Embed Size (px)
Citation preview

Long Term Survival of PLHIV
DR Chow TS Infectious Disease Unit Hospital Pulau Pinang
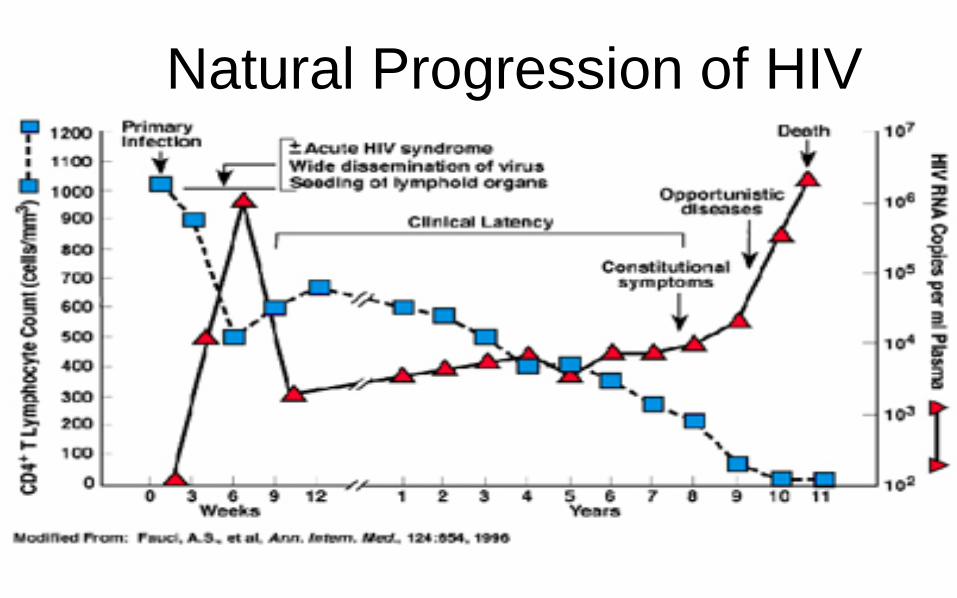
Natural Progression of HIV

Combination ART
cART
• Combination of antiretroviral drugs of at least 3 or more as a regime
• By using
• 2 NRTI plus – 1 NNRTI
– boosted PI.
– INSTI

Goal of Antiretroviral Therapy • Improve quality of life
• Reduce HIV-related morbidity and mortality
• Restore and/or preserve immunologic function
• Maximally and durably suppress HIV viral load
• Prevent HIV transmission

Therapeutic Goal of HAART R
elat
ive
Lev
els
Months Years After HIV Infection
CD4+ T-cells
Plasma HIV Viremia
Acute HIV infection Symptom
Viral Load: Limit of detection
? Long term durability
FIRST LINE FOREVER


MALAYSIA CONSENSUS GUIDELINES ARVT IN ADULT 2016

Current ARV Medications NRTI
Abacavir (ABC)
Didanosine (ddI)
Emtricitabine (FTC)
Lamivudine (3TC)
Stavudine (d4T)
Tenofovir (TDF)
Zidovudine (AZT,
ZDV)
NNRTI
Delavirdine (DLV)
Efavirenz (EFV)
Nevirapine (NVP)
Etravirine (ETR)
Rilpivirine (RPV)
PI
Atazanavir (ATV)
Darunavir (DRV)
Fosamprenavir (FPV)
Indinavir (IDV)
Lopinavir (LPV)
Nelfinavir (NFV)
Ritonavir (RTV)
Saquinavir (SQV)
Tipranavir (TPV)
Integrase Strand
Transfer Inhibitor (INSTI)
Raltegravir (RAL)
Dolutegravir (DTG)
Fusion Inhibitor
Enfuvirtide (ENF, T-20)
CCR5 Antagonist
Maraviroc (MVC)
9
HOW LONG CAN PLHIV SURVIVED WITH ART ?


Expected age of death of 35 year old men with CD4
95% CI (compare to General pop in UK 78 )
<200 71 (68-73)
200-349 78 (74-82)
> 350 77 (72-81)



PLHIV on LONG TERM ART
• More long term morbidity due to ART AE > OI of AIDS
• Need to deal with more NCD as aging is common among PLHIV
Choosing the right ART is important:
– Potent ART
– Toxicity (acute and long term)
– Simplicity (fixed dose combination)

ART accelerates comorbidities e.g. CVD, CKD, fractures
Comorbidities increase complexity of care
– reduce ART adherence
– reduce ART options
– increase in polypharmacy for those age 45+
Reported in only ~25% of initial ART trials, and under-assessed in routine care, so under-appreciated
Gifford et al, JAIDS 2000; DAD study group, AIDS 2010 ; Hasse et al, Clin Infect Dis 2011
Krentz et al. Antiviral Therapy, 2012; Lee et al, ADR Workshop, 2013; Shahmanesh et al, ADR workshop 2013
Choosing a lifelong ART – Considering comorbidities

Concern for Older Pts with ART
• AE from ART and concomitant drugs common
• Polypharmacy is common in older HIV-infected pts – Greater risk of drug–drug interactions
• Bone, kidney, metabolic, cardiovascular, and liver should be monitored closely
Slide credit: clinicaloptions.com DHHS Guidelines. July 2016.

ATHENA and Swiss HIV Cohort Studies: Polypharmacy Among HIV-Infected Pts on ART
• 5.2% of pts 50-64 yrs of age and 14.2% of pts ≥ 65 yrs of age received ≥ 4 meds other than ART
• Predicts that 20% of pts will be receiving ≥ 3 meds other than ART in 2030
Slide credit: clinicaloptions.com 1. Smit M, et al. Lancet Infect Dis. 2015;15:810-818. 2. Hasse B, et al. Clin Infect Dis. 2011:53;1130-1139.
ATHENA Modeling Study[1]
16,000
14,000
12,000
10,000
8000
6000
4000
2000
0
Pe
op
le (
n)
3+ comedications 2 comedications 1 comedication No comedication
2010 2015 2020 2025 2030
Swiss HIV Cohort Study (N = 8444)[2]
Prospective Observational Study
< 50 Yrs 50-64 Yrs ≥ 65 Yrs
100
80
60
40
20
0
Pa
rtic
ipa
nts
(%
)
n = 5761 n = 2233 n = 450
No comedication
1 comedication
2 comedication
3 comedications
4+ comedications

Elderly : ART and comorbidities Scenario Consider Avoiding
CKD (eGFR
< 60 mL/min)
TDF, especially in RTV-
containing regimens
Osteoporosis TDF
CVD risk ABC
Hyperlipidemia
PI/RTV

Key Interactions: Boosted PI- or NNRTI-Containing ART Regimens
Regimen Key Drug–Drug Interactions
Boosted PI
ATV/RTV
LPV/RTV
DRV/RTV
Avoid lovastatin, simvastatin (lipid-lowering agents),
salmeterol (asthma/COPD medication)
Use caution with other lipid-lowering agents (eg, atorvastatin,
rosuvastatin, pravastatin)
Use caution with/avoid specific antiarrhythmics (eg,
amiodarone)
Avoid PPIs (eg, omeprazole) with ATV
RPV Avoid PPIs (eg, omeprazole, pantoprazole), dexamethasone
EFV No notable comedications to avoid for EFV; consider alternative
corticosteroid to dexamethasone
Slide credit: clinicaloptions.com References in slidenotes.
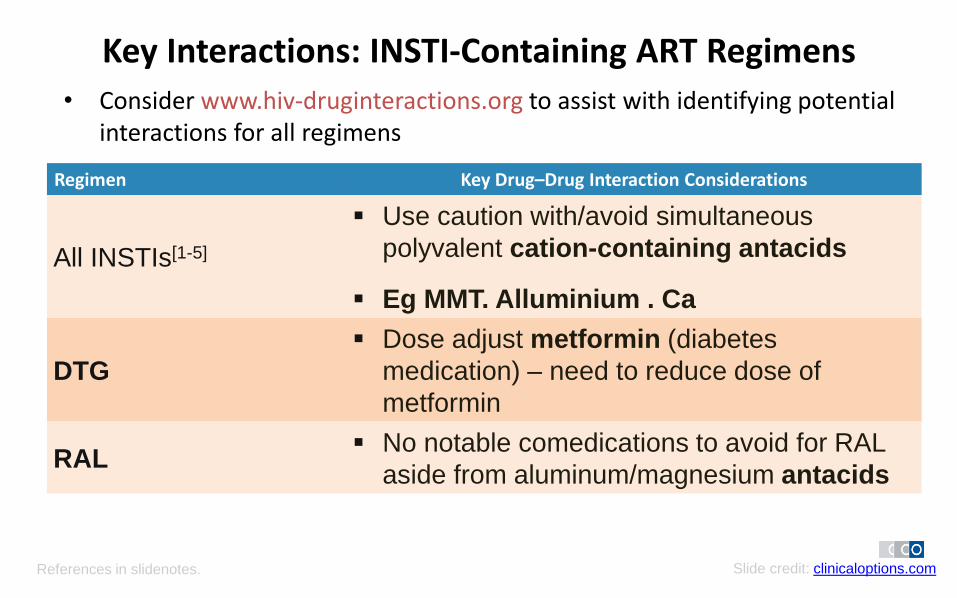
Key Interactions: INSTI-Containing ART Regimens
• Consider www.hiv-druginteractions.org to assist with identifying potential interactions for all regimens
Regimen Key Drug–Drug Interaction Considerations
All INSTIs[1-5]
Use caution with/avoid simultaneous
polyvalent cation-containing antacids
Eg MMT. Alluminium . Ca
DTG
Dose adjust metformin (diabetes
medication) – need to reduce dose of
metformin
RAL No notable comedications to avoid for RAL
aside from aluminum/magnesium antacids
Slide credit: clinicaloptions.com References in slidenotes.

An Aging Population of PLHIV

Decreased Life Expectancy in Older HIV-Positive Adults in Modern ART Era • Population-based cohort study of survival in HIV-infected pts (n = 2440) and
uninfected controls matched by age and sex (n = 14,588) in Denmark
HIV-Negative
Controls
1996-2014
2006-2014
2000-2005
1996-1999
HIV-Positive Pts
1.00
0.75
0.50
0.25
0
Pro
bab
ility
of
Surv
ival
50 60 70 80 Age (Yrs)
Legarth RA, et al. J Acquir Immune Defic Syndr. 2016;71:213-218. Slide credit: clinicaloptions.com

ATHENA: Older Pts Becoming More Prevalent in the HIV-Infected Population
• Observational cohort of 10,278 HIV-infected pts in the Netherlands
• Modeling study projections: – Proportion of HIV-positive
pts ≥ 50 yrs of age to increase from 28% in 2010 to 73% in 2030
– Median age of HIV-positive pts on combination ART to increase from 43.9 yrs in 2010 to 56.6 yrs in 2030
Smit M, et al. Lancet Infect Dis. 2015;15:810-818.
Pro
po
rtio
n o
f H
IV-P
os
itiv
e P
ts
1.0
0.9
0.8
0.7
0.6
0.5
0.4
0.3
0.2
0.1
0 2010 2015 2020 2030 2025
> 70 yrs of age
60-70 yrs of age
50-60 yrs of age
40-50 yrs of age
30-40 yrs of age
< 30 yrs of age
Slide credit: clinicaloptions.com

Comorbidities n 0.68 0.80 1.03 1.15 1.47 0.89 1.35 1.52 1.65 2.04
HIV-negative (n=452)
HIV-positive (n=489)
100
%
80
60
40
20
0
3+ 2 1 0
Significantly more cardiovascular disease, liver disease, renal failure and cancer in HIV+
Comorbidities more common in HIV
Schouten et al. Clin Infect Dis 2014

AGEhIV: Older HIV-Infected Pts at Increased Risk for Multiple Comorbidities
• Cross-sectional analysis of comorbidity prevalence in prospective cohort study of HIV-infected pts (n = 540) vs controls (n = 524) ≥ 45 yrs of age
Schouten J. Clin Infect Dis. 2014;59:1787-1797.
Slide credit: clinicaloptions.com
Pts
(%
)
50
30
20
10
0
40
P < .001
P = .018 P = .008 P = .044
HIV-uninfected pts HIV-infected pts

Factors Related to Non-AIDS Comorbidities in HIV-Infected Pts
Warriner AH, et al. Infect Dis Clin North Am. 2014;28:457-476. Slide credit: clinicaloptions.com
• AGING
• Chronic HIV
infection
• ART toxicity
• HCV and other
coinfections
• Genetics
• Obesity, exercise,
diet, smoking
• Stress
• Depression
Inflammation and
fibrosis
Dyslipidemia
Insulin resistance
Decreased physical
functioning
Cardiovascular
Renal
Metabolic
Functional
Neuropsychiatric
Factors Conditions End Organ
Disease
Is HIV immune activation ? OR immune destruction?
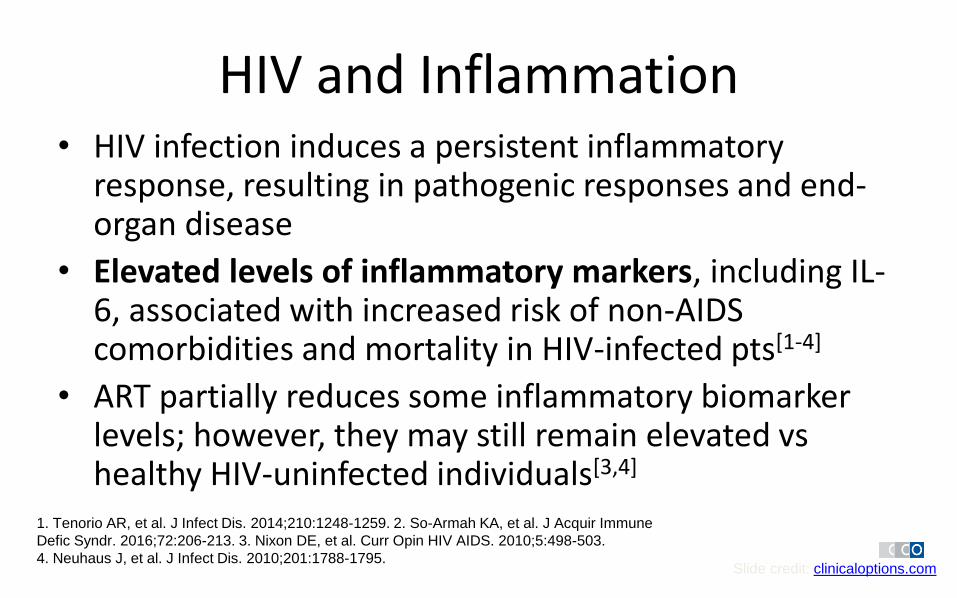
HIV and Inflammation • HIV infection induces a persistent inflammatory
response, resulting in pathogenic responses and end-organ disease
• Elevated levels of inflammatory markers, including IL-6, associated with increased risk of non-AIDS comorbidities and mortality in HIV-infected pts[1-4]
• ART partially reduces some inflammatory biomarker levels; however, they may still remain elevated vs healthy HIV-uninfected individuals[3,4]
Slide credit: clinicaloptions.com
1. Tenorio AR, et al. J Infect Dis. 2014;210:1248-1259. 2. So-Armah KA, et al. J Acquir Immune
Defic Syndr. 2016;72:206-213. 3. Nixon DE, et al. Curr Opin HIV AIDS. 2010;5:498-503.
4. Neuhaus J, et al. J Infect Dis. 2010;201:1788-1795.

Inflammation Associated With Disease in Treated HIV Infection
• Mortality[1-4]
• Cardiovascular disease[5]
• Cancer[6]
• Venous thromboembolism[7]
• Type 2 diabetes[8]
• Radiographic emphysema[9]
• Renal disease[10]
• Bacterial pneumonia[11]
• Cognitive dysfunction[11]
• Depression[13]
• Functional impairment/frailty[14]
References in slidenotes. Slide credit: clinicaloptions.com

Case discussion 2008
– 54-year old man
– Presented with Pneumocystis pneumonia
– CD4 20, VL > 2 million cp/ml
– Underlying HTN, DM (creatinine 80 , clearance 62 ml/min)
– commences ART with TDF/FTC/EFV 2 weeks later
2009 – switched to TDF-FTC + LPV/r because of ongoing CNS side effects of EFV (VL <20)
– CD4 > 350 , plasma HIV RNA always <20 copies/mL
– Dev chronic diarrhoea but “not too bad” (no LOW)
2017 (now 63 year old man) smoker , BMI 30 TG 14.3 , Total Choleterol 6.4, HDL 0.8
FBS 9.8
BP 160/90
Creatinine 80 ---- 150 umol/ml (creatinine clearance = 62 declined to 45ml/min )

Current Medication:
• ART: TDF/FTC/LPV/r
• HTN : perindropril 4 mg OD , amlodipine 10 mg OD
• Hyperlipidemia: Atorvastatin 60 mg ON and Lipanthyl penta 145 mg ON
• DM: Metformin 1 gm BD , Gliclazide 80 mg BD
Total medicine = 8 types

What is the issue here ?
1. Aging
2. CKD
3. Hyperlipidemia (Cholesterol and TG)
4. DM uncontrolled
5. HTN uncontrolled
6. Increased ASCVD risk
7. Bone health

HIV and CVD , HTN

CVD Mortality Higher in HIV-Infected (Even With Virologic Suppression)
• Analysis of CVD-related mortality in HIV-infected pts in New York City HIV Surveillance Registry 2001-2012 (N = 145,845)
– 71% male; median age: 49 yrs
• From 2001-2012, CVD mortality increased in HIV-infected pts (from 6% to 15%) while decreasing in the general population
• Age-adjusted rate of CVD mortality markedly decreased for HIV-infected pts with virologic suppression
– HIV-1 RNA ≥ 400 copies/mL, 8.02/1000 PY
– HIV-1 RNA < 400 copies/mL, 3.99/1000 PY
– General population, 3.22/1000 PY
Slide credit: clinicaloptions.com Hanna DB, et al. Clin Infect Dis. 2016;63:1122-1129.

HIV Infection
ARV
*Metabolic syndrome ARV: antiretroviral therapy; hs-CRP: high-sensitivity C-reactive protein Adapted from Carr A. Clinical Care Options HIV. Available at: www.clinicaloptions.com/hiv
CVD Risk Factors in the
HIV Population
Gender
CVD Risk
- -
Diabetes
Lipids*
Family History
Abdominal Obesity*
Hyper- tension*
Cigarette Smoking
Hyper-glycemia* Insulin
Resistance
Inactivity, Diet
Age
Orange = Modifiable Green = Non-modifiable Purple = HIV-associated
hs-CRP?

Hypertension is more prevalent HIV-Infected Pts
• Analysis of HTN in HIV-infected pts in UNC CFAR HIV Clinical Cohort, 1996-2013 (N = 3141)[1]
• Hypertension incidence
– 1996: 1.68 cases/100 PY
– 2013: 5.35 cases/100 PY
• Key risk factors
– Age
– Obesity
– Diabetes
– Renal insufficiency
– Nadir CD4+ cell count < 500 cells/mm3
• Analysis of HTN in HIV-infected (n = 527) and HIV-uninfected (n = 517) persons in AGEhIV cohort[2]
• HTN rate higher among HIV-infected vs HIV-uninfected persons
– 48% vs 36%; aOR: 1.65; 95% CI: 1.25-2.19
Slide credit: clinicaloptions.com 1. Okeke NL, et al. Clin Infect Dis. 2016;63:242-248.
2. van Zoest RA, et al. Clin Infect Dis. 2016;63:205-213.

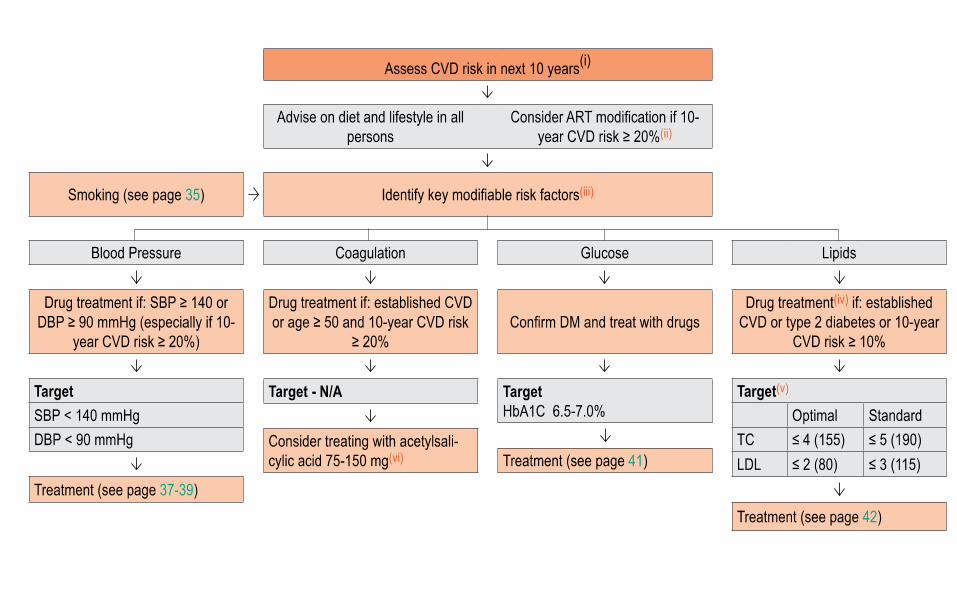
LIPID: To Treat or Not To Treat ASCVD Risk Estimator
Slide credit: clinicaloptions.com tools.acc.org/ASCVD-Risk-Estimator/.
Consider High Intensity Statin and Aspirin
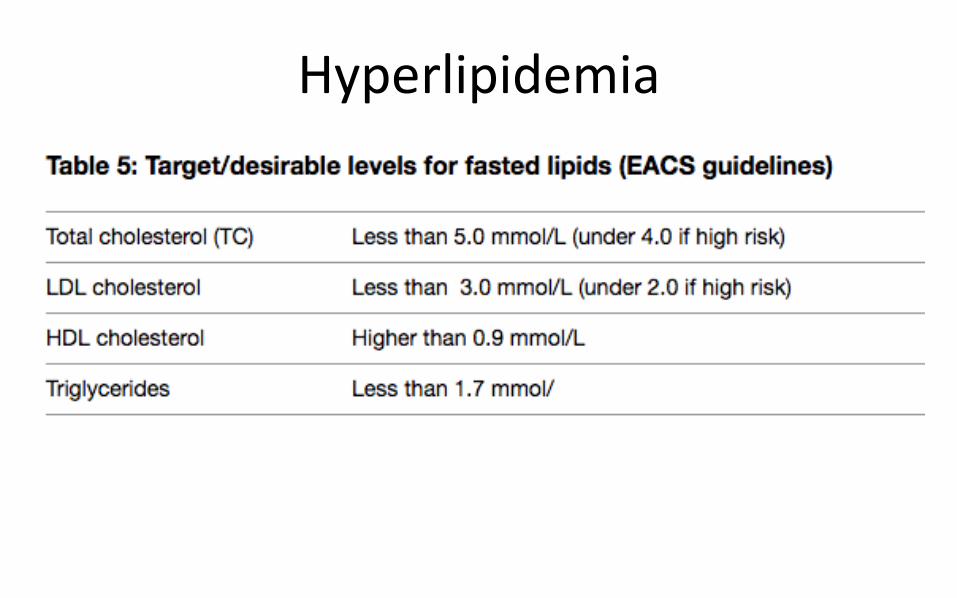
Hyperlipidemia


Approach to HIV+ on ART with high ASCVD risk
Slide credit: clinicaloptions.com
Observation Recommendations
HIV-infected pts have
increased CVD risk
Virologic suppression can reduce CVD risk
Controlling other metabolic comorbidities (many of which occur
more frequently in HIV-infected pts) can also reduce the risk of
CVD
HTN, T2DM, CKD, lipid abnormalities
Lifestyle modification (exercise, diet, smoking cessation) may
also reduce risk
ART can increase
dyslipidemia
Manage lipids with statin therapy; consider potential DDIs with
boosted PI- or COBI-containing regimens
Numerous challenges exist
in treating HIV infection in
aging pts
Assess comorbidities and potential interplay with ART
regimens
Bone, lipid, or cardiovascular abnormalities can be
exacerbated by specific therapeutics
Consider polypharmacy and potential DDIs

Approach to Lipid-Lowering (Statin) Therapy
Slide credit: clinicaloptions.com
• HIV-infected patients are at increased risk for ASCVD[1,2]
– ART can cause increases in triglycerides and total, VLDL, LDL, and HDL cholesterol
• Prescribing statins can be challenging due to DDIs, insulin resistance, adverse events, and increased pill burden[1]
Aspect of Statin Therapy Recommendation
Goal of therapy CVD risk reduction[1]
Screening
A fasting lipid panel should be obtained in all newly diagnosed HIV-infected
pts[1,3]
Lipid screening annually[3]
Treatment
Statin therapy is first-line therapy for elevated LDL-C and non-HDL-C[1]
Moderate- or high-intensity statin therapy should be considered[1]
Lifestyle therapy is the recommended first step[4]
Other Patient-provider discussion is central to decisions on drug treatment[1]
References in slidenotes.

Slide credit: clinicaloptions.com Dubé MP. Lipid management. 2015. p. 241-255.
PI- or COBI-Containing Regimens
High-Intensity Statin Moderate-Intensity Statin Low-Intensity Statin
Atorvastatin 20 mg Atorvastatin 10 mg Pravastatin 10-20 mg
Rosuvastatin 10-20 mg Rosuvastatin 5 mg Fluvastatin 20-40 mg
Pravastatin 40-80 mg*
Simvastatin and lovastatin are contraindicated for pts receiving a PI, COBI, and/or RTV
*With darunavir, reduce pravastatin to 20-40 mg
NNRTI-, RAL-, or DTG-Containing Regimens
High-Intensity Statin Moderate-Intensity Statin Low-Intensity Statin
Atorvastatin 40-80 mg Atorvastatin 10-20 mg Pravastatin 10-20 mg
Rosuvastatin 20 mg Rosuvastatin 10 mg Fluvastatin 20-40 mg
Pravastatin 40-80 mg
Lovastatin 40 mg Lovastatin 20 mg
Simvastatin 20-40 mg Simvastatin 10 mg
Suggested Statins with ART
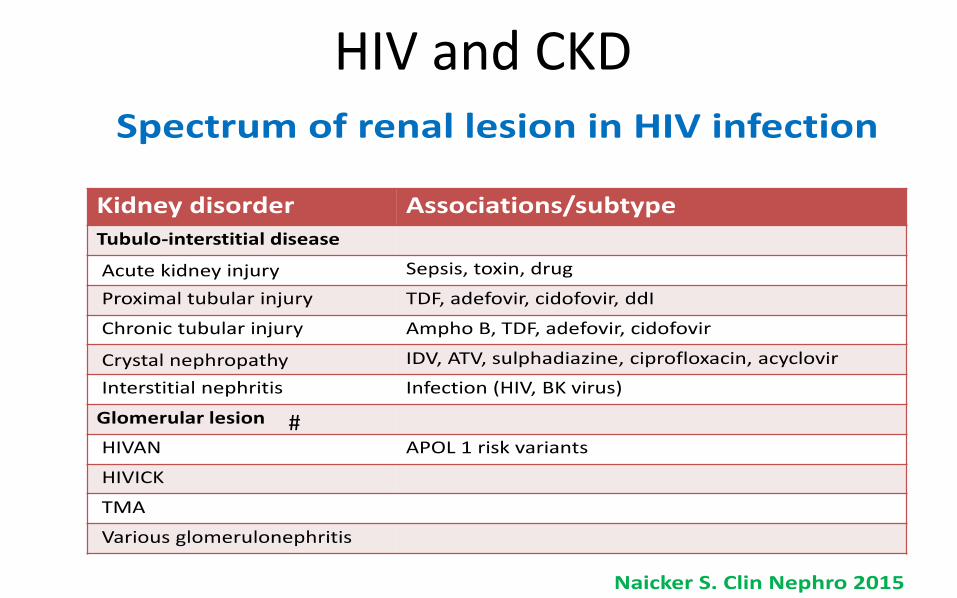
HIV and CKD
#

#
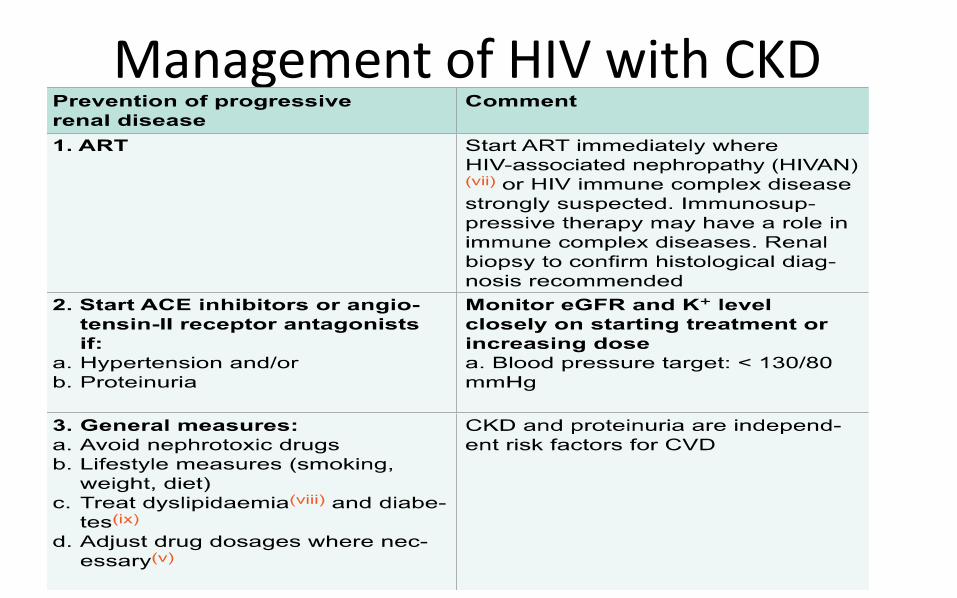
Management of HIV with CKD

Monitoring Kidney Disease
For eGFR: Use CKD-EPI formula based on serum creatinine, gender, age and ethnicity because eGFR quantification is validated > 60 mL/ min. The abbreviated modification of diet in renal disease (aMDRD) or the Cockcroft-Gault (CG) equation may be used as an alternative; see http://www.chip.dk/Tools.
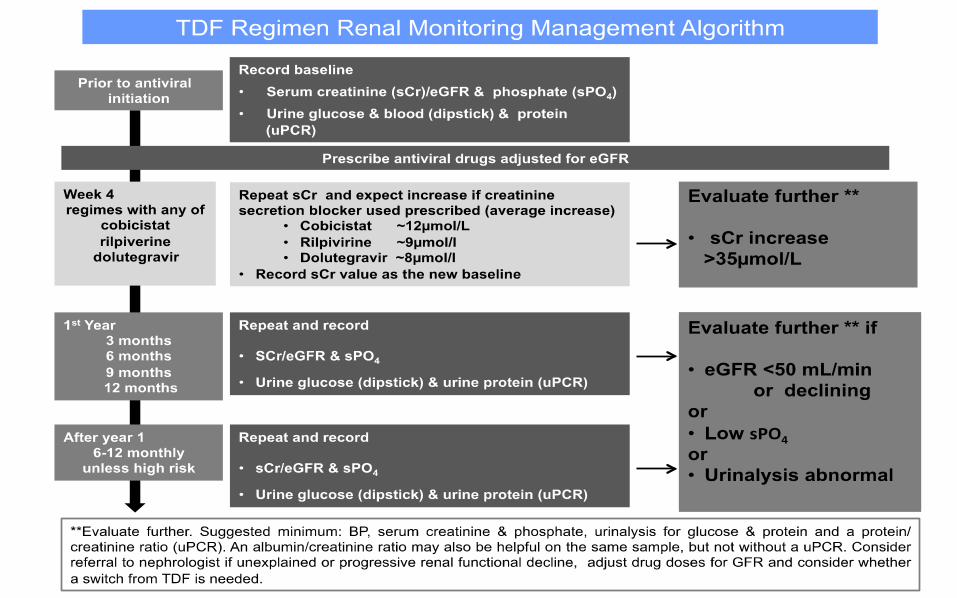

Monitoring RP
4 weeks 3months 3 months 3 months 3 months 6 months 6 months
HAART
BP, RP, BP, RP, U FEME, UPCR
If creatinine clearance <50 ml/min Urine RBC ++
US KUB Refer Nephrologist

Definition of CKD • eGFR < 60 ml/min for > 3 months. • If not known to have CKD, confirm the eGFR
within 2 weeks. • Use of DTG, COBI and RTV boosted PIs is
associated with an increase in serum creatinine/reduction of eGFR due to inhibition of proximal tubular creatinine transporters without impairing actual glomerular filtration:
• consider new set point after 1-2 months
http://kdigo.org/ home/guidelines/ckd-evaluation-management)

ARV- TDF associated Nephrotoxicity TDF - Proximal tubulopathy with any combination of:
1. Proteinuria:
• urine dipstick ≥ 1, or confirmed increase in UP/C > 30 mg/mmol
2. Progressive decline in eGFR and eGFR < 90 mL/min
3. Phosphaturia: confirmed hypophosphataemia secondary to increased urine phosphate leak
Assessment: • Tests for proximal renal tubulopathy/renal Fanconi syndrome • Consider renal bone disease if hypophosphataemia of renal origin: measure 25(OH) vitamin D, PTH, DXA scan
Consider stopping TDF if: • Progressive decline in eGFR and no other cause • Confirmed hypophosphataemia of renal origin and no other cause • Osteopenia/osteoporosis in the presence of increased urine phosphate leak

ARV- PI associated Nephrotoxicity • ATV / IDV (DRV) induced
nephrolithiasis • Crystalluria • Hematuria • Leucocytes in urine • Loin pain • AKI
Assessment: • Urinalysis for crystalluria/stone analysis • Exclude other cause for nephrolithiasis • Renal tract imaging including CT scan
Consider stopping IDV/ATV if: • Confirmed renal stones • Recurrent loin pain +/- haematuria
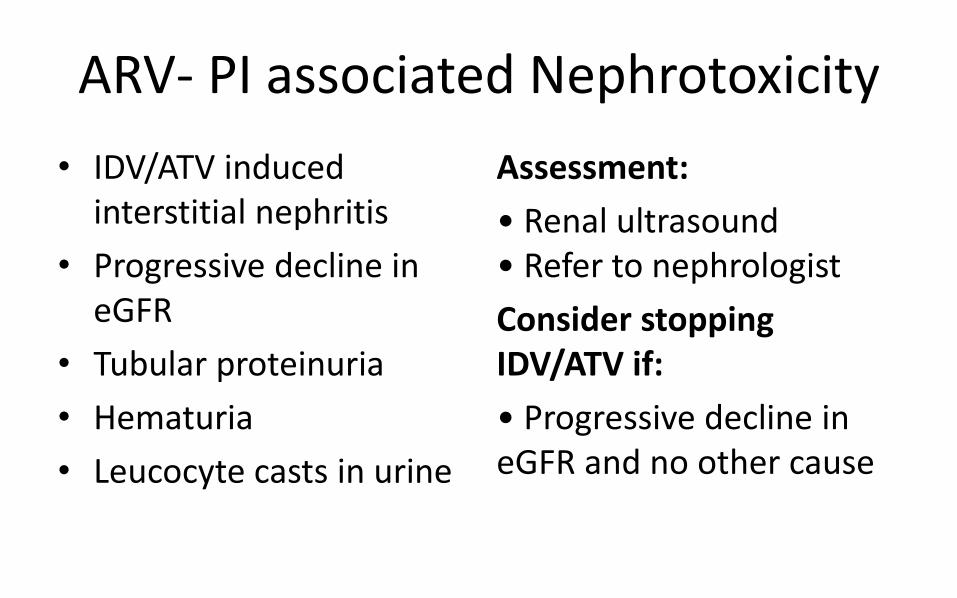
ARV- PI associated Nephrotoxicity
• IDV/ATV induced interstitial nephritis
• Progressive decline in eGFR
• Tubular proteinuria
• Hematuria
• Leucocyte casts in urine
Assessment:
• Renal ultrasound • Refer to nephrologist
Consider stopping IDV/ATV if:
• Progressive decline in eGFR and no other cause

Dosage of ARV adjustment for CKD
No dose adjustment
NRTI Abacavir, zidovudine
All NNRTI
All PI/r
All INSTI
• Dose adjustment needed NRTI
ARV > 50 30-49 10-29 <10
3TC 300 mg OD
150 mg OD
100 mg OD
50 mg OD
FTC No single agent
TDF 300 mg OD
300 mg every 48 H
#300 mg every 72 H
#300 mg weekly
Tenvir EM One tab OD
One tab every 48 H
Use single agent
# not recommended but if no alternative

HIV on ARV with Frailty and Bone health

The Concept of Frailty • Multisystem clinical syndrome that reflects biological rather than chronological age; regarded as
an end-stage state[1]
• Associated with loss of functional homeostasis, inability to recover fully after stressors, and morbidity and excess mortality[1]
• Other tools: FRAIL Scale, Study of Osteoporotic Fractures (SOF) index, Clinical Frailty Scale[3-5]
Slide credit: clinicaloptions.com References in slidenotes.
Fried Frailty Phenotype[2]
Frailty Characteristic Clinical Criteria*
Shrinking Unintentional weight loss (> 10 lbs) in prior year, sarcopenia
Muscle weakness Poor grip strength (lowest quintile by sex, BMI)
Poor endurance/exhaustion Self-reported exhaustion
Slowness Walking time per 15 ft (slowest quintile by sex, height)
Low activity Low kcal/week expenditure (lowest quintile by sex)
*Frailty defined as presence of ≥ 3 criteria; prefrailty as presence of 1-2 criteria.

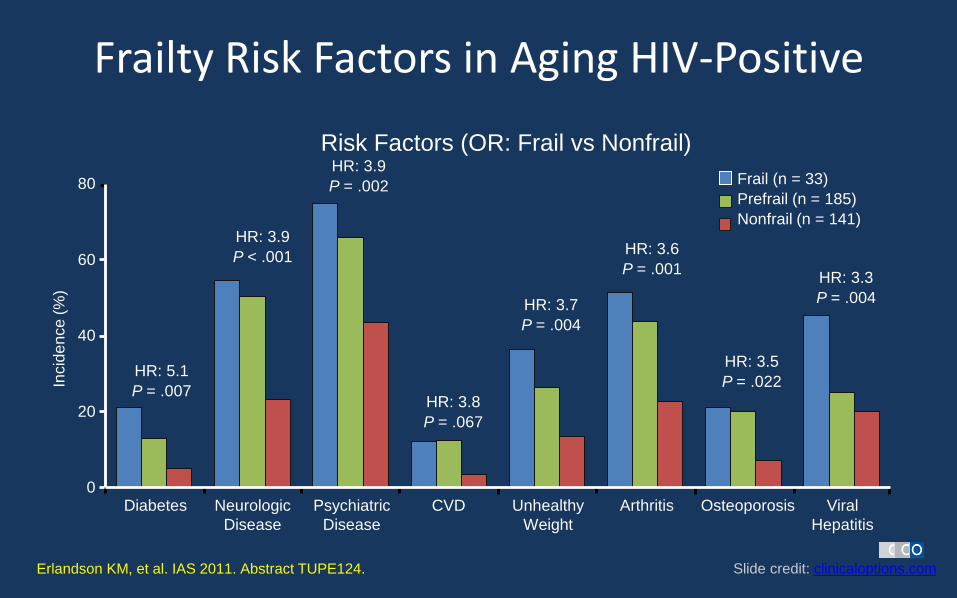
Frailty Risk Factors in Aging HIV-Positive
Slide credit: clinicaloptions.com Erlandson KM, et al. IAS 2011. Abstract TUPE124.
Incid
en
ce (
%)
Diabetes
Frail (n = 33)
Prefrail (n = 185)
Nonfrail (n = 141)
Risk Factors (OR: Frail vs Nonfrail)
Neurologic
Disease
Psychiatric
Disease
CVD Unhealthy
Weight
Arthritis Osteoporosis Viral
Hepatitis
HR: 5.1
P = .007
HR: 3.9
P < .001
HR: 3.9
P = .002
HR: 3.8
P = .067
HR: 3.7
P = .004
HR: 3.6
P = .001
HR: 3.5
P = .022
HR: 3.3
P = .004
0
20
40
60
80

ART Considerations for Pts With Bone Complications
TDF – Consider avoiding TDF: associated with greater
decrease in BMD along with renal tubulopathy, urine phosphate wasting, and osteomalacia
– Consider ABC/3TC TDF/FTC + INSTI OR PI/r: – Significantly greater BMD loss with PI/r vs RAL-based
regimens (when used with FTC/TDF)[2]
– DTG/ABC/3TC associated with less bone turnover than EFV/TDF/FTC[3]
1. DHHS Guidelines. July 2016. 2. Brown TT, et al. J Infect Dis. 2015;212:1241-1249.
3. Tebas P, et al. AIDS. 2015;29:2459-2464. Slide credit: clinicaloptions.com

Fracture Prevalence Increased in Older HIV-Infected Pts
• Meta-analysis: HIV-positive pts had 6.4-fold increased risk of low BMD and 3.7-fold increased risk of osteoporosis[1]
(8525 HIV-infected pts compared with 2,208,792 uninfected pts in Partners HealthCare System, 1996-2008[2])
Slide credit: clinicaloptions.com
Women Men
Age (Yrs)
7.0
6.0
5.0
4.0
3.0
2.0
1.0
0
Fra
ctu
re P
reva
len
ce
/
10
0 P
ers
on
s
30-39 40-49 50-59 60-69 70-79
P = .002
(overall comparison)
HIV
Non-
HIV
HIV
Non-
HIV
Age (Yrs)
7.0
6.0
5.0
4.0
3.0
2.0
1.0
0 F
ractu
re P
reva
len
ce
/
10
0 P
ers
on
s
20-29 30-39 40-49 50-59 60-69
P < .0001
(overall comparison)
1. Brown TT, et al. AIDS. 2006;20:2165-2174. 2. Triant V, et al. J Clin Endocrinol Metab. 2008;93:3499-3504.

http://www.shef.ac.uk/FRAX; McComsey et al, Clin Infect Dis 2010; http://www.eacsociety.org/Portals/0/Guidelines_Online_131014.pdf
Fracture risk assessment
1 2

Bone disease screening and diagnosis in HIV
Esp TDF
Classic risk factors: older age, female gender, hypogonadism, family history of hip fracture, low BMI (≤
19 kg/m2), vitamin D deficiency, smoking, physical inactivity, history of low trauma fracture, alcohol excess
(> 3 units/day), steroid exposure (minimum prednisone 5
mg/qd or equivalent for > 3 months)
If T-score normal, repeat after 3-5 years in risk groups
1, 2 and 5; no need for re-screening with DXA in risk groups 3 and 4 unless risk factors change and only
rescreen group 6 if steroid
use ongoing.

Ch
an
ge
(%)
Low BMD therapy: prevention / drug therapy
http://www.nof.org/files/nof/public/content/resource/913/files/580.pdf; Huang et al, AIDS 2009
General
Reduce risk of falls
Exercise
– weight-bearing
– muscle strength
– balance training
Vitamin D and calcium
replacement /
supplementation
Avoid TDF /PI
Bisphosphonate therapy
Bisphosphonate treatment of:
• alendronate 70 mg once weekly po;
• risedronate 35 mg once weekly po;
• ibandronate 150 mg po or 3 mg iv every 3 months;
• zoledronic acid 5 mg iv once yearly.

Recommendations for Evaluation of Bone Disease in HIV
Brown TT, et al. Clin Infect Dis. 2015;60:1242-1251. Slide credit: clinicaloptions.com
HIV-Infected Population Assessment Monitoring
Men 40-49 yrs of age
Premenopausal
women
≥ 40 yrs of age
Assess risk of fragility
fracture using FRAX
For pts with FRAX score ≤ 10%,
monitor FRAX in 2-3 yrs
For pts with FRAX score > 10%,
perform DXA
Men ≥ 50 yrs of age
Postmenopausal
women
Pts with fragility
fracture history,
receiving chronic
glucocorticoids, or at
high risk of falls
Assess BMD using
DXA
For pts with advanced
osteopenia, monitor DXA in 1-2
yrs
For pts with mild or moderate
osteopenia, monitor DXA in 5 yrs
For pts started on
bisphosphonates (significantly
reduced BMD or fracture
history), repeat DXA in 2 yrs

ART and frailty Observation Recommendations
Frailty is more prevalent
among HIV-infected vs HIV-
uninfected individuals
Assess pts for frailty;
consider Fried Frailty Phenotype or other available
tests
Fracture prevalence and low
BMD common among pts
with HIV
Some ART regimens have
larger impact on BMD loss
than others
Assess pts for BMD loss or risk of bone disease
depending on risk factors
For pts at risk for or with BMD loss or bone
disease, consider ART modifications
Backbone: consider ABC/3TC > TDF/FTC
Greater BMD loss observed with PI-based
regimens vs INSTI based regimens

HIV on ARV and Liver dysfunction

Abnormal LFT in HIV
• Co infection with HCV and HBV
• Opportunistic infections
• Non-viral causes of abnormal LFT: common etiologies – Drug-induced liver injury (DILI) – include herbs,
supplements and ART
– Alcohol
– Fatty liver in HIV - multifactorial, potentially reversible etiology for chronic liver disease
– Autoimmune hepatitis
Acharya C, et al. Clin Liver Dis 2015 Feb;19(1):1-22. Molina PE, et al. Curr HIV Res. 2014;12(4):265-75.

1. DILI-Liver toxicity of antiretroviral drugs Drug Class Drug Severe ALT Elevation (%)*
NRTI Lamivudine15
3.7-3.8
Tenofovir16
4
Zidovudine17
4.1
Emtricitabine18
2-5
Abacavir19
6
Didanosine20
6
Stavudine21
6-13
NNRTI Rilpivirine22
<1-2
Etravirine23
2.6
Delavirdine24
4.1-5.1
Efavirenz25
2-8
Nevirapine26
5.3-14
PI Nelfinavir††27
1-2
Indinavir28
2.6-4.9
Darunavir/ritonavir†29
5.6-6.9
Fosamprenavir/ritonavir30
4-8
Ritonavir31
5.3-8.5
Atazanavir/ritonavir32
3-9
Tipranavir/ritonavir33
9.7
Lopinavir/ritonavir34
3-11
CCR5 blocker Maraviroc35
2.4
Integrase inhibitor Raltegravir36
4
Fusion inhibitor Enfuvirtide37
5.4-6.2
Jones M, Núñez M. Semin Liver Dis 2012 May;32(2):167-76.
DILI, drug-induced liver injury; NRTI, nucleoside reverse transcriptase inhibitor; NNRTI, nonnucleoside reverse transcriptase inhibitor; PI, protease inhibitor; CCR5, chemokine receptor type 5; ALT, alanine aminotransferase; ULN, upper limit of normal. * Note. No data provided in package insert for Saquinavir.

DILI-Liver Toxicity of Antiretroviral drugs
Jones M, Núñez M. Semin Liver Dis 2012 May;32(2):167-76. Jones M, Nunez M. Semin Liver Dis 2012 May;32(2):167-76.
GRADING of LIVER Dysfucntion



Cancer and HIV


Cancer screen in HIV
Others NCD – HAND

Back to the Case 2008
– 54-year old man
– Presented with Pneumocystis pneumonia
– CD4 20, VL > 2 million cp/ml
– Underlying HTN, DM (creatinine 80 , clearance 62 ml/min)
– commences ART with TDF/FTC/EFV 2 weeks later
2009 – switched to TDF-FTC + LPV/r because of ongoing CNS side effects of EFV (VL <20)
– CD4 > 350 , plasma HIV RNA always <20 copies/mL
– Dev chronic diarrhoea but “not too bad” (no LOW)
2017 (now 63 year old man) smoker , BMI 30 TG 14.3 , Total Choleterol 6.4, HDL 0.8
FBS 9.8
BP 160/90
Creatinine 80 ---- 150 umol/ml (creatinine clearance = 62 declined to 45ml/min )

What is the issue here ?
• Aging • CKD • Hyperlipidemia
(Cholesterol and TG) • DM uncontrolled • HTN uncontrolled • Increased ASCVD risk • Bone health
• Frailty – avoid TDF • Avoid TDF (adjust dose) • High ASCVD risk > 50 % • Avoid ABC • Hyperglycemia and
hyperlidemia – due to Kaletra
• Optimised anti HTN and antilipid
• Anti platelet therapy

Modify ARVT
• First line/ Never failed therapy (Intolerant to NNRTI) • Cessation of smoking, start aspirin 75 mg OD • Atorvastatin 60 mg OD – 80 mg OD ( BUT once
stopped PI/r , TG and Chol level will reduced and blood sugar as well)
• Continue fenofibrate • Add ezetimibe 10 mg OD? • Switched PI/r ? • NNRTI ? Which one ?

NEAT 022: Switch From Boosted PI to DTG in Suppressed Pts With High CV Risk
PI-based regimens associated with increased risk of dyslipidemia[1]
NEAT 022: international, randomized, open-label phase IV study[2,3]
– Primary endpoints at Wk 48: proportion with HIV RNA < 50 c/mL (ITT), change in total plasma cholesterol
1. Ofotokun I, et al. Clin Infect Dis. 2015;60:1842-1851.
2. Gatell JM et al. IAS 2017. Abstract TUAB0102. 3. ClinicalTrials.gov. NCT02098837. Slide credit: clinicaloptions.com
Pts with stable HIV-1 RNA
< 50 c/mL on PI/RTV + 2 NRTIs,
high CV risk,*
no resistance mutations, no VF
(N = 415)
Immediate switch to DTG + 2 NRTIs†
(n = 205)
Continue
PI/RTV + 2 NRTIs
(n = 210)
Deferred switch to
DTG + 2 NRTIs†
Wk 48 Wk 96
*> 50 yrs of age and/or Framingham risk score > 10% at 10 yrs. †NRTIs to remain the same
throughout study.

NEAT 022: Switch From Boosted PI to DTG in Suppressed Pts With High CV Risk
• Switching to DTG noninferior to continuing boosted PI through Wk 48
• Switching to DTG associated with improved lipid profile vs continuing boosted PI through Wk 48
Gatell JM et al. IAS 2017. Abstract TUAB0102. Slide credit: clinicaloptions.com
No emergent resistance in pts with VF
No significant differences in grade 3/4 AEs, serious AEs, AE-related d/c
Virologic Success
Virologic Nonresponse
No Virologic
Data
ITT
Po
pu
lati
on
(%)
Treatment difference: -2.1% (95% CI: -6.6% to 2.4%)
4.9 4.4
100
80
60
40
20
0
93.1 95.2
2.0 0.5
DTG PI/RTV 10
5
0
-5
-10
-15
-20
-25
DTG PI/RTV
0.7
-8.7
-11.3
0.5
4.2 2.0 1.1
2.5 0.4
-18.4
-7.7 -7.0
TC Non-HDL-C TG LDL-C HDL-C TC/HDL
Ratio
P < .001 P < .001
P < .001
P < .001 P < .001
P = .286
Mea
n C
han
ge
Fro
m B
L to
Wk
48
(%
)

Case discussion
• High CVD risk with hyperlipidemia secondary to PI/r
• Renal function declining (creatinine clearance < 50 ml/min)
• Issue of Aging, bone health and frailty
Avoid ABC, and TDF, avoid PI /r
• Dolutegravir 50 mg OD + 3TC 150 mg OD

Summary • With ART, life expectancy of PLHIV has increased • Appropriate Mx of co morbidities : CV, Renal , Liver , Bone, CNS and
Cancer screening need to be done as part of the Mx for HIV • Multidisciplinary approach
– Monitor not only CD4 and HIV VL – Metabolic screen and CVD risk modification – Renal function and liver function – Cancer screen – Bone health and Fried frailty score – Neurocognitive assessment IHDS and MOCA
• ART prolonged survival of PLHIV, maintain quality of health is ultimate aim