Embed Size (px)
Citation preview

RADIOLOGY—PICTORIAL ESSAY
Magnetic resonance imaging in adults with epilepsy:A pictorial essayJolandi van Heerden,1 Patricia M. Desmond,1 Brian M. Tress,1 Patrick Kwan,2 Terence J. O’Brien2 andElaine H. Lui1
1Department of Radiology and 2Departments of Medicine and Neurology, The Royal Melbourne Hospital, The University of Melbourne, Melbourne,
Victoria, Australia
J van Heerden MBChB, MMed (radiology),
FRANZCR; PM Desmond MSc MDBS FRANZCR;
BM Tress MDBS FRANZCR FRCR; P KwanBMedSci, MBBBC, FRACP, PhD; TJ O’BrienMBBS, FRACP; EH Lui MBBS, MMed
(radiology), FRANZCR.
CorrespondenceDr Jolandi van Heerden, Department of
Radiology, The Royal Melbourne Hospital, 300
Grattan Street, Parkville, Melbourne, Vic. 3050,
Australia.
Email: [email protected]
Conflict of interest: None of the authors have
conflicts of interest to declare.
Disclaimer: No funding was received for
this pictorial essay. All the images have
been anonymised and were collected
retrospectively.
Submitted 28 November 2013; accepted 07
December 2013.
doi:10.1111/1754-9485.12150
Summary
This pictorial essay highlights the role of the radiologist as a member of theadult epilepsy multidisciplinary team, and gives an overview of MRI-evidentepileptogenic lesions.
Key words: adult neuroimaging; magnectic resonance imaging;neuroradiology.
Background
Epilepsy is a chronic neurologic condition characterisedby recurrent epileptic seizures as clinical manifesta-tions of abnormal, excessive neuronal activity, affecting0.5–1% of the world population.1 The diagnosis andmanagement of patients with epilepsy have evolved intoa multidisciplinary team approach involving neurolo-gists sub-specialised as epileptologists, neurosurgeons,neuropsychiatrists, neuropsychologists, social workers,specialist nurses, counsellors, nuclear medicine physi-cians and radiologists.1
The primary role of a radiologist is to assess for thepresence of structural abnormalities that may be a causeof the epilepsy. Magnetic resonance imaging (MRI) is
currently the structural imaging modality of choice. Mag-netic resonance imaging in combination with clinicalassessment, electroencephalography, single-photonemission computed tomography and/or positron emis-sion tomography aid with diagnosis and management.
In treatment-refractory cases where multidisciplinaryclinical, radiological, nuclear medicine and electro-physiological findings are concordant, surgical resectionof a focal epileptogenic lesion situated in a non-eloquentbrain region can be considered. In this context, theradiologist can further assist with preoperative planning.
Seizure classification is complex and evolving and canbe classified by mode of seizure onset (generalised/focal), aetiology (genetic, structural/metabolic, un-known) or by syndromes.2 Although the precise
bs_bs_banner
Journal of Medical Imaging and Radiation Oncology •• (2014) ••–••
© 2014 The Royal Australian and New Zealand College of Radiologists 1

terminology is under revision, the clinical importance ofwhether there is impairment of awareness during aseizure is well recognised. Structural lesions identifiableby MRI often (but not always) present with focal epilepsyand knowledge of typical seizure symptoms and signscan help target the search for a subtle structural lesion(Table 1).1 For instance, focal onset seizures associatedwith impaired awareness most frequently emanate fromthe temporal lobe, where the commonest associatedstructural abnormality is mesial temporal sclerosis(MTS). However, a structural potentially epileptogeniclesion may not be the cause of a patient’s epilepsy, andcorrelation with clinical, electroencephalography and/orother nuclear medicine imaging findings is essential.
Utilisation of a targeted epilepsy protocol will optimisethe detection of subtle lesions. Recently, an ‘essential6’ sequence protocol has been suggested that includesvolumetric T1WI, thin-section two-plane fluid-attenuated inversion recovery and T2WI (angled to thehippocampi) as well as a haemosiderin/calcification-sensitive sequence.3
a
c d e
b
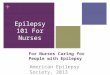
Fig. 1. Mesial temporal sclerosis (MTS). (a) Thin section coronal T2WI MRI showing typical left mesial temporal sclerosis (thick white arrow). The left hippocampus
has a reduced volume, loss of internal architectural definition and increased signal. (b) Coronal fluid-attenuated inversion recovery MRI in a different patient
demonstrating loss of grey–white matter differentiation in the right anterior temporal lobe with increased signal, often associated with ipsilateral MTS/temporal lobe
epilepsy. (c) and (d) Preoperative functional MRI (fMRI) in a patient with left-sided MTS showing ipsilateral language dominance with dominant left Wernicke’s area
activation (long white arrow in d) and bilateral Broca’s area activation (short white arrows in c). (e) Post-hippocampectomy sagittal T1WI shows a small volume
residual hippocampal posterior body and tail (white arrow).
Table 1. Typical seizure symptoms related to various regions of the brain1
Likely location of
epileptogenic focus
Symptoms and signs
Frontal lobe Bizarre complex behaviour
Forced eye deviation
Mesial temporal lobe Odd smell
Feelings of fear
Butterflies in stomach
Deja vú
Depersonalisation experiences
Supplementary motor cortex Fencer posturing
Motor cortex Focal tonic limb movement
Sensory cortex Paresthesias
Numbness
Pain (rare)
False sense of inability to move limb
Occipital lobe Haemianopia
Flashing lights
Visual distortion
Subjective feeling of eye movement
Visual hallucination (rare)
Nystagmus (rare)
J van Heerden et al.
© 2014 The Royal Australian and New Zealand College of Radiologists2

Mesial temporal sclerosis
Mesial temporal sclerosis is the commonest epileptogenicabnormality detected on MRI in patients with drug-resistant focal epilepsy.4 Well-planned and executed sur-gical resection in appropriately selected patients withMTS has a good prognosis for long-term seizure control.5
High-resolution coronal T2WI sequences angled to thehippocampi are needed to optimally evaluate for thecharacteristic changes of MTS, namely increased T2WIsignal, reduced volume and loss of architecture in theaffected hippocampus (Fig. 1a).4,6 In addition, loss of the
gray–white matter differentiation in the ipsilateral ante-rior temporal lobe is seen in up to 58% of patients withdrug-resistant temporal lobe epilepsy and 64% ofpatients with MTS (Fig. 1b).7 Less frequently, ipsilateral
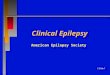
Fig. 2. Right amygdala dysplasia. Coronal T2WI MRI shows enlargement with
increased signal of the right amygdala (black arrow). Amygdala dysplasia was
confirmed histopathologically.
a b c
Fig. 4. Developmental abnormalities. (a) Coronal fluid-attenuated inversion recovery MRI shows type IIb focal cortical dysplasia involving the right superior frontal
sulcus with a characteristic ‘transmantle sign’ (thin white arrow) in a patient with other remote left parietal and left temporal regions of trauma-related cortical injury
(thick white arrows). (b) Volumetric coronal T1WI MRI shows left parietal polymicrogyria with small irregular gyri and thickened cortex (black arrow). (c) Volumetric
axial T1WI MRI demonstrates complex cortical migration and organisation abnormalities with right temporal polymicrogyria (thick black arrow), right temporal
closed lip schizencephaly (thin black arrow), as well as abnormal gyration and morphology of the right hippocampus (white arrows).
Fig. 3. Normal variation. Coronal T2WI MRI shows incomplete inversion of the
left hippocampus. The left hippocampus is more rounded and vertically orien-
tated with preserved signal. In this case, the internal hippocampal architecture
is preserved; however, in some cases, mild blurring may be observed. The
adjacent collateral sulcus is vertically orientated (thick white arrow) with result-
ant irregular shape of the left ventricular temporal horn (black arrow). The left
fornix is inferiorly displaced (thin white arrow).
MRI in adults with epilepsy
© 2014 The Royal Australian and New Zealand College of Radiologists 3

a bFig. 5. Grey matter heterotopia. (a) Volumetric
coronal T1WI MRI shows extensive bi-hemispheric
subcortical grey matter band heterotopia (black
arrows). (b) Coronal T2WI shows a tiny focus of
periventricular nodular grey matter heterotopia
along the roof of the right temporal horn (white
arrow).
a b c
Fig. 6. Sturge Weber syndrome. (a) Axial contrast-enhanced T1WI MRI demonstrates enhancing left occipital pial angiomatosis (white arrows). (b) Axial T2WI shows
left hemispheric atrophy. (c) Susceptibility weighted imaging sequence shows angiomatosis with cortical mineralisation (white arrows). Imaging findings correlated
with the clinically evident cutaneous ‘port wine stain’.
a b c
Fig. 7. Tuberous Sclerosis. Imaging in a patient with worsening seizures in the context of known tuberous sclerosis previously lost to follow-up demonstrating an
interval left frontal high grade glioma. (a) Axial fluid-attenuated inversion recovery MRI shows typical imaging findings related to tuberous sclerosis with left occipital
subcortical tubers (short thick black arrow) and right frontal radial glial bands (long thin black arrows) as well as left periventricular sub-ependymal nodules (white
arrows). (b) and (c) Coronal contrast-enhanced T1WI MRI and axial MRI cerebral blood volume (CBV) perfusion map demonstrate an interval heterogeneously
enhancing left frontal high-grade glial tumour with cortical extension (thick black arrows).
J van Heerden et al.
© 2014 The Royal Australian and New Zealand College of Radiologists4

a b
c
Fig. 8. Low-grade tumours – histopathologically
confirmed. (a) Axial fluid-attenuated inversion
recovery MRI shows a non-enhancing low-grade
glioma involving the left uncus and amygdala
(white arrow). (b) Coronal T2WI MRI demonstrates
a dysembioplastic neuroepithelial tumour involv-
ing the cornu ammonis (CA1–3) of the right
hippocampus (white arrow). (c) Coronal contrast
enhanced T1WI shows a ganglioglioma with
enhancing (black arrow) and non-enhancing cyst-
like (white arrow) components involving the left
para-hippocampal gyrus and fusiform gyrus.
a bFig. 9. Extra-axial tumours causing seizures. (a)
Coronal T2WI MRI shows a craniopharyngioma
with heterogeneous sellar and supra-sellar
proteinaceous cyst-like components impressing
on the left mesial temporal lobe (white arrow) that
correlated with electroencephalography (EEG)
findings. (b) Coronal contrast-enhanced T1WI MRI
shows a right fronto-parietal meningioma (white
arrow) with adjacent cortical and subcortical
signal change (black arrow) with EEG correlation.
a bFig. 10. Traumatic brain injury. (a) Axial T2WI MRI
shows bi-frontal cortical and subcortical
encephalomalacia (white arrows) with ex-vacuo
dilatation of the right ventricular frontal horn. (b)
MRI susceptibility weighted imaging in the same
patient shows trauma-related blood product
deposition along the genu and splenium of the
corpus callosum (black arrows) as well as
bi-frontal cortical superficial siderosis (white
arrows).
MRI in adults with epilepsy
© 2014 The Royal Australian and New Zealand College of Radiologists 5

fornix and mamillary body atrophy can also be seen.4,6
Bilateral MTS is not uncommon, and there is a knownassociation between MTS and a second epileptogeniclesion, particularly cortical dysgenesis, necessitatingcareful assessment of the adjacent cortex and amygdalaas well as the contralateral hippocampus.4 Altered amyg-dala signal with volume increase raises the possibility ofamygdala dysplasia (Fig. 2) or tumour4 (with post-ictalchange a differential), whereas volume loss suggestsamygdala sclerosis.6
Preoperative lateralisation of language dominancewith functional MRI (Fig. 1c,d) can complement preop-erative neuropsychology assessment. A modified partial
mesiotemporal resection can be considered in MTS ipsi-lateral to the side of language dominance to reducethe risk of post-surgical memory-related word-findingdifficulty.8
Following hippocampectomy, it is important tocomment on the amount of residual hippocampus as wellas the extent of post-surgical gliosis to guide decisionmaking if further surgery is considered in the context ofseizure recurrence (Fig. 1e).
One potential pitfall to be aware of is incompletehippocampal inversion – a non-epileptogenic congenitalvariant found in approximately 19% of the general popu-lation (Fig. 3).9
a b c
d e f
Fig. 11. Infection. (a–c) Axial contrast-enhanced T1WI, diffusion-weighted imaging and apparent diffusion coefficient map show a left occipital rim-enhancing,
centrally restricting bacterial abscess (white arrows) with intra-ventricular breakthrough (black arrows). (d) Axial T2WI MRI shows right temporal encephalomalacia
as a late consequence of herpes simplex virus encephalitis. (e–f) Axial T2WI MRI and coronal contrast-enhanced T1WI demonstrating the colloidal vesicular stage
of neurocysticercosis involving the right anterior temporal pole with marked peri-lesional inflammatory reaction (black arrow in e) and lesional rim enhancement as
well as dot-like enhancement of the scolex (white arrow in f).
J van Heerden et al.
© 2014 The Royal Australian and New Zealand College of Radiologists6

Developmental abnormalities
Abnormalities of cortical migration and organisation canbe subtle and should be carefully searched for usinghigh-resolution volumetric imaging with multi-planarreconstructions.
Focal cortical dysplasia (FCD) results from abnormalfocal cortical organisation and is categorised into threetypes on histopathology.10 FCD is classically detectedwith grey–white matter junction blurring and abnormalsubjacent white matter signal.10 Type I is classicallyassociated with focal hypoplasia (‘deep sulcus sign’).10
Type IIb (Taylor’s type with balloon cells) is commonlyassociated with subcortical white matter hyperintensitytapering towards the ventricle (‘transmantle sign’)(Fig. 4a) best appreciated on T2WI and fluid-attenuatedinversion recovery sequences.10
Polymicrogyria and schizencephaly are caused byabnormalities in neuronal migration and cortical organi-sation and have characteristic radiological appearances(Fig. 4b,c).11
Grey matter heterotopia relates to arrested or dis-rupted migration of groups of neurons from periven-tricular germinal zone to cortex and can manifest asperiventricular nodular heterotopias, band heterotopiasor nodular subcortical heterotopias (Fig. 5).11
In the adult population, the diagnosis of congenitalphakomatoses such as tuberous sclerosis and SturgeWeber syndrome (Fig. 6) causing epilepsy is oftenalready established, but occasionally, radiologists maystill be the first to suggest these conditions. In patients
with established diagnoses, follow-up imaging shouldevaluate for interval change (Fig. 7).
Tumours
In young adults with epilepsy, particular tumours toconsider include ganglioglioma, dysembryoplastic neuro-epithelial tumour (DNET), pleomorphic xanthoastro-cytoma (PXA), pilocytic astrocytoma, low-grade gliomaand oligodendroglioma (Fig. 8).12 Tumours can haveassociated FCD (FCD IIIb); thus, peri-tumoural cortexshould also be carefully examined.10,11
In the older adult population, high-grade gliomas(Fig. 7b,c), metastases and other rarer tumours thatclassically involve dural surfaces such as gliosarcomasshould be considered.12
Extra-axial tumours can also cause seizures (Fig. 9).12
Trauma
Traumatic brain injury resulting in contusions, extra-axial haemorrhages or diffuse axonal injury has a highincidence of both early- and late-onset seizures(Fig. 10).13
Infection
Focal seizures can be caused by meningitis but areparticularly associated with instances of focal viral orbacterial cerebritis or abscess formation2 (Fig. 11a–d).Atypical organisms such as neurocysticercosis and
a b c
Fig. 12. Vascular lesions. (a) Axial T2WI MRI shows a right parietal arteriovenous malformation (white arrow) with a superficial nidus involving cortex. (b) Axial T2WI
MRI shows the characteristic ‘pop corn’ appearance of two cavernomas involving the right cerebral peduncle (thick white arrow) and right mesial temporal lobe (thin
white arrow) with associated circumferential haemosiderin blooming (c) Volumetric axial contrast-enhanced T1WI MRI show developmental venous anomalies (black
arrows) associated with the cavernomas shown in (b).
MRI in adults with epilepsy
© 2014 The Royal Australian and New Zealand College of Radiologists 7

tuberculosis can be epileptogenic in all disease phases(Fig. 11e,f).
Vascular
Supra-tentorial cerebral vascular malformations mostfrequently associated with epilepsy are cavernomas andarteriovenous malformations (AVMs), particularly wheninvolving cortex and the temporal lobes (Fig. 12).14
Cavernomas are benign, angiographically occult lesionsconsisting of intertwined clusters of sinusoidal vascularchannels.14 AVMs represent a cluster/nidus of directlycommunicating arteries and veins without an interveningcapillary network.14 Based on size, location and drainage,AVMs are classified using the Spetzler–Martin system forthe purposes of surgical prognostication.14
Haemorrhage as a complication in both AVMs andcavernomas can result in seizures even in previouslyasymptomatic lesions.14
Epileptic seizures can develop as an early or lateconsequence of both arterial and venous corticalinfarcts.15
Conclusion
This pictorial essay highlights the radiologist’s role in theadult epilepsy multidisciplinary team and reviews MRI-evident epileptogenic lesions that should be considered.
References
1. Fisher RS, Stein A, Karls J. Epilepsy for theNeuroradiologist. AJNR 1997; 18: 851–63.
2. Berg AT, Berkovic SF, Brodie MJ, Buchhalter J, CrossJH et al. Revised terminology and concepts fororganization of seizures and epilepsies: report of theILAE Commission on Classification and Terminology.Epilepsia 2010; 51: 676–85.
3. Wellmer J, Quesada CM, Rothe L, Elger CE, Bien CG,Urbach H. Proposal for a magnetic resonance imagingprotocol for the detection of epileptogenic lesionsat early outpatient stages. Epilepsia 2013; 54:1977–87.
4. Malmgren K, Thom M. Hippocampal sclerosis –origins and imaging. Epilepsia 2012; 53 (Suppl 4):19–33.
5. Lowe A, David E, Kilpatrick C, Matkovic Z, Cook M,Kaye A, O’Brien TJ. Epilepsy surgery forpathologically proven hippocampal sclerosis provideslong term seizure control and improved quality oflife. Epilepsia 2004; 45: 237–42.
6. Chan S, Erickson JK, Yoon SS. Limbic systemabnormalities associated with mesial temporalsclerosis: a model of chronic cerebral changes due toseizures. Radiographics 1997; 17: 1095–110.
7. Mitchell LA, Jackson GD, Kalnins RM, Saling MM, FittGJ et al. Anterior temporal abnormality in temporallobe epilepsy: a quantitative MRI and histopathologicstudy. Neurology 1999; 52: 327–36.
8. Mintzer S, Sperling MR. When should a resectionsparing mesial structures be considered for temporallobe epilepsy? Epilepsy Behav 2008; 13: 7–11.
9. Bajic D, Wang C, Kumlien E, Mattsson P, Lundberg S,Eeg-Olofsson O, Raininko R. Incomplete inversion ofthe hippocampus – a common developmentalanomaly. Eur Radiol 2008; 18: 138–42.
10. Colombo N, Tassi L, Galli C, Citterio A, Russo GLet al. Focal cortical dysplasias: MR Imaging,histopathologic, and clinical correlations in surgicallytreated patients with epilepsy. AJNR 2003; 24:724–33.
11. Shorvon SD, Andermann F, Guerrini R (2011) TheCauses of Epilepsy: Common and Uncommon Causesin Adults and Children. Cambridge University Press,Cambridge.
12. Beaumont A, Whittle IR. The pathogenesis of tumourassociated epilepsy. Acta Neurochir (Wien) 2000;142: 1–15.
13. Kazemi H, Hashemi-Fesharaki S, Razaghi S, Najafi M,Kolivand PH et al. Intractable epilepsy andcraniocerebral trauma: analysis of 163 patients withblunt and penetrating head injuries sustained in war.Injury 2012; 43: 2132–5.
14. Brown RD, Fleming KD, Meyer FB, Cloft HJ, PollockBE et al. Natural history, evaluation and managementof intracranial vascular malformations. Mayo Clin Proc2005; 80: 269–81.
15. Beghi E, D’Alessandro R, Beretta S, Consoli D, CrespiV et al. Incidence and predictors of acutesymptomatic seizures after stroke. Neurology 2011;77: 1785–93.
J van Heerden et al.
© 2014 The Royal Australian and New Zealand College of Radiologists8