Embed Size (px)
Citation preview

Keywords: Lung
doi:10.1016/j.jgo.2013.09.036
Track 1 - Solid Tumours in the ElderlyLung cancer in eldery patientsP033Post ablation chemotherapy improves outcomes followingpercutaneous radiofrequency ablation for local control ofsolid lung tumors in elderly patientsP. Andrew1,*, S. O'Connor2, S. Jerat3, R. Lee-Ying4. 1Department of InternalMedicine, The Ottawa Hospitals, Ottawa, Canada; 2City University, London,United Kingdom; 3ATLAS Medical Research Inc., Edmonton; 4Department ofMedical Oncology, Tom Baker Cancer Centre, Calgary, Canada
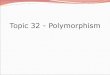
Introduction: With a burgeoning population of elderly patients withlung cancer deemed non-surgical, increasing utilization of minimally-invasive, safe, repeatable, tissue-preserving techniques such as percu-taneous radiofrequency ablation (RFA) is occurring for the manage-ment of solid tumors. However, it is unknownwhether a strategy of RFAplus post ablation chemotherapy (PAC) improves locoregional andsurvival outcomes in aged patients.Objectives: We compared local tumor recurrence and survivaloutcomes of RFA plus PAC versus RFA alone for management ofprimary and metastatic solid lung tumors in non-surgical patients.Methods: Searched PubMed, the Cochrane Library, EMBASE, andCANCERLIT databases from January 2000 to December 2012. Blindedduplicate screening for data extraction. Population was deemed non-surgical, with solid lung tumors, both primary and/or metastatic.Generated aggregate effect estimates from constituent studies forthree outcomes (e.g., local tumor progression [LTP], overall survival[OS], and disease-free survival [DFS]) with comparison of pooledfixed effect analyses concerning RFA plus PAC versus RFA alone.Results: RFA plus PAC group versus RFA alone group: LTP of 15% overmedian follow-up of 31 months [range 12 to 59] versus 19% overmedian follow-up of 21 months [range 12 to 29]; odds ratio (OR)0.73 (95% CI: 0.61-0.86, p b 0.05) at 12 month follow-up. OS was 89%versus 78%, respectively, at 12 month follow-up; OR 1.52 (95% CI:1.16-2.00, p = 0.003). DFS was 90% versus 82%, respectively, at12 month follow-up; OR 3.18 (95% CI: 2.04-4.96, p b 0.05). Forrestplots for the outcomes of LTP, OS, and DFS are shown. Sensitivityanalyses were robust, publication bias relatively narrow, and Qstatistic b21; p N 0.13 for all outcomes.Image:
Conclusion: A strategy of RFA plus PAC retards LTP, but lengthensboth OS and DFS. Elderly patients most likely to benefit from thisstrategy would be non-surgical candidates with relatively goodperformance status who could tolerate both RFA and PAC.
Disclosure of Interest: None Declared
Keywords: Lung, Translational research
doi:10.1016/j.jgo.2013.09.037
Track 1 - Solid Tumours in the ElderlyLung cancer in eldery patientsP034Lung cancer in women: Do tumors behave differently in theelderly? A prospective comparison of World07 data baseR. Gironés1,* on behalf of ICAPEM,M. Provencio2 on behalf of ICAPEM,M.Majem3 on behalf of ICAPEM, P. Garrido4 on behalf of ICAPEM, E. Felip5 onbehalf of ICAPEM, E. Felip5 on behalf of ICAPEM, N. Viñolas6 on behalf ofICAPEM, A. Artal7 on behalf of ICAPEM, L. Isla8 on behalf of ICAPEM, E.Carcereny9 on behalf of ICAPEM, C. García-Campelo10 on behalf ofICAPEM, P. Lianes11 on behalf of ICAPEM, R. De las Peñas12 on behalf ofICAPEM and ICAPEM: Asociación para la investigación de cáncer depulmón enmujeres. 1Medical Oncology, Hospital Lluis Alcanyis, Xàtiva;2Medical Oncology, Hospital Puerta del Hierro, Madrid; 3MedicalOncology, Hospital Sant Pau, Barcelona; 4Medical Oncology, HospitalRamón y Cajal, Madrid; 5Medical Oncology, Hospital Vall d'Hebron;6Medical Oncology, Hospital Clinic, Barcelona; 7Medical Oncology,Hospital Miguel Servet; 8Medical Oncology, Hospital Lozano Blesa,Zaragoza; 9Medical Oncology, Hospital Germans Trias i Pujol, Badalona;10Medical Oncology, Complexo Hospital A Coruña, Coruña; 11MedicalOncology, Hospital de Mataró, Barcelona; 12Medical Oncology, Hospitalde Castellón, Castellón, Spain
Introduction: Lung cancer appears to behave differently inwomen.Women are more likely to present with adenocarcinoma,diagnosed at localized disease and have better survival(1).It's unclear,however, whether elderly lung cancer women had a different naturalhistory than youngerObjectives: To investigate differences in epidemiology,types of presen-tation,tumor characteristics,treatment and survival between youngerand older women with lung cancer included in a prospective Spanishmulticenter registryMethods: Wolrd07 is an epidemiological multicentre prospectiveregistration of women with lung cancer attended at Spanishinstitutions. From October 2007 to October 2012. Last follow up:April 2013. Clinicopathologic and tumor information was pro-spectively collected and compared between age groups. Survivalwas determined as the interval form the date of cancerdiagnosis to the date of death. The institution’s ethical reviewboard approved this study. All of the patients provided writteninformed consentResults: 38 institutions registered 2081 patients. Patient’s characteris-tics are reported in table. Caucasian race (98%,p:0,899). Some hormonalfactors shown statistical differences; however number of children wassimilar (median: 2; 0-10). Smoking habits differ from both groups.Median pack years and passive smokerwere equal (40 py; 37% passive).34% in both groups had family history of lung cancer. Non-small celllung cancer was significantly more frequent in elderly group. Stage IVprevailed In both groups (62-63%). Most younger patients receivedthird (14% vs 6%, p b 0,001) and forth lines for metastatic disease (6% vs1,4% p b 0,001). At last follow up; 44% younger versus 52% elderly haddied (p:0,001). Overall survival: 24,7 months versus 19.4 p:0.003.Analysis survival by prognostic factors shown differences in survival forgroups ages by stages (best for younger)
2013 SIOG Poster Abstracts S39

Conclusion: in this national population-based study of 2081 womenwith lung cancer, elderly had some epidemiologic characteristics thatdiffer from younger ones. These could suggest that elderly lungcancer women had a different natural history and potentiallydifferent tumor biology, considering a different molecular event forcarcinogenesis. Although stages were similar at diagnostic; excludingsurgery, elderly were significantly undertreated. This date is similarfor all elderly lung patients. Survival was also poor for elderly andthis significant association with stage could be related to thisundertreatment. These findings deserve further analysis to evaluatecauses for undertreatment, improving understanding of this devas-tating disease, predominantly in elderly women
Disclosure of Interest: None Declared
Keywords: Epidemiology, Lung
Reference1. Wisnivesky Juan P, Halm Ethan A. Sex differences in lung cancer survival: Do
tumors behave ifferently in elderly women? J Clin Oncol 2007;25:1705–1711.
doi:10.1016/j.jgo.2013.09.038
Track 1 - Solid Tumours in the ElderlyLung cancer in eldery patientsP035Carboplatin plus gemcitabine as first-line treatment in eldelrypatients with non-small-cell lung cancer: Preliminary results of amulticenter phase ii trial by the Hellenic Oncology ResearschGroup (HORG)L. Vamvakas, A. Karampeazis*, S. Agelaki, N. Kentepozidis, A. Polyzos,A. Kotsakis, K. Kalbakis, C. Christofyllakis, E. Kontopodis, A.G. Pallis, V.Georgoulias. Hellenic Oncology Research Group (HORG), Athens, Greece
Introduction: Non-small-cell lung cancer (NSCLC) is a disease of theelderly. Platinum/gemcitabine doublet is considered an optimalchemotherapeutic regimen for NSCLC treatment; however, it has notbeen evaluated in the elderly. In a previous phase I study conducted byHORG, the maximum tolerated dose of the biweekly carboplatin/gemcitabine was determined in elderly patients with NSCLC.Objectives: This phase II study was designed in order to evaluate theefficacy and safety of carboplatin/gemcitabine combination as first-line treatment in elderly patients with advanced and metastaticNSCLC.Methods: Chemotherapy-naive patients with NSCLC, ≥70 years,non-frail according to comprehensive geriatric assessment wereenrolled. Patients received carboplatin (AUC x 2.5) and gemcitabine(1100 mg/m2) on days 1 and 15 every 4 weeks, for a maximum of sixcycles. The primary end-point of the study was overall response rate(ORR).Results: Thirty-eight patients (male/female: 92%/8%) have beenaccrued till the data cut-off date. Median age was 77 (range, 70-83)years; 29 (76.3%) patients had stage IV disease and 31 (81%) hadECOG performance status (PS) 0-1. At the time of the analysis 35patients were evaluable for response analysis and 38 for toxicity. Inan intention-to-treat analysis, 10 partial responses were recorded foran ORR of 28.6% (95% CI: 13.6 – 43.5%). After a median follow-uptime of 9.2 months, median progression-free survival was6.7 months (95% CI: 0.5-16.3) and median overall survival was12.1 months (95% CI: 7.4-16.8). Grade 3-4 neutropenia was observedin 6 (15.8%) patients, grade 3-4 thrombocytopenia in 4 (10.5%),grade 3 anaemia in 2 (5.3%) and grade 2-3 fatigue in 9 (23.7%)patients. There was no febrile neutropenia or toxic deaths observed.Conclusion: These preliminary results suggest that the biweeklyregimen of carboplatin and gemcitabine demonstrates significant
activity with manageable toxicity in selected elderly patients withadvanced and metastatic NSCLC. The study is still ongoing.
Disclosure of Interest: None Declared
Keywords: Clinical trials
doi:10.1016/j.jgo.2013.09.039
Track 1 - Solid Tumours in the ElderlyColorectal cancer in elderly patientsP036A retrospective analysis regarding the parameters, whichinfluence the administration of adjuvant chemotherapyin for elderly patients (N70 years) with stage II or III colon cancerin the daily clinical practiceN. Asimakopoulou1, P. Papakonstantinou1, J. Souglakos1, A.Karampeazis2, Z. Saridaki1, P. Koinis1, A. Matikas1, C. Nikolaou1, V.Georgoulias1, L. Vamvakas1,*. 1Department of Medical Oncology, Univer-sity General Hospital of Heraklion, Heraklion; 2Department of MedicalOncology, 417 NIMTS Veterans’ Hospital, Athens, Greece
Introduction: The administration of adjuvant chemotherapy in elderlypatients with stage III and/or “high risk” stage II colon cancer has beenproven effective and safe in a several retrospective studies. Despite that,in several studies indicates that a significant percentage of elderlypatients with colon cancer were not treated with adjuvant treatment.Objectives: To retrospectively evaluate the parameters whichinfluence the decisions for the administration of adjuvant chemo-therapy in elderly patients (aged more than 70 years) with operablestage II or III colon cancer, in the daily clinical practice.Methods: The studywas a retrospective analysis based on archive data ofthe Department of Medical Oncology at the University Hospital ofHeraklion. All available data for patients aged N70 years,with stage II or IIIcolon cancer from 1-1-2003 until 31-12-2012 were recorded andanalyzed.Results: Totally 272 patients were included in the study. Onehundred seventy-four (61%) of the patients presented stage III coloncancer and the rest 36% stage II disease. The median age was 76 yearsof age (71-89), 61% were males; in 59% of them the primary tumorwas located in the left colon. In addition, 43% of the patients hadhigh-grade tumors and 21% of them presented mucinous features.The median Charlson’s score for the entire population was 2, themedian BMI was 28.03, while 20 (7.5%) patients suffered from ageriatric syndrome. Adjuvant chemotherapy was administered in143 patients (82%) with stage III disease and in 46 (47%) patientswith stage II colon cancer. Reasons for dining of adjuvant treatmentwere: i) low risk stage II colon cancer (38 patients, 14%); ii) presenceof a geriatric syndrome (18 patients, 7%); iii) Carlson’s score N3 (21patients, 8%); iv) age more than 85 (4 patients, 2%). Oxaliplatin-fluoropyrimidines combinations were administered in 48 out of the143 (33.5%) treated patients with stage III disease and in 8 (9%) outof 46 treated patients with stage II colon cancer. Adjuvant treatmentwas completed as scheduled in 72% and 74% of patients with stage IIIand II colon cancer, respectively. Reasons for discontinuation weretoxicity (14%), disease progression (7%) or patients’ preference (7%).Treatment related death was recorded in 3 patients (1%). Treatmentdiscontinuation were more frequent in patients aged more than 80year, those with Charlson’s score N 2 and in those treated with anoxaliplatin-based regimen. After a median follow-up of 5.6 years the5-years Disease Free Survival (DFS) was 69% and 64% for patientswith stage II and III colon cancer, respectively. Likewise, 5-yearsoverall survival was 63% and 60% for stage II and III disease,respectively.
2013 SIOG Poster AbstractsS40








![[Najib Razali] Islamic REITS - prres.net REITs.pdfDo Islamic REITs Behave Differently from Conventional REITs? – Empirical Evidence from Malaysian REITs Sing Tien Foo National University](https://img.dokumen.tips/doc/110x75/5abe8db57f8b9a7e418d14eb/najib-razali-islamic-reits-prres-reitspdfdo-islamic-reits-behave-differently.jpg)