Embed Size (px)
Citation preview

SEARCH 011: Peripheral Reservoir of HIV DNA in Monocytes Pivotal to Cognition in HIV Version 1.5, August 6, 2012
PI: V. Valcour
CLINICAL STUDY PROTOCOLSEARCH 011: Peripheral Reservoir of HIV DNA in Monocytes Pivotal to Cognition in HIV
PROTOCOL TEAMPrincipal Investigator:Victor Valcour MDAssistant ProfessorMemory and Aging Center, UCSF675 Nelson Rising Lane, Suite 190San Francisco, CA 94158email: [email protected]: 415-476-1895fax: 415-476-4800Co-InvestigatorsJintanat Ananworanich MD, PhD Protocol Clinical DirectorChief, SEARCHThai Red Cross AIDS Research Center 104 Rajdamri Rd. Tower 2, 2nd floorPathumwan, Bangkok 10330email: [email protected]: 011-66-2-254-2566-9fax: 011-66-2-254-2567
Silvia Ratto-Kim PhD, Protocol Laboratory DirectorAssociate Researcher, HACRP and United Sates Military HIV Research ProgramHenry M. Jackson Foundation13 Taft Court. Rockville MD 20850email: [email protected] : +1301 251-8354 fax : +1301 762-4177
Victor DeGruttola PhD, Protocol Biostatistician655 Huntington AvenueBuilding II, Room 439ABoston, Massachusetts, USA 02115email: [email protected]: 617 432-2820
Mark deSouza PhD, MPH, Associate Laboratory InvestigatorDepartment of Retrovirology, USAMC-AFRIMS315/6 Rajvithi Rd, Bangkok, Thailandemail: [email protected]: 011-66-2-644-4888 ext 1515fax: 011-66-2-644-4824
Yotin Chinvarun MDDivision of Neurology, Department of MedicinePhramongkutklao Hospital315/6 Rajvithi Rd.Bangkok 10400, Thailandemail: [email protected]: 66 02-354-7660
Pasiri Sithinamsuwan MD, Associate Clinical InvestigatorNeurologist, Co-investigatorDivision of Neurology, Department of Medicine315/6 Rajvithi Rd.Bangkok 10400, ThailandEmail: [email protected]: 01-847-6034
Nittaya Phanuphak MD, Associate Clinical InvestigatorThai Red Cross AIDS Research Centre104 Rajdamri Road, PathumwanBangkok 10330, Thailandemail: [email protected]: 66 2 253 0996fax: 66 2 253 0998
James Fletcher MD, Co-investigatorSEARCHThai Red Cross AIDS Research Center 104 Rajdamri Rd. Tower 2, 2nd floorPathumwan, Bangkok 10330email: [email protected]: 011-66-22-254-2566-9fax: 011-66-2-254-2567
Thep Chalermchai MD, Co-investigatorSEARCHThai Red Cross AIDS Research Center 104 Rajdamri Rd. Tower 2, 2nd floorPathumwan, Bangkok 10330email: [email protected]: 011-66-2-254-2566-9fax: 011-66-2-254-2567
Bruce Shiramizu MD, Associate Laboratory Investigator
Page 1 of 31
SEARCH 011: Peripheral Reservoir of HIV DNA in Monocytes Pivotal to Cognition in HIV Version 1.5, August 6, 2012
PI: V. Valcour Professor, HACRP, University of Hawaii3675 Kilauea Avenue, Leahi HospitalHonolulu, Hawaii USA 96816email: [email protected]
Alexandra Schuetz, Ph.D.Research ScientistDepartment of Retrovirology, USAMC-AFRIMS315/6 Rajvithi Rd, Bangkok, Thailandemail: [email protected]: 011-66-696-2700 x 4912fax: 011-66-2-644-4824
External ConsultantsBruce Brew MBBS MD FRACDepartment of Neurology Level 4 Xavier Building, St. Vincent's HospitalVictoria St, DarlinghurstSydney, Australia 2010email: [email protected]
David Clifford MDSeay Professor of Clinical Neuropharmacology in NeurologyWashington University School of MedicineNeurology, Box 8111660 South EuclidSaint Louis, Missouri, USA 63110email: [email protected]
Sukalaya Lerdlum MDDepartment of Radiology, Chulalongkorn Hospital and SEARCHThai Red Cross AIDS Research Center 104 Rajdamri Rd. Tower 2, 2nd floorPathumwan, Bangkok, Thailand 10330email: [email protected]
Robert Paul PhDAssistant Professor, University of MissouriBehavioral Neuroscience/NeuropsychologyOne University Blvd., 412 Stadler HallSt. Louis, Missouri, USA 63121 email: [email protected]
Pom Sailasuta PhDSpectroscopy Unit, Huntington Medical Research Institute, 10 Pico StreetPasadena, California, USA 91105
email: [email protected]
Cecilia Shikuma MDProfessor, Hawaii AIDS Clinical Research ProgramUniversity of Hawaii3675 Kilauea Avenue, Leahi HospitalHonolulu, Hawaii USA 96816email: [email protected]
Henrik Zetterberg MD PhDInstitute of Neuroscience and Physiology Department of Psychiatry and Neurochemistry The Sahlgrenska Academy at the University of Gothenburg S-431 80 Mölndal SWEDEN phone: 46 31 3430142
Nicolas Chomont MDVaccine and Gene Therapy Institute (VGTI) of Florida 11350 SW Village Parkway 3rd Floor Port St Lucie Florida, USA 34987 phone: +1 (772) 345-4788 fax: +1 (772) 345-3675 email: [email protected]
Clinical MonitorSomchai Sriplienchan, MD, MPHChief of disease preventionDepartment of Retrovirology, USAMC-AFRIMS315/6 Rajvithi Rd, Bangkok, ThailandE-Mail: [email protected] Number: 011-66-2-644-4888 ext 1505Fax number: 011-66-2-644-4824
Study NurseMs.Somporn Tipsuk RN Clinical nurseSouth East Asia Research Collaboration with Hawaii(SEARCH)Thai Red Cross AIDS Research Center 104 Rajdamri Rd. Tower 2, 2nd floorPathumwan, Bangkok 10330email: [email protected] : 011-66-2-254-2566-9fax: 011-66-2-254-2567
SPONSOR AND FUNDING AGENCY
Page 2 of 31

SEARCH 011: Peripheral Reservoir of HIV DNA in Monocytes Pivotal to Cognition in HIV Version 1.5, August 6, 2012
PI: V. Valcour National Institute of Neurological Disorders and Stroke (NINDS)/NIH Bethesda, Maryland, USA.
STUDY CLINICAL SITESPhramongkutklao Medical CenterChulalongkorn University including the Thai Red Cross AIDS Research Center
Page 3 of 31
SEARCH 011: Peripheral Reservoir of HIV DNA in Monocytes Pivotal to Cognition in HIV Version 1.5, August 6, 2012
PI: V. Valcour SCHEMATitleSEARCH 011: Peripheral Reservoir of HIV DNA in Monocytes Pivotal to Cognition in HIV
ParticipantsSixty HIV+ individuals stratified by pre-HAART peripheral blood mononuclear cell (PBMC) HIV DNA level (30 above or equal to 5000 copies/106 cells and 30 below 5000 copies/106 cells). All HIV-subjects will be ARV-naïve and intend to start ARV in the month following enrollment.
Primary Objectives(1) To determine the long-term relationship between cognition and HIV DNA in circulating PBMCs and monocytes (CD14+ PBMCs) among patients initiating HAART for the first time(2) To define the longitudinal relationships between CD14+ HIV DNA and: (a) cerebrospinal fluid (CSF) biomarkers of immune activation (neopterin, MCP-1, and IL-6), (b) CD14+ supernatant markers of immune activation (MCP-1 and IL-6), and (c) increased myoinositol/creatine ratio by MRS(3) To prospectively determine the performance characteristics of the International HIV Dementia Scale and the neuropsychological z-score composite summary score (NPZcomp) in Thailand
Study DesignThis application focuses on the role of PBMC HIV DNA in HIV-associated neurocognitive disorders (HAND). Early evidence suggests it is a robust marker of HAND in ARV-naïve and ARV-treated individuals. This study is designed to prospectively determine the predictive value of HIV DNA in an HIV population from Bangkok, Thailand initiating HAART for the first time. Primary dependent variables include neuropsychological testing summary scores, consensus diagnostic categorization of HAND, and blood, CSF and MRS markers of inflammation. CSF HIV RNA is a principle covariate. We propose that HIV DNA will remain detectable in a subset of patients despite undetectable plasma and CSF HIV DNA and that HIV DNA levels in CD14+ PBMCs will correlate to markers of inflammation at all time points. We posit that baseline HIV DNA in CD14+ PBMCs will predict attenuated cognitive recovery. Finally, we intend to test the performance characteristics of both the NPZcomp and the International HIV Dementia Scale for the diagnostic categories of HAND in Thailand.
Study ProcedureHIV-infected Individuals intending to initiate ARV for the first time (n=60) will be identified in Bangkok, Thailand and screened for PBMC HIV DNA level. Individuals will be stratified by high (more than or equal to 5000 copies/106 cells, n=30) or low (less than 5000 copies/106 cells, n=30). All HIV individuals will undergo evaluations at baseline, 6 months, and annually for up to 4 years and will include: brain MRI/MRS neuropsychological testing, neurological examination, blood draw. Lumbar puncture will be optional at baseline and 12 months for persons who agree to participate to this study procedure. Blood monocytes will be separated and cultured to obtain supernatants to assess inflammation and to determine HIV DNA levels in cellular subsets (CD14+, CD14-). Blinded to HIV DNA levels and international HIV Dementia Scale data, a consensus conference will determine HAND diagnoses using 2007 criteria.1 Neuropsychological data will be compared to previously enrolled, age- and education-stratified HIV-negative controls from Bangkok.
Study DurationSix years with two years of enrollment and four years duration per enrolled participant.
SponsorNational Institute of Neurological Disorders and Stroke, National Institutes of Health, USA
Study SitesCoordination site:
SEARCH/The Thai Red Cross AIDS Research Centre (TRCARC), 104 Rajdamri Road, Pathumwan Bangkok 10330, Thailand
Version 1.5 Page 4 of 31
SEARCH 011: Peripheral Reservoir of HIV DNA in Monocytes Pivotal to Cognition in HIV Version 1.5, August 6, 2012
PI: V. Valcour Clinical sites:
Phramongkutklao Medical Center (PMK), 315 Rajvithi Rd Bangkok 10400, Thailand Chulalongkorn University Hospital and TRCARC, Rajdamri Road, Pathumwan, Bangkok 10330, Thailand
Data management and statistical support sites:
SEARCH, Bangkok, Thailand Department of Biostatistics, Harvard School of Public Health
Laboratory sites:
AFRIMS Department of Retrovirology (U.S. Component), 315/6 Rajvithi Rd., Bangkok 10400, Thailand Hawaii HIV and Immunobiology Lab/HACRP, University of Hawaii, Honolulu, Hawaii, USA Thai Red Cross AIDS Research Centre (TRCARC), 104 Rajdamri Road, Pathumwan Bangkok 10330,
Thailand Vaccine and Gene Therapy Institute (VGTI) of Florida, 11350 SW Village Parkway, 3rd Floor, Port St. Lucie,
Florida, USA 34987 Institute of Neuroscience and Physiology, Department of Psychiatry and Neurochemistry, The Sahlgrenska
Academy at the University of Gothenburg S-431 80 Mölndal, Sweden
Version 1.5 Page 5 of 31

SEARCH 011: Peripheral Reservoir of HIV DNA in Monocytes Pivotal to Cognition in HIV Version 1.5, August 6, 2012
PI: V. Valcour TABLE OF CONTENTS
Protocol title and personnel..........................................................................................................................1Schema........................................................................................................................................................4Protocol:1. Abbreviations used..................................................................................................................................72. Ethics.......................................................................................................................................................83. Location of study.....................................................................................................................................94. Duration of study...................................................................................................................................105. Objectives..............................................................................................................................................116. Background and significance................................................................................................................127. Study population...................................................................................................................................158. Study design and methodology............................................................................................................189. Laboratory procedures.........................................................................................................................2010. Risks, benefits, research-related injury and confidentiality.................................................................2211. Data collection, management, and analysis........................................................................................2412. Participant compensation....................................................................................................................2513. Literature cited.....................................................................................................................................26
Appendix I (Table of follow-up for subjects)...............................................................................................30
Version 1.5 Page 6 of 31

SEARCH 011: Peripheral Reservoir of HIV DNA in Monocytes Pivotal to Cognition in HIV Version 1.5, August 6, 2012
PI: V. Valcour 1. LIST OF ABBREVIATIONS AND DEFINITIONS OF TERMS
3TC lamivudineAAN American Academy of NeurologyAb AntibodyADL Activities of Daily LivingAFRIMS Armed Forces Research Institute of Medical SciencesAIDS Acquired immunodeficiency syndromeAPNAC Asia Pacific NeuroAIDS ConsortiumARV antiretroviral therapyBD Becton-DickinsonCAR capacity assessment recordCBC Complete blood countCDR Clinical Dementia Rating ScaleCFR Code of Federal Regulations (USA)Cho cholineCIDI Composite International Diagnostic InterviewCr creatineCRF Case Report FormCRF01_AE Circulating Recombinant Form AECRR continuing review reportCSF cerebrospinal fluidd4T stavudine DoD Department of DefenseDMSO dimethyl sulfoxideDSM Diagnostic and Statistical Manual of Mental DisordersDTI Diffusion Tensor ImagingFACS Fluorescence Activated Cell SorterFDA Food and Drug AdministrationFWA Federal wide assuranceGCP Good Clinical PracticeGDS Global Deficit ScoreGNPI Global Neuropsychological ImpairmentGPO Government Pharmaceutical OrganizationGPO-vir combination ARV pill of stavudine, lamivudine, and nevirapineGPO-virZ combination ARV pill of zidovudine, lamivudine, and nevirapine HAART highly active antiretroviral therapyHACRP Hawaii AIDS Clinical Research ProgramHAD HIV-associated DementiaHAND HIV-associated neurocognitive disorderHIV human immunodeficiency virusHSRRB Human Subjects Research Review Board (WRAIR)IADL Instrumental Activity of Daily LivingICD International Classification of DiseasesICH International Conference on HarmonizationIL- InterleukinIRB Institutional Review BoardLP Lumbar PunctureMCP-1 monocyte chemotactic protein-1MCMD Minor Cognitive Motor DisorderMI myoinositol M/MФ monocyte/macrophageMOPH Ministry of Public Health
Version 1.5 Page 7 of 31

SEARCH 011: Peripheral Reservoir of HIV DNA in Monocytes Pivotal to Cognition in HIV Version 1.5, August 6, 2012
PI: V. Valcour MRI magnetic resonance imagingMRS magnetic resonance spectroscopyNAA N-acetyl-aspartate National Institutes of Neurological Disorders and Stroke/National Institutes of HealthNVP nevirapineNPZcomp neuropsychological z-score composite summary scoreOHRP Office for Human Research ProtectionsPAOFI Patients Assessment of Own Functioning InventoryPBMC peripheral mononuclear cellsPCR Polymerase Chain ReactionPI Principal InvestigatorPIN Personal Identification NumberPMK Phramongkutklao Medical CenterPOC Point of contactPTT Prothrombin Time / Partial Thromboplastin TimeRNA ribonucleic acidRTA Royal Thai ArmySAS Statistical Analysis SystemSEARCH Southeast Asia Research Collaboration with HawaiiSIV Simian Immunodeficiency VirusTNF- Tumor Necrosis FactorTRCARC Thai Red Cross AIDS Research CenterUH University of HawaiiULN upper limit of normalUnited States Army Medical Center – Armed Forces Research Institute of the Medical SciencesUSAMMDA U.S. Army Medical Materiel and Development AgencyUSAMRMC U.S. Army Medical Research and Materiel CommandVGTI Vaccine and Gene Therapy InstituteWHO World Health OrganizationWRAIR Walter Reed Army Institute of ResearchZDV zidovudine
2. ETHICS2.1 Institutional Review Boards (IRBs)The Principal Investigator (PI) agrees to provide the Institutional Review Boards (IRBs) with all appropriate materials, including the protocol, proposed informed consent document, other written participant information, and any proposed advertising material and any changes made to these documents subsequent to submission. This study will not be initiated until appropriate IRB approvals of the protocol and informed consent document have been obtained in writing by the Principal Investigator. Appropriate reports on the progress of the study by the Principal Investigator will be made to the IRBs and the Sponsor in accordance with applicable Thai and U.S. governing regulations and in agreement with policy established by the Sponsor.
2.2 Office for Human Research Protections (OHRP) or Department of Defense (DoD) Assurance numbers of participating Institutions:
Chulalongkorn University Hospital (SEARCH, Thai Red Cross) FWA00000943Harvard School of Public Health FWA00002642Royal Thai Army Medical Department (Phramongkutklao Medical Center) FWA00001813University of Hawaii FWA00003526University of California San Francisco FWA00003470WRAIR FWA00000015
Version 1.5 Page 8 of 31

SEARCH 011: Peripheral Reservoir of HIV DNA in Monocytes Pivotal to Cognition in HIV Version 1.5, August 6, 2012
PI: V. Valcour
2.3 Informed ConsentA properly executed, written, IRB-approved informed consent (in Thai), in compliance with the Declaration of Helsinki, guidelines of the International Conference on Harmonization (ICH) and U.S. law 45 CFR §46, shall be obtained from each participant prior to performing any of the screening assessments. The investigator shall provide a copy of the IRB-approved informed consent to the participant and the signed original shall be maintained in the participant’s record file. Attention is directed to the basic elements that need to be incorporated into the informed consent under U.S. Federal Regulations for Protection of Human Subjects (45 CFR §46.116[a] ). Templates for the informed consents are provided in Appendix II. It describes the aspects involved in study participation. It is the investigator’s (or designee’s) responsibility to obtain this written informed consent from the participant, after adequate explanation of the aims, methods, anticipated benefits, and potential hazards of the study and before any protocol-specific procedures are administered. When decisional capacity is not clear, a legally authorized surrogate signs consent with the participant. In such cases, capacity is re-assessed at future visits and if the participant regains capacity to consent, they will be consented at that time.
3. Location of StudyCoordination site:
SEARCH/The Thai Red Cross AIDS Research Centre (TRCARC), 104 Rajdamri Road, Pathumwan, Bangkok 10330, ThailandClinical sites:
Phramongkutklao Medical Center (PMK), 315 Rajvithi Rd Bangkok 10400, Thailand Chulalongkorn University Hospital and TRCARC, Rajdamri Road, Pathumwan, Bangkok 10330, Thailand
Data management and statistical support sites:
SEARCH, Bangkok, Thailand Department of Biostatistics, Harvard School of Public Health
Laboratory sites:
AFRIMS Department of Retrovirology (U.S. Component), 315/6 Rajvithi Rd., Bangkok 10400, Thailand Hawaii HIV and Immunobiology Lab/HACRP, University of Hawaii, Honolulu, Hawaii, USA Thai Red Cross AIDS Research Centre (TRCARC), 104 Rajdamri Road, Pathumwan Bangkok 10330,
Thailand Institute of Neuroscience and Physiology, Department of Psychiatry and Neurochemistry, The Sahlgrenska
Academy at the University of Gothenburg, Sweden Vaccine and Gene Therapy Institute (VGTI) of Florida, 11350 SW Village Parkway, 3rd Floor, Port St. Lucie,
Florida, USA 34987
3.1 Study Responsibilities (by Institution)
SEARCH/The Thai Red Cross AIDS Research Centre (TRCARC): SEARCH will coordinate the clinical portion of this study, including recruitment of subjects, consenting, and clinical protocol management. Participants will be seen at SEARCH for neuropsychological testing and physical examinations. SEARCH will conduct screening PBMC HIV DNA assays and manage all study data. SEARCH operates in Thailand under TRCARC which utilizes the Chulalongkorn University IRB.
Phramongkutklao Medical Center (divisions of Neurology and Infectious Diseases, Department of Medicine): Participants will be screened and attend study visits at PMK Medical Center. Lumbar punctures will occur at PMK, Division of Neurology. The infectious diseases division will facilitate recruitment and assist with HIV care of the subjects. PMK laboratory will perform routine assays.
Version 1.5 Page 9 of 31

SEARCH 011: Peripheral Reservoir of HIV DNA in Monocytes Pivotal to Cognition in HIV Version 1.5, August 6, 2012
PI: V. Valcour Chulalongkorn University: Participants will undergo MRI/MRS at Chulalongkorn University Hospital.
AFRIMS, Department of Retrovirology and TRCARC: Storage of samples and immunological assays, including cell separation, will occur at AFRIMS and the TRCARC laboratory complex. Specimens will be stored and shipped to collaborators as indicated in the protocol.
HACRP (Hawaii HIV and Immunobiology Lab): HACRP will complete cells separation and assays of HIV DNA in subsets for enrollment and subsequent assays.
Harvard School of Public Health: Harvard will direct statistical analysis in coordination with the PI and the SEARCH data management team.
The Institute of Neuroscience and Physiology, Sweden: The Department of Psychiatry and Neurochemistry will perform novel biomarker assays.
VGTI (Florida): The laboratory at VGTI will complete cellular marker assays.
3.2 Personnel role and responsibilityVictor Valcour MD (Principal Investigator) will have final responsibility for all protocol issues and will primarily coordinate all administrative issues and over-see clinical issues with Dr. Ananworanich. He will work with Dr. DeGruttola for all data analyses and will direct all publications.
Jintanat Ananworanich MD (Protocol Clinical Director) will be responsible for all day-to-day clinical aspects of this protocol. She will directly manage protocol flow and report directly to the PI. She will be responsible for collection of clinical data and is listed as the point of contact (POC) in the consent forms.
Nittaya Phanuphak MD (Associate Clinical Investigator) will assist Dr. Ananworanich with all activities as outlined above. Pasiri Sithinamsuwan MD (Associate Clinical Investigator) will be the primary protocol neurologist and work directly with Drs. Ananworanich and Chalermchai to evaluate participants.
Silvia Ratto-Kim PhD (Protocol Laboratory Director) will direct all laboratory aspects of the protocol, including processing, storage, shipping and completion of all immunological assays with the direct assistance of Mark deSouza PhD, MPH (Associate Laboratory Investigator) who will be primarily responsible for day-to-day management of immunological assays. Bruce Shiramizu MD (Associate Laboratory Investigator) will oversee all HIV DNA assays in Thailand and the US.
Alexandra Schuetz, PhD (Research Scientist) has recently joined the Department of Retrovirology at AFRIMS. She will help with the day to day operation of the protocol. She will conduct part of the experiments proposed together with the laboratory technician. She will be under the direct supervision of Dr. deSouza.Victor DeGruttola PhD (Protocol Biostatistician) will direct statistical analyses.
Somporn Tipsuk RN will be the primary study nurse responsible for the day-to-day management of the study. She will also perform the neuropsychological testing.
There are several external consultants on the protocol. Bruce Brew MBBS MD FRAC will provide external expertise on the interpretation of CSF assays. David Clifford MD and Robert Paul PhD will provide external validation of consensus conference determinations. Sukalaya Lerdlum MD and Pom Sailasuta PhD will provide expertise in the interpretation of MRI and MRS data. Cecilia Shikuma MD will provide logistical support for fiscal and administrative issues at the University of Hawaii, as needed. Henrik Zetterberg MD PhD will supervise the performance of novel CSF biomarkers. Nicolas Chomont MD will supervise the performance of cellular marker assays.
4. Duration of studyJuly 2008– July 2014 (6 years – 2 years of recruitment and 4 years of follow-up)
Version 1.5 Page 10 of 31
SEARCH 011: Peripheral Reservoir of HIV DNA in Monocytes Pivotal to Cognition in HIV Version 1.5, August 6, 2012
PI: V. Valcour 5. ObjectivesActivated cells of the monocyte/macrophage (M/MФ) lineage play a pivotal role in the pathogenesis of HIV-associated Dementia (HAD)2. The accumulation of perivascular macrophages is observed in brain tissue of individuals with HAD and is a better marker of brain injury than is the presence of HIV virus. This pattern remains present in the era of HAART3. The expansion of peripheral M/MФ subsets displaying an activated phenotype is associated with HAD4 and with encephalopathy in SIV-infected macaques5.
Our recent data demonstrate that the level of HIV DNA within PBMCs is a better marker of cognitive dysfunction than is the degree to which expansion of M/MФ expressing an activated phenotype is observed. Our published data demonstrate a relationship between high PBMC HIV DNA and cognitive dysfunction in HAART-naïve patients with advanced HIV disease6 and among individuals heavily treated with HAART even when plasma HIV RNA is undetectable7. Based on preliminary data, PBMC HIV DNA likely represents the degree of HIV infection in circulating M/MФ rather than lymphocytes.
Whether mild cognitive impairment in HAART-treated patients represents an active or passive (permanent brain damage) process is an area of considerable controversy in the field of HIV cognitive disorders with important public health consequences in developed and resource-limited countries. We hypothesize that a critical aspect of incomplete cognitive recovery with HAART lies in the continued presence and brain trafficking of HIV-infected M/MФ resulting in continued active instigation of CNS inflammation, viral seeding, and neuronal dysfunction. The proposed work intends to define the long-term dynamic relationship between cognition and the inability of HAART to eradicate HIV DNA infection of the peripheral M/MФ reservoir. We will also define the relationship between M/MФ HIV DNA and CNS infection, inflammation, and neuroinjury by measuring such markers in CSF, monocyte (CD14+) supernatants, and by MR spectroscopy (MRS).
Specific Aim I: To determine the long-term relationship between cognition and HIV DNA in circulating PBMCs and monocytes (CD14+ PBMCs) among patients initiating HAART for the first timeHypotheses to be tested:
(a) HIV DNA will remain detectable 2, 3, 4, and 5 years after initiating HAART in a subset of patients despite suppressed plasma HIV RNA. Higher baseline HIV DNA will predict subsequent detectable HIV DNA at all time points.
(b) Baseline HIV DNA in PBMCs and in CD14+ cells will predict worse performance on the NPZcomp at 12 months. We will investigate the functional form of this relationship to determine if a cut-point (threshold) optimizes this relationship.
(c) Patients with detectable compared to undetectable CD14+ HIV DNA will perform worse on the concurrent NPZcomp at all time points, despite suppressed plasma HIV RNA. Baseline CD14+ HIV DNA level will be an important predictor of subsequent NPZcomp, even after adjusting for the current CD14+ HIV DNA level. .
(d) The relationship between monocyte HIV DNA and cognition will be independent of CSF HIV RNA at all time points
Specific Aim II: To define the longitudinal relationships between CD14+ HIV DNA and: (1) CSF biomarkers of immune activation (neopterin, MCP-1, and IL-6) and neuroinjury (neurofilament), (2) CD14+ supernatant markers of immune activation (MCP-1 and IL-6), and (3) increased myoinositol/creatine ratio by MRSHypothesis to be tested:
(a) CD14+ HIV DNA will correlate with concurrent CD14+ supernatant markers of immune activation (MCP-1 and IL-6), to concurrent elevated myoinositol/Creatine ratio in frontal white matter by MRS, and to concurrent CSF immune activation (neopterin, IL-6, and MCP-1) at all time points.
Specific AIM III: To prospectively determine the performance characteristics of the International HIV Dementia Scale and the NPZcomp in ThailandHypothesis to be tested:
Version 1.5 Page 11 of 31
SEARCH 011: Peripheral Reservoir of HIV DNA in Monocytes Pivotal to Cognition in HIV Version 1.5, August 6, 2012
PI: V. Valcour (a) Using a cut-off of 10, the International HIV Dementia Scale will accurately categorize great than 75% of HAD cases based on consensus conference diagnosis.
(b) The NPZcomp will accurately categorize more than 75% of cases as dementia/non-dementia. Improvement in discriminatory power of the NPZ metric may be possible by using linear discriminant function analysis.
Specific Aim IV: To test feasibility of diffusion tensor imaging in Bangkok(a) Corpus Callosum fractional anisotropy will increase with HAART.
6. Background and significance6.1. The neuro-immunology of AIDSHIV encephalopathy, the pathologic equivalent to HAD, is characterized by gliosis, microglial nodules, perivascular macrophage accumulation and the presence of multinucleated giant cells8. The encephalopathy is associated with immune activation and inflammation seemingly out of proportion to the amount of HIV virus present in the brain2. The mechanisms underlying HAD likely involve a significant contribution of indirect mechanisms, including a prominent role for inflammatory pathways mediated by cells of the monocyte/macrophage (M/MФ) lineage2,9.
Activated M/MФ are potent agents in inflammatory reactions resulting in many potential markers2,10-12. Two such markers, MCP-1 and neopterin, are readily measurable in CSF and, in the era before HAART, predicted HAD13. The clinical onset of neurological disease and its acceleration as immune function fails, directly relate to the dysregulation and accumulation of activated macrophages in the perivascular areas of the CNS, many of whom are infected14. Although the presence of virus in the CNS appears to be required for disease induction, the number of inflammatory macrophages rather than staining for virus is the best indicator of neural damage and cognitive deterioration in SIV-encephalitis15. It is hypothesized that critical events initiating the development of dementia occur outside of the brain16. Our model is consistent with other published hypotheses of peripheral monocyte infection2,16, whereby peripherally infected monocytes, upon meeting the brain microvascular endothelium, are able to self-initiate transmigration to the brain possibly related to an activated state. These cells then transfect other resident cells (astrocytes, microglia) resulting in activation, secretion of cytokines and chemokines and oxidative stress ultimately contributing to neuronal dysfunction and HAD (figure 1).
Version 1.5 Page 12 of 31
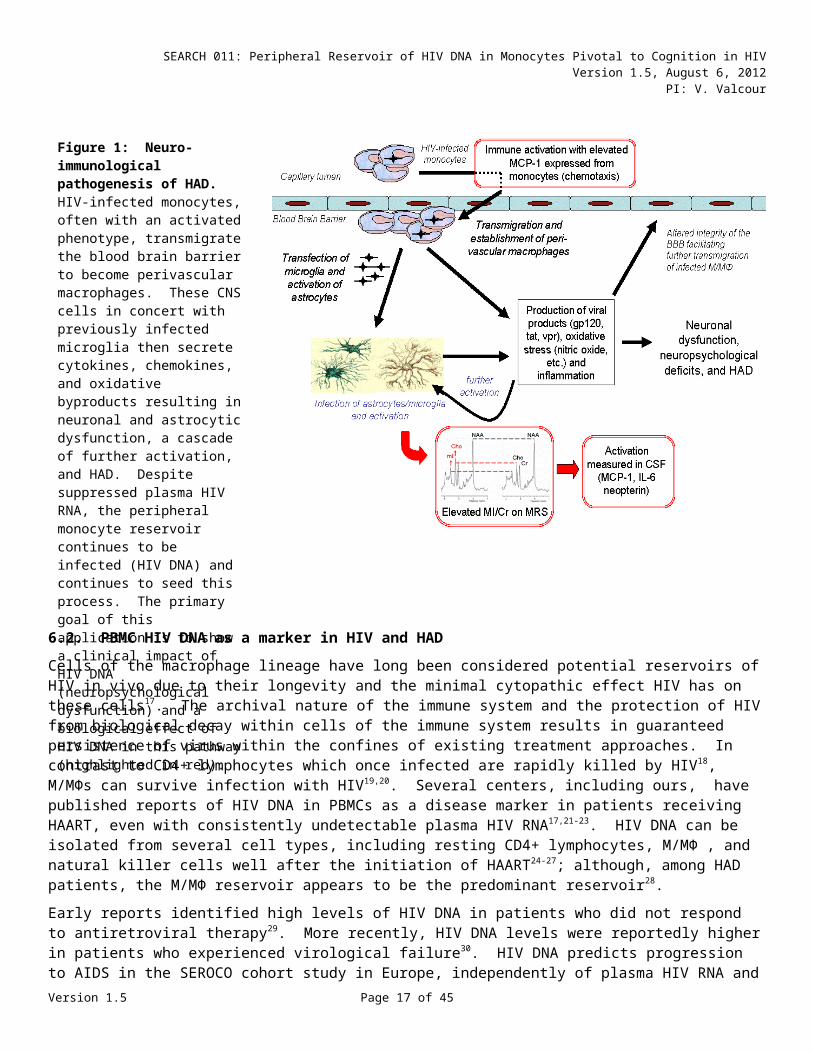
Figure 1: Neuro-immunological pathogenesis of HAD. HIV-infected monocytes, often with an activated phenotype, transmigrate the blood brain barrier to become perivascular macrophages. These CNS cells in concert with previously infected microglia then secrete cytokines, chemokines, and oxidative byproducts resulting in neuronal and astrocytic dysfunction, a cascade of further activation, and HAD. Despite suppressed plasma HIV RNA, the peripheral monocyte reservoir continues to be infected (HIV DNA) and continues to seed this process. The primary goal of this application is to show a clinical impact of HIV DNA (neuropsychological dysfunction) and a biological effect of HIV DNA in this pathway (highlighted in red).
SEARCH 011: Peripheral Reservoir of HIV DNA in Monocytes Pivotal to Cognition in HIV Version 1.5, August 6, 2012
PI: V. Valcour
6.2. PBMC HIV DNA as a marker in HIV and HADCells of the macrophage lineage have long been considered potential reservoirs of HIV in vivo due to their longevity and the minimal cytopathic effect HIV has on these cells17. The archival nature of the immune system and the protection of HIV from biological decay within cells of the immune system results in guaranteed persistence of virus within the confines of existing treatment approaches. In contrast to CD4+ lymphocytes which once infected are rapidly killed by HIV18, M/MФs can survive infection with HIV19,20. Several centers, including ours, have published reports of HIV DNA in PBMCs as a disease marker in patients receiving HAART, even with consistently undetectable plasma HIV RNA17,21-23. HIV DNA can be isolated from several cell types, including resting CD4+ lymphocytes, M/MФ , and natural killer cells well after the initiation of HAART24-27; although, among HAD patients, the M/MФ reservoir appears to be the predominant reservoir28.
Early reports identified high levels of HIV DNA in patients who did not respond to antiretroviral therapy29. More recently, HIV DNA levels were reportedly higher in patients who experienced virological failure30. HIV DNA predicts progression to AIDS in the SEROCO cohort study in Europe, independently of plasma HIV RNA and CD4 counts31. This finding has been recently confirmed in the French prospective PRIMO Cohort, where patients are enrolled at the time of primary HIV infection and progression was defined as the occurrence of AIDS-related clinical event or a CD4 count <350 cells/mm3. Compared with patients who did not have progression, those with progression had significantly lower CD4 counts at diagnosis, higher plasma HIV RNA, and higher HIV DNA levels. However, only the CD4 count and HIV DNA level independently predicted progression in multivariate models32. Our data indicate that HIV DNA is a risk for HAD in both treated and untreated HIV patients6,7.
6.3. Evidence for incomplete recovery of cognitive deficits after HAARTWidespread use of HAART is associated with a 50% reduced incidence of cognitive impairment in population-based studies33-35. Among patients treated with HAART most patients now show a milder form of impairment
Version 1.5 Page 13 of 31
SEARCH 011: Peripheral Reservoir of HIV DNA in Monocytes Pivotal to Cognition in HIV Version 1.5, August 6, 2012
PI: V. Valcour and the clinical course may vary with a waxing and waning pattern36-38. Controversy remains regarding the propensity to have cognitive decline in the face of suppressed HIV RNA in plasma and CSF. While most patients stabilize or slowly improve, published reports identify decline in cognitive function in a minority of patients. In one study 30% of patients demonstrated reliable cognitive decline by standard neuropsychological testing over an assessment period of several years37. In another study, HIV-infected individuals did not return to anticipated premorbid testing levels at 3 years39. In the Hawaii Aging with HIV Cohort, we are able to identify decrements in cognitive performance longitudinally among HIV patients compared to matched controls and are able to identify patients who progress in diagnostic categories despite undetectable HIV RNA. Whether these changes are associated with an active process relating to PBMC HIV infection is the focus of the planned work.
6.4. MR Spectroscopy in HIVProton magnetic resonance spectroscopy (MRS) is a non-invasive method used for determining the in-vivo concentration of brain metabolites40. Several cell types are distinguishable with commonly measured metabolites, including: neurons by N-acetyl-aspartate (NAA) and glial or inflammatory cells by myoinositol (MI) and choline (Cho)40. CNS HIV infection is associated with changes in brain metabolite concentrations detected by MRS. Reduced NAA/Cr ratios and increased MI/Cr and Cho/Cr ratios are typically reported, indicating direct effects on both neuronal and glial cell concentrations41-51. Reduced NAA/Cr and increased Cho/Cr ratios are seen in HIV individuals relative to controls41,48 with further accentuation associated with mild cognitive motor disorder (MCMD)43. These changes occur most prominently in subcortical structures including the frontal white matter, basal ganglia and thalamus52-56; although, frontal white matter measures may be most accurate due to technical challenges in measures of basal ganglia. The importance of inflammation in producing the observed changes in glial cell markers is also supported by further exacerbation of these changes in patients with progressive multifocal leukoencephalopathy57-59.
6.5. HIV-infection, HAD and healthcare in Thailand As of 2005, 580,000 Thai nationals were living with HIV, about 100,000 live in Bangkok alone60. The Thai Ministry of Public Health (MOPH) report in February 2007 identified 34,290 persons with HIV receiving care at MOPH hospitals in Bangkok with another 15,584 cared for in the three surrounding provinces61. Our collaborators working with the Anonymous Clinic at the Thai Red Cross Society in Bangkok screen about 500 persons each month and reports an HIV prevalence rate of 15% in this clinic62. The predominant viral strains circulating in Thailand are HIV-1 subtype B and CRF01_AE; however, in Bangkok, most patients are infected with CRF01_AE. All Thai HIV-infected patients can access ARV and laboratory monitoring at no cost through the national health care program. The 2007 Thai guidelines recommend ARV initiation for persons with a CD4 count less than 200 cells/mm3 or an AIDS defining illness63; roughly equivalent to recommendations of the World Health Organization64. Thailand‘s campaign to scale up ARV access in 2003 was possible because of the production of generic ARV by the Thai Government Pharmaceutical Organization (GPO). The two recommended fixed dose combination first line regimens are GPO-vir (stavudine (d4T), lamivudine (3TC), and nevirapine (NVP) and GPO-virZ (zidovudine (ZDV), 3TC, NVP). As of November 2006, 87,018 patients were receiving ARV through the national health care program. Of these, approximately 7,000 live in Bangkok61.
Few data exist concerning dementia among HIV patients in Thailand. Early published work identified neurocognitive differences among symptomatic and asymptomatic HIV patients compared to seronegative controls65. Symptomatic HIV patients showed deficits in a number of tests including color trails, grooved pegboard, trail making, and verbal fluency. In contrast, asymptomatic HIV patients differed from controls only in the grooved pegboard. More recent work from the Asia Pacific NeuroAIDS Consortium (APNAC) identifying HAND as a common complication in Thailand66.
Version 1.5 Page 14 of 31

SEARCH 011: Peripheral Reservoir of HIV DNA in Monocytes Pivotal to Cognition in HIV Version 1.5, August 6, 2012
PI: V. Valcour 7. Study Population7.1. ParticipantsSixty HIV participants will be enrolled and stratified by PBMC HIV DNA levels, either high (greater than or equal to 5000 copies/106 cells) or low (less than 5000 copies/106 cells). Individuals will be enrolled into each group until filled. Screening PBMC HIV DNA levels will be performed at SEARCH in real-time with less than one-week turnaround time. All individuals will intend to initiate ARV due to meeting MOPH guidelines for such. The protocol team will work with the primary care physician to facilitate initiation of standard ARV care; however, initiation of ARV is not a requirement of the study and ARV will not be provided by the study.
7.2 Consent processThe research nurse will discuss the protocol and review the consent form (in Thai) with potential participants. The research nurse will assure that subjects have the capacity to consent using a Capacity Assessment Record (CAR) as a guideline before consenting. The CAR guides the research staff to ensure that all key elements of consent are met. Should capacity be unclear, a protocol physician will confirm capacity. Research staff will evaluate subject willingness to participate and capacity to consent on an ongoing basis with consideration of minimizing coercion.
Individuals lacking clear capacity to consent who choose to participate will sign the protocol Assent Form and the legal authorized representative will sign consent. Based on Thai law (Article 4 of The Child Protection Act 2003 of the Constitution of the Kingdom of Thailand), the Legally Authorized Representative or “guardian” is defined as the "parent, persons providing care, adopter and guardians according to the Civil and Commercial Code, including step parents, guardian of a child's safety, employer, as well as any other person providing care or shelter to a child." No documentation is required to support guardianship status in Thailand. The Protocol Clinical Director and associate investigators will be available by phone and/or appointment to answer questions upon request. Prospective participants will be given ample time to read the consent form and have all questions answered prior to signing the consent and provided with a copy of the consent. The study nurse will assign a study number to each volunteer so that no identifier will be available for the laboratory personnel and external consultants. The study nurse will be responsible for the management of the list.
Evaluation and enrollment of participants is designed in a manner to protect individuals from coercion. All participants are eligible for HIV treatment external to the protocol and such treatment is not dependent upon the enrollment into this protocol. Monetary compensation is modest and designed to cover expenses related to missed work and transportation related to study procedures. Research staff will evaluate participant willingness to participate on an ongoing basis with consideration of minimize coercion and to assure ongoing assent/consent to the protocol.
7.3 Clinical Protocol7.3.1 Recruitment sites: Participants will be recruited using IRB-approved fliers/advertisement posted in various locations such as the PMK infectious diseases and neurology clinics and the Anonymous Clinic at the Thai Red Cross AIDS Research Center (TRCARC) and by “word of mouth” among HIV social networks. Interested participants will be referred to the protocol nurse for screening.
7.3.2 Participant selection: Sixty HIV-infected individuals meeting MOPH criteria to initiate HAART and planning to initiate HAART within a month of screening. Consequently, all participants will have plasma CD4 counts at less than 350 cells/mm3. Individuals will be enrolled into high and low PBMC HIV DNA groups as described above. Once an arm is filled, individuals screening into that group will not be enrolled. Since most patients in our past cohorts were between 30-40 years of age and nearly all had less than 12 years of education, we anticipate that groups will be relatively well matched by these two variables. To ensure that these variables are not greatly disparate between groups, an interim evaluation of group means will occur after each15 cases are enrolled and adjustment to recruitment strategies be directed, if needed.
7.3.3 Exclusion criteria:
Head injury with loss of consciousness greater than 1 hour or cognitive sequela
Version 1.5 Page 15 of 31
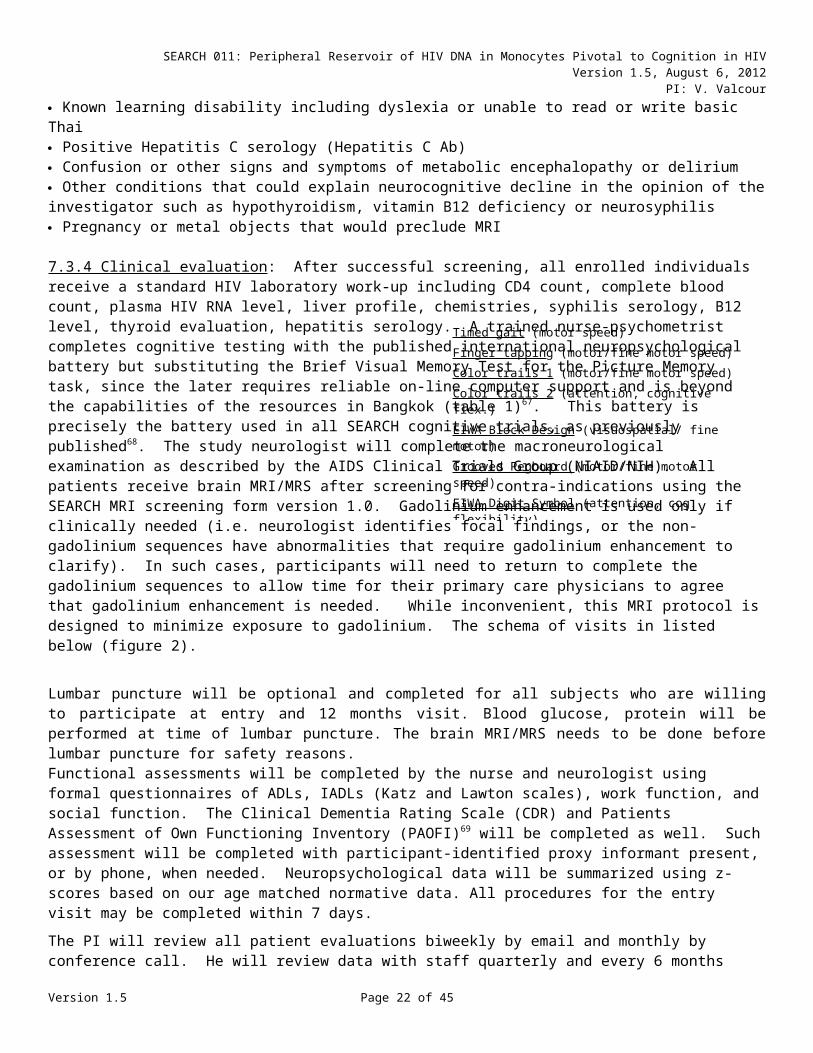
Timed gait (motor speed)Finger tapping (motor/fine motor speed)Color trails 1 (motor/fine motor speed)Color trails 2 (attention, cognitive flex.)EIWA Block Design (visuospatial/ fine motor)Grooved Pegboard (motor/fine motor speed)EIWA Digit Symbol (attention, cog. flexibility)WHO/UCLA Auditory Verbal Learning (verbal mem.)Brief Visual Memory Test – revised (visual mem.)Verbal Fluency – animals and first names (verbal fluency)Table 1: WHO International Battery for HIV (B J Psych 1991)
SEARCH 011: Peripheral Reservoir of HIV DNA in Monocytes Pivotal to Cognition in HIV Version 1.5, August 6, 2012
PI: V. Valcour Current/past illicit drug use or positive drug screen for methamphetamines, amphetamines, or cocaine at screening or entry. Any of the following laboratory abnormalities:
o PT/PTT > the upper limit of normal (ULN) or INR > 1.1o Hemoglobin < 9.0 mg/dLo ALT > 5x ULNo serum creatinine > 2x ULN or creatinine clearance < 30 cc per min by Cockroft-Gault formula
Acute illness within 30 days prior, persistent and active AIDS-defining OI of any organ system or autoimmune disease. Current or recent fevers or meningeal signs suggestive of CNS opportunistic infection CNS opportunistic infection, past or present (Patients diagnosed with opportunistic infection after CSF examination will be excluded from further analysis. In such a situation, an additional patient will be enrolled) History of pre-existing neurologic disease to include stroke, multiple sclerosis or psychiatric illness including schizophrenia, bipolar disorder, anxiety disorder, panic attacks, major depression, or post traumatic stress disorder. Patients with past depression that is controlled and patients with or minor depressive symptoms will be allowed to enroll. Known learning disability including dyslexia or unable to read or write basic Thai Positive Hepatitis C serology (Hepatitis C Ab) Confusion or other signs and symptoms of metabolic encephalopathy or delirium Other conditions that could explain neurocognitive decline in the opinion of the investigator such as hypothyroidism, vitamin B12 deficiency or neurosyphilis Pregnancy or metal objects that would preclude MRI
7.3.4 Clinical evaluation: After successful screening, all enrolled individuals receive a standard HIV laboratory work-up including CD4 count, complete blood count, plasma HIV RNA level, liver profile, chemistries, syphilis serology, B12 level, thyroid evaluation, hepatitis serology. A trained nurse-psychometrist completes cognitive testing with the published international neuropsychological battery but substituting the Brief Visual Memory Test for the Picture Memory task, since the later requires reliable on-line computer support and is beyond the capabilities of the resources in Bangkok (table 1)67. This battery is precisely the battery used in all SEARCH cognitive trials, as previously published68. The study neurologist will complete the macroneurological examination as described by the AIDS Clinical Trials Group (NIAID/NIH). All patients receive brain MRI/MRS after screening for contra-indications using the SEARCH MRI screening form version 1.0. Gadolinium enhancement is used only if clinically needed (i.e. neurologist identifies focal findings, or the non-gadolinium sequences have abnormalities that require gadolinium enhancement to clarify). In such cases, participants will need to return to complete the gadolinium sequences to allow time for their primary care physicians to agree that gadolinium enhancement is needed. While inconvenient, this MRI protocol is designed to minimize exposure to gadolinium. The schema of visits in listed below (figure 2).
Lumbar puncture will be optional and completed for all subjects who are willing to participate at entry and 12 months visit. Blood glucose, protein will be performed at time of lumbar puncture. The brain MRI/MRS needs to be done before lumbar puncture for safety reasons.Functional assessments will be completed by the nurse and neurologist using formal questionnaires of ADLs, IADLs (Katz and Lawton scales), work function, and social function. The Clinical Dementia Rating Scale (CDR) and Patients Assessment of Own Functioning Inventory (PAOFI)69 will be completed as well. Such assessment will be completed with participant-identified proxy informant present, or by phone, when needed. Neuropsychological data will be summarized using z-scores based on our age matched normative data. All procedures for the entry visit may be completed within 7 days.
The PI will review all patient evaluations biweekly by email and monthly by conference call. He will review data with staff quarterly and every 6 months will convene a consensus with all evaluating staff members to determine cognitive diagnoses using 2007 criteria1. Consensus conference members will be the (Thai) study neurologist, the study nurse/psychometrist, the protocol Clinical Director (J. Ananworanich) and the PI (V. Valcour). Validation of the consensus conference will occur with external consultants, David Clifford (HIV Version 1.5 Page 16 of 31
SEARCH 011: Peripheral Reservoir of HIV DNA in Monocytes Pivotal to Cognition in HIV Version 1.5, August 6, 2012
PI: V. Valcour neurologist), and Robert Paul (HIV neuropsychologist) on an annual basis. A consensus diagnosis will categorize as: (1) cognitively normal, (2) asymptomatic neurocognitive impairment, (3) Minor Neurocognitive Disorder, and (4) HIV-associated Dementia, as published1. Dementia severity will be assigned using the Memorial Sloan Kettering scale. Members will be blinded to HIV DNA level and the International HIV Dementia Scale (to facilitate AIM III), but will have access to all neuropsychological, neurological, and functional information.
7.3.5 HAART treatment and Longitudinal follow-up: It is anticipated that all participants will initiate ARV within 30 days of screening in the context of their clinical care. ARV treatment is not provided by this protocol; although, our team will assist patients to promptly begin treatment through their primary medical care services and encourage adherence. A similar protocol in SEARCH 001 resulted in 29/30 initiating HAART and adherence was nearly 100% at one year. Through the government-sponsored program, all individuals typically begin the same ARV regimen of lamivudine, stavudine, and nevirapine (GPOvir™), or a new combination of lamivudine, zidovudine, nevirapine (GPOvir-Z™). There are standardized substitutions for intolerance or contraindication to these medications. Thus, it is anticipated that all participants will receive this relatively standardized regimen, minimizing variability between groups. Phone calls will be made at least every 3 months to encourage adherence (more frequently in the first 6 months) and to maximize retention. Individual who do not start HAART by 6 months will be discontinued from the protocol.
7.3.6 Definition of major cognitive outcomes: The primary cognitive endpoint will be the NPZcomp, as described in the introduction and preliminary data (RAVLT total score, digit symbol, and timed gait scores). Secondary analyses will employ the consensus diagnoses of HIV-associated Neurocognitive Disorders. Two additional continuous scales of neuropsychological performance will be available for post-hoc analyses as well as individuals NP scores. One scale will be the global NPZ score, the arithmetic average of z-scores from all tests. In addition, we have defined a Global Deficit Score (GDS) using a method established by Heaton et al70, which utilizes a weighted score of all available neuropsychological data (see preliminary data).
7.3.7 Co-enrollment: Participants are eligible for co-enrollment in other protocols. For co-enrollment in any protocol, staff will monitor blood draws to ensure not more than 70 cc per visit and no more than 3 visits in the screening period (30 days). We intend to maintain two separate charts for each study that the patient enrolls. Relevant lab tests may be copied and placed into each file (e.g., radiology films, psychometric testing, etc.).
For co-enrollment in SEARCH 007 which intends to evaluate t-cell specific responses in patients with and without dementia as the initiate HAART for the first time, additional studies required for this protocol include MRS (optional for SEARCH 007), and an additional 60cc blood draw. A screening hematocrit is part of both protocols to maximize safety with blood draws. MRI/MRS data, neuropsychological data, and basic laboratory tests (CD4 counts, HIV RNA levels, chemistries) will be shared between protocols, whenever possible. The MRI/MRS and neuropsychological profiles for both protocols are the same.
Version 1.5 Page 17 of 31

Figure 2: Study schema for enrollment and longitudinal follow-up.
SEARCH 011: Peripheral Reservoir of HIV DNA in Monocytes Pivotal to Cognition in HIV Version 1.5, August 6, 2012
PI: V. Valcour 8. Study design and methodology8.1 Clinical considerationsThe clinical procedure is described above. Participants will have ample opportunity to ask the study nurse questions about the study and receive answers prior to signing the informed consent. The study nurse will screen and enroll participants who are willing to participate and are eligible for study participation. At each visit, vital signs (blood pressure, temperature, pulse) and weight will be recorded prior to venipuncture to ensure safety. Urine pregnancy testing will be completed on female participants at screening as will a screen for metal objects that would exclude patients from MRI (and the study). On the day of MRI/MRS (within 30 days of screening), female subjects will be queried about the date of their last menstrual period and symptoms of pregnancy and the urine pregnancy test repeated should there be doubt. They will also be queried again about metal objects to minimize risk in the process of signing a standard hospital consent form to have the MRI/MRS done as it is standard practice in Thailand. After the MRI/MRS they will receive a lumbar puncture at baseline and 12 months (optional at 12 months).
Viral load and CD4 will be performed at AFRIMS and the TRCARC laboratory facilities. The PBMC and sera will be processed at AFRIMS and the TRCARC. The specimen storage will be kept at AFRIMS, TRCARC and University of Hawaii. Other clinical blood tests may be done at Phramongkutklao Hospital and the TRCARC. Results will be released to the study nurse and shared with the patient. If exclusion criteria are met at screening, the nurse will notify the individual of his/her ineligibility. The nurse will place a reminder call to the participants 1-2 days prior to their visits.
8.2 Methods pertinent to Aim IAim 1: To determine the long-term relationship between cognition and HIV DNA in circulating PBMCs and monocytes (CD14+ PBMCs) among patients initiating HAART for the first time.
60cc of blood will be obtained from participants at each visit for aims 1 and 2. Specimen processing and cell separation will take place in real-time at AFRIMS and the TRCARC in Bangkok, which has processed all cells for SEARCH 001. The cells will then be harvested and stored in DMSO (frozen) and shipped in batches to Dr. Shiramizu’s laboratory at the University of Hawaii and to the VGTI (Florida) laboratory for the HIV DNA assays6. Laboratory methodology for separation and DNA assays are described below and that for cognitive evaluations are described above. CSF and plasma HIV RNA levels will be completed at the AFRIMS and the TRCARC site on 2cc of plasma and 5 cc of CSF, respectively, using the Amplicor HIV-1 Monitor Ultra sensitive Assay (Roche Molecular System, Inc., Branchburg, NJ) following ultra-centrifugation to achieve detection levels of < 10 copies/ml. Viral subtype will be confirmed by V3 peptide ELISA serotyping with confirmation by gene sequencing, when indicated, as previously described 71.
Statistically, we will model the relationship between baseline and subsequent measures of HIV DNA using mixed effects models to the available data on log-transformed DNA. To relate baseline and subsequent measures of HIV DNA to NPZcomp, we will use multivariate regression, where the response vector is composed of the NPZcomp measurements over time and the predictor variables will include HIV DNA measurements at each time point, as well as baseline CD4 count, plasma HIV RNA, education, Thai Depression Inventory score, and age. The CSF portion of AIM I is designed to ensure that the effects observed are not due to increased central nervous system (CNS) viremia as measured by CSF HIV RNA levels. We can evaluate this hypothesis by including baseline and subsequent CSF HIV RNA measurements as covariates in the final multivariate regression model obtained as described in aim 1, and determine whether inclusion of this covariate affects the regression parameter for HIV DNA.
8.3 Methods pertinent to Specific Aim IIAIM 2: To define the longitudinal relationships between CD14+ HIV DNA and: (1) CSF biomarkers of immune activation (neopterin, MCP-1, and IL-6), (2) CD14+ supernatant markers of immune activation (MCP-1 and IL-6), and (3) increased myoinositol/creatine ratio by MRSVersion 1.5 Page 18 of 31
SEARCH 011: Peripheral Reservoir of HIV DNA in Monocytes Pivotal to Cognition in HIV Version 1.5, August 6, 2012
PI: V. Valcour 8.3.1 Collection of blood and CSF: 30cc blood will be obtained and processed at AFRIMS and the TRCARC at each time point for the measure of supernatant markers as well as needs for aim 1 (see methodology below). Lumbar puncture will be completed in the Department of Neurology, PMK or SEARCH clinic, The Thai Red Cross AIDS Research centre in standard fashion. The additional blood draw for 5 mL will be obtained for the measure of glucose and protein level to compare with CSF at the time of lumbar puncture. Specimens will be immediately transported to AFRIMS and the TRCARC for plasma and CSF RNA analyses. The tests that will be performed on leftover CSF samples will include cytokine/chemokine and biomarker assays (such as for MCP-1, neopterin, IL6, T-tau, P-tau, Abeta42, sAPPalpha, sAPPbeta, neurofilament light and other biomarkers relevant to immune response to HIV) at the Institute of Neuroscience and Physiology at the University of Gothenburg in Sweden. Cellular markers in CSF such as CD8+ T cell repertoire and gene arrays may also be performed on left over CSF samples at the VGTI laboratory in Florida, USA.
8.3.2 Methods relating to MRI/MR spectroscopy: All MRI and MRS studies will be performed at the Chulalongkorn Hospital, Bangkok, Thailand on the GE Signa 1.5T scanner with the latest version of software and hardware using a protocol as follows:
Structural MRI protocol: a short MRI 3D scout scan (30sec), followed by a 3D MRI acquisition (3D spoiled gradient echo, sagital plane with full brain coverage, minimum echo time with full echo, TR=20ms, flip angle=50 with resolution 1x1x1.4 mm3).
Single voxel Proton MRS: A volume head coil will be used for signal detection. Localized double spin-echo (PRESS) 1H MRS will be performed in 3 brain regions: frontal white matter, posterior cingulate gyrus gray matter and basal ganglia using the automated PROBE-P (Proton Brain Exam)72. The voxel size will be 8 cc. Prior to the PROBE-P scan, a quick one minute MRS scout using the same pulse sequence will be initiated for spectral quality assurance. If the reconstructed spectrum (automatic on the scanner after data acquisition is completed) exhibits high susceptibility effect (broad metabolite line widths and large lipid contamination), the voxel location will be adjusted slightly for a lesser susceptibility artifact and narrower line width. Automated optimization of gradient shimming, transmitter pulse power, receiver gain and water suppression will be performed prior to data acquisition. Two sets of single voxel data will be acquired for each location. The first set is the PROBE-P acquisition with 128 water-suppressed free-induction decays (FIDs) and 16 un-suppressed water FIDs with echo time (TE) of 35ms and the repetition time (TR) of 2s. The total acquisition time for one brain location is 4.5 min. The second set will be the measurement of T2 decay of the fully relaxed un-suppressed water FIDs, using the same PROBE pulse sequence at TR of 10 sec and 9 different TE values of 30, 35, 45, 65, 85, 120, 200, 500 and 1500 msec with one FID per TE step (total acquisition time of 90sec).
MRS Data Analysis: All 1H MRS data will be analyzed using the customized IDL program merged with the spectral analysis package, LCModel. Data processing consisted of an eddy-current correction based on the phase of the unsuppressed water signal, no line broadening prior to quantitation using LCModel. Correction for differences in cerebrospinal fluid (CSF) in each voxel location will be performed using a bi-exponential T2 fit of the un-suppressed data set.
LCModel Analysis Criteria: The absolute metabolite concentrations will be obtained with the Linear combination model (LCModel) analysis. Within LCModel, concentrations of metabolites are determined using a linear combination fit of individual in vitro metabolite spectra that comprise the ‘basis set’ for the in vivo data. We will use the standard basis-sets available from Stephen Provencher (s-Provencher.com), LCModel’s package developer. This basis set has been optimized for metabolite concentrations at 1.5T. Spectra will be included in the final analysis based on standard quality criteria.
8.3.3 Statistical Considerations: Rank-based correlation methods will be used at all time points. In addition, we will use multivariate regression models to combine data across time points and linear regression analysis will be used to estimate the impact of levels of HIV DNA on markers of immune activation, on both MI alone and on the MI/Cr ratio. Secondary analyses will be carried out on other markers with emphasis on cho, Cho/Cr ratio.
8.4. Methods pertinent to Specific AIM IIIAIM 3: To prospectively determine the performance characteristics of the International HIV Dementia Scale and the NPZcomp in Thailand
Version 1.5 Page 19 of 31

SEARCH 011: Peripheral Reservoir of HIV DNA in Monocytes Pivotal to Cognition in HIV Version 1.5, August 6, 2012
PI: V. Valcour Clinical considerations for the acquisition of these data are described above. Analyses will involve ascertainment of false positive and false negative observations for all observations at each time point using standard techniques. Reviewers will be blinded to the IHDS at consensus panel. The same approach will be used for categorization of HAD based on NPZcomp, using a cutoff of -0.7, based on our preliminary data estimates.
8.5 Methods prertinent to Specific AIM IV
AIM 4: To test feasibility of diffusion tensor imaging in Bangkok
If time permits at the end of MRI/MRS imaging, participants will be asked to complete Diffusion Tensor Imaging (DTI) using the following protocol: single-shot echoplanar imaging in 25 diffusion-sensitized directions each with a b-factor of 1000 s/mm2, TR/TE =12700/91, acquisition matrix=96x96; field of view=24cm, 2 interleaved series of 2 repeats, each containing 45 3-mm slices without gap. Image plane must be straight axial. Total acquisition time is about 11 minutes. Images will then be de-identified and transferred to Dr. Valcour’s laboratory for analyses using DTI studio.
9. Laboratory procedures9.1. Specimen handling and proceduresVenipuncture will be completed according to institutional guidelines for safety using universal precautions. Upon arrival at AFRIMS and TRCARC, samples will be labeled with a bar code identifying the study site, the protocol number, the PIN, and the visit number. The AFRIMS, TRCARC and HACRP laboratories are BL-2 facilities which use universal precautions and are equipped to handle HIV-1 infected samples in a safe manner. Samples will be shipped with information sheet that will clearly indicate that the samples are infected with HIV-1, per standard procedures.
9.2. Specimen archivingSpecimens not used immediately for assays will be stored frozen in AFRIMS and the TRCARC facility until the end of the study (up to 10 years from the beginning of the study) and then disposed. PBMCs will be stored at -140oC (Liquid Nitrogen tanks) and plasma/sera/CSF will be stored at -80oC at the AFRIMS Department of Retrovirology laboratory complex and the TRCARC. If residual samples remain after the studies done at HACRP, they will be retained in their repository until the end of the study (up to 10 years from beginning of the study) and then disposed. No new studies will commence without review and approval by the local IRBs and the WRAIR IRB. Studies may be related to the existing protocol or other protocols as directed by the protocol scientists.
9.3. Specimen shippingCryopreserved PBMC from AFRIMS and the TRCARC will be shipped to HACRP and the VGTI (Florida) laboratory for HIV DNA assays where they will be rapidly thawed for assays. We will use a dry shipper system, which will allow the shipment of cryopreserved PBMC in liquid nitrogen (LN2) vapor phase. Dry shipper systems assure maintenance of -160 ˚C for up to 14 days. Left over CSF specimens will be shipped to the Institute of Neuroscience and Physiology at the University of Gothenburg in Sweden to perform CSF biomarker assays and the VGTI (Florida) laboratory to perform cellular markers assays.
9.4. Laboratory methodologies9.4.1. PBMC Separation into CD14-Positive and CD14-Negative Subsets: Enrichment for monocytes will be performed by density gradient centrifugation with Percoll as previously described6. Based on previous data, we expect to isolate 1-10 x 107 cells per 30mL blood. The cells are then prepared for magnetic labeling of target monocytes (saving 2 x 106 PBMC for culture in real time and not frozen). Cell separation will be performed as per manufacturer’s instructions MACS Microbeads (Miltenyi Biotec, Auburn, CA) with 20 L microbeads labeling up to 1 x 107 target monocytes. Cells are pelleted and store in DMSO (2 x 106 aliquots per vial; 1 aliquot is not frozen and processed for culturing in real time) at –70oC for processing later. The column is washed with 3 x 500 L cold PBS. The MS column is removed from the magnet and placed in a sterile collection tube. One mL PBS is applied to the column to flush out the positive fraction by pipetting down the
Version 1.5 Page 20 of 31

SEARCH 011: Peripheral Reservoir of HIV DNA in Monocytes Pivotal to Cognition in HIV Version 1.5, August 6, 2012
PI: V. Valcour side of the column and using the plunger supplied with the column. Cells are counted and stored in DMSO (2 x 106 aliquots per vial; 1 aliquot used for culturing in real time) for processing later.
9.4.2. Monocyte culture for supernatants: PBMC will be separated by Percol and resuspend in equivalent 10x106 cells in 6mL culture media (RPMI with 10% FBS and 0.11g/L (or 1mM) sodium pyruvate. Cells will be placed in 6-12 well plates and incubated at 37C and 5% CO2 for at least 3 hours to allow monocytes to attach. Unattached cells are carefully aspirated and transferred to another plate to incubate. Fresh media is placed in both plates and incubated overnight. Supernatants are then recovered and stored at -70oC and batched shipped to Hawaii for cytokine assays which will be completed with standard elisa kits that are commercially available.
9.4.3. HIV DNA Quantification: The previously stored viable cells will be batched and shipped to the HACRP and the VGTI (Florida) laboratory73; saving 1 vial each of the CD14-positive and CD14-negative cells for cultures). Briefly, each aliquot of cells will be washed in PBS and pelleted. Lysis buffer [1L lysis buffer/105
cells; with 10 ml TE (10 mM Tris-HCl, 1 mM EDTA, pH 8.0), 100 L 0.1% Triton X-100 (0.001% final conc.), 100 L 1.0% SDS (0.01% final conc.), and 300 L proteinase K (stock @ 14mg/mL), which is added just before use will used to re-suspend the cell pellet followed by overnight rocking at 50oC. The reaction will be incubated at 94oC for 15 min to inactivate the proteinase K; DNA is precipitated, quantified and stored at -20oC. Reactions will be set up with equal amounts of DNA template with the following conditions: dNTP, 10X Taq polymerase buffer, Taq polymerase, 10% dimethyl sulfoxide, and HLADQα or β-globin primers. The conditions are: 94ºC/3 min, 30 cycles of 94ºC/1 min, 55ºC/1 min, 72ºC/1 min, 1 cycle of 94ºC/1 min, 55ºC/1 min, 72ºC/5 min. Then 10 μL of each reaction will be resolved on a 1% agarose/1.5% NuSieve (FMC Bioproducts, Rockland, ME) to assess adequate DNA. A standard plasmid was designed with one HIV copy (HXB2, GenBank accession #K03455) and one housekeeping gene, β-globin (GenBank accession # U20223), using two primer sets: HIV gag (to generate a 296bp product) and β-glo (to generate a 330bp product), which will be used for the HIV DNA assay as previously noted. DNA specimens will be prepared at 25 ng/L with 100 ng to be used in the analysis. Master mixes will contain either HIV or β-glo primer and probe sets, 1x iQ supermix (BioRad Laboratories, Hercules, CA), 100 ng sample, and water (final volume 25 L). Initial denaturation for 3 min is performed, followed by 45 cycles of 95°C/10 sec, 57°C/30 sec and final extension of 72°C/2 min. Plasmid dilutions from 106 to 101 gene copies will be used for the standard reference curve with non-HIV-1 infected genomic DNA as a negative control and three HIV-1 infected cell lines (8E5, OM10.1, ACH-2 NIH AIDS Research and Reference Reagent Program) DNA to be used as inter-assay calibrators. The calculations of HIV DNA copy per 106 cells will be obtained from the iCycler Real-Time Detection System Program. Cross contamination will be minimized using a HEPA-filter laminar flow hood and a thermalcycler located in a physically-isolated area. For the purpose of screening, PBMC (without separation to cellular subsets) will be completed at the SEARCH laboratory in collaboration with AFRIMS and the TRCARC.
9.4.4. CSF biomarker assays : Left over CSF will be spun and stored at –80˚C and will be used to isolate and sequence HIV, and for cytokine/chemokine and biomarker assays (such as MCP-1, neopterin, IL6, T-tau, P-tau, Abeta42, sAPPalpha, sAPPbeta, neurofilament light and other biomarkers relevant to immune response to HIV). All these specific tests will be performed at Institute of Neuroscience and Physiology at the University of Gothenburg in Sweden. Cellular markers such as CD8+ T cell repertoire and gene array may be performed on left over CSF at the VGTI (Florida) laboratory74. In selected samples, certain cellular markers may also be assessed in peripheral blood mononuclear cells for comparison with CSF results.
9.4.5. Laboratory quality assurance: Dr. Shiramizu will be responsible for assurance that HIV DNA analyses for preliminary assignment do not vary greatly from that of enrollment. Should values differ by more than 15%, re-training will occur. AFRIMS and the TRCARC maintain continuous quality assurance for assays which will be monitored by Dr. Alexandra Schuetz.
9.5 Power and sample size considerationsWe anticipate accruing 60 subjects (30 with high HIV DNA and 30 with low HIV DNA) with visits at 0, 6, 12, 24, 36, and 48 months. There will also be 26 enrolled cases from SEARCH 001 for the purpose of long-term
Version 1.5 Page 21 of 31
SEARCH 011: Peripheral Reservoir of HIV DNA in Monocytes Pivotal to Cognition in HIV Version 1.5, August 6, 2012
PI: V. Valcour follow-up of subjects after initiation of HAART. These data will be used as a validation set. Based on SEARCH 001, the attrition rate can be expected to be 2 cases/30 cases/year and an additional 2 cases/30 cases can be expected to have detectable plasma HIV RNA and therefore excluded from analysis. Conservatively reducing the cohort by 15% annually to include occasional cases of medication non-compliance and considering the 60 new cases, we anticipate having 60, 56, 51, 43, 37, and 31 observation pairs at baseline, 6, 12, 24, 36, and 48 months, respectively. This will result in an estimated 278 observations in the first 4 years.
We will calculate power based on a simple linear regression in which the total number of observations is reduced by a “variance inflation factor” arising from the correlation of repeated measurements across time points. This will approximate power for our multivariate regression. The variance inflation factor due to such correlation is [1 + (m-1)ρyρx], where m is the number of observations per subject, ρy is the intra-class correlation of the dependent variable (NPZcomp), and ρx is the intra-class correlation of the independent variable (HIV DNA).130 Based on pilot study data, we found correlations of NPZcomp scores ranging from 0.4 to 0.7; we use a conservative 0.6 for our power calculations here. Correlation of baseline and post-baseline DNA measurements ranged from 0.3 to 0.5, and correlation between post-baseline time points was considerably greater—up to 0.9; conservatively, we will use 0.8 for our calculations. Subjects will have an average of 4.6 visits, so the variance inflation factor is approximately [1+(4.6 -1)(.8)(0.6)] = 2.6. The equivalent number of independent observations is estimated to be 1/(2.6) = 0.39 times the total number of observations. An estimated 278 correlated observations, provides approximately equivalent information to 278 x 0.39 = 108 independent observations. Standard deviation for NPZcomp was estimated to be 0.66 among demented and 0.60 among non-demented from the pilot data; we will use 0.63 in our calculations. Standard deviation of log HIV DNA was 1.17 and 1.23 at baseline and 6 months, we use 1.2 in our calculations. Based on these estimates, we have 80% power to detect a slope of 0.14 in the regression of NPZcomp on HIV DNA, implying that for a 1-log reduction in DNA, we would expect a 0.14 increase in the NPZ score. As discussed above, we expect this to estimate power for the multivariate regression on NPZ score on HIV DNA at each time point. Adjustment for covariates like age and education may also improve power.
10. Risks, benefits, research-related injury and confidentiality10.1 Physical risks to the subjectsThere are few risks to this proposal. Concerning the venipuncture, there is a reasonable potential risk of slight pain and bruising with a very slight possibility of infection. A small volume will be drawn at each visit (<70cc). Te screening visit includes consideration of anemia to protect subjects. There is a possibility of psychological stress related to cognitive functioning tests. To minimize this, technicians will be trained in approaches needed to minimize this risk by our study neuropsychologist.
The risks of lumbar puncture include local discomfort after the procedure at the site of the lumbar puncture. There is a small risk for a headache or decreased blood pressure from the procedure or leaking of cerebral spinal fluid after the procedure. There is a small risk for infection and a very small risk of damage to nerves in the lumbar spinal roots. To minimize side effects of the lumbar puncture, this procedure will only be carried out by study physicians with training and experience and we will ask subjects to remain lying flat for about 20-30 minutes after the procedure and drink plenty of water after the procedure. All subjects will be informed of the risks and benefits of this procedure and will sign consent prior to the procedure. This protocol is designed within the standard-of-care for the procedure in Thailand.
Participants will undergo MRI/MRS of the brain. Discomfort with lying flat and claustrophobia/anxiety are other potential risks. Patients will be screened to ensure lack of contra-indication due to metal in the body, in accordance with standard of care. Gadolinium enhancement is not part of this protocol, unless deemed necessary for clinical purposes. In very rare circumstances, allergic reactions have been described. Recently, gadolinium contrast has been associated with renal failure in very rare situation and particularly among patients with baseline renal insufficiency. As such, patients with abnormal renal function, as measured by serum creatinine, are excluded from this study.
10.2. Adequacy of protection against risks
Version 1.5 Page 22 of 31
SEARCH 011: Peripheral Reservoir of HIV DNA in Monocytes Pivotal to Cognition in HIV Version 1.5, August 6, 2012
PI: V. Valcour Our staff will be trained and certified to conduct all study procedures including blood drawing and cognitive function testing. Maximal attention will be paid to maintaining the participants’ comfort and avoiding overtiring the participants. In the event of medical urgency, proper procedures will be followed. This could include informing the onsite physician who will provide necessary care or ensuring that the participant receives timely follow-up care from their primary care physician. The testing and procedures will take place in a fully functioning hospital capable of dealing with emergencies. There is a study physician available 24 hours a day.
Names and other identifiers will not be directly used on data and specimens to ensure confidentiality of participants. Only investigators will be able to cross match information with participant identity for the purposes of clinical care. IRB-approved consent will be obtained from all participants prior to enrollment.
10.3. Potential benefits of the proposed research to the subjects and othersEach HIV-seropositive participant will receive a comprehensive evaluation to identify cognitive problems. For participants with HAD, an evaluation for possible treatable etiologies will be sought. While this protocol does not provide HAART, there are no limitations regarding treatment and it is anticipated that all participants who are eligible will start HAART within 1 month of enrollment and our past experience suggests that adherence is enhanced with protocol participation. For patients with cognitive decline the lumbar puncture will provide important data to rule out opportunistic infectious disease. Brain MRI will be equally important to rule out alternative etiology to the impairments in cognition.
10.4. Importance of knowledge to be gainedThese data will significantly advance our understanding of why cognitive impairment does not fully resolve after the initiation of HAART. We anticipate validation of a marker and neuropsychological testing for early detection of dementia in HIV.
10.5. Inclusion of womenThe World Health Organization (WHO) estimates that 36% of HIV-positive adults in this general region are women. However this information may under-estimate the impact of the HIV epidemic on women in Thailand. (http://w3.whosea.org/women2/aids.htm). In our past trial, 67% of enrollees are women. The proposed work intends to enroll participants in the order that eligible patients are seen at the neurology clinic, to minimize selection bias. Women that test positive in pregnancy test will be excluded for their safety.
10.6. Inclusion of minoritiesThe clinical aspects of this work will be conducted in Thailand within a hospital that cares for Thai nationals. It is anticipated that 100% of the subjects will be Thai.
10.7 Inclusion of childrenTo minimize variability in the clinical characterization, we will study only adults who have completed development and education. In accordance with Ministry of Public Health guidelines for adults in clinical trials, all participants will be 20+ years old.
10.8 Research related injuryResearch related injury during the study will be responsibility of the volunteer covered under the universal health care that exists in Thailand. Dr. Ananworanich will assist the volunteer and refer him/her to the best possible care obtainable under universal coverage or insurance-paid health care and will follow up on the condition of the volunteer and aid the Thai physician when and where appropriate. The local sponsor (SEARCH/Thai Red Cross AIDS Research Centre) will give volunteers immediate treatment needed for their injuries and will assist in costs of treatment not covered by the Thai government insurance plan.
10.9 ConfidentialityThe investigator will maximize participant anonymity using standard techniques. Participants will not be identified in any reports on this study. All records to include Protected Health Information (PHI) such as HIV
Version 1.5 Page 23 of 31

SEARCH 011: Peripheral Reservoir of HIV DNA in Monocytes Pivotal to Cognition in HIV Version 1.5, August 6, 2012
PI: V. Valcour status, drug testing, hepatitis, and syphilis infection will be kept confidential to the extent provided by federal, state and local law. Protection of participant confidentiality will be preserved by assigning each study participant a patient ID number (PIN).
10.10 Early withdrawalAny volunteer is free to withdraw at any time. Since this is an observational study there is no risk to the volunteer if he/she wishes to withdraw. Such early termination will be noted in the database and data will be censored, when appropriate. Specimens from volunteers that have withdrawn will be maintained in the repository and will be disposed at the end of the study (up to 10 year from the beginning of the study) and then discarded. It is not anticipated that patients' cognitive symptoms will deteriorate, since all should be starting antiretroviral medications. Should this occur, the subject will be informed of her/his condition and the study team will work with the participant to ensure maximal care, including change in antiretroviral medications, and assessment of CSF suppression of HIV RNA, when indicated.
10.11 Requirements by law to communicate to the Thai government about blood tests There is no known requirement in Thailand to communicate to the government about blood tests.
11. Data collection, management, and analysis11.1 Data safety monitoring planThe proposed study is not a phase III study and there are no plans for involvement of a specific DSMB to be convened for this study. However, we intend to maximize the safety of the participants by monitoring for adverse experiences with weekly staff meetings and bi-weekly correspondence with the PI. The research team on site will review all laboratory values and follow-up will be instituted, if indicated. All serious adverse experiences will be reported immediately (within 24 hours of the investigator’s knowledge) to all IRBs involved in the study. All other adverse events will be compiled and also reported in a timely fashion to respective IRBs.
This is not an IND study. Records pertaining to each site will be maintained consistent with local IRB policies. Clinical source documents will be stored at the SEARCH office on the second floor of the Tower two building of the Thai Red Cross AIDS Research Center (104 Rajdamri Rd. Tower 2, 2nd floor, Pathumwan, Bangkok 10330) in a locked and secure room with limited access. For records handled at the WRAIR, AFRIMS, and TRCARC facilities, research data will be saved in notebooks and data files. Hard (paper) copies of data (that are in tabular or non-notebook format) will be transferred to long-term storage after trial final report is prepared and manuscripts are written. The documents will be maintained in the long term storage for up to 10 years.
11.2. Case report formsCase report forms (CRF) will be prepared for each participant. Source documented clinical and laboratory data will be transcribed to CRFs as data becomes available. Correction of data on CRFs must be made according to good clinical practice (GCP) principles. If corrections are made following review and signature by the investigator, he/she must be made aware of the changes and document this awareness. Data must be verifiable to the source data, which necessitates access to all original recordings, laboratory reports, and participant records. The investigator therefore agrees to allow sponsor access to participant records, and source data for such a circumstance.
11.3 Data monitoringClinical and lab data will be transferred to CRFs as the data become available. The senior clinical coordinator or designee on site will review the data to ensure that source document data are accurately transferred to the CRFs. CRF data will then be key entered into an ACCESS database and subjected to out of range and logic check by an automated program within excel and supplemented by a SAS program. Queries will be resolved by comparison to source data. The database is password protected and it is locate at SEACH office on the second floor of the Tower two building of the Thai Red Cross AIDS Research Center (104 Rajdamri Rd. Tower 2, 2nd floor, Pathumwan, Bangkok 10330).
11.4 Protocol deviations, amendments/modifications, and continuing review
Version 1.5 Page 24 of 31

SEARCH 011: Peripheral Reservoir of HIV DNA in Monocytes Pivotal to Cognition in HIV Version 1.5, August 6, 2012
PI: V. Valcour Deviations will be reported in the annual continuing review report (CRR). Amendments and modifications will be submitted to the local IRBs, as required. No changes in protocol conduct will be implemented until approval by the committees. Annual CRRs will be submitted to the local IRBs on or before the anniversary date of the study approval.
The following reporting requirements will be adhered to:
a) Any modifications that could potentially increase risk to subjects must also be submitted to the IRBs for approval prior to implementation. All other amendments will be submitted with the continuing review report.
b) Any deviation to the protocol that may have an effect on the safety or rights of the subject or the integrity of the study must be reported to the IRBs as soon as the deviation is identified..
c) The knowledge of any pending compliance inspection/visit by the OHRP, or other government agency concerning clinical investigation or research, the issuance of Inspection Reports, warning letters or actions taken by any Regulatory Agencies including legal or medical actions and any instances of serious or continuing noncompliance with the regulations or requirements will be reported immediately to the local IRBs.
11.5. Unanticipated problemsAn unanticipated problem involving risks to subjects or others is one that does not appear as a risk in the informed consent document and/or protocol. The Principal Investigator will be notified immediately if she is not present when the study staff learns of an unanticipated problem in which protocol execution has put subjects or others at a risk which does not appear in the informed consent document.
11.5.1 Reporting Unanticipated Problems: Reports of unanticipated problems will be promptly forwarded to the IRBs.
11.5.2 WRAIR IRB will review unanticipated problems related to this study only if they relate to the transfer, storage or processing of the specimens collected under this protocol
12. Participant compensationParticipants will be compensated 1000 baht for the visit that include neurological examination and neuropsychological testing, 500 baht for MRI/MRS, and 1500 baht for LP. These amounts are designed to compensate for transportation and missed work while not being coercive.
Version 1.5 Page 25 of 31

SEARCH 011: Peripheral Reservoir of HIV DNA in Monocytes Pivotal to Cognition in HIV Version 1.5, August 6, 2012
PI: V. Valcour
13. Literature Cited
1. Antinori A, Arendt G, Becker JT, et al. Updated research nosology for HIV-associated neurocognitive disorders. Neurology. Oct 3 2007.
2. Gonzalez-Scarano F, Martin-Garcia J. The neuropathogenesis of AIDS. Nat Rev Immunol. Jan 2005;5(1):69-81.
3. Masliah E, DeTeresa RM, Mallory ME, Hansen LA. Changes in pathological findings at autopsy in AIDS cases for the last 15 years. Aids. Jan 7 2000;14(1):69-74.
4. Pulliam L, Gascon R, Stubblebine M, McGuire D, McGrath MS. Unique monocyte subset in patients with AIDS dementia. Lancet. Mar 8 1997;349(9053):692-695.
5. Williams KC, Corey S, Westmoreland SV, et al. Perivascular macrophages are the primary cell type productively infected by simian immunodeficiency virus in the brains of macaques: implications for the neuropathogenesis of AIDS. J Exp Med. Apr 16 2001;193(8):905-915.
6. Shiramizu B, Ratto-Kim S, Sithinamsuwan P, et al. HIV DNA and Dementia in Treatment-Naive HIV-1-Infected Individuals in Bangkok, Thailand. Int J Med Sci. 2006;4(1):13-18.
7. Shiramizu B, Gartner S, Williams A, et al. Circulating proviral HIV DNA and HIV-associated dementia. Aids. Jan 3 2005;19(1):45-52.
8. Budka H. The neuropathology of HIV-associated brain injury. In: Gendelman HG, I; Everall, I; Lipton, S; Swindells,S., ed. The Neurology of AIDS, 2nd edition. New York: Oxford University Press; 2005.
9. Anderson E, Zink W, Xiong H, Gendelman HE. HIV-1-associated dementia: a metabolic encephalopathy perpetrated by virus-infected and immune-competent mononuclear phagocytes. J Acquir Immune Defic Syndr. Oct 1 2002;31 Suppl 2:S43-54.
10. Lawrence DM, Major EO. HIV-1 and the brain: connections between HIV-1-associated dementia, neuropathology and neuroimmunology. Microbes Infect. Mar 2002;4(3):301-308.
11. Kaul M, Garden GA, Lipton SA. Pathways to neuronal injury and apoptosis in HIV-associated dementia. Nature. Apr 19 2001;410(6831):988-994.
12. Gonzalez-Scarano F, Baltuch G. Microglia as mediators of inflammatory and degenerative diseases. Annu Rev Neurosci. 1999;22:219-240.
13. McArthur JC, Brew BJ, Nath A. Neurological complications of HIV infection. Lancet Neurol. Sep 2005;4(9):543-555.
14. Williams KC, Hickey WF. Central nervous system damage, monocytes and macrophages, and neurological disorders in AIDS. Annu Rev Neurosci. 2002;25:537-562.
15. Glass JD, Fedor H, Wesselingh SL, McArthur JC. Immunocytochemical quantitation of human immunodeficiency virus in the brain: correlations with dementia. Ann Neurol. Nov 1995;38(5):755-762.
16. Gartner S. HIV infection and dementia. Science. Jan 28 2000;287(5453):602-604.17. Sonza S, Mutimer HP, Oelrichs R, et al. Monocytes harbour replication-competent, non-latent HIV-1 in
patients on highly active antiretroviral therapy. Aids. Jan 5 2001;15(1):17-22.18. Perelson AS, Essunger P, Cao Y, et al. Decay characteristics of HIV-1-infected compartments during
combination therapy. Nature. May 8 1997;387(6629):188-191.19. Gendelman HE, Orenstein JM, Martin MA, et al. Efficient isolation and propagation of human
immunodeficiency virus on recombinant colony-stimulating factor 1-treated monocytes. J Exp Med. Apr 1 1988;167(4):1428-1441.
20. Garaci E, Palamara AT, Ciriolo MR, et al. Intracellular GSH content and HIV replication in human macrophages. J Leukoc Biol. Jul 1997;62(1):54-59.
21. Belmonte L, Bare P, Picchio GR, et al. Decreased recovery of replication-competent HIV-1 from peripheral blood mononuclear cell-derived monocyte/macrophages of HIV-positive patients after 3 years on highly active antiretroviral therapy. Aids. Jun 14 2002;16(9):1289-1292.
Version 1.5 Page 26 of 31
SEARCH 011: Peripheral Reservoir of HIV DNA in Monocytes Pivotal to Cognition in HIV Version 1.5, August 6, 2012
PI: V. Valcour 22. Shiramizu B, Gartner S, Cho M, et al. Assessment of HIV-1 DNA copies per cell by real-time
polymerase chain reaction. Front Biosci. Jan 1 2004;9:255-261.23. Zhu T, Muthui D, Holte S, et al. Evidence for human immunodeficiency virus type 1 replication in vivo
in CD14(+) monocytes and its potential role as a source of virus in patients on highly active antiretroviral therapy. J Virol. Jan 2002;76(2):707-716.
24. Finzi D, Blankson J, Siliciano JD, et al. Latent infection of CD4+ T cells provides a mechanism for lifelong persistence of HIV-1, even in patients on effective combination therapy. Nat Med. May 1999;5(5):512-517.
25. Wong JK, Hezareh M, Gunthard HF, et al. Recovery of replication-competent HIV despite prolonged suppression of plasma viremia. Science. Nov 14 1997;278(5341):1291-1295.
26. Zhang L, Ramratnam B, Tenner-Racz K, et al. Quantifying residual HIV-1 replication in patients receiving combination antiretroviral therapy. N Engl J Med. May 27 1999;340(21):1605-1613.
27. Valentin A, Rosati M, Patenaude DJ, et al. Persistent HIV-1 infection of natural killer cells in patients receiving highly active antiretroviral therapy. Proc Natl Acad Sci U S A. May 14 2002;99(10):7015-7020.
28. Shiramizu B, Shikuma C, Ratto-Kim S, Valcour V. HIV DNA in PBMC and Monocytes Associated with Dementia. Paper presented at: 14th Conference on Retroviruses and Opportunistic Infections2007; Los Angeles, California.
29. McDermott JL, Giri AA, Martini I, et al. Level of human immunodeficiency virus DNA in peripheral blood mononuclear cells correlates with efficacy of antiretroviral therapy. J Clin Microbiol. Jul 1999;37(7):2361-2365.
30. Pellegrin I, Caumont A, Garrigue I, et al. Predictive value of provirus load and DNA human immunodeficiency virus genotype for successful abacavir-based simplified therapy. J Infect Dis. Jan 1 2003;187(1):38-46.
31. Rouzioux C, Hubert JB, Burgard M, et al. Early Levels of HIV-1 DNA in Peripheral Blood Mononuclear Cells Are Predictive of Disease Progression Independently of HIV-1 RNA Levels and CD4+ T Cell Counts. J Infect Dis. Jul 1 2005;192(1):46-55.
32. Goujard C, Bonarek M, Meyer L, et al. CD4 cell count and HIV DNA level are independent predictors of disease progression after primary HIV type 1 infection in untreated patients. Clin Infect Dis. Mar 1 2006;42(5):709-715.
33. Sacktor N. The epidemiology of human immunodeficiency virus-associated neurological disease in the era of highly active antiretroviral therapy. J Neurovirol. Dec 2002;8 Suppl 2:115-121.
34. Cysique LA, Maruff P, Brew BJ. Prevalence and pattern of neuropsychological impairment in human immunodeficiency virus-infected/acquired immunodeficiency syndrome (HIV/AIDS) patients across pre- and post-highly active antiretroviral therapy eras: a combined study of two cohorts. J Neurovirol. Dec 2004;10(6):350-357.
35. Deutsch R, Ellis RJ, McCutchan JA, Marcotte TD, Letendre S, Grant I. AIDS-associated mild neurocognitive impairment is delayed in the era of highly active antiretroviral therapy. Aids. Sep 28 2001;15(14):1898-1899.
36. McArthur JC, Haughey N, Gartner S, et al. Human immunodeficiency virus-associated dementia: an evolving disease. J Neurovirol. Apr 2003;9(2):205-221.
37. Cysique LA, Maruff P, Brew BJ. Variable benefit in neuropsychological function in HIV-infected HAART-treated patients. Neurology. May 9 2006;66(9):1447-1450.
38. Cysique LA, Maruff P, Brew BJ. The neuropsychological profile of symptomatic AIDS and ADC patients in the pre-HAART era: a meta-analysis. J Int Neuropsychol Soc. May 2006;12(3):368-382.
39. Tozzi V, Balestra P, Galgani S, et al. Changes in neurocognitive performance in a cohort of patients treated with HAART for 3 years. J Acquir Immune Defic Syndr. Sep 1 2001;28(1):19-27.
Version 1.5 Page 27 of 31
SEARCH 011: Peripheral Reservoir of HIV DNA in Monocytes Pivotal to Cognition in HIV Version 1.5, August 6, 2012
PI: V. Valcour 40. Talos IF, Mian AZ, Zou KH, et al. Magnetic resonance and the human brain: anatomy, function and
metabolism. Cell Mol Life Sci. May 2006;63(10):1106-1124.41. Chong WK, Sweeney B, Wilkinson ID, et al. Proton spectroscopy of the brain in HIV infection:
correlation with clinical, immunologic, and MR imaging findings. Radiology. Jul 1993;188(1):119-124.42. Meyerhoff DJ, MacKay S, Poole N, Dillon WP, Weiner MW, Fein G. N-acetylaspartate reductions
measured by 1H MRSI in cognitively impaired HIV-seropositive individuals. Magn Reson Imaging. 1994;12(4):653-659.
43. Chong WK, Paley M, Wilkinson ID, et al. Localized cerebral proton MR spectroscopy in HIV infection and AIDS. AJNR Am J Neuroradiol. Jan 1994;15(1):21-25.
44. Jarvik JG, Lenkinski RE, Saykin AJ, Jaans A, Frank I. Proton spectroscopy in asymptomatic HIV-infected adults: initial results in a prospective cohort study. J Acquir Immune Defic Syndr Hum Retrovirol. Nov 1 1996;13(3):247-253.
45. Paley M, Cozzone PJ, Alonso J, et al. A multicenter proton magnetic resonance spectroscopy study of neurological complications of AIDS. AIDS Res Hum Retroviruses. Feb 10 1996;12(3):213-222.
46. Vion-Dury J, Salvan AM, Confort-Gouny S, Cozzone PJ. [Brain proton magnetic resonance spectroscopy. Indications for diagnosis and follow-up of HIV-related encephalopathy in the adult]. Presse Med. Sep 19 1998;27(27):1398-1405.
47. Wilkinson ID, Lunn S, Miszkiel KA, et al. Proton MRS and quantitative MRI assessment of the short term neurological response to antiretroviral therapy in AIDS. J Neurol Neurosurg Psychiatry. Oct 1997;63(4):477-482.
48. Wilkinson ID, Miller RF, Miszkiel KA, et al. Cerebral proton magnetic resonance spectroscopy in asymptomatic HIV infection. Aids. Mar 1997;11(3):289-295.
49. Harrison MJ, Newman SP, Hall-Craggs MA, et al. Evidence of CNS impairment in HIV infection: clinical, neuropsychological, EEG, and MRI/MRS study. J Neurol Neurosurg Psychiatry. Sep 1998;65(3):301-307.
50. Yiannoutsos CT, Ernst T, Chang L, et al. Regional patterns of brain metabolites in AIDS dementia complex. Neuroimage. Nov 2004;23(3):928-935.
51. Tarasow E, Wiercinska-Drapalo A, Kubas B, et al. Cerebral MR spectroscopy in neurologically asymptomatic HIV-infected patients. Acta Radiol. Mar 2003;44(2):206-212.
52. Chang L, Ernst T, Witt MD, Ames N, Gaiefsky M, Miller E. Relationships among brain metabolites, cognitive function, and viral loads in antiretroviral-naive HIV patients. Neuroimage. Nov 2002;17(3):1638-1648.
53. Lee PL, Yiannoutsos CT, Ernst T, et al. A multi-center 1H MRS study of the AIDS dementia complex: validation and preliminary analysis. J Magn Reson Imaging. Jun 2003;17(6):625-633.
54. Ernst T, Chang L. Effect of aging on brain metabolism in antiretroviral-naive HIV patients. Aids. Jan 1 2004;18 Suppl 1:S61-67.
55. Meyerhoff DJ, Bloomer C, Cardenas V, Norman D, Weiner MW, Fein G. Elevated subcortical choline metabolites in cognitively and clinically asymptomatic HIV+ patients. Neurology. Mar 23 1999;52(5):995-1003.
56. Suwanwelaa N, Phanuphak P, Phanthumchinda K, et al. Magnetic resonance spectroscopy of the brain in neurologically asymptomatic HIV-infected patients. Magn Reson Imaging. Sep 2000;18(7):859-865.
57. Chang L, Ernst T, Tornatore C, et al. Metabolite abnormalities in progressive multifocal leukoencephalopathy by proton magnetic resonance spectroscopy. Neurology. Apr 1997;48(4):836-845.
58. Simone IL, Federico F, Tortorella C, et al. Localised 1H-MR spectroscopy for metabolic characterisation of diffuse and focal brain lesions in patients infected with HIV. J Neurol Neurosurg Psychiatry. Apr 1998;64(4):516-523.
59. Iranzo A, Moreno A, Pujol J, et al. Proton magnetic resonance spectroscopy pattern of progressive multifocal leukoencephalopathy in AIDS. J Neurol Neurosurg Psychiatry. Apr 1999;66(4):520-523.
Version 1.5 Page 28 of 31
SEARCH 011: Peripheral Reservoir of HIV DNA in Monocytes Pivotal to Cognition in HIV Version 1.5, August 6, 2012
PI: V. Valcour 60. UNAIDS. AIDS Epidemic Update. 2007; www.unaids.org.61. MOPH. Epidemiology of HIV/AIDS in Thailand, Ministry of Public Health. 2007;
www.epid.moph.go.th.62. Khongphatthanayothin M, Tantipaibulvut S, Nookai S, Chumchee P, Kaldor J, Phanuphak P.
Demographic predictors of a positive HIV test result among clients attending a large metropolitan voluntary counselling and testing centre in Thailand. HIV Med. Jul 2006;7(5):281-284.
63. MOPH. National Guidlines for the clinical management of HIV infection in children and adults, 7th edition, 2007 in press2000.
64. WHO. World Health Organization. Scaling up antiretroviral therapy in resource-limited settings: Treatment guidelines for a public health approach, 20062006.
65. Maj M, Janssen R, Satz P, et al. The World Health Organization's cross-cultural study on neuropsychiatric aspects of infection with the human immunodeficiency virus 1 (HIV-1). Preparation and pilot phase. Br J Psychiatry. Sep 1991;159:351-356.
66. Wright E, Brew B, Lal L, et al. Poster E-130: High prevalence of neurocognitive impairment, symptomatic peripheral neuropathy and depression in HIV infected outpatients within the Asia Pacific Region: Findings fo the Asia Pacific NeuroAIDS Consortium (APNAC) study. Paper presented at: Conference on Retroviruses and Opportunistic Infections2006; Denver, Colorado, USA.
67. Maj M, Janssen R, Starace F, et al. WHO Neuropsychiatric AIDS study, cross-sectional phase I. Study design and psychiatric findings. Arch Gen Psychiatry. Jan 1994;51(1):39-49.
68. Valcour VG, Sithinamsuwan P, Nidhinandana S, et al. Neuropsychological abnormalities in patients with dementia in CRF 01_AE HIV-1 infection. Neurology. Feb 13 2007;68(7):525-527.
69. Chelune G, Heaton RG, I; Matthers, C;, Lehman R. Neuropsychological and personality correlates of patients' complaints of disability. In: Tarter R, Goldstein G, eds. Advances in clinical neuropsychology. Vol 3. New York: Plenum Press; 1986.
70. Carey CL, Woods SP, Gonzalez R, et al. Predictive validity of global deficit scores in detecting neuropsychological impairment in HIV infection. J Clin Exp Neuropsychol. May 2004;26(3):307-319.
71. Gaywee J, Artenstein AW, VanCott TC, et al. Correlation of genetic and serologic approaches to HIV-1 subtyping in Thailand. J Acquir Immune Defic Syndr Hum Retrovirol. Dec 1 1996;13(4):392-396.
72. Webb PG, Sailasuta N, Kohler SJ, Raidy T, Moats RA, Hurd RE. Automated single-voxel proton MRS: technical development and multisite verification. Magn Reson Med. Apr 1994;31(4):365-373.
73. Chomont N, El-Far M, Ancuta P, et al. HIV reservoir size and persistence are driven by T cell survival and homeostatic proliferation. Nat Med. Aug 2009;15(8):893-900.
74. Janbazian L, Price DA, Canderan G, et al. Clonotype and repertoire changes drive the functional improvement of HIV-specific CD8 T cell populations under conditions of limited antigenic stimulation. J Immunol. Feb 1 2012;188(3):1156-1167.
Version 1.5 Page 29 of 31

SEARCH 011: Peripheral Reservoir of HIV DNA in Monocytes Pivotal to Cognition in HIV Version 1.5, August 6, 2012
PI: V. Valcour Appendix I: Table of follow-up for subjects (n=60)
Screening Entrya 6 months 1 year Annually after one year
Early terminationb
Inclusion/exclusion form XBaseline demographics XVital signs, body weight X X X X X XNeurological examination X X X X XNeuropsychological evaluation X X X X XMRI, MRS, DTI Xk Xk Xk
Lumbar Puncture (LP) Xc Xc
IHDS X X X XInterim evaluation form X X X X XLaboratory/Specimens
CBC X (2ml) X (2ml) X (2ml) X (2ml) X (2ml)Chemistriesd X (5ml) X (5ml)Glucose X (3ml) X (3ml) i X (3ml) i
Total protein X (2ml) i X (2ml) i
PT/PTT X (3ml) X (3ml)e
HCV Serology X (3ml)TSH/free T4 X (3ml)Serum Cryptococcal Antigen X (3ml)VDRL with FTA-abs if (+) X (3ml)B12 Level X ( 3ml)Urine Toxicology Screen X X X X XUrine for repository X XUrine pregnancy test X X X X XHIV Viral Load (RNA)f X (3ml) X (3ml) X (3ml) X (3ml) X (3ml)Screening HIV DNA in PBMC X (5ml)Monocyte HIV DNA and monocytes for supernatantsf X(30ml) X(30ml) X (30ml) X(30ml) CD4/CD8 counts X (3ml) X (3ml) X (3ml) X (3ml) X (3ml)CSF cell count, glucose and protein X
CSF viral load and repositoryf X Xc
PBMC and sera storage g X (30ml)h X (30ml) X (29ml) X (30ml)Total volume of blood 33 ml 66-72j ml 68 ml 70-76j ml 68 ml 13 ml
Version 1.5 Page 30 of 31

SEARCH 011: Peripheral Reservoir of HIV DNA in Monocytes Pivotal to Cognition in HIV Version 1.5, August 6, 2012
PI: V. Valcour a. Entry visit will occur within 45 days of the screening visit and before initiation of ARV. Most cases will enroll within 30 days. All procedures will be completed
within 7 days. b. Early termination studies will be completed only when participant is agreeablec. LP is optional at baseline and 1 yeard. Chemistries include cholesterol, Triglycerides, T Bili, Alk Phos, ALT, and Creatinine.e. PT/PTT completed only if participant agreeable to LPf. Blood draw for HIV RNA, HIV DNA, and supernatants to occur on the day of LP, when LP occurs. g. Blood draw for PBMC/sera will be done on the same day of HIV RNA, HIV DNA and supernatantsh. In cases of co-enrollment with other studies, blood draw for specimen storage may be completed at screening rather than entry.i. Additional 3+2 mL blood draw for glucose and protein level on the same day of LP performed at baseline and 1 yearj. Total volume of blood if LP performed.k. MRI, MRS, and DTI are optional procedures.
Version 1.5 Page 31 of 31





























