence
•Recrudescence of falciparum it is caused by parasites persisting in circulation at sub clinical level following previous attack.
•Malarial relapse due to delayed development of hypnozoites in liver
• There is no hypnozoites in falciparum
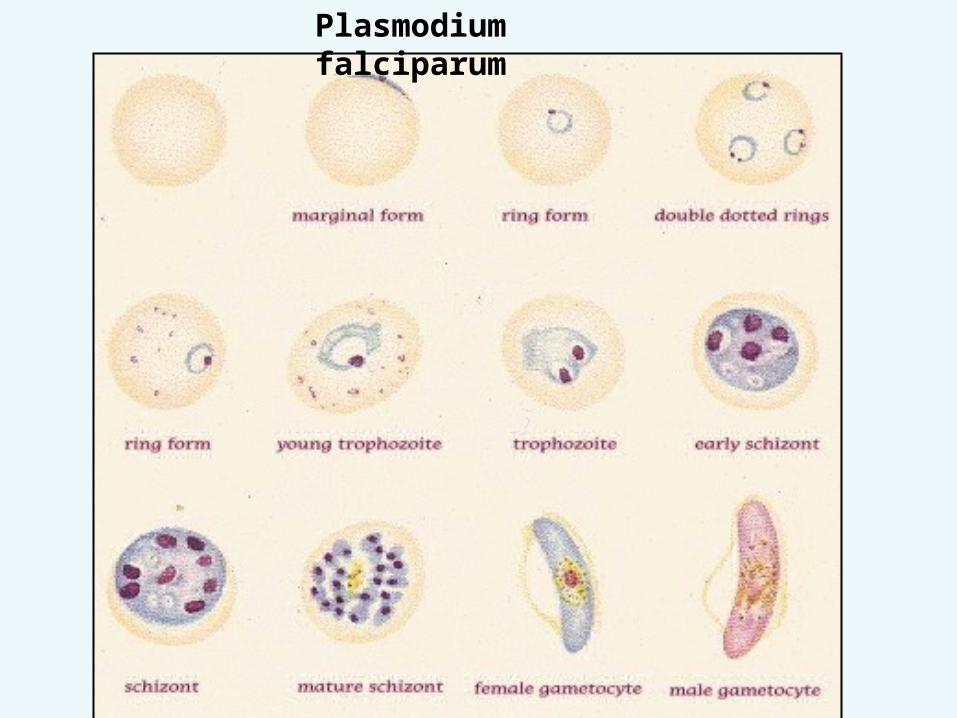
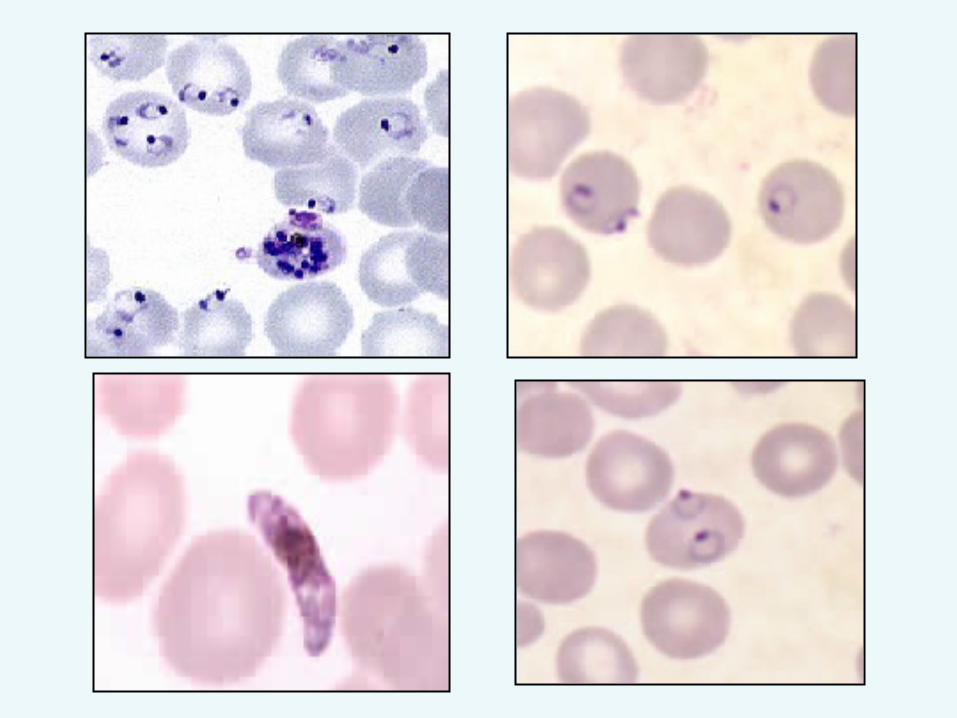
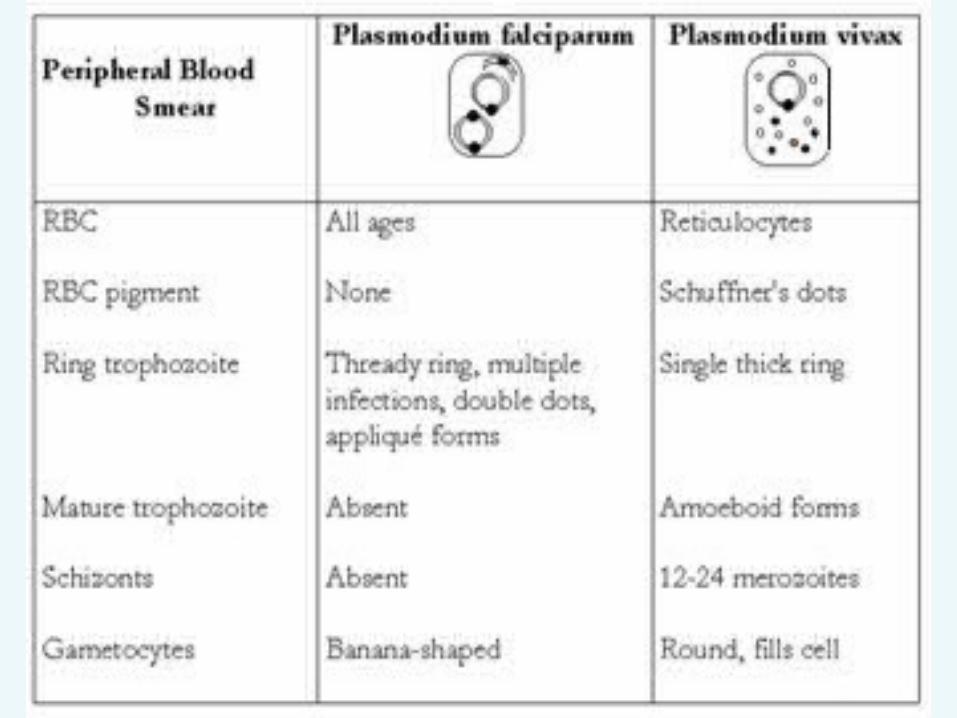
Plasmodium falciparum
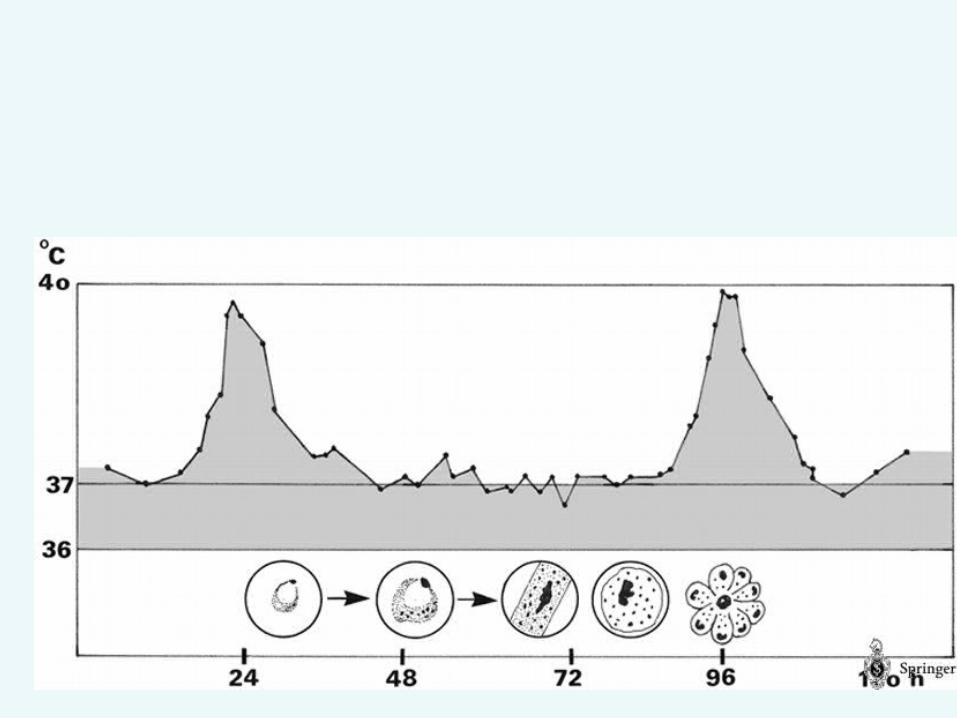
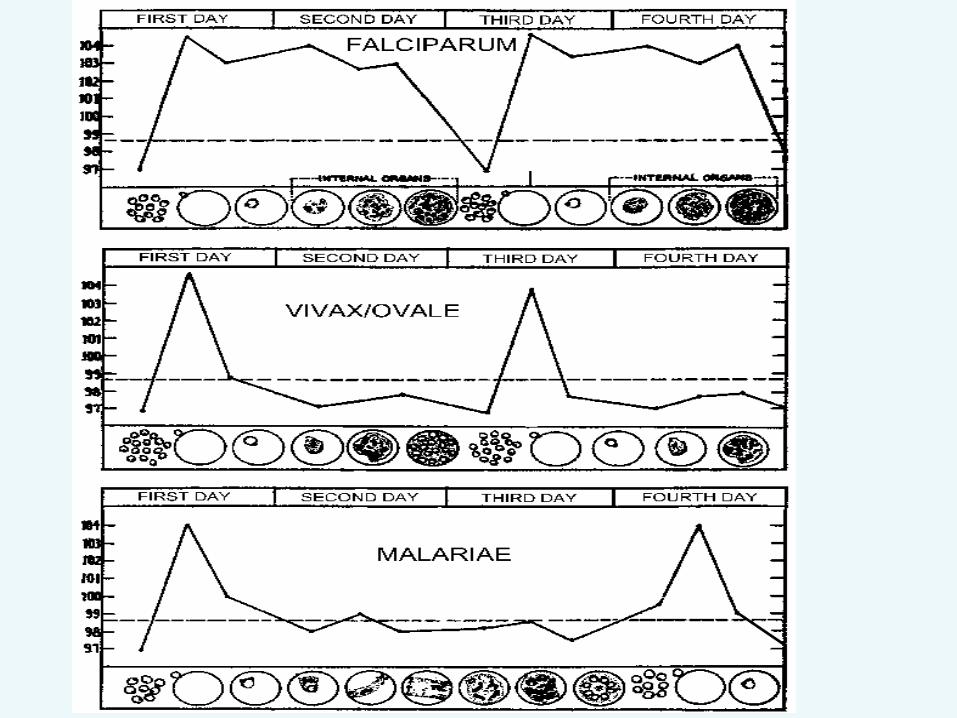
IN life cycle of P.falciparum• There is No hypnozoite stage no relapse.• Erythrocytic cycle takes 36-48 hours • Schizont contain 8-32 merozoites .• Large number of RBCs infected and many cell contain more than one trophozoite.• only ring stage and gametocyte in peripheral blood.
Anemia can be sever and rapid
•Mainly due to mechanical distraction of parasitised RBCs.
•RBCs Phagocytosed in spleen and destroyed Due to lose of deformability .
•Aplastic anemia due to effect of malarial toxins on B.M.
•Hemolytic destruction (immune sensitization).
• Erythrocytic schizogony take place in capillaries of deep organs.
(Ring and gametocyte only that appeared in blood film).
• Adhererance phenomena lead to congestion ,hypoxia ,blockage and rupture of small blood vessels, (DIC) disseminated intravascular coagulation.
• High level of parasitaemia up to 30-40 % of RBCs infected (5% considers sever).
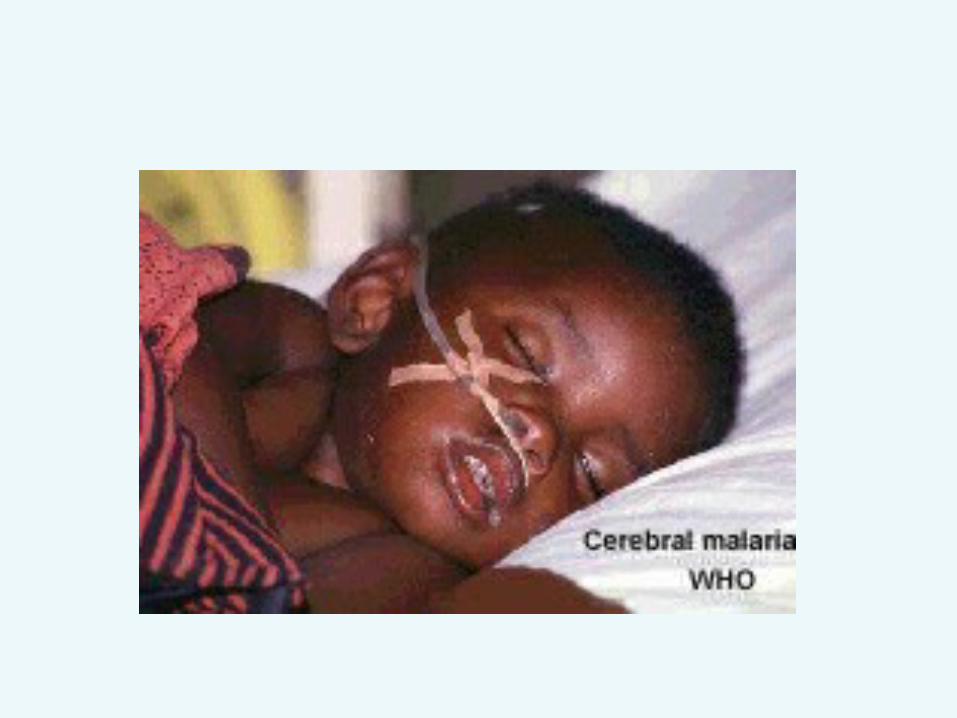
• Cerebral malaria :parasitized RBCS and fibrin block capillaries and small bl. Vessels (may causing un-arousable coma)
•Black-water fever :rapid and massive intravascular hemolysis of both parasitized and non-parasitized RBCs
Urin appears dark red to brown-black Renal failure hemoglbinurea
• Diarrhea and vomiting • Pulmonary edema • Hypoglycemia• Hyperpyrexia• Pregnant women

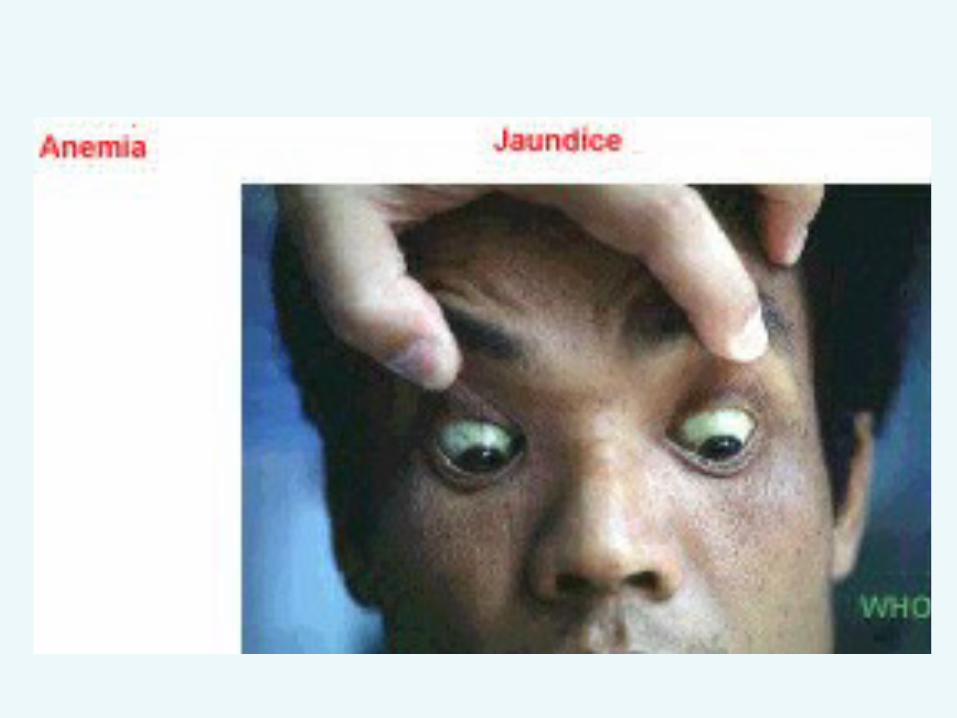
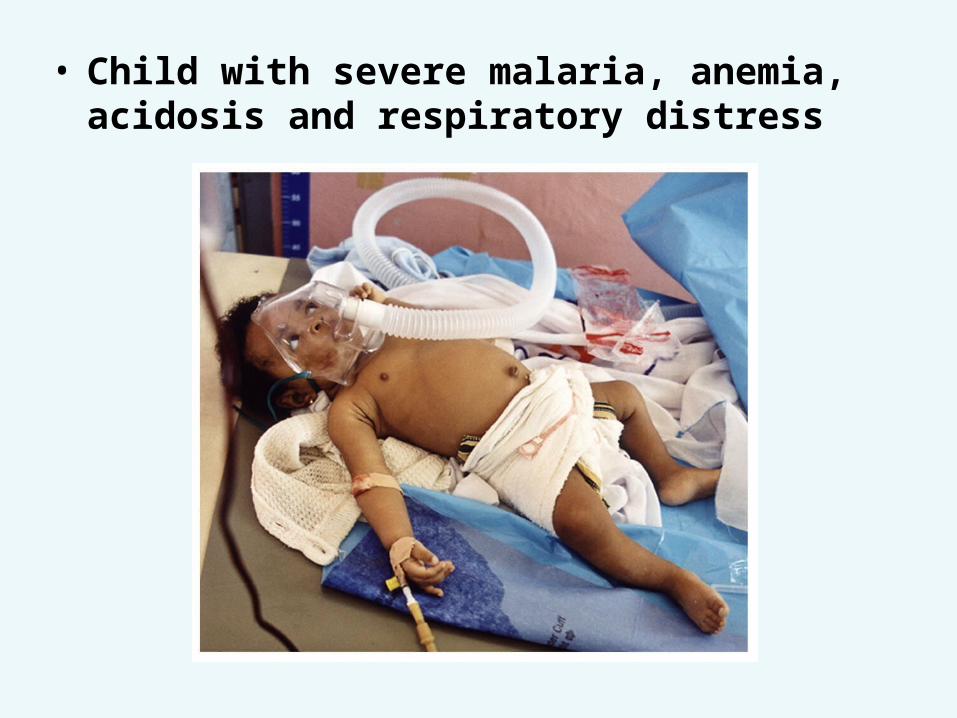
• Child with severe malaria, anemia, acidosis and respiratory distress
•P. ovale and P. vivax infect immature red blood cells
• P. malariae infects mature red cells.
• P. falciparum infects both.
Laboratory Diagnosis• microscopic identification of
parasites in blood is most certain method of confirming infection with plasmodium.
•Examination of thick (large amount) and thin blood film relation of parasite to RBCs and rate of infection
•Serologloy used in epidemiology.
Thick smear should be examined in all suspected cases of malaria because of its ability to detect parasites even when the parasitemia is low.
A thin film is used for species and stage identification and to provide information regarding erythrocytes, leukocytes, and platelets.
High parasitemia, growing stages of parasites (trophozoites and schizonts) and pigment-laden neutrophils indicate poor prognosis.
In case of uncertainty in identification of the species in severe malaria patients, it should always be considered as
P. falciparum.
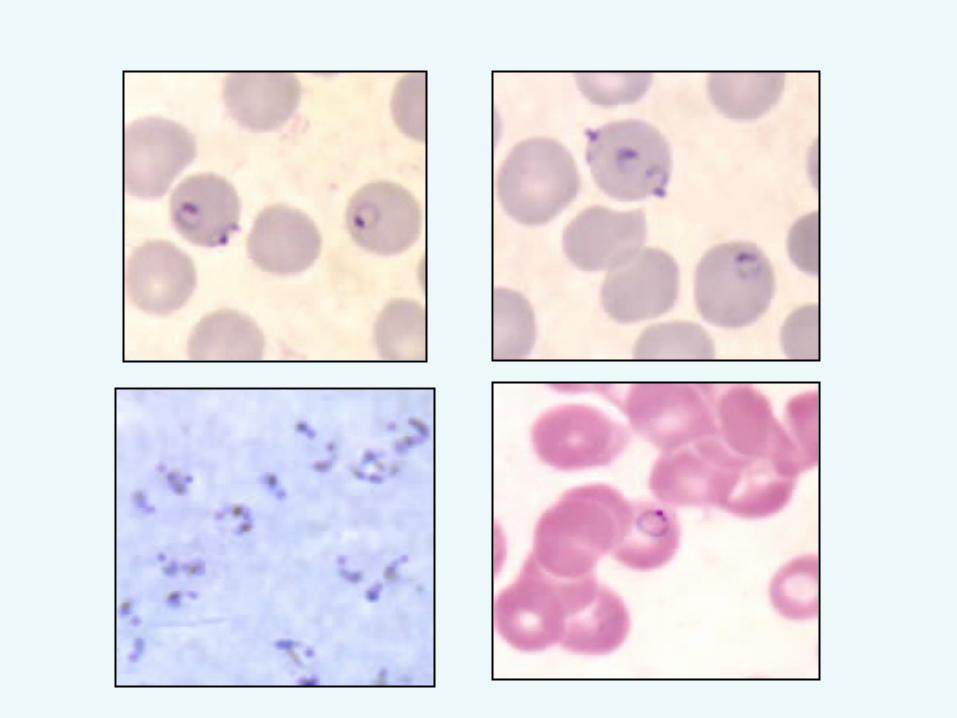
P.f. ring
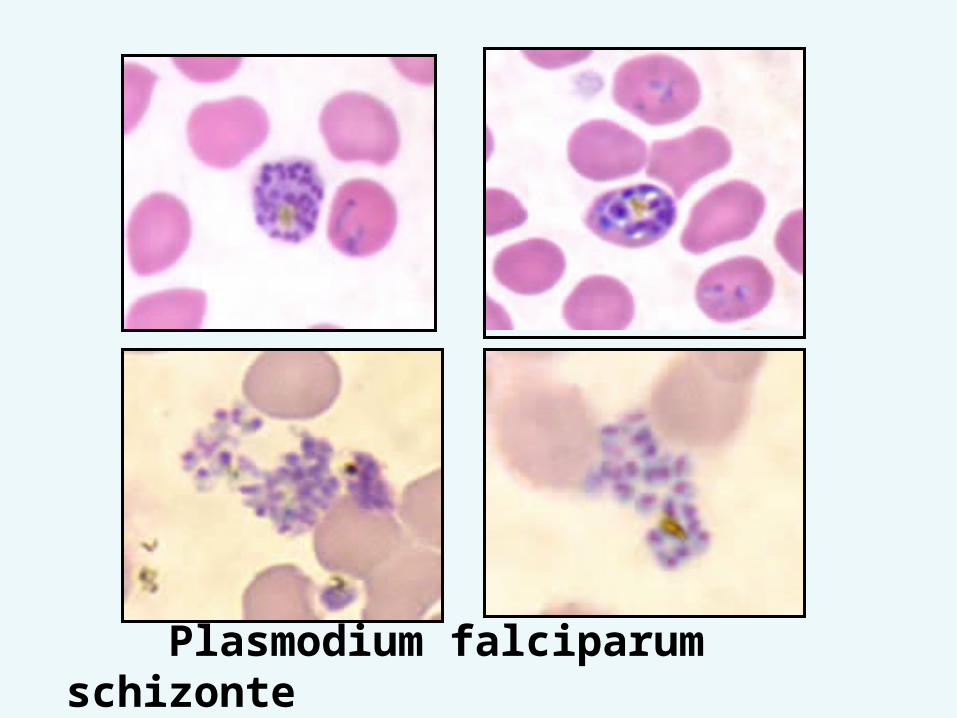
Plasmodium falciparum schizonte
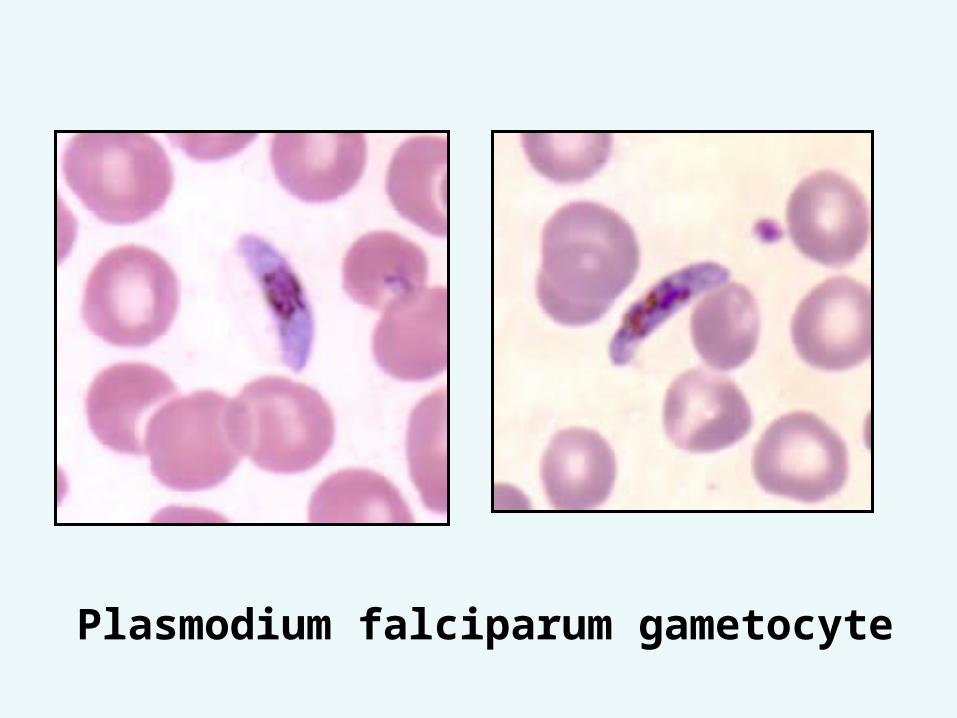
Plasmodium falciparum gametocyte
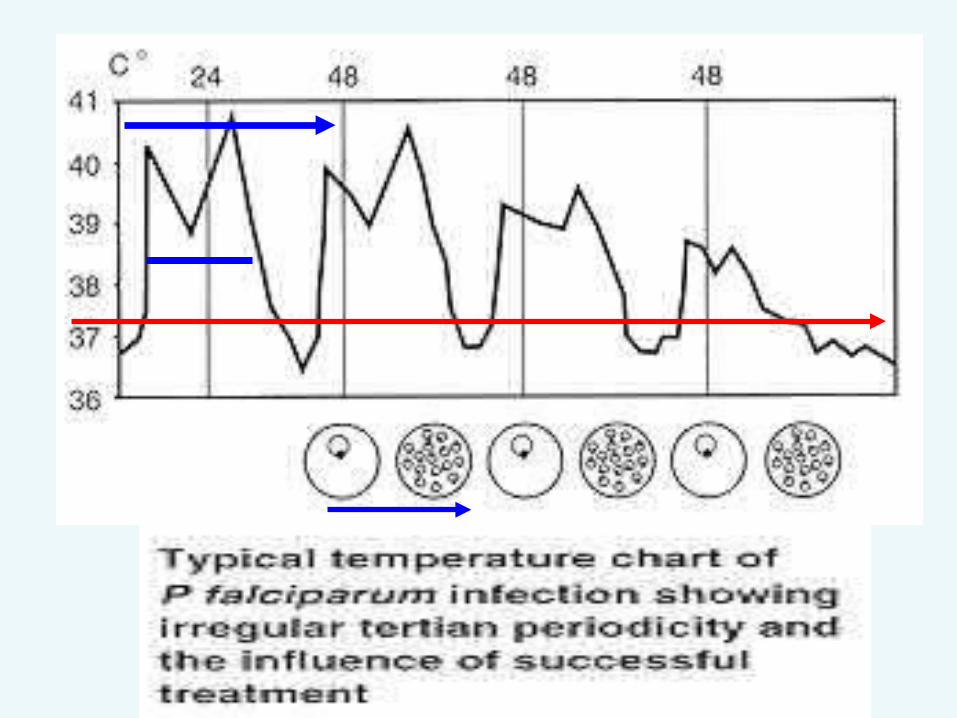
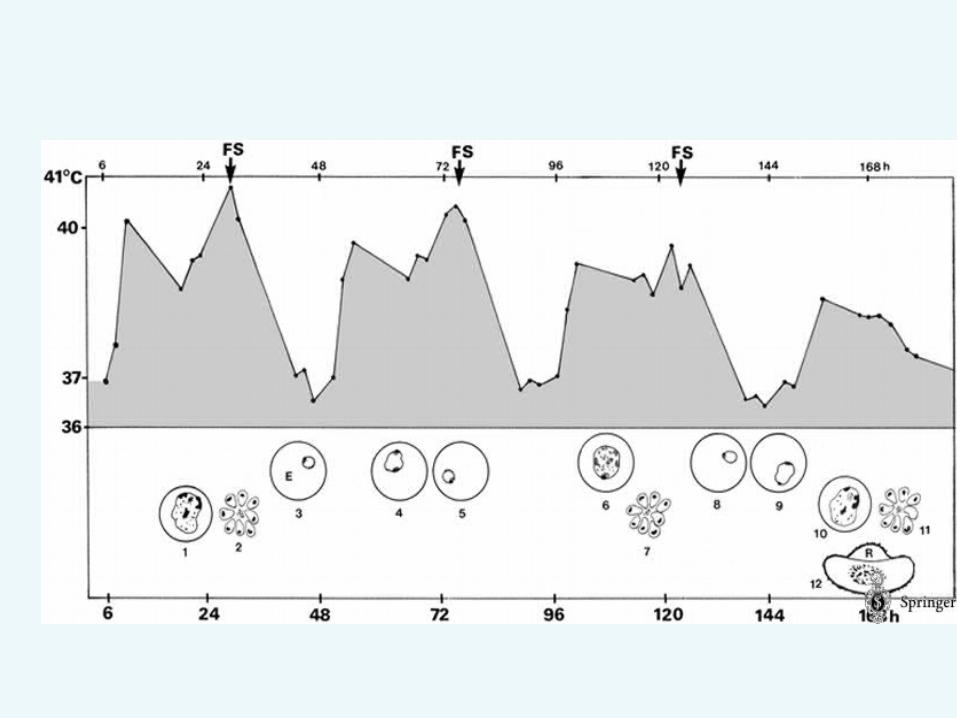
Plasmodiun vivax• Rarely infected RBCs exceed 2% infection less sever than P.f.• P.v synchronized :regular 48h pattern
of fever • All form of parasites
trophozoites ,schizontes and gametocyte can be found in blood films.
• enlargement of RBCS, schuffner`s dotes
• Spleen enlargement and anemia• Relapse are feature of P.vivax• Patient must receive treatment both
for attack and against relapsing form. (primaquine)
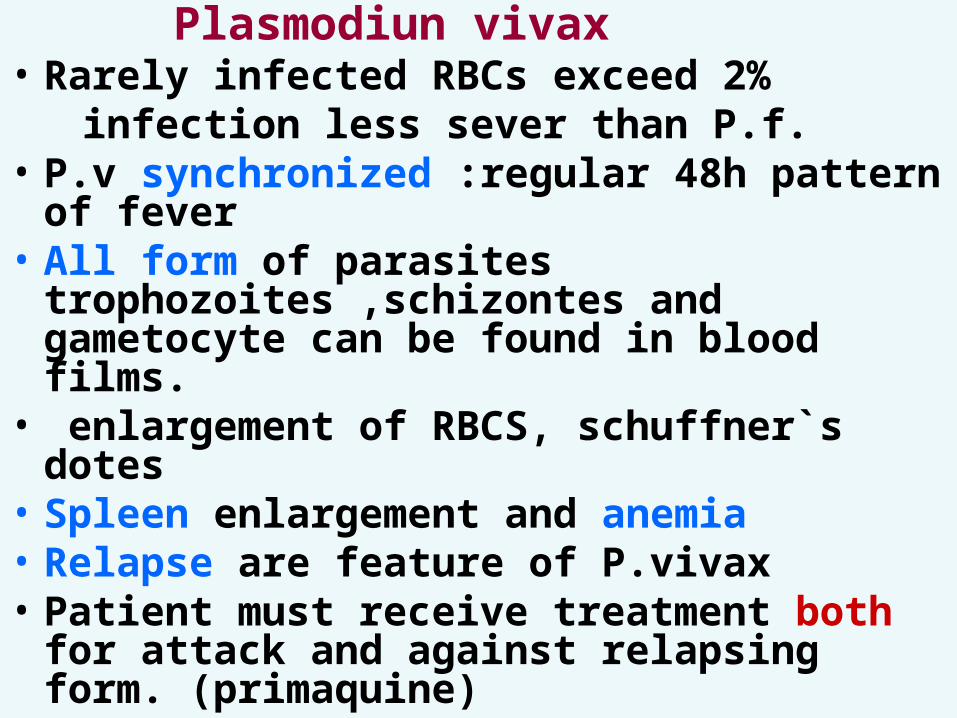
Plasmodium vivax ring stage of trophozoite
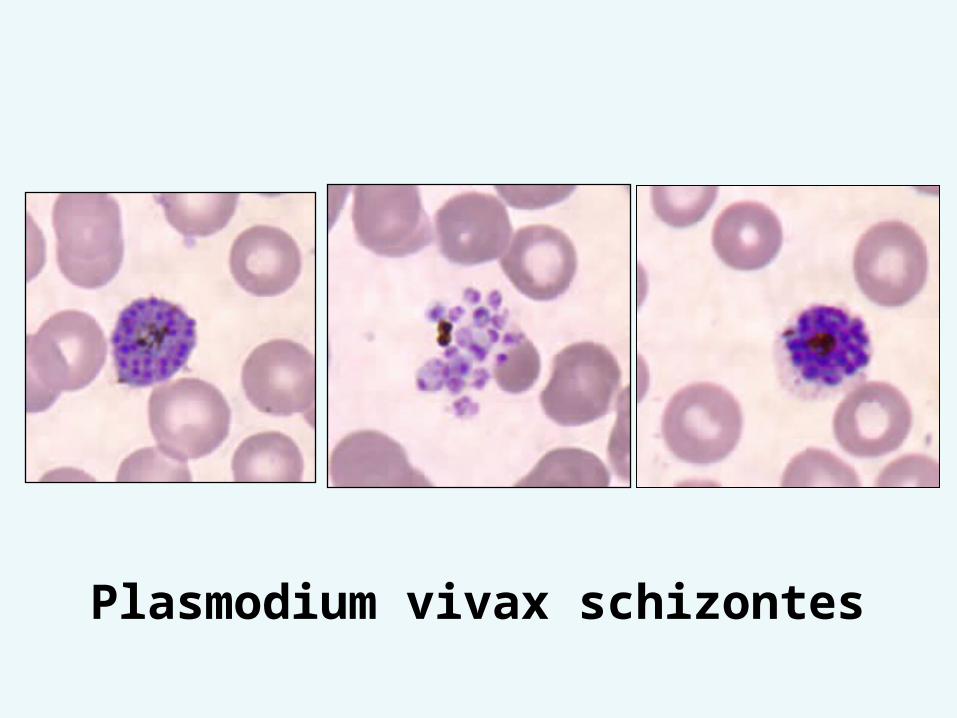
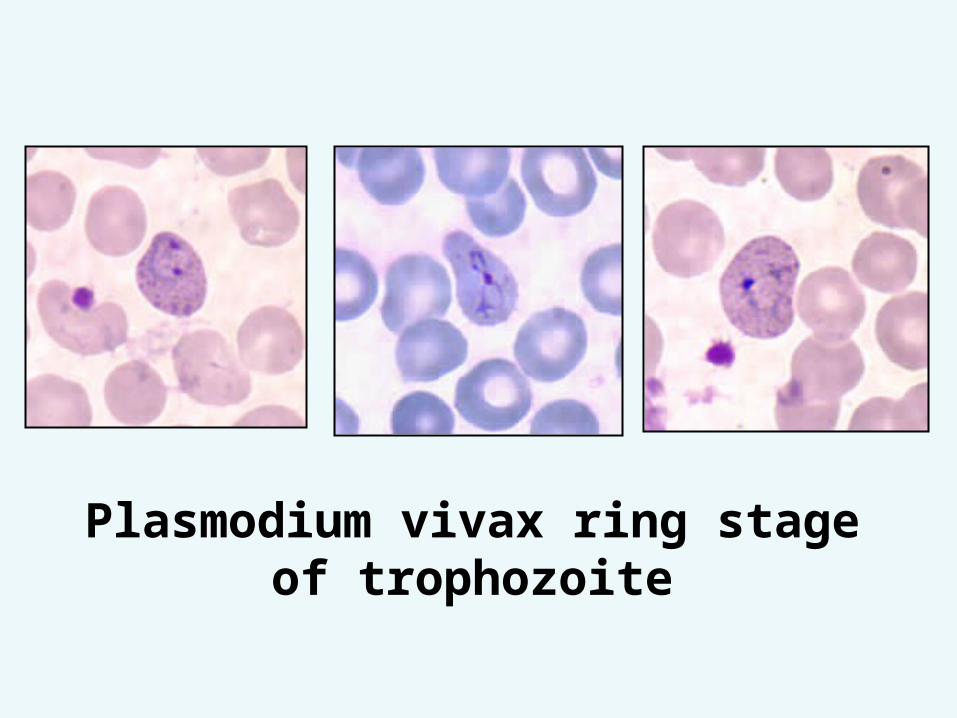
Plasmodium vivax schizontes
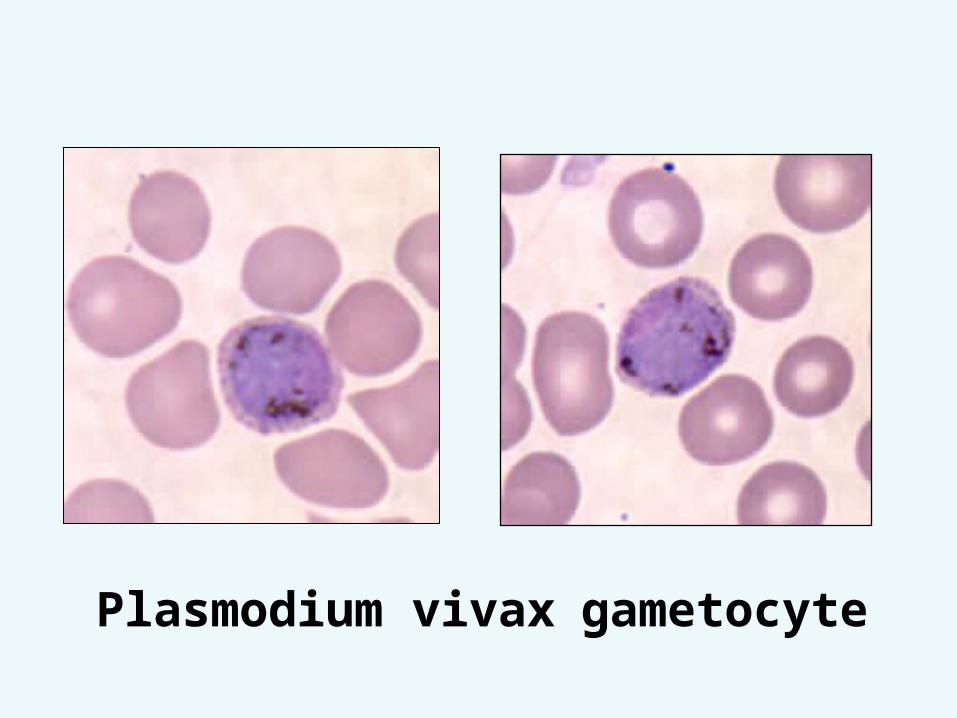
Plasmodium vivax gametocyte
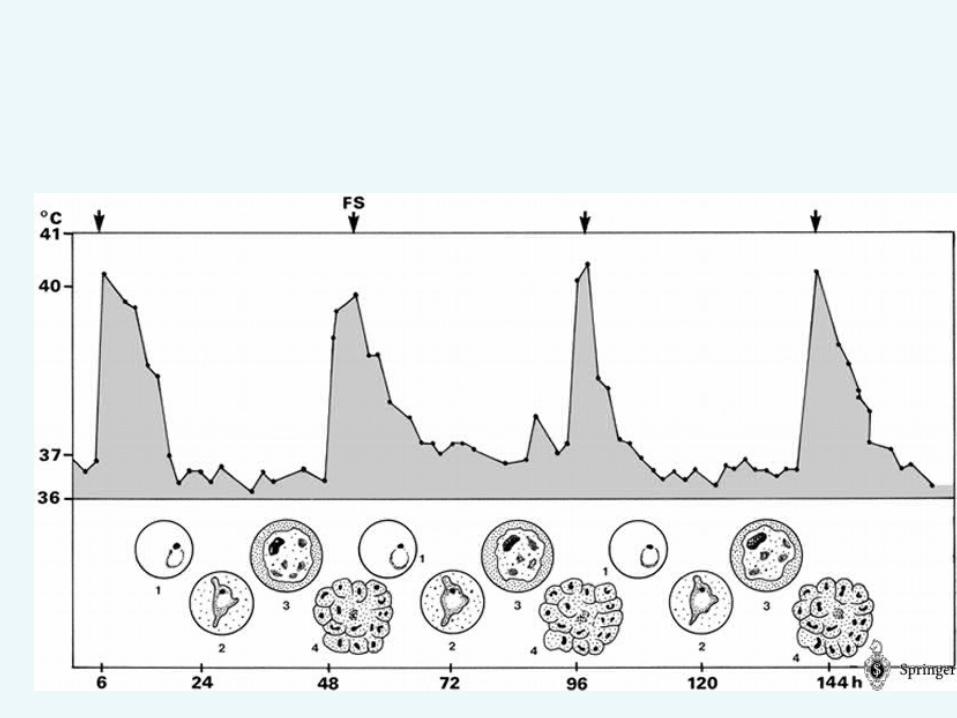
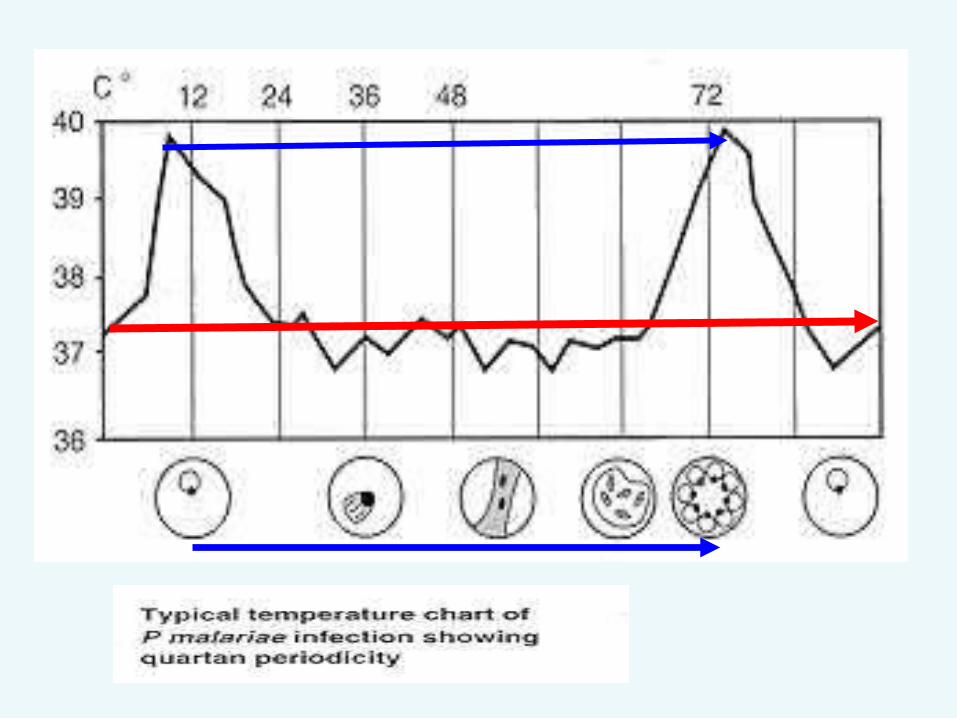
Plasmodium malariae• Cycle synchronized every 72 h.
(quarten)• Spleen enlarge early.
•Nephrotic syndrome which progress to renal failure caused by damage to kidney following deposion of antigen-antibody complex on glomerular membrane of kidney (proteinuria ,low serum albumin oedema)
• Recrudescence can occur.
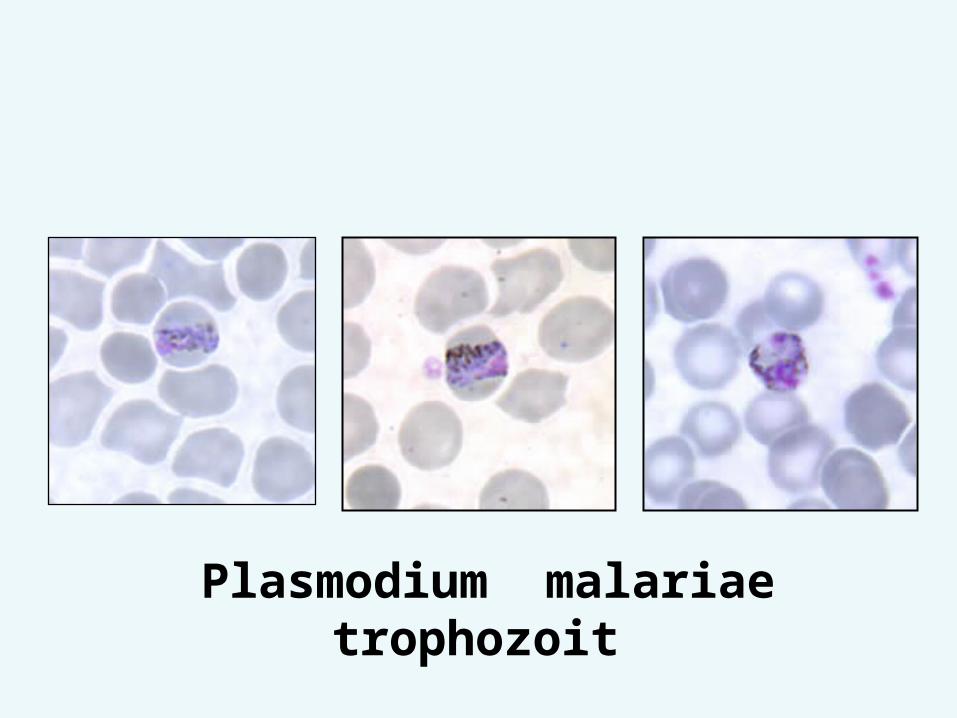
Plasmodium malariae trophozoit
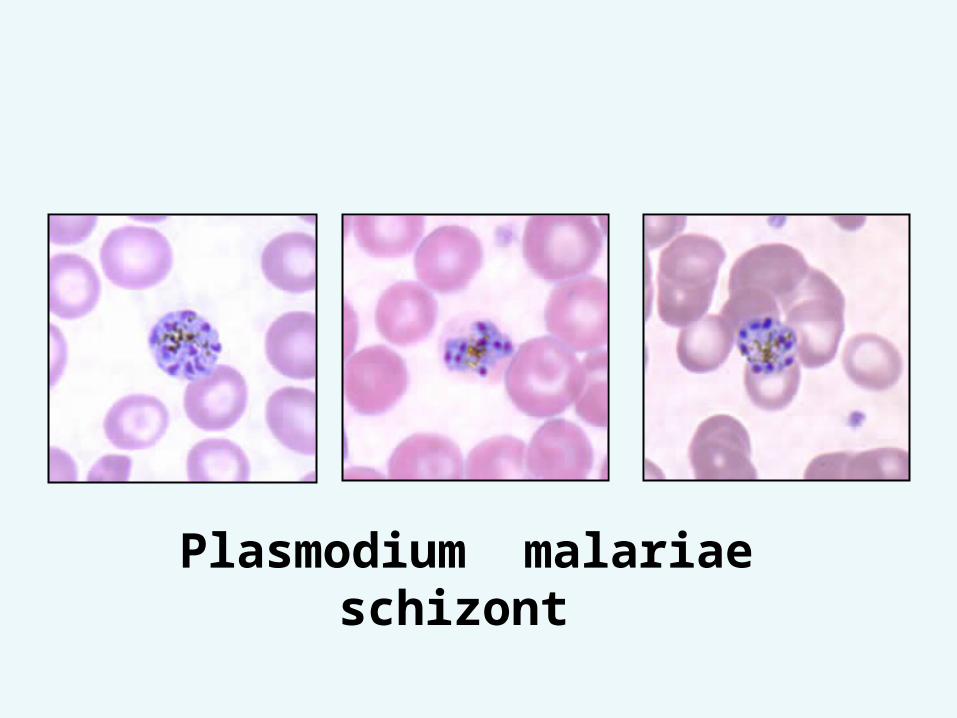
Plasmodium malariae schizont
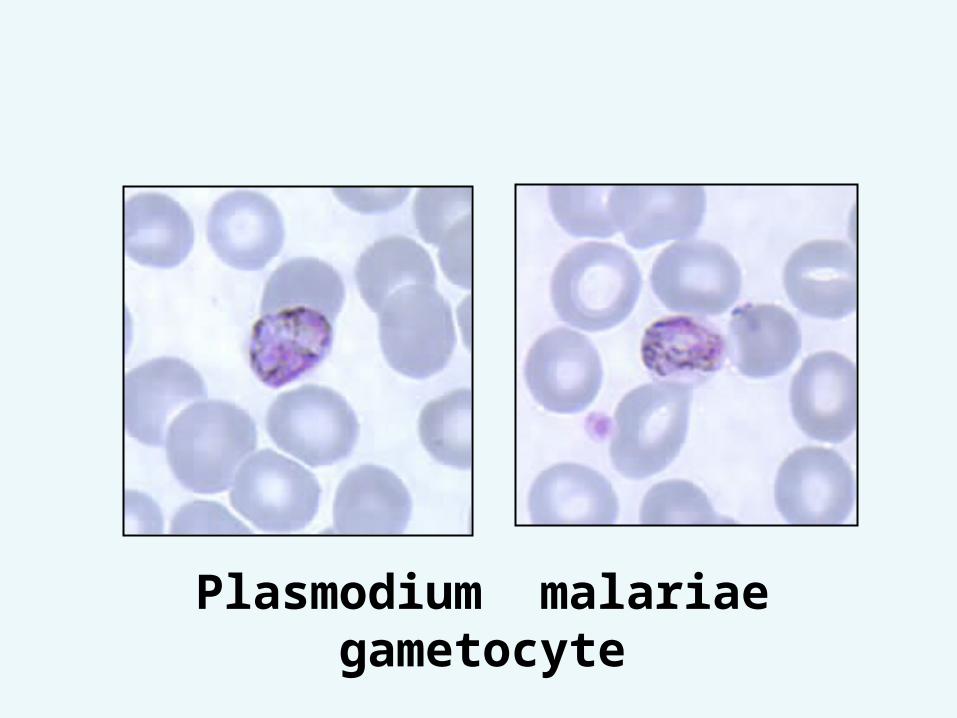
Plasmodium malariae gametocyte
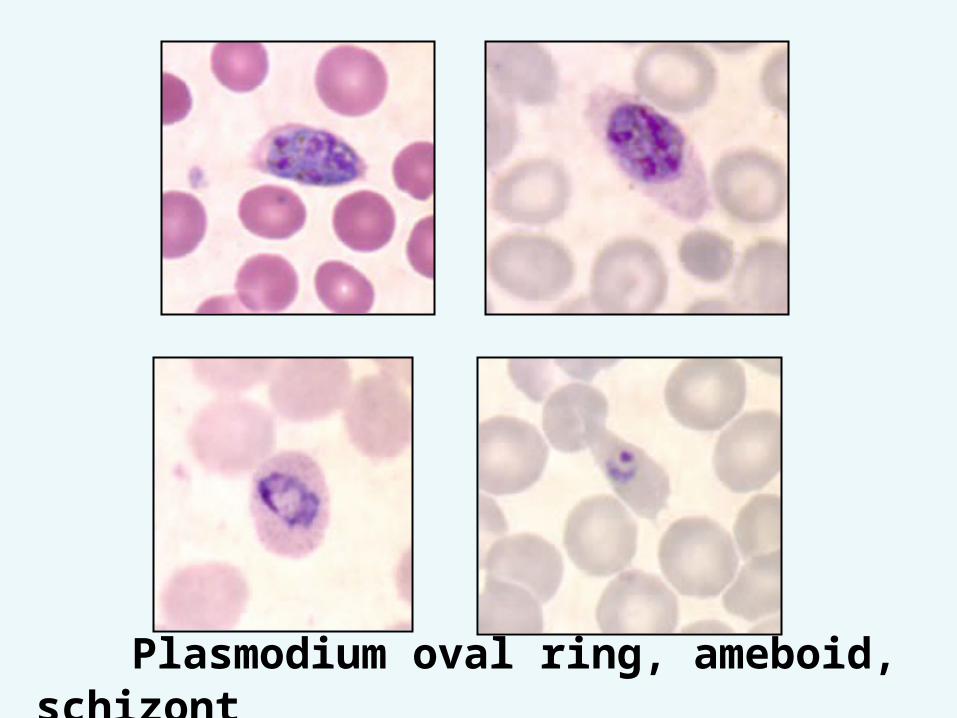
Plasmodium oval ring, ameboid, schizont
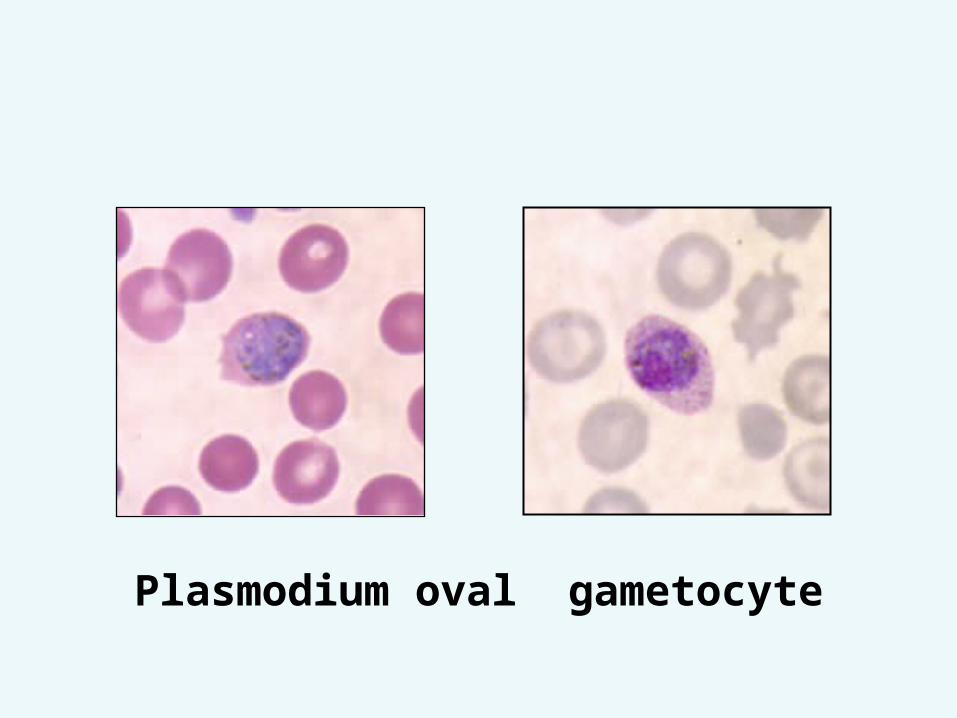
Plasmodium oval gametocyte
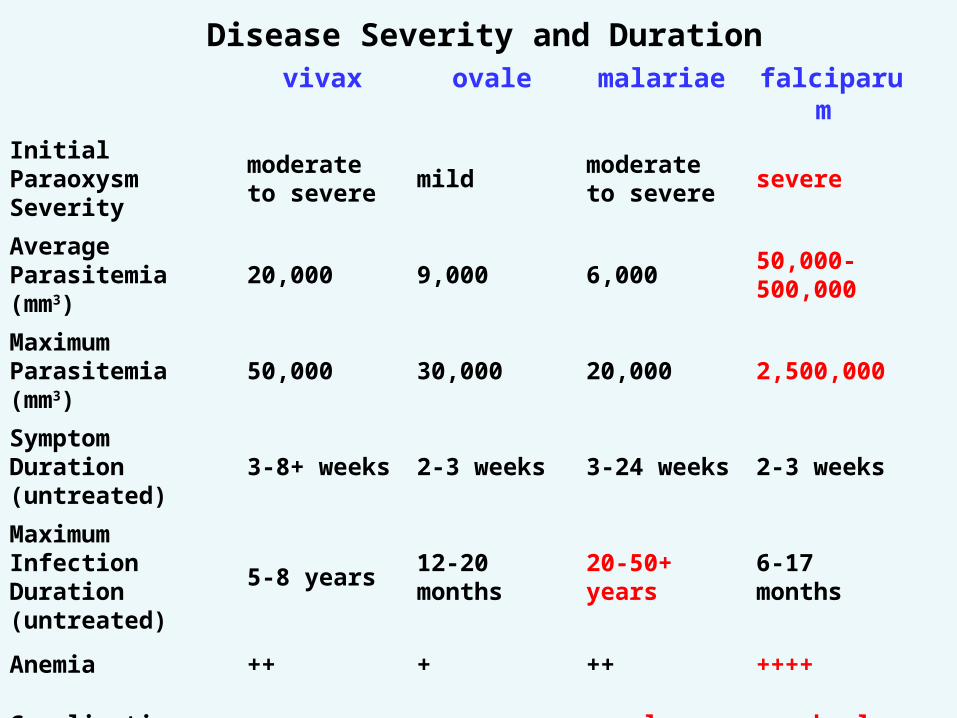
Disease Severity and Durationvivax ovale malariae falciparu
m
Initial Paraoxysm Severity
moderate to severe
mildmoderate to severe
severe
Average Parasitemia (mm3)
20,000 9,000 6,00050,000-500,000
Maximum Parasitemia (mm3)
50,000 30,000 20,000 2,500,000
Symptom Duration (untreated)
3-8+ weeks
2-3 weeks3-24 weeks
2-3 weeks
Maximum Infection Duration (untreated)
5-8 years12-20 months
20-50+ years
6-17 months
Anemia ++ + ++ ++++
Complications renal cerebralModified from Markell and Voge's Medical Parasitology
High parasitemia, growing stages of parasites (trophozoites and schizonts) and pigment-laden neutrophils indicate poor prognosis.
In case of uncertainty in identification of the species in severe malaria,it should always be considered as P. falciparum.
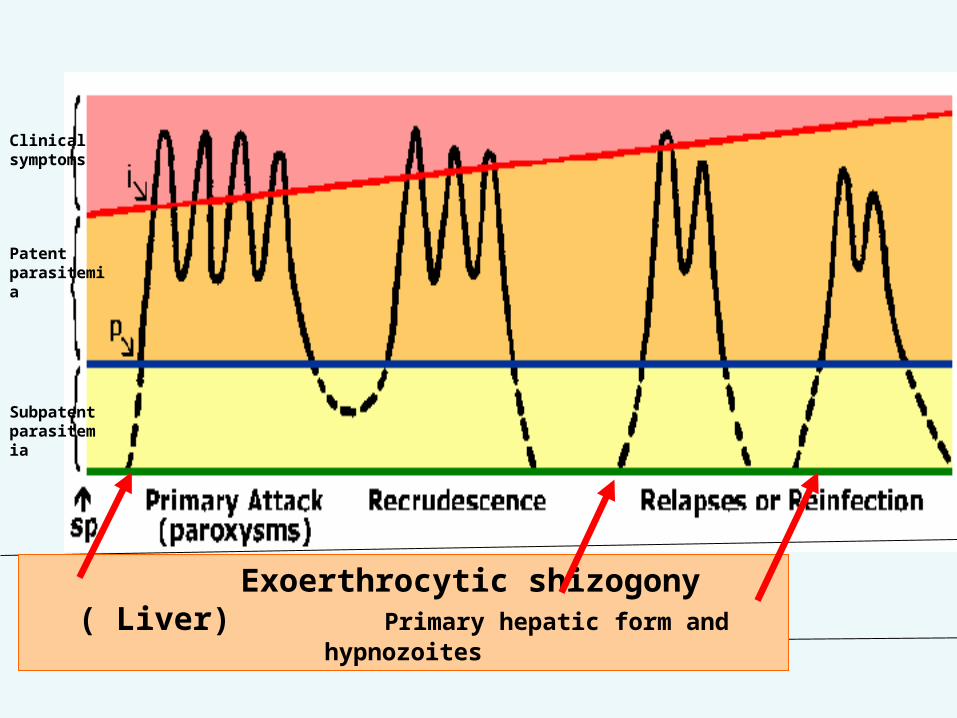
Exoerthrocytic shizogony ( Liver) Primary hepatic form and hypnozoites
Clinical symptoms
Patent parasitemia
Subpatent parasitemia

Geographical Distributions• p.vivax widespread in tropical and
subtropical areas • range extends into temperate areas • relatively uncommon in Africa • P falciparum. widespread, but
primarily in tropics and subtropics • P malariae broad, but spotty
geographical distribution • P. ovale• primarily tropical Africa, especially
western coast
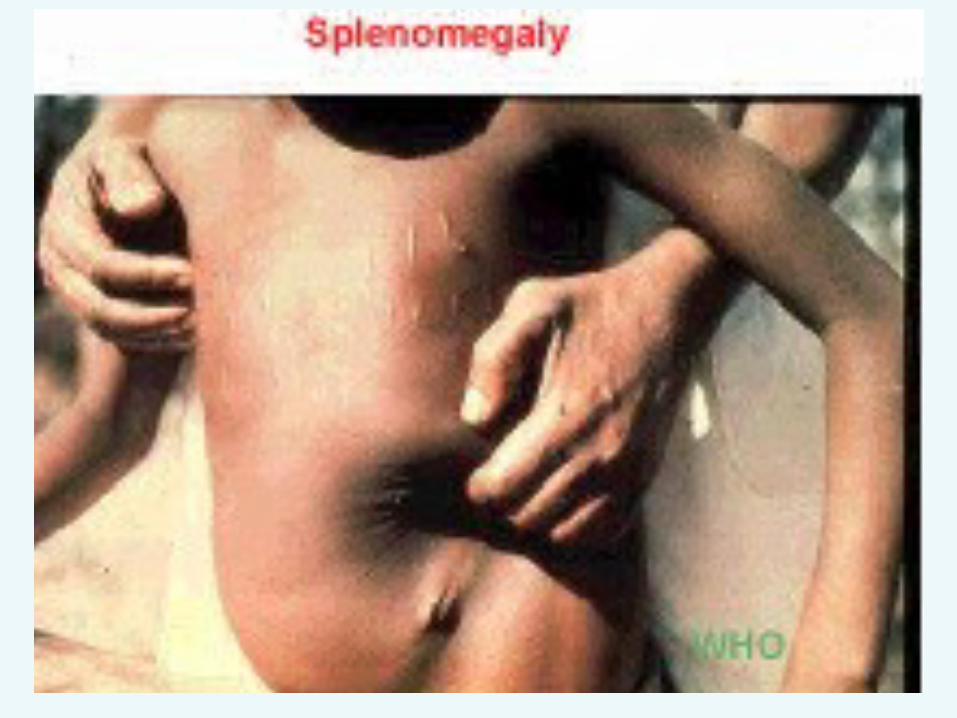
Diagnosis•history of being in endemic
area •symptoms: fever, chills,
headache, malaise •splenomegaly, anemia •microscopic demonstration of
parasite (blood smear)•antigen detection PCR
amplification of parasite DNA
Treatment Blood stages:
erythrocytic stages (Asexual schizogony)
• Chloroquine• Quinine• pyrimethamine +sulfadoxine (fansidar)• Mefloquine, halofantrine• Gametocytes: primaquine• Liver stages (in vivax, ovale
species) primaquine
In malignant malaria all is right except:
1.black water fever.2.Relapse .3.disseminated
intravascular coagulation (DIC).
4.Adhesion phenomena.5.Cerebral malaria.6.Acute renal failure
In benign tertian malaria all can occur except :
1.attack every 48 hours.2.Relapse 3.Splenomegaly 4.Un arousable coma5.High parasitamia
In Erythrocytic cycle of P.vivax:
1.Enlargement of RBCs.2.schuffner`s dots.3.DIC.4.Splenomegaly+ anaemia5.recrudescence
In P.falciparum1.High parasitemia2.Multiple infection.3.Enlargement of RBCs4.Erythrocytic tertian or sub
tertian schizogony.5.Maurer`s dots6.Adhesion phenomena
(DIC)
In P. malariae:1.Splenomegaly2.Band shape trophozoites.3.Recrudescence4.Antigen antibodes complex
depostion in glomeruli with nephrotic syndrome
5.relapse
Inoculation of the sporozoites into a new human host lead to inchoation of:
1 Exo-erythrocytic cycle (Tissue cycle) Pre-erythrocytic cycle
2 -Erythrocytic cycle.3 -Sporogonic cycle.4 -Sexual cycle.
Malarial releapse is due to1. Merozoite.2. Sporozoite.3. Hypnozoite.4. trophozoite5. schizonte
The clinical manifestations of the disease is due to:
1. Erythrocytic cycle. 2. Exo-erthrocytic cycle.3. Sporogonic cycle.4. Rupture of infected RBC and
release malarial pigments and toxin.
Infective stage in saliva of female Anopheles is:
1. Merozoite.2. Schizonte.3. Trophozoite.4. Sporozoite.

Feature of intestinal and tissue protozoa:• Entamoeba histolytica, G.lamblia are
motile organisms that multiply and encyst in intestinal tract. they form cyst which excreted in faces. Invasive strains of
E histolytica multiply in intestinal wall.• Cryptospordium multiply intracellular in
cells. It produces oocysts which are excreted in feces.
• T.gondii muliply intracelluler in reticuloendothelial cell and cell of brain and other organs of body.
• T.vaginalis is motile and multiplies in the urogenital tract cyst forms are unknown
Infection is by ingesting • cysts (E.histolytica, G.lamblia) or • oocyst (Cryptosporidium,T.gondii) in food,water,or from hands
contaminated with infected feces. T.gondii can also be transmitted
congenitally and by ingesting the parasites in under-cooked meat of intermediate hosts.
T.vaginalis is transmitted sexually (no cyst).
Humans are important hosts of E. histolytica, G.lamblia and T.vaginalis.
Animal are natural definitive hosts of Cryptosporidium and T.gondii .
• Laboratory confirmation of E.histolytica infection is by finding amoebae or cysts in feces or by detecting antibodies in serum (invasive amoebiasis)
• Giardiasis diagnosed by finding motile flagellates or cysts in feces or flagellates in duodenal aspirates.
• Infection with Cryptosporidium is diagnosed by finding oocyst in feces
• Toxoplasmosis is usually diagnosed serologically.
• T. vaginalis infection is usually confirmed by detecting flagellates in vaginal or uretheral discharge or urine.