Embed Size (px)
Citation preview

299
Haematological diseases :periodontal manifestationsand patient management.
Certain systemic diseases or disequilibriums can have repercussions on the periodontium. The majority of hemo-pathies present periodontopathic signs being often the first manifestations of this hemopathy. These afflictionsrequire special attention by the practician. During patient management, certain precautions should be taken
with regards to infectious and hemorrhagenic risks.
Keywords :HematologyPeripheral manifestationsPeriodontiumRisk Prevention
U n certain nombre d'affections ou de déséquilibres organiques peuvent avoir un retentissement au niveau paro-dontal. La plupart des hémopathies peuvent s'accompagner de signes parodontaux qui sont parfois les pre-mières manifestations.
Ces maladies nécessitent une prise en charge particulière de la part du chirurgien dentiste. Lors de cette prise encharge, des précautions sont à prendre en ce qui concerne les risques infectieux et hémorragiques.
accepté pour publication le 15/05/02 Rev Odont Stomat 2002;31:299-320
A. BOUZIANE*, L. BENRACHADI**, O.K. ENNIBI**, L. ABDELLAOUI**, N. BENZARTI***
* Résidente au service de Parodontologie, CCTD Rabat** Professeur agrégé en Parodontologie à la Faculté de Médecine Dentaire de Rabat*** Professeur de l’enseignement supérieur, Chef de service de Parodontologie, CCTD Rabat
Revue d’Odonto-Stomatologie /novembre 2002
Maladies hématologiques :manifestations parodontaleset prise en charge.
Mots clés :HématologieManifestation à distanceParodonteRisquePrévention
PARODONTIE

300Revue d’Odonto-Stomatologie /novembre 2002
PARODONTIE
L es maladies hématologiques ou hémopathies sontdes affections caractérisées par une atteinte deséléments figurés du sang. Par extension, on y
incorpore les troubles de l'hémostase dus à une anoma-lie vasculaire et les tumeurs constituées par certainséléments figurés présents dans le sang (lymphomes)(Samson et coll., 1999).Ces maladies hématologiques sont à l'origine de mani-festations buccales et parodontales différentes selonl'étiologie, dues aussi bien à la maladie primaire qu'auxeffets secondaires des thérapeutiques mises en œuvre.Elles peuvent être groupées en quatre grands syndromes :les désordres leucocytaires non prolifératifs comme laneutropénie, les syndromes anémiques, les syndromesprolifératifs telle que la leucémie et les troubles de l'hé-mostase qui peuvent aussi être à l'origine de manifes-tations parodontales représentées essentiellement pardes gingivorragies (Szpirglas et Benslama, 1999 ;Szpirglas et Lacoste, 1994).L'établissement d'un diagnostic précoce d'une hémopa-thie sur l'observation de signes buccaux et parodontauxdevient de plus en plus rare car la maladie est rapide-me nt confirmée par les exa me ns de labora t o i re.Cependant ces hémopathies, étant donnée leur prise encharge multidisciplinaire, nécessitent de la part du chi-rurgien dentiste d'adopter une attitude particulière tantdu point de vue prophylactique que thérapeutique.
Les désordres leucocytaires non prolifératifs peu-vent être classés sur le plan quantitatif en terme d'in-suffisance (leucopénie) ou d'excès (leucocytose) et surle plan qualitatif en terme d'anomalie fonctionnelle(Roche 1996). La neutropénie, désordre leucocytaire leplus fréquemment rencontré, correspond à une diminu-tion des polynucléaires neutrophiles (PN) au-dessous de1800/mm3. On parle d'agranulocytose quand ce chiffreest < 500/mm3. La neutropénie peut être d'originegénétique comme la neutropénie familiale et cyclique,ou acquise rencontrée en cas de leucémie, d'insuffisan-ce médullaire, d'agranulocytose pure et s'observe surtoutcomme une complication de la chimiothérapie antimito-tique (Szpirglas et Lacoste, 1994 ; Sebahoun 1999).
Pour exercer leur fonction protectrice, les poly-nucléaires neutrophiles (PN) exercent plusieurs actions :chimiotaxie, phagocytose et destruction de l'antigène.
H ematologic diseases or hemopathies are disor-ders characterized by an impairment of diffe-rent blood constituents. In a wider sense we
include those hemostatic disorders resulting from vascu-lar abnormalities and tumors brought on by the presenceof certain elements in the blood (lymphomas) (Samsonet al., 1999).These hematologic diseases are the source of variousoral and periodontal manifestations depending on theetiology; either the sequels of the actual disease or thetherapeutic side effects. Grouped within the realms offour main hemopathic syndromes: non-proliferativewhite blood cell disorders like neutropenia, anemicconditions, proliferative disorders like leukemia, andhemostatic disorders : their periodontal manifestationsare most notabely gingivorrhagies (Szpirglas andBenslama, 1999 ; Spriglas and Lacoste, 1994). Nowadays, as blood diseases are precociously confir-med by laboratory analysis, it is rare to initially diagno-se haemopathies based on oral and periodontal manifes-tations. However, because of the multidisciplinary treat-ment of these hemopathies, the dental surgeon is requi-red to adopt an approach that is both prophylactic andtherapeutic.
Non-proliferative white blood cell disorders canbe quantitatively classified in terms of deficiencies (leu-copenia) or excesses (leucocytosis) and qualitatively interms of functional abnormalities (Roche 1996).Neutropenia, the most common leucocytic disorder, cor-responds to a decrease in polynuclear neutrophiles (PN)to less than 1800 / mm3. The term agranulocytosis isused when this figure is < 500 / mm3. Neutropenias canbe genetically acquired, as familial benign or periodicneutropenia, or acquired as in the case of leukemia,medullary insufficiency, and agranulocytosis, notablyobserved as a complication of antimitotic chemotherapy(Szpirglas and Lacoste,1994 ; Sebahoun 1999).
To exert their defensive role, the polynuclearneutrophiles (PN) act in several ways : by chemotaxis,phagocytosis, and destruction of the antigen. Individuals
Désordres leucocytairesnon prolifératifs
Non-proliferative whiteblodd cell disorders
Manifestations parodontales Periodontal manifestations

301
Les personnes présentant des déficiences quantitatives(neutropénie ou agranulocytose) et qualitatives (chi-miotactique ou phagocytaire) des PN présentent unedestruction sévère des tissus parodontaux (Kinane1999). Les défauts qualitatifs sont souvent associés àune destruction localisée affectant uniquement le paro-donte de certaines dents, alors que les déficiencesquantitatives (neutropénie) s’accompagnent générale-ment d'une destruction du parodonte de toutes lesdents (parodontite associée à la neutropénie) (Wiltonet coll., 1988).
La sévérité des manifestations parodontales estdirectement reliée à la sévérité de la neutropénie. Dansles formes les plus malignes, il existe une gingiviteulcéro-nécrotique (GUN) qui se manifeste par une ulcé-ration et une nécrose au niveau de la gencive margina-le, en plus d’un saignement (Roche 1996 ; Samson etcoll., 1999 ; Atkinson et coll., 2000). Dans la neutro-pénie cyclique qui est une affection assez rare, leslésions sont fréquemment sévères avec des poches paro-dontales profondes et une perte osseuse étendue, géné-ralisée atteignant la denture permanente. Parfois, larésorption osseuse peut être observée en denture lac-téale (Kinane 1999 ; Pindburg 1995).
En cas de neutropénie sévère (<500 PN/mm3),seuls les soins urgents et indispensables seront réalisésen milieu hospitalier.
En cas de neutropénie modérée (500 à 1000/mm3), une antibioprophylaxie sera prescrite avanttoute intervention. L’évolution de la maladie parodon-tale et des traitements réalisés est à surveiller réguliè-rement.
Lors des prescriptions, il faut éviter les médica-ments responsables d'agranulocytose comme les pyrazo-lés (ex : noramidopyrine), les sulfamides et les nitro-5-imidazolés (Girard et coll., 1997).
Les soins comme les surfaçages et la chirurgieparodontale, seront reportés jusqu'à ce que le patientsoit pris en charge sur un plan médical et que son sta-tut clinique soit satisfaisant (Roche 1996).
D'un point de vue prophylactique, un suivi pro-fessionnel régulier peut prévenir l'atteinte parodontale.Un mauvais contrôle de plaque aboutit à une patholo-gie parodontale. L'élimination de la plaque bactérienneet un bain de bouche au gluconate de chlorhexidine à0.2 % durant la neutropénie aide à maintenir la santéparodontale (Pernu et coll., 1996).
presenting with quantitative PN deficiencies (neutrope-nia or agranulocytosis) as well as with qualitative defi-ciencies (chemotactic or phagocytotic) suffer from seve-re periodontal tissue breakdown (Kinane 1999).Qualitative deficiencies are often accompanied by alocalized lesion affecting only the periodontium of cer-tain teeth, while the quantitative deficiencies (neutrope-nia) are often associated with the generalized destruc-tion of the periodontium (periodontitis associated withneutropenia) (Wilton et al., 1988).
The severity of the periodontal disease is directlyrelated to the severity of the neutropenia. In its mostmalignant forms, we may observe an acute ulceronecro-tic gingivitis (ANUG) with its clinical symptoms ofulceration, necrosis, and bleeding at the level of the freegingival margin (Roche 1996; Samson et al., 1999;Atkinson et al., 2000). In the case of periodic neutrope-nia, a rare disorder, the defects are frequently severe,associated with deep periodontal pockets and extensivegeneralized bone loss. Sometimes, bone resorption caneven be observed in the primary dentition (Kinane 1999;Pinburg 1995).
In the case of severe neutropenia (< 500 PN /mm3), only the most essential and urgent treatment willbe implemented, and this in a hospital environment.
In the case of moderate neutropenia (500 to1000/mm3), an appropriate antibiotic prophylaxis willbe administered prior to all dental interventions. Thetreatment protocol and the evolution of the periodontaldisease must be controlled regularly.
Any form of medication leading to agranulocyto-sis, such as pyrazoles (ex: noramidopyrine), sulphadrugs, and nitro-5-imidazoles should not be prescribed(Girard et al.; 1997).
Scaling and periodontal surgery shall be postpo-ned until the patient has been stabilised medically bytheir caring physicians and present a satisfactory clinicalstatus (Roche 1996).
From a prophylactic point of view, regular com-prehensive recalls can aid in preventing periodontalinvolvement. Poor plaque control will lead to periodon-titis. The elimination of bacterial plaque and the use of a0.2 % chlorhexidine gluconate mouthwash during theperiod of neutropenia helps to maintain periodontalhealth (Pernu et al., 1996).
Revue d’Odonto-Stomatologie /novembre 2002
Prise en charge Patient management

302Revue d’Odonto-Stomatologie /novembre 2002
PARODONTIE
L ' h é mostase est l'ensemble des phéno m è ne sphysiologiques qui concourent à l'arrêt du saignement,à la prévention des saignements spontanés et desthromboses. On peut reconnaître un trouble de l'hémos-tase avec les hémorragies gingivales.
L'hémostase primaire est l'ensemble des phéno-mènes qui aboutissent à la formation du clou plaquet-taire et à l'arrêt du saignement (Girard et coll., 1997).La thrombopénie correspond à un abaissement du nom-bre des plaquettes au-dessous de 150.000/mm3, alorsque la thrombopathie est une anomalie qualitative(Szpirglas et Benslama, 1999). Des anomalies comme lathrombasthénie de Glanzmann associe à la fois défautsqualitatifs et quantitatifs des plaquettes (Kantarci etcoll., 1996).
La thrombopénie peut être (Roche 1996) :• d'origine centrale (médullaire) par insuffisance ou
aplasie médullaire comme dans le cas de leucémie etmétastases de cancer,
• d'origine périphérique par excès de destruction pla-quettaire [coagulation intra-vasculaire disséminée(CIVD), allergie,…] ou au cours d'infections bacté-riennes et virales ou de causes médicamenteuses outoxiques.
La cause la plus fréquente de la thrombopathieest due à certaines médications comme celles conte-nant de l'acide acétylsalicylique, de la ticlopidine etd'autres anti-inflammatoires non stéroïdiens.
Les troubles de l'hémostase primaire peuvent semanifester par des pétéchies qui correspondent à destaches hémorragiques de surface.
(Szpirglas et Benslama, 1999 ; Dridi et coll., 1998)
D'autres syndromes hémorragiques comme lesgingivorragies spontanées sont dus aux troubles de lacoagulation. Ces troubles peuvent intéresser les 3temps de la coagulation :
The physiological phenomena which acts to stopbleeding and to prevent spontaneous bleeding andthrombosis is called hemostasia. Haemostasia disorderscan often be revealed by the clinical manifestation ofgingival bleeding.
The phenomena by which the formation of ablood clot arrests bleeding is called primary hemostasia(Girard et al., 1997). Thrombopenia corresponds to areduction in the number of platelets, a value below150.000 / mm3, while a thrombopathy is a qualitativeabnormality Szpirglas and Benslama, 1999).Abnormalities such as Glanzmann's thrombasthenia ischaracterised by both qualitative and quantitative plate-let defects (Kantarci et al.,1996).
Thrombopenia results from (Roche 1996): • central nervous system (medullary) aberrances,
medullary aplasia or deficiency as in the case of leu-kemia and metastatic cancer,
• peripheral aberrances resulting from excess plateletdestruction [ disseminated intra-vascular coagulation(DIVC), allergy,…] either during bacterial and viralinfections or due to medicamentous or toxic causes.
A thrombopathy is most frequently a side effectof certain medications such as those containing acetyl-salicylic acids, ticlopidine and other nonsteroidal anti-inflammatory agents.
The visible signs of primary haemostasis disor-ders can be petechiae (haemorrhagic surface spots).
(Szpirglas and Benslama, 1999 ; Dridi et al., 1998)
Other hemorrhagic syndromes such as sponta-neous gingivorrhagies are due to coagulation disorders.These may concern various levels of the 3 coagulationstages :
Troublesde l’hémostase
Hemostatic disorders
■ Troubles de l’hémostaseprimaire (thrombopénie,thrombopathie)
■ Primary hemostasiadisorders (thrombopenia,thrombopathy
■ Anomalies de la coagulation ■ Coagulation abnormalities

303
- la formation de la prothrombine par les voies extrin-sèque et intrinsèque,
- la formation de la thrombine,- et la formation de la fibrine.
• Les plus fréquentes de ces anomalies sont les troublesacquis médicamenteux par traitement avitaminique Kou héparinique. Le test utilisé dans ce contexte estl'INR (International normalized ratio ou test interna-tional normalisé). Son dosage est plus fiable par rap-port au taux de prothrombine (TP) appelé aussi tempsde Quick (TQ) dont les résultats sont variables d'unlaboratoire à un autre. L'INR correspond au rapport TQmalade/TQ témoin multiplié par un indice de sensibi-lité international (ISI) propre à chaque lot de lathromboplastine tissulaire. Un INR = 1 est l'équiva-lent d'un TP à 100%, l'INR augmente lorsque le TPbaisse. Un INR>2 [(TP) < 40%] comporte un risquehémorragique.
• Les hémophilies sont des maladies constitutionnelleshéréditaires récessives liées à l'X. Le plus souvent, ils'agit d'un déficit en facteur VIII, anti-hémophiliqueA, moins souvent du facteur IX, anti-hémophilique B.Il existe un allongement du temps global de coagula-tion et du temps de céphaline activé (TCA). La mani-festation orale la plus fréquente est un saignementépisodique, prolongé, qui peut être spontané ou trau-matique (Rose et Steinberg, 1998).
• La maladie de Willebrand est un trouble de l'hémos-tase qui est assez fréquent et qui associe un allonge-ment du temps de saignement (TS) au déficit en fac -teur anti-hémophilique A ou facteur VIII (par absen-ce d'adhésivité des plaquettes). Cliniquement, cettema l a d ie associe un purpura ecchy motique de smuqueuses buccales, surtout des gingivorragies spon-tanées, une certaine prédilection pour des hémorra-gies amygdaliennes et un risque hémorragique en casd'intervention comparable à celui des hémophiles.
Des tests simples de dépistage permettent l'ex-ploration de l'hémostase lors du bilan préopératoire. Untemps de saignement et une numération de plaquettesdans les normes permettent d'exclure toute anomalie del'hémostase primaire. En cas d'allongement du TS sansthrombopénie, le patient doit être dirigé vers un héma-tologue car des tests plus spécialisés comme le test d'ag-glutination des plaquettes (agrégométrie) seront néces-saires pour établir le diagnostic de thrombopathie.
- the formation of prothrombin by the extrinsic andintrinsic pathways,
- the formation of thrombine,- and the formation of fibrin .
• The most frequent abnormalities are side effects fromvitamin K or heparin medication. The test used to eva-luate the blood clotting cascade is the INR(International Normalized Ratio). Its dosage is morereliable with regard to the rate of prothrombine (alsoknown as Quick Time (QT)) for which the results varyfrom one laboratory to another. THE INR correspondsto the relationship between the QT patient / QTcontrol multiplied by the International SensitivityIndex (ISI) specific to each lot of tissue thromboplas-tin. An INR = 1 is equivalent to a PTof 100%, the INRincreases when the PT decreases. An INR>2 [(PT) <40%] indicates a hemorrhagic risk.
• Hemophilia is a reccesive hereditary disease linked tothe blood coagulation factor X. Most often it is rela-ted to a deficiency in factor VIII, anti-hemophilic A,and more rarely with the factor IX, anti-hemophilic B.Both the global coagulation time and the cephalineactivation time are prolonged. The most frequent oralsign is an occasional prolonged bleeding, which canbe either spontaneous or traumatic in origin (Rose andSteinberg, 1998).
• Willebrand’s disease is a rather frequent hemostasisdisorder which is associated with a prolonged blee-ding time (BT) due to a deficiency in the anti-hemo-philic A factor or factor VIII (by absence of plateletadhesion). Clinically, this affliction is associated withan ecchymotic purpura of the oral mucosa, noteablyspontaneous gingival bleeding, a certain tendency(prediliction) for bleeding of the tonsils and a hemor-rhagic risk in the case of surgery similar to that ofhemophiliacs.
As part of the preoperatory assessment, simplediagnostic tests are needed to understand the extent ofthe hemopathy. Primary hemostasis abnormalities canbe excluded by using bleeding time tests and standardplatelet counts. If the patient does not suffer from throm-bopenia but has a prolonged bleeding time, he shouldconsult a hematologist as more specialized tests will benecessary such as platelet agglutination tests (agregome-try) in order to diagnosis of type of thrombopathy.
Revue d’Odonto-Stomatologie /novembre 2002
Prise en charge Patient management

304Revue d’Odonto-Stomatologie /novembre 2002
PARODONTIE
Le TP ou mieux l'INR (tests des voies extrinsèqueet commune de la coagulation évaluant le complexeprothrombique : II, V, VII, X), le TCA (test des voiesintrinsèque et commune de la coagulation) et le dosa-ge du fibrinogène permettent l'exploration globale de lacoagulation. Un allongement isolé du TCA n'est pasobligatoirement associé à un risque hémorragique : ledéficit en facteur XII est totalement asymptomatiquemême s'il est sévère (Gaussem et Aiach, 1996). Seul undiagnostic précis de l'anomalie permet d'évaluer lerisque chirurgical de l'hémorragie. Les tests de dépis-tage des anomalies de l'hémostase primaire et de lacoagulation sont représentés dans le tableau suivant(Lesclous et Maman, 1993) :
An in-depth examination of the patient’s coagu-lation can be evaluated using the prothrombine time, oreven better, the INR ( tests concerning both the extrinsicand common coagulation pathways ,assessing the pro-thrombic complex: II, V,VII , X), and the time of cepha-line activation ( tests concerning both the intrinsic andcommon coagulation pathways) and the dosage of thefibrinogen. An isolated prolongation of the cephalineactivation time is not necessarily associated with ahemorrhagic risk: the deficiency in factor XII is totallyasymptomatic even if it is severe (Gaussem and Aiach,1996). The surgical risk of hemorrhage can only be esti-mated by a precise diagnosis of the coagulation abnor-mality. The tests to detect of abnormalities in primaryhaemostasis and coagulation are shown in the followingtable (Lesclous and Maman, 1993) :
Numération plaquettaire Temps de saignement INR Temps de Céphaline ActivéPlatelet count Bleeding time INR Écart de plus de 10 sec
150-400.000mm3 4-8 mn/10 mn* <1/ >2* par rapport au témoin* /100.000 mm3* More than 10 sec divergence
compared with the control*
ThrombopéniesThrombopenia ➚ N N
ThrombopathiesThrombopathies N ou ➚ N N
WillebrandWillebrand N N N ou “
Hémophilie A- BHemophilia A-B N N N
Déficit en facteursFactor deficiencies N NII, V, VII, X
Déficit en facteursFactor deficiencies N N NXI, XII
AfibrinogénémieAfibronogenemia N
* : valeurs à partir desquelles existe un risque hémorragique / values beyond which indicate a hemorrhagic riskN : valeur normale / normal value
Troubles de l'hémostase primaire
• En cas de thrombopénie sévère < 50.000/mm3, ou encas de thrombopathie, les interventions chirurgicalesnon urgentes sont différées jusqu'à normalisation dela fonction plaquettaire. Si le patient présente desgingivorragies, le brossage gingival doit être res-treint. Pour diminuer l'inflammation, des bains debouche à base d'antiseptiques seront prescrits. Enurgence, les soins sanglants seront réalisés aprèstransfusion plaquettaire.
Primary hemostasis disorders
• In the case of severe thrombopenia < 50,000 / mm3, orin the case of thrombopathy, all nonurgent surgicalinterventions are postponed until platelet functionreturns to normal. If the patient exhibits gingivorra-gies, gingival brushing must be restricted. To decrea-se inflammation, antiseptic mouthwashes are prescri-bed. For emergency care, all treatments incurring ableeding risk should be preceded by a platelet transfu-sion.

305Revue d’Odonto-Stomatologie /novembre 2002
• Les patients présentant une thrombopénie modérée(numération plaquettaire comprise entre 50.000 et100.000 cellules/mm3 ) avec un temps de saignementlégèrement prolongé, ne pourront recevoir que lessoins qui ne sont pas susceptibles d'induire un sai-gnement. Tous les autres soins nécessiteront une cor-rection préalable du temps de saignement grâce à latransfusion plaquettaire. Pour des soins simples, lecontrôle de saignement se fera grâce à l'usage destechniques d'hémostase locale à savoir les panse-ments compressifs résorbables, les colles chirurgica-les, les gouttières thermoformées et les sutures (lenombre de points ne doit pas être excessif pour limi-ter les points sanglants). Ils seront réalisés de préfé-rence avec un fil non résorbable, plus solide et plusrésistant qu'un fil résorbable et pouvant être mainte-nu en place pendant plusieurs jours (Dridi et coll.,2000). Dans tous les cas, une alimentation semi-liquide sera recommandée au patient pour limitertout traumatisme du caillot sanguin.
Lors des pre s c r i p t io ns, toute théra p e u t i q u emo d i f ia nt la fo nc t ion plaquettaire est à pro s c r i recomme les anti-inflammatoires non stéroïdiens (AINS)(Roche 1996 ; Girard et coll., 1997). En cas de traite-ment anti-agrégant plaquettaire, il y a potentialisationavec les salicylés et AINS qu'il est préférable d'éviter.
Patients sous anticoagulants(Roche 1996 ; Girard et coll., 1997 ;Pernu et coll., 1996)
Pour les patients sous anticoagulants (antivita-mines K (AVK) ou héparine) comme les patients atteintsde valvulopathies, les traitements ne doivent pas êtreinterrompus ou modifiés. L'efficacité du traitementanticoagulant par AVK est régulièrement suivie par lamesure de l'INR qui est souvent maintenu dans une zonethérapeutique de 2 à 3.• Avec un INR < 2 et les moyens d'hémostase locale que
le chirurgien dentiste doit posséder et maîtriser, ledétartrage-surfaçage et les extractions dentaires sim-ples peuvent être réalisés sans risque hémorragiquetrop important.
En pratique : pour les patients dont l'INR est habi-tuellement maintenu proche de 2 et en cas d'actessanglants mais simples (détartrage-surfaçage, extrac-tions simples ou en nombre limité, endodontie) ilfaut demander un INR pour le matin du jour de l'acteafin de vérifier sa valeur. Si sa valeur est < 2, l'actepeut être réalisé. Sinon, il est ajourné.
• Patients presenting with a moderate thrombopenia(compromised platelet count between 50,000 and100,000 cells / mm3) with a slightly prolonged blee-ding time, must not receive any treatment risking toinduce bleeding. All other treatment will require a pre-liminary platelet transfusion to regularize the bleedingtime. For simple interventions, control of the bleedingis accomplished by local hemostatic techniques, suchas resorbing compressive bandages, surgical glues,heatformed splints, and sutures (keeping their numberto a minimum to avoid points of bleeding). Moreresistant, non-resorbing sutures are chosen and mayremain in place for several days (Dridi et al., 2000). Inall cases, a semi-liquid diet is recommended to avoidblood clot trauma.
All medication such as nonsteroidal anti-inflam-matory drugs NSAIDs (Roche 1996; Girard et al., 1997)is contraindicated. Anticoagulant therapeutics are syner-giste with salycylates and NSAIDs, and therefore to beavoided as well.
Patients ReceivingAnticoagulation Therapy(Roche 1996 ; Girard et al., 1997 ;Pernu et al., 1996)
Patients undergoing anticoagulant treatments(antivitamin K (AVK) or herparin) as well as thosepatients suffering from heart valve pathologies shouldnot have their pharmaceutical treatments interrupted ormodified during their dental treatment. Regular INR rea-dings are obtained to evaluate the effectiveness of AVKanticoagulant therapy. The INR readings are often main-tained in the therapeutic zone of 2 to 3.• For an IRN < 2 , scaling, root planing, and extractions
may be performed without significant risk of bleedingby employing local hemostatic techniques.
Clinically : For patients whose INR is generally main-tained around 2 and in the case of simple but never-theless bleeding inducing procedures (scaling,rootplaning, simple extractions and/or limited in number,endodontics) an INR reading must be obtained themorning of the procedure. A value < 2 is acceptable,otherwise the appointment is postponed.

306Revue d’Odonto-Stomatologie /novembre 2002
PARODONTIE
• Pour les patients dont l'INR doit être maintenu > 2pour des raisons médicales, si l'acte thérapeutique estévalué comme pouvant entraîner un risque hémorra-gique, l'intervention doit être réalisée en milieuhospitalier avec au besoin un relais héparinique.
Pour le relais héparinique, la calciparine® estgénéralement utilisée. C’est un sel de calcium de l'hé-parine injecté par voies sous cutanées. L'héparinémiesurvient en 30-60 min et disparaît après une durée de8 à 14 heures. Une deuxième injection a lieu générale-ment 12 heures après la première. Dès que l'INR est bienstabilisé sur un allongement correct, le médecin trai-tant peut supprimer les AVK qui avaient été maintenusjusque là en couverture. Il est alors possible d'interve-nir dans cette fenêtre thérapeutique.
Pour cela, il suffit d'opérer à la fin de la périoded'action de la dernière injection de calciparine®. Lesinjections pourront être reprises quelques heures aprèsl'intervention, en fonction de l'importance de celle-ci etselon l'appréciation du praticien. Au cas où une hémor-ragie se déclarerait lors de la reprise de l'héparinothé-rapie, une injection de sulfate de protamine (1ml/1000UI d'héparine) permet de re s t a u rer l'hémo s t a s e(Pelissier et Alantar, 1990).
En cas de traitement anticoagulant (AVK), il y a :• potentialisation avec les salicylés et anti-inflamma-
toires non stéroïdiens ;• antagonisme avec les barbituriques, les anti-histami-
niques et le méprobamate ( sédatif) ;• aggravation du risque hémorragique avec les corticoï-
des à forte dose.
Il est souhaitable de ne pas utiliser ces médica-ments lors de la prescription.
Déficience d'un facteur de lacoagulation (hémophilie, Willebrand)
Chez l'hémophile, l'atteinte de la voie intrin-sèque faisant appel aux facteurs anti-hémophiliques està l'origine d'un INR (TP) normal et d'un TCA augmenté.Toute intervention présentant un risque hémorragique,qu'elle soit parodontale, endodontique ou chirurgicale,devra être précédée d'un contact avec l'hématologue etd ' exa me ns biologiques (Gira rd et coll., 1997).L'hémophilie est sévère lorsque le taux du facteur VIIIou IX est <1% par rapport au taux normal. Entre 1% et5%, l'hémophilie est modérée. Entre 6% et 30%, elle estmineure. Une valeur > 30 % correspond à l'hémophiliefruste caractérisée par une hémostase normale.
• Those patients needing to maintain an IRN < 2 due tospecific medical conditions, need to be treated in ahospital setting under heparin administration for anyprocedures risking to induce bleeding.
Subcutaneous injections of calciparine‚ a cal-cium salt of heparin, is used in these cases. The hepari-nemia appears in 30-60 minutes and disappears after 8 to14 hours. A second injection follows 12 hours after theinitial injection. As soon as the INR is stabilised, thetreating physicien can stop the AVK treatment.
During this therapeutic period it is possible toperform the necessary interventions, operating after thelast calciparine‚ injection. These injections may becontinued several hours following the surgery in relationto the involvement of the surgery and in accordance withthe practitioner’s judgement. In case of a hemorrhageduring the heparin therapy, an injection of protaminesulfate (1ml/1000 IU heparin) enables the restoration ofhemostasis (Pelissier and Alantar, 1990).
In the case of anticoagulant therapy (AVK), thereexists the :• potentialisation with salicylates and NSAIDs ;• antagonisme with barbituates, antihistamines, and
meprobamate (sedative) ;• increase in the risk of bleeding with high doses of cor-
ticoids.
These medications are consequently contraindi-cated.
Coagulation Factor Deficiencies(hemophilia, Willebrand’s Disease)
The hemophiliac has a normal INR and an increa-sed ACT due to the fact that the coagulation factordependant intrinsic pathway is affected. All interventions(periodontal, endodontic, or surgical), incurring a risk ofbleeding must be preceded by a consultation with ahematologist and the proper blood tests. (Girard andcoll., 1997). A hemophilia is considered severe when thelevel of factor VII or IX is < 1% in relation to the normallevel. Values between 1% and 5% indicate a moderatehemophilia whereas values between 6% and 30% indica-te a minor affliction. A minor Hemophilia has a valueof > 30% and is associated with a normal hemostasis.

307
Après approbation du médecin traitant, les soinsavec certaines précautions seront envisagés. Toutes lesp ro c é du res à l'orig i ne d'un saig ne me nt (avulsio ns,détartrage, mise en place de la digue, mise en place dematrices, etc.) peuvent être envisagées, mais avec uneextrême précaution et avec compensation du facteurdéficient. Ceci ne dispense pas de l'utilisation des tech-niques locales d'hémostase précédemment décrites.
Les anesthésies tronculaires sont contre-indi-quées car elles peuvent non seulement être à l'origined'un saignement mais aussi d'un hématome pouvantobstruer les voies aériennes. L'anesthésie strictementlocale peut être réalisée chez le patient hémophile carelle ne nécessite pas de compensation du facteur défi-cient lorsque cette déficience est légère ou modérée(entre 1% et 30%).
En post-opératoire, des antibiotiques per os sontprescrits ainsi que des antifibrinolytiques comme l'aci-de aminocaproïque, l'acide tranexamique assurant uneprotection du caillot. Des agents hémostatiques commela desmopressine ou l'étamsylate peuvent être béné-fiques dans la prévention du saignement dans le cas dela maladie de Von Willebrand et les formes modérées del'hémophilie. En solution, ces hémostatiques peuventêtre utilisés par voie générale, en bain de bouche oupour imprégner une compresse pour la compression d'unsite hémorragique.
Cependant, la desmopressine est sans efficacitéchez les patients présentant une hémophilie ou unWillebrand sévère. La voie intrinsèque de la coagula-tion étant atteinte, il existe un risque de saignementtardif. Les bains de bouche seront donc proscrits (Girardet coll., 1997 ; Roche 1996 ; Kantarci et coll., 1996 ;Dridi et coll., 2000).
Les anémies sont définies par la diminution dutaux d'hémoglobine en dessous de 13 g/dl chez l'hom-me adulte, 12 g/dl chez la femme adulte.
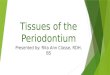
Un seul symptôme est habituellement commun àtoutes les anémies, c'est la pâleur des muqueuses(fig. 1) ; les autres signes stomatologiques doiventêtre mentionnés pour chaque type d'anémie (Szpirglaset Lacoste, 1994 ; Trachli et coll., 2000).
With the approval of the treating physician, den-tal treatment may be carried out. All procedures whichmay involve bleeding (extractions, scalings, placing ofthe rubber dam, fitting of matrices, etc.) can be foreseen,but with extreme precaution and with compensation ofthe deficient factor. Use of local hemostatic techniques,as previously mentioned, is recommended.
Troncular anesthesia is contraindicated as theymay induce not only bleeding, but also a hematomawhich could obstruct the air passages. A strictly localanesthesia can be administered to a hemophilic patientas a replacement of the missing factor is not necessarywhen the deficit is determined to be only minor ormoderate.
Postoperatory antibiotics per-os are prescribedalong with antifibrinolytic medication such as aminoca-proic acid and tranexamic acid to protect against bloodclots. Hemostatic agents such as desmopressine andetamsylate can be beneficial in the prevention of blee-ding in patients affected by Von Willebrand’s Diseaseand moderate forms of hemophilia. These hemostaticagents may be orally administered by means of amouthwash or by compressing an impregnated cottongauge over the site of bleeding.
However, the desmopressine is inefffective forhemophilic patients and those suffering from severecases of Willebrand's Disease. As their intrinsic path-ways are affected, there exists a risk of a delayed onsetof bleeding. Hemostatic mouthwashes are thus proscri-bed (Girard et al., 1997 ; Roche 1996; Kantarci et al.,1996 ; Dridi et al., 2000).
Anemias are characterized by the reduced levelof hemoglobin to below 13g/dl in adult males and 12g/dlin adult females.
Pale mucosa is the one most common symptomsamongst the various types of anemias (fig. 1). Other oralsigns must be mentioned for each different form of ane-mia (Szpirglas and Lacoste, 1994 ; Trachli et al., 2000).
Revue d’Odonto-Stomatologie /novembre 2002
Syndrômes anémiques Anemic syndromes
Manifestations parodontales Periodontal manifestations

308Revue d’Odonto-Stomatologie /novembre 2002
PARODONTIE
• L'anémie ferriprive ou sidéropénique est marquée parl'atrophie des muqueuses. Elle peut être due à des sai-gnements chroniques ou à une carence d'apport(Quessar et Benchekroun, 2000).
• L'anémie de Fanconi fait partie d'un tableau pancyto-pénique (diminution du nombre des trois lignées san-guines : plaquettes, globules rouges, globules blancs)qui aboutit vers l'âge de 10 ans à une aplasie médul-laire. C'est une maladie constitutionnelle qui compor-te des anomalies osseuses, des malformations rénaleset cardiaques, une grande fréquence des leucémies etde cancer. Sur le plan buccal, on peut noter des dys-chromies et une alvéolyse diffuse entraînant des mal-positions par migrations secondaires puis l'expulsiondes dents (Szpirglas et Benslama, 1999).
• Les thalassémies sont des désordres génétiques carac-térisés par une diminution de la synthèse d'une deschaînes de globine. Sur le plan buccal, elles sontcaractérisées par un accroissement important desmaxillaires à l'origine d'une béance et une déficiencede l'occlusion labiale, de malocclusion, et d'uneinflammation gingivale. Une raréfaction de l'os alvéo-laire avec trabéculation en barreaux d'échelle estaussi observée (Roche 1996).
• La drépanocytose est une hémoglobinopathie défor-mant les globules rouges. Fragiles et rigides, ils obs-truent les petits vaisseaux et la triade symptomatiqueassocie anémie à l'origine d'une gencive pâle, crisesdouloureuses vaso-occlusives et infections parfoismortelles.
L'acte chirurgical peut favoriser en postopératoi-re, dans le cas d'une anémie sévère (Hg<8g/dl), unallongement du temps de saignement et un retard decicatrisation. Une surveillance de la cicatrisation estalors nécessaire (Girard et coll., 1997).
• Sideropenic or iron deficient anemia is characterisedby the atrophy of the mucosa. It may be due to chro-nic bleeding or a nutritional deficiency (Quessar andBenchekroun, 2000).
• Fanconi’s Anemia results from a reduction in the threeblood forms: platelets, erythrocytes, and leucocytesthat leads to a medularry aplasia around 10 years ofage. This constitutional affliction is accompanied bybone abnormalities, renal and cardiac malformations,and frequently leukemias and cancer. At the oral level,we note dischromies and a diffuse alveololysis cau-sing dental malpositions from secondary migrations,followed by tooth loss (Szpirglas and Benslama,1999).
• Thalassemias are a heterogenous group of hereditaryhemolytic anemias which have in common a decrea-sed rate of synthesis of one or more hemoglobin poly-peptide chains. A substantial developement of the den-tal arcades is observed, which is responsible for gapsand a lack of lingual occlusion, occlusal disharmonies,and gingival inflammation. A rarefaction of the alveo-lar bone with ladder step-like trabeculations is obser-ved as well.
• Drepanocytemia or sickle cell anemia is a hemoglobi-nopathy resulting from deformed red blood cells. Stiffand fragile, these deformed erythrocytes obstructsmall blood vessels. The triad of symptoms is palegingiva, painful vaso-obstructive episodes, and infec-tions…some of which can be fatal.
In the case of a severe anemia (Hg < 8g/dl), apostoperatory prolonged bleeding time and healing per-iod is favored. Consequently, a close surveillance duringthe healing period is necessary (Girard et al., 1997).
Fig. 1 : Gencive pâle chez une patienteatteinte d'une anémie par carence de fer.
Pale mucosa in a patient suffering from irondeficient anemia.
1
Prise en charge Patient management

309
• Les actes à l'origine d'un saignement seront reportéspour qu'ils aient lieu dans les conditions optimales desécurité. Un taux d'hémoglobine de 10 g/dl est consi-déré comme un gage de sécurité pour les soins. Encas d'intervention indispensable chez un anémiquesévère et après un bilan d'hémostase (numération dela formule sanguine (NFS), temps de saignement (TS),plaquettes, INR, TCA), les actes selon leur nature etleur sévérité, seront réalisés en accord avec le méde-cin traitant et en prenant en considération les tech-niques locales de l'hémostase (Roche 1996).
• Chez le patient présentant une drépanocytose, uneantibioprophylaxie sera préconisée lors d'actes chirur-gicaux ou susceptibles d'être à l'origine d'infection.Toute infection d'origine bactérienne, en particulierdu tissu osseux sera traitée par une antibiothérapieadéquate pour prévenir tout risque d'ostéomyélite(Roche 1996).
C'est un syndrome myéloprolifératif caractérisépar une augmentation du nombre des globules rouges.On parle également de polyglobulie primitive. La causeest inconnue.
Comme pour toutes les polyglobulies, la muqueu-se est rouge violacée, œdématiée. Parfois, la maladie deVaquez se manifeste au niveau de la muqueuse par despétéchies, des ulcérations et de fréquentes gingivorra-gies parfois d'apparition spontanée. Ces manifestationssont la traduction des complications de la maladie duesà des thromboses ou à des troubles de l'hémostase(Girard et coll., 1997 ; Samson et coll., 1999).
Les manifestations buccales secondaires au trai-tement qui peuvent être des saignées (évacuation d'unecertaine quantité de sang) ou une chimiothérapie, fragi-lisent la muqueuse buccale (Aubert et Guittard, 1995).
Deux risques sont à connaître au cours de toutechirurgie : l'hémorragie et la thrombose par hypervisco-sité. Donc, un bilan d'hémostase, une NFS et un héma-
• All intervention which may result in bleeding shouldbe postponed, until optimal operating conditions arereached. A 10g/dl level of hemoglobin is consideredthe level of security to allow treatment. In the eventof an intervention on a severe anemic patient a bloodexam including blood count, bleeding time, platelets,INR, and ACT is requested. These acts are performedin cooperation with the treating physician and accor-ding to the nature and servereness the hemostasisaffliction, local hemostatic techniques may be calledfor. (Roche 1996).
• A patient suffering from drepanocyytemia requires anantibiotic prophylaxis prior to all surgical proceduresor treatments for afflictions that are of infective origin.All infections of bacterial origin, an in particular thatconcerning osseous tissue, should be treated by anadequate antibiotic therapy to avoid the risk of osteo-myelitis. (Roche 1996).
This is a myeloproliferative syndrome, characte-rized by an increase in the number of red blood cells. Itis also referred to as a (primitive polyglobuly). The rea-son is unknown.
As seen in all polyglobulies, the mucosa is violetred and oedemic. Sometimes Vaquez’s Disease hasmucosal manifestations such as petechiea, ulcerationsand frequent gingival bleeding, sometimes spontaneous.These manifestations are complications of thrombosesor hemostatic problems (Girard et coll.,1997 ; Samson etal., 1999).
Secondary oral manifestation as a result of (sai-gnees imposed bleeding) evacuation of a certain quanti-ty of blood or chemotherapy weakens the buccal muco-sa (Aubert and Guittard, 1995).
During any surgery one must be aware of twomajor risks: hemorrhage and thrombosis from hypervis-cosity. Thus, a coagulogram, an NFS and a hematocrite
Revue d’Odonto-Stomatologie /novembre 2002
Syndrômes prolifératifs
■ Maladie de Vaquez
Proliferative syndromes
■ Vaquez’s disease
Manifestations parodontales Periodontal manifestation
Prise en charge Patient management

310Revue d’Odonto-Stomatologie /novembre 2002
PARODONTIE
tocrite sont indispensables avant toute intervention.Lors des prescriptions, les antifibrinolytiques (acideaminocaproïque, acide tranexamique), sont à proscrirecar ils peuvent entraîner des thromboses (Girard etcoll., 1997).
Les leucémies sont des proliférations malignesdes tissus hématopoïétiques. Elles sont dues à des ano-malies chromosomiques ou à des irradiations et exposi-tion à certains composés chimiques. Les formes familia-les sont rares. Les leucémies sont classifiées selon leursmanifestations cliniques en forme aiguë ou chronique etselon leurs caractéristiques cytologiques en leucémieslymphoïdes et myéloïdes (Girard et coll., 1997). Le myé-logramme permet de mettre en évidence l'envahisse-ment du tissu médullaire par une grande quantité deleucoblastes. L'analyse cytologique permet de préciserle type cellulaire : lymphoblastique ou myéloblastique.
Les manifestations parodontales sont fonctionde l'état général du patient.
• Avant une prise en charge médicale, il s'agit essen-tiellement d'accroissement gingival, d'infections etd'ulcérations des muqueuses. Dans les formes aiguësprécoces, on retrouve des infections récurrentes, desgingivorragies et pétéchies, et un accroissement gin-gival observé chez 30 % des patients présentant uneleucémie myéloïde aiguë (Roche 1996 ; Khattab2002) (fig. 2-3). La tuméfaction gingivale due à l’in-filtration par les cellules leucémiques est générale-ment un signe de la leucémie myéloïde aiguë, maiselle est aussi évoquée dans d’autres formes notam-ment la leucémie lymphocytaire chronique (fig.4). Lesaignement gingival est associé à la thrombocytopé-nie (Le Breton 1997 ; Kinane 1999 ; Bimstein et coll.,2001). Sur le plan radiographique, des images clairesavec perte de la lamina dura et érosions des crêtesalvéolaires sont observées (Roche 1996).
• Ces manifestations évoluent avec la maladie. Ellessont aggravées par la chimiothérapie et la radiothé-rapie qui sont à l'origine d'une atrophie des muqueu-ses, d'une inflammation et d'une mucosite. De plus,l'usage de la chimiothérapie et de la radiothérapie està l'origine d'une immunodépression qui potentialiseles processus infectieux bactériens, et d'hémorragieslocales (sulculaires, gingivales, etc.) (Roche 1996 ;Campan et coll. 1999).
are necessary prior to all surgical interventions.Antifibrinolytic amino caproic acid and tranexamicacid are proscribed as they can cause thromboses(Girard et al., 1997).
Leukemias are malignant proliferations of hema-topoietic tissue due to chromosomal abnormalities,radiation, or contact with certain chemicals. Hereditaryforms are rare. Leukemias are classified according totheir clinical manifestations as either acute or chronicand for lymphoid and myeloid leukemias according totheir cytological characteristics (Girard et al., 1997). Amyelogram reveals the invasion of the medullary tissueby a large number of leucoblasts. The cytological ana-lysis enables the precision of the cell type : lymphoblas-tic or myeloblastic.
The periodontal manifestations are related to thepatient’s general state of health.
• Before being treated medically, the patient presentsessentially with gingival inflammation and growth,infections and ulcerations of the mucosa. In the earlyacute forms, we observe recurrent infections, gingivalbleeding, and petechiae, and gingival enlargement in30 % of patients presenting with an acute myeloge-nous leukemia (Roche 1996 ; Khattab 2002) (fig. 2-3).The gingivale tumefaction due to the infiltration bythe leukemic cells is often a sign of an acute myelo-genous leukemia, but is also observed in other forms,noteably in chronic lymphocytic leukemia (fig. 4).Gingival bleeding is associated with thrombocytope-nia (Le Breton 1997; Kinane 1999; Bimstein et al.,2001). Radiographically, the alveolar crests exhibitradiolucent images with a loss of the lamina dura anderosions (Roche 1996).
• These manifestations evolve with the disease and areaggravated by chemotherapy and radiotherapy whichcause atrophy of the mucosa, inflammation, and amucositis. In addition, chemotherapy and radiothera-py are responsible for an immunodepression thatpotentializes infectious bacterial processes and localhemorrages (sulcula, gingival, etc.) (Roche 1996 ;Campan et al., 1999).
■ Leucémies ■ Leukemias
Manifestations parodontales Periodontal manifestation

311
Deux risques dominent : le risque hémorragiqueet le risque infectieux. L'accord de l'hématologue estessentiel avant tout soin et une antibioprophylaxie estnécessaire avant tout acte chirurgical.
En phase aiguë de la maladieou au cours de la phase aplasiantede la chimiothérapie
La numération fait apparaître une aplasie sévère(moins de 1500 leucocytes/mm3, moins de 40.000 pla-quettes/mm3). Il ne faut pas intervenir généralement,et ne prescrire qu'une antibiothérapie massive à viséesymptomatique. En cas d’urgence qui semble noncontrôlable par les antibiotiques (abcès collecté, cellu-lites), l'éradication des foyers sera réalisée sous cou-verture antibiotique en milieu hospitalier (transfusionplaquettaire, légère alvéolectomie pour une fermeturecorrecte de la plaie, suture résorbable, gouttière com-pressive, …). Durant cette période d'aplasie profonde,on tentera de maintenir une hygiène minimale mais sys-tématique :
Two risks predominate: bleeding and infection.The hematologist’s consent is essential before all treat-ment and an antibiotic prophylaxis is necessary prior toall surgical interventions.
During the acute stageof the illness or during theaplaisante stage of chemotherapy
The blood count shows a severe aplaisie (lessthan 1500 leucocytes/mm3, less than 40,000 plate-lets/mm3). Generally, it is recommended not to interve-ne and only to prescribe massive antibiotic treatmentaimed at the symptomatology. In emergency caseswhich are deemed not controllable by antibiotics (col-lected abcess, cellulites) the eradication of the sourcewill be accomplished through antibiotic coverage in ahospital setting (platelet transfusion, minor alveolecto-my to allow the proper closing of the wound, resorbingsutures, compressive splint,…). During this period ofprofound aplasia, an attempt to maintain a systematicalthough minimally correct oral hygiene :
Revue d’Odonto-Stomatologie /novembre 2002
Fig. 2, 3 : Infiltration brutale de la gencive par les cellules tumorales chez une fille âgée de 13 ans atteinte d'une leucémiemyéloïde aiguë. Elle associe accroissement gingival et pétéchies.
Aggressive gingival infiltration by leukemics cells seen in a 13 year old girl. Gingival hyperplasia and petechiae are present.
2 3
Prise en charge Patient management
Fig. 4 : Accroissement gingival chez un enfant atteintde leucémie lymphoblastique chronique.
Gingival hyperplasia seen in a young boy with chroniclymphoblastic leukemia.
4

312Revue d’Odonto-Stomatologie /novembre 2002
PARODONTIE
• Bains de bouche antiseptique et antifongique : alter-nance de digluconate de chlorhexidine et d'un mélan-ge de bicarbonate et d'amphotéricine B (Marie etcoll., 1984) ;
• irrigation fréquente des lésions ulcéreuses au sérumphysiologique. Lorsque ces lésions sont trop doulou-reuses, une application de gel de xylocaïne visqueusepermettra une sédation temporaire (Marie et coll.,1984) ;
• un brossage dentaire prudent avec une brosse à denttrès souple provoque chez les patients motivés etayant subi une mise en état buccale préalable unléger saignement, mais évite les gingivorragies spon-tanées qui sont dues à la présence de plaque et detartre (Guichard et Planchand, 1999). Seules des dou-leurs aiguës ou des hémorragies spontanées peuventindiquer son interruption (Borowski 2002) ;
• lorsque l'état de la bouche est trop mauvais pour per-mettre le brossage, un écouvillonnage soigneux àl'eau oxygénée à 10 volumes des collets et des espa-ces interdentaires, assurent un minimum d'hygiène etde confort (Marie et coll., 1984).
En phase de rémission
Après contact avec le médecin traitant, des soinsdentaires peuvent être réalisés, ainsi que le traitementdes foyers infectieux (Girard et coll., 1997). En effet,entre les cures de chimiothérapie, les patients bénéfi-cient de périodes de rémission, au cours desquelles leurformule sanguine redevient quasiment normale, les met-tant ainsi à l'abri des infections graves et des hémorra-gies.
Il peut exister une toxicité cumulative qui faitque les éléments sanguins ne retrouvent pas leur niveaud'avant les différentes cures. Un nombre de polynu-cléaires supérieur à environ 1.500/mm3 et un nombrede plaquettes qui dépasse 50.000/mm3 autorisent lessoins dentaires. Par conséquent, le praticien peut etdoit, à ce moment, effectuer une mise en état aussicomplète de la bouche, mais à condition que ces soinssoient terminés suffisamment longtemps (à peu prèsune semaine) avant le début d'une nouvelle cure, afinde permettre une cicatrisation correcte lors de la futu-re mise en aplasie médullaire. Au cours de ces périodes,la couverture antibiotique des interventions n'est pasobligatoire. Elle dépendra, d'une part de l'atteinte neu-tropénique (±1500 PN/mm3 ), d'autre part de l'impor-tance de l'intervention prévue (Borowski 2002 ; Marie etcoll., 1984 ; Rutkauskas 2000).
• Antiseptic and antifongal mouthwashes: alternatingbetween chlorhexidine gluconate and a mixture ofamphotercin B and bicarbonate (Marie et al., 1984) ;
• Frequent irrigation of ulcerations with saline solution.When these lesions are too painful, temporary reliefmay be obtained by applying a viscous xylocaine gel(Marie et al., 1984) ;
• Careful tooth brushing with an extra-soft toothbrushmay evoke light bleeding in patients following certaintreatments, but will help to avoid spontaneous gingi-val bleeding due to the presence of dental plaque andcalculus (Guichard and Planchand, 1999). Only in thecase of acute pain or spontaneous bleeding is it indic-ted to interrupt this home care (Borowski 2002) ;
• When the oral condition is judged too poor to allowbrushing, careful wiping with a swab soaked withhydrogen peroxide (10%) along the free gingival mar-gins and interproximally will assure a minimumhygiene and comfort (Marie et al., 1984).
Phase of Remission
After the approval of the treating physicians,dental care can be started, as well as the treatment of theinfectious sources (Girard et al., 1997). Between ses-sions of chemotherapy, patients benefit from periods ofremission during which their blood count returns toalmost normal, protecting them from severe infectionsand hemorrages.
A cumulative toxicity may exist explaining whythe blood elements do not return to their pre-cure values.Polynuclear values beyond 1,500/mm3 and plateletnumbers exceeding 50,000 mm3 are favourable for den-tal care. Consequently, the dentist may and must reha-bilitate the patient as thoroughly as possible, but assu-ring to terminate these treatments around one weekbefore the start of another session of chemotherapy inorder to allow the time for healing before creating by thechemotherapy a new state of medullary aplasia. Duringthese periods, antibiotic coverage for interventions is notnecessary, but depends upon the neutropenic attack (+/-1500 PN/mm3) and the involvement of the foreseenintervention (Borowski 2002; Marie et al., 1984;Rutkauskas 2000).

313
Les prescriptions doivent se faire après avis del'hématologue car de nombreuses interactions médica-menteuses sont à redouter avec les antimitotiques.L'activité du méthotrexate est diminuée avec la péni-cilline, la kanamycine (aminoside) et les corticoïdes, etaugmentée avec les salicylates et les tétracyclines(Girard et coll., 1997). Le malade doit profiter de lapériode de rémission pour acquérir une hygiène dentai-re et buccale rigoureuse. L'emploi d'une brosse très sou-ple s'impose. Le praticien doit en outre recommanderl'utilisation du fil de soie, le massage des gencives àl'aide de gels gingivaux, des bains de bouche à based'antiseptiques fréquents (Marie et coll., 1984).
Les lymphomes sont des tumeurs malignes qui sedéveloppent au sein des tissus lymphoïdes (ganglionspar exemple) et qui diffusent à distance vers les autrestissus lymphoïdes (moelle osseuse, foie,…). Ils com-prennent la maladie de Hodgkin, les lymphomes nonhodgkiniens et le lymphome de Burkitt (Roche 1996).
Le myélome multiple ou maladie de Kahler estune prolifération maligne des plasmocytes qui sécrètenten règle une immunoglobuline monoclonale. Il s’accom-pagne le plus souvent de lésions osseuses avec hyper-calcémie et peut occasionner une insuffisance rénale.
Maladie de Hodgkin(Roche 1996 ; Girard et coll., 1997)
La maladie de Hodgkin est un lymphome carac-térisé par la présence dans les organes atteints de cel-lules réticulaires dystrophiques. Chez un sujet jeune,Les adénopathies cervicales prédominent dans le tableauclinique. On peut observer des tumeurs de la cavité buc-cale (amygdales, gencives) sous forme de nodules fermes.On peut aussi observer une ostéolyse diffuse ou uneostéo-condensation possibles.
Lymphomes non Hodgkiniens
Ils représentent un groupe hétérogène de proli-férations lymphoïdes. Ils sont deux fois plus fréquentsque les lymphomes Hodgkiniens et leur fréquence aug-mente avec l'âge (Roche 1996).
Prescriptions are given after consulting the trea-ting hematologist as interactions with the prescribedantimitotic agents are probable. Methotrexate’s activityis diminished by penicillin, kanamycin, and corticoids.Its activities are augmented by salicyclates and tetracy-clines (Girard et al., 1997). The patient needs to takeadvantage of the period of remission to obtain a rigorousoral hygiene. An extra soft toothbrush is highly recom-mended and the practitioner should recommend the useof dental floss, gingival massages with gingival gels,and frequent antiseptic mouthrinses (Marie et al., 1984).
Lymphomas are malignant tumors which developin lymphoid tissue (ganglions for example) and whichdiffuse towards other lymphoid tissues (bone marrow,l i v e r, …). They include Hodgkin’s Disease, non-Hodgkin’s lymphomas and Burkitt’s lymphoma (Roche1996).
Multiple myeloma or Kahler’s disease is a mal-ignant proliferation of plasmocytes which secretemonoclonal immunoglobulines. It is often seen alongwith bone lesions from hypercalcemia and kidney defi-ciency.
Hodgkin’s Disease(Roche 1996 ; Girard et al., 1997)
Hodgkin’s Disease is a lymphoma characterizedby the presence of dystrophic reticular cells in the affec-ted organs. In young patients, cervical adenopathiespredominate. Tumors of the oral cavity (tonsils, gingi-val) appear as firm nodules. Diffuse steolysis orcondensing osteitis may also be observed.
Non-Hodgkin lymphomas
They consist of a heterogenic group of lymphoidproliferations. Their occurrence increases with age, andare encountered twice as frequently (Roche 1996).
■ Lymphomes etmyélome multiple
Manifestations parodontales Periodontal manifestations
■ Lymphomas and multiplemyelomas
Revue d’Odonto-Stomatologie /novembre 2002

314Revue d’Odonto-Stomatologie /novembre 2002
PARODONTIE
Les lymphomes malins non hodgkiniens sont desproliférations plasmocytaires monoclonales malignesdéveloppées à partir des cellules des organes lymphoï-des secondaires. L'étiologie reste inconnue mais desfacteurs secondaires peuvent jouer un rôle très impor-t a nt comme l'immu no d é p re s s ion (Berberi et coll.,2000).
Sur le plan bucco-maxillo-facial, les lymphomesmalins non hodgkiniens ont deux traductions cliniques :une adénopathie cervico-faciale, ou une tumeur dupalais dur ou de la gencive, qui se traduit par une tumé-faction lisse, tendue, ferme, non douloureuse et d'allu-re inflammatoire. Le diagnostic différentiel est à établiravec le carcinome épidermoïde (Szpirglas et Benslama,1999) (fig.5).
Lymphome de Burkitt
Il résulte d'une prolifération des cellules B quisemble être associée à une infection par le virusd'Epstein Barr.
Les manifestations observées dans le cadre dulymphome de Burkitt sont représentées par des dépla-cements dentaires, une expansion de la corticale et unedéformation faciale (Roche 1996).
La phase de début siège dans la majorité des casau niveau prémolaire et molaire supérieures sous laforme de petits foyers intra-osseux radioclairs autourdes dents. L'évolution de cette tumeur de consistanceferme se fait vers le plancher de l'orbite, envahissant lesparties molles, avec un développement intrabuccal infil-trant le rebord alvéolaire et comblant le vestibule(Girard et coll., 1997).
Lymphomas are malignant monoclonal plasmo-cytotic proliferations which develop from secondarylymphoid organs. Their etiology remains uncertain, butsecondary factors such as a state of immunodepressionmay play an important role (Berberi et al ., 2000).
Clinically, malignant Non-Hodgkin Lymphomashave two consequences : a cervico-facial adenopathy, ora tumor of the hard palate or gingiva, which presents asa smooth,firm,distended but painless tumefaction withan inflammatory appearance. The differential diagnosisis to be made between an epidermoid carcinoma(Szpirglas and Benslama, 1999) (fig. 5).
Burkitt’s Lymphoma
This lymphoma results from the proliferation ofB cells which appear to be associated with an infectionby the Epstein -Barr virus.
Clinical manifestations of Burkitt’s Lymphomainclude migration of the dentition, cortical expansion,and facial deformation (Roche 1996).
In the majority of cases, the site of its inital phaseis the maxillary premolar and molar regions. Smallradiolucent intra -osseous lesions surrounding theseteeth are observed. This firm consistent tumor evolves inthe direction of the base of the orbit, invading the softregions, with an intraoral expansion infiltrating thealveolar borders and filling the vestibule (Girard et al.,1997).
Fig. 5 : Tumeur au niveau de la gencive etdu palais : manifestation d'un lymphomenon-Hodgkinien.
Palatal and gingival tumor associated witha Non- Hodgkin lymphoma.
5

315Revue d’Odonto-Stomatologie /novembre 2002
Pour tous les lymphomes, d'autres manifesta-tions cliniques sont liées aux effets de la chimiothéra-pie et de la radiothérapie. L'arsenal chimiothérapiqueagit par interférence avec le métabolisme des cellulestumorales. Ce métabolisme est différent de celui descellules normales, mais l'activité antimitotique ne s'ex-prime pas de façon exclusive et spécifique sur les cellu-les tumorales. Elle agit également sur les cellules sainesde l'organisme, en particulier celles à indice mitotiqueélevé (follicules pileux, cellules hématopoïétiques, épi-thélium buccal). Ces complications buccales sont ainside deux types :
• les unes résultant de l'effet direct sur la sphère buc-cale des agents utilisés (mucite, xérostomie, etc) ;
• les autres indirectes, par les conséquences au niveaude la cavité buccale d'une toxicité générale (infec-tions secondaires à la leucopénie et à l'immunodé-presssion, saignements buccaux secondaires à lat h ro m b o c y t o p é n ie) (Roche 1996 ; Guic h a rd etPlanchand, 1999).
Myélome multiple(Samson et coll., 1999 ; Roche 1996)
Contrairement au cas rare de plasmocytome soli-taire où le foyer osseux est rarement unique, le myélo-me multiple est caractérisé par plusieurs lésions osseu-ses localisées. Ces lésions sont présentes au sein desmaxillaires, dans la région des apex des molaires man-dibulaires (mimant des lésions périapicales) et auniveau de la branche montante et de l'angle mandibu-laires. Elles peuvent se développer et former des lésionstumorales nodulaires par envahissement des tissusmous. Ce sont les plasmocytomes extra-médullaires quipeuvent affecter les gencives réalisant une hypertrophielisse ou bourgeonnante localisée ou diffuse.
Avec l'évolution de la maladie, des résorptionsradiculaires, des mobilités dentaires sont observées. Aun stade avancé, des fractures pathologiques au niveaudes maxillaires, des gingivorragies et des pétéchies(d’origine thrombocytopénique) se manifestent. Onnote aussi une susceptibilité à l'infection et un saigne-ment excessif liés à la chimiothérapie.
La thrombocytopénie ainsi que les interférencesentre les immunoglobulines et les facteurs de la coagu-lation, associées aux lymphomes et au myélome multi-
In regards to all lymphomas, other clinical mani-festations are linked to the effects of chemotherapy andradiation therapy. The chemotherapeutic armamenta-rium acts by interfering with the tumor cell’s metabo-lism. Although this metabolism is already different fromthat of normal cells, the antimitotic therapeutic action isnot specifically limited to the tumer cells and thusaffects healthy cells as well, in particular those with highmitotic indexes (hair follicules, hematopoetic tissue,oral epithelium. There are 2 types of oral complicationsassociated with this therapy :
• those arising as a direct result of the agent (mucositis,xerostomia) ;
• those indirectly resulting from the patient’s generalstate of toxicity (secondary infections resulting fromthe leucopenia and immunodepression, secondary oralhemmorrage due to the thrombocytopenia) (Roche1996 ; Guichard and Planchand, 1999).
Multiple Myeloma(Samson et al., 1999 ; Roche 1996)
Contrary to the rare cases of SolitaryPlasmacytoma whose boney source is rarely the same, amultiple myeloma is characterised by numerous locali-zed osseous lesions.These lesions are seen in the maxil-la, apical regions of mandibular molars (imitating peria-pical lesions at the level of the ascending branch andangle of the mandibule). These lesions may develop andform nodular tumorous lesions by involvement of thesoft tissue. Extramedullary plasmocytomas may effectthe gingiva, evoking a smooth, localised budding, or dif-fuse hypertrophy.
As the disease evolves, root resorption and den-tal mobility is observed. At the advanced stage, patholo-gical fractures of the maxilla, gingivorrhagies, andthrombocytopenic provoqued petechiae may be obser-ved. A susceptibility to infection and excessive bleedingresulting from chemotherapy is seen as well.
Thrombocytopenia as well as interferences bet-ween immunoglobins and coagulation factors, associa-ted with lymphomas and multiple myelomas contribute
Prise en charge Patient management

316Revue d’Odonto-Stomatologie /novembre 2002
PARODONTIE
ple, contribuent à des désordres de la coagulation et del'hémostase exposant le patient à des complicationshémorragiques. Ces dernières sont aggravées par l'ané-mie associée à ces affections et par les effets de la chi-miothérapie et de la corticothérapie (les corticoïdespeuvent être à l'origine d'un purpura vasculaire en rap-port avec une fragilité capillaire) (Aubert et Guittard,1995). Ainsi toute situation favorisant un saignement(brossage inapproprié traumatique, affections parodon-tales préexistantes, dents fracturées ou mobiles, etc.)sera à corriger.
Il faut prévenir le risque hémorragique potentiel,en demandant une numération de la formule sanguine(NFS), une numération des plaquettes, l'INR et le TCAainsi que l’avis de l’hématologue. Les techniques loca-les d'hémostase (compression, sutures soigneuses etserrées, applications topiques d'agents hémostatiqueslocaux résorbables, application de colle biologique,etc.) doivent être utilisées. Dans le cas de manifesta-tions plus conséquentes, le médecin traitant seraconsulté et une transfusion plaquettaire pourra éven-tuellement être envisagée (Roche 1996).
Une antibioprophylaxie est indispensable lorsdes interventions chirurgicales chez les patients souschimiothérapie ou corticothérapie. Cette dernière justi-fie une antibioprophylaxie en raison de son effet immu-nosupresseur (inhibition de la multiplication des lym-phocytes) et de son action inhibitrice sur les fibroblas-tes (phase de réparation tissulaire).
Lors des prescriptions, il faut proscrire toutethérapeutique à toxicité hématologique (anti-inflam-matoires, sulfamides). La conduite à tenir chez lepatient sous chimiothérapie anticancéreuse est iden-tique à celle d'un leucémique.
Le granulome éosinophile (GE) de l'os, la maladiede Hand-Schüller-Christian et la maladie de Letterer-Siwe ont été regroupés sous le nom d'histiocytose X ourécemment, d'histiocytose à cellules de Langerhans.Leur dénominateur commun est le développement delésions granulomateuses avec une prolifération histio-cytaire (Pernu et coll., 1996). Les histiocytoses X asso-cient une prolifération de cellules histiocytaires (cellu-les phagocytaires) spumeuses d’allure bénigne à uneréaction éosinophile (Girard et coll., 1997).
to coagulation and hemostatic disorders exposing thepatient to the risk of hemorrhagic complications.Aggravated by chemotherapy and corticoid therapeuticassociated anemias (corticoids may cause a vascularpurpura from capillary fragility)(Aubert and Guittard,1995) Therefore, all conditions or behaviors which pro-mote bleeding (traumatic tooth brushing, periodontalafflictions, fractured or mobile teeth).
The risk of bleeding must be assessed from theblood count (TBC), platelet count, and the INR andTCA. The advise of the hematologist is to be obtained aswell. Local hemostatic techniques ( compression, meti-culous and tight sutures, topical hemostatic agents,application of biological glue, etc.) are employed. Incases of more severe manifestations, the treating physi-cian needs to be consulted, and a platelet transfusion caneventually be foreseen (Roche 1996).
An antibiotic prophylaxis is necessary prior tosurgical interventions for patients undergoing chemothe-rapy or corticotherapy. Premedication is justified in thislatter case as it causes immunosupression (by inhibitingthe multiplication of lymphocytes) and has an inhibitinginfluence on fibroblasts (phase of tissue healing).
When prescribing for these patients, all medicationhindering the hematologic system (anti-inflammatories,sulfamides) are to be avoided. The treatment approach fora patient undergoing anticancerous chemotherapy is thesame as for a patient suffering from leukaemia.
An eosinophilic granuloma (EG) of the bone,Hand-Schüller-Christian disease and Letterer-Siwe dis-ease are classified as an hytiocytosis X, or more recent-ly as a Langerhan’s cell histicytosis. Their commonmorphologic characterisitic is a granulomatous infiltra-tion with a histiocytic proliferation ( Pernu et al 1996).Histiocytosis X is associated with a proliferation of eosi-nophilic histiocytic cells (phagocytotic cells) with abenign appearance. (Girard et al., 1997).
■ Les histiocytoses Xou histiocytosesLangerhansiennes
■ Histiocytosis X orLangerhan’s histiocytosis

317Revue d’Odonto-Stomatologie /novembre 2002
• Le granulome éosinophile, ainsi nommé en raisond'une importante infiltration de polynucléaires éosi-nophiles au sein de la prolifération histiocytaire,représente la forme localisée et la moins sévère, de latriade d'histiocytoses Langerhansiennes. L'étiologiede la maladie reste en grande partie inconnue(Ünlü et coll., 1997).
Au niveau du crâne, le granulome éosinophiles'accompagne d'une lacune osseuse de découverte sou-vent fortuite (fig. 6).
Au niveau buccal, les manifestations de cettemaladie concernent (Szpirglas et Benslama, 1999) :
- une incidence maxillo-faciale (10 % de tous les GE),la mandibule est trois fois plus atteinte que le maxil-laire ;
- une tuméfaction douloureuse de la gencive bordant lalésion à évolution rapide ;
- une mobilité des dents adjacentes aux lésions osseu-ses avec conservation de la vitalité pulpaire ;
- des signes radiologiques : on note une ostéolyse plusou moins étendue avec des foyers d’ostéolyse uniquesou multiples de forme ronde et contours nets feston-nés et légèrement sclérosés. L'image en panier, au-dessus de laquelle la dent semble être suspenduereste l'un des éléments différentiels (Favre-D’Auvergneet coll., 1995 ; Pasler 1994) (fig.7) ;
The eosinophilic granuloma, named as such dueto the extensive infiltration of polynuclear eosinophilesin the midst of a histiocytic proliferation, represents alocalized, less severe form of the Langerhan’sHistiocytotic triad. The disease’s etiology remains forthe most part unknown (Ünlü et al., 1997).
At the cranial level, the eosinophilic granulomais accompanied by a lake of bone (fig. 6).
Oral manifestations may include (Szpirglas andBenslama, 1999):
- a maxillo-facial involvement (10% of all EGs), themandibule is concerned three times more frequentlythan the maxilla ;
- a rapidly evolving painful tumefaction of the free gin-gival margin ;
- a mobility of the teeth which conserve their vitality ;- radiographic signs: we observe a more or less extensi-
ve osteolysis with single or multiple round osteolyticsites which are clearly demarcated, scalopped, andslightly sclerosed. The basket-shaped image abovewhich the tooth seems to be suspended remains one ofits differential elements (Favre-Auvergne et al., Pasler1994) (fig.7) ;
Manifestations parodontales Periodontal manifestations
Fig. 6 : Cas d'histiocytose X : lacune osseuse au niveau du crâne.
Lacuna of cranial bone.
Fig. 7 : Image rétro-alvéolaire montrant une lyse osseuse de formearrondie au niveau de la 36.
Round osteolytic radiographic image of a first mandibular molar.
Les figures 6, 7, 8 et 9 représentent le même cas d’histiocytose X.
6,7,8, and 9 figures show illustrate the same case of histiocytotic X.
6 7

318Revue d’Odonto-Stomatologie /novembre 2002
PARODONTIE
- chez l'enfant, des ulcérations gingivales, œdèmes etdouleurs accompagnent les éruptions dentaires ainsiqu'une lyse alvéolaire (parodontale et péri-apicale) etune résorption radiculaire.
Le diagnostic est histologique après biopsie deslésions osseuses réalisée par un praticien spécialisé.L'examen anatomo-pathologique montre une proliféra-tion tumorale dense, constituée de cellules histiocytai-res. Les cellules tumorales sont pourvues d'un cytoplas-me abondant, légèrement éosinophile et d'un noyauvolumineux, irrégulier et parfois encoché (Ennibi etcoll., 1998) (fig. 8-9).
• Le syndrome de Hand-Schüller-Christian associe, chezl’adulte jeune ou le grand enfant, des lacunes osseu-ses (granulomes éosinophiles), une exophtalmie et und iabète ins i p ide par lésion post-hy p o p hy s a i re(Szpirglas et Benslama, 1999).En plus des manifestations du granulome éosinophile,on distingue des lésions gingivales plus fréquentes(inflammation, nécrose et récession) (Girard et coll.,1997).
• La maladie de Letterer-Siwe atteint le nourrisson etcomporte des adénopathies cervicales, une dermato-se diffuse, des infections sur lésions osseuses spéci-fiques (mastoïdites), des lésions pulmonaires et sou-vent, parfois isolément au début, des lésions osseu-ses maxillaires avec envahissement gingival diffus etexpulsion des germes dentaires temporaires et desfo l l icules des de nts perma ne ntes (Szpirglas etBenslama, 1994).
- in children, gingival ulcerations, painful oedemasaccompany dental eruptions and we find an alveolysis(periodontal and periapical), and root resorption.
The diagnosis is based upon the histology of theosseous lesions, following a biopsy performed by a spe-cialist. The anatomicopathological exam shows a densetumerous proliferation, consisting of histiocytic cells.The tumor cells contain a significant quantity of slightlyeosinophilic cytoplasm and a voluminous, irregular, andsometimes notched nuclei (Ennibi et al., 1998)(fig. 8-9).
• Hand-Schuller-Christian Disease is associated withosseous lacunas (eosinophilic granulomas), exopthal-mia, and insipid diabetes from post-hypophisic lesionsin young adults and older children (Szpirglas andBenslama, 1999).In addition to the manifestation of an eosinophilic gra-nuloma, we observe more frequent gingival lesions(inflammation, necrosis, and recession) (Girard et al.,1997).
• Letterer-Siwe Disease affects newborns and exhibitscervical adenopathies, diffuse dermatitis, infection ofspecific boney lesions (mastoiditis), pulmonarylesions and often, sometimes initially isolated oss-seous lesions of the maxilla with diffuse gingivalinvolvement and an expulsion of the primary dentalgerms and permanent dental follicules (Szpirglas andBenslama, 1994).
Fig. 8 : Coupe histologique x 100 HE montrant de nombreusescellules histiocytaires, avec un cytoplasme abondant, un noyaupolylobé et incurvé (laboratoire de l'Institut National d'Oncologiede Rabat).
Histiocytic cells with abondant cytoplasm and curved multilobu -lar nuclei :histologic vue X 100 HE.
Fig. 9 : Marquage net des cellules histiocytaires en rouge-brun auchromogène DAB avec la protéine S-100.
Histiocytic cells clearly marked in brownish-red by " chromogeneDAB and S-100 protein ".
8 9

319Revue d’Odonto-Stomatologie /novembre 2002
Après bilan radiographique panoramique et rétro-alvéolaire et demande de biopsie des lésions osseusespour diagnostic histologique, une approche multidisci-plinaire du traitement s'impose. Elle consiste en uneexérèse chirurgicale et éventuellement une chimiothéra-pie et corticothérapie en cas de lésions multiples.
Le curetage chirurgical des lésions constitue engénéral un traitement efficace du granulome éosinophi-le du tissu osseux, les corticostéroïdes pourraient êtreutilisés comme adjuvants surtout en cas de lésions mul-tiples. La posologie sera déterminée par le médecin trai-tant qui peut poser l'indication d'une chimiothérapie.
Les lésions consécutives au GE apparaissent àdes intervalles irréguliers, ce qui peut causer des pro-blèmes d'ordre diagnostique et retarder le début du trai-tement. Se pose aussi le problème d'une récidive. D'oùl'intérêt des examens cliniques suivis.
After panoramic and peri-apical radiographicexamination and a biopsy of the boney lesions allowingan histological examination, a multi-disciplinary treat-ment approach is necessary, consisting of a surgicalexcision and in the case of multiple lesions, chemothe-rapy, and corticotherapy.
The surgical curretage of the eosinophilic granu-lomatous lesion is an effective treatment; corticosteroidsmay be used additionally, especially in the case of mul-tiple lesion. The dose is determined by the treating phy-sician who may recommend chemotherapy.
Recurrent EG lesions appear in irregular inter-vals which may cause problems in diagnosing the illnessand delay the onset of treatment. As resistant cases pre-sent a problem, follow-up clinical exams are of greatinterest.
Prise en charge(Girard et coll., 1997 ; Ünlü et coll., 1997)
ConclusionLe rôle du chirurgien dentiste dans le dépistage de certaines formes des hémopathies est important. Les
manifestations buccales et parodontales peuvent constituer un signe d'appel ou d'orientation et faire recon-naître un syndrome neutropénique avec les ulcérations, thrombopénique avec les hémorragies, anémique avecla pâleur et prolifératif avec les hyperplasies gingivales. Cependant, ces manifestations n'ont aucun caractèrepathognomonique et doivent être replacées dans leur contexte biologique à partir d'un diagnostic de laboratoi-re. Devant une hémopathie connue, des précautions devront être prises vis à vis du risque infectieux et du risquehémorragique que peuvent présenter ces maladies hématologiques.
The role of the dentist in the detection of certain forms of hemopathies is crucial. The oral manifesta-tions may constitute a warning sign indicating: a neutropenia with ulcerations, bleeding accompanied anemicthrombopenia with paleness, and proliferative diseases with hyperplastic gingiva. However, these manifesta-tions have no particular pathognomic characteristic, and only through a laboratory diagnosis may wet apprecia-te their biological context. In face of a known hemopathy, these hematological afflictions may present withbleeding and infectious risk for which certain precautions must be taken.
Demande de tirés-à-part : Docteur Amal BOUZIANE - 12, rue Oued Zemn n°4 - 10 000 - Rabat.
RemerciementsNos remerciements au Dr Otmani Naïma de l'hôpital d'enfant de Rabat pour sa collaboration.
Patient management(Girard et al., 1997 ; Ünlü et al., 1997)
Traduction : Docteur Jane MATKOSKI

320Revue d’Odonto-Stomatologie /novembre 2002
PARODONTIE
320
ATKINSON J.C., O’CONNELL A., AFRAMIAN D.Oral manifestations of primary immunological diseases. J.Amer dent Ass 2000;131:345-356.
AUBERT F., GUITTARD P.L’essentiel Médical de Poche. H é m a t o l o g i e . E d .Marketing/Ellipses, Paris 1995;350-419
BERBERI A., KHAIRALLAH S., ELSAHILI N.Les lymphomes non hodgkiniens associés à une infectionau VIH : à propos de deux cas. R e v. O d o n t .S t o m a t.2000;29(1):23-27.
BIMSTEIN E., NEEDLEMAN H.L., KARIMBUX N.VAN DYKE T.E.Periodontal and gingival health and diseases.Ed:Martin-dunitz, London 2001;31-48.
BOROWSKI B.Soins dentaires et chimiothérapie aplasiantes : conseils pra-tiques. Chir Dent France 2002;1065:43-46.
CAMPAN P., GINESTE L., GUICHARD M.Que peut cacher une banale hypertrophie gingivale ? Rev.Odont.Stomat. 1999;28(3):157-163.
DRIDI S.M., WIERZBAC.B., MEYER J., PELLAT B.Syndromes hémorragiques : intérêt clinique des tests biolo -giques. Rev. Odonto.Stomat. 1998;27(3):165-177.
DRIDI S.M., ARRETO C.D., DANAN M.Chirurgie et hémostase. Réalités clin 2000;11(2):225-283.
ENNIBI O., BENRACHADI L., HAMDANI S., AMRANIM., BENZARTI N.A propos d’un cas d’histiocytose X maxillaire. Actualitésodont stomat 1998;203:379-387.
FAVRE-D’AUVERGNE E., GUILBERT F., AURIOL M.,LE CHARPENTIER Y.Tumeurs et pseudo-tumeurs non odontogéniques bénignesdes maxillaires. Encycl.Méd. Chir., Stomatologie-odonto-logie, 22-062-H-10, 1995, 8p.
GAUSSEM P., AIACH M.Exploration de l’hémostase en biologie clinique. Actualitésodont stomat 1996;193:71-77.
GUICHARD M., PLANCHAND P.O.Conduite à tenir chez le patient sous chimiothérapie anti-cancéreuse. Cah Ass dent franc. 1999;4:10-17.
KANTARCI A., CEBECI I., FIRATLI E., ATAMER T.,TUNCER Ö.Periodontal management of Glanzmann’s thrombasthenia :report of 3 cases. J Periodontol 1996;67:816-820.
KHATTAB M.Leucémies aiguës de l’enfant. Espérance méd2002;9(80):74-79.
KINANE D.F.Periodontitis modified by systemic factors. A n nPeriodontol 1999;4(1):54-63.
LE BRETON G.Traité de sémiologie et clinique odonto-stomatologique. Ed.CdP, Paris 1997.
LESCLOUS PH., MAMAN L.L’hémostase : exploration et conduite à tenir en odontolo-gie.Chir dent France 1993;646:49-53.
MARIE J.P., BOUTER A., FISHER J.M.Lésions bucco-dentaires et hémopathies malignes.Actualités odonto stomat 1984;146:217-231.
PASLER F.A.Atlas de médecine dentaire : radiologie. Ed. Flammarion,Paris 1994.
GIRARD P., JEANDOT J., QUEVAUVILLIERS J., PER-LEMUTER L. Dictionnaire médical du chirurgien dentiste. Ed Masson,Paris 1997.
PELISSIER A., ALANTAR S.A.Les antivitamines K: mode d’action, indications, principesde traitement, rôle de l’odontologiste. Actualités odont sto-mat 1990;169:
PERNU H.U., PAJARI U.H., LANNING M.The importance of regular dental treatment in patients withcyclic neutropenia. J periodontol 1996;67:454-459.
PINDBURG J.J.Atlas des maladies de la muqueuse buccale. Ed. Masson,Paris 1995.
QUESSARA., BENCHEKROUN S.L’anémie par carence martiale. Espérance méd2000;7(59):123-127.
ROCHE Y.Chirurgie dentaire et patients à risque.Evaluation et pré-cautions à prendre en pratique quotidienne.Ed:FlammarionMédecine-Sciences, Paris 1996.
ROSE L.F., STEINBERG B.J.Systemic complications that influence the successful treat-ment of adult periodontitis.In Periodontal therapy. Clinicalapproaches and evidence of success: Volume 1.Quintessence Pub Co, Inc Berlin 1998.
RUTKAUSKAS J.S.The medical necessity of periodontal care. P e r i o d o n t2000;23:151-156.
SAMSON J., ROSSIER S., CARRELJ.P.Hémopathies et médecine buccale. Réalités clin1999;10(3):407-429.
SEBAHOUN G.Agranulocytoses iatrogéniques : étiologie, diagnostic, trai-tement. Rev Prat (Paris) 1999;49:1355-1360.
SZPIRGLAS H., BENSLAMAL.Pathologie de la muqueuse buccale. Ed scientifiques etmédicales Elsevier, Nancy 1999.
SZPIRGLAS H., LACOSTE J.P.Manifestations buccales des hémopathies. E n c y c l .M é d .Chir., Stomatologie-odontologie, 22-050-A-10, 1994, 8p.
TRACHLI A., MADANI A., ZAFAD S., BENCHE-KROUN S.L’hémogramme. Espérance méd 2000;7(59):123-127.
ÜNLÜ F., GÜRSES N., SECKIN T., ÜNAL T.Multifocal eosinophilic granuloma with sequential perio-dontitis-like lesions. J.Clin Periodontol 1997;24:384-387.
WILTON J.M.A. and all.Detection of high-risk groups and individuals for periodon-tal diseases. J. Clin Periodontol 1988;15:339-346.








![PERIODONTIUM (10) [EDocFind.com]](https://img.dokumen.tips/doc/110x75/577d2ee51a28ab4e1eb0488d/periodontium-10-edocfindcom.jpg)