Embed Size (px)
Citation preview

Pediatr Nephrol (1991) 5:220-224 �9 IPNA 1991 Pediatric
Nephrology
Original article
Low-dose and heparin-free hemodialysis in children
Denis F. Geary, Mukesh Gajaria, Susan Fryer-Keene, and Jan Willumsen
Division of Nephrology, Department of Pediatrics, The Hospital for Sick Children, 555 University Avenue, Toronto, Ontario, Canada M5G 1X8
Received May 10; received in revised form September 6; accepted September 13, 1990
Abstract. Successful heparin-free hemodialysis has been reported in adults but not in children. A preliminary study was carried out to determine whether heparin-free he- modialysis was possible in children who were considered to have a high risk of bleeding, and if so, to identify the children in whom this technique might be expected to succeed. Of 28 heparin-free procedures, 21 (75%) were successful, a major clot developed in 4, and a minor clot occurred in 3. These children were 6 .76+4.57 years old and weighed 20.7_+ 11.3 kg. An activated clotting time (ACT) of less than 170 s was recorded in five of the six patients in whom clotting was observed (normal value 146 s with a range of 110-180 s). In a second prospective study, low-dose heparin was prescribed for patients with an ACT of less than 170 s, while the remaining children again underwent heparin-free dialysis. In this study only those patients with double-lumen vascular access and a predialy- sis systolic blood pressure greater than 80 m m H g were included. Their mean age was 12.25 _+4.61 years and their weights 32 .9+ 19.3 Kg. In 28 of 31 (90%)procedures, no clotting was observed. Minor clotting developed during the remaining 3 procedures, all in one child who weighed 8.5 kg (the only child weighing less than 10 kg). Heparin (9.6-+ 3.2 IU/kg body weight per hour) was administered during 18 successful procedures. This study shows that heparin-free hemodialysis is possible in children, particu- larly, but not exclusively, those with a coagulopathy. Clot- ting may be anticipated in children weighing less than 10 kg and in those in whom the ACT falls below 170 s. Heparin (10 IU/kg per hour) is recommended for these patients.
Introduction
Hemodialysis without anticoagulation has been performed in adults since 1979 [1] and appears to involve less risk of
Offprint requests to: D. F. Geary
hemorrhage than conventional regional heparinization [2, 3]. However, reports of heparin-free hemodialysis have recommended the use of blood flow rates that cannot be achieved in most children [2, 3]. This paper reports two studies undertaken to determine whether heparin-free he- modialysis could be performed in children.
The preliminary study investigated the feasibility of heparin-free hemodialysis in children and attempted to identify patients in whom the procedure is unlikely to succeed. The subsequent prospective study was designed to determine if low-dose heparin would allow completion of dialysis in those patients in whom clotting might other- wise be expected to occur.
Patients and methods
All children were dialyzed in the dialysis or intensive care units at The Hospital for Sick Children.
Preliminary study. All patients in the study required hemodialysis and were at increased risk of hemorrhage. They underwent dialysis pro- cedures in which heparin was not administered unless clotting was ob- served in the extra corporeal circuit. A dialysis procedure was defined as successful if it was completed within 15 rain of the prescribed time without heparin administration. It was defined as failed if dialysis could not be completed as prescribed without heparin, or the extracorporeal system clotted.
Urea, creatinine, platelets, prothrombin time (normal <13.5 s), and partial thromboplastin time (normal <40 s) were measured before and immediately after dialysis. Activated clotting time (ACT, Hemochron, International Technidyne, Edison, N. J.) was measured 5 min after starting dialysis and every 30 rain throughout the procedure. The normal value for the ACT using this method is 146 s (range 110-182 s).
Mean values for patients who successfully completed dialysis and those who did not were analyzed using the unpaired Student's t-test. The outcome for patients whose ACT was greater than 170 s compared with those with a lower ACT was analyzed by Fisher's exact test. AP value of less than 0.05 was considered statistically significant.
Prospective study. All children with increased risk of hemorrhage who required hemodialysis were eligible for study. However, based on infor- mation obtained in the preliminary study, the following patients were excluded:
1. Those with a single-lumen access line

Table 1. Preliminary study: clinical features and dialysis procedures
221
Patient No. of Age Weight Diagnosis Bleeding Coagulation Vascular Blood flow ACT no. pro- (years) (kg) risk disturbance access (ml/min) <170 s
cedures
Heparin Success
1 1 0.56 8.0 Hepatorenal Post liver Yes Hickman 20 1/1 0 0 failure transplant 10F (long,
single-lumen)
2 1 14.89 62.0 CRF Post No Quinton 250 1/1 0 0 nephrectomy Permcath
(adult)
3 5 6.93 14.3 CRF CVA 2/5 Cooke 12F 65- 80 2/3 0 3/5 TPN line
4 6 12.56 34.0 Hepatorenal Post liver Yes Mahurkar 110-175 2/6 0 4/6 failure transplant 10F
(femoral)
5 3 4.68 15.0 CRF Post-transplant Yes Cooke 12F 50 1/3 0 3/3 nephrectomy TPN line
6 4 1.40 10.0 ATN Post laparotomy Yes Mahurkar 32- 75 3/4 0 4/4 - sepsis 10F (femoral)
7 5 6.14 20.0 ATN Post cardiac Thrombo Mahurkar 75 1/5 0 4/5 b surgery cytopenia a 10F
4/5 (femoral)
8 3 6.64 25.0 CRF Post-transplant Yes Quinton 80-110 1/3 0 3/3 nephrectomy permcath
(pediatric)
ACT, Activated clotting time; CRF, chronic renal failure; ATN, acute tubular necrosis; CVA, cerebrovascular accident a Normal prothrombin time (PT) and partial thromboplastin time (PTT) b The occasion when platelet count was normal and ACT <170, clotted
2. Those with a double-lumen access line through which flow rates sufficient to provide a urea clearance of 3 ml/kg body weight per min could not be achieved
3. Those with systolic blood pressure less than 80 mmHg at the start of the procedure
The dialyzers were primed with 1 1 normal saline and 1,000 IU heparin, drained, and flushed with normal saline. During dialysis they were flushed with normal saline every 30 rain, using 25 ml for patients weighing less than 20 kg and 50 ml for bigger children. ACT was mea- sured 5 rain after starting dialysis and every 30 rain during the procedure. Heparin (10 IU/kg body weight) was administered if the ACT was less than 170 s or if clotting was observed in the extracorporeal circuit. A successful procedure was defined as one in which the dialysis was completed within 15 min of the prescribed time; a failed procedure was one which could not be completed due to clotting.
Urea and creatinine were measured at the beginning and end of each procedure. Mean values for patients who completed dialysis successfully and those who either did not or required heparin were compared using the unpaired Student's t-test. A P value of less than 0.05 was considered significant.
Results
Preliminary study
The diagnoses, the complicat ions placing the children at high risk of bleeding, and some features of their dialyses are listed in Table 1. Twenty-eight hemodialyses were un- dertaken in eight children, who had a mean age of 6 . 7 6 + 4 . 5 7 years and a mean weight of 2 0 . 7 + 1 1 . 3 kg (mean + SD). Al l dialyzers were hollow fiber with
Table 2. Comparison of successful and failed procedures in the prelimi- nary study
Successful Failed P value n=21 n= 7
PT (s) 17 --+4 15 -+2 0.57 PTT (s) 58 -+29 48 -+20 0.49 Platelets 92 + 96 110 -+96 0.72 Hct (%) 28 -+6 28 -+6 0.89 ACT (Hemochron) 231 -+ 97 170 -+ 7 0.14 Weight (kg) 21 -+9 27 -+ 18 0.22 A Urea (%) 39-+18 24_+13 0.12 Blood flow (ml/min) 79 -+44 120 _+92 0.12 Systolic BP (mmHg) 112 -+24 120 _+23 0.45 UF (ml/kg per rain) 0.39-+0.22 0.30_+0.13 0.36
Hct, Hematocrit; BE blood pressure; UF, ultra filtrate
PMMA, PAN, or polysulfone membranes . D o u b l e q u m e n central venous (12-F TPN line [Cook Inc., B loomington Indiana], Pediatric or adult Permcaths [Quinton Ins t rument Co., Seattle Washington]) or femoral (Mahurkar 10 F [Quinton Ins t rument Co., Seattle Washingron]) l ines were used in 27 of the 28 procedures. A long, s ingle- lumen Hickman 10-F central venous line was used in the only patient weighing less than 10 kg.
Dialysis was completed successfully without heparin in 21 (75%) procedures. Of the 7 failed procedures, a major clot prevent ing retransfusion developed in 4 and a minor clot in 3. A major clot developed in the only patient who
222
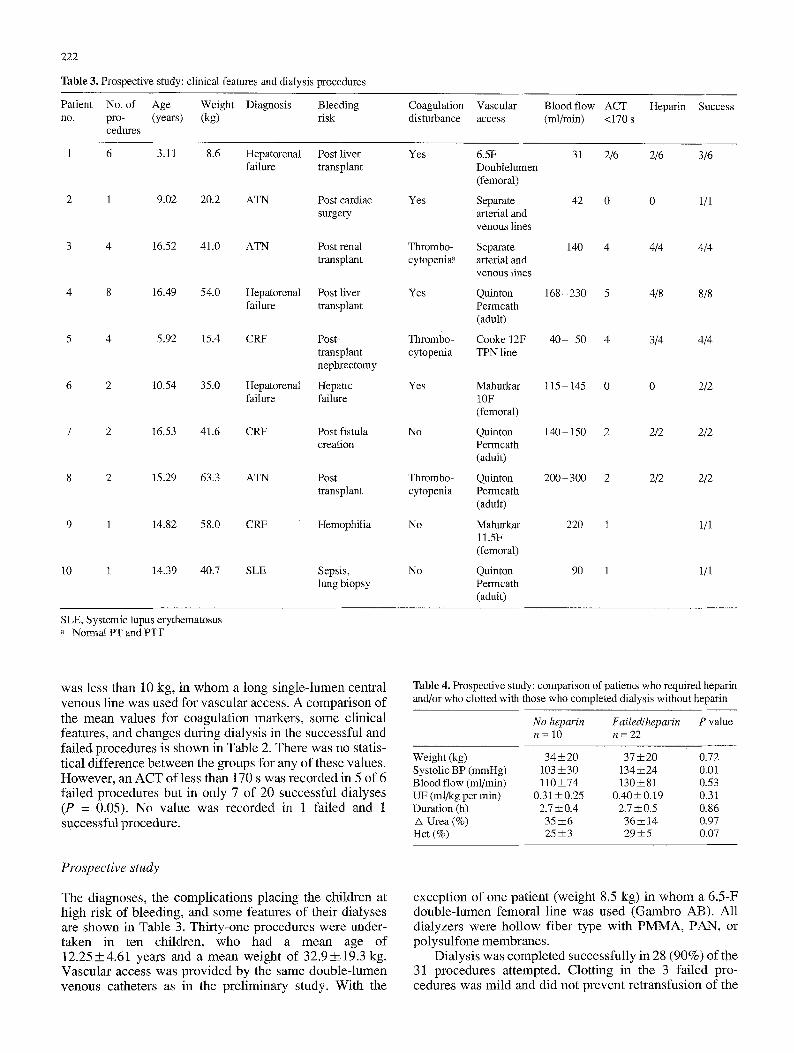
Table 3. Prospective study: clinical features and dialysis procedures
Patient No. of Age Weight Diagnosis Bleeding no. pro- (years) (kg) risk
cedures
Coagulation Vascular Blood flow ACT Heparin disturbance access (ml/min) <170 s
Success
1 6 3.11 8.6 Hepatorenal Post liver failure transplant
2 1 9.02 20.2 ATN Post cardiac surgery
3 4 16.52 41.0 ATN Post renal transplant
4 8 16.49 54.0 Hepatorenal Post liver failure transplant
5 4 5.92 15.4 CRF Post- transplant nephrectomy
6 2 1054 35.0 Hepatorenal Hepatic failure failure
7 2 16.53 41.6 CRF Post fistula creation
8 2 15.29 63.3 ATN Post transplant
9 1 14.82 58.0 CRF Hemophilia
10 1 14.39 40.7 SLE Sepsis, lung biopsy
Yes 6.5F 31 2/6 2/6 3/6 Doublelumen (femoral)
Yes Separate 42 0 0 1/1 arterial and venous lines
Thrombo- Separate 140 4 4/4 4/4 cytopenia ~ arterial and
venous lines
Yes Quinton 168 -230 5 4/8 8/8 Permcath (adult)
Thrombo- Cooke 12F 40- 50 4 3/4 4/4 cytopenia TPN line
Yes Mahurkar 115 - 145 0 0 2/2 10F (femoral)
No Quinton 140-150 2 2/2 2/2 Permcath (adult)
Quinton 200 - 300 2 Permcath (adult)
Mahurkar 220 1 11.5F (femoral)
Quinton 90 1 Permcath (adult)
Thrombo- 2/2 2/2 cytopenia
No 1/1
No 1/1
SLE, Systemic lupus erythematosus a Nomlal PT and PTT
was less than 10 kg, in w h o m a long s ing le- lumen central venous l ine was used for vascular access. A compar i son o f the mean values for coagula t ion markers , some c l in ica l features, and changes during d ia lys is in the successful and fa i led procedures is shown in Table 2. There was no statis- t ical d i f ference be tween the groups for any of these values. However , an A C T of less than 170 s was recorded in 5 of 6 fa i led procedures but in only 7 o f 20 successful d ia lyses (P = 0.05). No va lue was recorded in 1 fa i led and 1 successful procedure .
Prospective study
The diagnoses , the compl ica t ions p lac ing the chi ldren at h igh r isk of b leeding , and some features o f their d ia lyses are shown in Table 3. Thi r ty-one procedures were under- taken in ten chi ldren, who had a mean age o f 1 2 . 2 5 + 4 . 6 1 years and a mean weight of 32.9--+19.3 kg. Vascu la r access was p rov ided by the same doub le - lumen venous catheters as in the p re l iminary study. W i t h the
Table 4. Prospective study: comparison of patients who required heparin and/or who clotted with those who completed dialysis without heparin
No heparin Failed/heparin P value n= 10 n=22
Weight (kg) 34 ___ 20 37 + 20 0.72 Systolic BP (mmHg) 103 --+30 134_+24 0.01 Blood flow (ml/min) 110-+74 130-+81 0.53 UF (ml/kg per min) 0.31-+0.25 0.40-+0.19 0.31 Duration (h) 2.7 -+0.4 2.7 -+ 0.5 0.86 /x Urea (%) 35 -+6 36-+ 14 0.97 Hct (%) 25 -+3 29 -+5 0.07
except ion o f one pat ient (weight 8.5 kg) in whom a 6 .5-F doub le - lumen femora l l ine was used (Gambro AB). A l l d ia lyzers were ho l low f iber type with P M M A , PAN, or po lysu l fone membranes .
Dia lys i s was comple ted successful ly in 28 (90%) of the 31 procedures at tempted. Clot t ing in the 3 fa i led pro- cedures was mi ld and did not p revent re t ransfus ion of the

223
patient. All 3 episodes occurred in the smallest child (weight 8.5 kg) with the smallest vascular access (6.5 F double-lumen) and all 3 took place after at least 2 h of dialysis had been completed. In 18 of the 28 successful procedures heparin was administered because the ACT was less than 170 s; the mean dose used was 9.6+_3.2 IU/kg body weight per hour. Table 4 compares some clinical features as well as the procedures used in successful and failed dialyses and those requiring heparin.
Discussion
The early success with heparin-free hemodialysis in adults who were considered to be at high risk of bleeding compli- cations has been confirmed in recent studies [2-4]. How- ever, no information is available on the use of heparin-free hemodialysis in children. Furthermore, no guidelines are available to indicate which children might require heparin or what the minimal heparin requirement might be. Success rates of 90% have been reported using heparin- free hemodialysis in adults [3], and 98% of procedures may be completed successfully if low-dose heparin is added once early clotting is observed. Success rates of this magnitude would not be anticipated in children because of lower blood flow rates and smaller vascular access cannulae. Nonetheless, the results of our preliminary study show that, although clotting did occur in 25% of pro- cedures. Heparin-free hemodialysis is possible in most children, particularly those with a coexistent coagulopathy.
The occurrence of clotting in five of six children whose predialysis ACT was less than 170 s during the preliminary study suggests that this level of ACT may be used as a cut-off point below which heparin should be administered. This principle was applied in the prospective study and clotting was completely prevented in 90% of patients; when it did occur it was minor, did not prevent retranfu- sion, and did not develop until at least 2 h of dialysis had been completed. An ACT value of 170 s is approximately 20% greater than the normal value using the Hemochron method. This regimen is similar to that recommended for adults - that the ACT for controlled or tight heparinization be kept at 1.25 times the baseline value [5]. For patients with a coagulopathy, in whom the ACT is increased, the use of heparin is seldom necessary.
The dose of heparin (10 IU/kg) prescribed for children whose ACT was less than 170 s was chosen arbitrarily. In our prospective study this resulted in the actual use of a mean dose slightly less than 10 IU/kg body weight per hour, which is much less than the usual recommended heparin dose for pediatric hemodialysis [6, 7]. Therefore we feel it is appropriate to withhold a loading dose of heparin for high-risk hemodialysis patients and to adminis- ter 10 IU/kg of heparin only if the baseline ACT is less than 1.2 times normal. Thereafter ACT values are measured every 30 rain and heparin used as necessary to maintain the ACT greater than 1.2 times the baseline value.
It might be suggested that since the introduction of erythropoietin and the maintenance of higher hematocrit values than were previously observed in children with chronic renal failure, clotting would be more likely when
heparin-free hemodialysis is attempted. However, compar- ison of hematocrit values of our patients who did not re- quire heparin and those who did, or in whom clotting developed revealed no difference. Also, the majority of patients requiting low-dose or heparin-free dialysis have acute renal failure and are not maintained on erythro- poietin. Nonetheless, it has been suggested that blood transfusion be avoided whenever possible during dialysis if heparin use must be restricted [3]. If transfusion is neces- sary, blood should be administered through a peripheral intravenous line.
Anticoagulants other than heparin have been reported to prevent clotting in adults undergoing hemodialysis [8, 9]. However, these agents have been found to cause clinically significant side-effects [9, 10]. Furthermore, we are not aware of any experience with these agents in pedi- atric hemodialysis. The use of regional heparinization has been advocated in children but it is very labor intensive and has had no apparent advantage over low-dose heparin in adults [11]. In addition, hemorrhage may occur postdialy- sis as a rebound effect of the protamine used during re- gional heparinization [ 12].
The use of low-molecular-weight heparin has been re- ported to provide anicoagulation comparable with that achieved using standard heparinization but with potentially fewer side-effects [13]. However, the various available low-molecular-weight heparin fractions have widely vary- ing properties and there is no satisfactory means of meas- uring the in vivo activity of these compounds [14, 15]. This problem must be resolved before low-molecular-weight heparin can be advocated.
In both our preliminary and prospective studies, clot- ting developed most frequently in the two children who weighed less than 10 kg, as might have been expected. Nevertheless, dialysis was successfully completed on 3 oc- casions in one of these children and on another 3 occasions only minor clotting was observed after at least 2 h of dialy- sis. We believe the success in most of our patients resulted to a great degree from the use of double-lumen catheters. Clotting would be more likely with single-lumen catheters because of the degree of recirculation and hemostasis as- sociated with their use. A variety of flexible double-lumen catheters for central venous insertion are available, al- though most are not suitable for use in children less than 15 kg. For children weighing 8 - 15 kg we have used a 12-F double-lumen TPN line, which may also remain in situ for an extended time period. Babies smaller than 8 kg require separate venous and arterial access lines or smaller, semi- rigid double-lumen femoral lines.
Alterations of hemostasis and consumption of platelets, which may be reduced by the use of biocompatible mem- branes, have been reported during hemodialysis [16]. If these effects were increased in heparin-free hemodialysis, a bleeding tendency might be aggravated. However, Casati et al. [4] found little difference in hemostatic markers be- tween patients undergoing low-dose and heparin-free he- modialysis, and concluded that heparin-free hemodialysis is associated with a low risk of extravascular coagulation. This technique did not cause bleeding in our patients who had no pre-existing coagulation disturbance, e.g., post re- nal biopsy or post fistula creation. In the children with an

224
established coagulopathy, e.g., hepatic failure, increased bleeding was not observed. However, because of the sever- ity of the under ly ing bleeding disturbance in m a n y of our patients, this factor could not be precisely evaluated. The use of dialyzers that are maximal ly biocompat ible and are likely to involve min ima l consumpt ion of coagulat ion fac- tors is therefore recommended when low-dose or heparin- free hemodialysis is undertaken.
Acknowledgements. This paper was prepared with the assistance of Medical Publications, The Hospital for Sick Children, Toronto, Canada. Additional editorial assistance was provided by S. Geary.
References
1. Glaser P, Guesde R, Rouby JJ, Eurin B (1979) Haemodialysis without heparin is possible. Lancet II: 579-580
2. Caruana RJ, Raja RM, Bush JV, Kramer MS, Goldstein SJ (1987) Heparin free dialysis: comparative data and results in high risk patients. Kidney Int 31:1351 - 1355
3. Schwab SJ, Onorato JJ, Sharar LR, Denis PA (1987) Hemodialysis without anticoagulation. One-year prospective trial in hospitalized patients at risk for bleeding. Am J Med 83:405 -410
4. Casati S, Moia M, Graziani G, Cantaluppi A, Citterio A, Mannucci PM, Ponticelli C (1984) Hemodialysis without anticoagulants: effi- cacy and hemostatic aspects. Clin Nephrol 21:102-105
5. Sanders PW, Curtis JJ (1986) Management of anticoagulation for hemodialysis. In: Nissenson AR, Fine RN (eds) Dialysis therapy. Mosby, St. Louis, pp 39-41
6. Nevins TE, Mauer SM (1986) Infant hemodialysis. In: Nissenson AR, Fine RN (eds) Dialysis therapy. Mosby, St. Louis, pp 237-240
7. Donckerwolcke RA, Chantler C (1987) Dialysis therapy - he- modialysis. In: Holliday M (ed) Pediatric nephrology, 2nd edn. Wil- liams and Wilkins, Baltimore, pp 799 - 804
8. Pinnick RV, Wiegmann TB, Diederich DA (1983) Regional citrate anticoagulation for hemodialysis in the patient at high risk for bleed- ing. N Engl J Med 308:258-261
9. Zusman RM, Rubin RH, Cato AE, Cocchetto DM, Crow JW, Tolk- off-Rubin N (1981) hemodialysis using prostacyclin instead of he- parin as the sole antithrombotic agent. N Engl J Med 304:934-939 Kelleher SP, Schulman G (1987) Severe metabolic alkalosis compli- cating regional citrate hemodialysis. Am J Kidney Dis 9:235 -236 Swartz RD, Port FK (1979) Preventing hemorrhage in high-risk hemodialysis: regional versus low-dose heparin. Kidney Int 16:513 - 518 Hampers CL, Blanfox ND, Merrill JP (1966) Anticoagulation re- bound after hemodialysis. N Engl J Med 275:776-778 Schrader J, Stibbe W, Armstrong VW, Kandt M, Muche R, K6ster- ing H, Seidel D, Scheler F (1988) Comparison of low molecular weight heparin to standard heparin in hemodialysis/hemofiltration. Kidney lnt 33: 890- 896 Hemker HC (1989) A standard for low molecular weight heparin? Haemostasis 19:1-4 Fareed J, Walenga JM, Hoppensteadt D, Racanelli A, Coyne E (1989) Chemical and biological heterogeneity in low molecular weight heparins: implications for clinical use and standardization. Semin Thromb Hemost 15:440-463 Schmitt GW, Moake JL, Rudy CK, Vicks SL, Hamburger RJ (1987) Alterations in hemostatic parameters during hemodialysis with dialy- zers of different membrane composition and flow design. Platelet activation and factor VIII-related von Willebrand factor during he- modialysis. Am J Med 83:411-418
10.
11.
12.
13.
14.
15.
16.