Embed Size (px)
Citation preview
ILC2019
Post
er p
rese
nted
at:
CONCLUSIONS
Add your logos here
1 INTRODUCTION 2 METHODS
5
6 REFERENCES
7 CONTACT
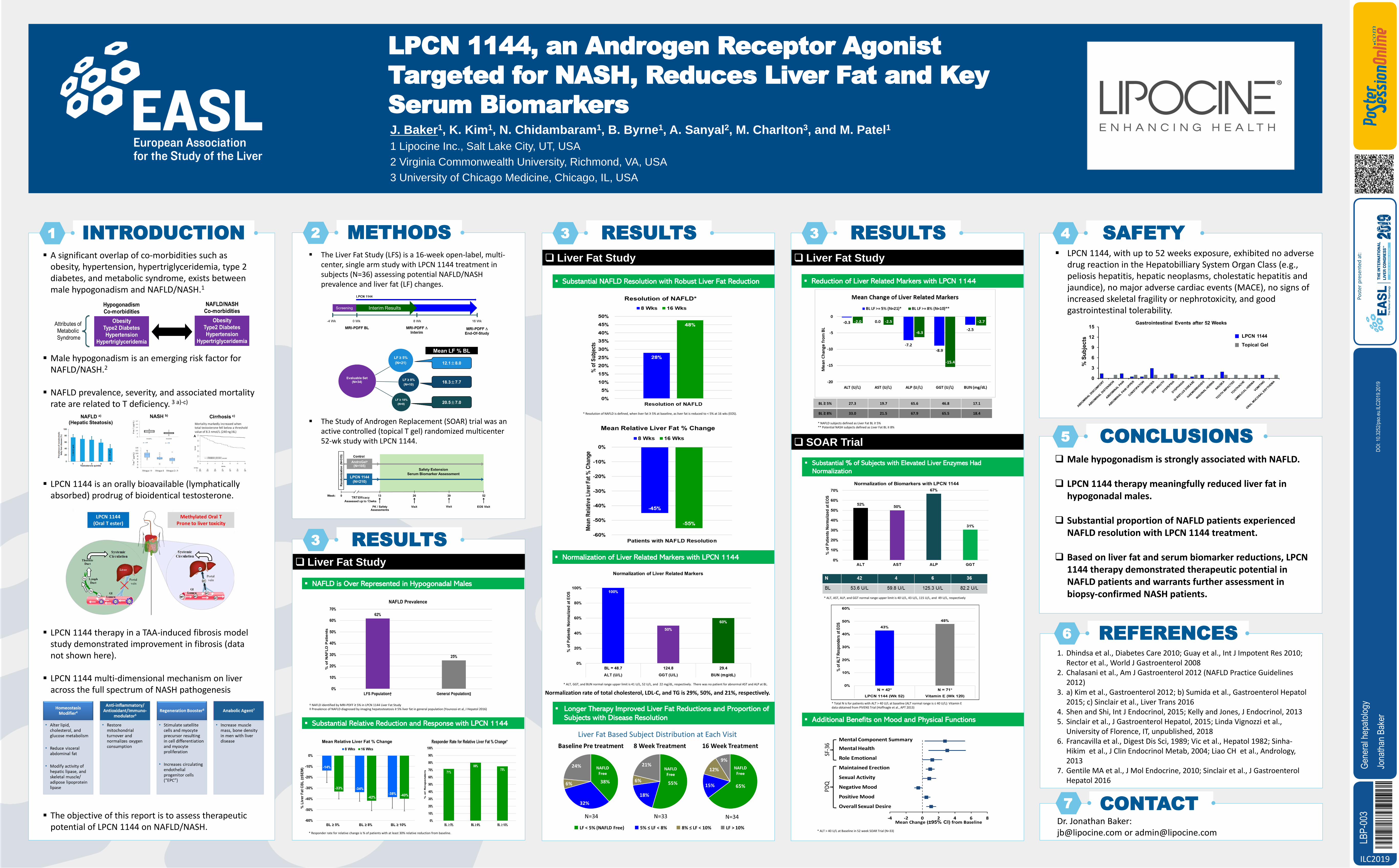
▪ A significant overlap of co-morbidities such as obesity, hypertension, hypertriglyceridemia, type 2 diabetes, and metabolic syndrome, exists between male hypogonadism and NAFLD/NASH.1
▪ Male hypogonadism is an emerging risk factor for NAFLD/NASH.2
▪ NAFLD prevalence, severity, and associated mortality rate are related to T deficiency. 3 a)-c)
▪ LPCN 1144 is an orally bioavailable (lymphatically absorbed) prodrug of bioidentical testosterone.
▪ LPCN 1144 therapy in a TAA-induced fibrosis model study demonstrated improvement in fibrosis (data not shown here).
▪ LPCN 1144 multi-dimensional mechanism on liver across the full spectrum of NASH pathogenesis
▪ The objective of this report is to assess therapeutic potential of LPCN 1144 on NAFLD/NASH.
❑ Male hypogonadism is strongly associated with NAFLD.
❑ LPCN 1144 therapy meaningfully reduced liver fat in hypogonadal males.
❑ Substantial proportion of NAFLD patients experienced NAFLD resolution with LPCN 1144 treatment.
❑ Based on liver fat and serum biomarker reductions, LPCN 1144 therapy demonstrated therapeutic potential in NAFLD patients and warrants further assessment in biopsy-confirmed NASH patients.
1. Dhindsa et al., Diabetes Care 2010; Guay et al., Int J Impotent Res 2010; Rector et al., World J Gastroenterol 2008
2. Chalasani et al., Am J Gastroenterol 2012 (NAFLD Practice Guidelines 2012)
3. a) Kim et al., Gastroenterol 2012; b) Sumida et al., Gastroenterol Hepatol2015; c) Sinclair et al., Liver Trans 2016
4. Shen and Shi, Int J Endocrinol, 2015; Kelly and Jones, J Endocrinol, 20135. Sinclair et al., J Gastroenterol Hepatol, 2015; Linda Vignozzi et al.,
University of Florence, IT, unpublished, 20186. Francavilla et al., Digest Dis Sci, 1989; Vic et al., Hepatol 1982; Sinha-
Hikim et al., J Clin Endocrinol Metab, 2004; Liao CH et al., Andrology, 2013
7. Gentile MA et al., J Mol Endocrine, 2010; Sinclair et al., J Gastroenterol Hepatol 2016
Dr. Jonathan Baker: [email protected] or [email protected]
▪ The Liver Fat Study (LFS) is a 16-week open-label, multi-center, single arm study with LPCN 1144 treatment in subjects (N=36) assessing potential NAFLD/NASH prevalence and liver fat (LF) changes.
▪ The Study of Androgen Replacement (SOAR) trial was an active controlled (topical T gel) randomized multicenter 52-wk study with LPCN 1144.
J. Baker1, K. Kim1, N. Chidambaram1, B. Byrne1, A. Sanyal2, M. Charlton3, and M. Patel1
1 Lipocine Inc., Salt Lake City, UT, USA
2 Virginia Commonwealth University, Richmond, VA, USA
3 University of Chicago Medicine, Chicago, IL, USA
LPCN 1144, an Androgen Receptor Agonist
Targeted for NASH, Reduces Liver Fat and Key
Serum Biomarkers
3 RESULTS 3 RESULTS
3 RESULTS❑ Liver Fat Study
† NAFLD identified by MRI-PDFF ≥ 5% in LPCN 1144 Liver Fat Study‡ Prevalence of NAFLD diagnosed by imaging hepatosteatosis ≥ 5% liver fat in general population (Younossi et al, J Hepatol 2016)
* Responder rate for relative change is % of patients with at least 30% relative reduction from baseline.
▪ NAFLD is Over Represented in Hypogonadal Males
▪ Substantial Relative Reduction and Response with LPCN 1144
❑ Liver Fat Study
▪ Substantial NAFLD Resolution with Robust Liver Fat Reduction
* Resolution of NAFLD is defined, when liver fat ≥ 5% at baseline, as liver fat is reduced to < 5% at 16 wks (EOS).
* NAFLD subjects defined as Liver Fat BL ≥ 5% ** Potential NASH subjects defined as Liver Fat BL ≥ 8%
▪ Reduction of Liver Related Markers with LPCN 1144
▪ Normalization of Liver Related Markers with LPCN 1144
Normalization rate of total cholesterol, LDL-C, and TG is 29%, 50%, and 21%, respectively.
❑ Liver Fat Study
▪ Longer Therapy Improved Liver Fat Reductions and Proportion of
Subjects with Disease Resolution
Liver Fat Based Subject Distribution at Each Visit
* ALT, AST, ALP, and GGT normal range upper limit is 40 U/L, 43 U/L, 115 U/L, and 49 U/L, respectively
▪ Substantial % of Subjects with Elevated Liver Enzymes Had
Normalization
❑ SOAR Trial
* Total N is for patients with ALT > 40 U/L at baseline (ALT normal range is ≤ 40 U/L): Vitamin E data obtained from PIVENS Trial (Hoffnagle et al., APT 2013)
* ALT > 40 U/L at Baseline in 52 week SOAR Trial (N=33)
▪ Additional Benefits on Mood and Physical Functions
SAFETY4
▪ LPCN 1144, with up to 52 weeks exposure, exhibited no adverse drug reaction in the Hepatobilliary System Organ Class (e.g., peliosis hepatitis, hepatic neoplasms, cholestatic hepatitis and jaundice), no major adverse cardiac events (MACE), no signs of increased skeletal fragility or nephrotoxicity, and good gastrointestinal tolerability.
BL ≥ 5% 27.3 19.7 65.6 46.8 17.1
BL ≥ 8% 33.0 21.5 67.9 65.5 18.4
* ALT, GGT, and BUN normal range upper limit is 41 U/L, 52 U/L, and 22 mg/dL, respectively. There was no patient for abnormal AST and ALP at BL.
LBP-
003
Jona
than B
aker
DOI: 1
0.325
2/pso
.eu.IL
C201
9.201
9
Gene
ral h
epato
logy





























