Embed Size (px)
Citation preview
Lynn McIntyre, MD MHSc FRCPC1 and Catherine L. Mah, MD FRCPC PhD2
1 Professor and Associate Scientific Director, Institute for Public Health, University of Calgary, [email protected] Scientist, Centre for Addiction and Mental Health and Assistant Professor, Dalla Lana School of Public Health, University of Toronto, [email protected]
With thanks to Ryan Lukic, Krista Rondeau, Patrick Patterson, and Laura Anderson
Rapid simulation of a deliberative dialogue process: A food insecurity policy workshop
P U B L I C H E A LT H 2 0 1 4 – C P H A c o n f e r e n c e M a y 2 8
2
Why are you here today?
You are a citizen of a major municipality, CPHA Metro. You have been invited to participate in a citizens’ dialogue on income support policy options to address food insecurity.
Please bring a ‘whole life perspective’ to this discussion, including your persona’s expected professional and personal roles, knowledge, values, and beliefs.
Chatham House Rule: You are completely free to use any of the information from today in your work and future deliberation, but neither the identity nor the affiliation of the speaker/participant should be revealed.
3
Exploration of issue and policy options (15 min)Conflict identification (20 min)Action formulation (20 min)
Dialogue AgendaPart 1: Rapid deliberative dialogue simulation
4
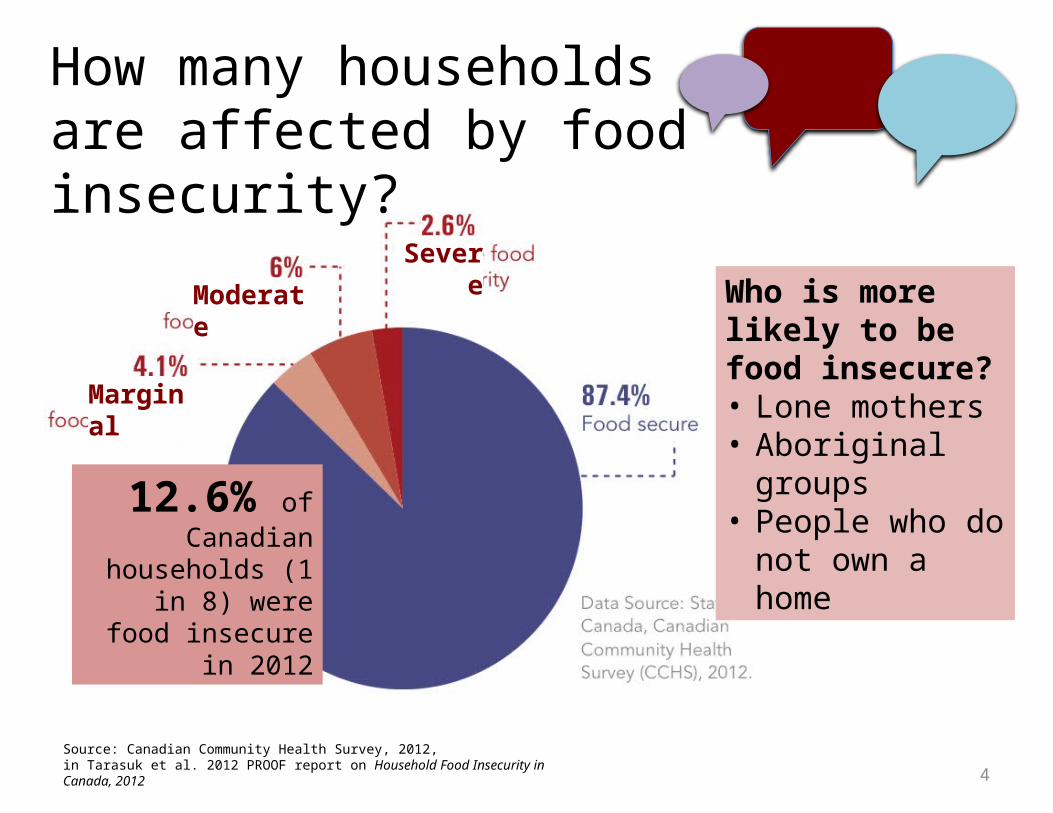
Marginal
Moderate
Severe
How many households are affected by food insecurity?
Source: Canadian Community Health Survey, 2012, in Tarasuk et al. 2012 PROOF report on Household Food Insecurity in Canada, 2012
Who is more likely to be food insecure?• Lone mothers• Aboriginal groups• People who do not
own a home12.6% of Canadian households
(1 in 8) were food insecure in 2012
5
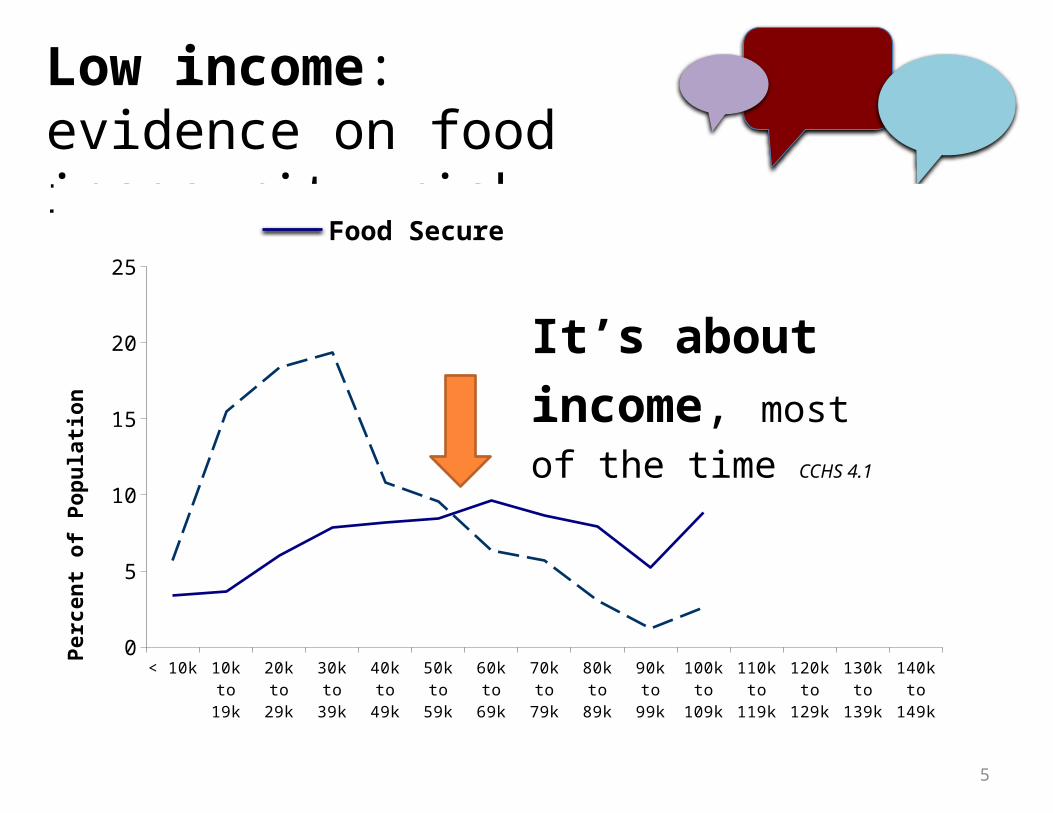
Low income: evidence on food insecurity risk
< 10k 10k to 19k
20k to 29k
30k to 39k
40k to 49k
50k to 59k
60k to 69k
70k to 79k
80k to 89k
90k to 99k
100k to
109k
110k to
119k
120k to
129k
130k to
139k
140k to
149k
0
5
10
15
20
25
Food SecureFood Insecure
Pe
rce
nt
of
Po
pu
lati
on
It’s about income, most of the time CCHS 4.1
6
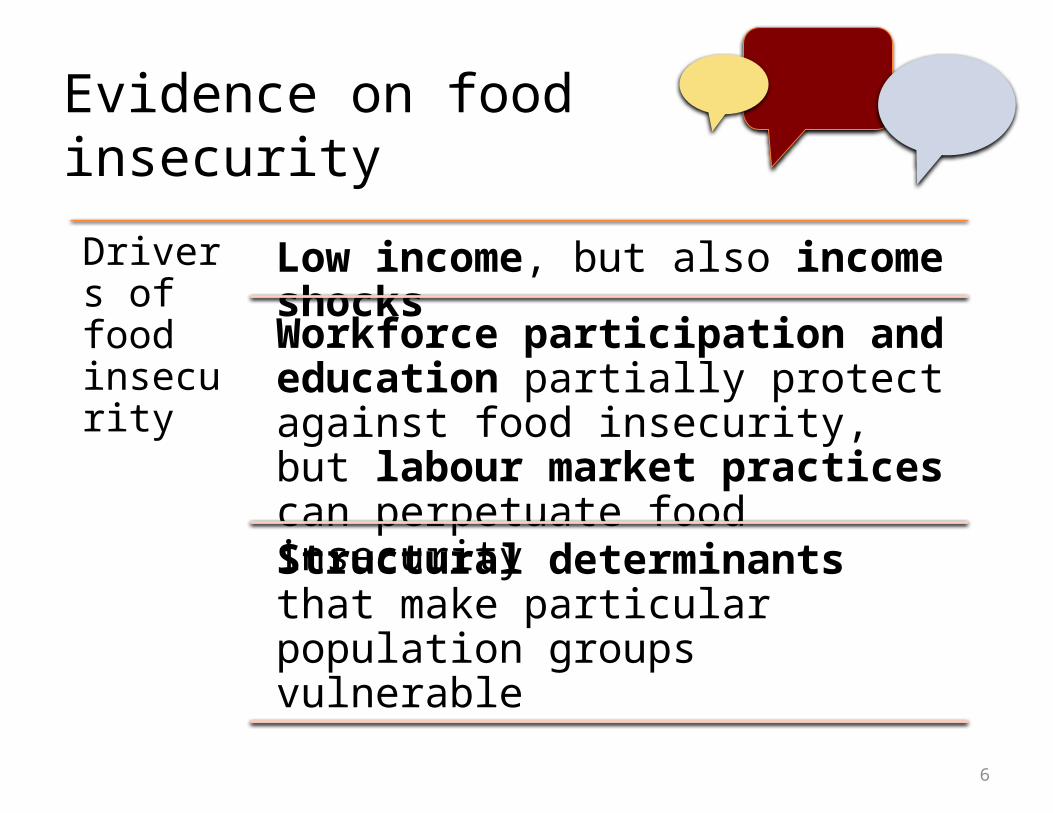
Evidence on food insecurity
Drivers of food insecurity
Low income, but also income shocks
Workforce participation and education partially protect against food insecurity, but labour market practices can perpetuate food insecurity
Structural determinants that make particular population groups vulnerable
7
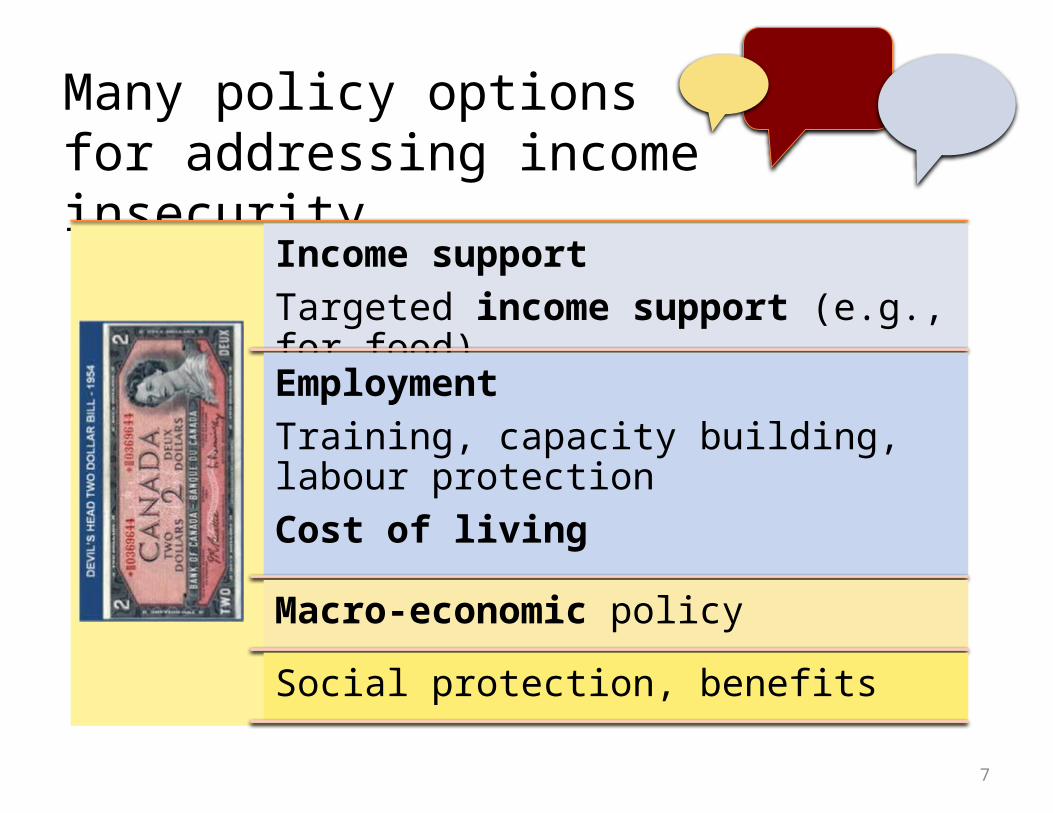
Many policy options for addressing income insecurity
Income supportTargeted income support (e.g., for food)
EmploymentTraining, capacity building, labour protectionCost of living
Macro-economic policy
Social protection, benefits
8
Evidence on income
Key example of this policy instrument: Guaranteed annual income for seniors through pension
Logic model:Addresses 1) income floor but also 2) budget shocks
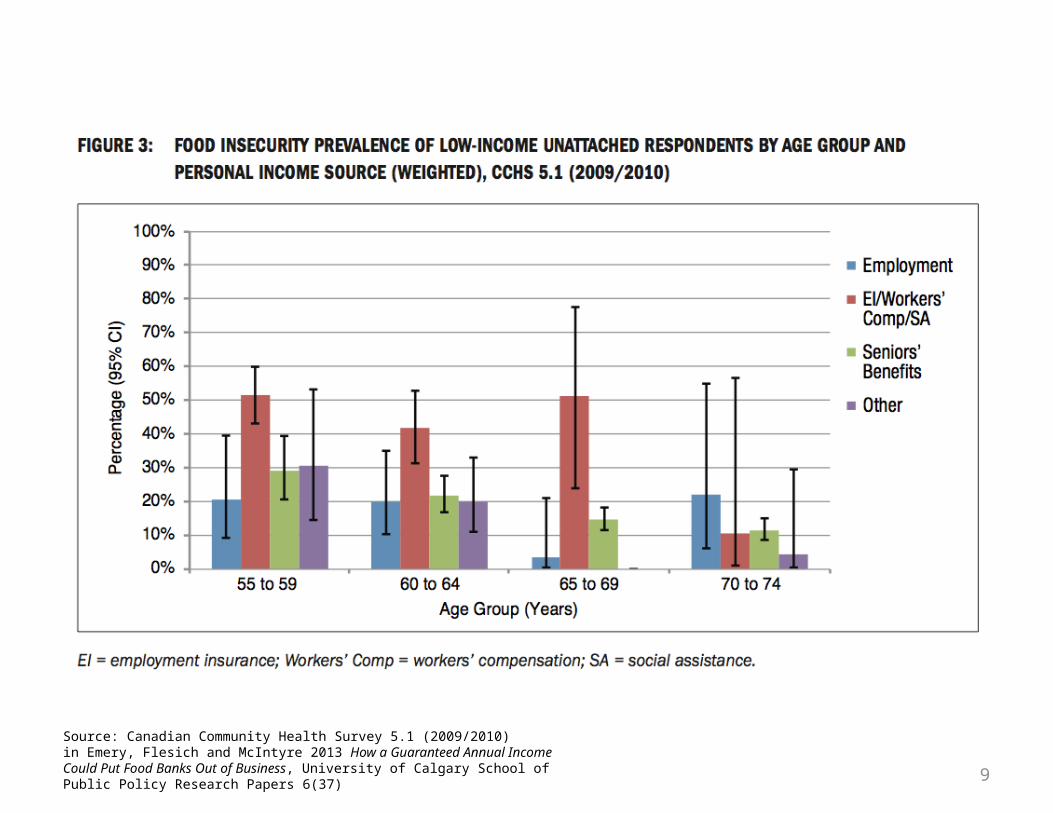
Evidence on effectiveness:Reduces food insecurity rates by more than half for age >65y
Implementation possibility:Universal guaranteed basic income (general tax revenues)
9
Source: Canadian Community Health Survey 5.1 (2009/2010) in Emery, Flesich and McIntyre 2013 How a Guaranteed Annual Income Could Put Food Banks Out of Business, University of Calgary School of Public Policy Research Papers 6(37)

10
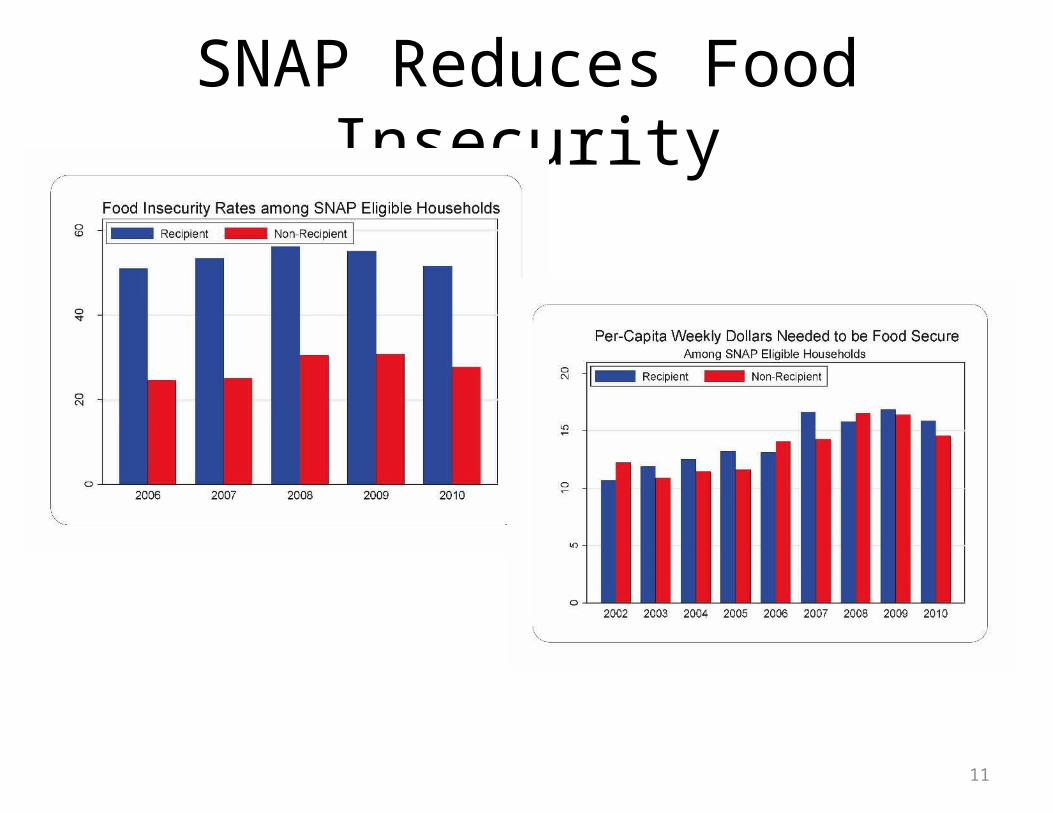
Evidence on income-for-food
Key example of this policy instrument: Supplemental nutrition assistance program (SNAP in US)
Logic model:Allows people to spend more on food relative to other goods than they would otherwise
Evidence on effectiveness:Reduces food insecurity (particularly households with children)
Implementation possibility:Targeted social assistance program (general tax revenues)
11
SNAP Reduces Food Insecurity
12
Deliberation part 1:Conflict identification
Which is the fairest approach, and why?
Guideline: your group does not need to come to a consensus, but you can if you wish
13
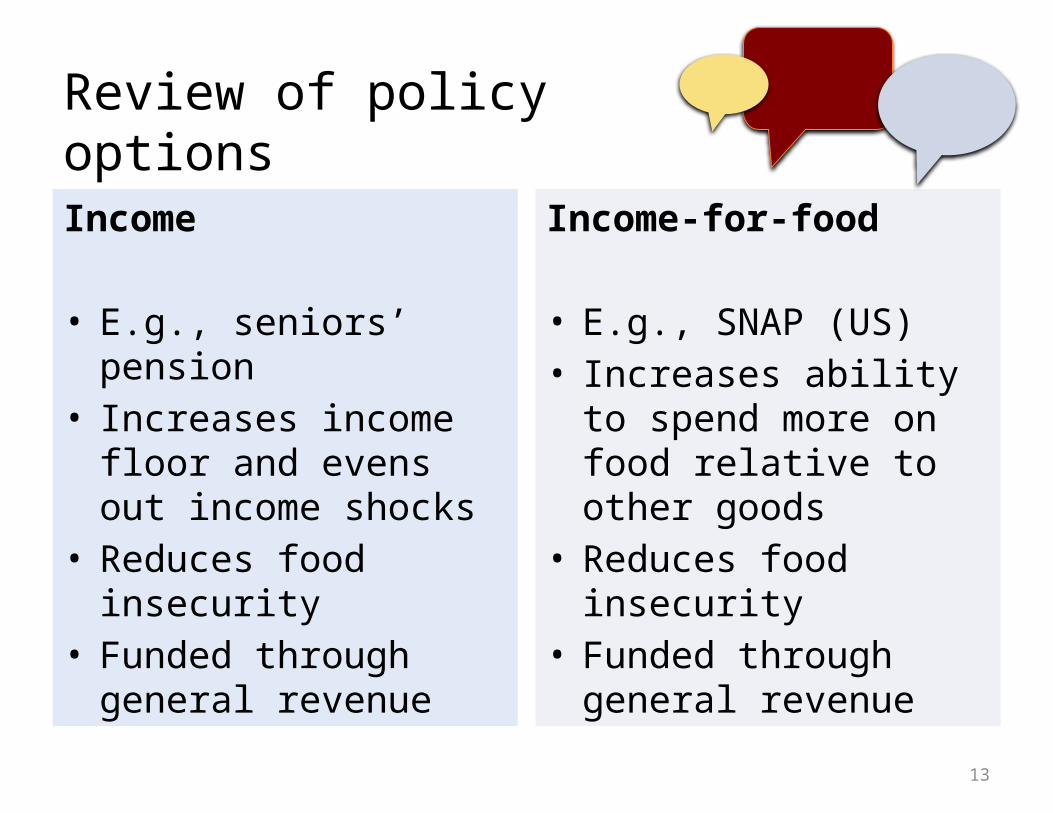
Income
• E.g., seniors’ pension• Increases income floor
and evens out income shocks
• Reduces food insecurity• Funded through general
revenue
Income-for-food
• E.g., SNAP (US)• Increases ability to
spend more on food relative to other goods
• Reduces food insecurity• Funded through general
revenue
Review of policy options
14
Deliberation part 2:Formulate action plan
Which policy option would you recommend and why?
Guideline: your group does not need to come to a consensus, but you can if you wish

15
Dialogue AgendaPart 2: Reflective evaluation; review of dialogue method and use in public health practice
Reflective evaluation of dialogue Report back and evaluation (15 min)Overview of deliberative dialogue methods and application to public health policy and practice (15
min)
Take home messages (5 min)

16
Reflective evaluation
1. How well did the dialogue process support discussion of a high-priority issue in order to inform action?
2. What features of the dialogue process worked best? What could be added or changed?
3. How did your role and background influence your participation?
Reflection
SUPPORT tools #14 (Lavis et al) http://www.health-policy-systems.com/supplements/7/s1

17
Review: Deliberativedialogue methods
Purpose: a transformative discussion
• A forum for transforming ideas, opinions, or action strategies though group deliberation
• For decision-makers: public engagement• For KTE: exchanging evidence on polarized issues• Representing public/community interests and values
Boyko et al. 2012; SUPPORT tools; Brown 2006; Davies and Burgess 2004

18
Review: Deliberativedialogue methods
Key elements:
• Appropriate venue/environment• Transparent process and rules of engagement• Timeliness of the issue
• Appropriate mix/representativeness of participation (different ways to achieve this)
• No ‘magic number’ of participants (often 8-15 for a citizens’ panel)
Boyko et al. 2012; SUPPORT tools; Brown 2006; Davies and Burgess 2004
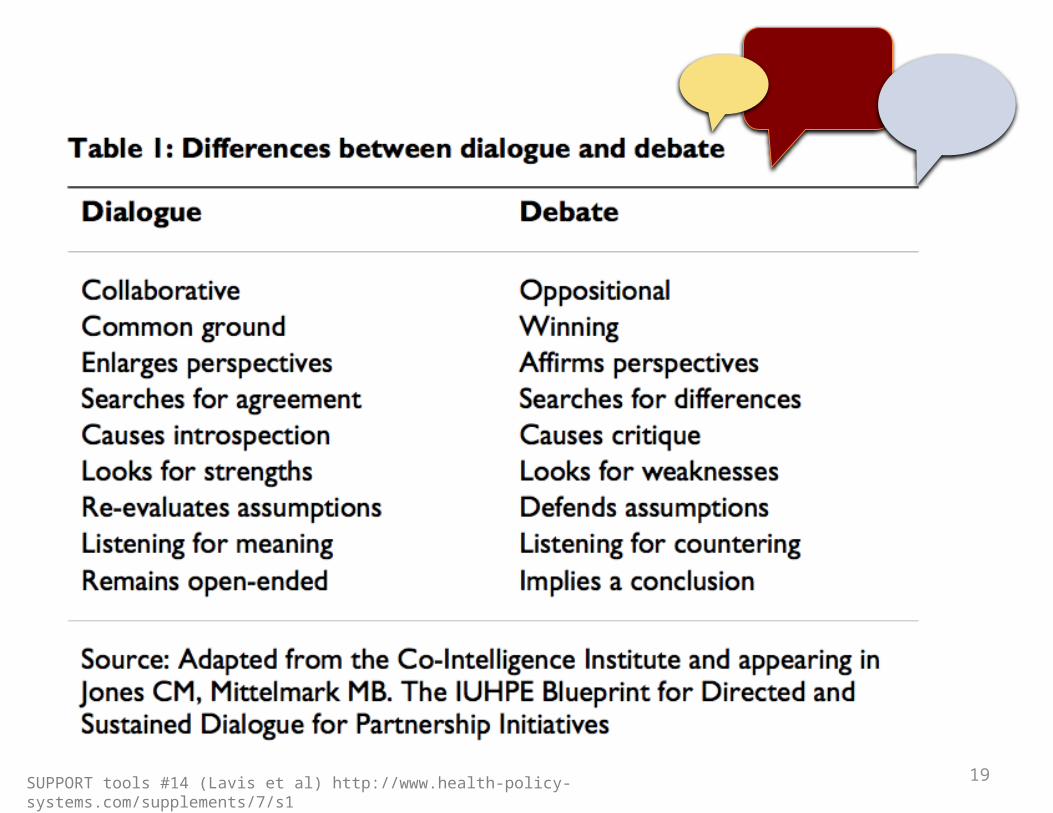
19SUPPORT tools #14 (Lavis et al) http://www.health-policy-systems.com/supplements/7/s1

20Health Canada 2000
Reflection
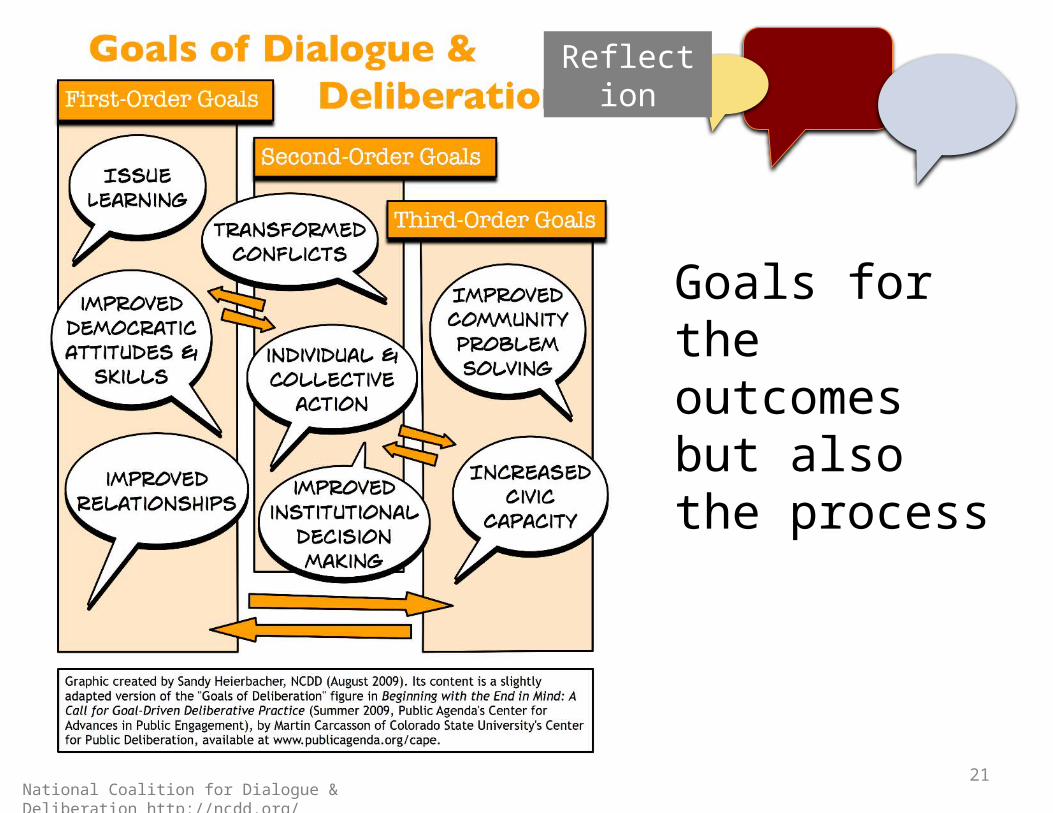
21
Reflection
National Coalition for Dialogue & Deliberation http://ncdd.org/
Goals for the outcomes but also the process
22
ReflectionAlso a part of reflective practice (civic professionalism)
23
Reflection
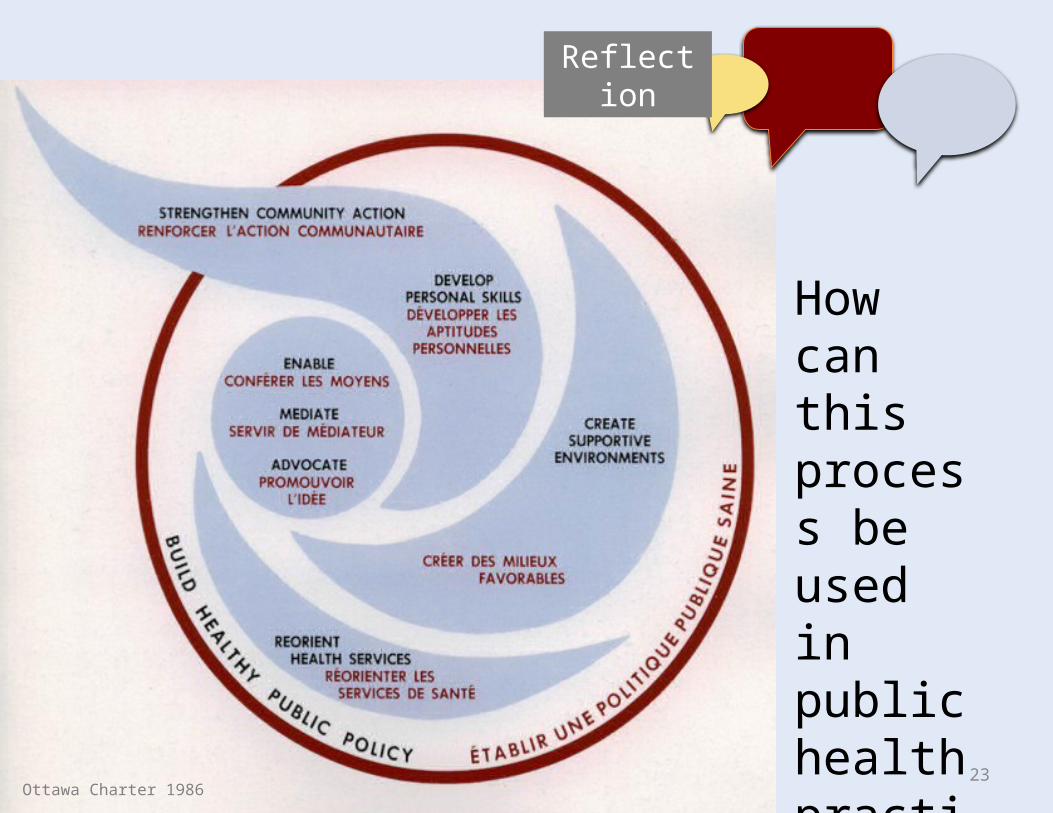
Ottawa Charter 1986
How can this process be used in public health practice?
24
Reviewing our objectives
Following this workshop, participants will be able to:
1. Identify key elements of a deliberative dialogue2. Formulate, with other citizens, a workable policy option
to act in a mutually acceptable way (but not necessarily consensus)
3. Describe at least two examples of public health practice scenarios in which deliberative dialogue methods could be applied
Reflection

25
Thank you!
PI: Valerie Tarasuk, Craig GundersenCo-Investigators: Lynn McIntyre, Catherine L. Mah, Herbert Emery, Jurgen Rehm, Paul Kurdyak