Embed Size (px)
Citation preview


Low Back Pain (LBP)
Topics covered: What is back pain ? Who gets back pain ? How can you stay Pain-Free ? Treatment approaches Where to go for more information
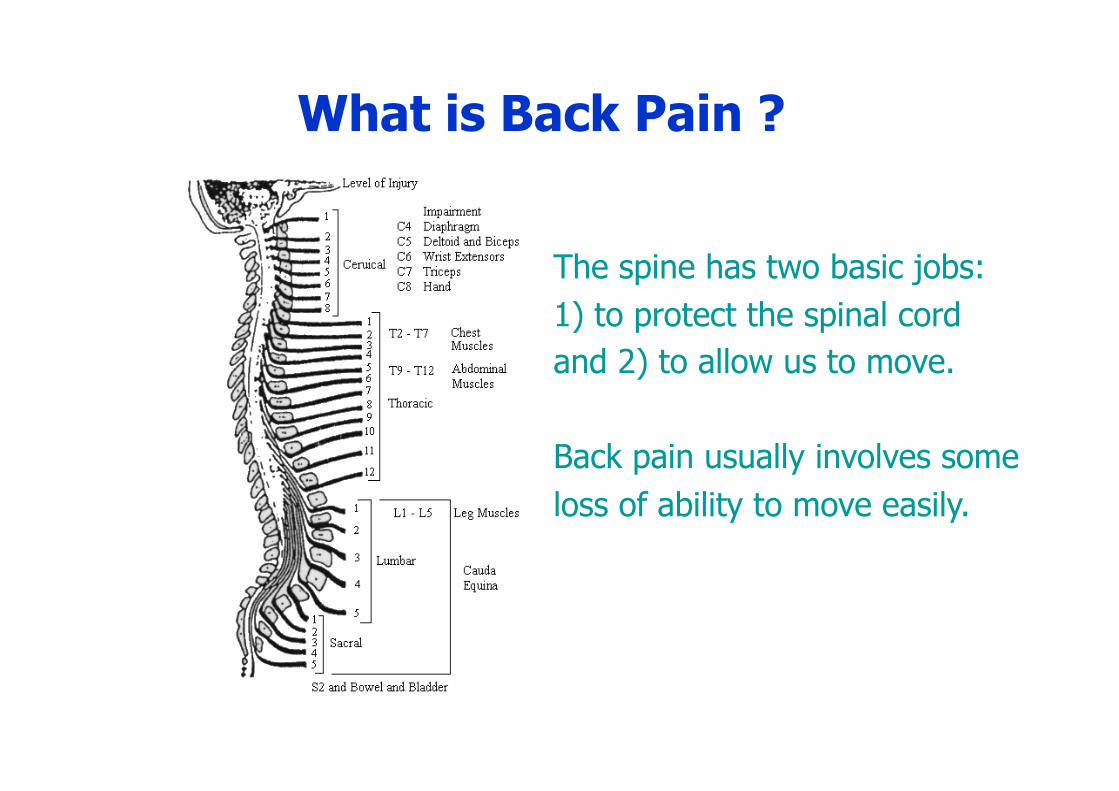
What is Back Pain ?
The spine has two basic jobs: 1) to protect the spinal cord and 2) to allow us to move.
Back pain usually involves some loss of ability to move easily.
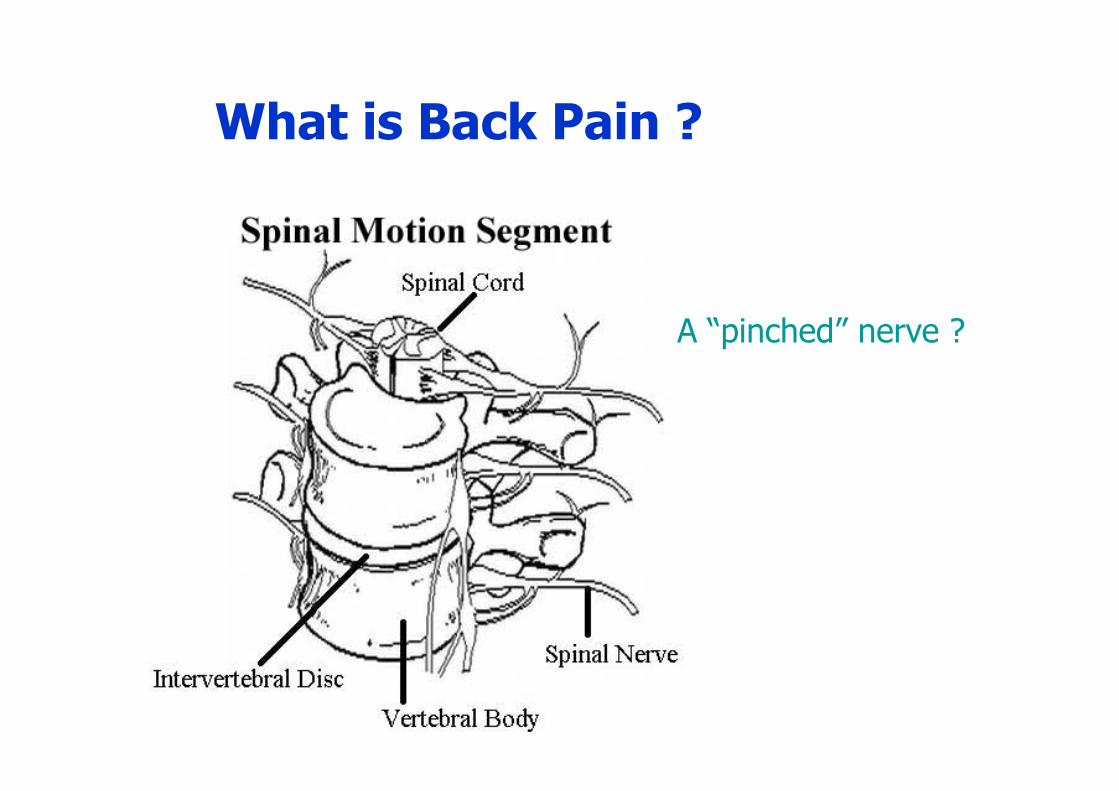
What is Back Pain ?
A “pinched” nerve ?

What is Back Pain ?
A “herniated” disc ?

Most disc herniations occur at L5-S1
At least 30% of the healthy symptomless population have clinically significant disc protrusions (Stadnik et al., 1998).
What is Back Pain ?

What is Back Pain ?
Several studies have shown that there is no correlation between MRI findings and patients’ low back symptoms.
1. Wittenberg et al., 1998 2. Smith et al., 1998
3. Savage et al., 1997

What is Back Pain ?
There are many more joints in the back than discs.
There are many more muscles than joints.
The most common cause of low back pain is when one or more muscles “forget” to relax. We call this a somatic dysfunction.

Common Sources of LBP Somatic dysfunction
Muscle in “spasm”
Nerve root
In somatic dysfunction, some muscles become overactive (“spasm”) and other muscles become inactive.

Joint receptors
vasculature
viscera
Connective tissues
Muscles
Internal organs
Blood vessels
Bones and ligaments
Joint Receptors
Muscle Spindles
Nocioceptors Pressure, temperature
chemical
Humoral Factors circulating hormones (gender-specific response) immune proteins cortisol

Common Sources of LBP
Any dysfunction involving the thoracic or lumbar spine, the sacroiliac joint or the hip can create low back pain.

Common Sources of LBP

Common Sources of LBP Disc 1. posteriorly - sinu vertebral nn. 2. laterally - gray rami communicantes a. branches of ventral rami 3. various types of nerve endings up to ½ annulus depth
Targets for dorsal primary ramus 1. facet joints
2. interspinous ligaments
3. back muscles
VPR
DPR
GRC SVN

Long dorsal si ligament
sacrotuberous ligament
sacrospinous ligament
sciatic nerve
piriformis
Common Sources of LBP

Role of the sacroiliac joint The coxal bones consist of a thin shell of
cortical bone (1-2 mm) over trabecular bone.
Muscles play an important role in helping the pelvis resist stress. When muscles can’t work due to pain, the risk of injury increases.

Role of the sacroiliac joint

The sacroiliac joint requires muscle activity to keep it stable. If muscles can’t work correctly, perhaps because of a somatic dysfunction, the joint becomes unstable and painful.
1
2 3
Role of the sacroiliac joint

Common Sources of LBP

Low Back Pain Topics covered: What is back pain ? Who gets back pain ? How can you stay Pain-Free ? Treatment approaches Where to go for more information
Who gets back pain ? Almost Everybody
Estimates run as high as 80% of the population.
Frequently associated with pregnancy.
Peak occurrence is between age 40 and 60.
Low Back Pain Topics covered: What is back pain ? Who gets back pain ? How can you stay Pain-Free ? Treatment approaches Where to go for more information

How Can You Stay Pain-free ? Have good genes – studies of identical twins show a reasonably strong genetic component to disabling low back pain.
Avoid sudden unintended movements. This is the presumed cause of most cases of somatic dysfunction.
Maintain good posture. A spine that is too flat or too curved increases stress on all the joints and the discs.
Exercise regularly and moderately.
Have regular check-ups by your physical therapist, to find and fix somatic dysfunctions before they cause bigger problems.

How Can You Stay Pain-free ?
Avoid sudden unintended movements. This is the presumed cause of most cases of somatic dysfunction.
A sudden movement: 1) creates a quick stretch on muscles and joints 2) increases pressure on discs 3) increases sensory stimulus to the spinal cord
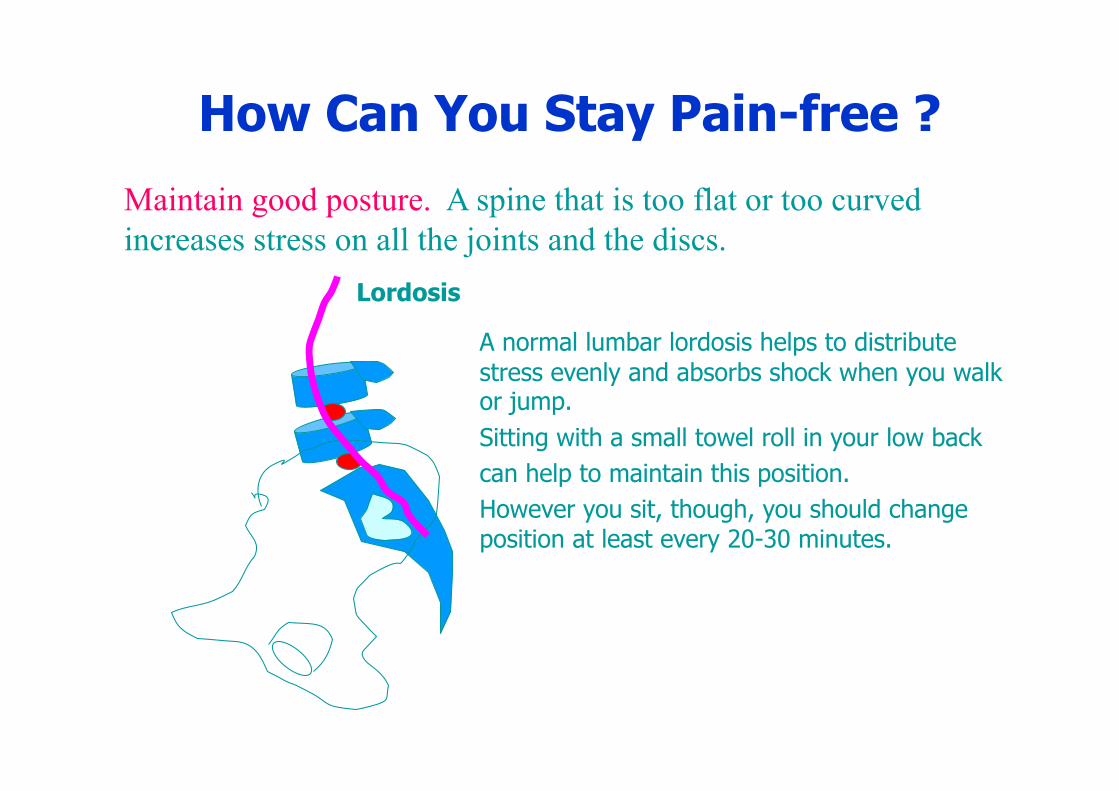
How Can You Stay Pain-free ? Maintain good posture. A spine that is too flat or too curved increases stress on all the joints and the discs.
Lordosis
A normal lumbar lordosis helps to distribute stress evenly and absorbs shock when you walk or jump. Sitting with a small towel roll in your low back can help to maintain this position. However you sit, though, you should change position at least every 20-30 minutes.

How Can You Stay Pain-free ?
Exercise regularly and moderately.
Begin slowly.
Don’t try to do too much at once.
Pick a good time.
Watch what you eat.
During the first hour after waking, the spine is 3 times as stiff because discs have swelled overnight (Adams et al., 1987). You should delay exercise for an hour or two after you wake up.

How Can You Stay Pain-free ?
Have regular check-ups by your physical therapist, to find and fix somatic dysfunctions before they cause bigger problems.
Everyone knows it’s important to have regular check-ups at the dentist to prevent little problems from becoming big ones.
Why is your spine any different ?
Regular spine health check-ups can prevent little problems from turning into big problems later.

Low Back Pain Topics covered: What is back pain ? Who gets back pain ? How can you stay Pain-Free ? Treatment approaches Where to go for more information

Adequate treatment must address all the factors involved in producing pain.
Adequate treatment starts with a good evaluation. A good evaluation must include an examination of muscle function.
Treatment Approaches

Treatment Approaches In general, treatment will involve three phases.
The process is known as “rehabilitation.”
1) Phase 1 a) identify and treat somatic dysfunctions.
2) Phase 2 - identify and treat specific muscle insufficiencies using a) exercise b) movement re- education).
3) Phase 3 - identify and treat specific functions needed for return to activity.
Treatment Approaches
Although for many years there was no agreement among
health professionals on how to best treat back pain,
there is now some evidence to suggest that this three-pronged
approach is the most effective treatment strategy for most patients.

Treatment Approaches phase 1
1. Effective non-specific techniques:
Hot packs, gentle ROM, mild exercise,
relaxation exercises, stress reduction , biofeedback,
acupuncture, healing touch, thermal ultrasound, PNF,
Craniosacral technique, thrust manipulation
2. Effective specific manual physical therapy techniques:
Muscle Energy, Strain/Counterstrain, Functional Technique,
Myofascial Release, Medical Exercise Therapy , thrust
manipulation.

Treatment Approaches phase 1
All specific manual therapy techniques (Muscle Energy, Counterstrain, Myofascial Release, Functional techniques and specific thrust technique) require the therapist to be well-trained in joint biomechanics.

Thrust techniques
High velocity, low amplitude thrust techniques can be used in the acute stage to correct somatic dysfunctions.
Low velocity joint mobilization techniques can also be used successfully.

Treatment Approaches phase 2
Identify specific muscle insufficiencies remaining from the period of somatic dysfunction.
Hides (1998) - 39 acute LBP patients, all had decreased multifidus size at one level (mostly L5). Randomly assigned to either specific exercise group (multifidus and transversus co-contraction) or general exercise group. Outcomes at 10 weeks identical. However, the multifidus in the general group was smaller than in specific exercise group. One year later, 84% of people in general group had back pain again, compared to only 30% in specific group.

Treatment Approaches phase 3
Identify requirements to return the patient to highest level of function possible.
This may involve providing orthotics to support weak arches, so that walking and running won’t stress the back, or perhaps a high level exercise program to keep the back healthy and pain-free.

Treatment Approaches Surgery Everyone will agree – surgery should be your
last resort.
Schofferman (1992) and Blair (1994), confirmed that psychological factors play a role in success of spinal surgery. Specifically, psychological trauma suffered in childhood negatively influenced the outcome of spinal surgery, regardless of surgical complexity or other medical factors. Among the factors the researchers considered were: physical or psychological abuse by a care-giver, abandonment, and use of drugs or alcohol by care-giver.

Succ
ess
Rat
e (%
)
Risk Factors
Spine Surgery Outcomes
Treatment Approaches Surgery

Back pain resources
Book The Back Pain Revolution Waddell, G. Churchill Livingstone, 1998
Evidence-Based Medicine online Pedro – The Physiotherapy Evidence database http://www.pedro.fhs.usyd.edu.au/
The Cochrane collaboration http://www.cochrane.org/

Back pain resources
Patient Resources online
http://www.mayoclinic.com/invoke.cfm?id=DS00171
http://www.apta.org
http://www.spine-health.com/
http://www.nismat.org/ptcor/lbp/
http://physicaltherapy.about.com/cs/lowbackpain/index.htm

Bechtel, R. 2001 “Physical characteristics of the axial interosseous ligament of the human sacroiliac joint” The Spine Journal 1(4): 255-259.
Blair, J., Blair, R., and Rueckert, P. 1994 “Pre-injury emotional trauma and chronic back pain. An unexpected finding” Spine 19(10): 1144-1147.
Burke, D., Gandevia, S. and McKeon, B.1983 "The afferent volleys responsible for spinal proprioceptive reflexes in man" J. Physiol. 339: 535-52.
Burke, D., Gandevia, S. and McKeon, B. 1988 "Responses to passive movement of receptors in joint, skin and muscle of the human hand" J. Physiol. 402: 347-361.
Cassidy, J. 1992 “The pathoanatomy and clinical significance of the sacroiliac joints” J Manipulative Physiol Ther 15(1): 41-42.
Back pain resources literature

Galm, R., Frohling, M., Rittmeister, M., and Schmitt, E. 1998 “Sacroiliac joint dysfunction in patients with imaging-proven lumbar disc herniation” Eur Spine J 7: 450-453.
Gandevia, S., Wilson, L., Cordo, P., and Burke, D. 1994 “Fusimotor reflexes in relaxed forearm muscles produced by cutaneous afferents from the human hand”. J. Physiol. 479: 499-508.
Gardner-Morse, M., Stokes, I. 1998 “The effects of abdominal muscle co-activatyion on lumbar spine stability” Spine 23(1): 86-92.
Hanten, W. and Chandler, S. 1994 "Effects of myofascial release leg pull and sagittal plane isometric contract-relax techniques on passive straight-leg raise angle” JOSPT 20(3): 138-44.
Back pain resources literature

Hides, J, Richardson, C, Jull, G. 1996 “Multifidus recovery is not automatic after resolution of acute, first-episode low back pain” Spine 21(23): 2763-2769.
Hodges, P., Cresswell, A., and Thorstensson, A. 1999 “Preparatory trunk motion accompanies rapid upper limb movement” Exp Brain Res 124(1): 69-79.
Hubbard, D, and Berkoff, G. 1993 “Myofascial trigger points show spontaneous needle EMG activity” Spine 18(13): 1803-1807.
Koes B, Bouter L, Knipshild P, Mameren H, Essers A, Houben J, Verstegens G, Hofheusers D. 1991 “The effectiveness of manual therapy, physiotherapy and continued treatment by the general practitioner for chronic nonspecific back and neck complaints: design for a randomized clinical trial. J of Manipulative Physiological Therapeutics 14(9): 498-502.
Back pain resources literature
Savage, R., Whitehouse, G., and Roberts, N. 1997 “The relationship between the magnetic resonance imaging appearance of the lumbar spine and low back pain, age and occupation in males” Eur Spine J 6(2): 106-114.
Schofferman, J., Anderson, D., Hines, R., Smith, G., and White, A. 1992 “Childhood psychological trauma correlates with unsuccessful lumbar spine surgery” Spine 17(6 Suppl): S138-144.
Snijders, C., Ribbers, M., deBakker, H., Stoeckart, R., and Stam, H. 1998 “EMG recordings of abdominal and back muscles in various standing postures: validation of a biomechanical model on sacroiliac joint stability” J Electromyogr Kinesiol 8(4): 205-214.
Stadnik, T., Lee, R., Coen, H., Neirynck, E., Buissert, T., and Osteaux, M. 1998 “Annular tears and disk herniation and contrast enhancement on MR images in the absence of low back pain or sciatica” Radiology 206(1): 49-55.
Back pain resources literature

Vilensky, J., O’Connor, B., Fortin, J., Merkel, G., Jiminez, A., Scofield, B., and Kleiner, J. 2002 “Histologic analysis of neural elements in the human sacroiliac joint”. Spine 27(11): 1202-1207.
Weishaupt, D., Zanetti, M., Hodler, J., and Boos, N. 1998 “MR imaging of the lumbar spine: prevalence of intervertebral disk extrusion and sequestration, nerve root compression, end plate abnormalities, and osteoarthritis of the facet joints in asymptomatic volunteers”. Radiology 209(3): 661-666.
Back pain resources literature





























