Embed Size (px)
Citation preview

MAGNETIC MISREACHING
David P. Carey1, Richard J. Coleman2 and Sergio Della Sala1
(1Neuropsychology Research Group, Department of Psychology, University of Aberdeen,Old Aberdeen, Scotland; 2Department of Neurology and Neurosurgery, Aberdeen Royal
Infirmary, Aberdeen, Scotland)
ABSTRACT
Ms D., a 76 year-old woman with a slowly progressive bilateral parietal lobedegeneration, showed an unusual variant of misreaching as yet unreported. When requiredto reach to a target in extrafoveal vision, she slavishly reached straight to the foveal fixationpoint instead (“magnetic misreaching”). Three dimensional recordings of limb movementsto foveal and extrafoveal targets revealed that her reach endpoints were determined by theplace she was looking, independent of the distance between target and fixation point. Thesign was present in both hands. Magnetic misreaching differs from motor misbehaviourswhich follow frontal lobe damage. The neuropsychological and behavioural profile of MsD., coupled with neuroimaging evidence suggest that magnetic misreaching is amanifestation of parietal lobe dysfunction.
INTRODUCTION
Poor reaching to non-foveated visual targets has been labelled as visual“mislocalization”, and is usually a consequence of parietal lobe dysfunction (e.g.Levine, Kaufman and Mohr, 1978; Ratcliff and Davies-Jones, 1972). This sign istypically considered as a less severe variant of “optic ataxia”, where patients areunable to reach to a visual target in spite of being able to “see” the target withfull foveal vision. Patients with full-blown optic ataxia may attempt to improvetheir visuomotor performance by prolonged fixation of the target beforemovement onset (e.g. Pause, Kunesch, Binkofski et al., 1989; Rondot, DeRecondo and Ribadeau Dumas, 1977) or by looking back and forth between thetarget and the reaching hand (Rizzo, Rotella and Darling, 1992). In mostinstances where visual mislocalization has been observed, the pattern of endpointerrors has not been reported (Levine et al., 1978; Rondot et al., 1977), the errorswere randomly distributed, or, in some patients, were clustered in a directiontowards the side of the lesion (Ratcliff and Davies-Jones, 1972). In this paperwe report the case of a patient who misreached when the targets were placed inextrafoveal vision. The peculiarity of her behaviour is that she consistentlyreached towards the point that she was foveating.
CASE REPORT
Ms D., a 76 year-old right-handed woman, presented with a three-yearhistory of increasing clumsiness with her right hand, as well as gait and balance
Cortex, (1997) 33, 639-652

difficulties. Her initial complaint was that fine movements of her right handwere impaired, causing deterioration of her handwriting. She then noticeddifficulties with balance and walking. When our assessment began, she displayeda dramatic limb-kinetic apraxia in both hands (although the right hand [25/72]was more impaired than the left [46/72] as assessed by the Ideomotor ApraxiaTest of De Renzi, Motti and Nichelli, 1980). A CT scan showed noabnormalities. However, two SPECT scans (January 1996 and October 1996)revealed progressive bilateral parietal hypoperfusion, worse in the lefthemisphere (see Figure 1). A recent (June 1997) magnetic resonance scan
640 David P. Carey and Others
Fig. 1 – SPECT scans of Ms D.’s brain taken on two separate occasions, January 1996 (A, C)and October 1996 (B, D). The first scan shows hypoperfusion in the left parietal cortex. After ninemonths, the left parietal hypoperfusion worsens and becomes apparent in the right parietal lobe aswell. Anatomical left appears on the left side of each image.
A B
C D

revealed cortical atrophy in the parietal cortex, worse in the left hemisphere andlargely restricted to the superior parietal lobe (Figure 2).
Neurological examination uncovered some disturbance of horizontal saccadesto command and increased muscle tone (worse on the right side). Agrasping/groping reflex (De Renzi and Barbieri, 1992) was elicited on oneoccasion, but such signs were absent at subsequent tests. Her neurologicalfeatures are similar to those reported in cases of corticobasal degeneration (Gibb,Luthert and Marsden, 1989; Massman, Kreiter, Jankovic et al., 1996; Pillon, Blin,Vidailhet et al., 1995; Rinnie, Lee, Thompson et al., 1994). In many respects MsD.’s illness is similar to cases of slowly progressive apraxia previously reportedin the neuropsychological literature (Azouvi, Bergego, Robel et al., 1993; DeRenzi, 1986; Dick, Snowden, Northen et al., 1989). During the period of ourassessments, Ms D. was still living alone, she was collaborative and witty, andher social behaviour was always appropriate. In formal neuropsychologicaltesting, she did not show deficits in language (e.g. Token Test = 34/36, DeRenzi and Faglioni, 1978) or short or long term memory (e.g. Digit Span = 6,Corsi Block Span = 4; WMS Logical Memory = 8.5). She did not haveunilateral neglect in cancellation or copying tasks. Her scores on screening testsfor dementia were normal (Mini-mental state examination = 27, Folstein, Folsteinand McHugh, 1975). Moreover, she performed within normal limits on testssupposed to assess executive functions (e.g. phonological fluency, F-A-S = 24,Benton and Hamsher, 1976; cognitive estimates = 5 errors, Shallice and Evans,
Magnetic misreaching 641
Fig. 2 – T2-weighted MRI scans of Ms D.’s brain from June 1997. Note the biparietal corticalatrophy, more evident in the left hemisphere. The atrophy is more pronounced in the superior thanthe inferior left parietal lobe. Anatomical left appears on the right side of both images.

1978; modified Wisconsin Card Sorting Test = 4 categories achieved with 2perseverative errors, Nelson, 1976). Ms D. had a profound constructional apraxiawhich affected her drawing, copying, WAIS-R Block Design (scaled score 1)and Object Assembly (scaled score 1) performance. Nevertheless, herperformance was better on visuospatial tests which do not call for constructionalability (e.g. Visual Object and Space Perception Battery Dot counting = 8/10,Position Discrimination = 20/20, Number Location = 8/10, Warrington andJames, 1991). She also showed a slowly progressive apraxic agraphia, and herreading was troublesome due to her difficulty in scanning the lines. She also haddifficulties with multiplication and long division.
A complete ophthalmological examination was unremarkable, including theabsence of any visual field defects as assessed by automatized Humphreyperimetry (although the previously described difficulties with horizontal saccadesto command were confirmed). However, some disturbances in her visually-guided behaviour were apparent in everyday tasks as well as during formaltesting. For example, she missed a hand she was attempting to shake, and placedher pen inappropriately while cancelling lines. Further investigation of hervisuospatial and visuomotor performance exposed a hitherto unreportedneurological sign, which we have labelled “magnetic misreaching”. This is thefocus of the present report.
MAGNETIC MISREACHING
Clinical Observations of Magnetic Misreaching
Ms D. had absolutely no difficulty pointing to or picking up small visualtargets when she was allowed to look at them (i.e. with foveal vision). When shewas not allowed to look directly at the targets, she failed. For example she wasasked to point to a peripheral twenty-pence coin, while looking at a centrallyplaced pound coin. Her first attempts were unsuccessful because she could notinhibit eye movements towards the coin she was supposed to touch.
After her early failures on this task, it was apparent that she was making asecond kind of error: often her hand would begin moving towards the fixationpoint (the pound coin) rather than the target (the twenty-pence coin). When weasked her to move very quickly (e.g. ballistically) she invariably reached to thepoint she was fixating, rather than the target. She was completely aware of thesemisreaching errors and appalled at the difficulty which she had in suppressingher movements to the non-target, fixation point. Informal testing suggested noobvious hemispatial asymmetries in the magnitude of magnetic misreaching. Weobserved the sign in several different testing conditions. Magnetic misreachingeven occurred when there was no visual target to be reached to: when she wasasked to reach into the hemifield opposite to her fixation, her movements weredrawn to the place she was looking at. Placing her hand into the oppositehemispace in order to provide additional (proprioceptive) cues did not attenuateher magnetic errors. If Ms D. was allowed to foveate a target, and then close hereyes before she was allowed to point, she was quite accurate.
642 David P. Carey and Others

Three-dimensional Recordings of Magnetic Misreaching
In a subsequent session, two months later, we examined her misreaching inmore detail, by recording her limb movements using a MacReflex motionanalysis system (Qualisys, Inc.). Videotapes of the session were used as a guideto the success or failure of her fixation efforts and to record herverbal/behavioural responses to her performance on each trial. Four separatetarget arrays were used. Each array contained 3, 4, or 5 coloured circles. Thecoloured targets were randomly arranged on separate 42 × 29.6 cm (A3) sheets.Ms D. was required to count (without pointing) the number of targets present ineach array and to judge which two of the visible targets were closest to oneanother and which two were farthest apart. Ms D.’s performance was errorlesson these perceptual tasks. After the perceptual judgements were made, Ms D.’sreaching behaviour was examined and recorded.
On foveal reaching trials, Ms D. was asked to point to each of the colouredtargets, in turn. She reached to targets with a high degree of accuracy when shewas allowed to foveate them (Figure 3, left). After foveal reaching trials werecompleted, the same array was used to test extrafoveal reaching. Ms D. wasrequired to look at a central black fixation cross while she reached towards aspecified target. She was allowed to look back and forth between fixation andthe target as many times as she wished before indicating her readiness to reach(reaching movements of patients with optic ataxia improve dramatically whensuch “pre-reach” eye movements to the target are allowed; Rondot et al., 1977).In these extrafoveal reaching trials, Ms D. reached to the fixation cross rather
Magnetic misreaching 643
Fig. 3 – Foveal and Extrafoveal Reaching. Left: Foveal Reaching. The dotted lines are actual x-y coordinates of the first four reaching movements to the first target array, made while Ms D. wasfree to look at each target. Right: Extrafoveal Reaching. These are the first four recorded attempts atextrafoveal reaching with the first target array. The three black circles and associated numbers werethe specified targets for the four reaches, each labelled with appropriate target number. In each caseMs D. was instructed to look at the central fixation cross while reaching for the specified target. Intwo of the reaches clear magnetic misreaching was observed (reaches 1 and 3a). After the reachattempt at target 2, Ms D. denied moving her eyes to the target. After the apparently successful reachto target 3 (reach 3b) Ms D. confessed to looking towards the target.

than the intended target (magnetic misreaching; see Figure 3, right). These errorswere unequivocal on 14 of 23 attempts. She was always aware of her errors andoften tried to self-correct before the trial ended. In 8 of the remaining 9 trials,Ms D. admitted to glancing at the target during the movement (e.g. reach 3b inFigure 3). On the remaining trial, when asked if she looked at the target, sheresponded “No, I don’t think so”. The movement path of this reach is depictedin Figure 3 (reach 2). Her initial heading and subsequent corrective movementssuggest a momentary glance towards the intended target. Magnetic misreachingwas also found when we made her fixate a target at a location well beyond thetesting array (not shown).
Magnetic Misreaching and Foveation Eccentricity
We carried out a further experiment in order to ascertain whether or notmagnetic misreaching was related to the eccentricity of the fixation point relativeto the target to be reached to. The target was located in the same placethroughout the experiment, while the position of the fixation point was variedfrom one block of trials to another. The target to be reached towards was a 1 cmdiameter, high contrast (66%) green star (luminance = 69 cd/m2) placed in righthemispace, 22 cm anterior to and 19 cm lateral to a central starting position. Inthe first six trials Ms D. was required to reach to the green star with her index
644 David P. Carey and Others
Fig. 4 – Right and left-handed magnetic misreaching. The panels depict reach paths which wereall supposed to be directed at the right-sided target (depicted in the figure as a circle). The fixationtarget for each block of reaches is indicated by the square in each panel.

finger while she was allowed to foveate it (control trials). For each subsequentblock of trials, Ms D. was informed that she was to point to the green star,while looking at a small gray marker which served as the fixation point. Sixtrials were conducted with three different horizontal fixation locations: 10, 20and 30 cm to the left of the star. As in the previous experiment, we videotapedthe entire session to help confirm the success of Ms D.’s fixation efforts.Additionally, one investigator sat at the end of the table and constantlymonitored her eye movements from a position where breaks in fixation wereeasy to spot. Figure 4 shows Ms D.’s performance using her right and left hand.It is clear from these figures that as the fixation point becomes more eccentric,the magnitude of the patient’s errors increases. The direction of her error is notrandom; she consistently reached towards the fixation point.
Terminal accuracy for each reach was calculated by averaging the X, Y andZ coordinates of the final frames of her movements and comparing the three-dimensional difference of these coordinates to calibration marker coordinates.The calibration coordinates were obtained by placing a MacReflex marker on thegreen star after each block of six trials was completed. Similar calibration trialswere collected for each of the 3 extrafoveal fixation targets. On one trial (in theblock of left 10 cm trials of the left hand), Ms D. actually looked at the greenstar. This trial was omitted from the analysis. Means and standard deviations ofher endpoint errors as a function of target-fixation distance and hand usedappear in Table I. These data confirm our earlier observations that Ms D.’smagnetic misreaching is present in both left and right hands, and is largelyindependent of the distance between the target and the fixation point. Since wepredicted that Ms D.’s terminal errors would increase as fixation eccentricityincreased, for each hand, Page’s L test (Siegal and Castellan, 1988) was used totest these two predictions. In both cases the hypothesis of increasing terminalerrors with increasing target eccentricity was supported (left hand: L(3) = 179, p < 0.01; right hand L(3) = 180, p < 0.01).
DISCUSSION
We observed a patient, Ms D., probably affected by corticobasaldegeneration, presenting with slowly progressive apraxia and balance difficulties.Longitudinal neuroimaging and neuropsychological examinations suggestedprimarily bilateral parietal pathology, more evident in the left hemisphere. Themost unusual feature of this case is “magnetic misreaching”. When she
Magnetic misreaching 645
TABLE I
Mean Endpoint Error (cm) as a Function of Hand Used and Fixation-target Distance (Standard deviations appear in brackets)
Fixation-target distance
Hand 0 (Foveating) 10 cm 20 cm 30 cm
Left 0.49 (0.31) 9.67 (0.81) 21.48 (1.80) 27.64 (4.90)Right 1.22 (0.63) 11.19 (4.23) 14.06 (3.04) 20.28 (4.31)

attempted to reach for a target in extrafoveal vision, she consistently reached forthe fixation point instead. To the best of our knowledge this sign has not beenpreviously reported.
It seems unlikely that her difficulties were related to parafoveal field defectsor difficulties in processing multiple visual targets. First, no field defects werenoted in a full ophthalmological examination. Second, Ms D. showed noevidence of simultanagnosia (e.g. her description of the Cookie Theft Picture[Goodglass and Kaplan, 1983] was complete and accurate). Third, she couldcount the number of target elements in the experimental arrays and describe thespatial relationships between them. Fourth, magnetic misreaching was alsoobserved in the absence of a visual target to be reached towards: when Ms D.was required to fixate on a target far into one hemispace, and to reach towardsthe opposite side of the table surface, she still reached towards the fixation point(i.e. problems “seeing” a peripheral target to be reached towards cannot accountfor magnetic misreaching). Fifth, patients with parafoveal field defects can beinaccurate when pointing to targets appearing in their blind visual field.However, their reach endpoints are by no means clustered around the fixationpoint or any other intact portion of their visual field (Perenin, 1997; Rizzo andDarling, 1996). In other words, if patients have trouble “seeing” a target, theydo not point “by default” to places which they can see.
Ms D.’s magnetic misreaching was not due to subtle difficulties withunderstanding or remembering task instructions. She was quite able to carry outcomplex multi-step procedures (e.g. in the modified Token Test, De Renzi andFaglioni, 1978). During the reaching tests, Ms D. was frequently reminded oftask instructions to the point where she actually exclaimed “I know what I’msupposed to do, I just don’t know how to do it!... My hand just won’t do whatI tell it to do!”. Furthermore, on some trials, Ms D. did manage to partiallyovercome the attraction of the fixation point, and landed in between the placewhere she was looking and the place she was attempting to reach (see Figure 4,Left 20 and Left 30 cm Foveation). This pattern is difficult to interpret in termsof confusion about the desired target in extrafoveal reaching trials.
Magnetic misreaching has some similarities with the motor misbehavioursreported in frontal lobe dysfunction. Denny-Brown (1956, 1958) describedpatients with frontal lesions who failed to inhibit their grasp of felt or seenobjects. There is no mention of a special role of foveal vision in generating thiscomplex manual activity, that Denny-Brown labelled “magnetic (or frontal)apraxia”. Magnetic apraxia was unilateral in most instances. More recently,Lhermitte (1983) called attention to a bilateral form of magnetic apraxia, that henamed “utilization behaviour”. Frontal patients with utilisation behaviour arecompelled to use objects even when there is no attempt to draw attention tothem and they are hidden from sight (Shallice, Burgess, Schon et al., 1989;Brazzelli, Colombo, Della Sala et al., 1994; De Renzi, Cavalleri and Facchini,1996). Clearly, utilisation behaviour does not depend upon the patients foveatingon the objects they covet. Moreover, patients showing either of these two signs,are typically unaware of the motor misbehaviour of the affected hand(s)(Lhermitte, Pillon and Serdaru, 1986; Brazzelli et al., 1994). A third motormisbehaviour which also resembles magnetic misreaching is anarchic hand
646 David P. Carey and Others
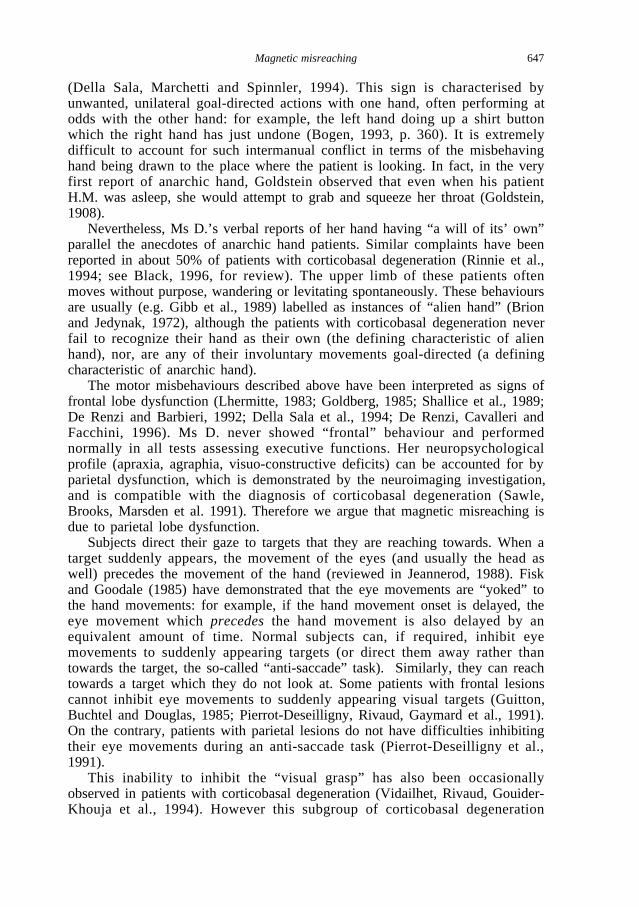
(Della Sala, Marchetti and Spinnler, 1994). This sign is characterised byunwanted, unilateral goal-directed actions with one hand, often performing atodds with the other hand: for example, the left hand doing up a shirt buttonwhich the right hand has just undone (Bogen, 1993, p. 360). It is extremelydifficult to account for such intermanual conflict in terms of the misbehavinghand being drawn to the place where the patient is looking. In fact, in the veryfirst report of anarchic hand, Goldstein observed that even when his patientH.M. was asleep, she would attempt to grab and squeeze her throat (Goldstein,1908).
Nevertheless, Ms D.’s verbal reports of her hand having “a will of its’ own”parallel the anecdotes of anarchic hand patients. Similar complaints have beenreported in about 50% of patients with corticobasal degeneration (Rinnie et al.,1994; see Black, 1996, for review). The upper limb of these patients oftenmoves without purpose, wandering or levitating spontaneously. These behavioursare usually (e.g. Gibb et al., 1989) labelled as instances of “alien hand” (Brionand Jedynak, 1972), although the patients with corticobasal degeneration neverfail to recognize their hand as their own (the defining characteristic of alienhand), nor, are any of their involuntary movements goal-directed (a definingcharacteristic of anarchic hand).
The motor misbehaviours described above have been interpreted as signs offrontal lobe dysfunction (Lhermitte, 1983; Goldberg, 1985; Shallice et al., 1989;De Renzi and Barbieri, 1992; Della Sala et al., 1994; De Renzi, Cavalleri andFacchini, 1996). Ms D. never showed “frontal” behaviour and performednormally in all tests assessing executive functions. Her neuropsychologicalprofile (apraxia, agraphia, visuo-constructive deficits) can be accounted for byparietal dysfunction, which is demonstrated by the neuroimaging investigation,and is compatible with the diagnosis of corticobasal degeneration (Sawle,Brooks, Marsden et al. 1991). Therefore we argue that magnetic misreaching isdue to parietal lobe dysfunction.
Subjects direct their gaze to targets that they are reaching towards. When atarget suddenly appears, the movement of the eyes (and usually the head aswell) precedes the movement of the hand (reviewed in Jeannerod, 1988). Fiskand Goodale (1985) have demonstrated that the eye movements are “yoked” tothe hand movements: for example, if the hand movement onset is delayed, theeye movement which precedesthe hand movement is also delayed by anequivalent amount of time. Normal subjects can, if required, inhibit eyemovements to suddenly appearing targets (or direct them away rather thantowards the target, the so-called “anti-saccade” task). Similarly, they can reachtowards a target which they do not look at. Some patients with frontal lesionscannot inhibit eye movements to suddenly appearing visual targets (Guitton,Buchtel and Douglas, 1985; Pierrot-Deseilligny, Rivaud, Gaymard et al., 1991).On the contrary, patients with parietal lesions do not have difficulties inhibitingtheir eye movements during an anti-saccade task (Pierrot-Deseilligny et al.,1991).
This inability to inhibit the “visual grasp” has also been occasionallyobserved in patients with corticobasal degeneration (Vidailhet, Rivaud, Gouider-Khouja et al., 1994). However this subgroup of corticobasal degeneration
Magnetic misreaching 647

patients also display prominent grasp reflexes and several other signs of frontallobe dysfunction (Jacobs, Adair and Heilman, 1994), which Ms D. did not. Eventhough we were unable to use sophisticated eye tracking to record the exactposition of her eyes during the tests, the few saccadic intrusions that she madewhile we recorded magnetic misreaching were easily identified. Furthermore, herreach endpoints provide strong additional evidence of the success of her fixationefforts in extrafoveal reaching trials.
Extrafoveal reaching requires inhibition of eye movements, as does the anti-saccade task. In addition, subjects must then move their hand to a target they arenot foveating. Ms D. was quite capable of inhibiting her eye movements totargets that she was attempting to reach. However, she invariably failed in herattempts to reach to non-foveated locations, because, much to her dismay, herhand was “magnetized” by the direction of her gaze. Her magnetic misreachingcan be interpreted as a pathological manifestation of the eye-hand yokingdescribed above.
Under normal circumstances, Ms D. did not find her hand drawn towardsany and all locations she happened to be looking at (although on some occasionsshe claimed that she found herself grasping an object which she did intend topick up. Such a symptom could be understood in relation to magneticmisreaching). Magnetic misreaching was observed when we required her toinitiate a goal-directed movement to an extrafoveal target. Before she wasrequired to reach, she routinely claimed that she could “see” both the target tobe reached to and the fixation point. The pathological “imbalance” of the motoraffordances of each potential “target” (the correct extrafoveal target versus theincorrect foveal “target”) was revealed only once the response was initiated. It ispossible that target selection mechanisms of parietal-frontal systems wereimpaired such that the movement was pre-programmed to be directed at thefixation point, in spite of Ms D.’s protests that she always knew what the targetto be reached towards was. Another possibility is that target selection wasappropriate, but that the oculomotor systems maintaining fixation somehow“hijacked” the manual response, leaving her at the mercy of a “default” eye-hand coordinating mechanism (which yokes gaze to hand movements). Althoughthe exact nature of the neural control of target selection, localization andacquisition have yet to be specified, these sorts of mechanisms are likely toinvolve cooperation of parietal and frontal lobe systems.
A number of neurophysiological studies have linked posterior parietal lobemechanisms to the guidance of both limb and eye movements. Cells with firingactivity related to reaching are numerous in the posterior parietal cortex andhave been well-described for over 20 years (e.g. Mountcastle et al., 1975; seeAndersen, Snyder, Bradley et al., 1997; Lynch, 1980, for reviews). Morerecently, sophisticated behavioural training and testing paradigms haveuncovered similar single-cell coding involved in the control and monitoring ofeye and head movements to visual targets. These cells related to the direction ofgaze are located in regions of the posterior parietal cortex which overlap withreaching-related cell activity (e.g. Brotchie, Andersen, Snyder et al., 1995;Galletti, Battaglini and Fattori, 1995; for review see Johnson, Ferraina, Garastoet al., 1997). For example, Brotchie et al. (1995) report that some neurons in the
648 David P. Carey and Others

posterior parietal cortex code for a particular gaze direction, whether or not thatdirection is specified by eye position in the head or head position on the torso.Such signals may provide important information for the control of handmovements to a visual target, since gaze movements are usually completedbefore head movements (see Jeannerod, 1988, 1997, for more completediscussion of these issues).
Although neural activity related to the control of arm movements and gazehas been found in the frontal lobes, and some of this activity may be related to“nonstandard sensorimotor mapping” (see Boussaoud, Di Pellegrino and Wise,1995; Wise, Di Pellegrino and Boussaoud, 1996, for reviews), several recentreports implicate the posterior parietal cortex in the control of both foveal andextrafoveal reaching. Snyder, Batista and Andersen (1997) found that in thelateral intraparietal area (LIP) and in a medial, posterior region, signals relatedto forthcoming arm and eye movements are largely segregated. Such signals maybe integrated in parietal visuomotor areas downstream from these regions, suchas areas 7m and V6 (Ferraina, Johnson, Garasto et al., 1997; Johnson et al.,1997). Some cells in these latter areas responded to an eye movement to a visualtarget, and some to a hand movement, but a majority had both hand- and eye-movement related properties. Previous studies have implicated these regions inthe control of reaching movements. For example, the oculomotor properties ofcells in this region are related to both saccadic activity and eye position beforeas well as after saccades (Galetti et al., 1995; Johnson et al., 1997). These areasalso contain cells with arm-movement related properties, and many areinfluenced by somatosensory information regarding limb position (Galletti,Fattori, Kutz et al., 1997). Of course, eye position information at the end of asaccade is likely to play a crucial role in the on-line modification of a handmovement towards a visual target (e.g. Fisk and Goodale, 1985). Taken together,these findings strongly suggest that the posterior parietal region of the primatebrain plays a role in coordinating eye-hand movements to suddenly appearingtargets, as well as inhibiting either the eye movement component (Snyder,Andersen and Brotchie, 1997) or the hand movement component (Ferraina et al.,1997).
Less is known about the precise anatomical organization of parietal lobe“extrafoveal” reaching centres in humans. Kawashima, Naitoh, Matsumura et al.(1996) conducted a positron emission tomography study of reaching tasks, underconditions where both eyes and hand were moved to the target or either eyesalone or hands alone were directed to the target. These authors conclude thattwo fields in the intraparietal sulcus are discernable; an anterior zone withmostly reach-related activation and a posterior zone with mostly saccade-relatedactivity.
In conclusion, the available evidence suggests that magnetic misreaching is asign of parietal lobe dysfunction. This sign was uncovered while our patient wasreceiving a series of detailed neuropsychological investigations. In this case, theabsence of aphasia, dementia, visual disorientation, gross sensorimotordisturbance and the like made the discovery of magnetic misreaching possible.The slow and specific nature of degeneration in Ms D.’s case caused theselective disruption of parietal networks, resulting in magnetic misreaching. In
Magnetic misreaching 649

other, less selective instances of parietal lobe damage (such as infarct of themiddle cerebral artery) several other related parietal networks will also becompromised, resulting in complete visuomotor/attentional disturbances such asHolmes-Balint syndrome. It is conceivable that if looked for carefully, magneticmisreaching will be detected in other patients with parietal lobe damage.
Acknowledgements. The authors would like to thank Dr. O. Turnbull for administrationand scoring of the frontal lobe tests, and Dr. C. Gray for his statistical advice. Prof. E. DeRenzi saw the patient with us and provided helpful advice. Mr. H. Atta conducted theopthamological examination. Dr. K. Scott-Brown measured the luminance of target andbackground used in the final experiment. Dr. F. Smith performed the MR scan and providedus with valuable neuroradiological advice. Dr. S. Jackson provided helpful comments on adraft of the manuscript. Finally, we are extremely grateful to Ms D. for her extraordinarypatience and endurance.
Some of these data were reported at the British Neuropsychological Society meeting inBirmingham, England (October 1996), and the 15th Annual European Workshop onCognitive Psychology in Bressanone, Italy (January 1997).
This research was supported by an equipment grant from the Research Committee,University of Aberdeen, to D.P. Carey and O.H. Turnbull.
REFERENCES
ANDERSEN, R.A., SNYDER, L.H., BRADLEY, D.C., and XING, J. Multimodal representation of space in theposterior parietal cortex and its use in planning movements. Annual Review of Neuroscience, 20:303-330, 1997.
AZOUVI, P., BERGEGO, C., ROBEL, L., MARLIER, N., DURAND, I., HELD, J.P., and BRUSSEL, B. Slowlyprogressive apraxia: Two case studies. Journal of Neurology, 240:347-350, 1993.
BENTON, A.L., and HAMSHER, K. DE S. Multilingual Aphasia Examination. Iowa City: University ofIowa, 1976.
BLACK, S.E. Focal cortical atrophy syndromes. Brain and Cognition, 31:188-229, 1996.BOGEN, J.E. The callosal syndromes. In K.M. Heilman and E. Valenstein (Eds.), Clinical
Neuropsychology(3rd edition). Oxford: Oxford University Press, 1993, ch. 11, pp. 337-408.BOUSSAOUD, D., DI PELLEGRINO, G., and WISE, S.P. Frontal-lobe mechanisms subserving vision-for-
action versus vision-for-perception. Behavioural Brain Research, 72:1-15, 1995.BRAZZELLI, M., COLOMBO, N., DELLA SALA , S., and SPINNLER, H. Spared and impaired cognitive abilities
after bilateral frontal damage. Cortex, 30:27-51, 1994.BROTCHIE, P.R., ANDERSEN, R.A., SNYDER, L.H., and GOODMAN, S.J. Head position signals used by
parietal neurons to encode locations of visual stimuli. Nature, 375:232-235, 1995.BRION, S., and JEDYNAK, C.-P. Troubles du transfert interhemispherique (callosal disconnection). A
propos de trois observations de tumeurs du corps calleux. Le signe de la main étrangère. RevueNeurologique, 126:257-266, 1972.
DELLA SALA , S., MARCHETTI, C., and SPINNLER, H. The anarchic hand: A fronto-mesial sign. In F. Bollerand J. Grafman (Eds.), Handbook of Neuropsychology, vol 9. Amsterdam: Elsevier, 1994, pp. 233-255.
DENNY-BROWN, D. Positive and negative aspects of cerebral cortical functions. North Carolina MedicalJournal, 17:295-303, 1956.
DENNY-BROWN, D. The nature of apraxia. The Journal of Nervous and Mental Disease, 126:9-32, 1958.DE RENZI, E. Slowly progressive apraxia and agnosia. Cortex, 22:171-180, 1986.DE RENZI, E., and BARBIERI, C. The incidence of the grasp reflex following hemispheric lesion and its
relation to frontal damage. Brain, 115:293-313, 1992.DE RENZI, E., CAVALLERI , F., and FACCHINI, S. Imitation and utilization behaviour. Journal of Neurology,
Neurosurgery and Psychiatry, 61:396-400, 1996.DE RENZI, E., and FAGLIONI, P. Normative data and screening power of a shortened version of the Token
Test. Cortex, 14:41-49, 1978.DE RENZI, E., MOTTI, F., and NICHELLI , P. Imitating gestures: A quantitative approach to ideomotor
apraxia. Archives of Neurology, 37:6-18, 1980.DICK, J.P.R., SNOWDEN, J., NORTHEN, B., GOULDING, P.J., and NEARY, D. Slowly progressive apraxia.
Behavioural Neurology, 2:101-104, 1989.FERRAINA, S., JOHNSON, P.B., GARASTO, M.R., BATTAGLIA -MAYER, A., ERCOLANI, L., BIANCHI , L.,
LACQUANITI, F., and CAMINITI , R. Combination of hand and gaze signals during reaching: Activity
650 David P. Carey and Others

in parietal area 7m of the monkey. Journal of Neurophysiology, 77:1034-1038, 1997.FISK, J.D., and GOODALE, M.A. The organization of eye and limb movements during unrestricted
reaching to targets in contralateral and ipsilateral space. Experimental Brain Research, 60:159-178,1985.
FOLSTEIN, M.F., FOLSTEIN, S.E., and MCHUGH, P.R. “Mini Mental State”: A practical method for gradingthe cognitive state of patient for the clinician. Journal of Psychiatric Research, 12:189-198, 1975.
GALLETTI , C., BATTAGLINI , P.P., and FATTORI, P. Eye position influence on the parieto-occipital area PO(V6) of the macaque monkey. European Journal of Neuroscience, 7:2486-2501, 1995.
GALLETTI , C., FATTORI, P., KUTZ, D.F., and BATTAGLINI , P.P. Arm movement-related neurons in thevisual area V6A of the Macaque superior parietal lobule. European Journal of Neuroscience, 9:410-413, 1997.
GIBB, W.R.G., LUTHERT, P.J., and MARSDEN, C.D. Corticobasal degeneration. Brain, 112:1171-1192,1989.
GOLDBERG, G. Supplementary motor area structure and function. Behavioural and Brain Sciences, 8:567-616, 1985.
GOLDSTEIN, K. Zur Lehre von der motorisschen Apraxie. Zeitschrift für Phychologie und Neurologie, 11:168-187, 1908.
GOODGLASS, H., and KAPLAN, E. The Boston Diagnostic Aphasia Examination. Boston: Lea and Febiger,1983.
GUITTON, D., BUCHTEL, H.A., and DOUGLAS, R.M. Frontal lobe lesions in man cause difficulties insuppressing reflexive glances and in generating goal-directed saccades. Experimental BrainResearch, 58:455-472, 1985.
JACOBS, D.H., ADAIR, J.C., and HEILMAN , K.M. Visual grasp in corticobasal degeneration. Annals ofNeurology, 36:679, 1994.
JEANNEROD, M. The Neural and Behavioural Organization of Goal-Directed Movements. Oxford:Clarendon Press, 1988.
JEANNEROD, M. The Cognitive Neuroscience of Action. Oxford: Blackwell Publishers Ltd., 1997.JOHNSON, P.B., FERRAINA, S., GARASTO, M.R., BATTAGLIA -MAYER, A., ERCOLANI, L., BURNOD, Y., and
CAMINITI , R. From vision to movement: Cortico-cortical connections and combinatorial properties ofreaching-related neurons in parietal areas V6 and V6a. In P. Thier and H.-O. Karnath (Eds.),Parietal Lobe Contributions to Orientation in 3D Space. Heidelberg: Springer-Verlag, 1997, pp.221-236.
KAWASHIMA , R., NAITOH, E., MATSUMURA, M., ITOH, H., ONO, S., SATOH, K., GOTOH, R., KOYAMA , M.,INOUE, K., YOSHIOKA, S., and FUKADA , H. Topographic representation in human intraparietal sulcusof reaching and saccade. Neuroreport, 7:1253-1256, 1996.
LHERMITTE, F. ‘Utilization behaviour’ and its relation to lesions of the frontal lobes. Brain, 106:237-255, 1983.
LHERMITTE, F., PILLON, B., and SERDARU, M. Human autonomy and the frontal lobes. I. Imitation andutilization behaviour: A neuropsychological study of 75 patients. Annals of Neurology, 19:326-334,1986.
LEVINE, D.N., KAUFMAN, K.J., and MOHR, J.P. Inaccurate reaching associated with a superior parietallobe tumor. Neurology, 28:556-561, 1978.
LYNCH, J.C. The functional organization of posterior parietal association cortex. Behavioral and BrainSciences, 3:485-534, 1980.
MASSMAN, P.J., KREITER, K.T., JANKOVIC, J., and DOODY, R.S. Neuropsychological functioning incortical-basal ganglionic degeneration: Differentiation from Alzheimer’s disease. Neurology, 46:720-726, 1996.
MOUNTCASTLE, V.B., LYNCH, J.C., GEORGOPOULOS, A., SAKATA , H., and ACUNA, C. Posterior parietalcortex of the monkey: Command functions for operation within extrapersonal space. Journal ofNeurophysiology, 38:871-908, 1975.
NELSON, H.E. A modified card sorting test sensitive to frontal lobe defects. Cortex, 12:312-324, 1976.PAUSE, M., KUNESCH, E., BINKOFSKI, F., and FREUND, H.-J. Sensorimotor disturbances in patients with
lesions of the parietal cortex. Brain, 112:1599-1625, 1989.PERENIN, M.-T. Optic ataxia and unilateral neglect: Clinical evidence for dissociable spatial functions in
posterior parietal cortex. In P. Thier and H.-O. Karnath (Eds), Parietal Lobe Contributions toOrientation in 3D Space. Heidelberg: Springer-Verlag, 1997, pp. 289-308.
PIERROT-DESEILLIGNY, C., RIVAUD , S., GAYMARD , B., and AGID, Y. Cortical control of reflexive visually-guided saccades in man. Brain, 114:1473-1485, 1991.
PILLON, P., BLIN, J., VIDAILHET , M., DEWEER, B., SIRIGU, A., DUBOIS, B., and AGID, Y. Theneuropsychological pattern of corticobasal degeneration: Comparison with progressive supranuclearpalsy and Alzheimers-disease. Neurology, 45:1477-1483, 1995.
RATCLIFF, G., and DAVIES-JONES, G.A.B. Defective visual localization in focal brain wounds. Brain, 95:1972.
RINNIE, J.O., LEE, M.S., THOMPSON, P.D., and MARSDEN, C.D. Corticobasal degeneration: A study of 36
Magnetic misreaching 651

cases. Brain, 114:1183-1196, 1994.RIZZO, M., and DARLING, W. Reaching with cerebral tunnel vision. Neuropsychologia, 35:53-63, 1997.RIZZO, M., ROTELLA, D., and DARLING, W. Troubled reaching after right occipito-temporal damage.
Neuropsychologia, 30:711-722.RONDOT, P., DE RECONDO, J., and RIBADEAU DUMAS, J.L. Visuomotor ataxia. Brain, 100:355-376, 1977.SAWLE, V., BROOKS, D.J., MARSDEN, C.D., and FRACKOWIAK, R.S.J. Corticobasal degeneration: A unique
pattern of regional cortical oxygen hypometabolism and striatl flurodopa uptake demonstrated bypositron emission tomography. Brain, 114:541-556, 1991.
SHALLICE, T., BURGESS, W.P., SCHON, F., and BAXTER, M.D. The origin of utilization behaviour. Brain,112: 1587-1598, 1989.
SHALLICE, T., and EVANS, M.E. The involvement of the frontal lobes in cognitive estimation. Cortex, 14:294-303, 1978.
SIEGAL, S., and CASTELLANI, N.J. Nonparametric Statistics for the Behavioral Sciences. New York:McGraw-Hill, 1988.
SNYDER, L.H., BATISTA, A.P., and ANDERSEN, R.A. Coding of intention in the posterior parietal cortex.Nature, 386:167-170.
VIDAILHET , M., RIVAUD , S., GOUIDER-KHOUJA, N., PILLON, B., BONNET, A.M., GAYMARD , B., AGID, Y.,and PIERROT-DESEILLIGNY, C. Eye movements in Parkinsonian syndromes. Annals of Neurology, 35:420-426, 1994.
WARRINGTON, E.K., and JAMES, M. The Visual Object and Space Perception Battery. London: TheThames Valley Test Company, 1991.
WISE, S.P., DI PELLEGRINO, G., and BOUSSAOUD, D. The premotor cortex and nonstandard sensorimotormapping. Canadian Journal of Physiology and Pharmacology, 74:469-482, 1996.
Dr. David Carey, Neuropsychology Research Group, Department of Psychology, University of Aberdeen, Old Aberdeen, Scotland,AB24 2UB.E-mail: [email protected]
(Received 7 July 1997; accepted 14 July 1997)
NOTE
L.J. Buxbaum and H.B. Coslett (Subtypes of optic ataxia: reframing the disconnectionaccount. Neurocase, 3: 159-166, 1997) observed a patient (D.P.) who reached towards theexaminer’s nose while trying to point to an object in his visual periphery. Although detaileddescription of the conditions in which this behaviour was (and was not) observed were notprovided, D.P. may have displayed magnetic misreaching. The potential presence ofmagnetic misreaching in another patient supports our contention that the sign may be foundin other cases of parietal lobe dysfunction.
652 David P. Carey and Others