Embed Size (px)
Citation preview

LOW TESTOSTERONE: WHEN, HOW & WHAT TO DO?
Premal Patel, MDAssistant Professor
Male Infertility, Microsurgery & Sexual MedicineUniversity of Manitoba
www.manitobafertility.com

Faculty/Presenter Disclosure
• Faculty: Premal Patel, MD FRCSC
• Relationships with financial sponsors:– Speakers Bureau/Honoraria: Aytu Biosciences, Boston Scientific
– Consulting Fees: Nestle Health, Boston Scientific
www.manitobafertility.com

Disclosure of Financial Support
• No financial disclosures to report
• Potential for conflict(s) of interest:• No Potential Conflict of Interests
www.manitobafertility.com
• No relevant conflict of interest for this talk
Mitigating Potential Bias
www.manitobafertility.com

Overview
• Understand the physiology and etiology of testosterone deficiency
• When and how to treat testosterone deficiency
• How to monitor patients on testosterone replacement therapy
www.manitobafertility.com

Production and Regulationof Testosterone
40% of serum testosterone is “bioavailable”
Free T2%
SHBG-bound T 60%
Albumin-bound T
38%
GnRH
LH FSHTestosterone
Testosterone
Sperm
Hypothalamus
Pituitary
Testis
www.manitobafertility.com

Prevalence of Low Testosterone:13.8 Million Men in the US
Overall, 38.7% of men >45y
have T-levels < 10.4 nmol/L
Pre
vale
nce
of
Low
T in
All
Enro
lled
P
atie
nts
(%
, 95
% C
I)
0
10
20
30
40
50
60
>85
Patient Age Range
45 to
54
55 to
64
65 to
74
75 to
84
www.manitobafertility.com

74
5250 50
4240
19
0
10
20
30
40
50
60
70
80
90
100
(%)
Prevalence of Low Testosterone in Other Conditions
Ob
esit
y
Dia
bet
es
Hyp
ert
ensi
on
Dys
lipid
emia
Ch
ron
ic O
pio
id U
se
AID
S
ED
www.manitobafertility.com

Hypogonadism in the Aging Man
• All components of testosterone decline with normal aging
• Decline in Leydig cell count and function
• Increase SHBG, lowers bioavailable T
• Not all men with low testosterone have symptoms or need treatment
www.manitobafertility.com

Age-Related Changes in Testosterone
Test
ost
ero
ne
(nm
ol/
L)
Age (Years)
10
12
14
16
18
20
30 40 50 60 70 80 90
(177)
(144)(151)
(158)
(109)
(43)
www.manitobafertility.com
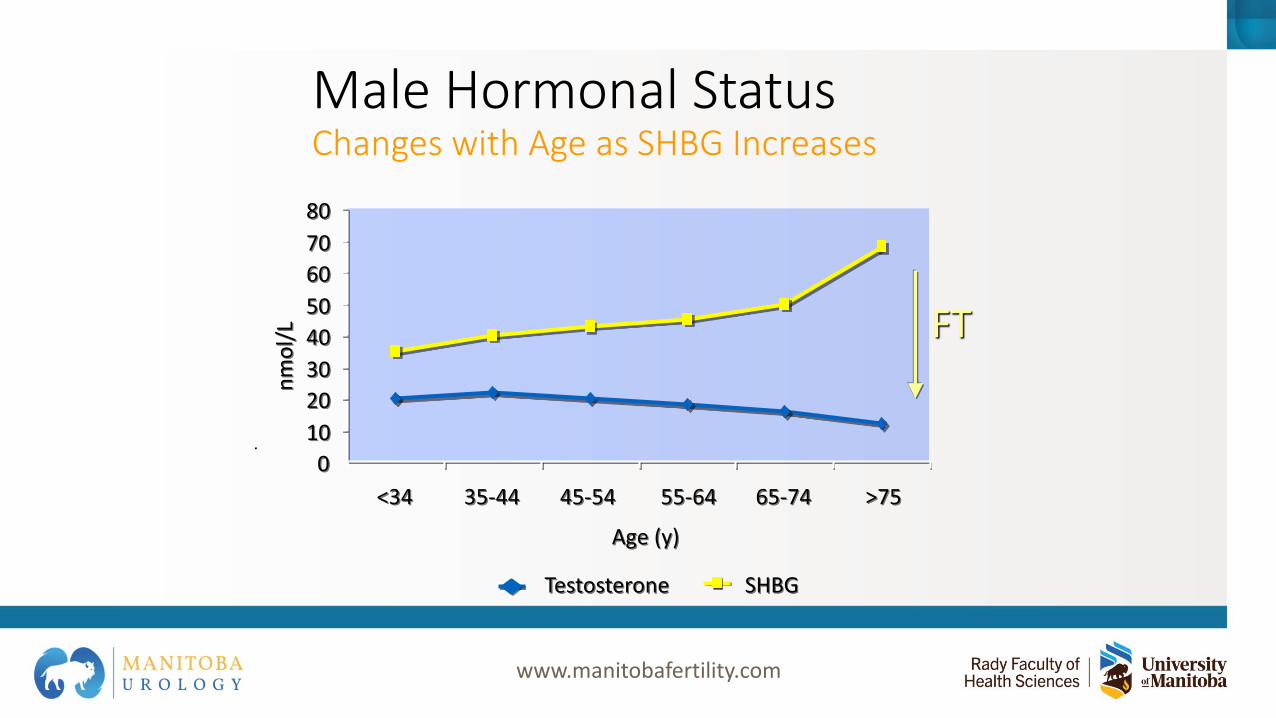
Male Hormonal StatusChanges with Age as SHBG Increases
FTn
mo
l/L
0
10
20
30
40
50
60
70
80
<34 35-44 45-54 55-64 65-74 >75
Age (y)
Testosterone SHBG
www.manitobafertility.com

Aging Males and MortalityMen with Low T May Not Live As Long
• 800 Men, 50-91 y, followed for 18 y
• 1/3 had low T
• Men with low T versus those with higher T had:
Increased levels of inflamm-
atorycytokines
Increased waist girth
3x more likely to
have metabolic syndrome
40% greater risk of death
www.manitobafertility.com

Aging Males and MortalityLow Serum T and Mortality in Male Veterans
Survival (y)
1.0
0.5
0.9
0.8
0.7
0.6
0 2 4 6 8 10
Cu
mu
lati
ve S
urv
ival
Men With a Low T-Level (n = 166)
Men With a Normal T-Level (n = 452)
T-Level Mortality (%)
Normal 20.1
Low 34.9
www.manitobafertility.com

The Impact of TestosteroneSkin
Hair growth, balding, sebum production
LiverSynthesis of serum
proteins
Male Sexual OrgansPenile growth,
spermatogenesis, prostate growth, and function
BrainLibido, mood
MuscleIncrease in strength and volume
KidneyStimulation of erythropoietin production
Bone MarrowStimulation of stem cells
BoneAccelerated linear growth,
closure of epiphyses
Guyton AC. In: Textbook of Medical Physiology. 8th ed. 1991:891-895.www.manitobafertility.com

Potential Effects of Hypogonadism
Long-term complications• Decline in libido and erectile function
• Increased body fat mass
• Decreased muscle mass, bone mass, and strength
• Possibly: fatigue, mood / cognitive changes
• Increased incidence of osteoporosis
www.manitobafertility.com

Testosterone and Sex
• ED exclusively related to hypogonadism is rare (5%)
• In hypogonadal men with ED, return to low level of normal testosterone range is adequate
• Libido is most likely to improve with treatment
• Spermatogenesis is greatly reduced with testosterone replacement, and may not be reversible with cessation (5% of men)
www.manitobafertility.com

It doesn’t take much for a man with testosterone to
become aroused
www.manitobafertility.com

www.manitobafertility.com

Diagnosis of Low Testosterone:
• Symptoms• Signs• Decreased T
www.manitobafertility.com
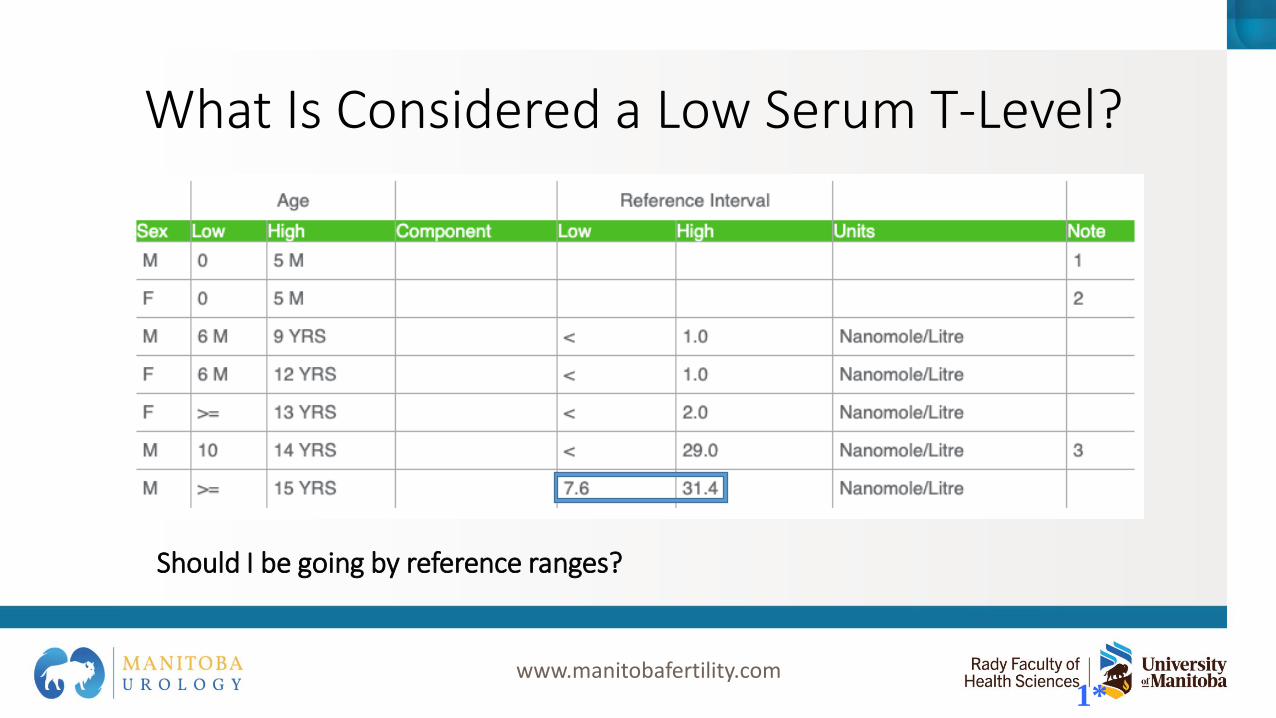
What Is Considered a Low Serum T-Level?
1*
Should I be going by reference ranges?
www.manitobafertility.com

What Is Considered a Low Serum T-Level?
• American Urological Association & Endocrine Society• Low Testosterone: < 10.4 nmol/L (300 ng/dL)
www.manitobafertility.com

Diagnostic Testosterone Testing: Initial Tests
• Serum Total Testosterone (free plus protein-bound)
Morning sample recommended in young men
• Serum Bioavailable T (free plus albumin-bound)
Measures albumin-bound and free testosterone
Best test, most expensive.
www.manitobafertility.com
Diagnostic Testosterone Testing: Additional Tests
• LH and FSH
• Serum Prolactin (TT < 5.2 nmol/L + low LH/FSH or signs/symptoms)
• Baseline PSA (in men > 50y or family history of Prostate Cancer)
• Baseline Hematocrit
www.manitobafertility.com

Confirmed low T (Total < 10.4 nmol/L)
OR
Free or Bio T < normal (Free T <179 pmol/L)
Low T
Low or normal LH+FSH
Prolactin, iron sats
Other pituitary hormones
Low T
High LH+FSH
Karyotype
Klinefelter Syndrome
Other Testicular Insult
Secondary Hypogonadism Primary Hypogonadism
MRI in
certain cases
www.manitobafertility.com
Key Symptoms and Signs Associated with Low Testosterone
Symptoms• Increased body fat,
BMI
• Reduced muscle bulk and strength
• Low BMD
• Loss of body hair (axillary and pubic), reduced shaving
Signs• Decreased energy
or motivation • Depressed mood• Diminished libido,
ED• Diminished work
performance• Poor concentration
and memory• Sleep disturbance
www.manitobafertility.com

www.manitobafertility.com

Testosterone Replacement Therapy:
Treatment Options
www.manitobafertility.com

Contraindications to Testosterone Therapy
• Breast or metastatic prostate cancer
• Cardiovascular disease (recent MI, angina or CHF; 3-6 months)
• Lump/hardness on prostate exam by DRE
• PSA >3 ng/ml that has not been evaluated for prostate cancer
• Severe untreated BPH (AUA/IPSS >19)
• Erythrocytosis (hematocrit >50%)
• Untreated obstructive sleep apnea
www.manitobafertility.com

Risks of Testosterone Replacement Therapy (TRT)
• Hepatic adverse effects with oral therapy
• Polycythemia
• Edema
• Gynecomastia
• Precipitation or worsening of sleep apnea
• Infertility
www.manitobafertility.com
Risks of Testosterone Replacement Therapy (TRT)
• Cardiovascular Disease?
• Prostate Cancer?
www.manitobafertility.com

100100 200200 300300 400400 800800500500 600600 70070000
Serum testosterone level (Serum testosterone level (ng/dLng/dL))
Pro
stat
e G
row
th (
PS
A)
Pro
stat
e G
row
th (
PS
A)
Saturation EffectSaturation Effect
Unsatu
rated
Unsatu
rated
““Normal Physiologic Range”Normal Physiologic Range”
Virtually Virtually
CastrateCastrate
SaturationSaturation Model of Physiologic Testosterone ReplacementModel of Physiologic Testosterone Replacement
120-150 ng/ml
= PSA
1*www.manitobafertility.com

TRT Treatment Options
Oral Tablets
Intramuscular
Injections
Transdermal
Gels
Transdermal
Patches
4*www.manitobafertility.com

How Do You Give Testosterone?
• Start at standard dose
• Check levels
• Therapeutic target• Serum testosterone in mid-normal range for healthy, young
men (14 – 17.5 nmol/L)
• Target in older men• Considerable disagreement among experts
• Aim for low-mid range (14 – 17.5 nmol/L)
www.manitobafertility.com

Non-genital Transdermal Patch
• Mimics normal diurnal rhythm
• Less increase in hematocrit than IM shots
• Start at 1-2 x 5 mg nightly to the skin of the back, thigh, or upper arm• Away from pressure areas
• Some men need 2 patches
• Skin irritation/redness/rashes
www.manitobafertility.com

Testosterone Gel
• Starting dose 5-10 grams daily
• Skin tolerates it well
• Potential transfer to others by skin contact• Cover the application site
• Wash hands with soap and water after application
• Wash skin before skin-to-skin contact with others
• T levels maintained when skin washed 4-6 hours after application
www.manitobafertility.com

Testosterone Enanthate or Cypionate Injections (IM)
• T levels are supraphysiologic, then gradually drop to hypogonadal range
• Peaks and valleys
• Fluctuation of mood or libido
• Relatively inexpensive if self-administered
• Start at 75-100 mg IM weekly
• Or 150-200 mg IM every other week
• Pain at injection site
• Excessive erythrocytosis (esp in older pts)
www.manitobafertility.com

Monitoring T Levels
• Target the mid-normal range
• Timing• Patch: 3-12 hours after application
• Gel: after 1-2 weeks of treatment
• Injections: 6 weeks after treatment, q 3months for 1st year, q 6months after
www.manitobafertility.com

Safety Monitoring
• Baseline• Testosterone level, DRE, PSA, Hematocrit
• Follow-up ~3 months then annually• Assess improvement/side effects
• Testosterone, Estradiol, Hematocrit, DRE
• PSA• age- and race-appropriate interval
• If osteoporosis – DXA at 1-2 years
www.manitobafertility.com

Testosterone for the Following Reasons May be Harmful
• To improve strength/athletic performance
• For physical appearance
• To prevent aging
www.manitobafertility.com
Management of adverse effects
• Erythrocytosis: • HCt > 53% - phlebotomy q 2 weeks +/- adjust
testosterone dosage
• Elevated serum estradiol • E > 60 pg/mL – anastrozole 1mg BIW
• Acne – minocycline
• Gynecomastia (with normal E) – tamoxifen 20mg BID
www.manitobafertility.com

Conclusions
• Low T in adult men is often underdiagnosed and undertreated
• T levels gradually diminish with age, often to hypogonadal levels (<10.4 nmol/L)
• TRT has several alternatives – gels, injections & patch
• TRT is safe with proper monitoring (PSA, HCt, estradiol)
• CaP and CV risks need to be discussed prior to TRT
3*www.manitobafertility.com

1. Adapted from Braunstein G.D.. In: Basic & Clinical Endocrinology. 5th ed. Stamford, Conn: Appleton & Lange; 1997:403-433.2. Mulligan T, et al. J Clin Pract, 60(7):762-769, 2006.3. Bodie J, et al. J Urol, 169:2262–2264, 2003.4. Daniell HW, J Pain, 3:377-384, 2002.5. Dobs AS, Clin Endocrinol Metab, 12:379-370, 1998.6. Grinspoon S, et al. Ann Intern Med, 129:18-26, 1998.7. Mulligan T, et al. Int J Clin Pract, 60:762–769, 2006.8. Tenover J.L. Endocrinol Metab Clin North Am. 1998;27:969-987.9. Swerdoff, R.S. Summary of the Consensus Session from the 1st Annual 10. Andropause Consensus Meeting. The Endocrine Society, April 2000.11. Adapted from Harman S.M., et al. J Clin Endocrinol Metab. 2001;86:724-731.12. Gray A, et al. J Clin Endocrinol Metab, 73:1016-1025, 1991.13. Kupelian V, et al. Clin Endocrin Metab, 91:843-850, 2006.14. Laaksonen DE, et al. Diabetes Care, 27(5):1036–1041, 2004.15. Laughlin G, et al. ENDO, Abstract OR55-2, 2007.16. Shores M, et al. Arch Intern Med, 166:1660-1665, 2006.17. Tenover J.L.. Endocrinol Metab Clin North Am. 1998;27:969-987.18. Bhasis, S., Mayo Clin Proc 2000; 75: S70.19. Leungwattanakij, S., et al, Mediguide to Urology, 2000; 13:1.20. Tenover J.L.. Endocrinol Metab Clin North Am. 1998;27:969-987.21. Petak S.M., et al. AACE Clinical Practice Guidelines. Available at: http://www.aace.com/clin/guidelines/hypogonadism.html.22. AACE Hypogonadism Task Force. Endocrinol Pract, 12:193-222, 2006.23. Bhasin S, et al. Testosterone Therapy for Hypogonadism Guideline. J Clin Endocrinol Metab, March 2018.24. Morales A, et al. Diagnosis and management of testosterone deficiency syndrome in men: clinical practice guidement. CMAJ December 08, 201525. Tenover J.L.. Endocrinol Metab Clin North Am. 1998;27:969-987.26. Braunstein G.D.. In: Basic & Clinical Endocrinology. 5th ed. Stamford, Conn: Appleton & Lange; 1997:403.27. Morgentaler A, Traish AM. Eur Urol. 2008;55:310-32028. Mulhall JP et al. Evaluation and Management of Testosterone Deficiency: AUA Guideline. J Urol. 2018 Aug;200(2):423-432.
References
www.manitobafertility.com
Questions?
@PremalPatelMD
For consults (Fax): 204-787-3040- Male Infertility
- Testosterone Deficiency
- Erectile Dysfunction
- Male Incontinence
- BPH
- Peyronie’s Disease
www.manitobafertility.com





























