Embed Size (px)
Citation preview

Low-dose dipyridamole treatment partially prevents diabetes mellitus-inducedvascular endothelial and renal abnormalities in rats
Arun Kumar Sharma a, Deepa Khanna a,⁎, Pitchai Balakumar b
a Department of Pharmacology, Rajendra Institute of Technology and Sciences (RITS), Sirsa 125 055, Indiab Pharmacology Unit, Faculty of Pharmacy, AIMST University, 08100 Bedong, Malaysia
a r t i c l e i n f o
Article history:Received 9 January 2014Accepted 12 January 2014Available online 23 January 2014
Keywords:Diabetes mellitusLow-dose dipyridamolePI3-KeNOSVascular endothelial dysfunctionNephropathy
Dipyridamole is a conventionally used platelet inhibitor employedfor the secondary prevention of transient ischemic attack. Dipyrida-mole could potentiate some of the vascular protective effects of nitricoxide (NO) [1]. Intriguingly, the vascular protective action ofdipyridamole was reported to be mediated by its stimulatory actionon endothelial nitric oxide synthase (eNOS) activity [2]. However, theeffect of dipyridamole in diabetes mellitus-induced vascular endothe-lial dysfunction (VED) is not yet known. There are strong associationsbetween diabetic VED and nephropathy [3,4]. Administration ofdipyridamole either alone or in combination with aspirin reducedthe incidence of proteinuria in patients with diabetic nephropathy [5].Dipyridamole at high-dose is considered proischemic, and it couldcause a marked coronary steal effect. Dipyridamole, however, at low-dose orallymight have aminimal hemodynamic effect [6]. The presentstudy investigated the effect of low-dose dipyridamole in diabetesmellitus-induced VED and nephropathy in rats.
The experimental protocol of this study was approved by the‘Institutional Animal Ethics Committee’. Wistar albino rats of eithersex (n = 6) weighing about 250 to 350 g were used. Group I (NormalControl), rats were maintained on standard food and water, and notreatment was given. Group II (Diabetic Control), rats were adminis-tered streptozotocin (STZ) (50 mg/kg, i.p., once), andwere allowed for8 weeks to develop experimental VED and nephropathy (rats showingblood glucose level of greater than 200 mg/dl after 72 h of STZadministration were selected and named as diabetics). Group III
(Dipyridamole per se), normal rats were administered low-dosedipyridamole (30 mg/kg/day, p.o.) for 4 weeks. Group IV (Dipyrida-), the diabetic rats after 4 weeks of STZ-administration were treated withlow-dose dipyridamole (30 mg/kg/day, p.o.) for 4 weeks. Groups V and VI(Wortmannin or L-NAME Incubated Aortic Ring of DipyridamoleTreated), the diabetic rats were treated with low-dose dipyridamole(30 mg/kg/day, p.o., 4 weeks) as mentioned in group IV. The in vitroeffects of wortmannin (100 nM) or L-NAME (100 μM) (the aortic ringwas incubated with either wortmannin or L-NAME for 30-min) onendothelium-dependent and -independent relaxation in the pheny-lephrine (3 × 10−6 M)-precontracted isolated aortic ring preparationwere evaluated. One way ANOVA, followed by Tukey's multiplecomparison test was employed to analyse the data.
STZ-induced diabetic rats developed VED and nephropathy in8 weeks. Diabetes mellitus-induced VED was associated with markedreduction in acetylcholine-induced endothelium-dependent relaxa-tion, decrease in aortic and serum nitrite/nitrate concentration, andinduction of oxidative stress and lipid alteration. Scanning electronmicroscopic and histological studies on thoracic aorta revealed amarked impairment in vascular endothelial integrity. Moreover,elevation of serum creatinine and blood urea nitrogen, and inductionof proteinuria accompanying with renal oxidative stress were noted indiabetic rats. However, treatment with low-dose dipyridamolepartially, but substantially prevented aforementioned vascularendothelial and renal abnormalities in diabetic rats without affectingthe elevated glucose concentration. Interestingly, incubation of aorticrings, isolated from dipyridamole-treated diabetic rats, with eitherwortmannin (inhibitor of phosphatidylinositide 3-kinase, PI3-K) or L-NAME (inhibitor of nitric oxide synthase, NOS) markedly abolisheddipyridamole-associated improvement in acetylcholine-inducedendothelium-dependent relaxation (Table 1, Figs. 1 and 2).
To summarize, dipyridamole in low-dose partially, but significantlyprevents diabetes mellitus-induced VED by activating endothelial PI3-K-eNOS-NO signalling pathways. The renovascular reduction ofoxidative stress might explain the mechanism pertaining to thepartial renoprotective action of low-dose dipyridamole in diabetesmellitus.
We express our gratitude to the management of RITS, Sirsa, Haryana,India for the support. The authors of this manuscript have certified that
⁎ Corresponding author at: Department of Pharmacology, RITS, Sirsa 125 055, India.E-mail address: [email protected] (D. Khanna).
Table 1Effect of low-dose dipyridamole on serum glucose, total cholesterol (TC) and kidney weight/body weight ratio (KW/BW) in diabetic rats.
Assessments Normal Control Diabetic Control Dipyridamole per se Dipyridamole Treated
Serum glucose (mg/dl) 92.26 ± 6.39 277.47 ± 30.23a 96.45 ± 8.27 272.94 ± 18.67Serum TC (mg/dl) 53.55 ± 4.52 95.87 ± 6.76a 55.13 ± 5.32 65.78 ± 9.42b
KW/BW (mg/g) 4.8 ± 0.44 6.88 ± 0.23a 4.7 ± 0.16 5.38 ± 0.63b
530 Letters to the Editor

they comply with the Principles of Ethical Publishing in the InternationalJournal of Cardiology.
References
[1] Kim HH, Liao JK. Translational therapeutics of dipyridamole. Arterioscler ThrombVasc Biol 2008;28:39–42.
[2] Venkatesh PK, Pattillo CB, Branch B, et al. Dipyridamole enhances ischaemia-induced arteriogenesis through an endocrine nitrite/nitric oxide-dependent path-way. Cardiovasc Res 2010;85:661–70.
[3] Balakumar P, Chakkarwar VA, Singh M. Ameliorative effect of combination ofbenfotiamine and fenofibrate in diabetes-induced vascular endothelial dysfunctionand nephropathy in the rat. Mol Cell Biochem 2009;320:149–62.
[4] Balakumar P, Chakkarwar VA, Krishan P, Singh M. Vascular endothelial dysfunction:a tug of war in diabetic nephropathy? Biomed Pharmacother 2009;63:171–9.
[5] Khajehdehi P, Roozbeh J, Mostafavi H. A comparative randomized and placebo-controlled short-term trial of aspirin and dipyridamole for overt type-2 diabeticnephropathy. Scand J Urol Nephrol 2002;36:145–8.
[6] Ye Y, Lin Y, Perez-Polo R, et al. Enhanced cardioprotection against ischemia-reperfusion injury with a dipyridamole and low-dose atorvastatin combination. AmJ Physiol Heart Circ Physiol 2007;293:813–8.
0
20
40
60
80
100
Dip Treated
L-NAME IncubatedAortic Ring of DipyridamoleTreated
Dip per se
Normal Control Diabetic Control
Wortmannin IncubatedAortic Ring of DipyridamoleTreated
aa
a
ab
b
b
b
b
a
c
c
c
c
cd
d
d
d
d
% P
reco
ntra
ctio
n
8 7 6 5 4-log M (Ach) 0
5
10
15
20
a
b
Aor
tic
Nit
rite
/ Nit
rate
(µ
mol
/mg
of p
rote
in )
0
5
10
15
20
a
b
Dipyridamole Treated
Dipyridamole per se
Normal Control
Diabetic Control
Seru
m N
itri
te/N
itra
te (
µ m
ol/ L
)
A B
DCC
BA
D
0
20
40
60
80
100
Dip Treated
L-NAME IncubatedAortic Ring of DipyridamoleTreated
Dip per se
Normal Control Diabetic Control
Wortmannin IncubatedAortic Ring of DipyridamoleTreated
% P
reco
ntra
ctio
n
8 7 6 5 4-log M (SNP)
a
b
c d
e f
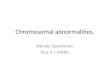
Fig. 1. Effect of low-dose dipyridamole on acetylcholine (Ach)-induced endothelium-dependent (a) and sodium nitroprusside (SNP)-induced endothelium independent (b)relaxation of aorta (in all figures and in the table, all values were represented as mean ± S.D., a = p b 0.05 vs Normal Control; b = p b 0.05 vs Diabetic Control; c = p b 0.05 vsDipyridamole Treated), on aortic nitrite/nitrate concentration (c), on serum nitrite/nitrate (d), on the integrity of vascular endothelium of aorta (e), the scanning electronmicroscopic study was performed to examine the integrity of vascular endothelium of the rat thoracic aorta using Zeiss EVOMA-10 scanning electron microscope (scalebar = 20 μm). (A) Normal Control; (B) Diabetic Control; (C) Dipyridamole per se; (D) Dipyridamole Treated, on the integrity of vascular endothelial layer of aorta (f). The histologicalexamination was performed using Motic Microscope BA310 (Motic, USA) in diabetic rats.
531Letters to the Editor

0167-5273/$ – see front matter © 2014 Elsevier Ireland Ltd. All rights reserved.http://dx.doi.org/10.1016/j.ijcard.2014.01.053
ab
c d e
0
5
10
15
20
a
b
Dipyridamole Treated
Dipyridamole per se
Normal Control
Diabetic Control
Seru
m T
BA
RS
(µ m
ol/L
)
0.0
0.5
1.0
1.5
2.0
a
b
Dipyridamole Treated
Dipyridamole per se
Normal Control
Diabetic Control
Seru
m C
reat
inin
e (m
g/dL
)
0
20
40
60
80
a
b
Dipyridamole Treated
Dipyridamole per se
Normal Control
Diabetic Control
Blo
od U
rea
Nit
roge
n (m
g/dL
)
0
10
20
30
40
a
b
Dipyridamole Treated
Dipyridamole per se
Normal Control
Diabetic Control
Mic
ropr
otei
nuri
a (m
g/24
hrs
)
0
100
200
300
a
b
Dipyridamole Treated
Dipyridamole per se
Normal Control
Diabetic Control
Ren
al T
BA
RS
(nan
omol
/g w
et t
issu
e w
t)
Fig. 2. Effect of low-dose dipyridamole on serum TBARS (a), on serum creatinine (b), on blood urea nitrogen (c), on microproteinuria (d) and on renal TBARS (e) in diabetic rats.
532 Letters to the Editor