Embed Size (px)
Citation preview

Long-Term Outcome of Patients with Acute CholecystitisReceiving Antibiotic Treatment: A Retrospective Cohort Study
Chih-Hung Wang • Hao-Chang Chou •
Kao-Lang Liu • Wan-Ching Lien • Hsiu-Po Wang •
Yao-Ming Wu
Published online: 1 November 2013
� Societe Internationale de Chirurgie 2013
Abstract
Background Few studies have followed patients who
received antibiotic treatment for acute cholecystitis (AC).
The present retrospective study investigated recurrence rates
of AC and analyzed factors associated with recurrence after
antibiotic treatment in adult AC patients.
Methods We analyzed patients treated with antibiotics for
AC between October 1, 2004, and November 30, 2010.
A Cox proportional hazards model was used to identify
factors associated with early recurrence. Generalized
additive models were applied to detect the nonlinear effects
of continuous covariates.
Results The study included 226 patients (mean age:
62.2 years; 144 men [63.7 %]). The average duration of
parenteral antibiotics was 8.0 days. Second-generation
cephalosporins were administered to 199 patients (88.1 %).
The Kaplan–Meier plot indicated that recurrences were
more frequent within 100 days of AC; these were defined
as early recurrences. The recurrence rate was 13.7 % (31/
226) at a median follow-up of 308.5 days (early recur-
rences: 19/226 [8.4 %]). The duration of parenteral anti-
biotic use significantly correlated with early recurrence
(hazard ratio: 0.83; 95 % confidence interval, 0.73–0.95;
p = 0.005). Generalized additive models revealed that
patients using parenteral antibiotics longer than 8 days
were less likely to suffer from early recurrence.
Conclusions The rate of recurrence of AC in patients who
received antibiotics alone was low. The recurrence rate was
higher within 100 days of AC. Because of the inherent
limitations of a retrospective study, further research is
needed to identify factors associated with early recurrence.
Introduction
Acute cholecystitis (AC) is an inflammatory disease of the
gallbladder, and [90 % of AC cases are associated with
gallstones [1]. Cholecystitis represents one of the most
common emergency admissions in surgical practice [2].
Cholecystectomy has been the gold standard treatment
for AC. However, the optimal timing for cholecystectomy
in patients with AC is a point of controversy. With the
advent of laparoscopic cholecystectomy, early surgery was
considered safe and cost effective for the management of
AC [2]. However, initial nonoperative treatment, including
antibiotic treatment with or without percutaneous transhe-
patic cholecystostomy (PTC), has been proposed for high-
risk patients to prevent postoperative morbidity, and
interval cholecystectomy (IC) has been reserved for
patients with recurrent AC [3]. Some researchers have
suggested that PTC, instead of IC, may serve as a definitive
treatment for AC [4].
C.-H. Wang � H.-C. Chou � W.-C. Lien (&)
Department of Emergency Medicine, National Taiwan
University and National Taiwan University Hospital, No. 7,
Chung-Shan S. Road, Taipei 100, Taiwan
e-mail: [email protected]
K.-L. Liu
Department of Medical Imaging, National Taiwan University
and National Taiwan University Hospital, No. 7, Chung-Shan S.
Road, Taipei 100, Taiwan
H.-P. Wang
Department of Internal Medicine, National Taiwan University
and National Taiwan University Hospital, No. 7, Chung-Shan S.
Road, Taipei 100, Taiwan
Y.-M. Wu
Department of Surgery, National Taiwan University and
National Taiwan University Hospital, No. 7, Chung-Shan S.
Road, Taipei 100, Taiwan
123
World J Surg (2014) 38:347–354
DOI 10.1007/s00268-013-2311-3

An increasing number of studies have investigated PTC
for AC, with a particular focus on elderly and other high-
risk patients with serious comorbidities [3, 4]. However,
many non-high-risk patients have completed antibiotic
treatment without IC in clinical practice [5], and the
management of these patients has not been well investi-
gated. In a population-based study, AC patients who did
not undergo IC comprised 43.2 % (11,118 of 25,743) of the
cohort, and the mean patient age was 64.3 years [5].
Although guidelines recommended IC for patients who
did not initially undergo early cholecystectomy, there were
many patients in clinical practice who did not return for IC
[5]. Knowledge of the prognosis for patients managed with
antibiotics alone for AC may aid clinicians in deciding for
or against surgical intervention. The present study was
carried out retrospectively with the aim of estimating the
recurrence rate in all adult AC patients receiving antibiotic
treatment. The factors associated with recurrence were also
investigated.
Materials and methods
This retrospective cohort study was performed by review-
ing the medical records of patients with AC who were
admitted through the emergency department of National
Taiwan University Hospital (NTUH) between October 1,
2004, and November 30, 2010. National Taiwan University
Hospital is a 2,600-bed urban medical center providing all
levels of care. Patients were identified using the interna-
tional classification of diseases, 9th Revision, clinical
modification codes 574.0, 574.3, 574.6, 574.8, 575.0,
575.12, and 575.4. Acute cholecystitis was diagnosed
through a combination of patient history, physical exami-
nation, and laboratory analysis. The diagnosis had to have
been confirmed by characteristic imaging findings on
ultrasonography (US) or computed tomography (CT)
according to the Tokyo guidelines [6]. Patients were
excluded if they had co-existing gallstone pancreatitis,
choledocholithiasis, or hepatobiliary malignancy. Patients
who solely received antibiotic treatment during their
admission were included for analysis. Patients with PTC
insertion were excluded. This study was approved by the
Institutional Review Board of NTUH prior to data
collection.
The basic demographics, presenting vital signs, chief
symptoms (fever or abdominal pain), physical findings
(including right upper quadrant tenderness and Murphy’s
sign), laboratory data (including white blood cell counts,
and C-reactive protein and bilirubin levels), imaging find-
ings (including gallbladder wall thickening, the presence of
gallstone, distention of the gallbladder, and surrounding
fluid accumulation) on US/CT, and the timing of antibiotic
use were recorded. Patients were graded according to the
Tokyo guidelines (Table 5 in appendix) [6]. Comorbidities
were recorded according to the Charlson comorbidity index
[7]. Gangrenous cholecystitis, emphysematous cholecysti-
tis, gallbladder perforation, empyema, and pericholecystic
abscess were categorized as complicated cholecystitis.
The primary outcome was the recurrence of AC after
antibiotic treatment. Secondary outcomes included IC and
death. The definition of early and IC varied across different
studies [2]. In this study, early cholecystectomy was
defined as cholecystectomy within the first 7 days after
symptom onset [2], whereas IC was defined as cholecys-
tectomy performed [7 days after symptom onset. Medical
records were reviewed regularly to determine whether
patients eventually returned for cholecystectomy after ini-
tial discharge.
Statistical analysis
Data analysis was performed with the R 2.12.1 software (R
Foundation for Statistical Computing, Vienna, Austria).
Categorical data were compared with Fisher’s exact test,
and continuous data were examined with the Wilcoxon
rank-sum test. A two-tailed p value of B0.05 was consid-
ered statistically significant.
For calculating recurrence-free survival curve in a
Kaplan–Meier plot, the starting time was defined as the
date of symptom onset and the event time as the date of AC
recurrence. Interval cholecystectomy, death, and the end of
data collection (May 31, 2011) were the censoring events.
The depicted Kaplan–Meier plot indicated that AC recur-
red more frequently within 100 days of symptom onset.
Therefore, recurrence and IC within 100 days of AC were
designated as early recurrence and IC, respectively.
Multivariate survival analysis was conducted to identify
factors associated with early recurrence or IC using the
Cox proportional hazards model. All potential covariates
for variable selection are listed in Table 1. The stepwise
variable selection procedure (with iterations between the
forward and backward steps) was applied to remove vari-
ables that were not significant and to determine the most
parsimonious model by minimizing the value of Akaike’s
information criterion. Generalized additive models were
applied to detect the nonlinear effects of continuous
covariates. Recurrence-free survival curves were compared
with a two-sided log rank test.
Results
A total of 947 patients with AC were admitted through the
emergency department between October 2004, and
November 2010. Of these, 168 patients with co-existing
348 World J Surg (2014) 38:347–354
123

Table 1 Demographic and clinical characteristics of enrolled patients
Characteristics All patientsa Patients with early
recurrenceaPatients without
early recurrenceap valueb
Number 226 19 207
Age (years) 62.2 (15.8) 57.0 (15.7) 62.7 (15.7) 0.115
Male 144 (63.7 %) 8 (42.1 %) 136 (65.7 %) 0.048*
Comorbidity
Diabetes mellitus 60 (26.5 %) 3 (15.8 %) 57 (27.5 %) 0.415
Cerebral vascular disease 20 (8.8 %) 3 (15.8 %) 17 (8.2 %) 0.229
Coronary artery disease 34 (15 %) 4 (21.1 %) 30 (14.5 %) 0.499
Malignancy 20 (8.8 %) 2 (10.5 %) 18 (8.7 %) 0.678
Charlson comorbidity index 1.1 (1.5) 1.1 (1.2) 1.1 (1.5) 0.704
Previous abdominal surgery 43 (19 %) 3 (15.8 %) 40 (19.3 %) [0.999
Clinical symptoms and signs on presentation
Body temperature 37.2 (1.2) 37.1 (1.3) 37.2 (1.1) 0.920
Body temperature [38 �C 56 (24.8 %) 5 (26.3 %) 51 (24.6 %) [0.999
Abdominal pain 183 (81.0 %) 17 (89.5 %) 166 (80.2 %) 0.540
Onset of symptoms before presentation
at emergency department (days)
2.1 (2.4) 2.5 (3.6) 2.1 (2.2) 0.642
Laboratory studies
White blood cell count, 103 lL 12.6 (5.6) 10.6 (3.6) 12.8 (5.7) 0.049*
Positive blood culture 41 (18.1 %) 2 (10.5 %) 39 (18.8 %) [0.999
Diagnostic tools
Ultrasonography (US) 186 (82.3 %) 13 (68.4 %) 173 (83.6 %) 0.115
Computed tomography (CT) 154 (68.1 %) 15 (78.9 %) 139 (67.1 %) 0.440
Findings on US or CT
Gallstones or sludge 193 (85.4 %) 16 (84.2 %) 177 (85.5 %) 0.745
Pericholecystic fluid 63 (27.9 %) 5 (26.3 %) 58 (28.0 %) [0.999
Fatty liver 109 (48.2 %) 9 (47.4 %) 100 (48.3 %) [0.999
Complicated cholecystitis 15 (6.6 %) 1 (5.3 %) 14 (6.8 %) [0.999
Severity grade per Tokyo guidelines 0.623
Grade I 145 (64.2 %) 11 (57.9 %) 134 (64.7 %)
Grade II 77 (34.1 %) 8 (42.1 %) 69 (33.3 %)
Grade III 4 (1.8 %) 0 (0.0 %) 4 (1.9 %)
Early operation indicated by surgeons 124 (54.9 %) 11 (57.9 %) 113 (54.6 %) 0.815
Early operation rejected by patients 96 (42.5 %) 9 (47.4 %) 87 (42.0 %) 0.809
Medical ward admission 201 (88.9 %) 16 (84.2 %) 185 (89.3) 0.450
Duration, days
Total antibiotics 14.4 (8.2) 10.4 (6.3) 14.8 (8.3) 0.010*
Parenteral 8.0 (4.8) 5.4 (4.0) 8.3 (4.8) 0.012*
2nd generation cephalosporins 199 (88.1 %) 16 (84.2 %) 183 (88.4 %) 0.482
Oral 6.4 (6.9) 5.1 (4.6) 6.5 (7.0) 0.250
Fever 1.8 (2.0) 1.5 (2.1) 1.9 (2.0) 0.255
Parenteral analgesic use 0.9 (1.3) 1.0 (1.0) 0.9 (1.3) 0.458
Nil per os 2.6 (2.1) 2.5 (2.3) 2.6 (2.1) 0.551
Hospital stay 8.7 (6.9) 7.4 (5.3) 10.7 (7.3) 0.029*
a Data are represented as mean (SD) or counts (%)b Comparison was made between patients with and without early recurrences
* p value \0.05
World J Surg (2014) 38:347–354 349
123

gallstone pancreatitis, choledocholithiasis, or hepatobiliary
malignancy were excluded. Of the remaining 779 patients,
395 patients underwent early cholecystectomy, 158
underwent PTC, and 226 completed antibiotic treatment.
The 226 patients who received antibiotic treatment alone
were further analyzed in the present study.
Table 1 summarizes the demographic and clinical
characteristics of the patients included in the study. There
were 144 male patients and 82 female patients with a mean
age of 62.2 years. 193 (85.4 %) patients had gallstones or
sludge detected on US or CT. The mean time from
symptom onset to presentation at the emergency depart-
ment was 2.1 days. Of the 226 patients studied, 124
(54.9 %) were considered suitable for early cholecystec-
tomy after surgeon consultation, whereas 96 patients
(41.2 %) rejected early cholecystectomy after discussion
with surgeons. The average duration of antibiotic use was
8.0 days for parenteral antibiotics and 6.4 days for oral
antibiotics. Second-generation cephalosporins were
administered to 199 patients (88.1 %).
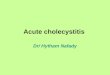
The Kaplan–Meier plot demonstrated that there were
more frequent recurrences within 100 days of AC than
during the subsequent period (Fig. 1). Accordingly, this time
point was used to differentiate between early and late events,
including recurrence and IC. As shown in Table 1, patients
with and without early recurrence did not differ significantly
in demographic or clinical characteristics, except in gender,
white blood cell count, the duration of total and parenteral
antibiotic use, and length of hospital stay.
Table 2 summarizes the primary and secondary out-
comes of the study patients. The median follow-up period
was 308.5 days. The mean time of IC and recurrence were
103.0 and 214.5 days, respectively. 62 patients (27.4 %)
underwent early IC, whereas 19 patients (8.4 %) experi-
enced early recurrence.
Multivariate survival analysis using a Cox proportional
hazards model revealed that the duration of parenteral
antibiotic use was significantly associated with early
recurrence (hazard ratio [HR], 0.81; 95 % confidence
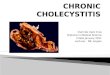
interval [CI], 0.71–0.93; p = 0.002). In Fig. 2, under the
generalized additive model, the nonparametric smoothing
plot shows that the probability of early recurrence was
lower in patients with parenteral antibiotic use for[8 days
than in patients with a shorter duration (B8 days) of anti-
biotic use.
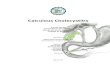
As shown in Fig. 3, Kaplan–Meier plots stratified by the
duration of parenteral antibiotic use demonstrated that the
rate of early recurrence was significantly higher for patients
who received parenteral antibiotics for B8 days than for
those who received it for [8 days (p = 0.028 by the log
rank test).
Baseline characteristics were compared between
patients with and without early IC. As shown in Table 3,
univariate analysis revealed significant differences between
groups in cerebrovascular disease and the Charlson
comorbidity index. Multivariate survival analysis using a
Cox proportional hazards model indicated that several
variables were significantly associated with early IC,
including age (60–85 years; HR, 2.09; 95 % CI, 1.23–3.55;
p = 0.007), male gender (HR, 0.60; 95 % CI, 0.36–0.99;
p = 0.045), Charlson comorbidity index (HR, 0.62; 95 %
CI, 0.48–0.81; p \ 0.001), surgeon recommendation for
early surgery (HR, 2.08; 95 % CI, 1.04–4.13; p = 0.037),
and early surgery option rejected by patients (HR, 0.37;
95 % CI, 0.18–0.76; p = 0.007) (Table 4).
Discussion
Population-based studies have reported that early chole-
cystectomy rates were *50 % in the United States from
2000 to 2005 [8] and only 14.7 % in England from 2003 to
2005 [5]. In England, of the 20,924 patients who did not
undergo an emergency cholecystectomy, 9,806 patients
(46.9 %) subsequently underwent IC, whereas the
remaining 11,118 patients (53.2 %) did not [5]. In our
Fig. 1 Kaplan–Meier plots of
the recurrence-free survival
curve in patients treated with
antibiotic treatment for acute
cholecystitis. Dotted lines
represent the 95 % confidence
interval
350 World J Surg (2014) 38:347–354
123

study, *35.4 % of patients (80/226) with initial antibiotic
treatment underwent IC, whereas 64.6 % of patients (146/
226) did not.
Few, if any, studies have reported the follow-up and
prognosis of AC patients who did not undergo IC. For
patients with gallstone disease,[50 % remained or became
asymptomatic during the long-term follow-up in a 10-year
prospective population-based cohort study [9]. Among
patients with severe symptoms, only 8.4 % developed
complications [9]. In a retrospective hospital-based study
by McGillicuddy et al. [3] the recurrence rate was *4 %
with a mean follow-up duration of 30 months in elderly
AC patients receiving antibiotic treatment alone. The
principal findings of our study showed a recurrence rate of
*13.7 % (31/226) with a median follow-up of 308.5 days.
Most patients who did not undergo cholecystectomy did
not experience recurrent AC.
McGillicuddy et al. [3] reported a much lower recur-
rence rate than our study (4 vs. 13.7 %). However, in the
study by McGillicuddy et al. a high proportion of patients
(78/126, 61.9 %) ended follow-up with death, which might
Table 2 Outcomes of enrolled patients
Outcome Enrolled patients
(n = 226)
Follow-up period (days) 308.5 (1,139.8)a
Total recurrence 31 (13.7 %)b
Total interval cholecystectomy 80 (35.4 %)b
Time to recurrence (days) 214.5 (343.3)c
Time to interval cholecystectomy (days) 103.0 (179.0)c
Patients with
Early recurrenced 19 (8.4 %)b
Late recurrenced 12 (5.3 %)b
Early interval cholecystectomyd 62 (27.4 %)b
Late interval cholecystectomyd 18 (8.0 %)b
Death from other causes 3 (1.3 %)b
a Data are expressed as the median (IQR)b Data are expressed as counts (%)c Data are expressed as the mean (standard deviation)d ‘‘Early’’ and ‘‘late’’ indicate the event occurred at B100 or
[100 days after initial onset of acute cholecystitis, respectively
Fig. 2 Generalized additive
models for the duration of
parenteral antibiotic use
adjusted by age and gender
Fig. 3 Kaplan–Meier plots
stratified by the duration of
parenteral antibiotic use
World J Surg (2014) 38:347–354 351
123

influence the observation of recurrence and underestimate
its real incidence. Nonetheless, their data were still valu-
able in the assessment of surgical risk–benefit profile in the
elderly group. Unlike the study by McGillicuddy et al.,
ours did not focus on the elderly group only. Our patients
were generally younger (mean age: 78.1 vs. 62.2 years)
and healthier (coronary artery disease proportion: 72.2 vs.
15 %) with comparatively lower anesthesia risk for emer-
gent operation than patients in the study by McGillicuddy
et al. By current accepted management standards of AC,
patients should receive emergent or IC if no contraindica-
tions exist, such as cardiopulmonary compromise. How-
ever, even though most of our patients were considered
suitable for early cholecystectomy (124/226, 54.9 %), only
35.4 % of them (80/226) received IC.
Riall et al. [10] reported significant mortality and mor-
bidity in patients with nonoperative treatment. However, the
diagnosis of AC in their study depended on the database
codes rather than review of medical records by clinicians.
The accuracy of database codes for AC had been questioned
[5]. We sometimes found that making the clinical distinction
between biliary colic and acute cholecystitis was difficult.
Because surgical or pathological proof of AC was not
available in the present study, the clinical findings of AC had
to be verified by imaging studies, such as US or CT, to ensure
correctness and validity of the diagnosis.
The Kaplan–Meier plot demonstrated that the recurrence
rate of AC was higher within 100 days of the initial onset of
symptoms than in the subsequent period (8.4 vs 5.3 %).
Conventionally, IC was performed 6–12 weeks after AC [2].
Therefore, we decided to focus our investigation on a com-
parison of patients who did and did not experience recur-
rence within 100 days of AC. Multivariate survival analysis
indicated that the duration of parenteral antibiotic use sig-
nificantly correlated with early recurrence: patients receiv-
ing parenteral antibiotics for [8 days suffered less from
early recurrence than those receiving antibiotics for
B8 days. Although this statistical association existed, the
effect of parenteral antibiotics was less likely to persist after
hospital discharge to prevent the early recurrence. Clinically,
it is possible that the reason patients received antibiotics for a
longer duration might be that they suffered from more severe
inflammation than those with shorter duration antibiotic
treatment. Also, fibrosis of the gallbladder after a period of
severe inflammation might have led to a lower recurrence
rate in the later period. Although we had controlled most
important clinical and laboratory variables in our model, we
may still have missed some important ones that would clarify
the problem of confounding by indication, which should be
further investigated in prospective researches. In contrast,
when compared with the early IC rate, the early recurrence
rate was relatively low (27.4 vs. 8.4 %). The number of
censoring events was almost three times the number of pri-
mary outcomes, which might further weaken the power of
statistical analysis.
In the present study, early cholecystectomy was defined
as cholecystectomy within 7 days of symptom onset. This
Table 3 Demographic characteristics of patients with and without
early IC
Characteristics Patients with
early ICaPatients
without
early ICa
p valueb
Number 62 164
Age (years) 62.7 (14.2) 62.0 (16.3) 0.845
Male 35 (56.5 %) 109 (66.5 %) 0.167
Comorbidity
Diabetes mellitus 14 (22.6 %) 46 (28.0 %) 0.500
Cerebral vascular
disease
1 (1.6 %) 19 (11.6 %) 0.017*
Coronary artery disease 6 (9.7 %) 28 (17.1 %) 0.212
Malignancy 5 (8.1 %) (9.1 %) [0.999
Charlson comorbidity
index
0.7 (1.1) 1.3 (1.6) 0.002*
Previous abdominal
surgery
10 (16.1 %) 33 (20.1 %) 0.572
Imaging findings in US or CT
Gall bladder stones or
sludge
57 (91.9 %) 136 (82.9 %) 0.095
Complicated
cholecystitis
6 (9.7 %) 9 (5.5 %) 0.367
Severity grade per Tokyo guidelines 0.759
Grade I 37 (60.3 %) 108(65.6 %)
Grade II 24 (38.1 %) 53 (32.5 %)
Grade III 1 (1.6 %) 3 (1.8 %)
Early operation indicated
by surgeons
33 (53.2 %) 91 (55.5 %) 0.767
Early operation rejected
by patients
22 (35.5 %) 74 (45.1 %) 0.228
Medical ward admission 53 (85.5 %) 148 (90.2 %) 0.344
a Data are expressed as mean (SD) or counts
* p value of \0.05
Table 4 Multivariate survival analysis for early IC using a Cox
proportional hazard model
Covariates Hazard
ratio
95 % confidence
interval
p value
Age 60–85 years 2.09 1.23–3.55 0.007*
Male gender 0.60 0.36–0.99 0.045*
Charlson comorbidity index 0.62 0.48–0.81 \0.001*
Early surgery recommended
by surgeons
2.08 1.04–4.13 0.037*
Early surgery rejected
by patients
0.37 0.18–0.76 0.007*
* p \ 0.05
352 World J Surg (2014) 38:347–354
123

time frame was chosen because some trials have suggested
that early operation performed during this period was as
safe as surgery performed within 3 days of symptom onset
[11]. In contrast, the timing of IC was more controversial.
The term interval has been interpreted liberally, as some-
where between a few weeks and a few months after AC,
time periods that were assumed to be sufficient for the
acute inflammation to subside completely [1]. In the past
40 years, including the eras of open and laparoscopic
cholecystectomy, most ICs reported in clinical trials were
performed between 6 and 12 weeks after AC [2]. However,
in some trials, IC was conducted earlier than 6 weeks after
AC; for example, Norrby et al. [12] defined IC as chole-
cystectomy after initial conservative treatment, and Chan-
dler et al. [13] defined it as cholecystectomy after the
resolution of symptoms or after 5 days of treatment. To
maximize the available information, we defined IC as
operations performed at least 1 week after symptom onset.
The total rate of IC in our study, including both early and
late operations, was 35.4 % (80/226). The rate of IC varied
significantly across studies from 23.8 % (44/185) to 80.7 %
(46/57) [3, 5, 14]. This wide variation may be explained by
differences in patient cohorts, selection by surgeons, and
most important, patient decisions. As noted in our analysis,
the attitude of patients toward early cholecystectomy sig-
nificantly correlated with early IC (HR, 0.37; 95 % CI,
0.18–0.76; p = 0.007). Patients who initially refused early
cholecystectomy were less likely to undergo IC in the future.
Other factors associated with early IC, including age, gender,
and the Charlson comorbidity index, may reflect the choices
made by surgeons and patients.
The results of population-based studies have shown that
[50 % of AC patients did not undergo early cholecystec-
tomy and[50 % of these patients did not undergo IC [5, 8].
The prognosis for these AC patients without surgery was
seldom reported. With advances in medical treatment, the
necessity of cholecystectomy may be further examined.
Percutaneous transhepatic cholecystostomy, a nonoperative
intervention, was studied as a bridge to surgery or as defin-
itive management in AC patients with high surgical risk [4].
However, few, if any, studies have investigated antibiotic
treatment in AC patients. Our results might provide some
important surgical risk–benefit information for patients or
clinicians and support a randomized, controlled trial to
compare AC patients who undergo early cholecystectomy
with those who receive antibiotic treatment.
The findings from our study do not indicate that anti-
biotic treatment was sufficient for patients with AC, but
tried to provide some benefit–risk profiles in this group.
Combined with the development of PTC in recent years,
the treatment algorithm for AC may be updated to focus on
nonoperative management, as many patients were inter-
ested in this method.
Limitations
The first limitation of the present study is that the number of
patients with recurrence was relatively small, which might
introduce a type II error. Second, although our hospital
provides all levels of care, the cohort from a single medical
center may introduce some selection bias. Third, the recur-
rence rate may have been underestimated because we could
not verify whether patients experienced recurrence or
underwent IC at other hospitals. However, all patients were
sent by emergency medical services to our emergency
department at the initial onset, suggesting that many would
be sent to our hospital by the service in the case of recurrence.
This may compensate to some extent for any underestima-
tion. Finally, because of the retrospective nature of this
study, there were no a priori criteria for surgical or antibiotic
treatment. This decision was negotiated between patients
and clinicians. Although this may introduce selection bias,
the result may be more applicable to daily practice.
Conclusions
The recurrence of AC in patients who received antibiotics
alone was low. The recurrence rate was higher within
100 days of AC. Because of the inherent limitations of a
retrospective study, further studies are needed to identify
factors associated with early recurrence.
Conflict of interest We declare that we have no conflicts of interest.
Funding None.
Appendix
See Table 5
Table 5 Severity according to the Tokyo guidelines for acute
cholecystitis
Grade Criteria
1 Mild Acute cholecystitis that does not meet the criteria
for a more severe grade
Mild gallbladder inflammation, no organ
dysfunction
2 Moderate 1. Elevated WBC count ([18,000/mm3)
2. Palpable tender mass in the right upper
abdominal quadrant
3. Duration of complaints [72 h
4. Marked local inflammation (biliary peritonitis,
pericholecystic abscess, hepatic abscess,
gangrenous cholecystitis, emphysematous
cholecystitis)
World J Surg (2014) 38:347–354 353
123

References
1. van der Linden W, Sunzel H (1970) Early versus delayed oper-
ation for acute cholecystitis. A controlled clinical trial. Am J Surg
120:7–13
2. Gurusamy K, Samraj K, Gluud C et al (2010) Meta-analysis of
randomized controlled trials on the safety and effectiveness of
early versus delayed laparoscopic cholecystectomy for acute
cholecystitis. Br J Surg 97:141–150
3. McGillicuddy EA, Schuster KM, Barre K et al (2012) Non-
operative management of acute cholecystitis in the elderly. Br J
Surg 99:1254–1261
4. Leveau P, Andersson E, Carlgren I et al (2008) Percutaneous
cholecystostomy: a bridge to surgery or definite management of
acute cholecystitis in high-risk patients? Scand J Gastroenterol
43:593–596
5. David GG, Al-Sarira AA, Willmott S et al (2008) Management of
acute gallbladder disease in England. Br J Surg 95:472–476
6. Hirota M, Takada T, Kawarada Y et al (2007) Diagnostic criteria
and severity assessment of acute cholecystitis: Tokyo guidelines.
J Hepatobiliary Pancreat Surg 14:78–82
7. Charlson ME, Pompei P, Ales KL et al (1987) A new method of
classifying prognostic comorbidity in longitudinal studies:
development and validation. J Chronic Dis 40:373–383
8. Csikesz N, Ricciardi R, Tseng JF et al (2008) Current status of
surgical management of acute cholecystitis in the United States.
World J Surg 32:2230–2236. doi:10.1007/s00268-008-9679-5
9. Festi D, Reggiani MLB, Attili AF et al (2010) Natural history of
gallstone disease: expectant management or active treatment?
Results from a population-based cohort study. J Gastroenterol
Hepatol 25:719–724
10. Riall TS, Zhang D, Townsend CM et al (2010) Failure to perform
cholecystectomy for acute cholecystitis in elderly patients is
associated with increased morbidity, mortality, and cost. J Am
Coll Surg 210:668–677
11. Wu JM, Wu YM, Lee CY et al (2012) Is early laparoscopic
cholecystectomy a safe procedure in patients when the duration
of acute cholecystitis is more than three days? Hepatogastroen-
terology 59:10–12
12. Norrby S, Herlin P, Holmin T et al (1983) Early or delayed
cholecystectomy in acute cholecystitis? A clinical trial. Br J Surg
70:163–165
13. Chandler CF, Lane JS, Ferguson P et al (2000) Prospective
evaluation of early versus delayed laparoscopic cholecystectomy
for treatment of acute cholecystitis. Am Surg 66:896–900
14. Casillas RA, Yegiyants S, Collins JC (2008) Early laparoscopic
cholecystectomy is the preferred management of acute chole-
cystitis. Arch Surg 143:533–537
Table 5 continued
Grade Criteria
3 Severe Acute cholecystitis accompanied by dysfunction
in any one of the following organs or systems
1. Cardiovascular dysfunction (hypotension
requiring treatment with dopamine [[5 lg/kg
per min] or any dose of dobutamine)
2. Neurologic dysfunction (i.e., decreased level
of consciousness)
3. Respiratory dysfunction (PaO2/FiO2 ratio,
\300)
4. Renal dysfunction (oliguria or creatinine
[2.0 mg/dL)
5. Hepatic dysfunction (PT-INR [1.5)
6. Hematologic dysfunction (platelet count,
\100,000/mm3)
WBC white blood cell, PaO2 partial pressure of oxygen in arterial
blood, FiO2 fraction of inspired oxygen, PT-INR prothrombin time-
international normalized ratio
354 World J Surg (2014) 38:347–354
123