Embed Size (px)
Citation preview

Journal of Surgical Oncology 2009;99:260–264
REVIEW
Lymph Node Assessment: Issues in Pathology
MAHMOUD A. KHALIFA, MD, PhD, FRCPC1* AND ANDY SMITH, MD, FRCSC
2
1Department of Pathology, Sunnybrook Health Sciences Centre, Toronto, Ontario, Canada2Department of Surgical Oncology, Sunnybrook Health Sciences Centre, Toronto, Ontario, Canada
Metastasis to regional lymph nodes detected in cancer surgery specimens is a significant prognosticator and is also critical for subsequent planning
of therapeutic options. Consequently, the status of regional lymph nodes has become a mandatory element of the synotic reporting on cancer
resection specimens. Although pathologic reporting of lymph node metastasis is conceptually straightforward, several subtle processing and
reporting issues deserve discussion. This review addresses pathology specific issues with particular emphasis on non-breast, non-cutaneous
cancers.
J. Surg. Oncol. 2009;99:260–264. � 2008 Wiley-Liss, Inc.
KEY WORDS: node assessment; lymph node pathology; nodal metastasis; cancer staging; quality reporting
INTRODUCTION
Lymph node assessment becomes an issue for the pathologist from
the moment the surgeon transfers the specimen from the operating
room to the pathology suite. This transfer is completed with varying
degrees of detail being supplied to indicate the clinical scenario [1]. At
this point the pathology team begins the process of specimen handling,
gross evaluation and microscopic assessment.
PROCESSING ISSUES WITH GROSSINGAND HANDLING
Lymph nodes can be dissected out of the fresh specimen or after its
fixation in formalin. Since lymph nodes are firmer than the surrounding
fat, they can be identified by diligent, gentle squashing of fat with one’s
fingers. Bouin’s solution has traditionally been regarded as a good
fixative that could enhance detection. Other special fixatives have been
used as revealing solutions to help identify smaller lymph nodes [2–4]
but with varying success in different specimen types [5]. The decision
as to whether to use visually enhancing revealing solutions on routine
basis and whether the search for lymph nodes should be done in the
fresh versus fixed specimen remain user-dependent, with no uniform
guidelines across different pathology laboratories or different speci-
men types. In general, these decisions are made on case-by-case basis
in accordance with the local standard operating procedures of each
laboratory.
Lymph nodes identified by gross assessment are counted with the
understanding that the most accurate and final count will be entered
into the pathology report after microscopic examination. Lymph nodes
are measured either individually or collectively with recording of the
sizes of the smallest and the largest nodes. Each detected lymph node,
depending on its size, is then serial sectioned perpendicular to its long
axis at 0.3 cm intervals. Some prosectors may choose to section lymph
nodes through the hilum in order to increase the chances for detecting
small metastases in this area. Slicing lymph nodes into thin sections is
practically more important than the exact plane of sectioning [6]. A
representative section of a grossly involved lymph node is considered
adequate. However, it has been recommended that all sections of
grossly negative lymph nodes be submitted for further processing and
microscopic examination [7,8]. It is advisable to ensure that all slices
of the lymph node(s) submitted in the same cassette be of comparable
thickness and size. Significantly different slice thickness within the
same cassette may lead to loss of tissue, and potentially micro-
metastasis, from the thinner slices while the histotechnologist trims the
block in an attempt to obtain a complete section of the thicker slice.
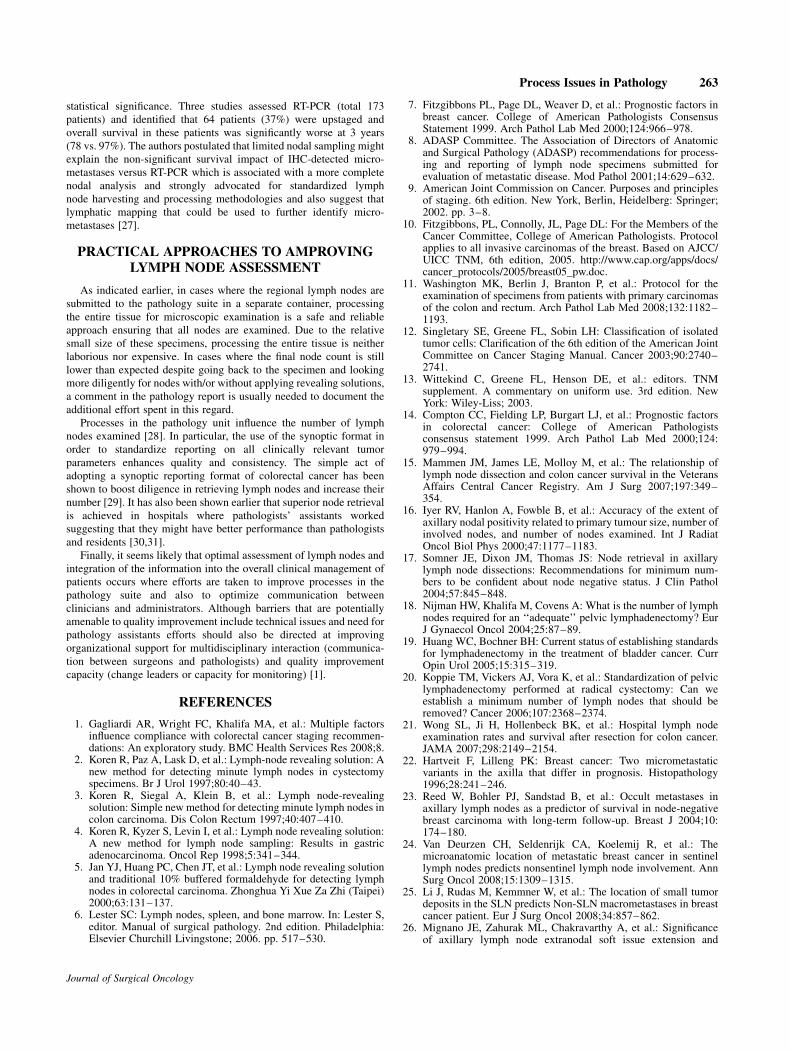
In the gross description portion of the pathology report it is
important to document the number of lymph nodes submitted
for sectioning and the specifics of their submission in each cassette.
Without this clear and detailed documentation, the exact number of
nodes can only be speculated leading to potentially serious interpreta-
tion problems (Fig. 1). Even with clear documentation of the
methodology used, confusion may still arise in rare situations. One
example is when a prosector identifies three lymph nodes; each
measuring 0.5 cm in greatest dimension, bisects each node and submits
all resultant six slices in the same cassette. If the microscopic
examination detects metastases in two of the slices on the final section,
the pathologist will not be able to conclusively decide whether the
metastatic lesions were actually present in one or two of the three
nodes originally submitted. The difference between metastasis to one
versus two lymph nodes could be important, depending on the clinical
setting. It is therefore, advisable that only slices of the same lymph
node be submitted together in the same cassette, unless one is dealing
with multiple small (less than 0.3 cm) nodes that can be submitted
together without bisecting or cutting.
*Correspondence to: Mahmoud A. Khalifa, MD, PhD, FRCPC, LaboratoryMedicine and Pathobiology, University of Toronto, Sunnybrook HealthSciences Centre, 2075 Bayview Avenue, Room E-400, Toronto, Ontario,Canada M4N 3M5. Fax: 416 480-4271.E-mail: [email protected]
Received 6 October 2008; Accepted 8 October 2008
DOI 10.1002/jso.21198
Published online 2 December 2008 in Wiley InterScience(www.interscience.wiley.com).
� 2008 Wiley-Liss, Inc.

INTERPRETATIONAL ISSUES WITHMICROSCOPY AND REPORTING
For the purpose of microscopic assessment of lymph node
metastases, a lymph node is defined as the lymphoid tissue of any
size with a recognizable internal nodal architecture including lymphoid
follicles, with or without germinal centers and lymphoid sinuses and is
surrounded by a fibrous capsule. Typically, a lymph node is round or
oval with a smooth contour. Irregular structureless collections of
lymphoid tissue with no fibrous capsule located in the fibroadipose
connective tissue around the resected organ do not count as lymph
nodes. When such irregular lymphoid collections, located in the
vicinity of an invasive carcinoma are involved by malignant cells, it is
regarded as part of the original tumor invading its surrounding
fibroadipose connective tissue. This distinction becomes particularly
important when the final count of lymph nodes, positive and/or
negative, will alter the pN categorization of the tumor. On the other
hand, direct extension of the primary tumor into a lymph node is
classified as a lymph node metastasis and is taken in consideration
while assigning a pN category [9].
The term macrometastasis refers to the intranodal presence of a
cluster of metastatic tumor cells larger than 2.0 mm. When metastatic
nodules are 0.2–2.0 mm in greatest dimension, they are classified as
micrometastasis. Similar to a macrometastasis, a micrometastasis
upgrades the pN category but is reported as pN1(mic). In many
diseases sites, the prognosis for patients with a solitary micrometastasis
is believed to be better than those with larger metastatic deposits.
However, the significance of multiple micrometastases in one lymph
node or multiple lymph nodes with micrometastases remains uncertain.
Multiple separate foci of micrometastases are still classified as
pN1(mic) [10,11]. The number of nodes that contain micrometastases
should be clearly specified in the pathology report since this may affect
treatment [10]. On the other hand, isolated tumor cells (ITCs), are
defined as single or small clusters of cells smaller than 0.2 mm in
greatest dimension, do not affect the pN categorization of the tumor.
Since ITCs do not usually induce recognizable histologic evidence of
malignant activity such as surrounding desmoplastic reaction, they
could be easily overlooked in H&E-stained routine tissue sections.
Their detection largely depends on the use of ancillary techniques
which are not routinely implemented. In fact, the use of immunohis-
tochemistry is still not recommended in routine examination of lymph
nodes for metastasis. The biologic significance of ITCs is unknown. It
has been recommended in breast pathology to use the pN0(iþ) and
pN0(i�) subcategories to distinguish between tumors in which the
ITCs are detected by the use of immunohistochemistry from those in
which detection is done in routinely stained H&E sections [12].
Similarly, the subcategories of pN0(molþ) and pN0(mol�) were
introduced to distinguish cases in which molecular methods such as
DNA analysis and reverse transcriptase polymerase chain reaction are
used [13]. It is also recommended that reporting of ITCs in colorectal
cancer follows the same principles [11].
It is important to remember that the pN category refers to the
status of regional lymph nodes. Metastases to non-regional lymph
nodes are reported under the pM category [9]. As expected, the
anatomic definition and guiding landmarks of ‘‘regional lymph nodes’’
are organ-dependent. Accordingly, clear communication between
surgeons and pathologists becomes crucial in cases where the exact
site of a submitted lymph node or a group of lymph nodes is ambiguous
and could make the difference between a pN and a pM categorization.
TECHNICAL ISSUES WITH NODE COUNTS
In order to accurately count regional lymph nodes, the pathologist
needs to include both lymph nodes present along the feeding blood
vessels that are usually located few centimeters from the resected
organ as well as the nodes present immediately adjacent to the organ
surface. The former nodes are usually sought for in the surrounding or
separately resected adipose tissue and are submitted in separate
cassettes for processing. Therefore, their sections are examined on
Journal of Surgical Oncology
Fig. 1. A histology slide with six sections of nodal structures whichcould represent 6, 3 (one in toto, one bisected, and one trisected),or just one large lymph node serially sections. Without a cleardocumentation as to how the tissue was submitted, speculative countscould create a serious problem.
Fig. 2. A photomicrograph of the uncinate margin in a pancreatico-duodenectomy specimen depicting a benign superior mesenteric lymphnode located at the surgical margin of excision (H&E 100�).
Process Issues in Pathology 261

separate slides. On the other hand, some organs (e.g., colorectum,
pancreas and lung) usually have lymph nodes imbedded in or
immediately adjacent in their outer layers and therefore, can be
included on the same slide depicting the tumor (Fig. 2). Accordingly, a
tumor nodule in these locations that is separate from the primary
carcinoma, even without histologic evidence of residual lymphoid
tissue is considered as an example of complete replacement of the
lymph node by a metastasis and is classified in the pN1 category as
long as it has the form and smooth contour of a lymph node. On the
other hand, if the nodule has an irregular contour, it should be classified
in the pT category as part of the primary tumor.
Regional lymph nodes are sometimes submitted to the pathology
suite as a separate specimen in a separate container as for example is
the case with prostatic, breast, cervical, uterine, ovarian and head and
neck cancers. Alternatively, regional nodes may be resected en bloc
with the cancer-harboring organ and are present in the same container
as is the case with colorectal, pancreatic, lung, kidney and urinary
bladder cancers. Still, in other cases a combination of both scenarios
may occur. Most pathology laboratories will handle the first scenario
by dissecting the grossly identifiable lymph nodes, submitting them as
previously described and also submit the remainder of the adipose
tissue to ensure that every possible lymph node in the specimen is
examined. This is technically possible because the entire specimen
submitted can usually fit in only few processing cassettes. In the second
scenario however, when less than expected lymph nodes are retrieved,
it is still prudent to go back to the specimen and aggressively submit
more adipose tissue or use a visually enhancing revealing solution.
Complete assessment of the regional lymph nodes ideally entails
removal of a sufficient number of lymph nodes to ensure the assigning
of the highest pN category [9]. Several studies have attempted to
address this issue in tumors of the colorectum [14,15], breast [16,17],
uterus [18], and urinary bladder [19,20]. However, the minimum
number of lymph nodes needed to confidently assign a pN0 category
has not been established in carcinomas of other organs such as ovary,
prostate or pancreas. The final number of resected lymph nodes is
dependent on the extent of the resection (i.e., surgeon factors) as well
as the degree of diligent search for the nodes in the resected specimen
(i.e., pathologist factors). In some cases, fewer than expected lymph
nodes are found even after extensive search. This could be attributed to
the fact that some unusual patients constitutionally have few lymph
nodes or the patient may have gone neoadjuvant chemo or radiation
therapy [6]. In the colorectum, 12 lymph nodes have been suggested as
the minimum number needed to confidently categorize the tumor in the
pN0 category [14]. For breast carcinoma, 16 nodes have been regarded
as a reasonable target to ensure a high level of confidence that the
axillary nodes are negative [17]. A statistical model has been suggested
to provide the clinician with a means for assessing the accuracy of the
number of positive axillary lymph nodes reported in patients with one
to three positive nodes [16]. Although some authors have suggested
that similar guidelines are needed to properly establish the extent of
lymphadenectomy for urinary bladder cancer [19], there has been no
evidence to date to suggest a minimum number of nodes in these
patients [20].
Several standard operating procedures in the anatomic pathology
laboratory are guided by benchmarks with numeric values. Hence the
suggested 12 lymph node benchmark in colorectal cancer cases serves
as a powerful example of a practical tool that can be used, directly or as
a surrogate, to assess many of the technical details involved in the
resection and pathologic assessment of colorectal cancer specimens.
The recommendations for its adoption as a quality indicator have
helped to lever efforts to standardize many procedural details in
anatomic pathology laboratories processing colorectal cancer resection
specimens. Expanding on the use of these benchmarks in order to
correlate them with clinical quality outcomes or to employ them as a
regulatory tool by third party payers is a risky leap in logic [21].
CHALLENGES TO INTERPRETING LYMPHNODE STATUS
Increased focus on the significance of lymph node status has led
to more diligent examination of nodes including bisecting or
serial sectioning large nodes, obtaining deeper sections and spending
more time examining H&E-stained sections under high power
magnification. This increased scrutiny has led to awareness of unusual
situations. Sometimes the pathologist will identify small clusters of
tumor cells that are limited to capsular lymphatics and/or subcapsular
sinus in the absence of nodal parenchymal involvement. It is now
believed that, in the absence of true parenchymal invasion, the mere
presence of tumor cells in subcapsular sinus is still a strong predictor of
overall survival [22,23]. Detection of such subtle tumor cells in
sentinel lymph nodes can predict the presence of more obvious
metastases in non-sentinel nodes [24,25] confirming that these cells
should be regarded as equal to parenchymal metastases found in
routine lymph node assessment.
Another challenge relates to lymph node assessment in resected
specimens following neoadjuvant therapy. In some of these specimens,
a lymph node may have a small collection of cell-free mucin, necrotic
debris or cholesterol clefts mixed with hemosiderin-laden macro-
phages. As long as no viable tumor cells are identified, these lymph
nodes are reported as negative (i.e., ypN0). Describing these findings in
a comment may be warranted to document that this finding may signify
the presence of a pre-treatment metastasis that was totally eradicated
by the neoadjuvant therapy.
A further unusual situation arises when a positive lymph node is
identified at the surgical margin, either in its entirety or, less
commonly, with the surgeon’s cut actually going through its
parenchyma. Some of the examples for this scenario include the root
of mesentry in a colectomy specimen, the edge of a mastectomy
specimen with an intramammary lymph node, and a superior
mesenteric lymph node in a pancreatico-duodencetomy specimen.
Since the metastasis in these situations is limited to the nodal
parenchyma it is counted under the pN1 category but the actual
surgical margin is still reported as negative. A description of this
finding is warranted in a comment in order to document its occurrence.
It is also worth mentioning that extranodal soft tissue extension of the
tumor into adjacent fat or muscle has been traditionally regarded as
a poor prognosticator since it is generally associated with a higher
number of positive lymph nodes. It is therefore, recommended to
document the presence of this finding in the pathology report. In some
cases, the extranodal extension is so extensive that individual nodes
cannot be separated and reliably counted. In these cases, the number
of positive lymph nodes may need to be estimated [6]. Whether
extranodal extension could be considered as an indication for
postoperative irradiation is still debatable and is certainly not the case
in every tumor site [26].
INCREASED SCRUTINY OF LYMPH NODES
Twenty-five percent of patients with Stage II colon cancers will
develop recurrence and die from colon cancer. It has been suggested
that further pathological investigations beyond routine histopatho-
logical evaluation such as immunohistochemistry (IHC) and serial
sectioning and/or reverse transcriptase-polymerase chain reaction
assay (RT-PCR), may identify node negative patients at high risk of
recurrence [27]. Studies of increased scrutiny or ultrastaging of lymph
nodes in colon cancer patients have demonstrated that this approach
does identify additional patients with lymph node metastases and this
may impact prognosis. Iddings et al. [27] completed a meta-analysis of
10 articles that assessed the prognostic effect of micro-metastases. IHC
identified a micrometastases in 32% of patients and the 3-year disease
free survival tended to be shorter (76% vs. 80%) but did not reach
Journal of Surgical Oncology
262 Khalifa and Smith
statistical significance. Three studies assessed RT-PCR (total 173
patients) and identified that 64 patients (37%) were upstaged and
overall survival in these patients was significantly worse at 3 years
(78 vs. 97%). The authors postulated that limited nodal sampling might
explain the non-significant survival impact of IHC-detected micro-
metastases versus RT-PCR which is associated with a more complete
nodal analysis and strongly advocated for standardized lymph
node harvesting and processing methodologies and also suggest that
lymphatic mapping that could be used to further identify micro-
metastases [27].
PRACTICAL APPROACHES TO AMPROVINGLYMPH NODE ASSESSMENT
As indicated earlier, in cases where the regional lymph nodes are
submitted to the pathology suite in a separate container, processing
the entire tissue for microscopic examination is a safe and reliable
approach ensuring that all nodes are examined. Due to the relative
small size of these specimens, processing the entire tissue is neither
laborious nor expensive. In cases where the final node count is still
lower than expected despite going back to the specimen and looking
more diligently for nodes with/or without applying revealing solutions,
a comment in the pathology report is usually needed to document the
additional effort spent in this regard.
Processes in the pathology unit influence the number of lymph
nodes examined [28]. In particular, the use of the synoptic format in
order to standardize reporting on all clinically relevant tumor
parameters enhances quality and consistency. The simple act of
adopting a synoptic reporting format of colorectal cancer has been
shown to boost diligence in retrieving lymph nodes and increase their
number [29]. It has also been shown earlier that superior node retrieval
is achieved in hospitals where pathologists’ assistants worked
suggesting that they might have better performance than pathologists
and residents [30,31].
Finally, it seems likely that optimal assessment of lymph nodes and
integration of the information into the overall clinical management of
patients occurs where efforts are taken to improve processes in the
pathology suite and also to optimize communication between
clinicians and administrators. Although barriers that are potentially
amenable to quality improvement include technical issues and need for
pathology assistants efforts should also be directed at improving
organizational support for multidisciplinary interaction (communica-
tion between surgeons and pathologists) and quality improvement
capacity (change leaders or capacity for monitoring) [1].
REFERENCES
1. Gagliardi AR, Wright FC, Khalifa MA, et al.: Multiple factorsinfluence compliance with colorectal cancer staging recommen-dations: An exploratory study. BMC Health Services Res 2008;8.
2. Koren R, Paz A, Lask D, et al.: Lymph-node revealing solution: Anew method for detecting minute lymph nodes in cystectomyspecimens. Br J Urol 1997;80:40–43.
3. Koren R, Siegal A, Klein B, et al.: Lymph node-revealingsolution: Simple new method for detecting minute lymph nodes incolon carcinoma. Dis Colon Rectum 1997;40:407–410.
4. Koren R, Kyzer S, Levin I, et al.: Lymph node revealing solution:A new method for lymph node sampling: Results in gastricadenocarcinoma. Oncol Rep 1998;5:341–344.
5. Jan YJ, Huang PC, Chen JT, et al.: Lymph node revealing solutionand traditional 10% buffered formaldehyde for detecting lymphnodes in colorectal carcinoma. Zhonghua Yi Xue Za Zhi (Taipei)2000;63:131–137.
6. Lester SC: Lymph nodes, spleen, and bone marrow. In: Lester S,editor. Manual of surgical pathology. 2nd edition. Philadelphia:Elsevier Churchill Livingstone; 2006. pp. 517–530.
7. Fitzgibbons PL, Page DL, Weaver D, et al.: Prognostic factors inbreast cancer. College of American Pathologists ConsensusStatement 1999. Arch Pathol Lab Med 2000;124:966–978.
8. ADASP Committee. The Association of Directors of Anatomicand Surgical Pathology (ADASP) recommendations for process-ing and reporting of lymph node specimens submitted forevaluation of metastatic disease. Mod Pathol 2001;14:629–632.
9. American Joint Commission on Cancer. Purposes and principlesof staging. 6th edition. New York, Berlin, Heidelberg: Springer;2002. pp. 3–8.
10. Fitzgibbons, PL, Connolly, JL, Page DL: For the Members of theCancer Committee, College of American Pathologists. Protocolapplies to all invasive carcinomas of the breast. Based on AJCC/UICC TNM, 6th edition, 2005. http://www.cap.org/apps/docs/cancer_protocols/2005/breast05_pw.doc.
11. Washington MK, Berlin J, Branton P, et al.: Protocol for theexamination of specimens from patients with primary carcinomasof the colon and rectum. Arch Pathol Lab Med 2008;132:1182–1193.
12. Singletary SE, Greene FL, Sobin LH: Classification of isolatedtumor cells: Clarification of the 6th edition of the American JointCommittee on Cancer Staging Manual. Cancer 2003;90:2740–2741.
13. Wittekind C, Greene FL, Henson DE, et al.: editors. TNMsupplement. A commentary on uniform use. 3rd edition. NewYork: Wiley-Liss; 2003.
14. Compton CC, Fielding LP, Burgart LJ, et al.: Prognostic factorsin colorectal cancer: College of American Pathologistsconsensus statement 1999. Arch Pathol Lab Med 2000;124:979–994.
15. Mammen JM, James LE, Molloy M, et al.: The relationship oflymph node dissection and colon cancer survival in the VeteransAffairs Central Cancer Registry. Am J Surg 2007;197:349–354.
16. Iyer RV, Hanlon A, Fowble B, et al.: Accuracy of the extent ofaxillary nodal positivity related to primary tumour size, number ofinvolved nodes, and number of nodes examined. Int J RadiatOncol Biol Phys 2000;47:1177–1183.
17. Somner JE, Dixon JM, Thomas JS: Node retrieval in axillarylymph node dissections: Recommendations for minimum num-bers to be confident about node negative status. J Clin Pathol2004;57:845–848.
18. Nijman HW, Khalifa M, Covens A: What is the number of lymphnodes required for an ‘‘adequate’’ pelvic lymphadenectomy? EurJ Gynaecol Oncol 2004;25:87–89.
19. Huang WC, Bochner BH: Current status of establishing standardsfor lymphadenectomy in the treatment of bladder cancer. CurrOpin Urol 2005;15:315–319.
20. Koppie TM, Vickers AJ, Vora K, et al.: Standardization of pelviclymphadenectomy performed at radical cystectomy: Can weestablish a minimum number of lymph nodes that should beremoved? Cancer 2006;107:2368–2374.
21. Wong SL, Ji H, Hollenbeck BK, et al.: Hospital lymph nodeexamination rates and survival after resection for colon cancer.JAMA 2007;298:2149–2154.
22. Hartveit F, Lilleng PK: Breast cancer: Two micrometastaticvariants in the axilla that differ in prognosis. Histopathology1996;28:241–246.
23. Reed W, Bohler PJ, Sandstad B, et al.: Occult metastases inaxillary lymph nodes as a predictor of survival in node-negativebreast carcinoma with long-term follow-up. Breast J 2004;10:174–180.
24. Van Deurzen CH, Seldenrijk CA, Koelemij R, et al.: Themicroanatomic location of metastatic breast cancer in sentinellymph nodes predicts nonsentinel lymph node involvement. AnnSurg Oncol 2008;15:1309–1315.
25. Li J, Rudas M, Kemmner W, et al.: The location of small tumordeposits in the SLN predicts Non-SLN macrometastases in breastcancer patient. Eur J Surg Oncol 2008;34:857–862.
26. Mignano JE, Zahurak ML, Chakravarthy A, et al.: Significanceof axillary lymph node extranodal soft issue extension and
Journal of Surgical Oncology
Process Issues in Pathology 263

indications for postmastectomy irradiation. Cancer 1999;86:1258–1262.
27. Iddings D, Ahmad A, Elashoff D, et al.: The prognostic effect ofmicrometastases in previously staged lymph node negative (N0)colorectal carcinoma: A meta-analysis. Ann Surg Oncol 2006;13:1386–1392.
28. Rieger NA, Barnett FS, Moore JW, et al.: Quality of pathologyreporting impacts on lymph node yield in colon cancer. J ClinOncol 2007;25:463.
29. Chan NG, Duggal A, Weir MM, et al.: Pathological reporting ofcolorectal cancer specimens: A retrospective survey in an academicCanadian pathology department. Can J Surg 2008;51: 284–288.
30. Galvis CO, Raab SS, D’Amico F, et al.: Pathologists’ assistantspractice: A measurement of performance. Am J Clin Pathol 2001;116:816–822.
31. Wright FC, Law CHL, Ritacco R, et al.: Barriers to optimalassessment of lymph nodes in colorectal cancer specimens. Am JClin Pathol 2004;121:663–670.
Journal of Surgical Oncology
264 Khalifa and Smith