Embed Size (px)
Citation preview

Douglas Slain, Pharm.D., BCPS, FCCP, FASHPAssociate ProfessorInfectious Diseases Clinical SpecialistWest Virginia University
Jason C. Gallagher, Pharm.D., FCCP, BCPSClinical ProfessorClinical Specialist, Infectious DiseasesTemple University
P. Brandon Bookstaver, Pharm.D., FCCP, BCPS (AQ‐ID), AAHIVPAssociate Professor & Vice ChairSC College of Pharmacy, University of South Carolina
Making Sense of Infectious Diseases Clinical Practice
Guidelines
DisclosuresThe program chair and presenters for this continuing education activity have reported no relevant financial relationships, except:
• Brandon Bookstaver ‐ Research Grant Recipient, Durata Therapeutics (now Actavis); Board Member, Durata Therapeutics (now Actavis)
• Jason Gallagher ‐ Consultant, Allergan, Cubist/Merck, and Theravance; Speakers Bureau, Cubist/Merck, Allergen, and Astellas
Practice QuestionAre you attending this session for recertification credit?
Yes, BCPS creditI am not seeking recert credit
Learning Objectives• Identify examples of practice changes that
resulted from guidelines.
• Critically evaluate guidelines for selected infectious diseases for relevance and applicability to current practice.
• Describe how selected infectious diseases guidelines should be applied in clinical practice and the areas in which they are likely to evolve.
Clinical Practice Guidelines: An updated definition
“Clinical practice guidelines are statements that include recommendations intended to optimize patient care that are informed by a systematic review of evidence and an assessment of the benefits and harms of alternative care options.”
Institute of Medicine Clinical Practice Guidelines We Can Trust 2011
Question 1:Which pharmacy organization(s) has/have co‐sponsored clinical practice guidelines with the Infectious Diseases Society of America (IDSA)?
American Society of Health‐System Pharmacists (ASHP)American College of Clinical Pharmacy (ACCP)Society of Infectious Diseases Pharmacists (SIDP)ASHP and SIDP
2015 ASHP Midyear Clinical Meeting Making Sense of Infectious Diseases Clinical Practice Guidelines
© 2015 American Society of Health-System Pharmacists 1

Antimicrobial Surgical Prophylaxis Guidelines
Two publications:• Am J Health‐Syst
Pharm;2013;70:195‐283.• Surg Infections 2013;14(1):73‐156.
Panel Composition• 3 Clinical Pharmacists
– Doug Fish– Keith Olsen– Doug Slain
• Surgeons• Infectious Diseases Physicians• 2 Pharmacist‐medical writers
National Guideline Clearinghouse
www.guideline.gov
Popular Infectious Diseases Guidelines• American Thoracic Society• HIV Guidelines
– Department of Health and Human Services Panel on Antiretroviral Guidelines for Adults and Adolescents
– International Antiviral Society–USA Panel• Centers for Disease Control and Prevention
(CDC)• Advisory Committee on Immunization
Practices (ACIP)
Infectious Diseases Society of America (IDSA)
• Has become synonymous with Infectious Diseases Clinical Practice Guidelines
• They currently publish or co‐sponsor over 60 clinical practice guidelines
• Dedicated significant resources to guideline development
• Established a translation bureau to facilitate accurate wording in multiple languages
IDSA’s Historical Step‐wise Path to Guideline Powerhouse
• Anti‐endotoxin Monoclonal Antibodies for Gram‐Negative Sepsis: Guidelines from the IDSA (1992)
• Evaluation of New Anti‐Infective Drugs for the Treatment of XYZ infection (1992)
• Quality Standard for Infectious Diseases (1994)• Guidelines for the Prevention of Opportunistic
Infections In HIV‐‐Partnered with U.S. Public Health Service (1995)
IDSA Guidelines
• IDSA Standards and Practice Guidelines Committee or expert panel often invites stakeholder organizations for either “Joint Guideline development” or “Endorsement”.
• Pharmacy partners– Society of Infectious Diseases Pharmacists (SIDP)– American Society of Health‐System Pharmacists
(ASHP)
2015 ASHP Midyear Clinical Meeting Making Sense of Infectious Diseases Clinical Practice Guidelines
© 2015 American Society of Health-System Pharmacists 2

IDSA Guidelines• Oversight by IDSA Standards and Practice
Guidelines Committee• Adopted the AGREE self‐assessment
Appraisal of Guidelines, Research, and Evaluation Collaboration
– Scope and Purpose– Stakeholder involvement– Rigor of development– Clarity and presentation– Applicability– Editorial independence
Brouwers MC et al. CMAJ 2010;182:E839‐42.
Level of Evidenceand
Recommendation
IDSA –U.S. Public Health Service Grading System
A Good evidence to support recommendation for use
B Moderate evidence to support recommendation for use
C Poor evidence to support recommendation for use
D Moderate evidence to support evidence against use
E Good evidence to support a recommendation against use
I Evidence from at least 1 randomized, properly controlled trial
IIEvidence from at least 1 well‐designed clinical trial without randomization, from cohort case‐controlled analytical studies (> 1 center), multiple time series, or dramatic results of uncontrolled experiments
III Evidence from opinions of respected authorities based on clinical experience, descriptive studies, or reports of expert committees
Strength of Recommendation
Quality of Evidence
Khan AR et al. Clin Infect Dis 2010;51:1147‐56.
Question 2:Using the IDSA‐U.S. Public Health grading system, the most common rating has been?
I‐AII‐AII‐B III‐B
Quality & Strength of Evidence of the IDSA Clinical Practice Guidelines
Evaluated 65 guidelines from 1994 to 2009
Khan AR et al. Clin Infect Dis 2010;51:1147‐56.
Level Of Evidence % of Recommendations Median % (IQR)
I 14.8 15.8 (5.8‐28.3)
II 29.7 30.9 (23.3‐43.2)
III 55.5 50.0 (38.1‐58.6)
Class of Recommendation
A 40.2 41.5 (28.7‐55.6)
B 37.7 40.3 (27.1‐47.9)
C 14.0 8.1 (1.8‐14.7)
Other 8.1 0 (0.6.7)
IQR=Interquartile range
Quality & Strength of Evidence of the IDSA Clinical Practice Guidelines
Evaluated 65 guidelines from 1994 to 2009
Khan AR et al. Clin Infect Dis 2010;51:1147‐56.
Level Of Evidence % of Recommendations Median % (IQR)
I 14.8 15.8 (5.8‐28.3)
II 29.7 30.9 (23.3‐43.2)
III 55.5 50.0 (38.1‐58.6)
Class of Recommendation
A 40.2 41.5 (28.7‐55.6)
B 37.7 40.3 (27.1‐47.9)
C 14.0 8.1 (1.8‐14.7)
Other 8.1 0 (0.6.7)
IQR=Interquartile range
2015 ASHP Midyear Clinical Meeting Making Sense of Infectious Diseases Clinical Practice Guidelines
© 2015 American Society of Health-System Pharmacists 3

Classes of Recommendation Across Levels of Evidence
Khan AR et al. Clin Infect Dis 2010;51:1147‐56.
% of Recommendations Median % (IQR)
I‐A 10.2 11.3 (3.8‐18.2)
I‐B 2.8 0.7 (0‐3.8)
I‐C 0.4 0 (0‐0)
I‐Other 0.8 ‐‐‐
II‐A 14.9 14.0 (5.7‐20.8)
II‐B 10.4 10.0 (4.9‐15.2)
II‐C 1.1 0 (0‐1.8)
II‐Other 2.4 ‐‐‐
III‐A 15.1 10.2 (0‐18.4)
III‐B 24.5 20.5 (10.3‐32.9)
III‐C 12.5 5.4 (0‐12.6)
III‐Other 4.9 ‐‐‐
IQR=Interquartile range
Classes of Recommendation Across Levels of Evidence
Khan AR et al. Clin Infect Dis 2010;51:1147‐56.
% of Recommendations Median % (IQR)
I‐A 10.2 11.3 (3.8‐18.2)
I‐B 2.8 0.7 (0‐3.8)
I‐C 0.4 0 (0‐0)
I‐Other 0.8 ‐‐‐
II‐A 14.9 14.0 (5.7‐20.8)
II‐B 10.4 10.0 (4.9‐15.2)
II‐C 1.1 0 (0‐1.8)
II‐Other 2.4 ‐‐‐
III‐A 15.1 10.2 (0‐18.4)
III‐B 24.5 20.5 (10.3‐32.9)
III‐C 12.5 5.4 (0‐12.6)
III‐Other 4.9 ‐‐‐
IQR=Interquartile range
GRADE SystemGrading of RecommendationsAssessmentDevelopmentEvaluation
• IDSA adopted the GRADE grading system (2012)• More detailed and explicit criteria for grading the quality of evidence
and the transparent process for making recommendations • This system requires that the assigned strength of a recommendation
is either “strong” or “weak.” • The main criterion for assigning a “strong” recommendation is that
the potential benefits clearly outweigh the potential risks.• For example see: Lipsky BA et al. Clin Infect Dis 2012;54:1679–84.
Guyatt G et al. J Clin Epidemiol. 2011;64:383‐94. Guyatt G et al. BMJ. 2008;336:924‐6.
GRADERubric
Lipsky BA et al. Clin Infect Dis.2012; 54:1679‐84. by permission of the Infectious Diseases Society of America.
Benefits of GRADE• Used by multiple organizations (World Health
Organization, American College of Physicians, American Thoracic Society, Cochrane Collaboration, etc.)
• Separates influence of study design from quality• Provides practical flexibility that is not dependent on
study design• Addresses study limitations, inconsistent results,
imprecision, and reporting bias
Question 3:Which of the following is an advantage of GRADE over U.S. Public Health grading system?
It is a more streamlined scale.It allows better correlation between study design and recommendation.It is a more transparent process of moving from evidence to recommendations.There are no advantages.
2015 ASHP Midyear Clinical Meeting Making Sense of Infectious Diseases Clinical Practice Guidelines
© 2015 American Society of Health-System Pharmacists 4

Guidance for Guideline DevelopmentTrustworthy
Medicare Improvements for Patients and Providers Act of 2008
“the Secretary of Health and Human Services shall enter into a contract with the Institute of Medicine of the National Academies under which the Institute shall conduct a study on the best methods used in developing clinical practice guidelines in order to ensure that organizations developing such guidelines have information on approaches that are objective, scientifically valid, and consistent”
http://resources.iom.edu/widgets/systematic‐review/infographic.html
STANDARDS FOR DEVELOPING “TRUSTWORTHY”CLINICAL PRACTICE GUIDELINES
1. Establishing Transparency2. Management of Conflict of Interest3. Guideline Development Group Composition4. Clinical Practice Guideline–Systematic Review Intersection5. Establishing Evidence Foundations for and Rating Strength of
Recommendations6. Articulation of Recommendations7. External Review8. Updating
Institute of Medicine (IOM) Clinical Practice Guidelines We Can Trust (2011)
ASHP Guideline Development Approach
1. Select authors2. Complete draft3. Council comments4. Revisions5. Public comments6. Revisions7. Council approval8. Board of Directors approval
ASHP Guideline Development Process
Obtain panel member agreement COI disclosure
Review by Council on Therapeutics (COT)
Draft guideline recommendations
Identify and document new evidence
Select Expert Panel members / Authors
Council on Therapeutics
Council on Pharmacy Practice
Council on Pharmacy Management
Council on Public Policy
Policy Week
Public ReviewRevisions
Revisions ASHP BOD approvalCOT approval Publication
2015 ASHP Midyear Clinical Meeting Making Sense of Infectious Diseases Clinical Practice Guidelines
© 2015 American Society of Health-System Pharmacists 5
Question 4:Which of the following is NOT a standard item in the IOM’s “Clinical Practice Guidelines We Can Trust” publication?
Management of Conflict of InterestInclusion of only level I and II dataClinical Practice Guideline–Systematic Review IntersectionExternal Review
Guideline Influence
Why Don't Physicians Follow Clinical Practice Guidelines?
Cabana MD et al. JAMA 1999;282(15):1458‐1465.
Knowledge Attitudes Behavior
Lack of familiarity Lack of outcome expectancy
Patient barriers
Lack of awareness Lack of agreement with guideline
Guideline barriers
Lack of self‐efficacy Environmental barriers
Lack of motivation/ Inertia of previous practice
Why don’t physicians and pharmacistsfollow guidelines?
• Survey of 163 pharmacists about 2009 vancomycin guidelines Rybak MJ et al. Am J Health‐Syst Pharm. 2009; 66:82‐98.
Davis SL et al. Pharmacotherapy. 2013; 33:1256‐63.
Therapeutic drug monitoring practice Never Sometimes Always
Trough concentration just before next dose at steady state, before 4th dose
0 % 54 % 45 %
No trough monitoring for patients with short courses of therapy and stable renal function
20 % 63 % 14 %
Loading doses in seriously ill patients and complicated infections to facilitate rapid target attainment
14 % 43 % 42 %
Validating Guidelines by Clinical Investigation
• Inconsistent results• Guidelines often tested in observational
studies• Possibility of a “Halo effect”• Publication bias
Marrie TJ. Clin Infect Dis 2005;41:1717‐9.
Regional Influence on Guidelines• Different recommendations in different countries
– Atypical pathogen coverage in North American community‐acquired pneumonia guidelines, but less important in European guidelines
• Don’t be the ugly American– Perspectives of single payer countries– Resource availability– Medical tourism– Physician autonomy– Conflict of interests– Politics
Mandell LA. Clin Infect Dis 2000;31:422‐5.
2015 ASHP Midyear Clinical Meeting Making Sense of Infectious Diseases Clinical Practice Guidelines
© 2015 American Society of Health-System Pharmacists 6

What Guidelines Are Not• Evidence‐based assumptions should be
assessed– Not all randomized, controlled trials are created
equal
• They do not always allow for personalized medicine– “one‐size‐does‐NOT‐fit‐all”
• Never a substitute for clinical judgement!
Even Hollywood knows
“The code is more what you'd call guidelines than actual rules”
‐‐Captain Hector Barbossa in Pirates of the Caribbean: The Curse of the Black Pearl
What Guidelines Can Do• Provide guidance for non‐experts (and experts)• Decrease “inappropriate” variation• Facilitate development of institutional guidelines
and protocols• Represent a standard of practice
– Pay for performance (i.e., CMS)– Legally defensible?
• Identify important gaps in knowledge• Serve as teaching references
Jason C. Gallagher, Pharm.D., FCCP, FIDSA, BCPSClinical Professor
Clinical Specialist, Infectious DiseasesTemple University
A Closer Look:Candidemia
Hospital‐acquired pneumonia (HAP) Methicillin‐resistant Staphylococcus aureus (MRSA)
Bloodstream Infections (BSIs) Intra‐abdominal infections (IAIs)
Question 5:In the treatment of candidemia caused by Candida albicans, my preferred agent is:
An echinocandinFluconazoleAn amphotericin B formulationVoriconazole
Candidemia
Pappas PG, Kauffman CA, Andes D, et al. Clin Infect Dis 2009;48:503‐35.
Clinical Practice Guidelines for the Management of Candidiasis: 2009 Update by the Infectious
Diseases Society of America
2015 ASHP Midyear Clinical Meeting Making Sense of Infectious Diseases Clinical Practice Guidelines
© 2015 American Society of Health-System Pharmacists 7

CandidemiaGuideline Recommended Options
Pappas PG, Kauffman CA, Andes D, et al. Clin Infect Dis 2009;48:503‐35.
Fluconazole
Echinocandin
LFAB(Lipid Formulation of
Amphotericin B)
Echinocandin
Non‐neutropenic
Neutropenic
OR
OR
Preferred if patient is moderately‐to‐severely ill
or has recent azole exposure
Recommended to de‐escalate to fluconazole if
isolate is likely susceptible
FluconazoleOR
Non‐critically ill patients without azole exposure
Most patients
What does the evidence say?Study Drug 1 Drug 2 Results
Mora‐Duarte 2002
Caspofungin AmBd Non‐inferiority, less AEs with caspofungin
Kuse 2007 Micafungin LAmB Non‐inferiority, less AEs with micafungin
Pappas 2007 Caspofungin Micafungin Non‐inferiority
Reboli 2007 Anidulafungin Fluconazole Superiority of anidulafungin
Mora‐Duarte JM, Betts R, Torstein C, et al. N Engl J Med 2002;347:2020‐9. Kuse ER, Chetchotisakd P, ad Cunha CA et al. Lancet 2007;369:1519‐27. Pappas PG, Kauffman CA, Andes D, et al. Clin Infect Dis 2009;48:503‐35. Reboli AC, Rotstein
C, Pappas PG, et al. N Engl J Med 2007;356:2472‐82.
AmBd‐ amphotericin B deoxycholate LAmB‐ liposomal amphotericin B
Anidulafungin vs. FluconazoleA Closer Look
Double‐blinded RCT of anidulafungin 200 mg x1, 100 mg IV q24hr vs. fluconazole 800 mg x1, then 400 mg IV q24hr
Reboli AC, Rotstein C, Pappas PG, et al. N Engl J Med 2007;356:2472‐82
Endpoint Fluconazole(n=118)
Anidulafungin
(n=127)
End IV Tx 71 (60.2%) 96 (75.6%)
End Tx 67 (56.8%) 94 (74.0%)
2‐week F/U 58 (49.2%) 82 (64.6%)
6‐week F/U 52 (44.1%) 71 (55.9%)
‐20 ‐10 0 10 20 30
15.4 (3.9 to 27.0)
17.2 (5.5 to 29.0)
15.4 (3.1 to 27.7)
11.8 (−0.6 to 24.3)
Fluconazole better Anidulafungin betterOutcome was global response, a compositeof microbiological and clinical success
Anidulafungin vs. FluconazoleA Closer Look
Pathogen Anidula Fluc P‐value Anidula Fluc P‐value
Candida albicans 77/81 (95) 57/70 (81) 0.01 60/74 (81) 38/61 (62) 0.02
Candida glabrata 15/20 (75) 18/30 (60) 0.37 9/16 (56) 11/22 (50) 0.75
Candida parapsilosis 9/13 (69) 14/16 (88) 0.36 7/11 (64) 10/12 (83) 0.37
Candida tropicalis 13/15 (87) 7/11 (64) 0.35 13/14 (93) 4/8 (50) 0.04
Other Candida 5/6 (83) 3/3 (100) 1.00 3/4 (75) 2/3 (67) 1.00
All Candida spp. 119/135 (88) 99/130 (76) 0.02 92/119 (77) 65/106 (61) 0.01
Reboli AC, Rotstein C, Pappas PG, et al. N Engl J Med 2007;356:2472‐82
Successful Microbiological Response Successful Global Response
Caspofungin vs. IsavuconazoleA Class Effect?
Double‐blinded RCT of caspofungin voriconazole vs. isavuconazole (IVPO) in 400 patients• Patients received at least 10 days of IV therapy
Basilea Pharmaceutical Ltd. Press Release. July 30, 2015. http://globenewswire.com/news‐release/2015/07/30/756194/10143853/en/Basilea‐reports‐topline‐results‐of‐isavuconazole‐phase‐3‐study‐in‐
candidemia‐and‐other‐invasive‐Candida‐infections.html
Endpoint IsavuconazoleCaspofungin/ voriconazole
End IV Tx 60.3% 71.1%
2‐week F/U 54.8% 57.2%‐20 ‐10 0 10 20
‐10.8 (‐19.9 to ‐1.8)
‐2.7 (−12.2 to 6.8)
Isavuconazole better Caspofungin/vori better
Question 6:According to guidelines, which of these patients in the ED should receive a “HAP‐like” antimicrobial regimen for his/her pneumonia:
AB, a 54‐year‐old man who has intermittent hemodialysis on MWFBC, 63‐year‐old woman with diabetes mellitus who has a diabetic foot ulcer and is receiving wound care for itCD, a 78‐year‐old man who is a resident of a long‐term care facilityAll of these patients
2015 ASHP Midyear Clinical Meeting Making Sense of Infectious Diseases Clinical Practice Guidelines
© 2015 American Society of Health-System Pharmacists 8

Hospital‐Acquired, Healthcare‐associated, and Ventilator‐associated Pneumonia
ATS/IDSA. Am J Respir Crit Care Med 2005;171:388‐415.
Antipseudomonal Beta‐lactam
Ciprofloxacin or Levofloxacin AminoglycosideOR
1
2
3
“HCAP”
• Was hospitalized for >2 days in past 90 days
• Resided in a long‐term care facility
• Attended a hospital or HD clinic
• Received recent IV antibiotic therapy, cancer chemotherapy, or wound care within 30 days
ATS/IDSA. Am J Respir Crit Care Med 2005;171:388‐415.Image: digivizer.com
Pneumonia in a patient who:
HCAP= Healthcare‐associated pneumonia
Unresolved Issues with HCAPIssue Evidence
HCAP is associated with high mortality, similar to HAP
Found in many (not all) studies
HCAP is associated with an excess of MDR pathogens
Not consistently true in studies
Empiric regimens are often inadequate Evidence largely absentMDR pathogens and inadequate therapy are the reasons for excess HCAP mortality
Not proven
Broad‐spectrum empiric antibiotics similar to those used for HAP are needed
Data not consistent
Ewig S, Welte T, Torres A. Curr Opin Infect Dis 2012;25:166‐75.MDR= multi‐drug resistant
HCAP at Temple University HospitalEvaluation of patients diagnosed with HCAP in the ED in 2012
Toussaint K et al. Interscience Conference of Antimicrobial Agents and Chemotherapy. Denver, CO. 2013.
HCAP Risk Factors
Present
Absent
No culture, 40
Normal flora, 21
MRSA, 1
P. aeruginosa, 3
Enterobacteriaceae, 4
B. cepacia, 1MSSA, 1
Sputum Cultures
HCAP – Does Guideline Adherence Improve Outcomes?
N=3295 Adherent Non‐adherent
CAP 86/1557 (6%)* 109/1097 (10%)*HCAP 6/35 (17%) 18/148 (12%)
Grenier C et al. J Antimicrob Chemother 2011;66:1617‐24.Attridge RT et al. Eur Respir J 2011;38:878‐87.
Overall GC‐HCAP GC‐CAP Non‐GC
Number 15071 1211 11408 245230‐day
mortality 12.6% 22.8% 9.9% 20.1%
Multicenter Cohort of VA Patients with Non‐ICU HCAP
Single Center Cohort of Canadian HCAP Pts
HCAP guideline use associated with
mortalityaOR 2.18
(1.86‐2.55)
*P<0.05
CAP‐ community‐acquired pneumoniaGC‐ guideline concordant
Lung Concentrations of ColistinShould We Use Aerosolized Drug?
• Some reports show colistin lung concentrations to be very low in both animal models and human infection
• Animal studies show better lung disposition and cure rates with aerosolized drug + IV vs. IV alone
Imberti R, Cusato M, Villani P, et al. CHEST 2010;138:1333‐9. Aoki N, Takeda K, Kikuchi Y, et al. J Antimicrob Chemother 2009;63:534‐42.Lu Q, Girardi C, Zhang M, et al. Intensive Care Med 2010;36:1147‐55.Valachis A, Samonis G, Kofteridis DP, et al. Crit Care Med 2015;43:527‐33.
Imberti et al performed a PK study of 13 pts who received IV CMS:
Cmax,avg = 2.21 ± 1.08 mcg/mL Ctrough,avg = 1.03 ± 0.69 mcg/mL
CBAL 2h = undetectable
Valachis et al performed a meta‐analysis of 16 studies comparing
IV CMS to IV + aerosolizedClinical Response: OR 1.57 (1.14‐2.15)
Mortality: OR 0.74 (0.54‐1.01)
2015 ASHP Midyear Clinical Meeting Making Sense of Infectious Diseases Clinical Practice Guidelines
© 2015 American Society of Health-System Pharmacists 9

Can Aerosolized Antibiotics Prevent Resistance?Aerosolized antibiotics (n=24)
Placebo(n=18)
P‐value
Number of organisms present at randomization eradicated
26/27 (96%) 2/23 (9%) <0.0001
Patients with eradication of resistant organisms
14/16 (88%) 1/11 (9%) <0.0001
Patients with new resistance during treatment
2/16 (13%) 6/11 (55%) 0.03
Number of patients receiving systemic antibiotics
24/24 (100%) 18/18 (100%)
1
Systemic antibiotic days (mean ± SD) 17.33 ± 10.99 14.61 ±10.81
0.4159
CPIS at baseline (mean ± SD) 9.3 ± 2.7 8.0 ± 2.1 0.5000
CPIS at end of therapy (mean ± SD) 5.3 ± 2.6 8.6 ± 2.6 0.0008
Palmer LB, Smaldone GC. Am J Resp Crit Care Med 2014;189:1225‐33.CPIS= clinical pulmonary infection score
Question 7:For the treatment of a bloodstream infection caused by MRSA with a minimum inhibitory concentration of 2 mcg/mL, my preferred drug is:
VancomycinDaptomycinIt dependsDude, I came here for you to tell me
MRSA Bloodstream InfectionsGuideline Recommended Options
Liu C, Bayer A, Cosgrove SE, et al. Clin Infect Dis 2011;52:1‐38
Daptomycin6 mg/kg daily
Vancomycin15 mg/kg q8‐12hrUncomplicated
Culture clearance <4 days, defervesence in 72 hours, no metastases or endocarditis
Complicated
OR
Daptomycin6‐10 mg/kg daily
Vancomycin15 mg/kg q8‐12hr
OR
x 2 weeks
x 4‐6 weeks
Liu C, Bayer A, Cosgrove SE, et al. Clin Infect Dis 2011;52:1‐38
Clinical Practice Guidelines by the Infectious Diseases Society of America for the Treatment of
Methicillin‐Resistant Staphylococcus Aureus Infections in Adults and Children
Harm Associated with Persistent MRSA Bacteremia
Hawkins C, Huang J, Jin N, et al. Arch Intern Med 2007;167:1861‐7. Chong YP, Park S‐J, Kim HS, et al. Medicine 2014;92:98‐108.
Ok HS, Lee HS, Park MH, et al. Korean J Intern Med 2013;28:678‐86.
Patients with persistent MRSA bacteremia have been show to have:• Higher relapse rates and attributable mortality
(Chong et al)• Higher 30‐day mortality (Ok et al)• Higher crude and attributable mortality,
longer hospital length of stay (Hawkins et al)
Van Hal SJ, Lodise TP, Paterson DL. The clinical significance of vancomycin minimum inhibitory concentration in Staphylococcus aureus infections: a systematic review and meta‐analysis. Clin Infect Dis. 2012;54:755‐71,
by permission of the Infectious Diseases Society of America.
OR for treatment failure = 2.69 (95% CI 1.60‐4.51)
High vs. Low Vancomycin MICs in Staphylococcus aureus BSIs
2015 ASHP Midyear Clinical Meeting Making Sense of Infectious Diseases Clinical Practice Guidelines
© 2015 American Society of Health-System Pharmacists 10
High vs. Low Vancomycin MICs in Staphylococcus aureus BSIs
Kalil AC, Van Schooneveld TC, Rupp ME, et al. JAMA 2014;312:1552‐64.
• Meta‐analysis of 38 studies of S. aureus BSIs evaluating mortality as an endpoint
• Attempted to control for age, APACHE II score, Charlson score, vancomycin exposure, endocarditis, ICU stay
• Did not evaluate clinical failure
N=8291 Overall MIC <1.5 mcg/mL
MIC 1.5‐2 mcg/mL
P‐value
30‐day mortality
26.1% 25.8% 26.8% 0.43
Elevated MICs in MRSA BSIsIs anything better than vancomycin?
Matched cohort of patients with deep‐seated MRSA BSI and Vanc MIC>1 mcg/mL who received vancomycin or an early change to daptomycin
Murray KP, Zhao J, Davis SL, et al. Clin Infect Dis 2013;56:1562‐9, by permission of the Infectious Diseases Society of America.
Parameter Daptomycin Vancomycin P‐value
Clinical Failure 17 (20%) 41 (48.2%) <0.001
30‐d Mortality 3 (3.5%) 11 (12.9%) 0.047
Persistent BSI 16 (18.8%) 36 (42.4%) 0.001
BSI duration, d 3 (2‐5) 5 (3‐8) 0.003
OR for clinical failure with vancomycin = 3.7 (1.9‐7.4)
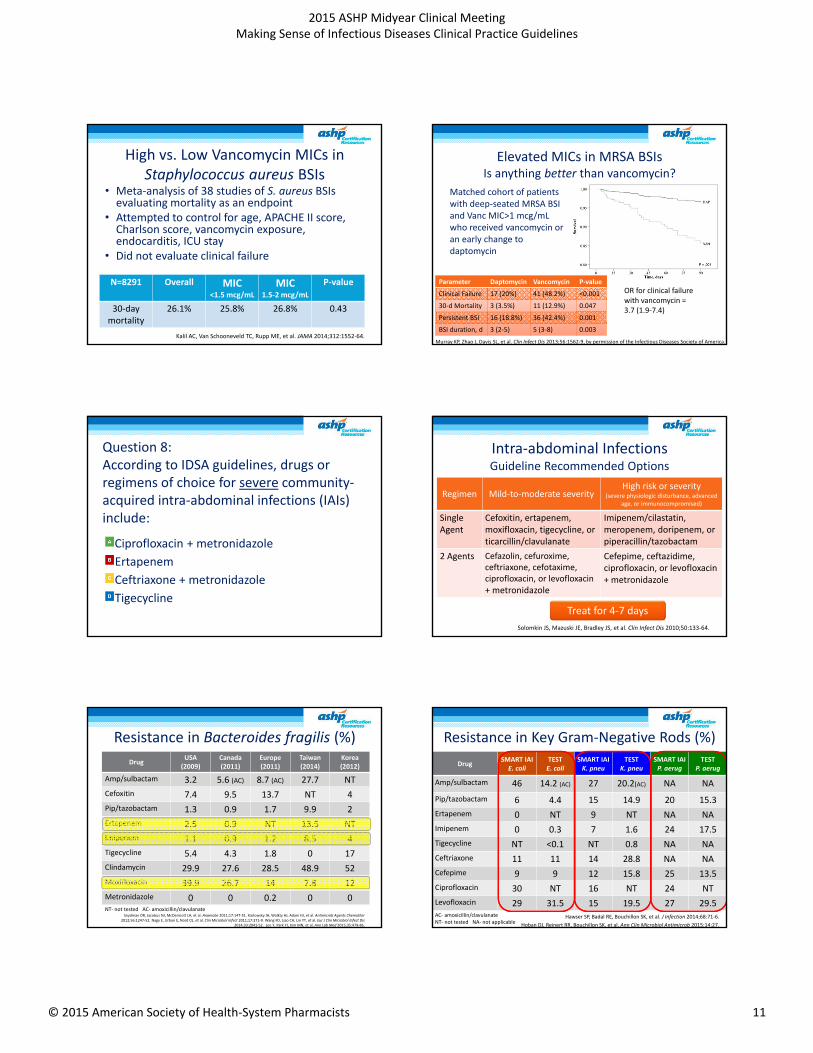
Question 8:According to IDSA guidelines, drugs or regimens of choice for severe community‐acquired intra‐abdominal infections (IAIs) include:
Ciprofloxacin + metronidazoleErtapenemCeftriaxone + metronidazole Tigecycline
Intra‐abdominal InfectionsGuideline Recommended Options
Regimen Mild‐to‐moderate severityHigh risk or severity
(severe physiologic disturbance, advanced age, or immunocompromised)
Single Agent
Cefoxitin, ertapenem, moxifloxacin, tigecycline, or ticarcillin/clavulanate
Imipenem/cilastatin,meropenem, doripenem, or piperacillin/tazobactam
2 Agents Cefazolin, cefuroxime, ceftriaxone, cefotaxime, ciprofloxacin, or levofloxacin+ metronidazole
Cefepime, ceftazidime, ciprofloxacin, or levofloxacin+ metronidazole
Solomkin JS, Mazuski JE, Bradley JS, et al. Clin Infect Dis 2010;50:133‐64.
Treat for 4‐7 days
Resistance in Bacteroides fragilis (%)Drug
USA (2009)
Canada (2011)
Europe(2011)
Taiwan(2014)
Korea(2012)
Amp/sulbactam 3.2 5.6 (AC) 8.7 (AC) 27.7 NTCefoxitin 7.4 9.5 13.7 NT 4Pip/tazobactam 1.3 0.9 1.7 9.9 2Ertapenem 2.5 0.9 NT 13.5 NTImipenem 1.1 0.9 1.2 8.5 4Tigecycline 5.4 4.3 1.8 0 17Clindamycin 29.9 27.6 28.5 48.9 52Moxifloxacin 39.9 26.7 14 7.8 12Metronidazole 0 0 0.2 0 0
Snydman DR, Jacobus NJ, McDermott LA, et al. Anaerobe 2011;17:147‐51. Karlowsky JA, Walkty AJ, Adam HJ, et al. Antimicrob Agents Chemother 2012;56:1247‐52. Nagy E, Urban E, Nord CE, et al. Clin Microbiol Infect 2011;17:371‐9. Wang FD, Liao CH, Lin YT, et al. Eur J Clin Microbiol Infect Dis
2014;33:2041‐52. Lee Y, Park YJ, Kim MN, et al. Ann Lab Med 2015;35:479‐86.
NT‐ not tested AC‐ amoxicillin/clavulanate
Resistance in Key Gram‐Negative Rods (%)Drug
SMART IAIE. coli
TEST E. coli
SMART IAIK. pneu
TESTK. pneu
SMART IAIP. aerug
TESTP. aerug
Amp/sulbactam 46 14.2 (AC) 27 20.2(AC) NA NAPip/tazobactam 6 4.4 15 14.9 20 15.3Ertapenem 0 NT 9 NT NA NAImipenem 0 0.3 7 1.6 24 17.5Tigecycline NT <0.1 NT 0.8 NA NACeftriaxone 11 11 14 28.8 NA NACefepime 9 9 12 15.8 25 13.5Ciprofloxacin 30 NT 16 NT 24 NTLevofloxacin 29 31.5 15 19.5 27 29.5
Hawser SP, Badal RE, Bouchillon SK, et al. J Infection 2014;68:71‐6.Hoban DJ, Reinert RR, Bouchillon SK, et al. Ann Clin Microbiol Antimicrob 2015;14:27.
AC‐ amoxicillin/clavulanate NT‐ not tested NA‐ not applicable
2015 ASHP Midyear Clinical Meeting Making Sense of Infectious Diseases Clinical Practice Guidelines
© 2015 American Society of Health-System Pharmacists 11

Points to Question• Moxifloxacin – useful?• Ertapenem for severe community‐acquired
infections?• Role of tigecycline?• Utility of levofloxacin/ciprofloxacin for severe
community‐acquired infections?• Duration of therapy?
IAIs: Duration of Therapy RCT of 518 patients with intra‐abdominal infections and adequate source control
– Control: 2 days of antibiotics after resolution of systemic inflammatory response syndrome (SIRS) criteria
– Short course: 4 days of antibiotics (fixed course)• Primary outcome (30 days): death, surgical site
infection, or recurrence
Sawyer RG, Claridge JA, Nathens AB, et al. N Engl J Med 2015;372:1996‐2005
GroupAge, yr
(Mean+SE)APACHE II(Mean+SE)
Colon/Rectum
n (%) Appendixn (%)
PrimaryOutcomen (%)
Abx days(median, IQR)
Control 52.2 +1.0 9.9 +0.4 80 (30.8) 34 (13.1) 58 (22.3) 8 (5‐10)*
Short Abx 52.2 +1.0 10.3 +0.4 34 (13.1) 39 (15.1) 56 (21.8) 4 (4‐5)*
*p<0.001 for difference
Key Takeaways• Key Takeaway #1: HCAP
– Over‐diagnosed, over‐treated• Key Takeaway #2: Candidemia
– Perhaps echinocandins are just better than azoles– Is the advantage “secured” by starting with an
echinocandin before changing to fluconazole?• Key Takeaway #3: MRSA BSIs
– Vancomycin MICs of 1.5 or 2 mcg/mL may be problematic
P. Brandon Bookstaver, Pharm.D., FCCP, BCPS (AQ‐ID), AAHIVPAssociate Professor & Vice Chair
SC College of Pharmacy, University of South Carolina
Making Sense of Clinical Guidelines
Clinical guidelines on the agenda• Clostridium difficile infection
• Community‐acquired pneumonia
• Antibiotic prophylaxis in surgery
• Antibiotic therapy in open fractures
Clostridium difficile InfectionManagement
2015 ASHP Midyear Clinical Meeting Making Sense of Infectious Diseases Clinical Practice Guidelines
© 2015 American Society of Health-System Pharmacists 12

Clostridium difficile infection: United States Guideline Comparison
Variables IDSA/SHEA Guidelines American College of Gastroenterology
Definition of Severe WBC >15,000 cells/mm3 or SCr >1.5x pre‐CDI level*Age mentioned, but not spec.
Serum albumin <3 g/dL PLUS WBC > 15,000 cells/mm3 or abdominal tenderness
Definition of Severe/Complicated
Hypotension or shock, ileus, megacolon
Attributable to CDI: Admission to ICU, hypotension, T >38.5°C, ileus/abdominal distention, MS changes, WBC > 35,000 or <2,000, lactate >2.2 mmol/L, or EOD
Treatment Mild/Moderate
Metronidazole (MTF) 500mg TID PO x 10‐14 days
MTR 500mg PO TID x 10 days
Treatment Severe Vancomycin (Vanc) 125mg PO QID x 10‐14 days
Vancomycin 125mg PO QID x 10 days
Treatment of Complicated
Vancomycin 500mg PO QID + MTR 500mg Q8 hours IV ; (Vanc PR if complete ileus)
Vancomycin 500mg PO QID PLUS MTR 500mg Q8 hours IV PLUS Vanc 500mg PR in 500 cc QID
Treatment of Recurrence
Initial – repeat courseMultiple – Vanc taper
Initial – repeat course; 2nd – Vanc taper; 3rd – Fecal microbiota transplant (FMT)
IDSA/SHEA Practice Guidelines for CDI. ICHE 2010;31(5):431‐5. Guidelines for diagnosis, treatment and prevention of CDI. Am J Gastroenterol 2013;108:478‐98.
Question 9:A 79 y/o man with Type II diabetes and hypertension is admitted for diarrhea (7 stools per day) and dehydration. He does not have noted abdominal distention but is lethargic. Blood pressure is 105/56 mmHg prior to fluid boluses. He is currently taking levofloxacin (Day 7 of 14 prescribed) for acute bacterial sinusitis. His WBC is 19,500 cells/mm3 and serum creatinine is 1.9mg/dl (baseline 1.1). CDI is high on the differential and Toxin B PCR is pending. He is admitted to a medical ward. Which initial therapy would you recommend?
Metronidazole 500mg PO Q8 hoursVancomycin 125mg PO Q6 hoursVancomycin 500mg PO Q6 hoursMetronidazole 500mg IV Q8 hours plus Vancomycin 125mg PO Q6 hoursFidaxomicin 200mg PO twice daily
What dose is the right dose for PO vancomycin in treatment of CDI?
Trial Intervention Results (Fecal Concentrations)
Keighley MRB, et al. BMJ 1978
A. RCT of PO vancomycin 125mg PO Q6 hours (n‐44)B. Prelim study 125mg vs 250mg vs 500mg impact on fecal concentrations
A. Day 2 = 351 (64‐760)Day 4 = 399 (152‐880)B. 500mg = 714 +/‐ 341250mg = 447 +/‐ 260125mg = 351 +/‐ 172 mcg/mL
Burdon DW, et al. JAC 1979
125mg vs. 250mg Q6 PO for CDI; fecal concentrations measured in subset
125mg group= 427mcg/mL (70‐740)250mg group=447mcg/mL (80‐1430)
Tedesco F, et al. Lancet 1978
500mg PO q6 hours Mean concentrations were 3,100 mcg/g
Baird DR. JAC 1989 125mg vs. 250mg PO Q6 hours; fecal conc. measured daily and 48 hours after d/c
Data detailed on following slide
Keighley MR, et al. BMJ. 1978;2:1667‐9. Burdon DW, et al. J Antimicrob Chemother. 1979; 5:307‐10. Tedesco F, et al. Lancet. 1978; 2:226‐8. Baird DR. J Antimicrob Chemother. 1989; 23:167‐9.
Fecal Conc. Comparison 125mg vs. 250mg
• N=13– Matrix & liquid
formulations
• Concentrations consistently at least 50‐1000x above MIC50/90=1mcg/mL
• Significant variation between pts.
• Vanc concentrations increased as stool became more formed
Baird DR. J Antimicrob Chemother. 1989; 23:167‐9. By permission of the British Society for Antimicrobial Chemotherapy
125 mg 250 mg
Rationale for “front‐loaded” dosing of PO vancomycin?
• N=15
• Comparing daily fecal [ ] between 125, 250 and 500mg using fluorescence polarization assay
• Day 1‐2 <50mcg/mL detected in ~20% of patients receiving 125mg Q6 hours
• >4 stools per day associated w/ significantly lower levels
Gonzales M, et al. BMC ID. 2010; 10:363.© 2010 Gonzales et al; licensee BioMed Central Ltd.
Available under public license at http://www.biomedcentral.com/1471‐2334/10/363
Difference in effectiveness between oral dosing regimens?
• N=46 patients w/ severe CDI randomized to 125mg or 500mg Q6 hours
• Avg duration of tx = 10 days and 91% resolution by 1 week– Impact was the same between groups, no difference in onset of action– Recurrence ~20% not different between groups
• Lam et al confirmed these results in follow‐up study of 76 severe CDI patients (n=25, low dose (LD) vs. n=53, high dose)– Day 10 clinical cure 64% LD vs. 60% HD, p=0.76– Recurrence 12% in LD vs. 2% in HD, p=0.09
Fekety R, et al. Am J Med 1989.
Daily Dose Resolution of Pain (days)*
Resolution of Diarrhea (days)*
0.5 g 2.1 (0.9) 3.8 (1.4)
2 g 2.7 (1.5) 4.3 (1.8)*P>0.05
Lam SW, et al. Int J Antimicrob Agents. 2013; 42:553‐8.Fekety R, et al. Am J Med. 1989; 86:15‐9.
2015 ASHP Midyear Clinical Meeting Making Sense of Infectious Diseases Clinical Practice Guidelines
© 2015 American Society of Health-System Pharmacists 13

Question 10:A 37 y/o woman with severe diarrhea (9 stools per day) and dehydration with acute kidney injury (SCr=2.7mg/dL) is admitted to the medical ICU secondary to hypotension unresponsive to initial IVF. Other pertinent labs include a lactate 3.1 mmol/L and WBC 31,000 cells/mm3. A C. difficile Toxin B PCR is positive 6 hours after admission. What is the most appropriate therapy in this patient?
Fidaxomicin 200mg PO BIDVancomycin 500mg PO QIDVancomycin 125mg PO QID plus Metronidazole 500mg IV Q8 hoursVancomycin 500mg PO QID plus Metronidazole 500mg IV Q8 hours plus Vancomycin 500mg PR QID
How do we manage the critically ill CDI patient?• Vanc/MTR combo therapy
versus vancomycin monotherapy – Vanc dosing variable– N=9 received PR vanc
• Critically ill:– Albumin <2.5g/dL – HR>90bpm – MAP<60mmHg – WBC>15,000cells/mm3
– Age>60 years – SCr >1.5 x baseline – T>38°C
Rokas CEE, et al. CID. 2015; 61:934‐41.
Multivariate regression model for predictors of survival:IV MTR: OR=4.5, CI (1.48 – 14.0)Albumin: OR=0.87, CI (0.78‐0.97)
OutcomeN (%)
Monotherapy, n=44
Combo therapy, n=44
In‐hospital mortality* 16 (36.4) 7 (15.9)
Time to death, mediandays (range)
21 (5‐174) 15 (6‐32)
Clinical Success
Day 6 9 (20.5) 6 (13.6)
Day 10 27 (61.4) 25 (56.8)
Day 21 33 (75) 37 (84.1)
LOS, median days (range) 20.5 (10‐64) 18 (6‐166)
LOS ICU, median days (range)
9 (4‐60) 11 (3‐68)
*p<0.05
Rectal vancomycin (VPR): worthy of consideration?• Conceptually:
– Reach drug concentrations in the distal one‐third of colon• Evidence:
• Concerns:– Appropriate delivery– Metabolic acidosis is rare effect of 0.9% NS in colon– Risk of perforation with tubes/enemas
Shetler K, et al. Surg Endosc. 2001;15:653‐9. Apisarnthanarak A, et al. Clin Infect Dis. 2002;35:690‐6.Kim PK, et al. Surg Infect (Larchmt) 2013;14:532‐9. Malamood M, et al. Clin Med Res. 2015;7:422‐7.
Study/Sample Size Dose of VPR Concomitant Therapy Outcome
Shetler et al (2001), n=7 250 mg Q6 hours All IV MTR, 5 of 7 PO Vanc
Resolution in 4 of 7 pts.
Apisarnthanarak et al (2002), n=9
Varied, 0.5 to 1 g Q4 to Q12 hours
All IV/PO MTR, 7 of 9 PO Vanc
Resolution in 8 of 9 pts.
Kim et al (2013), n=47 1g Q6 hours All IV MTR, PO Vanc 70% resolution without sx.
Malamood et al (2015), n=24
125 – 250 mg Q6 to Q8 hours
All MTR, 80% PO Vanc No difference in death/sx compared to no VPR group
Is there evidence for combination therapy beyond critically ill?
• Recent meta‐analysis by Li and colleagues examined 5 studies that compared monotherapy MTR or vancomycin versus combination therapy– 3 studies had 3 arms, allowing for multiple comparisons (8
total comparisons)
• No difference between monotherapy and combination therapy in rate of clinical cure or recurrence– Disease severity primarily outside of ICU, but variable– Rate of ADE slightly higher in combination therapy (could
have been driven by study w/ rifampin)Li R, et al. PLoS ONE. 2015; 10(10):e0137252.
Where should fidaxomicin (FDX) fit in treatment?
• Two, Phase 3 RCTs of fidaxomicin (200mg PO twice daily x 10 days) compared to vancomycin 125mg PO QID x 10 days– Clinical cure, FDX 88% vs. Vanc 87% (p=NS)– Cure without recurrence, FDX 71% vs. Vanc 57%
(p=0.0004)Acquisition Cost
Cost Effectiveness
Patient selection
Bedside tool
Cornely OA, et al. Lancet Infect Dis. 2012; 12:281‐9.Louie TJ, et al. N Engl J Med. 2011; 364:422‐31.
Do we have an optimal bedside assessment tool?
Miller et al derived and validated the ATLAS score for CDI response to therapy using data from FDX RCTs
Miller MA, et al. BMC ID. 2013; 13:148.Arora V, et al. J Hosp Infect. 2011; 79:23‐26.
Jacobson SM, et al. AJHP. 2015; 72:1871‐5.
Parameter 0 points 1 point 2 points
Age <60 years 60 – 79 years > 79 years
Concurrent systemic antibx (>1 day) No ‐‐‐ Yes
Temperature < 37.5 C 37.6 – 38.5 C > 38.5 C
WBC count <16,000 16,000‐25,000 >25,000
Albumin >3.5g/dL 2.6 – 3.6 g/dL <2.6 g/dL
Serum creatinine < 120 mmol/L 121‐179 mmol/L >180 mmol/L
Jacobson, et al. investigated ATLAS score to predict cure and recurrence in 245 patients receiving metronidazole, vancomycin or both.
48% of patients had severe disease; 71% taking concomitant antibiotics**Significant negative correlation between ATLAS score & cure rates, but not recurrence.
2015 ASHP Midyear Clinical Meeting Making Sense of Infectious Diseases Clinical Practice Guidelines
© 2015 American Society of Health-System Pharmacists 14

Fidaxomicin role in therapy – Cost effectiveness must be applied in decision –
Study Identification Conditions Studied Cost Effective?
Bartsch SM, et al. CID 2013
No FDX; FDX only and FDX by strain typing; $50,000/QALY threshold
Not as first‐line
Nathwani D, et al. JAC 2014
FDX vs. vancomycin , incremental cost‐effectiveness ratio (ICER) was primary outcome; $30,000 and $45,000/QALY thresholds
60% for severe68% first recurrence
Konijeti GG, et al. CID 2014
Recurrent CDI , FDX, MTR, Vanc, FMT; $50,000/QALY threshold
NoFDX <$1,359 would meet threshold
Stranges PM, et al. Value in Health 2013
FDX vs vancomycin, $100,000/QALY threshold
Yes$67,576/QALY
Bartsch SM, et al. CID. 2013; 57:555‐61. Nathwani D, et al. JAC. 2014; 69:2901‐12.Konijeti GG, et al. CID. 2014; 58:1507‐14. Stranges PM, et al. Value Health. 2013; 16:297‐304.
Community Acquired Pneumonia
Inpatient Community‐Acquired Pneumonia – IDSA/ATS Guidelines –
Scenario Antibiotic Recommendation (s) Level of evidence
Non‐ICU Respiratory FQ ORPreferred BL plus macrolide or doxycyclineErtapenem for selected patients
Level I
Level ILevel III (doxycycline)
Non‐ICU, PCN allergic Respiratory FQ
ICU Preferred BL plus either azithromycin or FQ
Level II (azithromycin)Level I (FQ)
ICU, PCN allergic Respiratory FQ plus aztreonam
Pseudomonal risk factors Antipneumococcal/pseudomonal BL plus ciprofloxacin or levofloxacin OR‐ BL plus AG and azithromycin or antipneumococcal FQ
Level III
Pseudomonal risk factorsPCN allergic
Aztreonam plus AG and antipneumococcal FQ
Respiratory FQ = moxi, levo or gemifloxacinPreferred BL = cefotaxime, ceftriaxone or amp/sulbactamAG = aminoglycoside
Mandell LA, et al. IDSA/ATS Guidelines for CAP. CID. 2007; 44:S27‐72.
Guidelines quickly become outdated
Mandell LA, et al. IDSA/ATS Guidelines for CAP. CID. 2007; 44:S27‐72.
Centers for Medicaid and Medicare Services (CMS) Update in 2015
• Core measures involving pneumonia have been retired– More flexibility given to hospitals for reporting
• Focus for antibiotics will be on sepsis, which could be secondary to pneumonia in many scenarios
http://www.jointcommission.org/core_measure_sets.aspx
Question 11:Pseudomonas Risk FactorsWhich of the following is/are risk factor(s) for Pseudomonal CAP?
COPD and/or smokingStructural lung diseaseRecent antibiotic exposureAsthma
Arancibia F, et al. Arch Intern Med. 2002; 162:1849‐58.
2015 ASHP Midyear Clinical Meeting Making Sense of Infectious Diseases Clinical Practice Guidelines
© 2015 American Society of Health-System Pharmacists 15

Question 12:Where does P. aeruginosa rank on common pathogen list for ICU CAP?
1st
3rd
5th
7th
Gross A, et al. Antimicrob Agents Chemother. 2014; 58:5262‐8.
“Double coverage” talk
• Guidelines recommend anti‐pseudomonal beta‐lactam plus an anti‐pseudomonal fluoroquinolone (preferred) or an aminoglycoside (alternative) in combination
Mandell LA, et al. IDSA/ATS Guidelines for CAP. CID. 2007; 44:S27‐72.
Reprinted from Master RN, et al. Analysis of resistance, cross‐resistance and antimicrobial combinations forPseudomonas aeruginosa isolates from 1997 to 2009. Int J Antimicrob Agents. 2011; 38: 291‐5, Copyright 2011, with permission from the
International Society of Chemotherapy.
**Keep in mind that blood isolates appear to be somewhat MORE susceptible – lower respiratory tract isolates may have higher rates of antibiotic resistance
P. aeruginosa resistance to FQs is well documentedCross resistance is also high
• Single center in Columbia, SC among 178 P. aeruginosaisolates with 17% resistance (n=30) to piperacillin/tazobactam, only 3 (10%) were susceptible to ciprofloxacin– Other institutions have supported these data ranging from
10‐21% susceptibility to FQs– Restrictions placed on ciprofloxacin use increased
susceptibility over a 4‐year period in 1 institution
• From The Surveillance Network (TSN) database, N=3731 aztreonam resistant isolates, 51% were also resistant to FQs
Master RN, et al. Int J Antimicrob Agents. 2011; 38: 291‐5.Internal Data, Palmetto Health Richland
Bosso JA, Gomez J. Abstract #232, ID Week 2014. Philadelphia, PA.
Although not stated explicitly in guidelines, need combination antibiogram
• Issue: What is the (your) minimum acceptable susceptibility (MAS) for treating patients hospitalized with CAP? – Survey of 360 pharmacists & physicians suggests MAS of 94%
(75th percentile) for pneumonia + bacteremia (Internal data, manuscript in preparation)
• Guidelines do not comment on a minimum acceptable susceptibility
• Use of local data with local guidelines is emphasized, yet use of combination antibiograms is not mentioned
Hagedorn M, et al. Clinician perception of minimum acceptable susceptibility for empirical antibiotic selection. Presented at ASHP Midyear Clinical Meeting, 7‐12 December 2014, Anaheim, CA. Abstract#6‐481.
Example of a Combination Antibiogram for P. aeruginosa
Susceptibility to single agent and combination antibiotic therapy
Beta‐lactamIsolates
, n
Single agent,%
Ciprofloxacin, %
Tobramycin, %
Amikacin, %
Colistin, %
Aztreonam 123 74.0 82.9 92.7 95.9 88.2
Cefepime 123 74.8 79.7 90.2 94.2 85.3
Ceftazidime 123 79.7 84.6 92.7 96.7 91.2
Imipenem 123 72.4 78.0 90.2 94.2 73.5
Meropenem 123 77.2 80.5 90.2 94.2 79.4
Piperacillin/ Tazobactam 123 76.4 82.1 91.1 95.0 88.2
Smith ZR, et al. J Oncol Pharm Pract. 2015. Available at: http://opp.sagepub.com/content/early/2015/05/08/1078155215586081.full.pdf+html
2015 ASHP Midyear Clinical Meeting Making Sense of Infectious Diseases Clinical Practice Guidelines
© 2015 American Society of Health-System Pharmacists 16

Managing CAP patients with allergies• Patients with beta‐lactam allergies compared to those without allergies
– Increased consumption of costly and more toxic antibiotics– Often receive second line agents with inferior/less clinical evidence
• Aztreonam is listed as alternative agent to substitute for beta‐lactam in PCN‐allergic patients
– Of 568 PSA isolates at hospital system (3 hospitals) over 2‐year period, aztreonam susceptibility was 51%
• **Remember, still poor susceptibility to FQ among aztreonam‐resistant isolates too.
Pathogen Percent Susceptibility to Aztreonam
Enterobacter sp. (n=1029) 76.9%
Pseudomonas spp. (n=1971) 68.5%
Sutherland CA, Nicolau DP. Clin Ther. 2015; 37:1564‐71.Internal Data, Palmetto Health Richland, 2014..
Can doxycycline have a bigger role?Study Intervention Outcomes Comments
Mokabberi R, et al. J Clin Pharm Ther 2010
RCT, single center –Doxycycline (n=35) vs. levofloxacin (n=30) for non‐ICU CAPReceived 10 days of tx, could transition to PO at anytime
LOS: D: 4 (1.8), L: 5.7 (2.05) days (p<0.001)Antibx costs sig lower in doxy armADE: no difference between groups, mild.No readmissions within 2 months
Patients had a pneumoniaseverity index=60 at admission
High risk excluded but ~30% had underlying COPD and DM
Teh B, et al. Clin Micro Infect 2012
Post‐hoc analysis of Australian CAP Study comparing beta‐lactam +Doxy (n=178) vs. beta‐lactam+Macrolide (n=680)
No difference in 30‐day mortalityMedian days to clinical stability & LOS lower in doxy arm
PSI>4 was equal in both groups, but “sicker” patients may have received macrolide tx. Results consistent among typical/atypical pathogens
Ailani RK, et al. Arch Intern Med 1999
RCT, Doxycycline (n=43) vs. other antibx (n=44) for CAPPatients excluded with severe disease requiring intubation or ICU admission
Time to clinical response, median LOS and cost of hosp all significantly less in doxycycline arm
Trial conducted in mid‐1990’s, may not reflect current status of antibiotic resistance. PCN and TCN resistance reported 10% and 17% in area at time.
Mokabberi R, et al. J Clin Pharm Ther. 2010 35:195‐200. Teh B, et al. Clin Microbiol Infect 2012; 18:E71‐3.Ailani RK, et al. Arch Intern Med. 1999; 159:266‐70.
Additional issues for macrolides• Ray WA, et al. demonstrated increased risk of CV death in patients receiving 5 days
of azithromycin in a Tennessee CMS databaseCumulative incidence/1 million courses– No antibiotic (ref), 29.8 Amoxicillin, 31.5 Azithromycin, 85.2 (HR=2.88, 1.79‐4.63)
• Schembri S, et al. demonstrated similar risk of CV events and acute coronary syndrome in patients receiving clarithromycin for COPD/CAP in a UK population
• Increasing resistance among Mycoplasma isolates– Bebear C, et al. 2011– Principi N, et al. 2013
• Use of macrolides in HIV+ patients when Mycobacterium spp. infections not yet ruled out = may lead to an increased risk of resistance
Bebear C, et al. Future Microbiol. 2011; 6:423‐31. Ray WA, et al. N Engl J Med. 2012; 366:1881‐90.Principi N, Esposito S. JAC. 2013; 68:506‐11. Schembri S, et al. BMJ. 2013; 346:f1235.
Yamada M, et al. Ped Infect Dis J. 2012; 31:409‐11.
One additional potential benefit of doxycycline‐ Does doxycycline protect against CDI? ‐
• Single center, 5‐year study (2005‐2010)– N=2734 hospitalizations,
2305 unique patients
Overall CDI Rate
Doxy Arm No Doxy Arm
5.6 per 10,000 ptdays
1.67 per 10,000 pt days
8.11 per 10,000 pt days
Per day of doxycycline useAdjHR: 0.73 (0.56‐0.96), p=0.03
Doernberg SB, et al. CID. 2012; 55:615‐20.
Variables No Doxy, n=1668
Doxy, n=1066
Age, mean 52.4±16.4 53.9±15.9
Male, n (%) 1037 (62) 735 (69)
Nonwhite 1099 (66) 693 (65)
Charlson comorbidity 2.4 (0.1) 2.7 (0.1)
Pneumonia 117 (7) 444 (42)
Ceftriaxone, days 3 (2‐5) 3 (3‐5)
Additional antibx, days 2 (0‐6.5) 0 (0‐4)
CDI 38 (2) 5 (0.5)
LOS prior to CDI 7 (4‐14) 7 (4‐12)
Surgical Prophylaxis & Prophylaxis in Open Fractures
Surgical Prophylaxis – it’s beyond Surgical Care Improvement Project (SCIP)
• As of 2015, CMS has retired all but one metric related to surgical prophylaxis
• SCIP‐Inf‐4 is the only remaining metric and it is currently suspended– Cardiac surgery patients with controlled postoperative
blood glucose
• ASHP/Surgical Infection Society (SIS)/SHEA Guidelines published in 2013– Data used through June 2010 Available at:
http://www.jointcommission.org/specifications_manual_for_national_hospital_inpatient_quality_measures.aspx
2015 ASHP Midyear Clinical Meeting Making Sense of Infectious Diseases Clinical Practice Guidelines
© 2015 American Society of Health-System Pharmacists 17

Question 13:At your institution, in which patient populations are methicillin‐resistant Staphylococcus aureus nasal colonization screening and treatment recommended?
Coronary artery bypass grafting onlyCABG + major orthopedic surgeriesMajority of major, non‐emergent surgeriesUnsure of our practices
When is MRSA colonization screening and treatment appropriate?
• Why worry about nasal carriage?– Associated with a RR=7.1 for developing surgical
site infection (SSI)
– Most cases of SSI secondary to S. aureus have been shown to be endogenous
– Correlation between MRSA nasal carriage and SSI in CABG clearly established
Kluytmans J, et al. J Infect Dis. 1995; 171:216‐9.von Eiff C, et al. N Engl J Med. 2001; 344:11‐6.
Datta R, Huang SS. CID. 2008; 47:176‐81.
When is MRSA colonization screening and treatment appropriate?
• ASHP/IDSA Guidelines– Orthopedic surgery recommendation is to screen
and decolonize all positive S. aureus patients with mupirocin
• IHI Guidelines
IHI Available at: http://www.ihi.org/Topics/SSIHipKnee/Pages/default.aspxBratzler DW, et al. AJHP. 2013; 70:195‐283.
– #3: Screen patients for Staphylococcus aureus (SA) carriage and decolonize SA carriers with 5 days of intranasal mupirocin
Study Study Design Population ReceivingDecolonization
Decolonizing Intervention
Relative Risk (RR) (95% CI) of Infection
Kalmeijer, et al. 2002
RCT All patients Mupirocin RR=0.59 (0.19, 1.83)
Price, et al. 2008
Observational Only S. aureus colonized pts.
Mupirocin RR=0.21 (0.01, 4.48)
Rao, et al. 2008 Observational Only S. aureuscolonized pts.
Mupirocin + Chlorhexidine
RR=0.11 (0.01, 0.82)
Kim, et al. 2010 Observational Only S. aureus colonized pts.
Mupirocin + Chlorhexidine
RR=0.41 (0.21, 0.80)
IHI Guidelines Available at: http://www.ihi.org/Topics/SSIHipKnee/Pages/default.aspx
Overall, weight analysis: RR=0.40 (0.23, 0.69)
Project JOINTS (Joining Organizations IN Tackling SSIs)
Preoperative S. aureus Screening/Decolonization Protocol before Total joint
arthroplasty (TJA)• 22.2% (228/1028) S. aureus colonization rate and only 0.8% MRSA
• Prosthetic joint infection (PJI) rate was higher in S. aureus carriers (3.9%, 9/228) than among non‐carriers (2.0%, 16/800), not statistically significant
• Treated & untreated carriers showed no statistically significant differences in overall PJI, 3.4% (3/89) vs. 4.3% (6/139), p=0.219– S. aureus PJI was 2.2% in treated and untreated, p=0.470
• Most of the S. aureus PJI occurred in non‐carriers, suggesting lack of causal relation between nasal colonization & S. aureus PJI – No clear benefit from screening/decolonizing carriers could be
demonstrated, especially given the low event rate overall
Sousa RJG, et al. J Arthroplasty. 2015.
MRSA Screening in Orthopedic Surgery
• Kim, et al. J Bone Joint Surg Am, 2010– Suggests that if institutional rates of SSI are high,
screening and de‐colonization may be appropriate—High rates of SSI no clearly defined, however rates of <3%
would be difficult to demonstrate positive impact of screening
• Dilogo, et al. Acta Med Indones, 2013– Lack of evidence to support linkage between MRSA
carrier state in patients, family members and medical personnel with SSI
Kim DH, et al. J Bone Joint Surg Am. 2010; 92:1820‐6.Dilogo IH, et al. Acta Med Indones. 2013; 45:202‐5.
2015 ASHP Midyear Clinical Meeting Making Sense of Infectious Diseases Clinical Practice Guidelines
© 2015 American Society of Health-System Pharmacists 18

Mupirocin resistance: Reason for concern?
Study Country Years No.Patients/No. of Isolates
Resistance Prevalence
Miller, et al. Canada 1990‐93 231/310 2.7 – 65%
Vivoni, et al. Brazil 1990‐95, 1996‐2000
43/43, 89/108 65%, 15%
Jones, et al. USA 2002 – 2004 338/302 13.2%
Walker, et al. USA 2004 50‐100 isolatesper era (5 eras)
67%
Lee, et al. Switzerland 2011 150/75 9 – 81%
Desroches, et al. France 2013 367 (isolates) 2.2%
Poovelikunnel T, et al. JAC. 2015.
Strategies for mupirocin use• Quantify and evaluate the need for and effectiveness of
mupirocin in your population– Cost effectiveness established?– Are alternatives needed? (Brown S, et al. APIC 2014, povidine‐
iodine nasal antiseptic a.m. of surgery)
• Monitor mupirocin resistance locally (if possible)– Models demonstrate (as expected) continued use of mupirocin
is predictive of resistance
• Monitor use of mupirocin and potential spread of multidrug resistance— Transmissible resistance has been demonstrated
Deeny SR, et al. JAC. 2015; 70:3366‐78.Poovelikunnel T, et al. JAC 2015.
How much is cefazolin contributing to reducing gram‐negative bacterial (GNB) SSI infections?• Best answer to this is we don’t know for sure
– While SSI secondary to GNB have decreased from 56% in 1986 to 34% in 2003, is this influenced by use of cefazolin? S. aureus, including MRSA, increased over same time frame
• Impact in beta‐lactam allergic patients?– Guidelines highlight the “low risk of cross‐reactivity” and recommend
avoiding cefazolin in patients with history of IgE‐mediated reaction– For gram‐positive cocci coverage, clindamycin and vancomycin are
primarily the alternatives provided unless need for gram‐negative coverage known (aztreonam, AG or FQ listed as alternatives)
• Adding vancomycin to cefazolin (best of both worlds?)– Addition resulted in postoperative acute kidney injury
Courtney PM, et al. Clin Orthop Relat Res. 2015; 473:2197‐203.Gaynes R, et al. CID. 2005; 41:848‐54.
Weigelt JA, et al. Am J Infect Control. 2010; 38:112‐20.
Open Fractures & Antibiotic Prophylaxis
Question 14:What is the most appropriate antibiotic selection for a Grade II open tibial fracture (2.5 cm wound, no visual contamination)?
No antibiotics indicatedCefazolin monotherapyCefazolin plus vancomycinVancomycin or cefazolin + aminoglycoside
Open fracture: Antibiotic Prophylaxis
Hoff WS, et al. J Trauma. 2011;70:751‐4.Hauser CJ, et al. Surg Infect (Larchmt). 2006;7:379‐405.
Gustillo Grade East Practice Guidelines AntibioticRecommendation1
Surgical InfectionSociety Antibiotic Recommendations
Duration of Prophylaxis
Grade I (<1 cm wound) Cefazolin
Cefazolin
24 hours after wound closure
Grade II (>1 cm wound withoutextensive soft tissue injury)
Cefazolin2 24 hours (SIS)48 hours (EAST)
Grade III (>10cm wound)IIIA: Adequate soft tissue coverageIIIB: Significant soft tissue lossIIIC: Associated vascular injury
Cefazolin + Aminoglycoside (once‐daily dosing)
48‐72 hours after initial injury, not to exceed 24 hours post wound closure
1Add penicillin for contamination where Clostridium spp. likely2Once‐daily dosing of aminoglycosides can be considered in Grade II
2015 ASHP Midyear Clinical Meeting Making Sense of Infectious Diseases Clinical Practice Guidelines
© 2015 American Society of Health-System Pharmacists 19
What do trauma surgeons think?Variable Grade I Grade II Grade III
Antibiotic Selection – use of aminoglycosides
2.4% (9/379) 15% (57/379) 59% (224/379), IIIa67% (253/379), IIIb
Use ofaminoglycosides w/ visual contamination
29.8% (113/179) ‐‐ 76.3% (289/379), IIIb
Duration of antibiotic prophylaxis1 for 48hr
29% (110/379) 33% (125/379) 39% (147/379)
154.4% continued antibiotics until next debridement regardless of Grade
Obremskey W, et al. J Orthop Trauma. 2014; 28:e198‐202.
What is the most appropriate duration?
• Single center study, n=1492 open fractures– Infection rate of 3.6% (54/1492)
• Patients received antibiotics (cefuroxime in 72% of cases) according to physician selection– Duration of antibiotics (24 hour (ref), 48‐72 hours, 96‐
120 hours, and >120hours) was not predictive of infection
– Only Grade III fractures (Grade I, ref) (aOR=12.5, 95% CI: 5.2‐30.4) and vascular injury (univariate analysis, OR=5.1,95% CI: 2.4‐10.7) were associated with increased risk of infection
Dunkel N, et al. Bone Joint J. 2013; 95‐B(6): 831‐7.
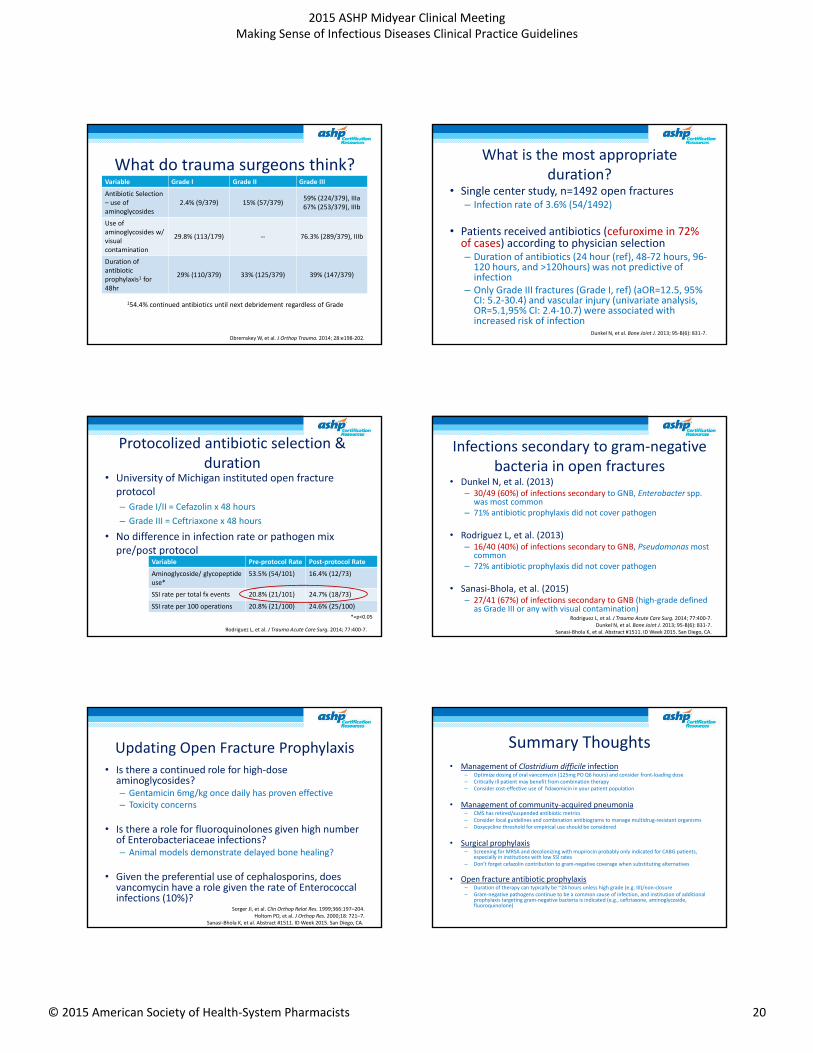
Protocolized antibiotic selection & duration
• University of Michigan instituted open fracture protocol– Grade I/II = Cefazolin x 48 hours– Grade III = Ceftriaxone x 48 hours
• No difference in infection rate or pathogen mix pre/post protocol
Rodriguez L, et al. J Trauma Acute Care Surg. 2014; 77:400‐7.
Variable Pre‐protocol Rate Post‐protocol Rate
Aminoglycoside/ glycopeptideuse*
53.5% (54/101) 16.4% (12/73)
SSI rate per total fx events 20.8% (21/101) 24.7% (18/73)
SSI rate per 100 operations 20.8% (21/100) 24.6% (25/100)*=p<0.05
Infections secondary to gram‐negative bacteria in open fractures
• Dunkel N, et al. (2013)– 30/49 (60%) of infections secondary to GNB, Enterobacter spp.
was most common– 71% antibiotic prophylaxis did not cover pathogen
• Rodriguez L, et al. (2013)– 16/40 (40%) of infections secondary to GNB, Pseudomonas most
common– 72% antibiotic prophylaxis did not cover pathogen
• Sanasi‐Bhola, et al. (2015)– 27/41 (67%) of infections secondary to GNB (high‐grade defined
as Grade III or any with visual contamination)Rodriguez L, et al. J Trauma Acute Care Surg. 2014; 77:400‐7.
Dunkel N, et al. Bone Joint J. 2013; 95‐B(6): 831‐7.Sanasi‐Bhola K, et al. Abstract #1511. ID Week 2015. San Diego, CA.
Updating Open Fracture Prophylaxis• Is there a continued role for high‐dose
aminoglycosides? – Gentamicin 6mg/kg once daily has proven effective– Toxicity concerns
• Is there a role for fluoroquinolones given high number of Enterobacteriaceae infections?– Animal models demonstrate delayed bone healing?
• Given the preferential use of cephalosporins, does vancomycin have a role given the rate of Enterococcal infections (10%)?
Sorger JI, et al. Clin Orthop Relat Res. 1999;366:197–204.Holtom PD, et al. J Orthop Res. 2000;18: 721–7.
Sanasi‐Bhola K, et al. Abstract #1511. ID Week 2015. San Diego, CA.
Summary Thoughts• Management of Clostridium difficile infection
– Optimize dosing of oral vancomycin (125mg PO Q6 hours) and consider front‐loading dose– Critically ill patient may benefit from combination therapy – Consider cost‐effective use of fidaxomicin in your patient population
• Management of community‐acquired pneumonia– CMS has retired/suspended antibiotic metrics– Consider local guidelines and combination antibiograms to manage multidrug‐resistant organisms– Doxycycline threshold for empirical use should be considered
• Surgical prophylaxis– Screening for MRSA and decolonizing with mupirocin probably only indicated for CABG patients,
especially in institutions with low SSI rates– Don’t forget cefazolin contribution to gram‐negative coverage when substituting alternatives
• Open fracture antibiotic prophylaxis– Duration of therapy can typically be ~24 hours unless high grade (e.g. III)/non‐closure– Gram‐negative pathogens continue to be a common cause of infection, and institution of additional
prophylaxis targeting gram‐negative bacteria is indicated (e.g., ceftriaxone, aminoglycoside, fluoroquinolone)
2015 ASHP Midyear Clinical Meeting Making Sense of Infectious Diseases Clinical Practice Guidelines
© 2015 American Society of Health-System Pharmacists 20

GRADERubric
Lipsky BA et al. Clin Infect Dis.2012; 54:1679‐84. by permission of the Infectious Diseases Society of America.
2015 ASHP Midyear Clinical Meeting Making Sense of Infectious Diseases Clinical Practice Guidelines
© 2015 American Society of Health-System Pharmacists 21

Van Hal SJ, Lodise TP, Paterson DL. The clinical significance of vancomycin minimum inhibitory concentration in Staphylococcus aureus infections: a systematic review and meta‐analysis. Clin Infect Dis. 2012;54:755‐71,
by permission of the Infectious Diseases Society of America.
OR for treatment failure = 2.69 (95% CI 1.60‐4.51)
High vs. Low Vancomycin MICs in Staphylococcus aureus BSIs
2015 ASHP Midyear Clinical Meeting Making Sense of Infectious Diseases Clinical Practice Guidelines
© 2015 American Society of Health-System Pharmacists 22

Answer Key:
1. D 2. D 3. C 4. B 5. Audience Polling Question 6. D 7. Audience Polling Question 8. A 9. B 10. C 11. A, B, & C 12. D 13. Audience Polling Question 14. B
2015 ASHP Midyear Clinical Meeting Making Sense of Infectious Diseases Clinical Practice Guidelines
© 2015 American Society of Health-System Pharmacists 1





























