Embed Size (px)
Citation preview

Miss. Anushree S. Deshpande Mr. Harshitkumar B. Patel Mr. Arvind D. Vasoya
By
Project submitted ToRajiv Gandhi University of Health Sciences,
Bangalore, Karnataka.
Department of Clinical Pharmacy,H.S.K Hospital and Research center &
Hanagal Shri Kumareshwar College of Pharmacy,Bagalkot- 587101, Karnataka, India
2014.
EVALUATION OF ANTIMALARIAL DRUGS USE IN A TERTIARY CARE TEACHING HOSPITAL
Doctor of PharmacyUnder the guidance of
Mr. MALLAPPA H. SHALAVADI M.Pharm, [Ph.D.]

INTRODUCTION

• India has the largest population in the world at risk of
malaria, with 85% living in malarious zones
•Malaria is a tropical disease transmitted by the female
Anopheles mosquito of which Anopheles gambiae is the
most efficient vector.

• It is caused by infection by the protozoan parasite of
the genus plasmodium, is a disease of global
importance.
• Malaria is a major cause of morbidity and mortality
in the developing world.
• It is a public health problem in more than 90
countries.

• Each year, between 300 and 500 million new cases
are reported worldwide.
• Around 1.5 million confirmed cases are reported annually by the
National Vector Borne Disease Control Programme (NVBDCP),
of which about 50% are due to Plasmodium falciparum.

• WHO now recommends that treatment policies for
falciparum malaria in all countries experiencing
resistance to monotherapies such as chloroquine,
sulphadoxine-pyrimethamine and amodiaquine, should
be combination therapies preferably those containing an
artemisinin derivative.
• Artemisinin and its derivatives are a group of drugs
that possess the most rapid action of all current drugs
against Plasmodium falciparum malaria.

Page 7
• Patient counseling on malaria.
•To identify the potential drug-drug interactions in prescriptions.
•Adjusting doses in appropriate patients (e.g., Patients with
impaired renal or hepatic function).
Role Of Pharmacist

Study Methodology

Study procedure
• The study is approved by Institutional Human
Ethics Committee [Ref: SNMC/PG/2013-
14/2885], S.N.M.C and H.S.K Hospital and
research Centre, Bagalkot.
• The study will be conducted in accordance
with the ethical principles of the ethics
committee guidelines

• This study was conducted in S.N Medical College
and HSK hospital and research center Bagalkot.
• We have taken cases from general medicine and
Pediatric Departments.
• It is a 850 bedded general hospital run by the BVV
Sangha.
Study site

Study criteria
Inclusion criteria
- Patients diagnosed with malaria.
- Patients of all age group of either sex.
- Patients receiving anti-malarial drugs.
Exclusion criteria
- Patients attending outpatient department

Source of data
• Past prescription.
• Patient data collection form, patient case notes
• Lab data reports.
• Treatment charts .
• Drug intervention and interaction form.
• Interviewing patients.
• Discharge cards/advice on discharge.

Methodology
• Personal visit made on daily basis to general medicine ward and
pediatric wards to identify the patients who were diagnosed with
malaria.
•Patient demographic details were collected.
•Clinical data was collected.
•Name of drug, dose, frequency, duration and cost of treatment
noted in patient data collection form.

• Potential drug-drug interactions in the treatment regimen have
to be assessed using Micromedex-2.0.
• The inpatient data collected and created separately in computer
based format, stored and retrieved when they required in MS
office format.

RESULTS
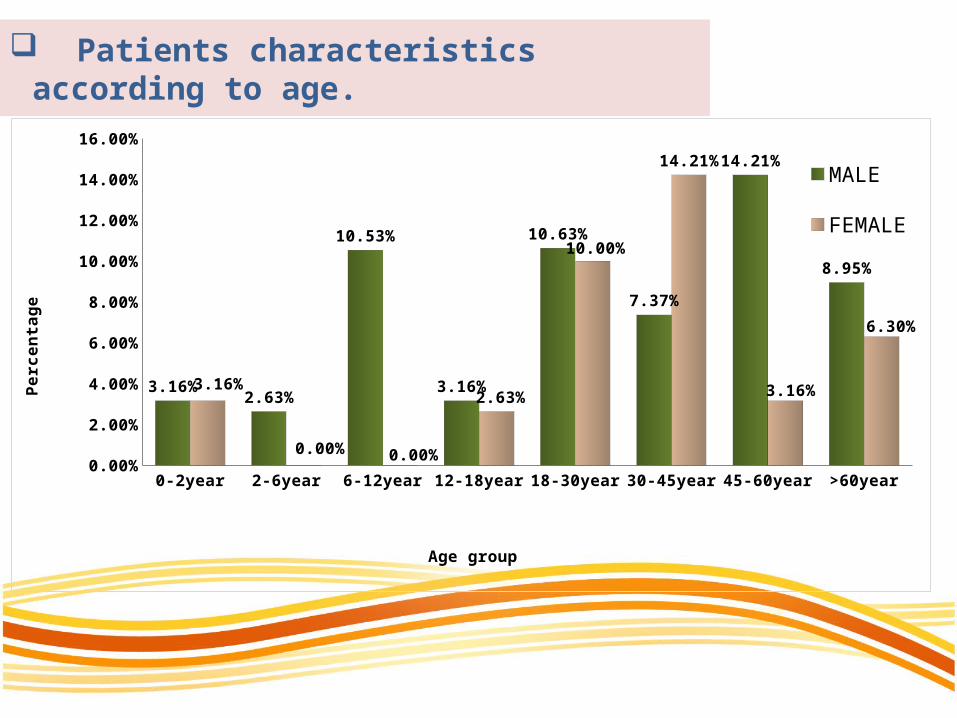
Patients characteristics according to age.
0-2year 2-6year 6-12year 12-18year 18-30year 30-45year 45-60year >60year0.00%
2.00%
4.00%
6.00%
8.00%
10.00%
12.00%
14.00%
16.00%
3.16%2.63%
10.53%
3.16%
10.63%
7.37%
14.21%
8.95%
3.16%
0.00% 0.00%
2.63%
10.00%
14.21%
3.16%
6.30%
MALE
FEMALE
Age group
Perc
enta
ge

Pattern of malaria parasite infection in patient visiting tertiary care hospital
Plasmodium falciparum
Plasmodium vivax
Mixed
Clinical malaria
Complicated malaria
0.00% 20.00% 40.00% 60.00% 80.00%
58.69%
8.69%
6.52%
6.52%
19.50%
Percentage of prescription
Percentage

Number of uncomplicated malaria cases
Plasmodium vivax
Plasmodium falciparum
Pregnant women with plasmodium falciperum
Mixed clinical malaria
0.00%
10.00%
20.00%
30.00%
40.00%
50.00%
60.00%
70.00%
80.00%
8.11%
70.27%
2.70%
10.81% 8.11%

Antimalarial drugs prescribed for patient visiting tertiary care hospital
Artesunate
Aretsunate+Pyrimethamine+Sulphadoxine
Artemether/Lumefantrine
Chloroquine phosphate
Doxycycline
Primaquine
Hydroxy chloroquine sulfate
Quinine
0.00% 5.00% 10.00% 15.00% 20.00% 25.00%
14.40%
19.70%
17.42%
12.12%
23.49%
8.33%2.28%2.28%
Percentage of prescription of antimalarial drugs

Antimalarial drugs given in complicatedmalaria cases
Artesunate
Artesunate+sulphadoxine+ Pyrimithamine
Doxycycline
Chloroquine
Artemether & lumefantrine
Primaquine
0 0.5 1 1.5 2 2.5 3 3.5
2
2
3
2
3
2
Number of antimalarial drugs

Artesunate prescribed for patient visiting tertiary care hospital
Antimalarial drug
Malaria cases (n=46)
Non malarial cases (n=52)
Number of prescription
Percentage (%)
Number of prescription
Percentage (%)
Artesunate 25 54.34 17 32.69
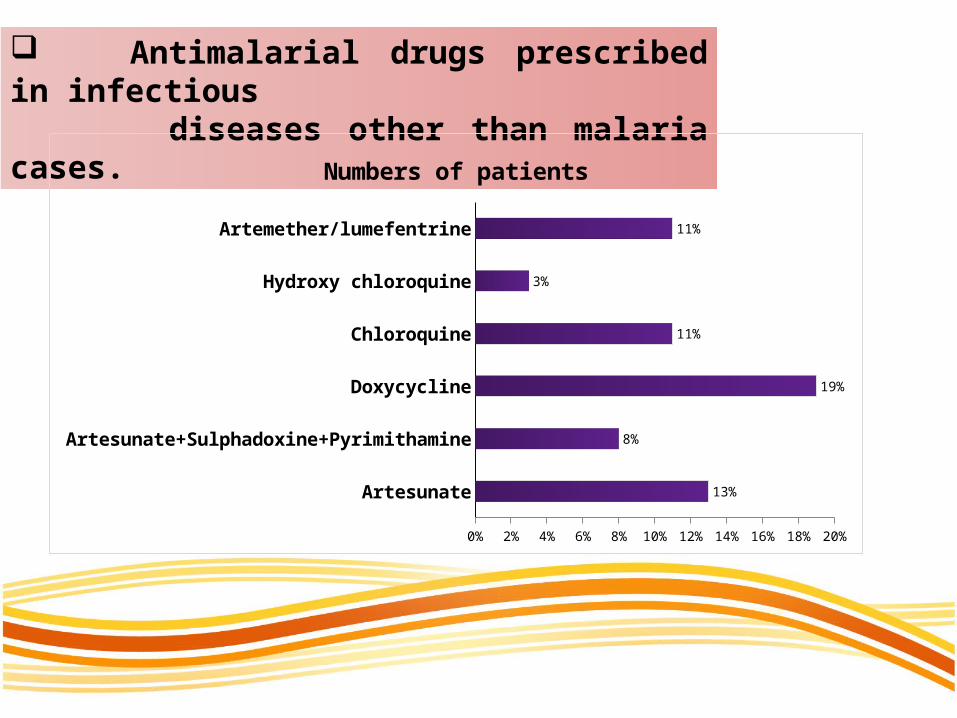
Antimalarial drugs prescribed in infectious diseases other than malaria cases.
Artesunate
Artesunate+Sulphadoxine+Pyrimithamine
Doxycycline
Chloroquine
Hydroxy chloroquine
Artemether/lumefentrine
0% 2% 4% 6% 8% 10% 12% 14% 16% 18% 20%
13%
8%
19%
11%
3%
11%
Numbers of patients

Pattern of drugs regimen prescribed for patients
1 Drug therapy
2 Drugs therapy
3 Drugs therapy
4 drugs therapy
5 Drugs therapy
0.00% 5.00% 10.00% 15.00% 20.00% 25.00% 30.00% 35.00%
26.84%
24.48%
30.61%
9.18%
1.02%Percentage
Percentage

Drug interaction found in prescriptions.
Major Moderate Minor Contraindicated0.00%5.00%
10.00%15.00%20.00%25.00%30.00%35.00%40.00%45.00%50.00%
43.24%
32.43%
18.92%
8.11%
Percantage

Drug-drug interaction of artemisinin derivatives with other drugs in malaria and nonmalarial cases.
Infection Drug-drug interactions Percentage
Malarial cases(n=46) 1 2.17%
Non malarial
cases(n=52)
7 13.46%

Assessment of rationality of antimalarial drugs prescribed for patient according to guidelines.
plasmodium vivax
plasmodium falciparum
mixed
clinical malaria
complicated malaria
0.00% 10.00% 20.00% 30.00% 40.00% 50.00% 60.00% 70.00% 80.00%
12.00%
52.00%
12.00%
12.00%
12.00%
4.76%
66.67%
0.00%
0.00%
28.57%irrational
rational

Clinical outcome
Outcome Number of patients Percentage
Improved 22 47.83%
Cured 24 52.17%
Worsened 00 00.00%
Expired 00 00.00%
Total 46 100%

Drug use evaluation of antimalarial drugs prescribed for patients with help of prescribing indicator.
Indicator Data
Average no of drug 1.42
I.V. injection(percentage) 44.89%
Cost of antimalarial drug prescribed for patient visiting tertiary care hospital.
Indicator Data
Average drug cost 1085.22 Rs
Percentage drug cost on injection 86.51 %

Discussion
• Drug use indicator has provided easy & convenient
measures to assess optimal drug used in health facilities.
• In our study, we collected total 98 cases prescribed with
antimalarial drugs amongst them 60.5% were male and
39.49% female, which was also seen in previous studies
conducted in various areas
• Out of 46 malarial cases, 78.78% were positive for
plasmodium falciparum and 21.22% were positive for vivax
and mixed type. This indicate Plasmodium falciparum is
more common in this area of Karnataka for malarial
infection.
• Major prescription of antimalarials were 19.70% of artesunate +
sulfadoxine + pyrimethamine, 17.42% of artemether +
lumifantrine, artesunate 14.4%.
• Prescribing artesunate alone leads to development of resistance
according to NVBDCP. Artesunate should be given in
combination with Sulfadoxine/Pyrimethamine or lumefantrine.
• Three drug combination was more prescribed i.e 30.61%. Almost
all combination contain artemisinin derivatives which was in
accord with guidelines.

• In malarial cases, we found 45.65% of irrational prescription and
82.69% of non malarial cases.
• More irrational procreation arise for patients suffering with
plasmodium falciparum malaria this will shows our hospital
clinicians are not adhered to guidelines to treat the malarial cases.
• Prescribing indicators shows 44.879% of I.V. injections were
prescribed, this will increase cost of the prescriptions as injections
are costlier than oral therapy.
• The cost of injections was found 86.51% out of total cost. This
because I.V. preparations were used more and are much more
expensive.

Conclusion Our study shows that inappropriate use of antimalarial drugs was high
among patient with plasmodium falciparum and nonmalarial patients.
Irrational prescriptions are high which indicate non adherence to
guidelines. Cost of therapy is very high thus it contribute economic
burden on patients.
Bagalkot is endemic for Plasmodium falciparum & Plasmodium vivax
malaria and there is requirement of rational prescriptions for
betterment of therapy for malaria.
This result should inform education of health professional and rational
drug use policy and to reduce the cost of prescription.
Recommendation
This study has to be conducted in other hospital of Baglakot district.

Annexure

Antimalarial drug cost documentation form
Name of drug
Cost of drug
1 2 3 4 5 6 7 8 9 10 Cost per day
Total[Total Day × cost per day]
Total
Name of the Staff Incharge : Signature of staff Incharge : Remarks of the staff Incharge :

Acknowledgement
• With great pleasure and pride we express our deepest thanks to our guide,
Mr. Mallappa H. Shalavadi, Department of Pharmacy Practice, H. S. K
College of Pharmacy, Bagalkot.
• It is our privilege to extend our cordial and humble thanks to Dr. I. S.
Muchchandi, principal, and Dr.Chandrasekhar. V. M Professor and HOD,
H. S. K College of Pharmacy, Bagalkot.
• We also express our humble thanks to Dr. Ashok. Mallapur Principal and
Dr. Chandrashekar T M. Dean, S. N Medical College & HSK Hospital and
Research Centre, Bagalkot.















![malaria [Autosaved].ppt](https://img.dokumen.tips/doc/110x75/563db79c550346aa9a8cabc6/malaria-autosavedppt.jpg)














