Embed Size (px)
Citation preview
Magnetic Resonance Imaging of the Hip Hollis G. Potter, MD
Chief, MRI Director of Research, Dept. of Radiology & Imaging
Hospital for Special Surgery Professor of Radiology
Weill Medical College of Cornell University
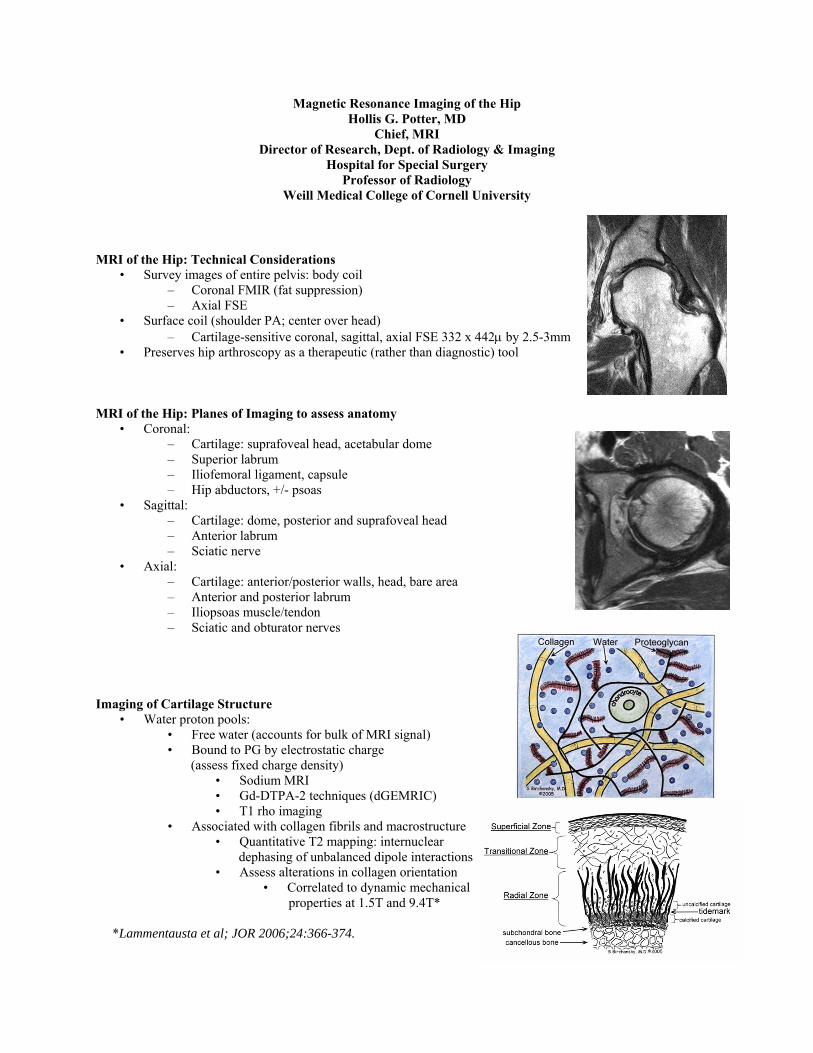
MRI of the Hip: Technical Considerations
• Survey images of entire pelvis: body coil – Coronal FMIR (fat suppression) – Axial FSE
• Surface coil (shoulder PA; center over head) – Cartilage-sensitive coronal, sagittal, axial FSE 332 x 442μ by 2.5-3mm
• Preserves hip arthroscopy as a therapeutic (rather than diagnostic) tool MRI of the Hip: Planes of Imaging to assess anatomy
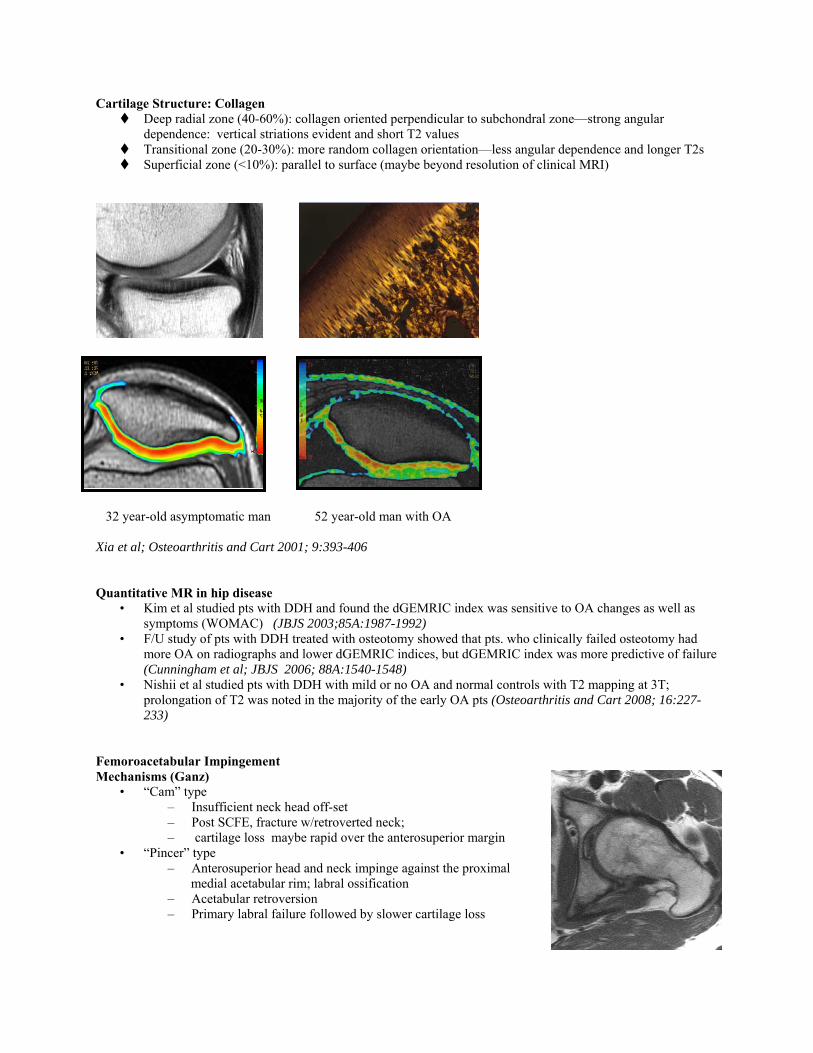
• Coronal: – Cartilage: suprafoveal head, acetabular dome – Superior labrum – Iliofemoral ligament, capsule – Hip abductors, +/- psoas
• Sagittal: – Cartilage: dome, posterior and suprafoveal head – Anterior labrum – Sciatic nerve
• Axial: – Cartilage: anterior/posterior walls, head, bare area – Anterior and posterior labrum – Iliopsoas muscle/tendon – Sciatic and obturator nerves
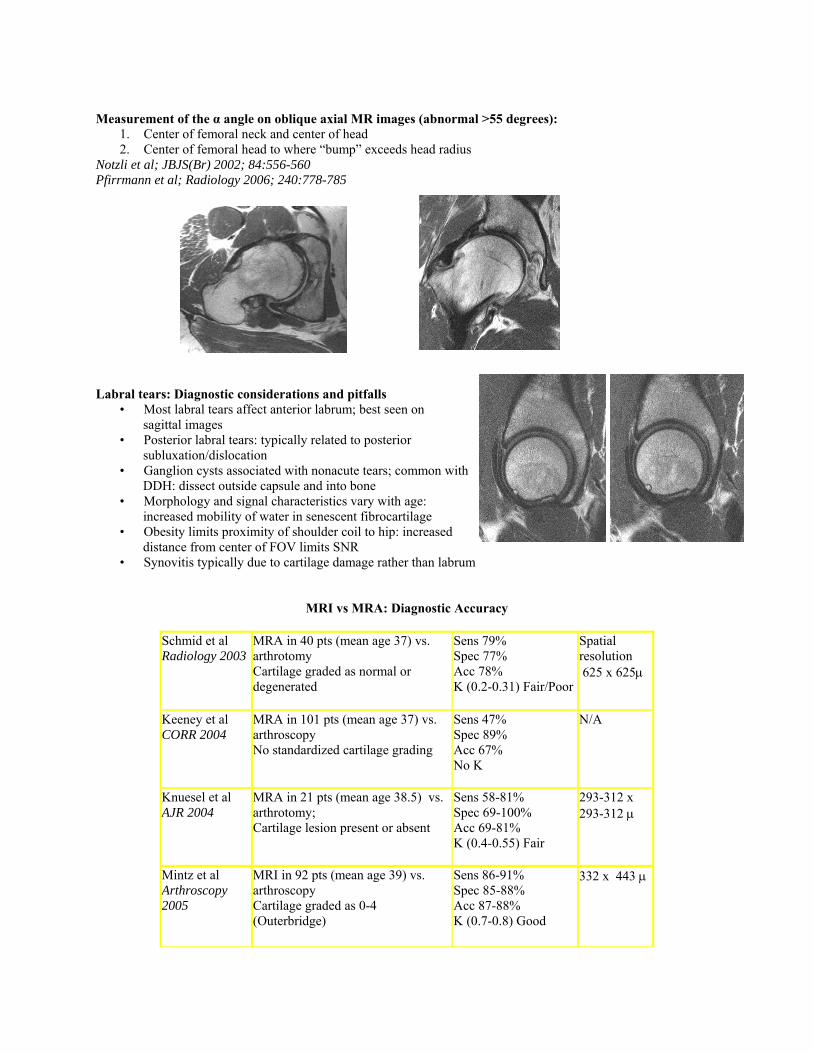
Imaging of Cartilage Structure
• Water proton pools: • Free water (accounts for bulk of MRI signal) • Bound to PG by electrostatic charge (assess fixed charge density)
• Sodium MRI • Gd-DTPA-2 techniques (dGEMRIC) • T1 rho imaging
• Associated with collagen fibrils and macrostructure • Quantitative T2 mapping: internuclear dephasing of unbalanced dipole interactions • Assess alterations in collagen orientation
• Correlated to dynamic mechanical properties at 1.5T and 9.4T* *Lammentausta et al; JOR 2006;24:366-374.
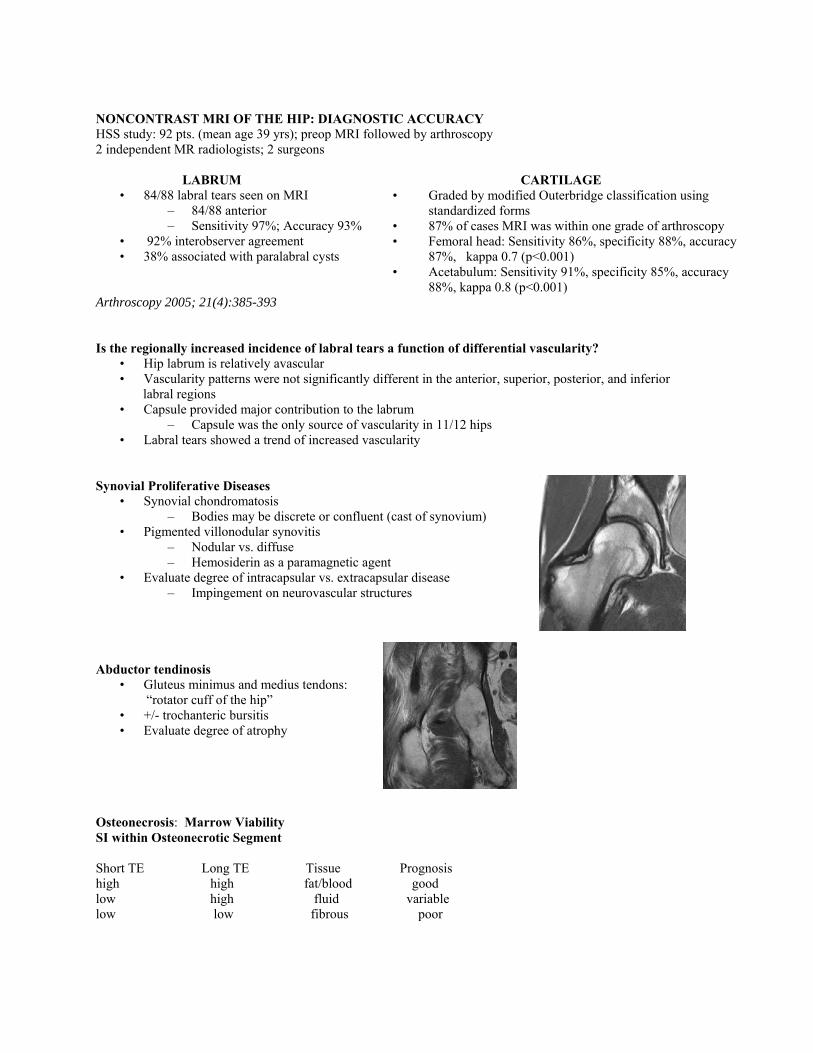
Cartilage Structure: Collagen Deep radial zone (40-60%): collagen oriented perpendicular to subchondral zone—strong angular
dependence: vertical striations evident and short T2 values Transitional zone (20-30%): more random collagen orientation—less angular dependence and longer T2s Superficial zone (<10%): parallel to surface (maybe beyond resolution of clinical MRI)
32 year-old asymptomatic man 52 year-old man with OA Xia et al; Osteoarthritis and Cart 2001; 9:393-406 Quantitative MR in hip disease
• Kim et al studied pts with DDH and found the dGEMRIC index was sensitive to OA changes as well as symptoms (WOMAC) (JBJS 2003;85A:1987-1992)
• F/U study of pts with DDH treated with osteotomy showed that pts. who clinically failed osteotomy had more OA on radiographs and lower dGEMRIC indices, but dGEMRIC index was more predictive of failure (Cunningham et al; JBJS 2006; 88A:1540-1548)
• Nishii et al studied pts with DDH with mild or no OA and normal controls with T2 mapping at 3T; prolongation of T2 was noted in the majority of the early OA pts (Osteoarthritis and Cart 2008; 16:227-233)
Femoroacetabular Impingement Mechanisms (Ganz)
• “Cam” type – Insufficient neck head off-set – Post SCFE, fracture w/retroverted neck; – cartilage loss maybe rapid over the anterosuperior margin
• “Pincer” type – Anterosuperior head and neck impinge against the proximal medial acetabular rim; labral ossification – Acetabular retroversion – Primary labral failure followed by slower cartilage loss
Measurement of the α angle on oblique axial MR images (abnormal >55 degrees):
1. Center of femoral neck and center of head 2. Center of femoral head to where “bump” exceeds head radius
Notzli et al; JBJS(Br) 2002; 84:556-560 Pfirrmann et al; Radiology 2006; 240:778-785 Labral tears: Diagnostic considerations and pitfalls
• Most labral tears affect anterior labrum; best seen on sagittal images • Posterior labral tears: typically related to posterior subluxation/dislocation • Ganglion cysts associated with nonacute tears; common with DDH: dissect outside capsule and into bone • Morphology and signal characteristics vary with age: increased mobility of water in senescent fibrocartilage • Obesity limits proximity of shoulder coil to hip: increased distance from center of FOV limits SNR • Synovitis typically due to cartilage damage rather than labrum
MRI vs MRA: Diagnostic Accuracy
Schmid et al Radiology 2003
MRA in 40 pts (mean age 37) vs. arthrotomy Cartilage graded as normal or degenerated
Sens 79% Spec 77% Acc 78% Κ (0.2-0.31) Fair/Poor
Spatial resolution 625 x 625μ
Keeney et al CORR 2004
MRA in 101 pts (mean age 37) vs. arthroscopy No standardized cartilage grading
Sens 47% Spec 89% Acc 67% No Κ
N/A
Knuesel et al AJR 2004
MRA in 21 pts (mean age 38.5) vs. arthrotomy; Cartilage lesion present or absent
Sens 58-81% Spec 69-100% Acc 69-81% Κ (0.4-0.55) Fair
293-312 x 293-312 μ
Mintz et al Arthroscopy 2005
MRI in 92 pts (mean age 39) vs. arthroscopy Cartilage graded as 0-4 (Outerbridge)
Sens 86-91% Spec 85-88% Acc 87-88% Κ (0.7-0.8) Good
332 x 443 μ
NONCONTRAST MRI OF THE HIP: DIAGNOSTIC ACCURACY HSS study: 92 pts. (mean age 39 yrs); preop MRI followed by arthroscopy 2 independent MR radiologists; 2 surgeons
LABRUM CARTILAGE
• 84/88 labral tears seen on MRI • Graded by modified Outerbridge classification using standardized forms
• 87% of cases MRI was within one grade of arthroscopy • Femoral head: Sensitivity 86%, specificity 88%, accuracy
87%, kappa 0.7 (p<0.001) • Acetabulum: Sensitivity 91%, specificity 85%, accuracy
88%, kappa 0.8 (p<0.001)
– 84/88 anterior – Sensitivity 97%; Accuracy 93%
• 92% interobserver agreement • 38% associated with paralabral cysts
Arthroscopy 2005; 21(4):385-393 Is the regionally increased incidence of labral tears a function of differential vascularity?
• Hip labrum is relatively avascular • Vascularity patterns were not significantly different in the anterior, superior, posterior, and inferior labral regions • Capsule provided major contribution to the labrum
– Capsule was the only source of vascularity in 11/12 hips • Labral tears showed a trend of increased vascularity
Synovial Proliferative Diseases
• Synovial chondromatosis – Bodies may be discrete or confluent (cast of synovium)
• Pigmented villonodular synovitis – Nodular vs. diffuse – Hemosiderin as a paramagnetic agent
• Evaluate degree of intracapsular vs. extracapsular disease – Impingement on neurovascular structures
Abductor tendinosis
• Gluteus minimus and medius tendons: “rotator cuff of the hip” • +/- trochanteric bursitis • Evaluate degree of atrophy
Osteonecrosis: Marrow Viability SI within Osteonecrotic Segment Short TE Long TE Tissue Prognosis high high fat/blood good low high fluid variable low low fibrous poor

Stress Fractures • MRI is more sensitive than radiographs or Tc99-MDP bone scan • Shows wider spectrum of stress reaction to bone • Accelerated remodeling → fatigue → exhaustion → fracture • Soft tissue edema → periosteal reaction
→ cortical fracture → nonunion High Resolution Noncontrast MR Imaging
• Strict attention to imaging technique imperative • Consider optimized noncontrast imaging as an alternative to intra-articular contrast:
– Visualize “native” capsule – Preserves MR as noninvasive – Reduced cost – Increased patient throughput; increased unit productivity – Same images sensitive for cartilage, ligament and labral pathology
References 1. Siebenrock KA, Schoeniger R, Ganz R. Anterior femoroacetabular impingement due to acetabular
retroversion. J Bone Joint Surg 2003; 85A(2):278-286. 2. Abe I, Harada Y, Oinuma K, Kamikawa K, Kitahara H, Morita F, Moriya H. Acetabular labrum: Abnormal
findings at MR imaging in asymptomatic hips. Radiology 2000; 216:576-581. 3. Schmid MR, Nötzli HP, Zanetti M, Wyss TF, Hodler J. Cartilage lesions in the hip: Diagnostic effectiveness
of MR arthrography. Radiology 2003; 226:382-386. 4. Leunig M, Swelen S, Ungersböck, Ito K, Ganz R. Evaluation of the acetabular labrum by MR arthrography. J
Bone Joint Surg 1997; 79B:230-234. 5. Lecouvet FE, Vande Berg BC, Malghem J, Lebon CJ, Moysan P, Jamart J, Maldague BE. MR imaging of the
acetabular labrum: Variations in 200 asymptomatic hips. Am J Roentgenol 1996; 167:1025-1028. 6. Ferguson SJ, Bryant JT, Ganz R, Ito K. The influence of the acetabular labrum on hip joint cartilage
consolidation: A poroelastic finite element model. J Biomech 2000; 33(8):953-960. 7. Moorman III CT, Warren RF, Hershman EB, Crowe JF, Potter HG, Barnes R, O’Brien SJ, Guettler JH.
Traumatic posterior hip subluxation in American football. J Bone Joint Surg 2003; 85A(7):1190-1196. 8. Kelly BL, Shapiro GS, DiGiovanni CW, Buly RL, MD, Potter HG, Hannafin JA. Vascularity of the hip
labrum: A cadaveric investigation. Arthroscopy 2005; 21(1):3-11. 9. Mintz DN, Hooper TR, Connell DA, Buly R, Padgett DE, Potter HG. Magnetic resonance imaging of the hip:
detection of labral and chondral abnormalities using non-contrast imaging. Arthroscopy 2005; 21(4):385-393. 10. Pfirrmann CWA, Mengiardi B, Dora C, Kalberer F, Zanetti M, Hodler J. Cam and pincer femoroacetabular
impingement: Characteristic MR arthrographic findins in 50 patients. Radiology 2006; 240(3):778-785. 11. Cunningham T, Jessel R, Zurakowski D, Millis MB, Kim YJ. Delayed gadolinium-enhanced Magnetic
Resonance Imaging of cartilage to predict early failure of bernese periacetabular osteotomy for hip dysplasia. J Bone Joint Surg 2006; 881:1540-1548.
12. Kim YJ, Jaramillo D, Millis MB, Gray ML, Burstein D. Assessment of early osteoarthritis in hip dysplasia with delayed gadolinium-enhanced Magnetic Resonance Imaging of cartilage. J Bone Joint Surg 2003; 85A(10):1987-1992.
13. Nishii T, Tanaka H, Sugano, N, Sakai T, Hananouchi T, Yoshikawa H. Evaluation of cartilage matrix disorders by T2 relaxation time in patients with hip dysplasia. Osteoarthritis Cart 2008; 16:227-233.








![Appendix 1 HIP Male and Female - University of East Anglia · App14.1!HIP!v3.2_02_05_2012!!!!!Health’Improvement’Profile[HIP]’ ’’’’’’’’’’’’’’’’’’’’’’’’’’’’(HIP)–’Male](https://img.dokumen.tips/doc/110x75/5f0af26b7e708231d42e1f1c/appendix-1-hip-male-and-female-university-of-east-anglia-app141hipv3202052012healthaimprovementaprofilehipa.jpg)




















