Embed Size (px)
Citation preview
Page
Lungemboli och CTLungemboli och CT
Var stVar ståår vi r vi idag?idag?Ulf Nyman, docentUlf Nyman, docent
Institutionen fInstitutionen föör r translationelltranslationell medicinmedicin
Divisionen fDivisionen föör medicinsk radiologir medicinsk radiologi
SkSkåånes universitetssjukhus, Malmnes universitetssjukhus, Malmöö

Page
•• Stefan RosforsStefan Rosfors•• klinisk fysiolog, Sklinisk fysiolog, Söödersjukhuset, Stockholmdersjukhuset, Stockholm
•• Klas Klas MMåårere•• radiolog, Universitetssjukhuset, Linkradiolog, Universitetssjukhuset, Linkööpingping
•• Ulf NymanUlf Nyman•• radiolog, Lasarettet i Trelleborgradiolog, Lasarettet i Trelleborg
•• Margareta Margareta HellgrenHellgren--WWåångdahlngdahl•• gynekolog, SU/gynekolog, SU/ÖÖstra Sjukhuset, Gstra Sjukhuset, Gööteborg.teborg.
SBU-report 158/2002Blodpropp Blodpropp –– fföörebyggande, diagnostik och rebyggande, diagnostik och behandling av venbehandling av venöös s tromboembolismtromboembolism
DiagnostikDiagnostik
• Stefan Rosfors• klinisk fysiolog, Södersjukhuset, Stockholm
• Klas Måre• radiolog, Universitetssjukhuset, Linköping
• Ulf Nyman• radiolog, Lasarettet Trelleborg
• Margareta Hellgren-Wångdahl• gynekolog, SU/Östra Sjukhuset, Göteborg.
SoS:s arbetsgrupp SoS:s arbetsgrupp –– VVåård av blodpropprd av blodpropp
•• David BergqvistDavid Bergqvist kkäärlkirurgirlkirurgi
•• Mats EliassonMats Eliasson internmedicininternmedicin
•• Bengt ErikssonBengt Eriksson ortopediortopedi
•• Henry ErikssonHenry Eriksson internmedicininternmedicin
•• Margareta HellgrenMargareta Hellgren--WWåångdahl ngdahl gyn/obstetrikgyn/obstetrik
•• KarlKarl--GGöösta Ljungstrsta Ljungströömm kirurgikirurgi
•• Ulf NymanUlf Nyman radiologiradiologi
•• Sam SchulmanSam Schulman hematologihematologi
www.socialstyrelsen.se/riktlinjer

Page
Googla Koagulationscentrum Region Skåne
US = UltrasonographyScintigraphy
CT = computed tomography
DD--dimerdimer
Clinical probability

Page
KliniskKlinisk osannolikosannolik PE & PE & negativnegativ DD--dimerdimer
3 3 mmåånadersnaders uppfuppfööljningljning fföörr VTEVTE
•• AntalAntal ((metaanalysmetaanalys)) 10 94110 941
•• PE PE frekvensfrekvens 21%21%
•• KliniskKlinisk osannolikosannolik & & negneg DD--dimerdimer 27% (2227% (22--34)34)
•• FalsktFalskt negativanegativa (95% KI)(95% KI) 0.4% (0.20.4% (0.2--0.7) 0.7)
LucassenLucassen MetaMeta--analysis Ann Intern Med 2011;155:448analysis Ann Intern Med 2011;155:448--60.60.
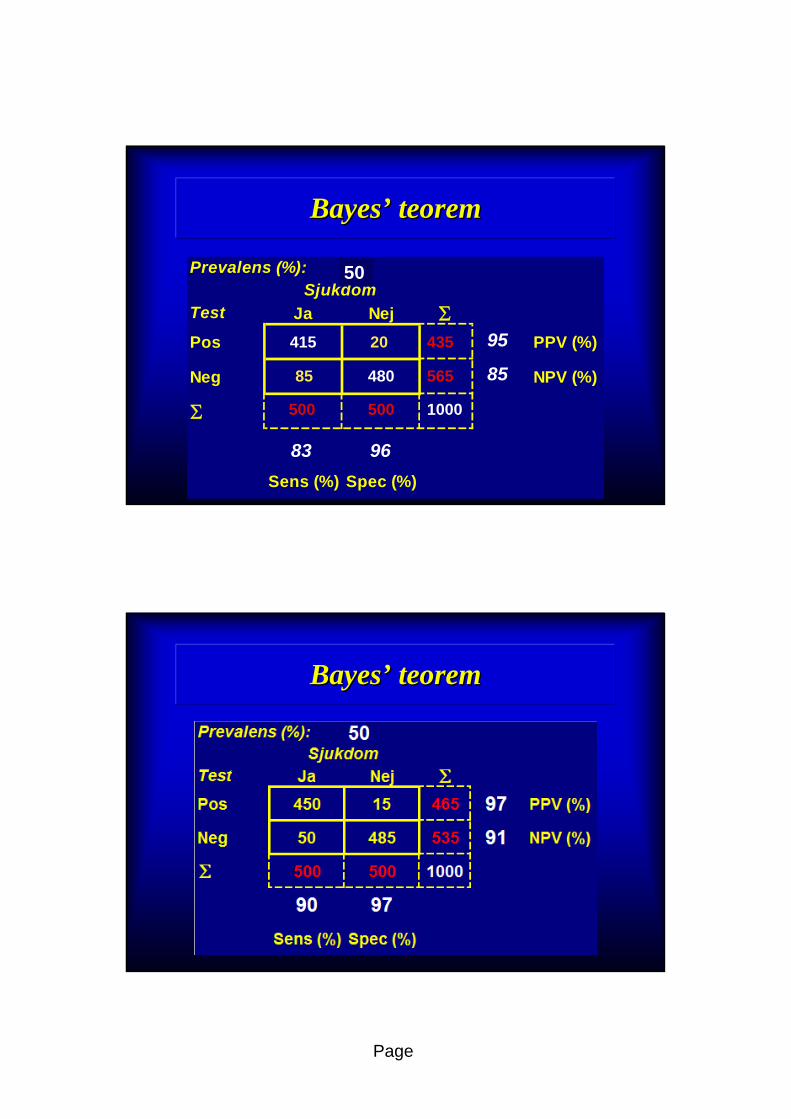
BayesBayes’’ theoremtheorem
•• Thomas Bayes (1702Thomas Bayes (1702--1761)1761)
•• English clergyman/mathematicianEnglish clergyman/mathematician•• Fellow of Royal SocietyFellow of Royal Society
•• ””Essays towards solving a probaEssays towards solving a proba--
bility in the doctrine of chancesbility in the doctrine of chances””•• Found after his death and published 1763Found after his death and published 1763
Taube & Malmquist. Räkna med vad du tror. Bayes’ sats i diagnostiken. Läkartidningen 2001;98(24):2910-2913.Barnard Biometrika 1958;45(parts 3&4):293-315

Page
BayesBayes’’ theoremtheorem
PIOPED II PIOPED II (NEJM 2006;345:2317(NEJM 2006;345:2317--27)27)
Prospective Prospective multicentermulticenter investigation in USAinvestigation in USA

Page
CT for CT for acuteacute pulmonarypulmonary embolismembolism
SensSens SpecSpec
••PIOPEDPIOPED--IIII 83%83% 96%96%
•• 84% 484% 4--row row detectordetector
•• 16% 816% 8--1616--row row detectordetector
Stein et al. New Eng J Med 2006;354;2317-27.
Negative Negative computedcomputed tomographytomography
””LowLow”” sensitivitysensitivity
•• Bilateral ultrasound on all negative CT (80%)Bilateral ultrasound on all negative CT (80%)
•• FedulloFedullo & & TapsonTapson NEJM 2003;349:1247NEJM 2003;349:1247--5656
•• RoutineRoutine CT CT venographyvenography (100%)(100%)
•• Cham et al. Radiology 2005;234:591Cham et al. Radiology 2005;234:591--594594

Page
5
19
66
6
23
54
0
20
40
60
80
Låg Måttlig Hög
DVTLE
Percentage 48 35 17
DVT (20%) LE (17%)11 studies 4 studiesn: 3034 n: 2840
J Thromb Haemost 2003;1:1888
Wells Wells clinicalclinical criteriacriteria of DVT and PEof DVT and PE
VTE%
LowLow ModerateModerate HighHigh
BayesBayes’’ teoremteorem
Prevalens (%): 30
Test Ja Nej Pos PPV (%)
Neg NPV (%)
Sens (%) Spec (%)
Sjukdom
1000900100
88186417
1193683
9683
70
98
10

Page
BayesBayes’’ teoremteorem
PIOPED II PIOPED II (NEJM 2006;345:2317(NEJM 2006;345:2317--27)27)
Clinicians (and radiologists) should Clinicians (and radiologists) should
probably think twice before accepting a probably think twice before accepting a
PE diagnosis in a patient in whom the PE diagnosis in a patient in whom the
disease is thought to be clinically unlikely disease is thought to be clinically unlikely
””unless CTA is undisputedly positiveunless CTA is undisputedly positive””
Perrier & Bounameaux. Letter to the Editor JAMA 2006;345:2383-4
Page
BayesBayes’’ teoremteorem
Prevalens (%): 30
Test Ja Nej Pos PPV (%)
Neg NPV (%)
Sens (%) Spec (%)
Sjukdom
1000500500
56548085
43520415
9683
95
85
50
BayesBayes’’ teoremteorem

Page
Management studyManagement study
•• Patients w. negative CT are not Patients w. negative CT are not anticoagulatedanticoagulated
•• apart from other indications than VTEapart from other indications than VTE
•• Clinical followClinical follow--up for 3 monthsup for 3 months
•• Objective testing in case of DVT/PE symptomsObjective testing in case of DVT/PE symptoms
•• VTE VTE ≤≤1.5% (upper 95% CI <3%) acceptable 1.5% (upper 95% CI <3%) acceptable
Negative CT Negative CT -- Outcome studiesOutcome studiesPos DPos D--dimerdimer or high or high clinclin prob/clinprob/clin likely PElikely PE
AuthorAuthor YearYear NN VTE VTE (3mo (3mo f/uf/u))
FrequencyFrequency Upper 95% CIUpper 95% CI
•• van van StrijenStrijen 20032003 510510 0.8%0.8% 1.6% 1.6%
•• PerrierPerrier 20052005 524524 1.7%1.7% 2.8%2.8%
•• GhanimaGhanima 20052005 329329 0.9%0.9% 1.9%1.9%
•• van Bellevan Belle 20062006 22492249 1.3%1.3% 1.8%1.8%
•• AndersenAndersen 20072007 694694 0.4%0.4% 0.9%0.9%
•• RighiniRighini 20082008 558558 0.9%0.9% 1.7%1.7%

Page
Konklusion
•• CT missar smCT missar småå LE som inte tycks LE som inte tycks
krkrääva behandlingva behandling
•• Ingen indikation fIngen indikation föör rutinmr rutinmäässig ssig
venundersvenundersöökningkning vid negativ CT vid negativ CT
•• Huvudsakliga problemet med CT Huvudsakliga problemet med CT
äär r ööverdiagnostik verdiagnostik
Isolated Isolated subsegmentalsubsegmental (ISS) PE(ISS) PE
•• MultiMulti--slice CT allows better visualization of slice CT allows better visualization of
subsegmentalsubsegmental arteries, hence the rate of arteries, hence the rate of
isolated isolated subsegmentalsubsegmental PE may increasePE may increase
•• It is unclear whether the riskIt is unclear whether the risk--benefit ratio of benefit ratio of
anticoagulant therapy is favorableanticoagulant therapy is favorable
Carrier et al. J of Thrombosis & Haemostasis 2010;8:1716-22

Page
Rate of isolated subsegm PERate of isolated subsegm PESystematic review & metaSystematic review & meta--analysesanalyses
SingleSingle--slice (n=15)slice (n=15) MultiMulti--slice (n=11)slice (n=11)
Carrier et al. J of Thrombosis & Haemostasis 2010;8:1716-22
Rate of isolated Rate of isolated subsegmsubsegm PEPE
Systematic review & metaSystematic review & meta--analysesanalyses
SingleSingle--slice (n=15)slice (n=15) MultiMulti--slice (n=11)slice (n=11)
33--5 mm slices5 mm slices 11--2 mm slices2 mm slices
4.7%4.7% 9.4%9.4%
44--det: 7.1%det: 7.1%
1616--det: 6.9%det: 6.9%
64 64 detdet: 15%: 15%
Carrier et al. J of Thrombosis & Haemostasis 2010;8:1716-22
Higher rate of VTEHigher rate of VTE
during during f/uf/u of of negneg CTCT
due to FN diagnosis?due to FN diagnosis?

Page
Rate of isolated subsegm PERate of isolated subsegm PE
Systematic review & metaSystematic review & meta--analysesanalysesSingleSingle--slice (n=15)slice (n=15) MultiMulti--slice (n=11)slice (n=11)
3 months VTE risk after negative CT3 months VTE risk after negative CT
0.9%0.9% 1.1%1.1%
44--det: 1.4%det: 1.4%
1616--det: 0.6%det: 0.6%
64 det: 0.8%64 det: 0.8%
Carrier et al. J of Thrombosis & Haemostasis 2010;8:1716-22
Rate of isolated Rate of isolated subsegmsubsegm PEPE
MultiMulti--slice CT increases the rate of slice CT increases the rate of subsegmsubsegm PE PE
w/o lowering the 3 w/o lowering the 3 mosmos risk of VTE of negative CT risk of VTE of negative CT
suggesting that they are not clinically relevantsuggesting that they are not clinically relevant
Carrier et al. J of Thrombosis & Haemostasis 2010;8:1716-22

Page
Rate of Rate of subsegmentalsubsegmental PEPE
SubsegmentalSubsegmental PE most prevalent in lowPE most prevalent in low--
probability V/Q scan (PIOPED)probability V/Q scan (PIOPED)
Patients w. low/intermediate V/Q and Patients w. low/intermediate V/Q and
negative serial proximal US can be safely negative serial proximal US can be safely
left without anticoagulation left without anticoagulation
Carrier et al. J of Thrombosis & Haemostasis 2010;8:1716-22
Isolated Isolated subsegmentalsubsegmental PEPE
•• Reported isolated Reported isolated subsegmentalsubsegmental PE should be PE should be
reviewed by an reviewed by an experiencedexperienced radiologistradiologist
•• Poor Poor interobserverinterobserver agreementagreement
•• If isolated If isolated subsegmentalsubsegmental, consider serial , consider serial
proximal US, especially if at risk for ACproximal US, especially if at risk for AC
•• Prospective management study underwayProspective management study underway
•• No AC if normal bilateral serial proximal USNo AC if normal bilateral serial proximal US
•• France, Switzerland and CanadaFrance, Switzerland and Canada

Page
V/Q mismatchV/Q mismatch
DifferentialdiagnoserDifferentialdiagnoser
SBUSBU--rapport 158rapport 158--II/2002II/2002
Kapitel 3.6 Skintigrafi, sid 130Kapitel 3.6 Skintigrafi, sid 130
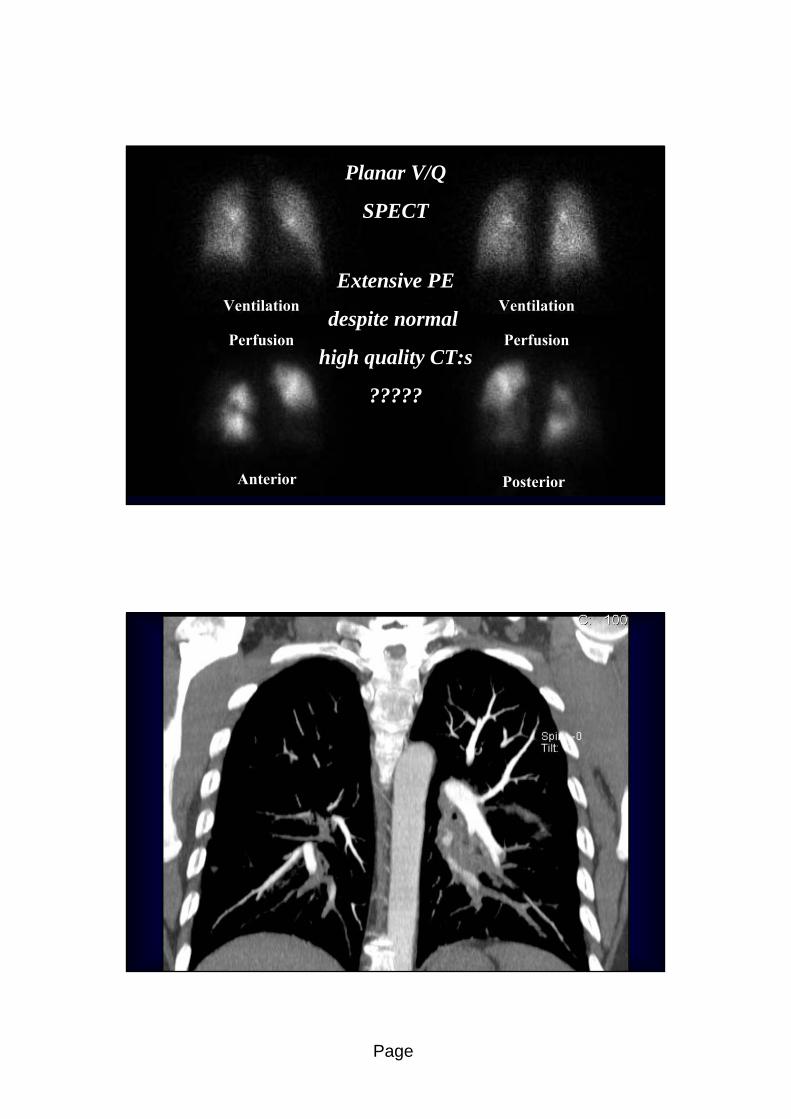
Pulmonary embolism?Pulmonary embolism?
•• Man, 44 years, arabic originMan, 44 years, arabic origin
•• Hodgkin lymphomaHodgkin lymphoma
•• HighHigh--quality CT Mayquality CT May--Oct 2009 neg for PEOct 2009 neg for PE
•• 370 HU, no artefacts370 HU, no artefacts
•• peripheral vessels well depictedperipheral vessels well depicted
Page
Lungembolism?Lungembolism?
VentilationVentilation
PerfusionPerfusion
VentilationVentilation
PerfusionPerfusion
Anterior Posterior
Planar V/QPlanar V/Q
SPECTSPECT
Extensive PEExtensive PE
despite normal despite normal
high quality CT:shigh quality CT:s
??????????

Page
Anatomisk obstruktionsgradAnatomisk obstruktionsgrad
1. BNP (brain natriuretic peptide), computed tomography or echocardiography.2. Cardiac troponin, T or I-positivea) In case of chock/hypotensionthere is no need to evaluate the right ventricleEuropean Society of Radiology guidelines (www.escardio.org/guidelines)

Page
Risk stratificationRisk stratification
•• Anatomical obstruction scoreAnatomical obstruction score
•• Right ventricular dysfunctionRight ventricular dysfunction
•• dilatation RV (dilatation RV (load) secondary to load) secondary to pulmonary resistancepulmonary resistance
•• inflow to left heartinflow to left heart, reduced left ventricle, reduced left ventricle
•• coronary insufficiency, right ventricular failure coronary insufficiency, right ventricular failure
•• initially increased pulmonary artery pressure now fallsinitially increased pulmonary artery pressure now falls
RV/LV ratio 2:1<1 normal
>1.5 warning!
65% obstruction index
Septum
Page
RenalRenal impairmentimpairment
•• DosesDoses decreasesdecreases with with increasedincreased detectordetector rowsrows
•• DoseDose per kg per kg bodybody weightweight
•• 120 kVp 120 kVp 80 kVp80 kVp
•• increasedincreased iodineiodine attenuation*1.6attenuation*1.6
•• DecreasedDecreased cardiac outputcardiac output•• high high ageage + + renalrenal impairmentimpairment cardiac cardiac diseasedisease
•• HalvedHalved CM CM dosedose –– 300 300 150 mg I/kg150 mg I/kg
•• IncreasedIncreased tubetube loadingloading (mAs)*4(mAs)*4•• to to keepkeep image image noisenoise constantconstant, , radiationradiation increasedincreased by 50%by 50%
Acta Radiol 2009;50:181Acta Radiol 2009;50:181--193193
Eur Radiol 2010;20:1321Eur Radiol 2010;20:1321--30.30.
Page
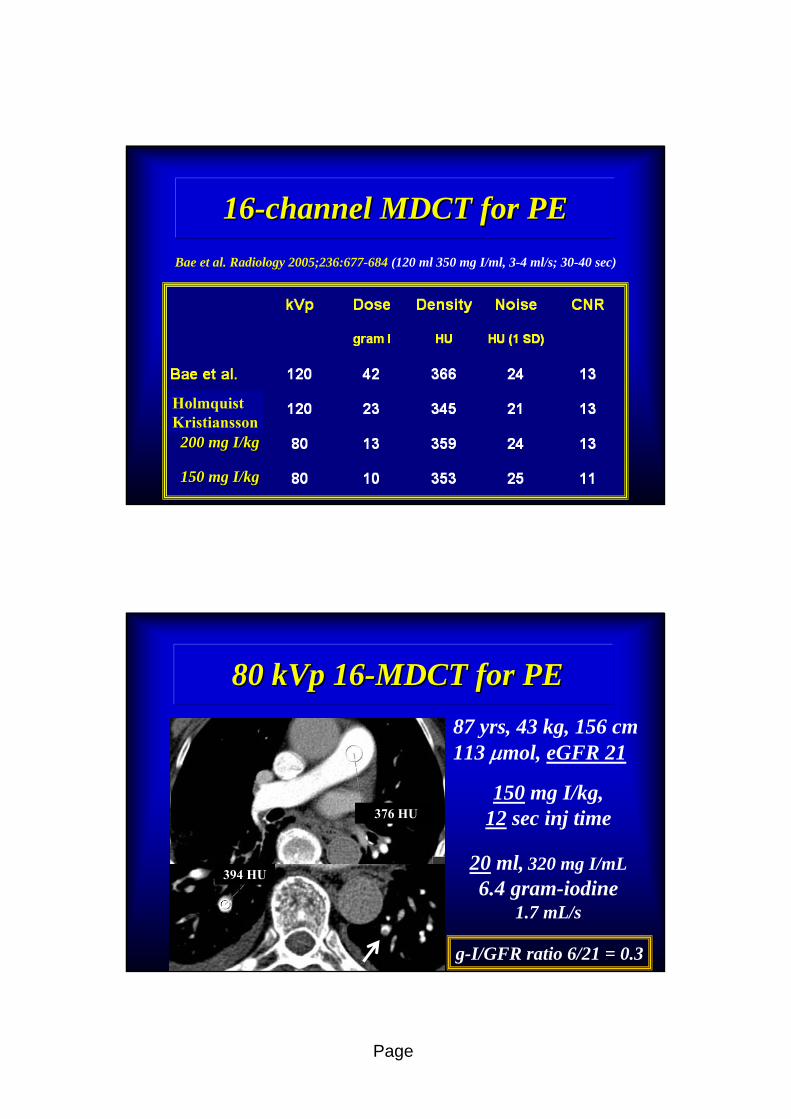
1616--channel MDCT for PEchannel MDCT for PE
Bae et al. Radiology 2005;236:677-684 (120 ml 350 mg I/ml, 3-4 ml/s; 30-40 sec)
200 mg I/kg200 mg I/kg
150 mg I/kg150 mg I/kg
HolmquistKristiansson
80 kVp 1680 kVp 16--MDCT for PEMDCT for PE
87 yrs, 43 kg, 156 cm 113 mol, eGFR 21
150 mg I/kg,12 sec inj time
20 ml, 320 mg I/mL6.4 gram-iodine
1.7 mL/s
g-I/GFR ratio 6/21 = 0.3
376 HU
394 HU
Page
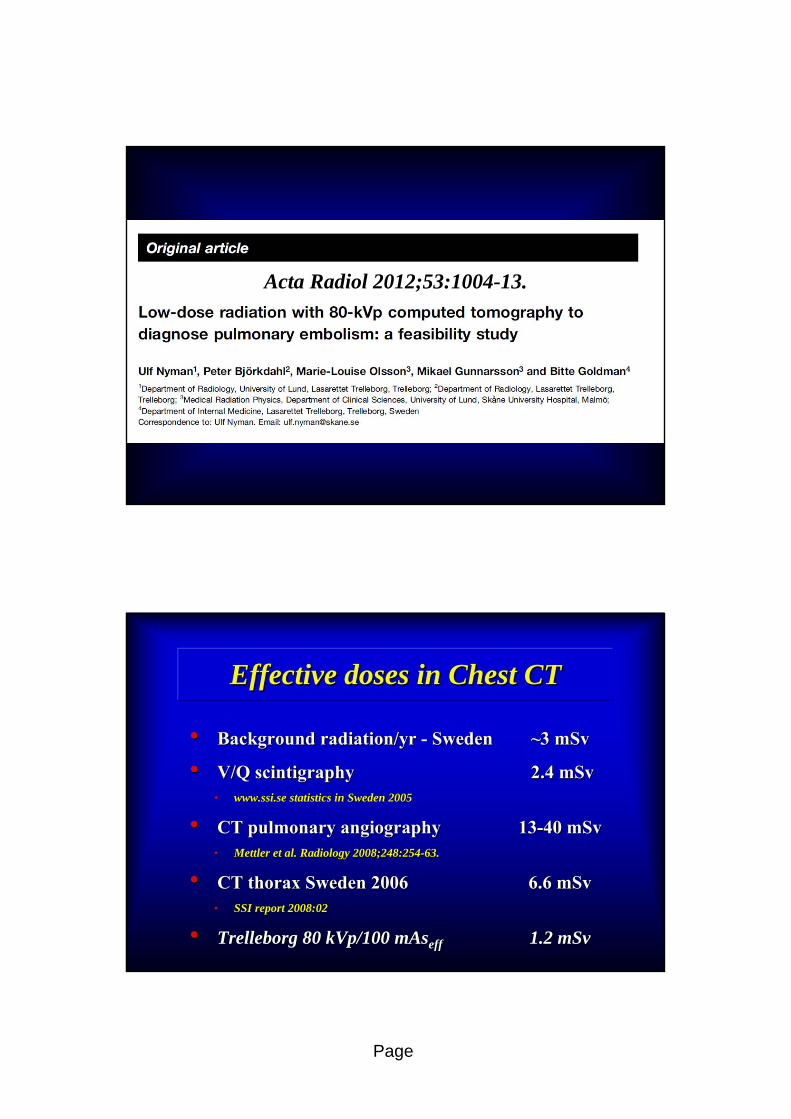
Acta Radiol 2012;53:1004Acta Radiol 2012;53:1004--13.13.
EffectiveEffective dosesdoses in in ChestChest CTCT
•• BackgroundBackground radiationradiation/yr /yr -- SwedenSweden ~~3 3 mSvmSv
•• V/Q V/Q scintigraphyscintigraphy 2.4 2.4 mSvmSv•• www.ssi.sewww.ssi.se statisticsstatistics in Sweden 2005in Sweden 2005
•• CT CT pulmonarypulmonary angiographyangiography 1313--40 40 mSvmSv•• MettlerMettler et al. Radiology 2008;248:254et al. Radiology 2008;248:254--63.63.
•• CT thorax Sweden 2006CT thorax Sweden 2006 6.6 6.6 mSvmSv•• SSI SSI reportreport 2008:022008:02
•• Trelleborg 80 kVp/100 Trelleborg 80 kVp/100 mAsmAseffeff 1.2 1.2 mSvmSv

Page
3838--year old, pregnant 20th weekyear old, pregnant 20th weekLäkartidningen 2010;107(15);989-94.
Leung et al.
Radiology
2012;262:635-646
Page
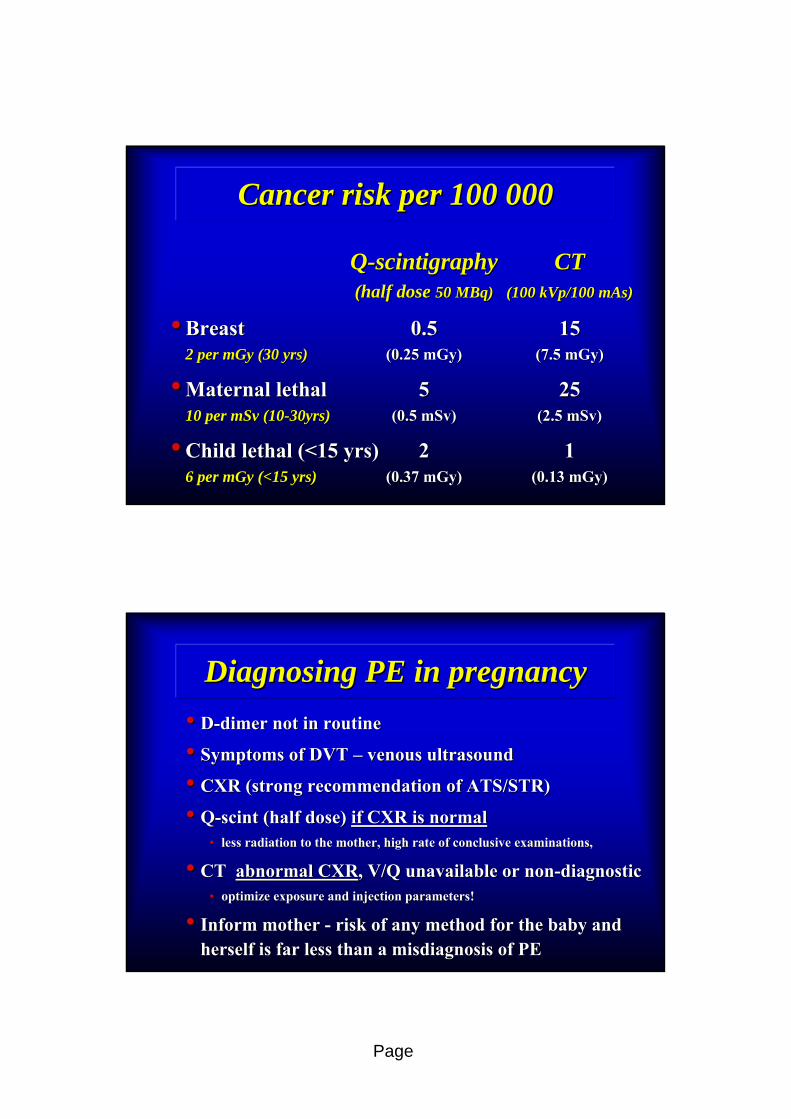
Cancer risk per 100 000Cancer risk per 100 000
QQ--scintigraphyscintigraphy CTCT(half dose (half dose 50 MBq)50 MBq) (100 kVp/100 mAs)(100 kVp/100 mAs)
•• Breast Breast 0.50.5 15152 per mGy (30 yrs)2 per mGy (30 yrs) (0.25 mGy)(0.25 mGy) (7.5 mGy)(7.5 mGy)
•• Maternal lethal Maternal lethal 55 252510 per mSv (1010 per mSv (10--30yrs)30yrs) (0.5 mSv)(0.5 mSv) (2.5 mSv)(2.5 mSv)
•• Child lethal (<15 yrs)Child lethal (<15 yrs) 22 116 per mGy (<15 yrs)6 per mGy (<15 yrs) (0.37 mGy)(0.37 mGy) (0.13 mGy)(0.13 mGy)
DiagnosingDiagnosing PE in PE in pregnancypregnancy
•• DD--dimerdimer not in not in routineroutine
•• Symptoms of DVT Symptoms of DVT –– venousvenous ultrasoundultrasound
•• CXR (strong CXR (strong recommendationrecommendation of ATS/STR) of ATS/STR)
•• QQ--scintscint ((halfhalf dosedose) ) ifif CXR is normalCXR is normal•• less less radiationradiation to the to the mothermother, high , high raterate of of conclusiveconclusive examinations, examinations,
•• CT CT abnormalabnormal CXRCXR, V/Q , V/Q unavailableunavailable or or nonnon--diagnosticdiagnostic•• optimizeoptimize exposureexposure and and injectioninjection parameters!parameters!
•• InformInform mothermother -- risk of risk of anyany methodmethod for the baby and for the baby and herselfherself is far less is far less thanthan a a misdiagnosismisdiagnosis of PEof PE

Page
Sammanfattning
•Över- ej underdiagnostik största problemet
•Hö-kammarpåverkan kan identifieras
•Stråldoserna under kontroll
•Risk för kontrastnefropati minimalt problem
•Skint 1:a handsmetod för gravida, CT när skint
kan vara inkonklusivt eller inte är tillgängligt























![[Michael Nyman] the Piano](https://img.dokumen.tips/doc/110x75/563dbae5550346aa9aa8c3d3/michael-nyman-the-piano-5692eec0f00f6.jpg)





![the piano michael nyman book[1]](https://img.dokumen.tips/doc/110x75/5571f1d649795947648bbc1e/the-piano-michael-nyman-book1.jpg)