Embed Size (px)
Citation preview

Clinical Endocrinology (1989, 22, 807-8 15
MAGNESIUM ADMINISTRATION REVERSES THE HYPOCALCAEMIA SECONDARY TO HYPOMAGNESAEMIA
DESPITE LOW CIRCULATING LEVELS OF
VITAMIN D 25-HYDROXYVITAMIN D AND 1,25-DIHYDROXY
M . FUSS, E. COGAN, C. GILLET. R . KARMALI, J . GEURTS, A. BERGANS, H . BRAUMAN, R . BOUILLON A N D J . CORVILAIN
Seriiices de Mt!decine Interne et de Biologie Clinique, H6pitul Uniuersitaire Brugniunn, UniuersitP Libre de Bruxelles, Brussels, Belgium, and Luborutoriurn i’oor E.xperiinentele
Geneeskunde, Kutholieke Uniuersiteit Leuven, Rega Instituut, Leuveii, Belgium
( Receitred 15 October 1984; returneclfor revision I 9 November 1984;JinalIj~ revised 15 Janimrji 1985; accepted 25 January 1985)
SUMMARY The effect of parenteral administration of magnesium was studied in five patients with hypomagnesaemic hypocalcaemia. The initial metabolic state was characterized by a normal level of serum immunoreactive parathyroid hormone (iPTH), and by low or undetectable serum 25-hydroxyvitamin D (250HD) and 1,25-dihydroxyvitamin D (1,25 (OH)2D). A parathyroid response was elicited by the acute intravenous injection of magnesium chloride. In contrast, 1,25(OH)lD did not change up to 24 h after the injection. Intramuscular magnesium sulphate restored serum magnesium and calcium to normal, whereas iPTH was transiently increased. 250HD remained low and unchanged. 1,25(OH)2D rose very slowly, but the correction of hypocalcemia began before any change in 1,25(OH)zD levels could be demonstrated. Thus, the early correction of hypocalcemia mainly depended on the restoration of an adequate parathyroid function independently of the secretion of 1,25(OH)*D.
The pathogenesis of the hypocalcaemia due to severe hypomagnesaemia (Heaton & Fourman, 1965; Shils, 1969) is not yet fully understood. The release of parathyroid hormone (PTH) is impaired in this condition (Anast et al., 1972; Medalle & Waterhouse, 1973; Suh et al., 1973; Chase & Slatopolsky, 1974; Bar et al., 1975; Anast et al., 1976; Rude et al., 1978; Ralston et al., 1983) and restored by the administration of magnesium (Chase & Slatopolsky, 1974; Anast et al., 1976; Rude et al., 1978; Ralston et al., 1983). Whether there is a refractoriness of the target end-organs to PTH (Estep et al., 1969; Connor et al., 1972; Rude et al., 1978; Muldowney et al., 1979), especially bone, remains controversial (Suh et al., 1973; Chase & Slatopolsky, 1974; Anast et al., 1976). Impaired release of PTH
Correspondence: Dr M. Fuss, Service de Medecine Interne, Hapita1 Universitaire Brugmann, Place Van Gehuchten 4, 1020 Bruxelles, Belgium.
807

808 M . Fuss et al.
and refractoriness of the renal 1 alpha, 25 hydroxylase system to PTH, if present, would presumably not allow adequate synthesis of 1,25-dihydroxyvitamin D (1,25(OH)2D). This, however, has not been demonstrated, nor is i t known whether 1,25(OH)2D contributes to the correction of hypocalcaemia following magnesium administration. To answer these questions we investigated the effect of magnesium supplementation in five patients with this condition.
MATERIAL A N D METHODS Patients
As shown in Table I , five patients presented with hypomagnesaemic hypocalcaemia, due to severe chronic alcoholism or to intestinal malabsorption. None of them had clinical or radiological evidence of bone disease.
Protocol of study
All patients gave informed consent to be investigated before, during and after the administration of magnesium. They were on a normal hospital diet. Serial measurements were made to study the effect of magnesium on blood calcium, phosphate, immunoreac- tive parathyroid hormone (iPTH), 25-hydroxyvitamin D (250HD), 1,25(OH)>D. vitamin D binding protein (DBP) and on fasting urinary cyclic AMP (CAMP), hydroxyproline and maximum tubular reabsorptive capacity for phosphate (TmP04/GFR). The acute effect of an intravenous infusion of magnesium chloride (2.6 mEq of magnesium/kg of body wt in 30 sec) was estimated in the first four cases. The effect of intramuscular injections of magnesium sulphate (5.1 mEq of magnesium/kg a day) over a period extending from 5 to 20 d was studied in all cases.
Analrtical procedures
Serial measurements of iPTH, 1,25(OH)?D and DBP in each patient were made in the same assays to avoid interassay variations. 1,25(OH)zD (limit of detection: 5 pg/ml of serum) was measured by the method of Bouillon et ul. (1980). 250HD (limit of detection : 2 ng/ml) was determined following Belsey et al. (1974). DBP was measured by radial immunodiffusion (Bouillon et al., 1977). Immunoreactive PTH was measured with the mainly N-terminal specific (Bouillon et al., 1975) 21 1/32 antiserum (Wellcome Ltd UK). Urinary CAMP was determined by the method of Tovey et al. (1974) and urinary hydroxyproline by the technique of Delfosse et al. (1975). Magnesium was measured by atomic absorption spectrophotometry and creatinine (Cr), calcium and phosphate by standard methods using a Techicon Auto Analyzer. TmP04/GFR was calculated by the method of Walton & Bijvoet (1975) using phosphate and creatinine levels from fasting serum and urine. Statistical comparisons were made using the paired Student’s t-test.
RESULTS Biochemical data before magnesium administration
Initial blood and urine data are given in Table 1. Serum creatinine was normal in all but one patient. Serum calcium and magnesium were low. Serum albumin was normal in three patients and low in Patients 1 and 3.

s h T
able
1. B
lood
and
urin
e da
ta in
five
pat
ient
s pr
esen
ting
with
hyp
omag
nese
mia
5
Seru
m
Plas
ma
Fast
ing
urin
e S
' b
Age
(yea
rs)
3 Se
x Pa
tient
D
iagn
osis
1 60
F
2 36
F
3 56
M
4 51
M
5 85
F
Mal
abso
rptio
n
Alc
ohol
ism
Alc
ohol
ism
Alc
ohol
ism
Mal
abso
rptio
n
Cr
Ca
(mm
ol/l)
(m
mol
/l)
80
1.10
142
1.83
80
2.20
80
1.78
71
1.98
0.65
0.
37
<2
19
0.52
0.
53
7 <
5
1.03
0.
45
<2
16
1.07
0.
37
7 1
5
- D
BP
iPT
H
Ca/
Cr
cAM
P/G
FR
Tm
P04/
GFR
z a 0
3
(pgi
ml)
(p
g/m
l)
(mm
ol/p
mol
) (n
mol
idl)
(m
mol
/l)
b E
239
620
0.12
7 -
0.52
s. c
0.80
B 3
-
-
-
8 e
-
330
0.04
0 4.
1 0.
45
3 64
620
0.11
6 4.
4
358
630
0.02
0 3.
8 1.
23
3 36
9 42
0
s g.
SE
18
0.18
0.
13
0.04
1.
2 2.
9 31
62
0.
028
0.2
0.19
.t"
M
ean
91
1.78
0.
76
0.39
4.
0 12
.0
333
524
0.07
6 4.
1 0.
75
N
53-1
06
2.25
-2.6
3 0.
80-1
.45
0.7+
1.00
12
-30
2G70
22
0460
30
G62
0 0.
0284
339
1.3-
3.6
06-1
.45
2 n 0 2
Cr,
crea
tinin
e; C
a, ca
lciu
m; P
, pho
spha
te;
Mg,
mag
nesi
um; 2
50H
D, 2
5-hy
drox
yvita
min
D;
1,25
-(O
H)z
D,1
,25
dihy
drox
yvita
min
D; D
BP,
vita
min
D b
indi
ng
prot
ein;
IPT
H,
amin
o-te
rmin
al im
mun
orea
ctiv
e pa
rath
yroi
d ho
rmon
e; C
AM
P. c
yclic
AM
P; T
mP0
4/G
FR:
max
imum
of
tubu
lar
reab
sorp
tive
capa
city
for
5
phos
phat
e.
5.

810 M . Fuss et al.
Plasma 250HD and 1,25(OH)zD were low or undetectable, DBP was normal in the four patients in whom it was measured.
Serum iPTH level was inappropriately low (524 f 62 SEM pg/ml) considering the low serum calcium in all cases. Indeed, in a different group of nine vitamin D-deficient patients (250HD: 3.1 t 0.5 ng/ml) with a comparable degree of hypocalcaemia (Ca : 2.0 f 0.08 mmol/l) and a serum magnesium higher than 0.65 mmol/l (0.8 1 k 0.04 mmol/l) serum iPTH was higher (1 537 k 192 pg/ml).
Fasting urinary CAMP, when measured, was slightly elevated. The calculated TmP04/GFR was low in two out of four patients.
No correlation could be found between the values of iPTH and cAMP or TMPOd/GFR, between 1,25(0H)zD and 250HD levels nor between 1.25(OH)2D and the indices of parathyroid function.
Acute effect of niagnesiutn adtninistration
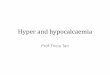
A 30 sec intravenous injection of magnesium chloride induced an increase of serum magnesium to about 1.70 mmol/l and, as shown in Fig. 1, was followed by: (1) a sharp and marked increase of plasma iPTH in two out of four patients, (2) an increase of urinary cAMP in three patients, including the two cases in which iPTH remained unchanged, (3) an increase of the fractional excretion of phosphate in the two patients in which it was measured. (4) no change in serum calcium or phosphate.
1
1 2500b \
c - E 2000
I500
-. 01 a - E 4 CJ 1000
L
20 t-
(rnin) Time
Fig. I . Effect of a 30 sec i .v . magnesium chloride injection (arrows) on plasma parathyroid hormone (iPTH), 1.25-dihydroxyvitarnin D ( 1,25(OH)zD). fractional excretion of phosphate (FEP) and urinary cyclic A M P (CAMP) in four patients with hypornagnaesemic hypocalcaemia. Hatched areas represent normal ranges.

s. T
able
2. B
lood
and
urin
e da
ta b
efor
e, d
urin
g an
d af
ter
mag
nesi
um r
eple
tion
b
3 2
Fast
ing
urin
e a a-
Ca
P 25
0HD
1,
25-(
0H)~
D
DB
P iP
TH
cA
MP/
GFR
0 2
Seru
m
Plas
ma
Mg
(mm
ol/l)
(m
mol
/l)
(mm
ol/l)
(n
g/m
l) (P
sim
u Pg
iml)
(pg/
mU
(n
mol
/dl)
5
Patie
nt
I II
**
III*
I
I1
I11
I 11
* I1
1 I
I1
I11
I 11
* 11
1 I
I1
I11
I I1
11
1 I
I1
I11
S'
1 0.
21
0.70
0.
70
1.1
2.1
2.3
0.48
0.
58
0.71
<
2
12
12
15
24
50
- - -
405
750
440
4.1
7.0
4.2
3
5 0.
37
0.82
0.
53
2.0
2.3
2.2
1.16
1.
32
1.29
7
7 9
15
17
18
36
9 29
6 34
6 42
0 67
5 64
0 -
5.6 -
2 8 3. k
SE
0.
04
0.08
0.
04
0.2
0.1
0.1
0.16
0.
19
0.16
1.
2 1.
0 1.
4 2.
9 1.
4 6.
5 31
37
25
48
83
61
0.
2 0.
7 0.
4 c,
2 0.
37
1.07
0.
70
1.8
2.3
2.2
0.97
1.
42
1.03
<
2
<2
<
2
19
22
35
239
280
302
620
1100
57
0 -
~ ~
3 0.
53
1.15
0.
74
2.2
2.4
2.5
0.52
1.
42
1.65
7
6 6
<5
18
35
364
399
387
605
810
800
4.4
3.9
3.4
4 0.
45
0.74
0.
66
2.0
2.5
2.5
1.10
1.
61
1.55
<
2
3 <
2
16
18
14
358 - -
600
630
525
3.8
4.2
3.0
$ M
ean
0.39
0.
90
0.66
1.
8 2.
3 2.
3 0.
85
1.27
1.
25
4.0
4.0
4.2
12.0
19
.8
30.0
33
3 32
5 34
5 53
0 79
3 59
5 4.
1 5.
2 3.
5
Abb
revi
atio
ns a
nd n
orm
al v
alue
s, s
ee T
able
1. D
ata
are
mea
n of
the
val
ues
befo
re M
g ad
min
istr
atio
n (I
). hi
ghes
t val
ues
obta
ined
dur
ing
Mg
adm
inis
trat
ion
(11)
. and
mea
n of
the
valu
es fo
llow
ing
Mg
disc
ontin
uatio
n (1
11).
2 r;- 8 2 s
Stat
istic
al s
igni
fican
ce co
mpa
ring
per
iods
I1 to
I, o
r 11
1 to
11:
*P<O
.O5;
**P< 0.
005.

812 M . Fuss et al.
n
c
F T 600
200 2 a‘, n .-p
0 5 10 15 20 Time (days)
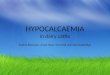
Fig 2 Time-course of the effects of magnesium administration (arrow) over 20 days in patient Number I ( 0 ) Plasma iPTH. (0) I,ZS(OH)2D
The increase of iPTH and/or of CAMP was not followed by an increase of plasma 1,25(OH)2D in any case, during the next 15 and 120 min or in the next 24 h.
Chronic eflect of magnesium administration
The effect of intramuscular magnesium sulphate over at least 5 d was evaluated in each patient. Data reported in Table 2 correspond to the mean of the values in the days before magnesium therapy (I), to the highest values obtained during magnesium administration (11) and to the mean of the values in the 7 d following magnesium discontinuation (III), respectively.
Serum magnesium and calcium increased under therapy virtually to normal values in all patients and remained normal or decreased slightly after discontinuation of the treatment. No significant variation of serum albumin could explain the increase of serum

Vitamin D metabolites in hjyomagnesaemic Iiypocalcaernia 813
50 r
. . I I I I I I
0.1 0.2 0.3 0.4 0.5 0.6 Urinary Ca/Creat
(rnrnol /,urnol)
Fig. 3. Relationship between urinary hydroxyproline and calciumicreatinine ratios in patient Number 1,days 1 to 1O.y=14Ox+25;R=0~94; P<O.OI.
calcium. Serum phosphate increased and plasma iPTH became supranormal in all cases. The already elevated urinary CAMP excretion further increased in two of three cases.
The low plasma 250HD remained unchanged during the whole period of the study. Circulating 1,25(OH)*D levels rose slowly under magnesium therapy and remained low. After withdrawal of magnesium supplementation, 1,25(OH)2D showed an additional increase within the normal range in three patients. Plasma DBP measured in three patients showed no significant change.
The time course of the modifications induced by magnesium administration in the first patient is shown in Fig. 2. The urinary hydroxyproline, repeatedly measured in this patient, was well correlated with the urinary calcium during the initial correction of hypocalcemia (Fig. 3).
DISCUSSION
As in previous reports (Anast et al., 1972; Suh et al., 1973; Medalle & Waterhouse, 1973; Chase & Slatopolsky, 1974; Bar et al., 1975; Anast et al., 1976; Rude et al., 1978; Ralston el al., 1983) the parathyroid response in our five hypomagnesaemic patients was inappropriate to the low serum calcium.
The low or undetectable levels of serum 250HD were presumably due to a vitamin D-deficient supply and/or to intestinal malabsorption, but not to a low circulating DBP level.
The low circulating 1,25(OH)*D levels in our patients are at variance with the normal level in a patient described by Ralston et al. (1983) and with the high level in a case reported by Jacob et al. (198 1). The concentration of 1,25(OH)2D measured in Ralston’s patient was probably influenced by the administration of pharmacological doses of

814 M . Fuss et al.
1 r-hydroxyvitamin D; Jacob's patient was recovering from acute renal failure and had received large doses of vitamin D and oestrogens.
The low circulating 1,25(OH)?D in our patients before magnesium supplementation was inappropriate for the circulating concentrations of calcium and phosphate. This could be related to a low substrate concentration. However. I ,25(OH)2D increased following magnesium supplementation without any detectable change in 250HD levels. Since the iPTH levels were only inappropriately low but not undetectable, it is possible that magnesium deficiency in itself depressed the renal 1 alpha, 25 hydroxylase activity. This mechanism seems likely since isolated kidney mitochondria need magnesium to convert tritiated 250HD to 1,25(OH)rD (Fraser & Kodicek, 1979). Tracer studies in hypomagnesemic patients are in agreement with our hypothesis :circulating labelled 1,25(OH)?D following the administration of labelled cholecalciferol was low compared with the levels measured in nutritionally matched controls (Stanbury & Mawer, 1978). Two cases of rickets associated with hypomagnesemia (Reddy & Sivakumar, 1974) did not respond to massive doses of vitamin D until magnesium supplements were administrated. It is possible that these cases illustrate inhibition of the 1 alpha, 25 hydroxylase system due to magnesium deficiency.
The acute administration of magnesium chloride was followed by a sharp increase in circulating iPTH and/or by an increase of urinary cyclic AMP excretion. No change of plasma 1,25(OH)lD was observed up to 24 h after the injection, whereas plasma 1,25(OH)?D increases within hours in normal men in response to the parenteral administration of parathyroid extracts (Eisman et al., 1979; Prince et al., 1983). Thus, if the parathyroid function was improved by the i.v. injection of magnesium, no response of the kidney cells in terms of 1,25(OH)?D release was observed.
Following chronic administration of magnesium, iPTH rapidly increased and hypocal- cemia was progressively reversed. Serum 1,25(OH)?D rose as in the patient of Ralston et al. (1983), but this rise was very slow. In fact, hypocalcemia was virtually corrected in most cases in spite of a low 1,25(OH)rD. That the correction of hypocalcemia mainly depended on the action of PTH on bone is supported by the parallelism between calcium and hydroxyproline in the urine of Patient 1 during the first ten days of treatment.
Our work shows that the hypocalcemia was associated with, and possibly worsened by low circulating levels of 1,25(OH)zD. All the abnormalities were converted following magnesium administration. The rise of 1.25(OH)zD. however, was delayed compared to that of calcium. The correction of hypocalcemia seemed mainly to be due to the restoration of adequate parathyroid function, independently of 1,25(OH)2D.
A C K N O W L E D G E M E N T S
This work was supported by the grant 3.4543.79 of the FRSM of Belgium. The authors acknowledge C. Steppe and I. Jans for valuable technical work, the nurses of the Endocrine Unit, and Mrs Soffers for drawing the figures.
R E F E R E N C E S
ANAST. C.S.. MOHS. J.M., KAPLAN, S.L. & BURNS. P.W. (1972) Evidence for parathyroid failure in magnesium
ANASJ. C.S.. WINNACKER, J., FORTE, L. & BURNS. T.W. (1976) Impaired release of parathyroid hormone in deficiency. Science, 177, 606-608.
magnesium deficiency. Journal of Clinical Endocrinology and Meraholisni. 42. 707-71 7.

Vitamin D metabolites in hypomagnesaemic hypocalcaenzia 815
BAR, R.A., WILSON, H.E. & MAZZAFERRI, E.L. (1975) Hypomagnesem~c hypocalcemia secondary to renal magnesium wasting. A possible consequence of high-dose gentamicin therapy. Annals of Internal M~dicine, 82,646-649.
BELSEY, R.E., DE LUCA, H.F., & POTTS, T.T. JR (1974) A rapid assay for 25-OH-vitamin D3 without preparative chromatography. Journal of Clinical Endocrinology and Meiaholism, 38, 104~&105 I .
BOUILLON, R., VERBERCKMOES. R. & DE MOOR, P. (1975) Influence of dialyate calcium concentration and vitamin D on serum parathyroid hormone during repetitive dialysis. Kidney Iniernutional, 7, 422432.
BOUILLON, R., VAN BAELEN, H . & DE MOOR, P. (1977) The measurement of the vitamin D binding protein in human serum. Journal of Clinical Endocrinology and Meiaholism, 45,225-231.
BOUILLON, R., DE MOOR, P., BAGGLIONI, E.G. & USKOKOVIC. M.R. (1980) A radioimmunoassay for 1,25-dihydroxycholecaIciferol. Clinical Chemisiry, 26, 562-567.
CHASE, L. & SLATOPOLSKY, E. (1974) Secretion and metabolic efficacy of parathyroid hormone in patients with severe hypomagnesemia. Journal of Clinical Endocrinology and Meiaholism, 38, 363-37 1.
CONNOR, T.B., TOSKES, P., MAHAFFEY, J., MARTIN, L.G., WILLIAMS, J.B. & WALSER, M. (1972) Parathyroid function during chronic magnesium deficiency. Johns Hopkins Medical Journal. 131, 100-1 17.
DELFOSSE, L., ORLOFF, S., RAO, V.H., SHOSBERG, E., & VERBRUGGEN. L. (1975) Automated analysis of hydroxyproline in urine. Indian Journal of Biochemistry and Biophyssics, 12, 28&282.
ESTEP, H., SHAW, W.A., WALTHINGTON, C., HOBE. R., HOLLAND, W. & TUCKER, S.G. (1969) Hypocalcemia due to hypornagnesemia and reversible parathyroid in responsiveness. Journal of Clincal Endocrinology and Metabolism, 29, 842-848.
EISMAN. J.A., WARK. J.D., PRINCE, R.L. & MOSELEY, J .M. (1979) Modulation ofplasma I ,25-dihydroxyvitamin D in man by stimulation and suppression tests. Lancet, ii, 931-933.
FRASER, D.R. & KODICEK, E. (1979) Unique biosynthesis by kidney of a biologically active vitamin D metabolite. Nature, 228, 764766.
HEATON, F.W. & FOURMAN, P. (1965) Magnesium deficiency and hypocalcemia in intestinal malabsorption. Lancet, ii, 5k-52.
JACOB. A.I., PENNELL, J.P., LAMBERT, P.N. & GAVELLAS, G. (1981) Vitamin D metabolites and parathyroid hormone in hypomagnesemic hypocalcemia. Mineral~lectrol.vie Metabolism, 6, 3 16322.
MEDALLE, R. & WATERHOUSE, C . (1973) A magnesium-deficient patient presenting with hypocalceniia and hyperphosphatemia. Anna1.r of Iniernal Medicine, 79, 76-79.
MULDOWNEY, F.P., MCKENNA. T.J., KYLE, L.H., FREANEY, R. &SWAN, M. (1979) Parathormone-like effect of magnesium replenishment in steatorrhea. New England Journal of Medicine, 281, 6 1-68.
PRINCE, R.L.. WARK. J.D., OSMOND, S., OPIE, J.M., EAGLE, M.R. & EISMAN, J.A. (1983) A test of 1,25-dihydroxyvitamin D-, secretory capacity in normal subjects for application in metabolic bone diseases. Clinical Endocrinology, 18, 127-133.
RALSTON, S., BOYLE, I.T., COWAN, R.A., CREAN. G.P., JENKINS. A. & THOMSON. W.S. (1983) PTH and vitamin D responses during treatment of hypomagnesaemic hypoparathyroidism. Acta Endocrinologica. 103,
REDDY, V. & SIVAKUMAR, B. (1974) Magnesium-dependent vitamin-D-resistant rickets. Lancet. i , 963-965. RZJDE, R.K., OLDHAM, S.B., SHARP, C.F. & SINGER, F.R. (1978) Parathyroid hormone secretion in magnesium
deficiency. Journal of Clinical Endocrinology and Metaholism, 41, 800-806. SHILS, M.E. (1969) Experimental human magnesium depletion. Medicine, 48, 61-85. STANBURY, S.W. & MAWER, E.B. (1978) Clinical aspects of vitamin D metabolism. Magnesium deficiency and
magnesium-dependent rickets. In Vitamin D (ed D.E.M. Lawson), pp 255-386. Academic Press, London. SUH, S.M., TASHJIAN, A., MATSUO, A,, PARKINSON, D. & FRASER, D. (1973) Pathogenesis of hypocalcernia in
primary hypomagnesemia: normal end-organ responsiveness to parathyroid hormone, impaired para- thyroid gland function. Journal of Clinical Inuesiigaiion, 52, 153-160.
TOVEY, K.C., OLDHAM, K.G., & WHELAN. S.A.M. (1974) A simple direct assay for cyclic AMP in plasma and other biological samples using an improved competitive protein binding technique. Clinicu Cl7imica Aria, 56,221-234.
WALTON, J.J., & BIJVOET, O.L.M. (1975) Nomogram for derivation of renal threshold phosphate concentration. Lunrei, ii, 309-3 10.
53 5-5 38.