Embed Size (px)
Citation preview
Ant~rior communicatir.g artery
Posterior communic~ting artery
Internal carotid artery
Middle cerebral artery
labyrinthine artery
Anterior inferior cerebellar artery
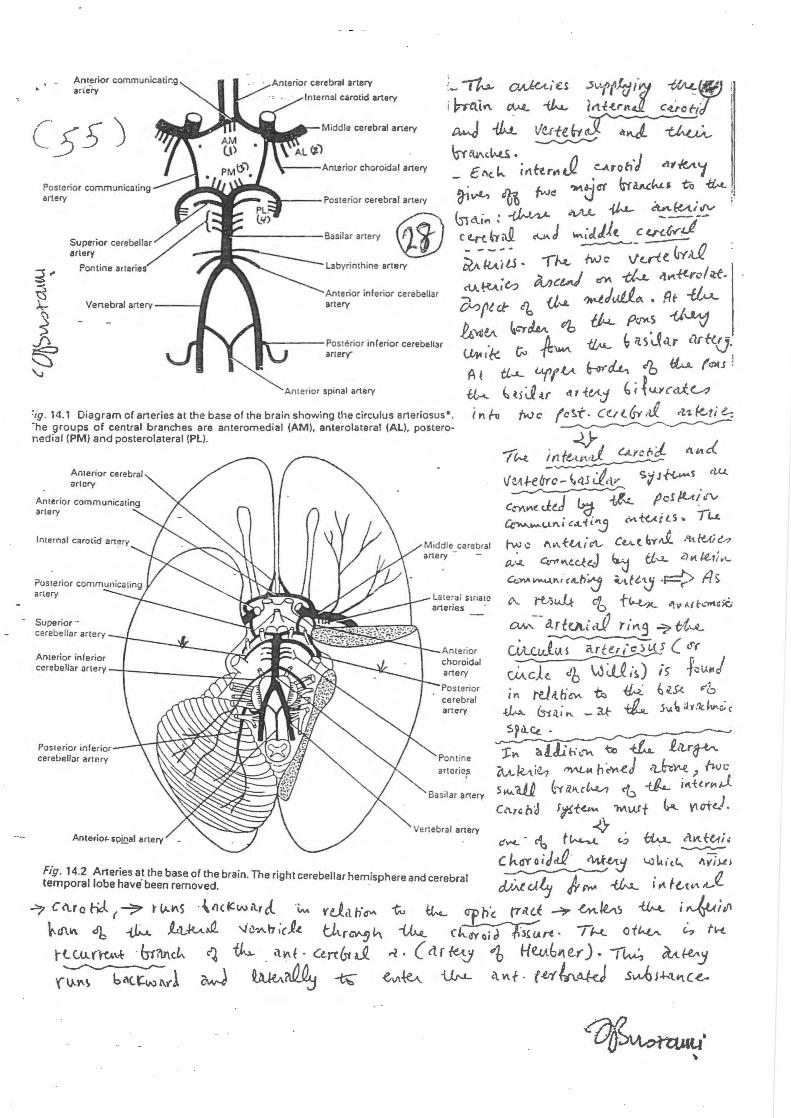
'ig. 14.1 Diagram of arteries at the base of the brain showing the circulus arteriosus•. -he groups of central branches are anteromedial (AM), anterolateral (Al l. posteronedial (PM) and posterolateral (Pl).
Anterior cerebral artery
Internal carotid art~ty
Superior cerebellar artery
Anterior inferior
cerebellar ~rtery -r-----~~t._..)j~~~,a:l
Posterior in terior cerebellar artr.ry
Antef'iol'-sp!Qal artery
Anterior choroid<ol artery
Posterior cerebral artery
Fig. 14.2 Arteries a~ the base of the brain. The right cerebellar hemisphere and cerebral temporal lobe have been removed.
~ C <\.ro Hc:l f ~ t ~~s · -\nc~w a., d. \>..dlll\ db -{).,...a_ .A...t_1_-k.A& '-I~~A b ;cJ.c.
r t. tu. rl"C.t.\.t . btfu\cL, ~ ~ (\~f-
z.wj
~L,,·tt, ~t ;l}LJ
i l't f(A~-..,v~
\
· ..
. --~--··---------·-- ··.- -..... _________ . .. -
-:· • .I J. ·... . .
IU4 Q-e cerebral a . -- -- .
1l•r1o r c •f"'ebral •·-
ftr kn' u . f''--'11 rlJ i i' .U'\JL CAr t-Lf 5 rr ; rl fu ~
--r.k ~'"M ,, i"' . c\ T k.r ,· .-j Jl.A./l. 0~ I dJ <~·~),~e. ( 5 J 4'i "'~-~J ~ ~ li~er?../. { ,....,...J .- () t't-1..(, 1 Kd'"' ~
Slt~ _ trr.(~ ,~~ ~ ~ 'Mid~~R. cc..~c <n-.J 4 • r"' q JJ/n ... rv. ~ \"'-~\~- ~.;jJ- ftUfl ( ttA.c.l...uJ ') kA,I ch cot~J-~ _.':n w:l Uv,) rc (<.,·~ -tt.'-L\.A.
lc.LO<>d 5<-<f~ ~""" -7 f<.u..ur~nf (rroo<~ db ~ .. 1· cw{rrJ... ··1 .
:-l"'J -tt~~ fc·Sf0\iC'- ?ilrts. ( t~<lttS) {~:l ~ ,uj 1 Ct~UJ].:d..t_ tru() ~r"tfl, -tk ~ 0-V'--{ · c L.,. cv c; d .J. ,\ ·
?v-,,·... ~~~ J ~~ h c{ ftu._ r:Jiclu.-, /-tf2.t~J"u ~ J.r c~ hd e..A I R ( k~"( t i J .~ cl '
Jv..IJA ~ -1;1,'\IL Hc:Jd/" ~ 1~ ... Vilr;H<~ (na'1d"" cf6 +4. Vt·r!dv~~ r "dC\A~~e......,
ftri4,· .. J. s~N '~ t<M-s ~ ~
/rrJ<AiJ lvp~ db ~;cJ(so.G ~
Pcs-l · cv..<J;vJ..
1 _:
' ~~-~ ..
... •· ........ ~· -:-·.
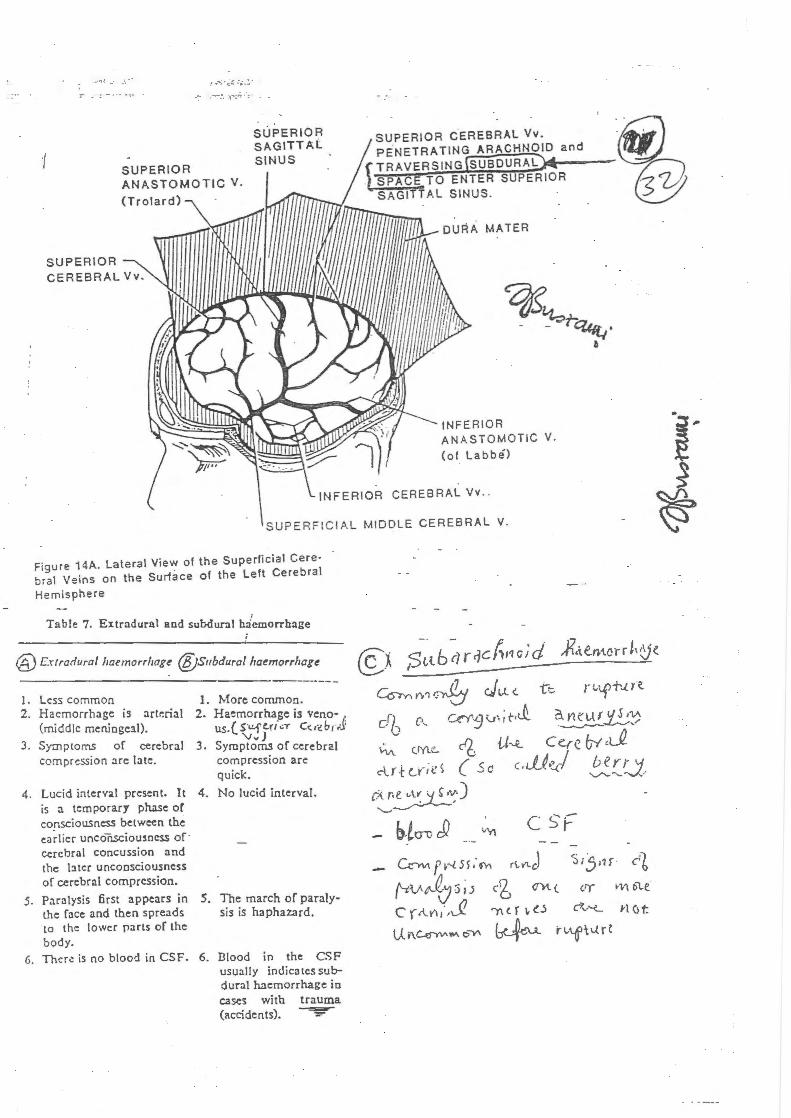
SUPERIOR ANASTOMOTIC V.
(Trolard)
SUPERIOR SAGITTAL SINUS
·~ ~~~~®
and
11/llifii///1111/U tmr'Trrrr..,.___
SUPERIOR
MATER
INFERIOR ANASTOMOTIC V.
(of Labbe)
CEREBRAL Vv . .
SUPERFICIAL MIDDLE CEREBRAL V.
Figure 14A. Lateral View of the Superficial Cere· bra! Veins on the Sunace of the Left Cerebral
Hemisphere
I
Table 7. Extradural and subdural h:iemorrh::age
@Extradural ltaemorrltag~ @subdural lra~morrlrag~
1. Less common 2. Haemorrhage is artt:rial
(middle meniogeal).
1. More common. 2. Ha~morrhage is veno
us. ( S"l.!.fe.ri~T C<r·~brJ 'Vv)
3. Symptoms of cerebral 3. Symptoms of cerebral compression are late. compression are
quick.
4. Lucid interval present. It 4. No lucid interval. is a temporary phase or consciousness between the earlier uneonscioumcss of · cerebral concussion and the J:ucr unconsciousness of cerebral compression.
s. Paralysis first appears in !.he face and then spreads to the lower parts of the body.
G. Thcr.: is no blood in CSF.
5.
6.
The march of paraly-sis is haphazard.
Dlood in the CSF usually indica tes subdural haemorrhage io cases with trauma (accidents). ~
Co-rv.. t">'l ~ J l.l <. tc
c-~ c.... u:Y 9 v• ; t-•J.. {J~ c e.r e (;y "_Q ~ (IY\.~ c'6
clr-H .... nd ( Sc '.JJ~I !:.!_!..~.J. (~~;)
C.~ ft--l5s,·~ rt l"l c} ~· . c1 - ~i.)r1f
('-tV~.J 3 1 J cg C1t'l ( or wt6le
c rAn,· ,J? ')'\ n " o c7'v'-L l'l ()t
u. f\~¥11\ c5Y' ~ r~o-tfil..{r{
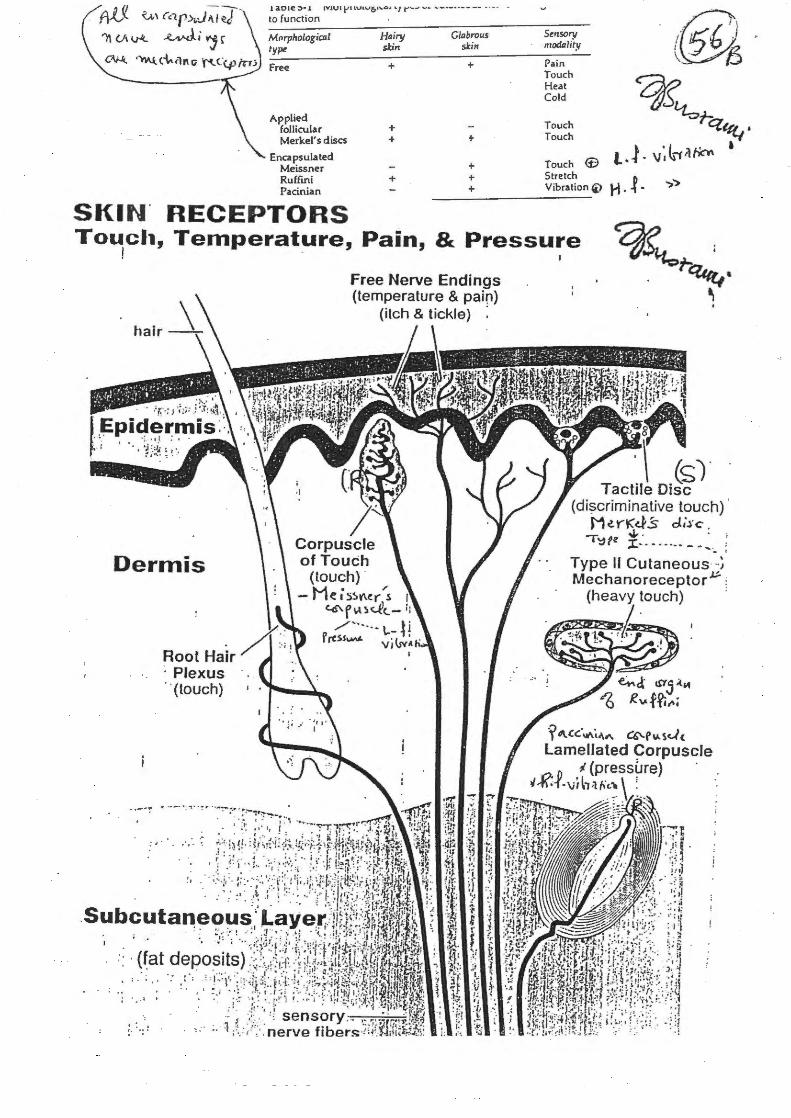
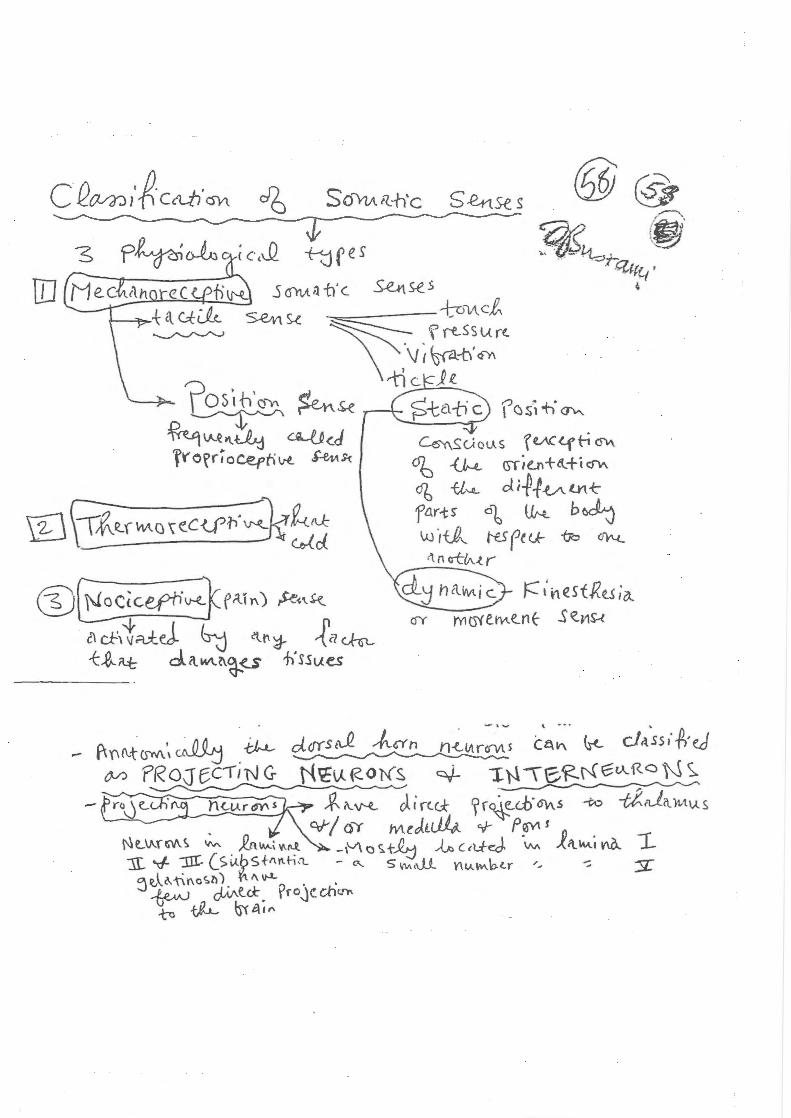
SENSORY SYSTEM I Skin Receptors @
c Receptors in the skin monitOI{3b~s of cutaneous sensation~: tactile, thermal, and pain.
--~--~------~----~--~~~ . - ~
TACTILE SENSATIONS Touch Receptors Corpuscles of Touch (Meissner's corpuscles): encapsulated nerve endings; rapidly adapting touch receptors that recognize exactly what point of the body is touched. Root Hair Plexuses: dendrites arranged in a network around hair follicles; rapidly adapting touch receptors that detect movement when hairs are disturbed. Tactile Discs (Merkel's discs I Type I Cutaneous Mechanoreceptor) : expanded nerve endings (flattened dendrites); slowly adapting touch receptors for discriminative touch. Type II Cutaneous Mechanoreceptors (end organ of Ruffini): expanded nerve endings embedded in the dermis; slowly adapting receptors that detect heavy and continuous touch.
Pressure & Vibration Receptors Lamellated Corpuscles (Pacinian corpuscles) : oval structures composed of a cOimective tissue capsule, layered like an onion, that enclose a dendrite; rapidly adapting receptors that respond to pressure and high frequency vibrations. Corpuscles of Touch (Meissner's corpuscles) : rapidly adapting receptors that respond to low frequency vibrations, as well as to pressure and touch stimuli.
Itch & Tickle Receptors Free Nerve Endings Free nerve endings are the receptors for both tickle and itch sensations.
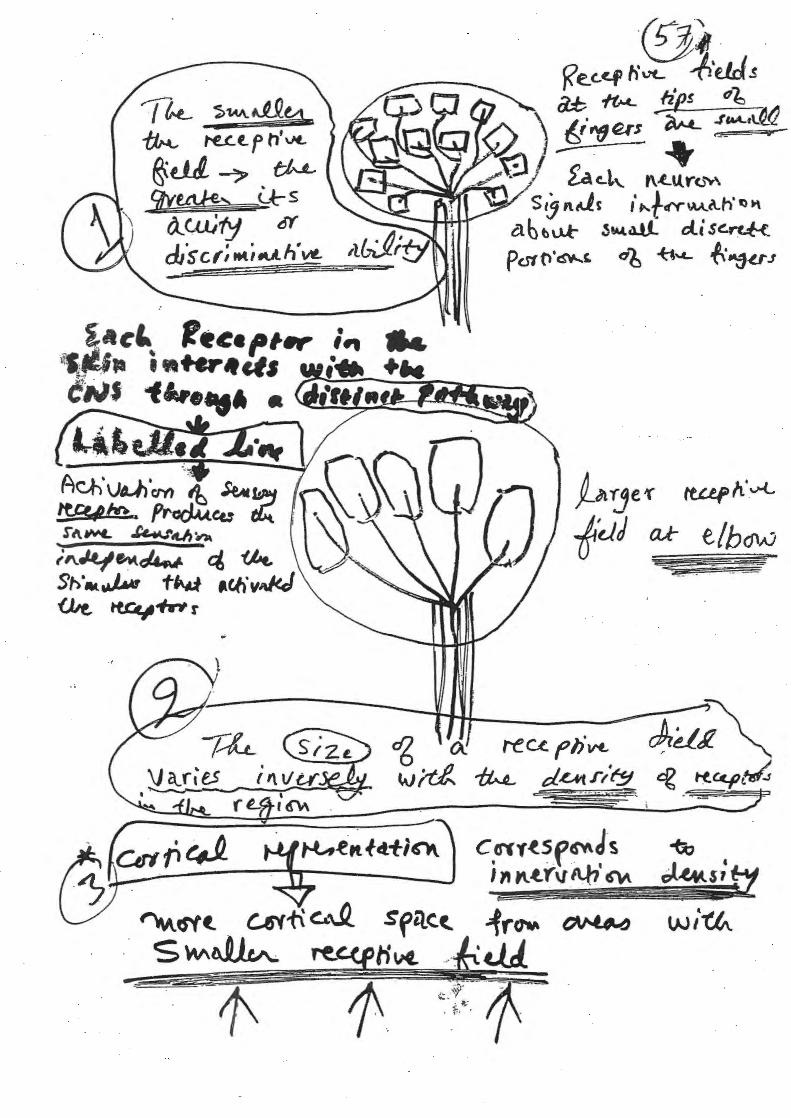
Adaptation Rapidly adapting receptors respond at the onset and removal of a stimulus with a burst of action potentials. Slowly adapting receptors respond throughout the duration of a stimulus with a sustained discharge. Receptive Fields The receptive field is the region of the skin that is monitored by a given sensory receptor. If a receptor has a small receptive field it provides precise information about the shape and texture of the object indenting the skin. These receptors are highly concentrated at the fmger tips. A large receptive field can cover a whole fmger or part of the palm. These receptors respond to vibrations, stretching of the skin, and movement of joints.
THERMAL SENSATIONS (Thermoreceptors) Free Nerve Endings The sense receptors for cold and warm are called therrnoreceptors. They
are free (naked) nerve endings. 8receptors are most sensitive to temperatures above 25 C (77 F); above 45 C pain recep
tors are stimulated (burning sensation).~receptors are most responsive to temperatures between 10 C & 20 C (50 - 68 F); below 10 C pam receptors are stimulated (freezing sensation). Both warm and cold receptors adapt rapidly; sensations disappear within minutes.
PAIN SENSATIONS (Nociceptors) Free Nerve Endings The sense receptors for pain are called nociceptors. They are free (naked)
nerve endings located between cells of the epidermis. Nociceptors respond to all types of high intensity stimuli and stimuli that cause tissue damage.
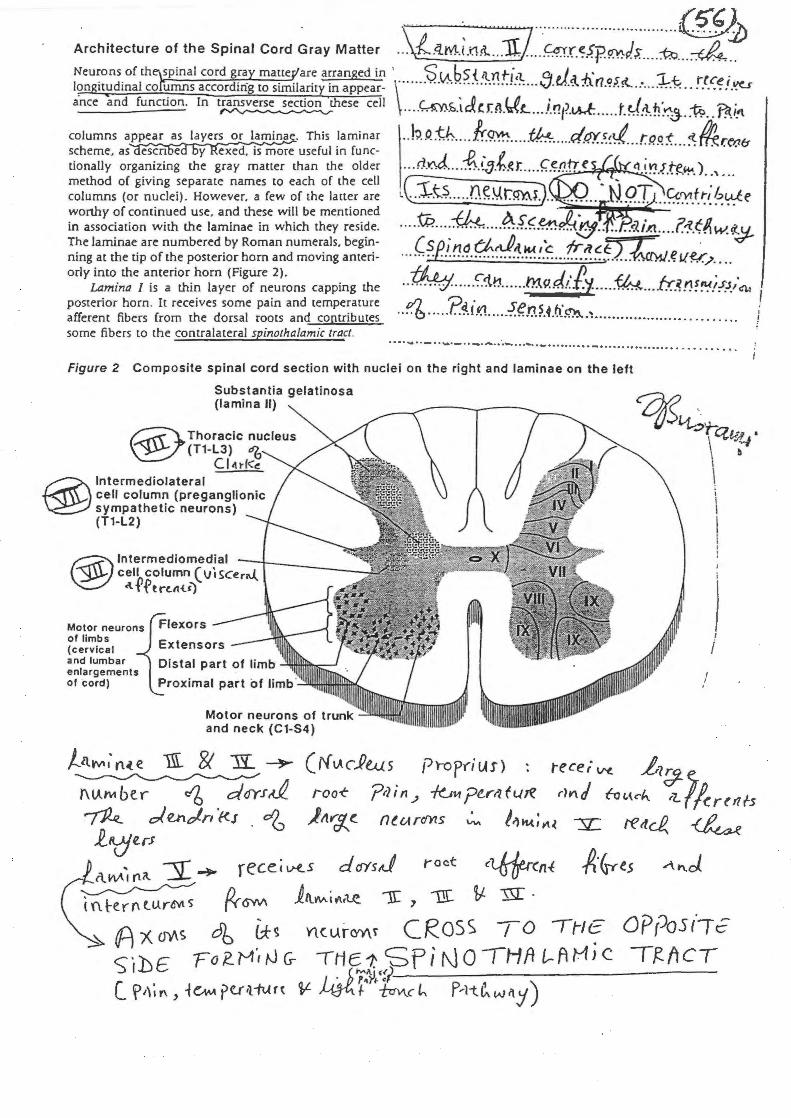
\ • • • T •n n• nnn •nn•nwn•@}) Architecture of the Spinal Cord Gray Matter ... {.4.M.t.i:15t ... JL .... ·.~.f.~fp~J$. .. .. i::Q ... ~ .. Neurons of th~spinal cord gray mauef'are arranged in · S (A.,bS' { iln t-i<t. 111 J. .l J..' - . l?ngit!ldinal cofumns according to similarity in appear- \······ ··· ······ ··· ·· ··· ········V .. ~~.:t.lr7.~J.!t. . : .... .,l.;-.~ · · !.~C.~? f.~ ance and function. In t~these cell .. .. ~h.tJcr.~.'JL .. .i.!!t?.tA.k. .... .t.~.1-.fl~~j. . i9 .. 'Rt.i!l
columns appear as layers or laminae. This laminar .. b.Rtb .... fr..~ ..... tk!:. ..... d.t!r.~~~ .. r.RP."!-: ... ~~re11& scheme, as escn e y exed, is more useful in func- o v · · · tionally organizing the gray mauer than the older ... rl.~ ... ::~.(:}:h~r. .... (.~!J.Vf t1 ~~..f.~.~.) ...... . . method of giving separate names to each of the cell ( -r . . ~ . columns (or nuclei). However, a few of the latter are L\_ .. +.-t~ ..... r.H~\.f.t~i).. ... .. ... N..9.T ... ~'!."-~~~ ~~e worthy of continued use, and these will be mentioned -r:... ~ A 0 . in association with the laminae in which they reside. .. ... VY. ................. . .. ~<!-.~pf.-;{.!!J· · .. .. ~~i,;t ... .f.1-l!tw.~
~h:g1:~;ea;i;r~f~~:~;~e~i~~ ~~:aann~u:O:i~;· ~~~:~~ ... (~fi~.q-~~~-~!.~ ... t!:.i!.~tJ. . J..:~J.~UY/ .... orly into the anterior hom (Figure 2) . -h1., , 1 c. J. /) ~I. • • .
Lamina I is a thin layer of neurons capping the .. ~.~ ....... 1J:'!. ...... t'IJ.9.~t. t.y. .... ~ ... f!:.~n~~!!..J.'41 posterior hom. It receives some pain and temperature VJ ?_q_ fVI Sen S n' ! afferent fibers from the dorsal roots and coptributes .... ~ ...................... .... .4 .... ~.~ . .... ... ...... .. . ..... .. . . . . .. f some fibers to the contralateral spinothalamic tract. ·
····-·· - · ·-· - ·· - ··' ···-···"-··-· ··· · ·· ·· · -· · · ···· · · ·· · ···· ..... . .... 0 •• •
Figure 2 Composite spinal c ord section with nuclei on the right and laminae on the left
Substantia gelatinosa (lamina II)
® Intermediolateral cell column (preganglionic sympathetic neurons) (T1-l2)
® lntermedlomedial cell column (vlsceri\..(. .tfftn.tt-tt)
Motor neurons of limb s (cervical and lumbar enlargements of cord)
' i
) I I I
Motor neurons of trunk and neck (C1-S4)
( ;'( v.cPws ['Jr-op(i us) tece; w. .1,1{?-
roo-t ?rlin"' -k._,Yipe-rrlfLJ~ riYI.d fot.~ch. r7_.1~r(tl{.5 )tt~(. nt.r.A.rdl'l.s """ !l)fiiA.;,..,J.. :;;c tettcJ!.. ~
A·&t-es
OPPost'-rc Tf?_{tCT
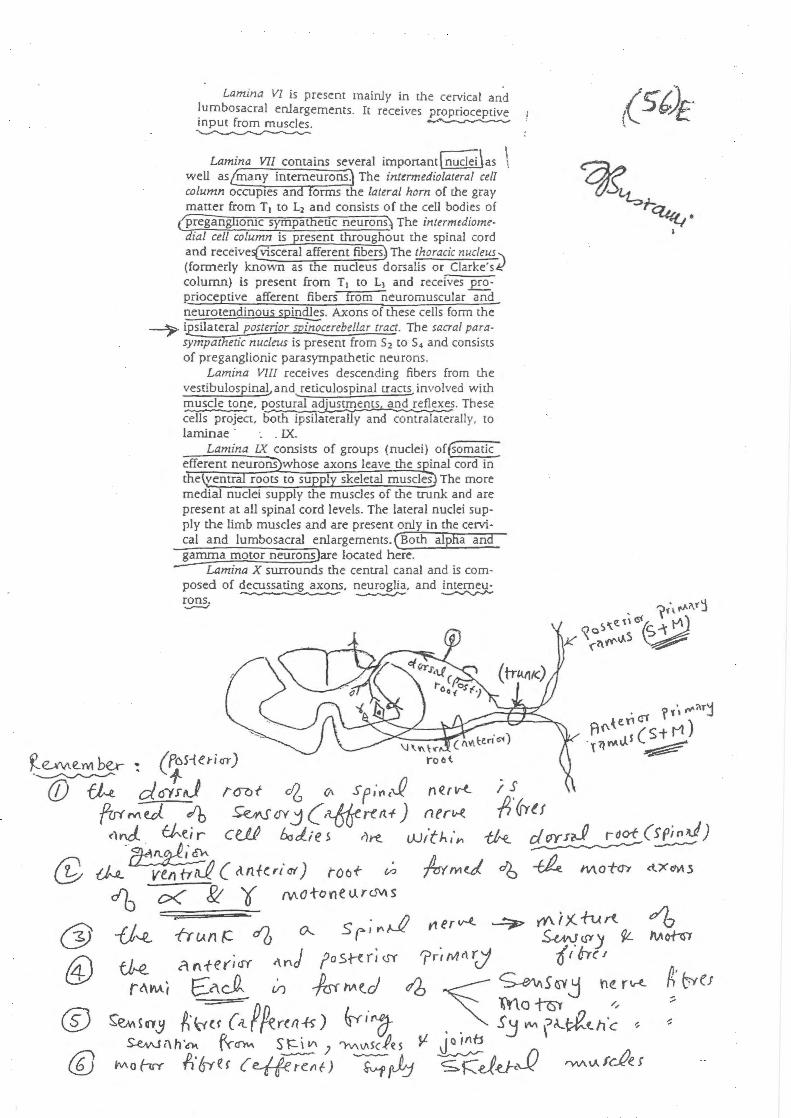
Lamina VI is present mainly in the cervical and ~umbosacral enlargements. It receives proprioceptive mput from muscles. ~ ~
Lamina VII contains several imponam[ffiid'ci\as \ well as{many intemeurons.) The intermediolateral cell rolumn occuptes and forms the lateral horn of the gray matter from T1 to L2 and consists of the cell bodies of
(Eregangiioruc sympatheoc neurons) The intermtdiomedial cell column is resent throughout the spinal cord and receive visceral afferent fibers The thoracic nucleUJ.\ (formerly known as e nucleus dorsalis or Clarke's~ column) is present from T1 to L1 and receives~Rrioceptive afferent fibers from neuromuscular and neurotendinous spindles. Axons of these cells form the
~ ~ilateral posterior mTiiOcerebellar tract. The sacral parasympathetic nucleus is present from $ 2 to $ 4 and consists of preganglionic parasympathetic neurons.
Lamina VIII receives descending fibers from the vestibulospinalJ and.._reticulospinal rractsJ involved with muscle tone, J:9,Stural adjus!!Eents, and reflexe_?. These cells project, both ipsilaterally and conrralaterally, ro laminae · . . IX.
Lamina IX consists of groups (nuclei) of (Somatic: efferent neurons whose axons leave the s inal cord in
e ven roots to su l skeletal muscles The more medial nuclei supply the muscles of the trunk and are present at all spinal cord levels. The lateral nuclei supply the limb muscles and are present only in the cervical and lumbosacral enlargements. (Both alpha and
J::arnma motor neuro~are located here. Lamina X surrounds the central canal and is com
posed of decussating axons, neuroglia, and intemeu-~ --........r- ~
rons . ....,.-./
~~ ': (7s-teri<rr) (f) ~ c/. o-yrJ iCRJ{ c,Z {}I Sf,"Yl c~ n€r K iS
frrr M e.J. efb ~ ov j (·Ysff re tt-f) n e rH. /J' (rru c1nJ CJ,...e.ir ce.J..P b,J..;es r)rt_ l)..)ftJ-. 1',._ ~ drrrn.f rdo-f(S('inJ) ~ ~-----@ -{)...R_ ven tr-;J ( <tnferit!f) roo+- (/.} ~M~ o6 ~ Mo-t-ch ct.XeM.s
db c< J!t 0 M o to n e u rc.rv, s
-()~ 11 u n t:2
tJ,.e_
/k ~~~to ~ M!Lt. f h'vt..
&jtll ~ t;b.L ~ ~s
a._Ctt,ty cr d/sc,; tM;.u.h"~
~ fjt. '( ftUI' h' v-<..
tdJ ru- e!b<JW %£ - - ---=---
c.nr~Sf~~-s 1" "-t.rvA.b ~ ~
~cNt. l:Aff\ CA.~ Sfil.<:t. ~rf1tt\ ~ S W\~ Hvt. .. --. . «i.J.
- '1' 1'
ill
m §fWt(J\<:CU'~'"'1rt~ ®G§<ce.f"liv}fAl") !<'"~
C\cf,iA±J- ~ tlt\~ ,{a~ -k -R il.:t d. aM. 2\~ u fl s.s u es
-----
Cerebral cortex
I 1\ Sen so ry radiation
(fost ·li mb ~ ,'!.(1;u.)
Thalamus '3 r:_cL al-JlA. nett'r6"'r'\
/[\ Tract in brain stem
Brain stem ~wl.. (/(ell/-. 'Y\ 4l r C'Y\
1' i ~~~j~~) ~ ~ Tract in spinal cord
I Spinal ~~ t\J crrJ.~..., cord '1'\ U.tr€n
L.._ _____ __. (. "'-nH.foAA~ •
I '=-:JH~) Central sensory nerve (dorsal nerve root}
Dorsal root 15-t (j( dtt ganglion 'Y\t(.(ron
1'. Peripheral sensory I nerve
Recepto' I (b)
LUMBAR '\
ill ·.• •. . ;,.., i ...
., ....
Thalamic radiation lS'~ffi!j ; raJi.~ tic1 ~ott· ·.
. (i rv.b/11\f· 0\f~~ · Medial
lemniscus
Vantralaplno·
'
thalamic tract
r LatarallplnO· ~ thalamictract
A•\~ ~o.l .t.~ e. rtj ~";>tfMI'
Thalamua (apecific aenaory relay nucloil
\}tV\-trcbiU l\1. ~rlc.~tvr>l)
Nucleus / gracilisand
cuneatus
Fasciculus • gracilis and . cuneatua (doraal columns)
Dorsal root ganglion '
/call
>___,j.__ Touch
)--..IT--Touch ) 7 Pain, 1 -cold, I. .
Sensory nerve _warmth 1 \
-itch o1 fic~A ~ . .MIDLINE - s ClC~.td Sert fttll'b.' ~
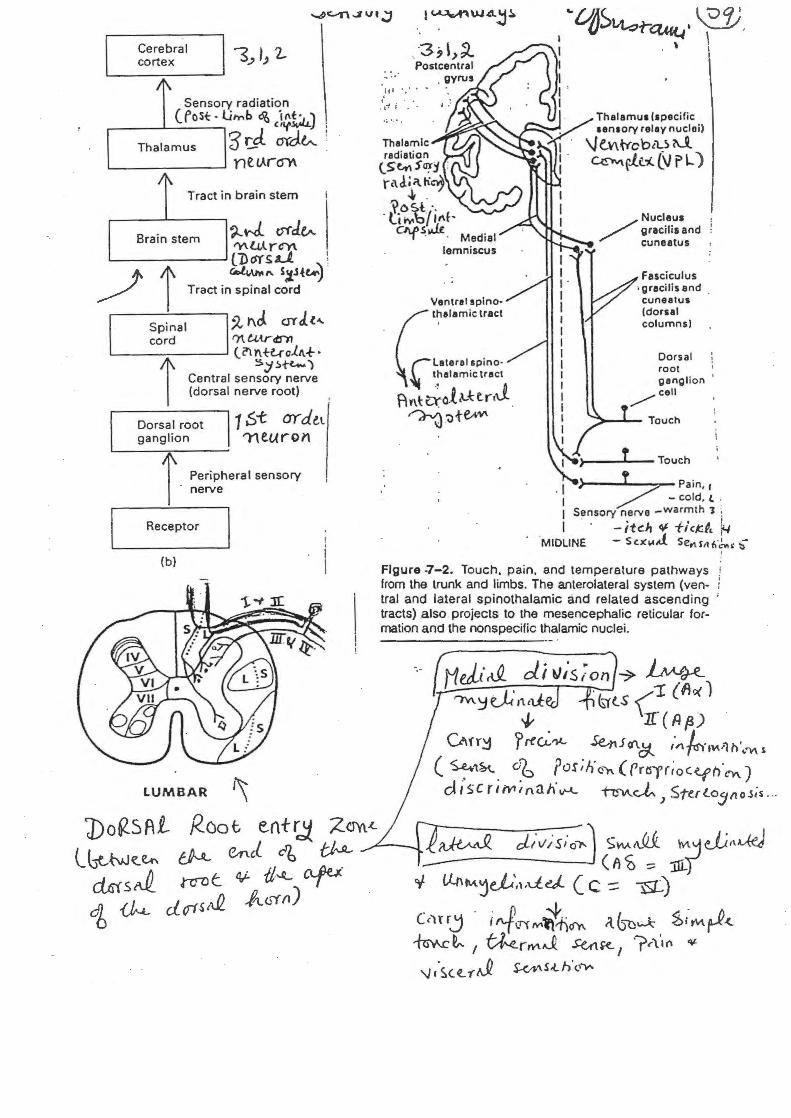
Figure -7-2. Touch, pain, and temperature pathways from the trunk and limbs. The anterolateral system (ventral and lateral spinothalamic and related ascending ' tracts) .also projects to the mesencephalic reticular formation and the nonspecific thalamic nuclei.
J1Jj&_ d.i tJ;s,~on ~ ~ f")y\_~~·tt~tl: . (srtS ('! (~o<)
I
-} 1f(Af3)
Owr~ ? rtU:.'lt- Se-nJ f/\.C:t. ,·~,~-, ... ,_;1 n'._'\1\ s.
( ~'\~ . ~b fos;Hcr. (Pr0'r;oC{jh.cn) d 1 sc r li'Y1t nail'~ "h:!V\.vi-) Sterto511 o5:s . ..
J)o62.5AL lbt-M~~ dtsls~ cfb~
Root e.nt tJ :ZCYYt.<.
~ emd db tJ~ ~- cllvis;~) ~w-1\.Ui M'-jJi~\~ ------J_ (A<; :::: :ilL)
nrn t ~ u~ CLfU d or s ,...Q 1/l.. <rr {l)
Y (,LnMje_L',,,deJ. ( C :::; -g_)
(c)Hj · i ":{cr"f IV'~cf't\ ({~~ ~iMrJz ~~ t ~rrVlJ. S-utt<-, ?~,··(\ ¥
'J 1 '$.(~ 'f Af2 S-</1,'\S.t. h'<.,.,..
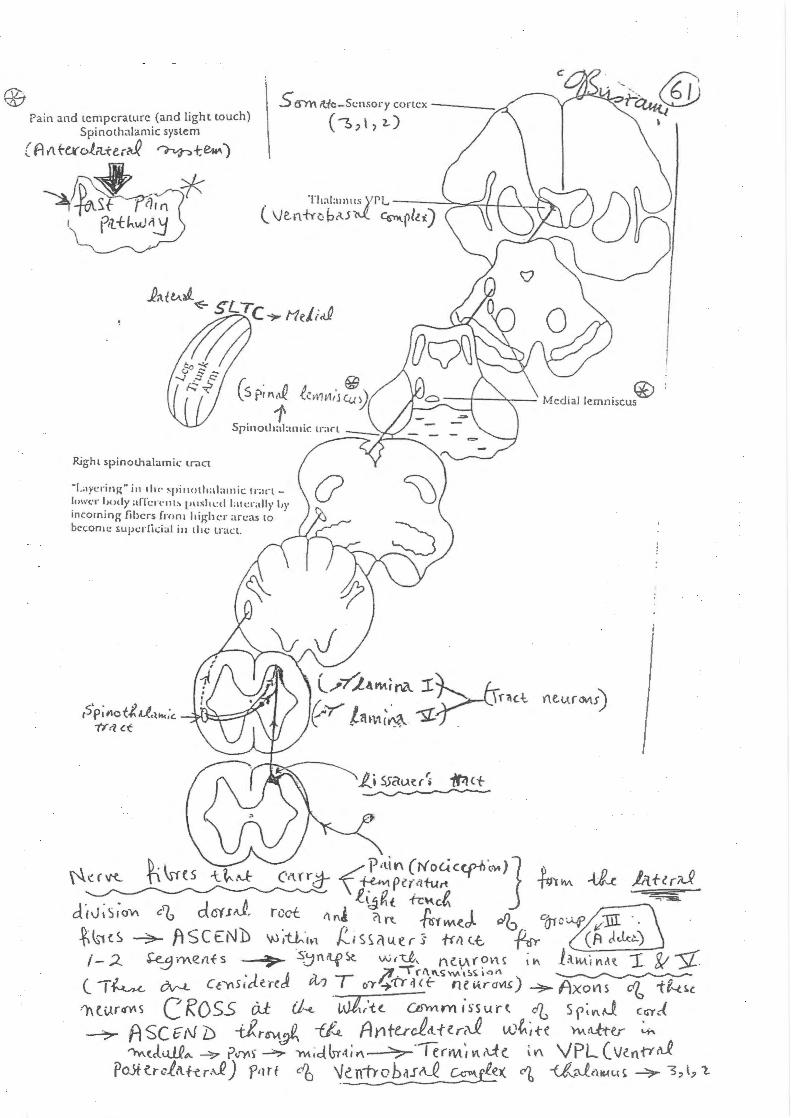
5 IJYl'\ rt-ie-S<:nsory cortex----Pain and temperature (and light touch)
Spinothalamic system
(A r'\ texol.rt.te.r~ ~+.~)
~~"·* ' ptt-t~w~
Right spinothalamic.: tract
-Layering-" in tlu· ~pinotl1alamic 1r;1nl<>h't.:l' body aiTcrnll' pushl:d l.ltc.:r;dl}' '"' incoming fibers fmm high<·r areas to · become supc.:l'lic.:ial iu th<: u·acL.
(~,\,1-)
I
SpinothalamicJ · tract
So":'atic ~ area/ /1;inal
~'"~o•d _,..--_ Viscus
Convergence
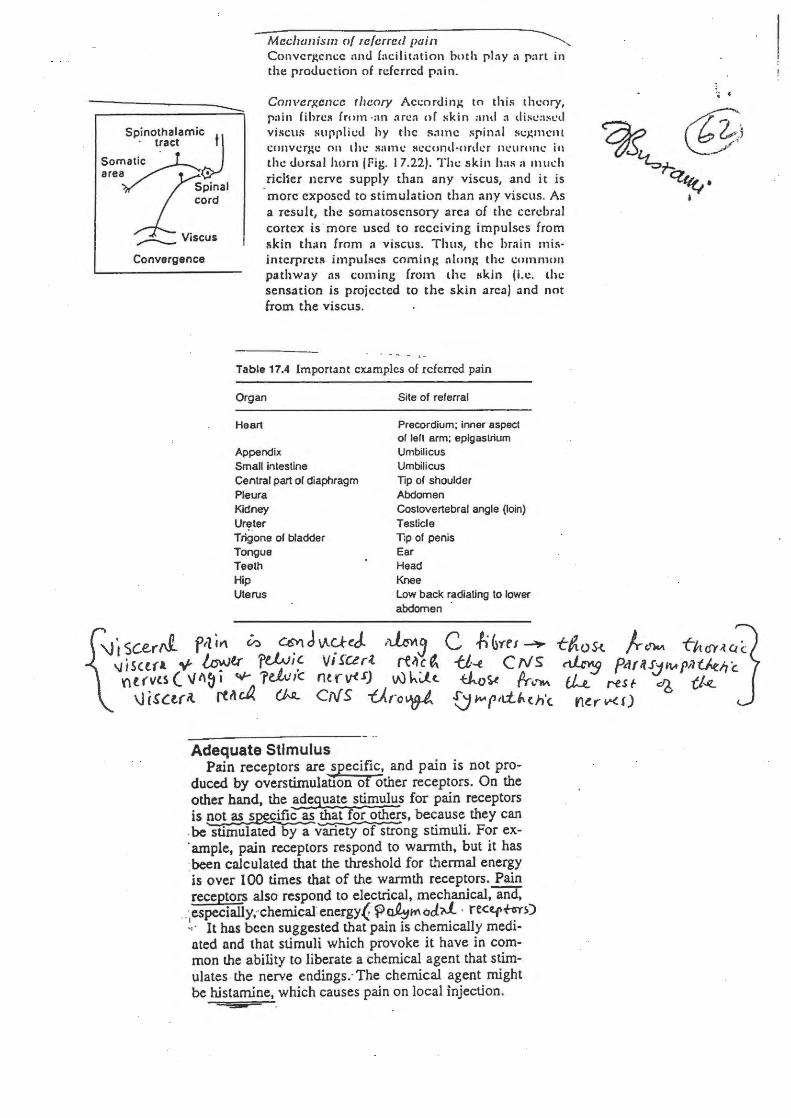
Mcclwuism of rc/crrccl pain ~--Convcr~cncc and facilitation both pin y :1 part in the production of referred p ai n.
Converxcncc theory Accordin~ to this theory, pain fibres from ·an arcn o( skin and :1 disc;ISL'd viscus supplicd hy the same spinnl sc).:mcnt conver)4e on the :wmc sccond-onlcr neurone in the dorsal horn I fig. 17.22). The skin has :1 much richer nerve supply than any viscus, and it is more exposed to stimulation than any viscus. As a result, the somatosensory area of the cerebral cortex is · more used to receiving impulses from skin th<~n from :1 viscus. Thus, the hmin mis· interprets impulses coming nlon~ thc common pathway as coming from the 11kin ji.e. the sensation is projected to the skin :1rea) and not from the viscus.
Table 17.4 Important eXAmples of referred pain
Organ
Heart
Appendix Small intestine Central part ol diaphragm Pleura Kidney Ur~_ter Trigone of bladder Tongue Teeth Hip Uterus
Site of referral
Precordium; inner aspect of lefl arm; epigastrium Umbilicus Umbilicus Tip of shoulder Abdomen Costovertebral angle (loin) Testicle T;p of penis Ear Head Knee Low back radiating to lower abdomen ·
Adequate Stimulus Pain receptors are specific, and pain is not pro
duced by overstirnulation of other receptors. On the other hand, the adeguate stimulus for pain receptors is pot as s~ific as that fot others, because they can
. be stimulated by a variety of strong stimuli. For ex-
. ample, pain receptors respond to warmth, but it has ·been calculated that the threshold for thermal energy ·is over 100 times that of the wannth receptors. Pain receptors also respond to electrical, mechanical, and,
.:especially,-·chemicafenergy( ~~Mod.i>L · re<trffi~) ~, · It has been suggested that pain is chemically mediated nnd that stimuli which provoke it have in common the ability to liberate a chemical agent that stimulates . the nerve endings.· The chemical agent might be histamine, which causes pain on local injection.
., .
VISCERAL PAIN
There are three fundamental types of visceral pai:.1: 1 pure visceral pain.:. felt in the region of the affected organ, 2 visceral referred pain, projected into the somatic territory of the corresponCting spinal nerves, 3 yiscerosomatic pain, caused by the spread of visceral disease to somatic structures.(..~ 'P .\A;~
ft_~ ,C. Cc1"o'\ fT <l ~· d'P. t:f't ~ "~ i f"Cfl\ t.U ...
,-;;:~=~~,;.,· ,_sl:) .{ ~ ~ "" loJ.L. • • • Pure v1scera am ~~·ats ~ ~,_,; .. ,-ry This is characteristically ~ and d~e_p;seatesi and often accompanied by autonomic respol.!§.eS (sweating or nausea). It is experience_4_~s- th! initial _pain in int~tinal, bili:ry or u_!!teric.{o_!:>..s_tr~s~o]', or when the capsule of a solid organ (liver, kidney or pancreas) is stretched by underlying disease.
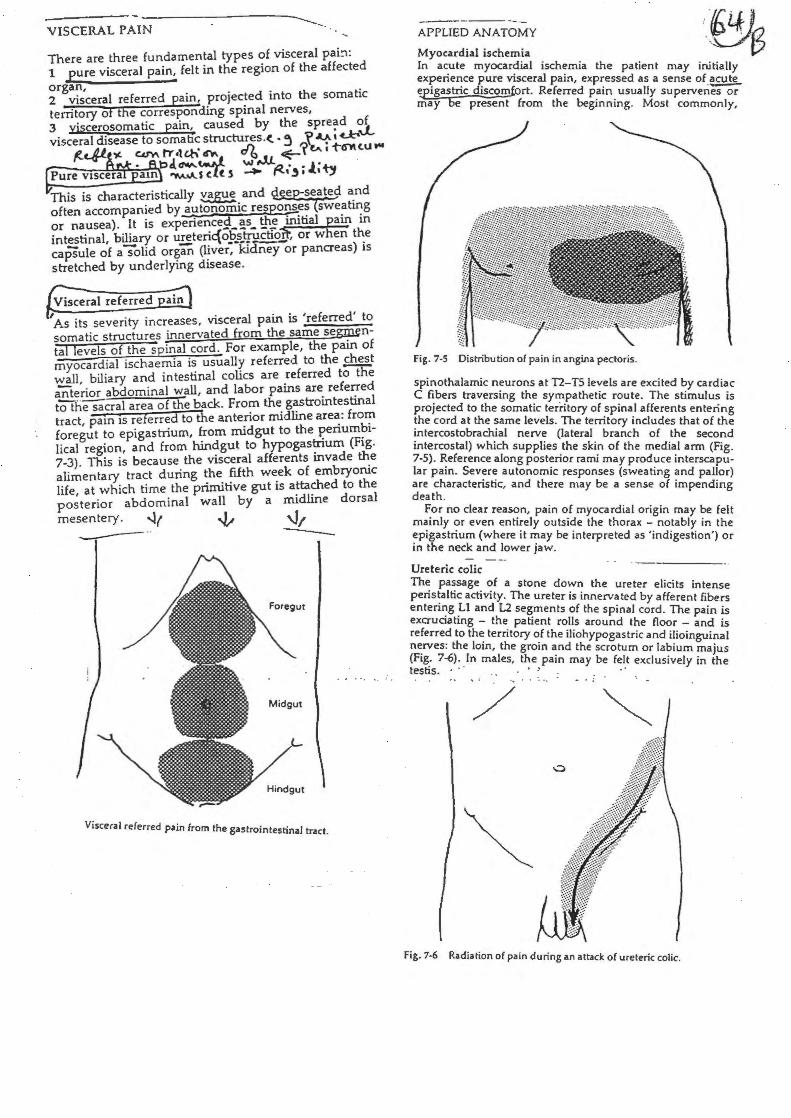
I As its severity increases, visceral pain is 'referred' to somatic structures innervated from the same se~ntal levels of the spinal cord. For example, the pain of myocardial ischaemia is usually referred to the chest ~II, biliary and intestinal colics are referred tO"tile anterior abdominal wall, and labor pains are referred tOThesacral area of the back. From the gastrointestinal tract, pain IS referred to the anterior midline area: from foregut to epigastrium, from midgut to the periumbilical region, and from hindgut to hypogastrium (Fig. 7-3). This is because the visceral afferents invade the alimentary tract during the fifth week of embryonic life, at which time the primitive gut is attached to the posterior abdominal wall by a midline dorsal mesentery. -.lr ~ \.}/ ----·· --
Visceral referred pain from the gastrointestinal tract.
APPUED ANATOMY ... -~ Lf , Myocardial ischemia ,0'~ In a~ute myocardial ischemia the patient may initially ex~ne~ce J:lure visceral pain, expressed as a sense of acute ~astric discom.fort. Referred pain usually superveriesc>; may be present from the beginning. Most commonly,
Fig. 7-5 Distribution of pain in angina pectoris.
spinothalamic n~urons at T2-T5levels are excited by cardiac C ~bers traversmg th~ syl"!'pathetic route. The stimulus is prOJected to the somatic terntory of spinal afferents entering !he cord at the same levels. The territory includes that of the ~ntercostobrach_ial nerve (lateral branch of the second mtercostal) wh1ch supplies the skin of the medial arm (Fi . 7-5). ~eference along posterior rami may produce interscap~lar pam. Sev~r~ autonomic responses (sweating and pallor) are charactenshc, and there may be a sense of impending death.
~or no clear reason, pain of myocardial origin may be felt m~mly ?r even entirely outside the thorax - notably in the ~p1gastnum (where it may be interpreted as 'indigestion') or tn the neck and lower jaw.
Ureteric colic Th~ pa~sage_ ~f a stone down the ureter elicits intense pe~s~alti~ actiVIty. The ureter is innervated by afferent fibers en en~g. 1 and L2 segments of the spinal cord. The pain is excruoating - the_ patient rolls around the floor - and ·s referred to th~ tern tory of the iliohypogastric and ilioingui~l n~rves: the !om, the groin and the scrotum or labium ma·us (Flg: 7~) : _In males, t~e. pain may be felt exclusively in lhe testis. . . .. - . :
/
Fig. 7-6 Radiation of pain during an a ttack of ureteric colic.
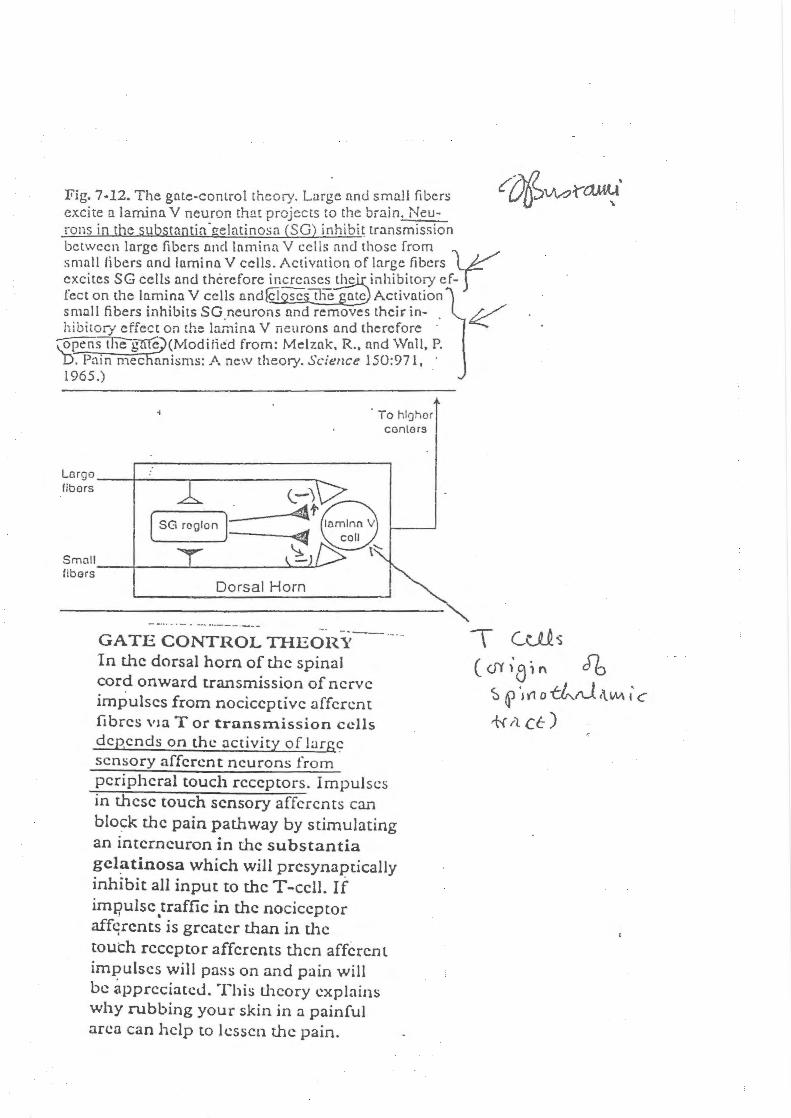
Fig. 7-12. The gate-control theory. Lurgc nntl small fibers excite a lamina V neuron that projects to the brain. Neurons in the substnntia-gelatino.sn (SG) inhibi~ transmission between lnrgc fibers nnd lnminn V cells nnd those from small fibers nnd lamina V cells. Activation of large fibers L~ excites SG cells and therefore increases the· inhibitory ef- j feet on the lamina V cells and~sc:tl1e nte Activation small fibers inhibits SG neurons nnd removes their in- K hibitOrf effect on the irunina V neurons and therefore · ~Sillegme (Modified from: Melznk, R., nnd Wall, P. D. Pntn mec anisms: A new theory. Science 150:971, · 1965.) .
Dorsal Horn
To hlnhor cantors
GATE CONTROL THEORY--1n the dorsal horn of the spinal cord onward transmission of nerve impulses from nociceptive afferent fibres Vla Tor transmission cells depends on the activity of large; sensory afferent neurons from peripheral touch receptors. Impulses in these touch sensory afferents can blo~k the pain pathway by stimulating an interneuron in the substantia gcl~tinosa which will presynaptically inhibit all input to the T -cell. If impulse traffic in the nociceptor
I •
affqrcnts is greater than in the touch receptor affercnts then afferent impulses will pass on and pain will be appreciated. This theory explains why rubbing your skin in a painful arcn can help to lessen the pain.
\ Culs
c d)' 'a;" Jb ~ ~ ·~(1 o ~rJ •\Vv\ I c
+<it ct)
t t -STT STT--
-Nc(P~ !I'{ ( -::. lo c..tt > ce r ulu.l s ""' r OV\ s
N R. M = t( t,A. ,.Q<M ~ f2_ «_fit t. "h'\~"\c.,(.S (('ems)
----- -CST
. tt~~ t'\l\ -sf, ~ T- ce.il s ;: «<tj fr\ · cb Sfi Ill~ ·(t, .l.b.~~,;i c.
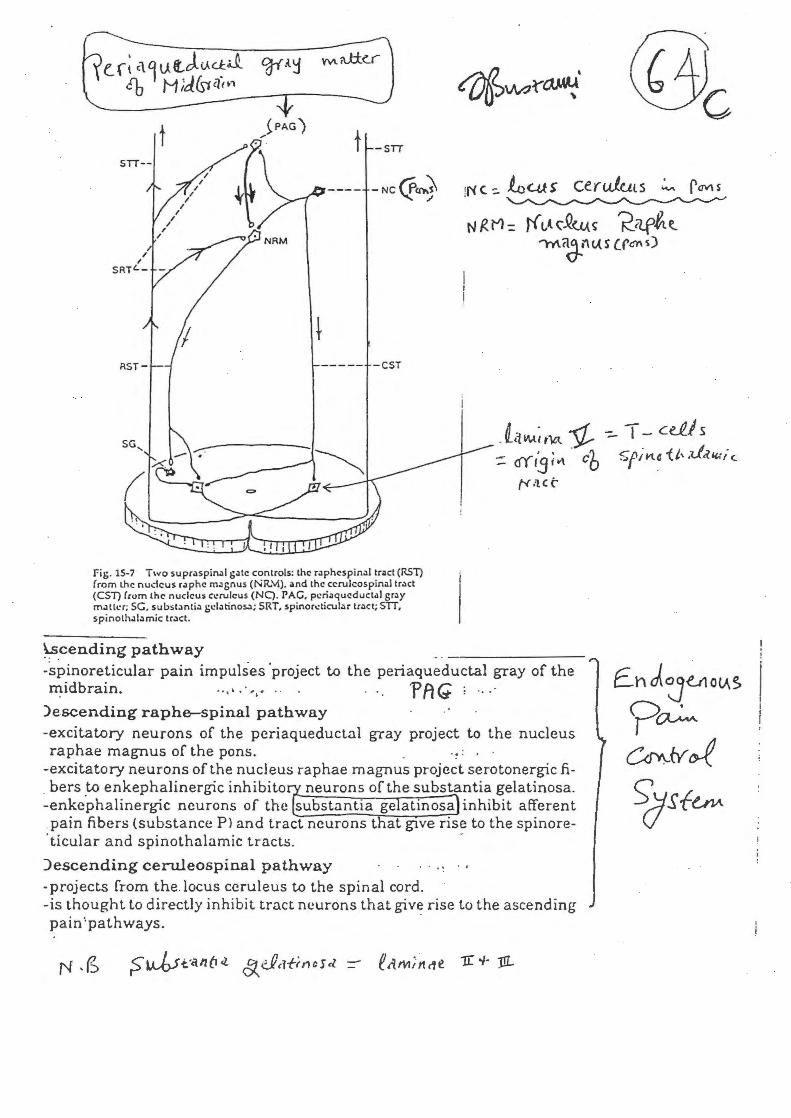
Fig. 15-7 Two supraspinal g.:~te controls: the r.:~phespinaltnct (RST) from the nudcus raphe m.:~gnus (NR.'-'1). 01nd the ccrulcospinaltract (CST) from the nucleus c.:rulcus (NQ. PAC, pcri;~qucductal gr.:~y maHer; SG. subst.:~ntia gd.1tinos..:l; SRT, spinor.:ticular tract; SIT, spinoth.:~l.:~mic tr.:~ct .
~.cending pathway
ty.'lCC:
-spinoreticular pain impulses 'project to the periaqueductal gray of the midbrain. . .... , , . . . -p fl G ; ... ·
)escending raphe-spinal pathway -excitatory neurons of the pcriaqueductal gray project to the nucleus raphae magnus of the pons. .
-excitatory neurons of the nucleus raphae magnus project serotonergic fi bers to enkephalinergic inhibito neurons of the substantia gelatinosa.
-enke.phalinergic neurons of the substantia ge atinosa inhibit afferent pain fibers (substance P> and tract neurons t at glVe rise to the spinore-
. ticular and spinothalamic tracts. -
)escending ceruleospinal pathway . · . . -projects from the locus ccruleus to the spinal cord. -is thought to directly inhibit tract neurons that give rise to the ascending pain'pathways. ·
f..hJJUto~~ ?~ ~/:{~
~Sfe_,v.
s <:n'Y\ '!(f-ie_ Sehsoty cortex t'3,t, 't)
Thalamus / (ventrobasal nuclear complex)
\IPL
Sensory I 1
decussation /:
Gracile nucleus \
I I
Medial lemniscus
Internal arcuate fibres
Cuneate nucleus -Gracile and cuneate tracts
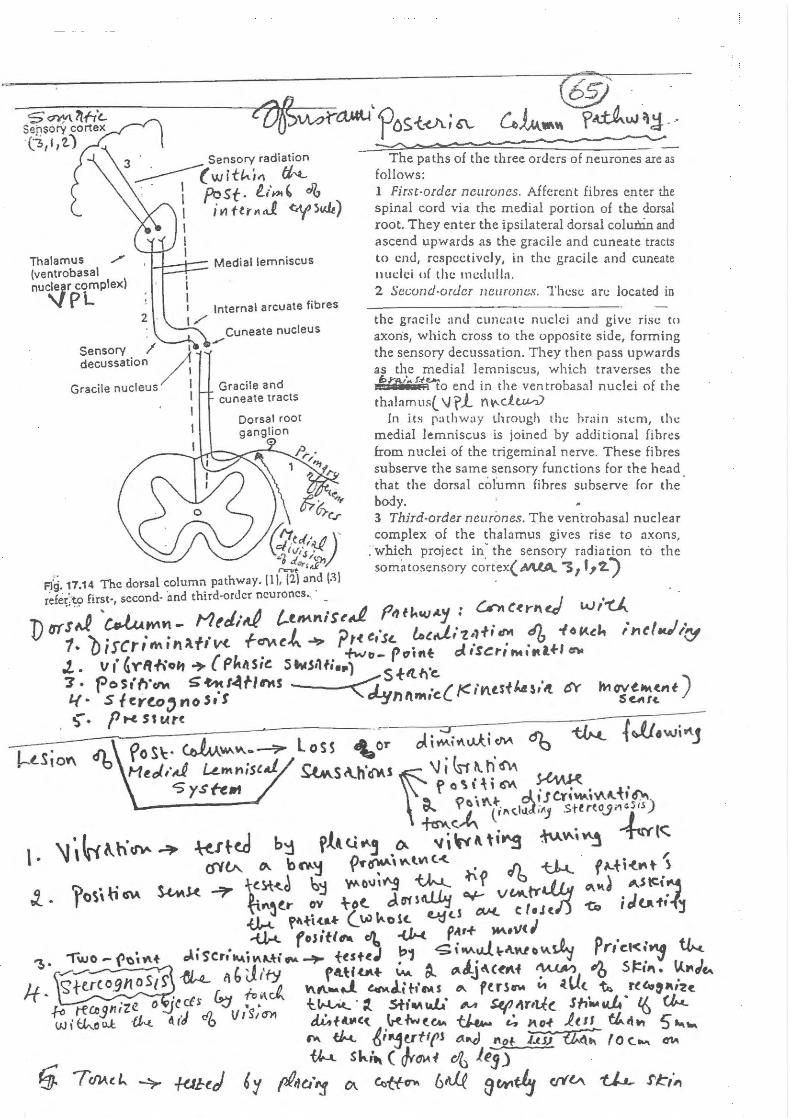
The paths of the three orders of neurones are as follows: 1 First-order neuruncs. Afferent fibres enter the spinal cord via the medial portion of the dorsal root. They enter the ipsilateral dorsal colunln. and ascend upwards as the gracile and cuneate tracts to end, respectively, in the gracile and cuneate nudci of the medulla. 2 Sec.:ond-ordcr 11eurones. Tht:sc ar<.: located in
the gracile and cun<.:;llc nuclei ;mu give rise to axons, which cross to the opposite side, forming the sensory decussation. They then poss upwords as the medial lemniscus, which traverses the E>r.t!l~ uu... d · I h I l · f I 1!1 :: to en 111 t 1e ventra as::1 nuc et o t 1e
thalamus(_ \Jrl m~ .. d.u.v.V In its pathway through thc brain stem, the
medial lemniscus is joined by additional fihres from nuclei of the trigeminal nerve. These fibres subserve the same sensory functions for the head that the dorsal cofumn fihres subserve for the body. 3 Third-order neuri::mes. The ventrohasal nuclear complex of the thalamus gives rise to axons,
. which project in· the sensory radiation to the somatosensory co.rtex( M.tA.. '3 1 f? ~)
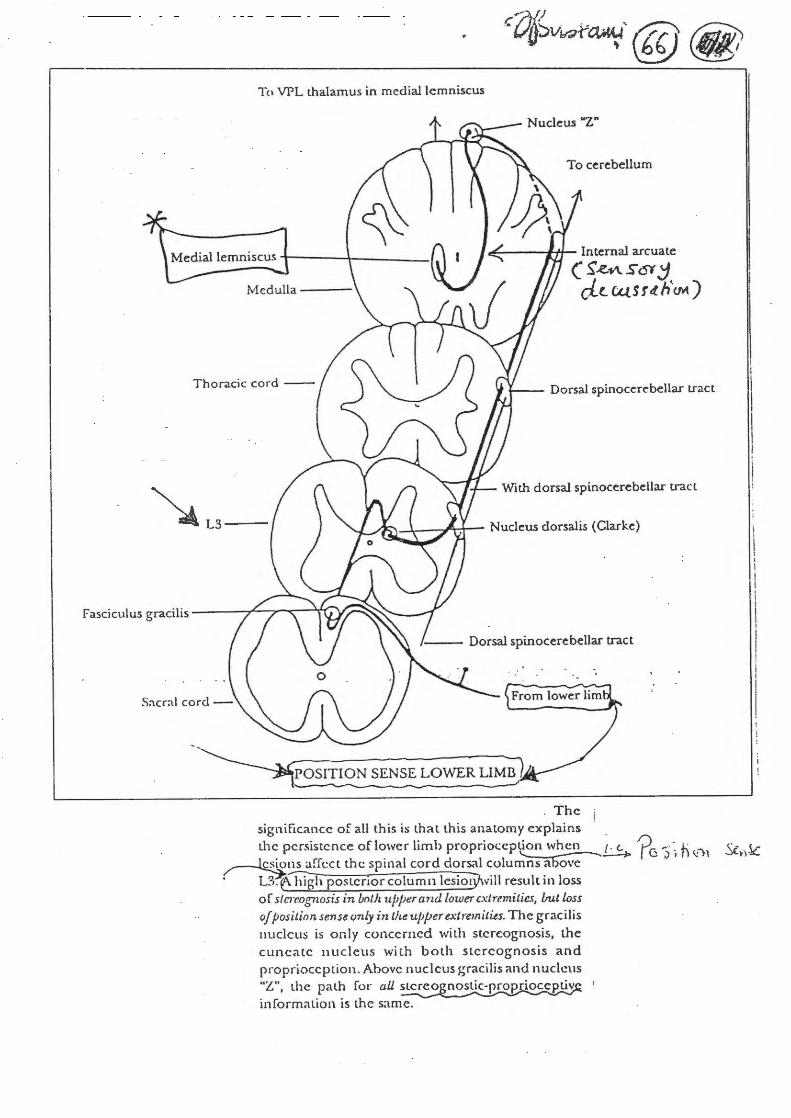
To VPL thalamus in medial lemniscus
To cerebellum
"'----*+1-- Internal arcuate
( S'..e.n s <--;y ~ cl..(_ t4S r tt. HeM )
Dorsal spinocerebellar tract
~L3-With dorsal spinocerebellar tract
POSITION SENSE LOWER LIMB
. The i significance of all this is that this anatomy explains · the persistence of lower limb proprioception when (. (. 0r. ~ · · . .h: "' c. ( r ....______.....~ r ~ ;) , 11 ~ ,, ..){.~,.l(_
~~cct the spinal cord dors~l columns above · L3.e- high postcnor column lesiotywill result in loss
of slcrr.ognosis in both ujJjJer and lower extremities, /.rut loss
of position sense only in the upper extremities. The gracilis nucleus is only concerned with stereognosis, the cuneate nucleus with both stereognosis and proprioception. Above nucleus gracilis and nucleus "Z", the path for all stereo nostic-proprioceptiv information is the same.
FI\SC: IClJ L IJS C UI'!EATUS
FASCICULUS GRACILIS
X CERVICAL
\
rw
LUMBAR ) 1 . ... -·
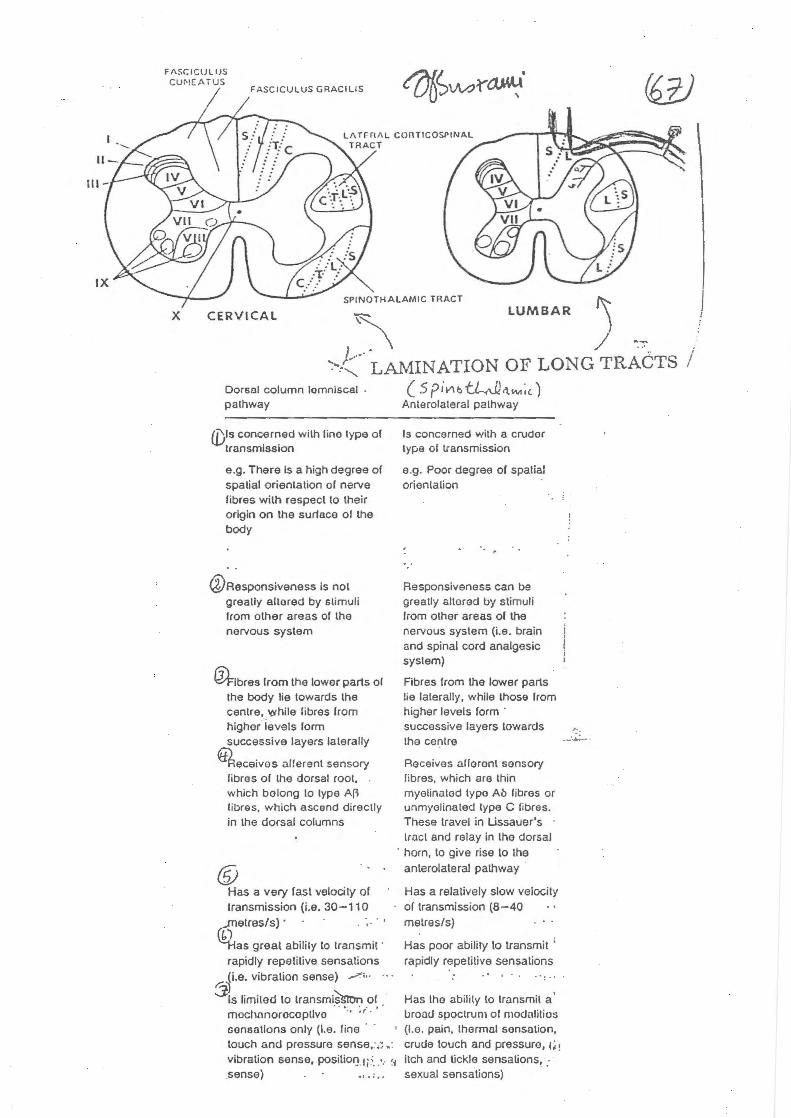
>:-....... LAMINATION OF / -:-:-.-..
LONG TRACTS I Dorsal column lomnlscal palhway
{Dis concerned wilh l ine type of transmission
e .g. There Is a high degree of spalial orientation of nerve fibres with respect to their origin on the surface of the body
@Responsiveness is not greatly altored by slimuli from other areas of the nervous system
~!bras from the lower parts of the body lie towards the cenlre, while fibres from higher levels form successive layers lalerally
~eceivos al!erenl sensory fibres of the dorsal root, . which bolong lo type A() Iibras. which ascend direc lly in the dorsal columns
® Has a very fast velocity of transmission (i.e. 30-110
cQ;etres/s) · · . · •. · •
) as great ability to lransmit ·
rapidly repetitive sensations (i.e. vibration sense) .-; · · ·
r::~ 3 ts limited to transmi~ of "I • • I
mochonorocoptlvo • "
( 5 pivu:.tl-.-Jl.'l.IM;<.) Anterolateral palhway
Is concerned wilh a cruder type of transmission
e.g. Poor degree of spatial orientalion
Responsiveness can be greatly sllorad by stimuli from olher areas of the nervous system (i.e. brain and spinal cord analgesic syslem)
Fibres from the lower parts lie laterally, while those from higher levels form · successive layers towards lhe cenlre
Receives aileron\ sensory fibres, which are thin myelinaled typo Ab libros or unmyelinated type C fibres. These travel in Ussauer's lracl and relay in the dorsal
· horn, to give rise to the anterolateral pathway
Has a relatively slow velocity or transmission (8-40 metres/s)
Has poor ability to transmit ' rapidly repetitive sensations
Has the ability to transmit a ' uroocJ spoclrum of modalilios
sensations only (I.e. line · · touch and pressure sense;.;.·
• (I.e. pain , thermal sonsolion, crude touch and pressure, 1i !
vibration sense, positiol} fi~. : .. !1 itch and tickle sensations, : sense) •• . . . . sexual sensations)
\
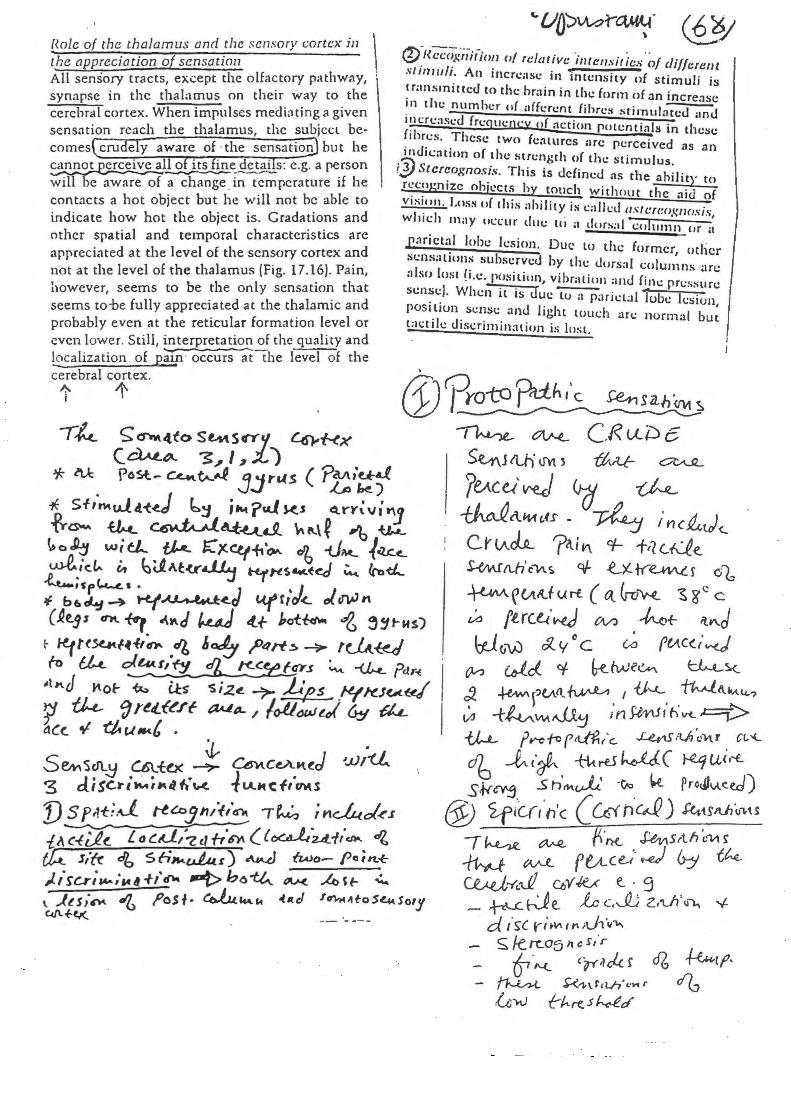
Hole of the thalamus and the s ensory cortex in \
1 the appreciation of sensation All sensory tracts, except the olfactory pathway, synapse in the thalamus on their way to the cerebral cortex. When impulses mediating a given sensation reach the thalamus, the subjccl becomes cru e y aware of · the sensation but he ~~ o its ine detai s: e.g. a person will T)e aware of a cwhange~ in7c~pcrature if he . contacts a hot object but he will not he able to indicate how hot the object is. Gradations and other spatial and temporal characteristics are appreciated at the level of the sensory cortex and not at the level of the thalamus !Fig. 17.16). Pain, however, seems to be the only sensation that seems to-be fully appreciated at the thalamic and probably even at the reticular format ion level or even lower. Still, interpretation of the quality and !9calization of p;u.n · occurs ;t"the level of the cerebral cortex.
t 1'
j. . S ~sen..~ Ult.O<. ---'>- C6vt. c eA~ t.d ~JJ 1ti... 3 d. i sc,. i ~;"If 1.· \rt. lu..,. c i-,-CM. s
f)sp~t;.J t-tc.o1"'i/tnt ~~ in~ol<.r ill c-l~!. L o~d./7.c1 ftG'A ( {~'u_-f(chO. ~
t};..t_ J/(r db Sfi~~Au..lu.~) ~ fwo~ pc;n.~ J..isc..r;...,.;~«f+l'~ -t>h6~ ov.< Asf- .,:...
@Y (f?~t(;;(;c~·iiit-io~J of relative .. intt:nsit fcs ~/different stmJuh: An lltcrc;tsc in intensity of stimuli is ~ r;lllsrmttcd ro the brain in the form of an incre:~sc ~~~ the number of :rffcrent fihre~ stimulated and J~tcrcascd frequency of :lction potentials in these frhres. These twn features :trc percet'ved · .•. . as an
. tnu,'cattnn of the strength of the stimulus. !J) $tcrcoxnosis. This is defined as the ahili . rccn~n · 1 · 1 t} to . . rze o )!CCts )y touch without the aid of vrs•.':n. I.os~ of this ability is calkd flstc:rt:ognosis, wluch may occur due to ;J dorsal column ur tt
p:~rictnl lobe h.:sion. Due to the former tl . . . · , o 1cr sc..:nsaLwn~ suhserved by the dorsal columns an: ;~ l.so. ~us c !•.c. p~lsi.tion, vibration ;utJ fine pressure.: sen~~) . When 1l ts Juc tu ;t parictal lube lcsiun POSI.llun . scnsc and light touch arc normal bu~ l;H.:tile drscrimination is lost.
. ([YPrcrto p.ct.ht'c ~sah·"" ~ ~ ~ C.R u.-i~ e s~j ll.h' 0'\1 ~ ttvLr c::7'vUL
?v.ce) v-e) ~ ~ ~ i\.1111. c,H • ~ ;' n c 1.t.t,) ~ c.r v..~ ?;~.; V\ ct- fil c.Qe. ~ !Lh' c"\11. s oJ- u tr~ f o1, ~ r (AA...f u r-£. c tt &-r:.i'.M... ~ z c c
V-' ftrc~·~ W) ·~+- it...J W(J-w £ y
0 c V-l ft-i.C<..(.,..J.
CVJ &rid.. cf fre_ Me~ ~5.<..
c1 +e-'W\~'ull.. ~. ' v'-'--.. ~l\"""t4..? ~ -t tv:.""" t<JJ.~ in ShtJ r h II'(_ .c=::t> -tW- ft"Cfo ('ttift/c.. .Le,..U it..h 'c1-\l Ct,'(.
rfb ~ c'rf.. . +t-t ~ WJ ( ~ ui r-t. S.f<~ S h,..,.uJ.;. ·V., k Predlv.se.d)
@ <if/cr,·n'c ( wn·c~) f4H~t.l)o,u ~~ ~~ ~·TK. ~Srth~V\~ ~ tvJ.. f v..c e-:· ~.d 6-:1 th..
\ ..ttsi~ d'6 f'oSI· eo..l.u~c.. ~«d f~lftoS4Sory Ciflf~
CR .. /..U.rrc.~ OJ Y K..< e. · 9 - ~k}e_ lc c.JJ Z.tLfi'IJ"-. '{.
d ~ ·~c ri~VI.tl'\iJ,·v-..,.. ~ /erc.05 h cs,·r
& ."-(_ C.,-r4 c4. f d6 ~ ~·Hfcth' •·.,...r
,G;.....v 1:-hrt.. .5 f.-.dd'
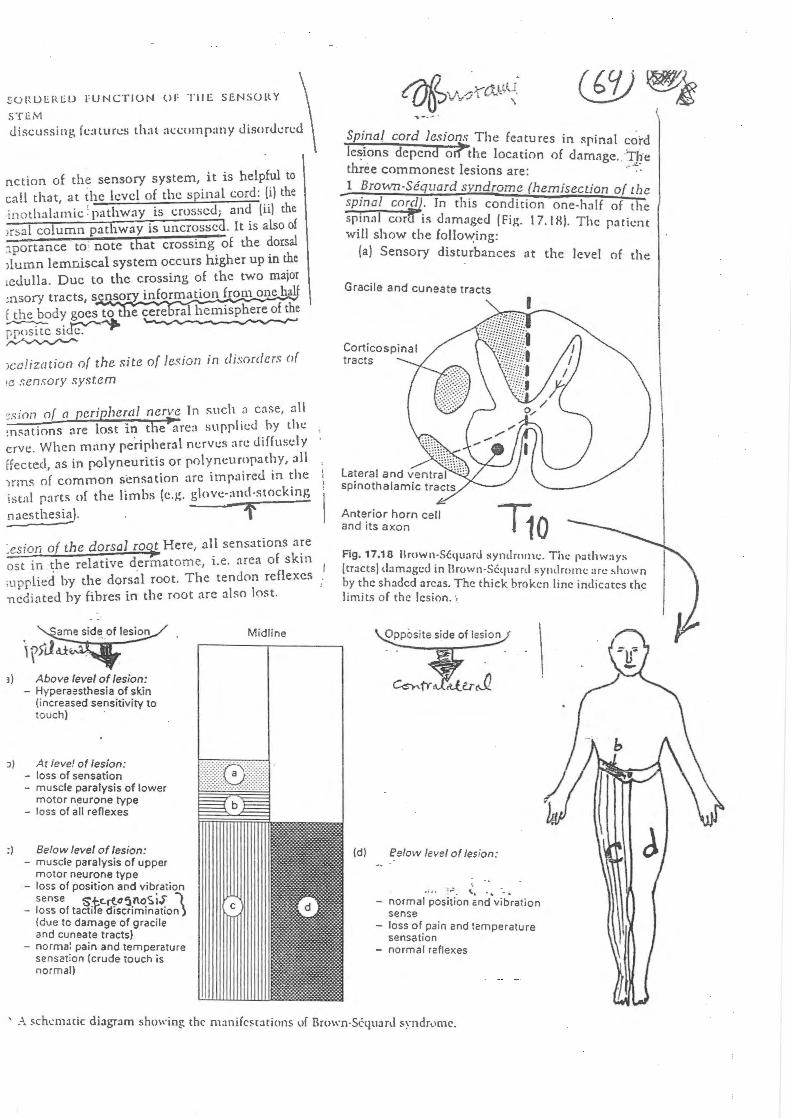
!:ORO!:.IU.~O FUNCTION OF TilE SENSORY \
STEM
discussing features that :H.:<.:omp:my Jiso~Jcrcd
nction of the sensory system, it is helpful to call that, at the level of the spinal cord: (i) the inothal:unic : pathway is crossed; and (ii) the >rsal column pathway is uncrossd. It is also of :tportance to note that crossing of the dorsal >lumn lemniscal system occurs higher up in the tcdulla. Due to the crossing of the two major :nsory tracts, sensorY information from one b f the body goes tot 1e cere ral hemisphere of the ~si~~ ~
>calization of the site of lesion in disorders of 1e sensory system
~sion of o peripheral nerve In such :'1 case, ~til :n~ations are lost in the~rca supplied by the crvc. When many peripheral nerves arc diffusely ffected, as in polyneuritis or polyneuropathy, all 1nns of common sensation arc impaired in the istal parts of tht! limbs (c.~. g\ov~:-ancl·stockinJ; nacsthesia). f .esion of the dorsal roQt Here, all sensations are ost in ~he relative d.ery;;atome, i.e. area of skin ;upplied by the dorsal root. The tendon reflexes ncdiated by fibres in the root are also lost.
3) Above level of lesion: - Hyperaesthesia of skin
(increased sensitivity to touch)
J) At !eve! of lesion: - loss of sensation - muscle paralysis of lower
motor neurone type - loss of all reflexes
:) Below level of lesion: - muscle paralysis of upper
motor neurone type - loss or position and vibration
sense Stc.rta5noS iS' I - loss or tactife discrimination)
(due to damage of gracile and cuneate tracts)
- norma: pain and temperature sensation (crude touch is normal)
Midline
Sp~nal cord lesions The features in !':pinal cord lel!'lOns depend oit"the location of damage. Tire three commonest lesions are: ·"":
_1 ~rown-Sequard srndrome (hemisection of the sp~nal wrd. Tn thts condition one-hnlf of the spmnl cor is dnmnged (Firr l? IH) Tl . '11 1 ,.... · · le pnttent Wl s 1ow the follo~ing:
(a) Sensory disturbances at the level of the
Gracile and cuneate tracts
Corticospinal tracts
Anterior horn cell and its axon 11o Fig. 17.18 1\rown_-Scqu:ml syndrOitH.:. The pathway:. (tracts) damaged tn Brown·SC:qu:m l symlromc arc :.hown ~y t.hc shaded areas. The thick broken line indicates the ltmJts o f the lesion.
(d) eg/ow level of lesion:
... :,: ~· . - normal position ~nd.vibration
sense - loss of. pain and temperature
sensat•on - normal raflexes
' A schl:nutic diagram showing the manifc!' t:ltions of Rruwn·Scquard !'\·ndr,,mc.
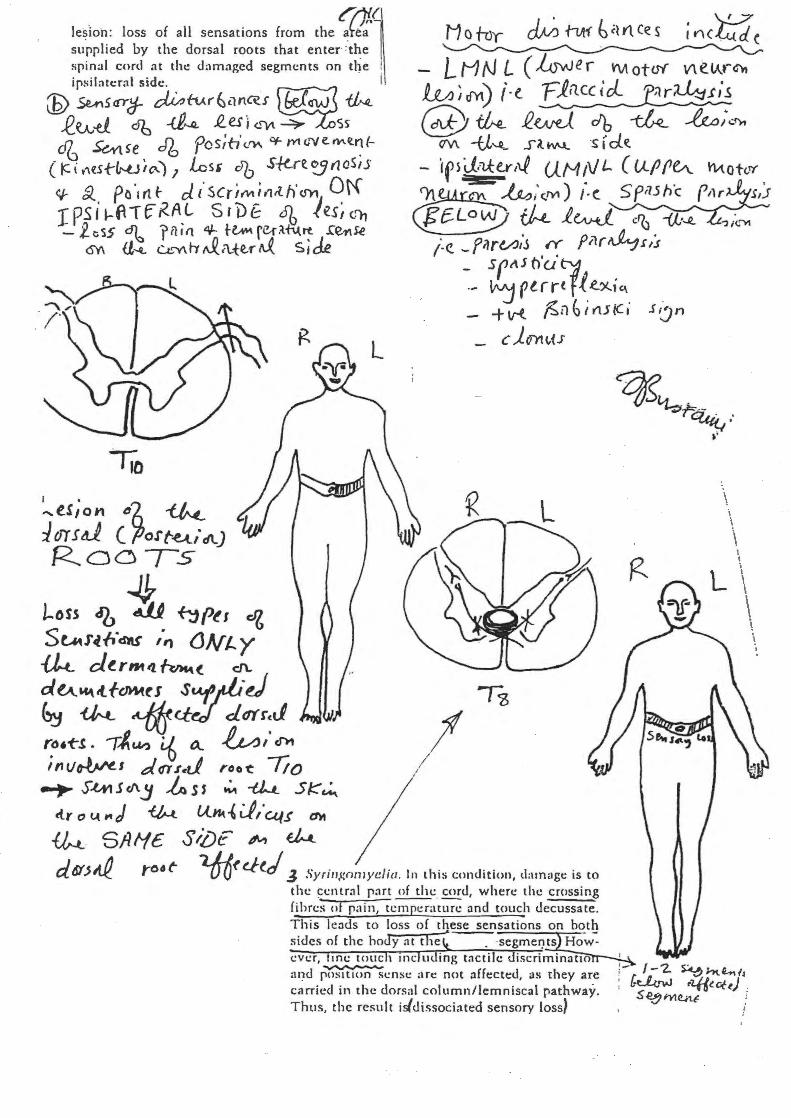
. r~~ le~ion: loss of all sensations from the a~e~· supplied by the dorsal roots that enter·=·the spinal cord :tt the dam:tgcd segments on t~e ipsilatcrnl side . I
M o trJy ~ fllt1 b cl t1. ce s i n<'tidc
LMN L ( hswer \'\Aot<N V\elAt-~ l.M I 0r1) (e. Fin.cc icl. ;}r~.t;.s (E) 5ul5<IY~ ~fv..r~c1n.~J ~ ~
R_~-d db -<i,.JJ_ .e_es; <-~ ~S5 @ fh_ R.~ db ~ ~; .. fM
(/\/\ -u~ s~~ ·s rde. cJG ~ ~e db pos;b' c.fl-\ Of- m <i"V e. Mil.~ l( ~i t'\~5{-~i"'-) 1 Lcsr db .S-1!-re.~(laS,s e;- &.. po·1rtf- c/..t'scriMi,,tth'<JYt Ot'{ r p s i ~ fl T f K A. L s I D & 6b J es ~ <-'1, - l cSS ~ r il t fl i3J.- t~ fC-rilt\.trt .(~)e
- ·,rsJ.=u:er~~ U.MtVL ( Uf'f1(A_ h.-tot<-tl'
~~;.c.IYl) i-c. Sf,Uh'c f1lr s,'.J ~ ~ l.w.J. ''b -a·~ ;~r>t1
/<?.. _filrt/.J;S .r: fi1r~.r/s <SY\ a~ u..'""' rr &.. f\._{e.t' rJ. s; de
lio I •
-ts,on "A ~ t dY S 41 ( fJott.e..t.itlt) Roo-,-s
4 l-oss <fb d11 ~Pt1 ell
_ 5fti.SOUt"j} .
-- ~ ptrr( f{.e.~'" +v-t ;<;n~ir'lJtCi 1':Jn
L _ c J.UYt~vU
S tM r ~ lid'lt$ ;,., (J N t.. y ~ dt.rm'l. fvM,..t_ d\..
dtA'44.tlfcMA.ti Suf_;h·d ~ ~ ~ct~ d(f(r:J rt1•-t"S. TiUI? L6 tl &, cS'l1
inv~s d~$d roo-t: Tio ~ S-tMJtl\ j ~ ss ~ -tJ.....t. 5~~ ~r o l.( ,. J ~ lhk { J,·CA./5 (1)t
I ,
~ SAI-fc SiiJE ~ ~ d6J'J,.f_ 1"06 t lfrO(c./ld _; Syritr,t:nmye/ia. In this condition, darn;~gc is to
the ~entr:tl p:lrt of the cord, where the crossing fihrc;;ol pain, tc~H~ and touch decussate. This leads to loss of these sensations on both sides of the hoJy nt theJ . ·segmeryts How~ ever, me touc 1 rnc u ins; t:tctile discriminatlo ____..._ ;u~d pos1t1on sense Me not afft:ctt:d, as they are cnrricd in the dorsal column/lemniscal pathway. Thus, the result isldissociated sensory loss}
\ i \ i \ . .
L \ \ \ \
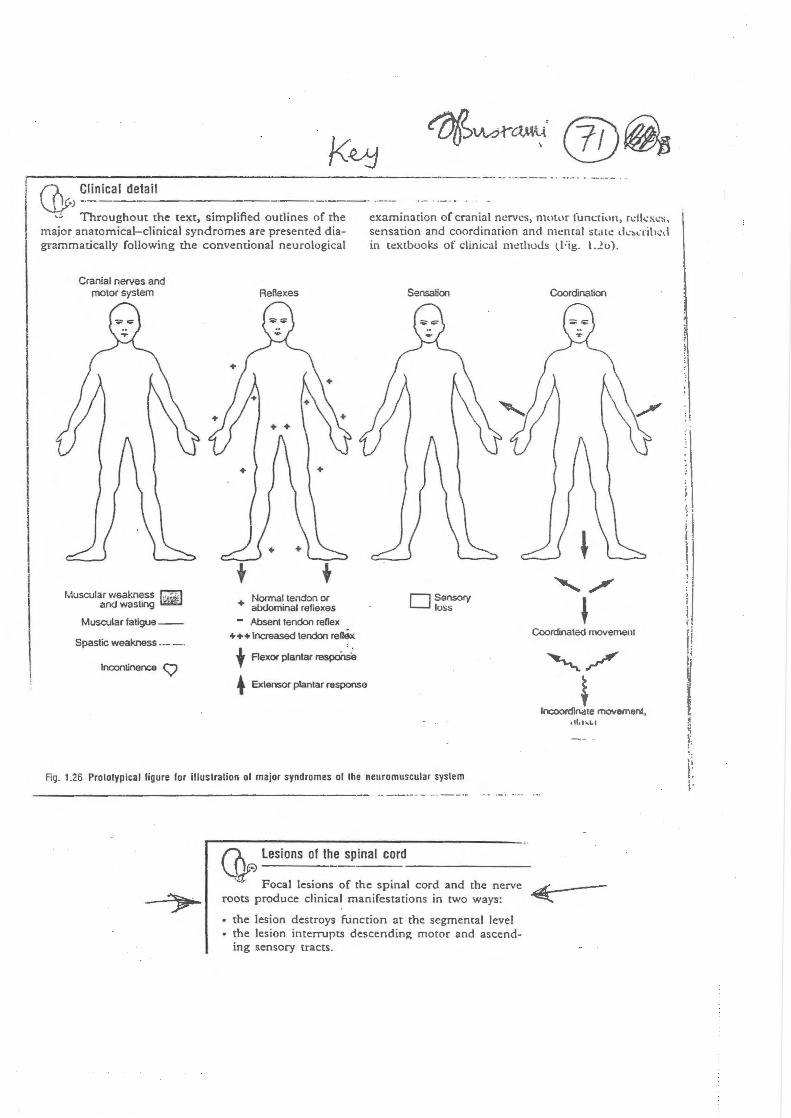
,----------------------------------· ··-- ·-. -- . -· ·-{).. Clinical detail ~·)-- ---------------- -
-:. Throughout the text, simplified outlines of the major anatomical-clinical syndromes are presented diagrammatically following the conventional neurological
examination of cranial nerves, nwt~lr function, n:lkxc~. sensation and coordination and mcmal state d.:~.:rih.:, l
in tc!Xtbooks of clinical methods tFig. l.2o) .
Cranial nerves and motor system
Muscular weakness ~ andwasling ~
Muscular fatigue--
Spastic weakness---·
Incontinence <::;
Reflexes
+ Normal tendon or alxJominal reflexes
- Absent tendon renex +++Increased tendon ren$c
t Aexor plantar respoilse
• Extensor plantar response
Sensation Coordination
D Sensory loss
Coordnated movemenl
"_,./
~ Incoordinate movement,
.1l.Ur .. &.l
Fig. 1.26 Prololypical llgure lor Illustration of major syndromes of the neuromuscular system
(0 lesions of the spinal cord
~Focal lesions of the spina_l_c_o_r_d_a_n_d-th_e_n_e_rv_c_LA:.---
roots produce clinical manifestations in rwo ways: ~
• the lesion destroys function at the segmental level • the lesion interrupts descending motor and ascend
ing sensory tracts.
'
ij r. !I ;j
\I
!l l ~ ~
'\ r
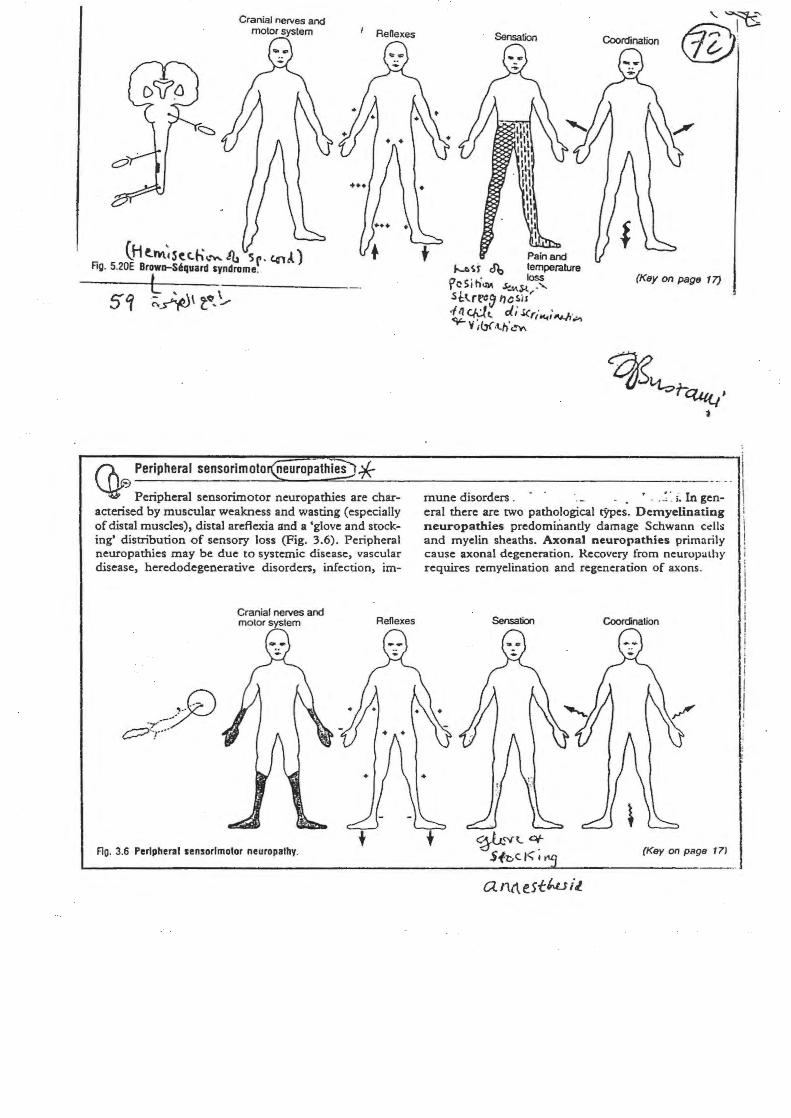
Cranial nerves and motor system
(H t.~~S~t.h~o""- 41 s . c.otl) Fig. 5.20E Brow~t-S6quard syndrome~
L . '
(/\~ Peripheral sensorlmoto neuropathies :f ~'!J Peripheral sensorimotor neuropathies are characterised by muscular weakness and wasting (especially of distal muscles), distal areflexia and a 'glove and stocking' distribution of sensory loss (Fig. 3.6). Peripheral neuropathies may be due to systemic disease, vascular disease, heredodegenerative disorders, infection, im-
Cranial nerves and motor system
Ao. 3.6 Peripheral sensorimotor neuropathy.
Renexes
\..~ ~I \!.!/':
(Key on page 17)
mune disorders . . ' .. ~ ·. ;. In general there are two pathological cypes. Demyelinating neuropathies predommantly damage Schwann cc:lls and myelin sheaths. Axonal neuropathies primarily cause axonal degeneration. Recovery from neurupalhy requires remyelination and regeneration of axons.
Sensation Coordination
(Key on page 171
a nl\e.stwil..
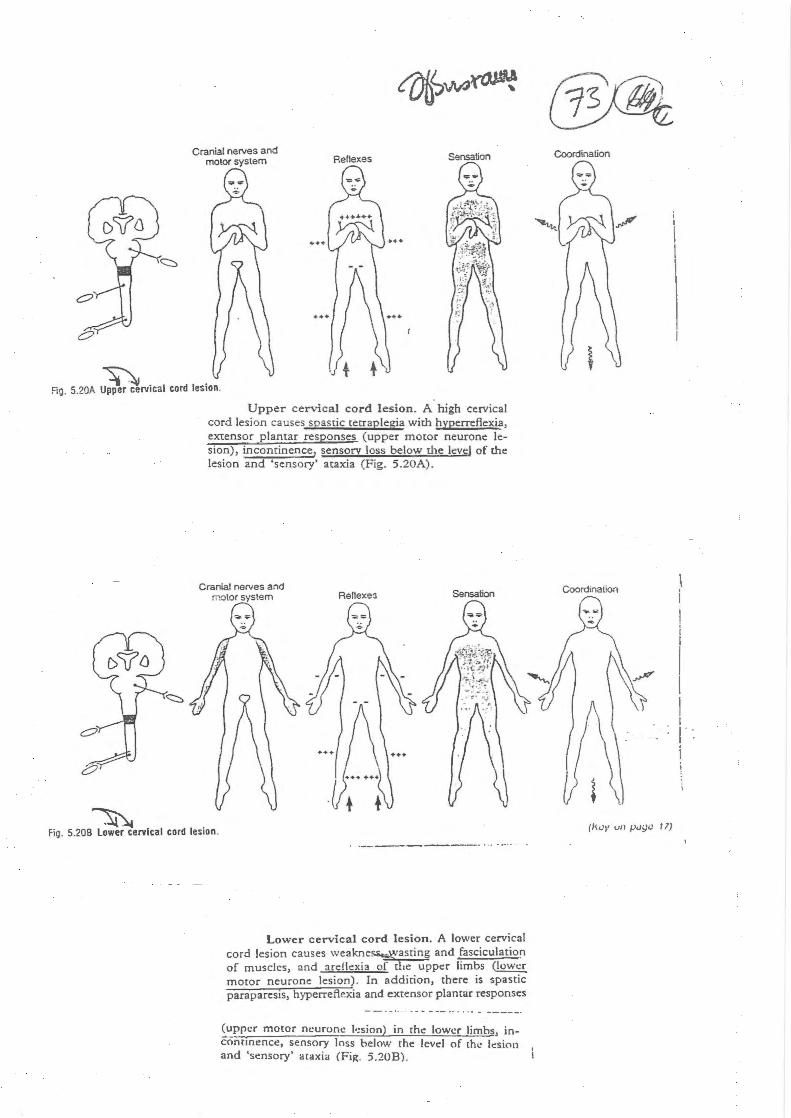
Cranial nerves and motor system Reflexes SensatiOn
Fig. 5.20A ~rvical cord lesion.
Upper cervical cord lesion. A . high cervical cord lesion causes spastic tetraplegia with hyperreflexia, extensor plantar responses (upper motor neurone lesion), incontinence, sensory loss below the levs;l of the lesion and 'sensory' ataxia (Fig. 5.20A).
~ Fig. 5.208 Lower cervical cord lesion.
Lower cervical cord lesion. A lower cervical cord lesion causes weakne~asting and fasciculation of muscles, and arellexia of du: upper limbs (lower motor neurone lesion). In addition, there is spastic paraparesis, hyperreflexia and extensor plantar responses
~':ppcr moto r neuro ne.: l•:sion) in rhe lower limbs, inconrmence, sensory loss below the level of thc ksion and 'sensory' ataxia (Fig. 5.20B).
Coordination
Coordination
(k/JI' vii J).Ji}C I 7)
i I
I I I I j' : I
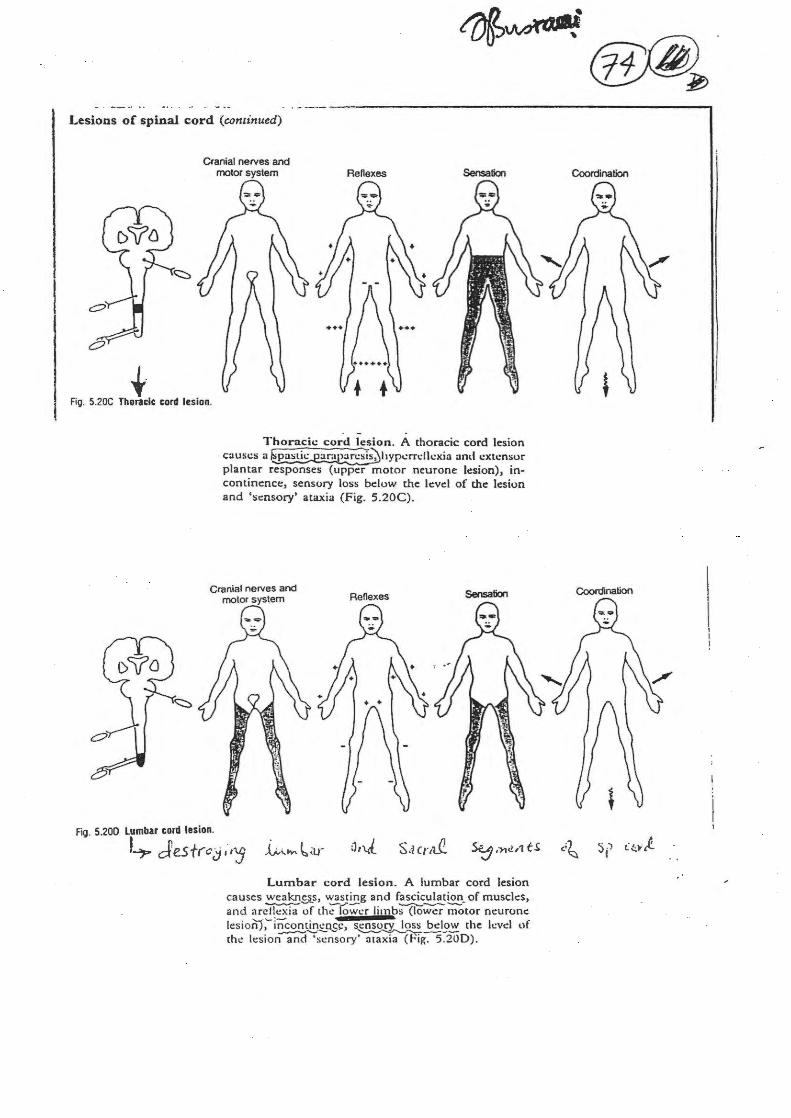
Lesions of spinal cord (continued)
t·
Cranial nerves and motor system Rene xes Sensation
Fig. 5.20C Thoracic cord lesion.
fig. 5.200 Lumbar cord lesion.
Thoracic cord lesion. A thoracic cord lesion causes a ~hypcrrcllcxia and extensor plantar responses (upper motor neurone lesion), incontinence::, sensory loss below the lc:vd of the: lesion and 'sensory' ataxia (Fig. 5.20C).
L,. Jesfrcj ;,'5 Lumbar cord lesion. A lumbar cord lesion
causes~~· ~sr~g and f~~~- of muscles, and arcflcxia of th..: rower limbs (lower motor neurone lesion};-incontinc~c, sensorY. loss bdow rhe level of
.....,.__...._~- ~---the h:sion and 'sensory' ataxia (Fig. 5.200).
Coordination
Coordination
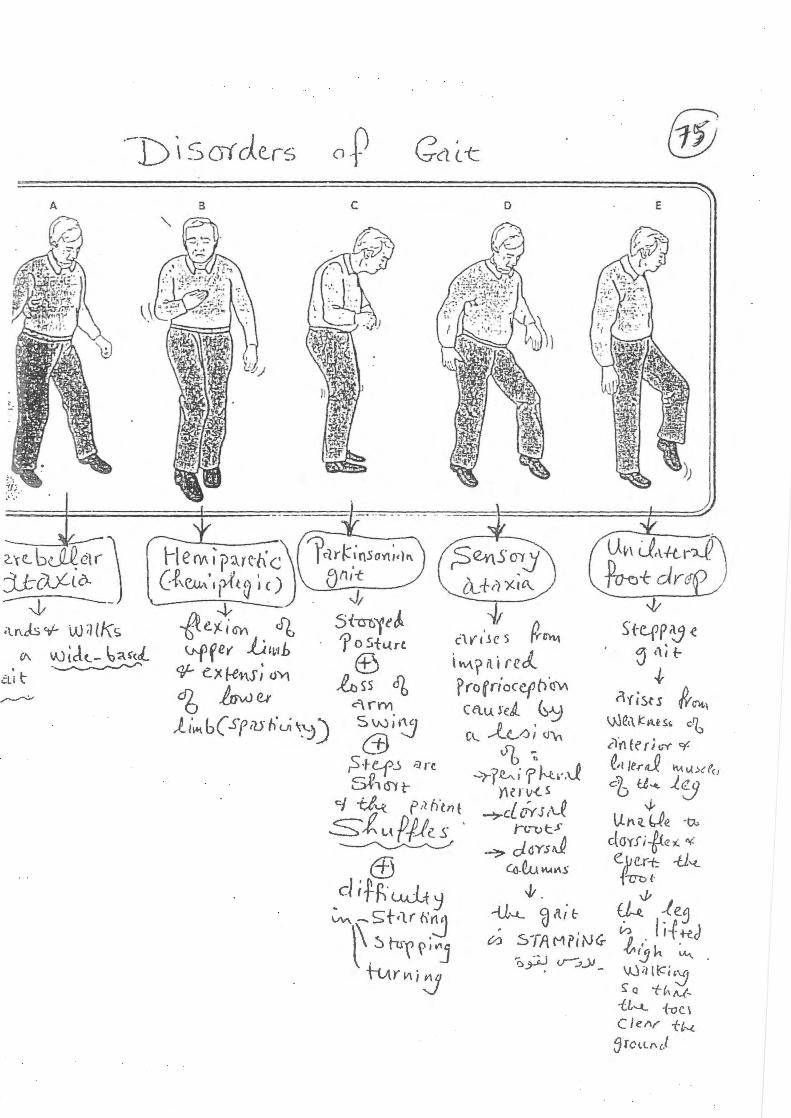
.-D \ S ()( de.rs
A
Grt. b~ctr .. J j_t-ci.Y-t o. ~ •lnc:ls ~ W ;) ll\s
(1\ VJ td<...- ~~{(J.. -~
C:l; t
8
o.r c
Gc1 (. -c
D
. I c\n·~e 5 ~~ i ""'r it i reJ. ProfriocCfO.fS\1\ CQu_l"eA_ ~~ Cl... ~(/) ; (JV\
V"b~ ~rl~'? N:.~-.J
Y\UII-t. S
~cLiYsl\...e r<rvt.>"
....::> d.dYSJ ((}.~~1'\S
@ E l
... l.: ·.· •
,,
/ .·~
.. ¥~
J ~ ./·
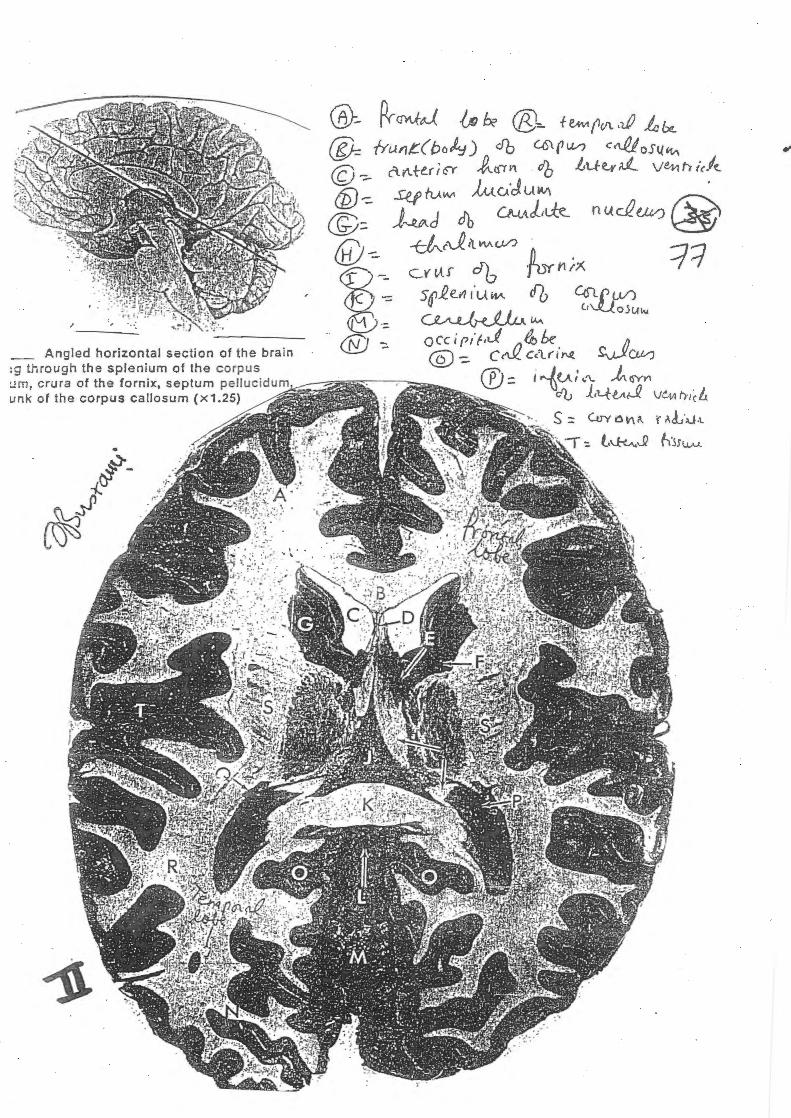
Angled horizontal section of the brain tg through the splenium of the corpus um, crura of the fornix, septum pellucidum unk of the corpus callosum (x1.25)
~t\s~l~c--~,..f'~ , __
Fi'- u .
]t, \-\~c,~~
)
Ct\ t.{.O.
1)\.V\
l e_.,'\ ~ ~01 ~ ""'"c.l
. f
. ; ;,
. ~~·.
'• ,~
f'on- .: ~ b I)
i t1t~r~~ . ~.r,J.~
_ .. -~-- -- . :~· .·~ - .
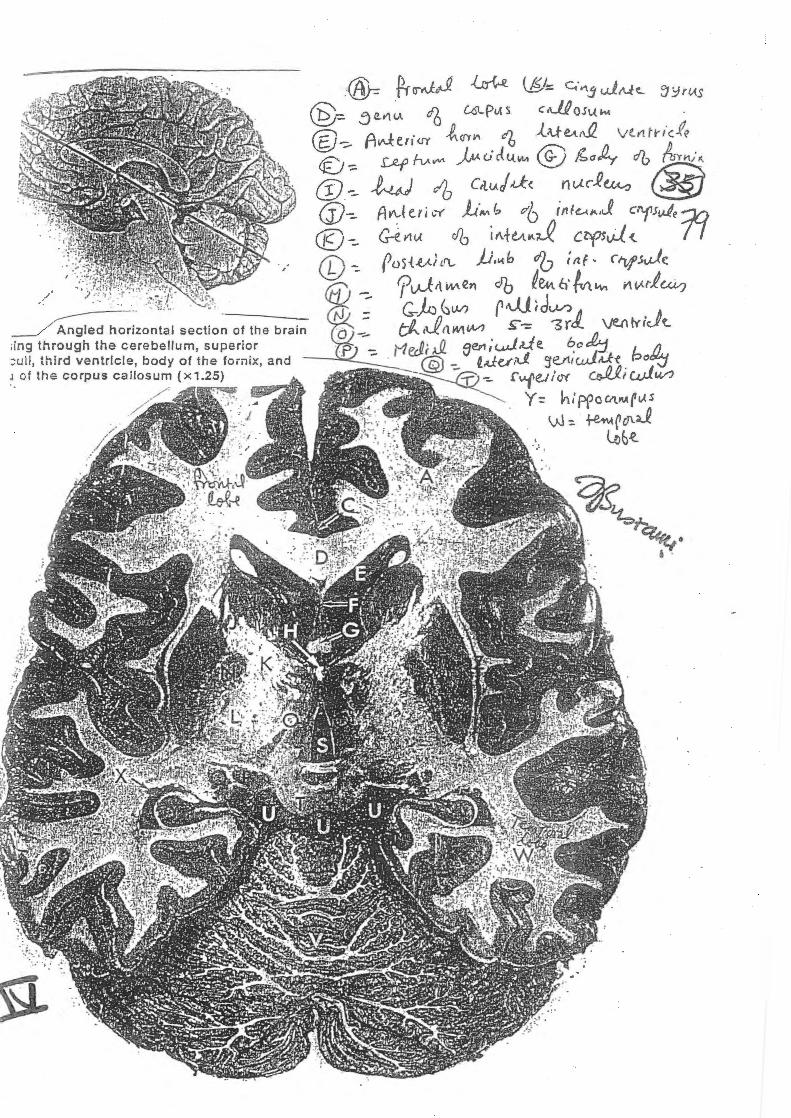
~~;~ontal section of the brain dng through the cerebellum, superior :;uli, t h ird ventricle, body of the forn ix, and J of the corpus callosum (x1.25) ·. ,//
-~
· .. ~
. .. ' ~ ...... :J .
·' · ..





























