Embed Size (px)
Citation preview

Inf. J. Radiarion Oncology Biol. Phys.. Vol. 13, pp. 1167-l 172 Printed in the U.S.A. All rights reserveI.
0360-3016/87 $3.00 + .oO Copyright 0 1987 Pergamon Journals Ltd.
??Original Contribution
LONG-TERM RESULTS OF LOW DOSE TOTAL BODY IRRADIATION FOR ADVANCED NON-HODGKIN LYMPHOMA
M. L. M. LYBEERT,’ J. H. MEERWALDT~ AND W. DENEVE’
‘Department of Radiotherapy, Brussel, Belgium; ‘Rotterdamsch Radiotherapeutisch lnstituut, Rotterdam, The Netherlands
Sixty-eight patients received fractionated low dose total body irradiation (LTBI) as treatment for non-Hodgkin lymphoma (NHIL) at the Rotterdamsch Radio-Therapeutisch Instituut (RRTI) in the period 1973-1979. Ninety percent (61/68) of these patients had advanced disease (Stage III + IV). According to current malignancy grade classifications, 3~4 patients had low grade NHL, 10 intermediate, and 19 high grade. In 5 cases no exact grading was possible. LTBI was given 3 times a week, midline dose 0.1 Gy, using 6 or 25 MeV photons to a mean total dose of 1.78 Gy. Initial response rate for low, intermediate, and high grade NHL was resp. 84, 42, and 40%. The main prognostic factor for survival and recurrence-free survival (RFS) was malignancy grade. Probability of uncorrected survival at 10 years for low, intermediate, and high grade was resp. 34,0 and 0%. Probability of RFS at 10 years was resp. 19, 0, and 0%. Neither stage nor sex had any influence on survival. Age was reversely correlated with survival, but was not correlated with RFS. Influence of prior therapy (18 patients) on survival and RFS was separately analyzed. Neither survival nor RFS of unfavorable histologic type NHL (high and intermedi- ate grade) was influenced. On the other hand patients with a favorable histologic type NHL (low grade) had a significantly (p .< 0.05) better RFS if they received LTBI as initial treatment, but survival was not significantly influenced. RFS at 5 and 10 years of patients who received LTBI as first treatment was respectively 32% and 27%. No treatment rel,ated complications were noted. Subsequent chemotherapy in case of relapse was not hampered by previous LTBI. The high response rate and extended RFS, without maintenance therapy, makes LTBI a prefera- ble first line treatment for patients with advanced stage low grade NHL.
Fractionated low dose TBI, Non-Hodgkin lymphoma.
INTIRODUCTION
The interest in fractionated low dose Total Body Irradia- tion (LTBI) as systemic therapy in advanced Non-Hodg- kin lymphoma (NHL) was revived in the early 1970’s by the favorable results of Johnson et aL7-’
In 1973 this technique was started under the impulse of Qasim’5g16 at the Rotterdamisch Radio-Therapeutisch Instituut (RRTI) in an attempt to provide a systemic therapy that would be less toxic but as effective as the chemotherapy, used until then. First only pretreated pa- tients were accepted, but later on, as results were very encouraging, LTBI was used as first line treatment for all types of NHL. TBI for NHL has always been a rather controversial subject. The idea of curing a systemic dis- ease with a total dose as low as about 2 Gy divided in multiple small doses, given in 1 or 2 months, is hard to understand. Yet it is possible, as described in previous
papers.2A49,‘6 The long-term experience at the RRTI is analyzed in this report.
METHODS AND MATERIALS
Patients characteristics Between 1973 and 1979, 68 patients with NHL were
treated with LTBI at the RRTI. Ages ranged from 22-82 years, with a mean age of 56 years. Male/female ratio was 34/34. The period of complaints before onset of any therapy was significantly longer for low grade NHL (mean 11.4 months) than for intermediate and high grade NHL (resp. 7.7 and 7.0 months). Patient character- istics at onset of LTBI and dose of LTBI are summarized in Table 1. Clinical characteristics were evenly distrib- uted although high malignant NHL presented more of- ten with a leukemic blood cell count. LTBI was the first modality of treatment for 47/68 patients.
Reprint requests to: J. H. Meerwaldt, Ph.D., Rotterdamsch beek, Liiwenberg). We wish to thank G. Storme, S. Van Belle, Radio-Therapeutisch lmtituut, Groene Hilledijk 301, 3075 E.A. Rotterdam, The Netherlands.
and M. Van Lancker for reviewing the manuscript, M. Nijssen
Acknowledgment-The Lymphoma group of the RRTI is for logistic assistance, L. D’Hauwers and R. Van den Berghe for preparing the manuscript, and G. Vercruysse and M. De
greatly acknowledged for the opportunity to study this material Beukeleer for preparing the figures. (Qasim, Van Andel, Eyk:enboom, Meerwaldt, Sizoo, Hagen- Accepted for publication 27 February 1987.
1167
1168 1. J. Radiation Oncology 0 Biology 0 Physics August 1987, Volume 13, Number 8
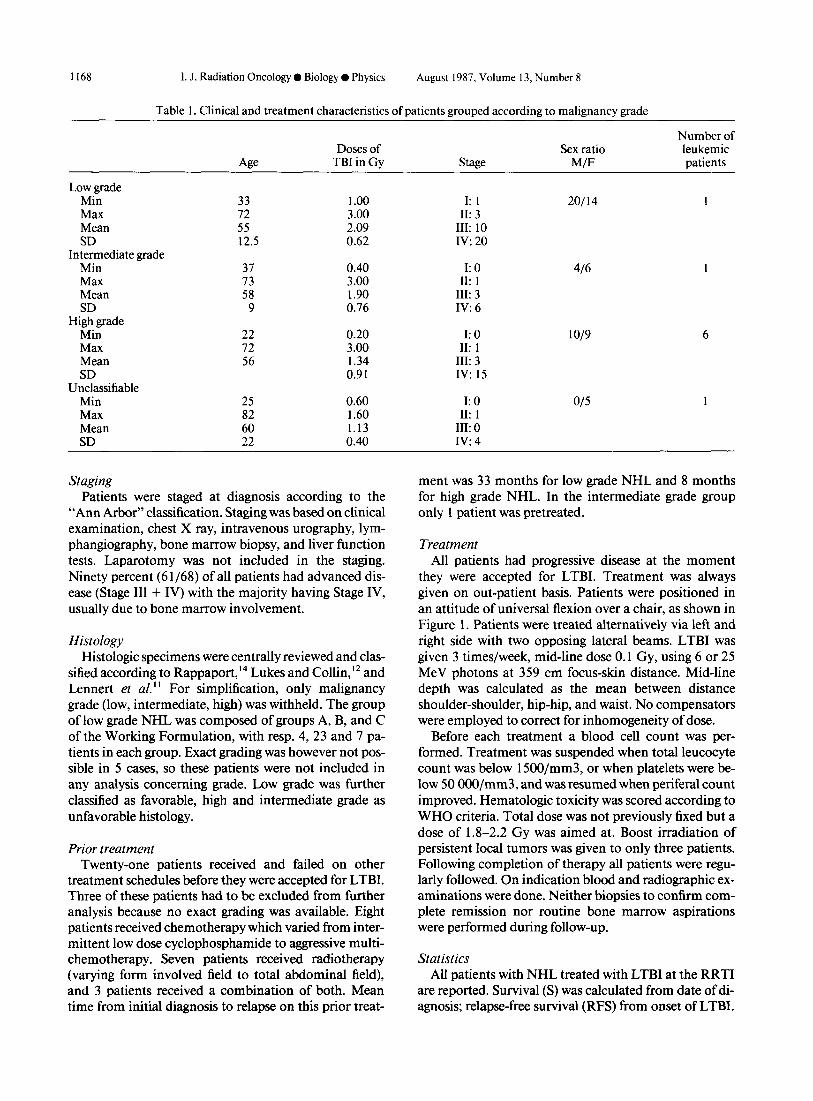
Table 1. Clinical and treatment characteristics of patients grouped according to malignancy grade
Low grade Min Max Mean SD
Intermediate grade Min Max Mean SD
High grade Min Max Mean SD
Unclassifiable Min Max Mean SD
Age
33 72 55 12.5
37 73 58
9
22 72 56
25 82 60 22
Doses of TBI in Gy
1 .oo 3.00 2.09 0.62
0.40 3.00 1.90 0.76
0.20 3.00 1.34 0.91
0.60 1.60 1.13 0.40
Stage
I: 1 II: 3
III: 10 IV: 20
I: 0 II: 1
III: 3 Iv:6
I: 0 II: 1
III: 3 IV: 15
I: 0 II: 1
III: 0 IV: 4
Sex ratio M/F
20114
416
1019
O/5
Number of leukemic patients
1
1
Staging Patients were staged at diagnosis according to the
“Ann Arbor” classification. Staging was based on clinical examination, chest X ray, intravenous urography, lym- phangiography, bone marrow biopsy, and liver function tests. Laparotomy was not included in the staging. Ninety percent (6 l/68) of all patients had advanced dis- ease (Stage III + IV) with the majority having Stage IV, usually due to bone marrow involvement.
Histology Histologic specimens were centrally reviewed and clas-
sified according to Rappaport, l4 Lukes and Collin, ‘* and Lennert et al.” For simplification, only malignancy grade (low, intermediate, high) was withheld. The group of low grade NHL was composed of groups A, B, and C of the Working Formulation, with resp. 4,23 and 7 pa- tients in each group. Exact grading was however not pos- sible in 5 cases, so these patients were not included in any analysis concerning grade. Low grade was further classified as favorable, high and intermediate grade as unfavorable histology.
Prior treatment Twenty-one patients received and failed on other
treatment schedules before they were accepted for LTBI. Three of these patients had to be excluded from further analysis because no exact grading was available. Eight patients received chemotherapy which varied from inter- mittent low dose cyclophosphamide to aggressive multi- chemotherapy. Seven patients received radiotherapy (varying form involved field to total abdominal field), and 3 patients received a combination of both. Mean time from initial diagnosis to relapse on this prior treat-
ment was 33 months for low grade NHL and 8 months for high grade NHL. In the intermediate grade group only 1 patient was pretreated.
Treatment All patients had progressive disease at the moment
they were accepted for LTBI. Treatment was always given on out-patient basis. Patients were positioned in an attitude of universal flexion over a chair, as shown in Figure 1. Patients were treated alternatively via left and right side with two opposing lateral beams. LTBI was given 3 times/week, mid-line dose 0.1 Gy, using 6 or 25 MeV photons at 359 cm focus-skin distance. Mid-line depth was calculated as the mean between distance shoulder-shoulder, hip-hip, and waist. No compensators were employed to correct for inhomogeneity of dose.
Before each treatment a blood cell count was per- formed. Treatment was suspended when total leucocyte count was below 1500/mm3, or when platelets were be- low 50 OOO/mm3, and was resumed when periferal count improved. Hematologic toxicity was scored according to WHO criteria. Total dose was not previously fixed but a dose of 1.8-2.2 Gy was aimed at. Boost irradiation of persistent local tumors was given to only three patients. Following completion of therapy all patients were regu- larly followed. On indication blood and radiographic ex- aminations were done. Neither biopsies to confirm com- plete remission nor routine bone marrow aspirations were performed during follow-up.
Statistics All patients with NHL treated with LTBI at the RRTI
are reported. Survival (S) was calculated from date of di- agnosis; relapse-free survival (RFS) from onset of LTBI.

Low dose TBI for advanced NHL 0 M. L. LYBEERT et al. 1169
Fig. 1. Patient in treatment position, centered in the middle of the radiation beam.
Curves of probability of actuarial uncorrected survival and RFS were calculated according to the Kaplan- Meier” method. Significance of differences between groups was assessed according to the log-rank test.
IRESULTS
Prognostic factors The most important prognostic factor for survival and
RFS was malignancy grade, as shown in Figures 2 and 3. As can be seen in IFigure 3, initial response of low, intermediate, and high grade NHL was resp. 84%-42%- 40%. Only low grade NHL showed a reasonable long RFS ( 19% at 10 years). Neither stage nor sex (p > 0.5) had influence on survival. On the other hand age did in- fluence survival. Considering the whole group, age was reversely correlated with survival, with highest p-value at 65 years of age (p < 0.02). This was also found when the low malignancy group was analyzed separately. Age did not influence RFS.
Influence ofprevious therapy As mentioned before, 18 patients with known malig-
nancy grade NHL failed prior treatment regimens and
Fig. 2. Probability of survival according to malignancy grade.
received TBI as second line therapy. Neither survival nor RFS of unfavorable histologic type (high and intermedi- ate grade) was significantly influenced by previous ther- apy. Survival of the favorable histologic group (low grade) was also not influenced, but difference in RFS was significant (p < 0.05). Median duration of RFS was much longer in the group of patients who received LTBI as initial treatment, and long-term RFS (27.3% at 10 years) was only observed in this group. Results of this analysis were summarized in Table 2.
Dose-eflect relationship No significant dose-effect relationship was found, only
a trend, (p = 0.1) towards a better RFS in low grade NHL receiving more than 2.0 Gy (Fig. 4).
Therapy-related complications. LTBI was very well tolerated without any noticeable
side-effects (e.g. nausea, vomiting, hair loss). All patients were able to carry on their normal work or activities. The only limiting toxicity was hematological and was ex- pressed as a decrease in blood thrombocyte and leuko- cyte count. Fall of these two parameters paralleled each other and was gradual. WHO toxicity score was 0 for most patients at start of LTBI, except 7,5 of whom were pretreated. Two patients had toxicity score 1, four pa-
Fig. 3. Probability of recurrence-free survival according to ma- lignancy grade.

1170 I. J. Radiation Oncology 0 Biology ??Physics August 1987. Volume 13, Number 8
Table 2. Comparison of survival and RFS for favorable and unfavorable groups
Favorable histology Unfavorable histology (Low grade) (High + intermediate grade)
25 patients 20 patients LTBI as initial 9 patients LTBI as initial 9 patients
treatment pretreated treatment pretreated
Probability of survival at
5 years 10 years
Probability of Remission rate Median Duration RFS at: 5 years
10 years
48% 35%
88% 29 months
32% 27.3%
p > 0.7
p < 0.05
55% 33%
78% 10 months
11% -
15% -
45% 13 months
- -
p > 0.3
p> 0.3
11% -
33% 5 months
- -
tients had toxicity score 2, and one patient had toxicity score 3 (thrombocytopenia) due to extensive bone mar- row involvement. WHO toxicity score decreased to a mean nadir of 2.1 and 2.2 for resp. thrombocytes and leucocytes after a mean period of resp. 46 days (SD: 32 days) and 49 days (SD: 30 days) after onset of LTBI. A gradual recovery was noted after cessation of LTBI. Nei- ther long-term effects on thrombocyte and leucocyte counts nor secondary leukemias were observed during follow-up.
Secondary therapy Patients failing to achieve a complete remission on
LTBI or who relapsed later on, were treated with a wide variety of treatment modalities. Chemotherapy was mostly given, but also involved field radiotherapy. Five patients received more than one course of LTBI. (Table 3).
Chemotherapy regimens, in second line after LTBI, were mostly based on a combination of cyclophospha- mide, vincristine, and prednisone (CVP), but adria- mycin, procarbazine, mustine, and other alkylating agents were also given. Chemotherapy was well tolerated
100 _ LOW Grade
Fig. 4. Influence of total dose of TBI on probablity of RFS for low grade NHL.
and hematologic toxicity was mild. However, obtained remissions were generally of short duration.
DISCUSSION
The management of patients with NHL has always been a controversial problem. Even the need for immedi- ate therapy has been questioned in selected cases of indo- lent advanced-stage low-grade lymphoma’s.6 LTBI was introduced as a less toxic alternative for chemotherapy. As results were encouraging-and as several centers con- firmed it’s clinical efficacy’.2.3 indications for LTBI were gradually enlarged, and high and intermediate grade NHL were also treated.
Prognostic factors As could be expected, the main prognostic factor
proved to be malignancy grade; all other factors were less important. Difference between high and low grade NHL was obvious, while intermediate grade indeed had an in- termediate prognosis, although intermediate grade NHL behaved more like high grade NHL in respect to survival and RFS after TBI. Chemotherapy is nowadays the first line treatment for high and intermediate grade NHL, but it was remarkable that LTBI induced a 40% remission rate. Possibly due to the limited number of low stage NHL, stage did not influence survival. Age did have an influence on survival, but not on RFS. The older the pa- tient, the worser the prognosis. No clear ceasure was found, but more a gradual decline. This was observed both in the entire group and in the low malignancy group.
Prior therapy It is often stated that LTBI is not an effective secondary
therapy for patients failing on other modalities of treat- ment.‘,’ As can be seen in Table 2, survival of both groups-favorable and unfavorable histology-was not influenced by prior therapy nor was RFS of patients with

Low dose TBI for advanced NHL 0 M. L. LYBEERT et al.
Table 3. Clinical characteristics of five patients who received more than one course of TBI
1171
Grade Dose RFS after RFS after
first course 1 st course 2nd course Total dose Survival (months)
from first TBI
H 1.4 Gy 5 months 4 months 7.3 Gy 33 dead P.D. H 2.4 Gy 5 months 3 months 3.9 Gy 22 dead P.D. ? 2.0 Gy 14 months 0 months 3.6 Gy 25 dead P.D. I 2.5 Gy 27 months 18 months 5.1 Gy 114 alive P.D. L 2.3 Gy 17 months 26 months 3.5 Gy 9 1 alive P.D.
H = high grade; ? = malignancy grade unknown: I = intermediate grade; L = low grade; P.D. = progressive disease.
unfavorable histology. Remissions induced in patients with unfavorable histology were of short duration. Pa- tients surviving at 5 years were in fact salvaged by subse- quent chemotherapy. ‘This fact indicates that it is still possible to administer effective chemotherapy after LTBI and to induce long term survival in a few patients. However, patients with favorable histology had a sig- nificantly better RFS (p < 0.05) if they had received LTBI as initial treatment, so failure on previous therapy did imply a negative selection. Patients who received LTBI as first treatment had a RFS of 32% at 5 years, and RFS remained 27.3% at 10 years, indicating that a pla- teau was reached after 5 years. The RFS at 10 years of 27.3% in this study is comparable with the 30% RFS at 10 years reported by Mendenhall et al. l3 These figures contradict the statement that almost no patients will re- main disease-free at 10 years.” LTBI does induce pro- longed relapse-free survival, without need of mainte- nance therapy. This is of considerable importance to the patient as absence of maintenance therapy is the main difference between TB[ and other treatments modalities (e.g. CVP, single agent chemotherapy), producing com- parable survival and RFS figures.5,9
A trend (p = 0.1) towards a better RFS was noted in low grade NHL treated to a total dose of more than 2 Gy. This difference was only noted during the first 3 years of follow-up.
Complications Technically, LTBI is easy applicable, and is associated
with minimal subjective toxicity. No real treatment re- lated complications were noted and hematologic toxicity was acceptable with a mean increase in WHO toxicity of 2.1 and 2.2 points for respectively thrombocytes and leucocytes. As Carabell et al.’ already reported, treat- ment possibilities in case of relapse are not compromised by LTBI. These relapses can be treated with chemother- apy or involved field radiotherapy and most patients will tolerate this subsequent treatment without difficulty. It is even possible to give a second or even a third course of LTBI (Table 3). Some patients had a leukemic peripheral blood count before onset of LTBI, but no new incidents of leukemia were observed during follow-up. This is in contrast to the observation of Carabell et al., ’ who noted 2 cases of leukemia, after treatment with chemotherapy of a relapse on LTBI.
Conclusion The very high response rate which lasts for an expected
period of time with a minimum of attendant morbidity and without maintainance therapy makes LTBI a prefer- able first line treatment for patients with advanced stage low grade malignancy NHL. LTBI does not compromise subsequent treatment in case of relapse.
REFERENCES
1.
2.
3.
4.
5.
Carabell, S.C., Chaffey, J.T., Rosenthal, D.S., Moloney, W.C., Hellman, S.: Results of total body irradiation in the treatment of advanced non-Hodgkin’s lymphoma’s. Cun- cer43: 994-1000, 1979. Chaffey, J.T., Hellrnan, S., Rosenthal, D.S., Moloney, W.C.: Total body irradiation in the treatment of lympho- cyticlymphoma. Cancer Treat. Rep. 61: 1149-l 152, 1977. Chaffey, J.T., Rosenthal, D.S., Pinhur, G., Hellman, S.: Advanced lymphosarcoma treated by total body irradia- tion. Br. J. Cuncer31(Suppl. 2): 441-449, 1975. Choi, N.C., Timothy, A.R., Kaufman, S.D., Carey, R.W., Aisenberg, AC.: LOIN dose fractionated whole body irradi- ation in the treatment of advanced non-Hodgkin’s lym- phoma. Cancer43: 1.636-1642,1979. Hoppe, R.T., Kushl.an, P., Kaplan, H.S. Rosenberg, S.A.,
6.
7.
8.
9.
Brown, B.W.: The treatment of advanced stage favorable histology non-Hodgkin’s lymphoma. A preliminary report of a randomized trial comparing single agent chemother- apy, combination chemotherapy and whole body irradia- tion. B/o&58(3): 592-598, 1981. Homing, S.J., Rosenberg, S.A.: The natural history of ini- tially untreated low grade non-Hodgkin’s lymphomas. N. Engl. J. Med. 311: 1471-1475, 1984. Johnson, R.E.: Evaluation of fractionated total body irra- diation in patients with leukemia and disseminated lym- phomas. Radiology 86: 1085- 1089, 1966. Johnson, R.E.: Total body irradiation (TBI) as primary therapy for advanced lymphosarcoma. Cancer 35: 242- 246,1975. Johnson, R.E., Canellos, G.P., Young, R.C., Chabner,

1172 I. J. Radiation Oncology 0 Biology 0 Physics
B.A., De Vita, V.T.: Chemotherapy (CVP) versus radio- therapy (TBI) for stage III and IV poorly differentiated lymphocytic lymphoma. Cancer Treat. Rep. 62: 32 l-325, 1978.
10. Kaplan, H.S., Meier, P.: Non-parametric estimations from incomplete observations. Am. Stat. Assoc. J. 53: 457-480, 1958.
11. Lennert, K., Stein, H., Kaiserling, E.: Cytological and funktional criteria for the classification of malignant lym- phoma. Br. J. Cuncer31(11): 29, 1975.
12. Lukes, R.J., Collin, R.D.: Immunologic characterization of human malignant lymphomas. Cancer 34: 1488,1974.
13. Mendenhall, N.P., Marcus, R.B., Thar, T.L., Million, R.R.: Management of advanced non-Hodgkin’s lym-
August 1987. Volume 13. Number 8
phoma: Results of prospective trial of total body irradia- tion (Abstr.). Ann. J. Clin. Oncol. 8: 16, 1985.
14. Rappaport, H.: Tumors of the hematopoietic system. In Atlas of Tumor Pathology, section 3, fascicle 8. Washing- ton, D.C., U.S., Armed Forces Institute of Pathology, 1966.
15. Qasim, M.M.: Total body irradiation in non-Hodgkin lymphoma. Strahlentherapie 149: 364-367, 1975.
16. Qasim, M.M.: Total body irradiation as a primary therapy in non-Hodgkin lymphoma. Clin. Radiol. 30: 287-289, 1979.
17. Urba, W.J., Longo, D.L.: Cytologic, immunologic and clinical diversity in non-Hodgkin’s lymphoma: Therapeu- tic implications. Sem. Oncof. 12(3): 250-267, 1985.





























