Embed Size (px)
Citation preview

Long-term outcome after endoscopic stent therapyfor complications after bariatric surgery
Atif Iqbal • Brent Miedema • Archana Ramaswamy •
Nicole Fearing • Roger de la Torre •
Youngju Pak • Caleb Stephen • Klaus Thaler
Received: 6 May 2009 / Accepted: 13 April 2010 / Published online: 13 July 2010
� Springer Science+Business Media, LLC 2010
Although bariatric surgery effectively reduces the mortality
risk from obesity-related comorbidities [1, 2], it is associ-
ated with a 1–5% risk of anastomotic complications.
Anastomotic leaks have traditionally been treated with a
combination of drainage with long-term parenteral nutri-
tion or postanastomotic enteral nutrition, allowing the leak
to heal. Strictures at the gastrojejunostomy are initially
treated with repeated endoscopic dilation, but revisional
bariatric surgery is needed for refractory strictures with its
associated high complication rate. Chronic fistulas are
initially treated conservatively but often need high-risk
revisional surgery. Recently, endoscopic covered stents
have been used successfully for treatment of anastomotic
complications after esophageal resection [3–5]. Case series
evaluating stents to treat anastomotic leaks after Roux-en-
Y gastric bypass have shown success [6–9]. However, the
numbers of patients enrolled in these studies are small, and
only short-term outcomes are reported.
The primary aim of this study is to present long-term
healing rates after endoscopically placed covered stents in
the treatment of various anastomotic complications after
bariatric surgery. The secondary aim is to analyze symptom
improvement scores, complications, and factors affecting
stent migration.
Materials and methods
We performed a retrospective analysis of all patients
treated with endoscopic stents for staple-line complications
after bariatric surgery from January 2007 to January 2009.
The study was approved by the University of Missouri
Institutional Review Board.
Inclusion criteria were patients who underwent either
Roux-en-Y gastric bypass or sleeve gastrectomy with
subsequent anastomotic complications defined as acute
staple-line leaks, chronic anastomotic fistulas or refractory
anastomotic strictures. Acute leaks were defined as those
occurring within 1 month postoperatively. Refractory
anastomotic strictures were defined as persistent clinically
significant strictures that were endoscopically dilated more
than twice without resolution. Chronic fistulas were defined
as enterocutaneous or gastrogastric fistulas for longer than
1 month.
The stents were placed using both endoscopic and
fluoroscopic guidance with endoscopy being used to
delineate the area of leak, stricture or fistula. This pathol-
ogy was then marked with either a radiopaque marker on
the skin surface or by injecting water-soluble contrast in
the mucosa adjacent to the pathology to use as an internal
marker. Strictures were identified and dilated for at least
Presented at the SAGES 2009 Annual Meeting, April 22–24, 2009,
Phoenix, AZ.
Electronic supplementary material The online version of thisarticle (doi:10.1007/s00464-010-1203-y) contains supplementarymaterial, which is available to authorized users.
A. Iqbal � B. Miedema (&) � A. Ramaswamy � N. Fearing �R. de la Torre � C. Stephen � K. Thaler
Department of General Surgery, University of Missouri
Columbia, One Hospital Drive, MC 520E McHaney, Columbia,
MO 65212, USA
e-mail: [email protected]
A. Iqbal
e-mail: [email protected]
Y. Pak
Office of Medical Research, University of Missouri Columbia,
One Hospital Drive, MC 520E McHaney, Columbia, MO 65212,
USA
123
Surg Endosc (2011) 25:515–520
DOI 10.1007/s00464-010-1203-y
1 min with an 18-mm balloon before stenting. A flexible
guide wire was passed through the endoscope and down the
Roux limb or duodenum, depending on whether a gastric
bypass or sleeve was performed. The endoscope was then
removed, and fluoroscopy was used to position the stent
across the leak or stricture using the guide wire and radi-
opaque marker to position the stent properly. Repeat
endoscopy was performed to assess the need for placement
of additional stents if adequate proximal or distal coverage
was not achieved or if angulation was encountered at the
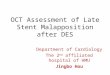
ends of the stent. Figure 1 presents the most common
pattern of stent positioning by the end of the study.
Both nitinol (Alimaxx-ETM, Alveolus Inc, Charlotte,
NC) and polyester (PolyflexTM, Boston Scientific Inc,
Natick, MA) silicone-covered stents were used in this
series. The polyester stent comes in 16, 18, and 21 mm
diameters, with varying lengths of 9, 12 or 15 cm. The
deployment system has a 12–14 mm diameter. The nitinol
or metal based stents come in 18 and 22 mm diameters, but
in 10 or 12 cm lengths; the metal-covered stents come in a
7-mm delivery system that makes passage possible through
tighter strictures. We used more nitinol stents as the study
progressed due to its decreased migration rate.
The day after stent placement, an upper gastrointestinal
contrast study was done. If no leak was present, a diet was
started. Oral nutrition consisted of a high-protein liquid diet
identical to that started in postoperative bariatric surgery
patients. After hospital discharge, patients were seen weekly
and an abdominal radiograph was taken to confirm adequate
stent position. Patients who started having abdominal pain or
dysphagia were evaluated with esophagogastroduodeno-
scopy and upper gastrointestinal contrast study.
The primary outcome measured was resolution rate.
Anastomotic leak resolution was defined as absence of
contrast extravasation from the bowel after the stent was
removed. Stricture resolution was defined as ability to
tolerate a regular diet after stent removal with symptomatic
and radiological improvement. Secondary outcome mea-
sures included procedure time, symptomatic improvement,
type of stent used, complications, and migration rates.
Complications were defined as a significant deviation from
the expected course that resulted in morbidity such as
failure of stent therapy, recurrent stricture or fistula, stent
migration, mucosal incorporation, and stent fracture or
kinking requiring removal. Stent migration was defined as
either radiologic or endoscopic evidence of migration with
uncovering of the area of leak, stricture or fistula. Criteria
for placement of[1 stent was less than 5 cm overlap in the
distal esophagus, proximal jejunum or radiological leak of
contrast between two stents. A standardized telephone
questionnaire was administered to assess improvement in
symptoms in all patients. The questionnaire used a 0–10
score for symptoms such as chest pain, heartburn, dys-
phagia, regurgitation, abdominal pain, nausea/vomiting,
type of diet, and dietary tolerance. The questionnaire was
administered by the same physician in all patients.
The statistical analysis was performed using the Fisher’s
exact test for categorical variables, and the Kruskal–Wallis
test to compare distributional differences in continuous or
ordinal outcome measures. Pairwise comparisons among
three groups were conducted where significance was found
from the Kruskal–Wallis test. In these multiple pairwise
tests, p-values B0.01 were considered significant; for all
other tests, p-values B0.05 were considered significant.
The analysis was done using SAS version 9.2.
Results
Twenty-six patients (14 leaks, 6 strictures, 3 fistulas, 2
leaks followed by stricture, and 1 leak followed by fistula)
were treated with a total of 55 endoscopic stent procedures
(27 polyester, 28 nitinol). Mean age was 47 years (range
30–67 years), and there were 19 females and 7 males. The
procedures included Roux-en-Y bypass in 24 patients and
sleeve gastrectomy in 2 patients, with mean operative time
for stent placement of 56 min. Demographic characteristics
of the patient population are shown in Table 1.Fig. 1 Most common pattern of stent placement during the later part
of the study. Arrow marks site of leak
516 Surg Endosc (2011) 25:515–520
123
Oral feeding was started in 81% of patients within 24 h
of stenting. The stent was removed after a mean of 27, 18,
and 49 days for the leak, stricture, and fistula group,
respectively. All patients with strictures had considerable
pain after stent placement that led to its removal within
8 days, except for one patient who tolerated the stent for
15 weeks. Short-term postoperative outcomes are shown in
detail in Tables 2 and 3.
The overall complication rate for the 55 stent placement
procedures was 47% (Table 4). Stent migration was the
most common complication (40%). Migrated stents could
be retrieved endoscopically in 82% cases, and passed
through the entire gastrointestinal (GI) tract in 9%. Lapa-
roscopic stent removal for stent-related complications was
necessary in 4 out of the 55 stents placed (7%), with the
indication being stent migration in 2 patients (4%), stent
incorporation into bowel mucosa in 1 patient, and a lapa-
roscopic omental patch for enterotomy in the Roux limb
after endoscopic stent extraction in 1 patient. One of the
two patients requiring laparoscopic stent extraction for
migration had a stricture, while the other had a fistula.
There was no mortality.
The factors significantly affecting the migration rate are
shown. Migration rate was significantly lower for nitinol
stents, overlapping stents, polyester stents C15 cm, nitinol
stents C12 cm, and for the last 30 stents placed as com-
pared with the first 25 stents (Table 5).
Of the 55 stents placed, 5 were 16 mm, 13 were 18 mm,
and 37 were 22 mm in diameter. No correlation between
stent diameter and migration rate was seen. Also, stent
length was 90 cm in 7, 100 cm in 15, 120 cm in 24, and
150 cm in 9. However, many of these patients had over-
lapping stents, thus the functional length may have been
greater. The length of the individual stents did not correlate
with migration rates.
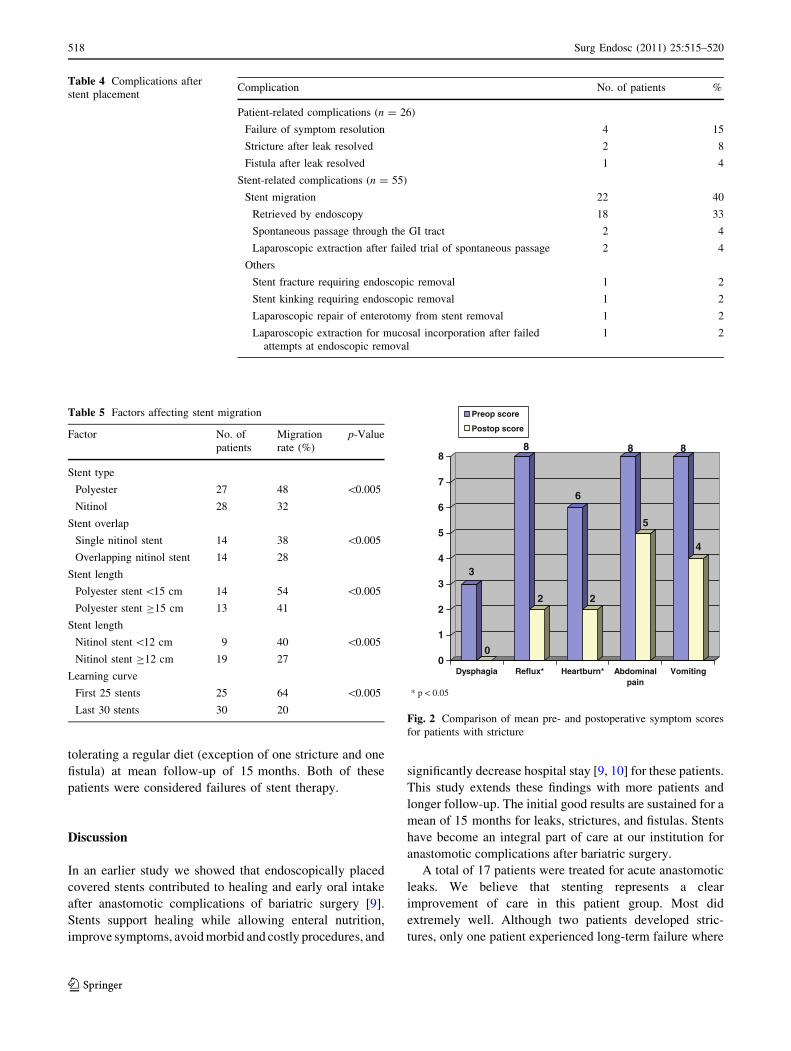
Symptomatic improvement occurred in 92% of patients
at long-term follow-up. Pre- and postoperative symptom
scores obtained by telephone questionnaire are compared
in Figs. 2 and 3 for patients with strictures and fistulas,
respectively. Patients with leaks underwent stent placement
emergently and had no baseline scores with which to
compare. Long-term outcomes ([1 year) are shown in
Table 6.
Resolution of leak, fistula or stricture after stent treat-
ment occurred in 22 of 26 patients (85%), at a mean of 46,
56, and 9 days for leak, fistula, and stricture, respectively.
Resolution was documented by radiographic imaging,
which occurred in the outpatient setting an average of
6 days after stent removal. A single stent procedure was
sufficient for either complete healing of the leak/fistula or
symptomatic improvement of the stricture in 12 patients
(46%). This included seven patients with leak, four with
stricture, and one with fistula. Fourteen patients required
two or more stenting sessions.
Four patients (15%) with leak (one), fistula (one) or
stricture (two) failed stent therapy. Two patients required
surgical intervention (one leak, one fistula). The leak
patient who failed was early on in our series and did not
undergo laparoscopic washout at the time of stent place-
ment despite evidence of abdominal contamination. Most
subsequent patients with leaks underwent laparoscopic
drainage with stent therapy unless the leak was diagnosed
within 24 h of initial surgery and no extraluminal collec-
tion was found on computed tomography (CT) scan. The
fistula patient was considered a failure after seven stent
placements were unsuccessful in healing the fistula and
reoperation was required. The two stricture patients who
failed stent therapy underwent two endoscopic dilations
after stent removal, with one patient tolerating a regular
diet at follow-up while the other continued to have inade-
quate fluid intake. Twenty-four patients (92%) were
Table 1 Demographic data of patients undergoing stent placement
for bariatric complications
Sex
(M:F)
Agea
(years)
Time of stent placement
after bariatric surgery
(weeks)a
Leak (n = 17) 7:10 49 \1
Stricture (n = 6) 0:6 46 70
Fistula (n = 3) 0:3 46 51
a Mean
Table 2 Short-term patient-related outcomes after initial stent
placement for bariatric complications (n = 26)
Mean time
stented (#)
Mean time to
healing (days)
Immediate
nutrition (%)
Leak (n = 17) 3 49 92
Stricture (n = 6) 1* 18 100
Fistula (n = 3) 4 56 50
* Group significantly different from the other two groups
Table 3 Short-term stent-related outcomes after stent placement for
bariatric complications (n = 55)
OR time
(min)
Mean days
stented
Complication
rate (%)
Migration
rate (%)
Leak (n = 17) 63 27 29* 37
Stricture (n = 6) 63 18* 50 18
Fistula (n = 3) 42 49 66 67
OR operating room
Complication rate includes failures and operative extraction of stents
for migration, incorporation or enterotomy but excludes stent
migration
* Group significantly different from the other two groups
Surg Endosc (2011) 25:515–520 517
123
tolerating a regular diet (exception of one stricture and one
fistula) at mean follow-up of 15 months. Both of these
patients were considered failures of stent therapy.
Discussion
In an earlier study we showed that endoscopically placed
covered stents contributed to healing and early oral intake
after anastomotic complications of bariatric surgery [9].
Stents support healing while allowing enteral nutrition,
improve symptoms, avoid morbid and costly procedures, and
significantly decrease hospital stay [9, 10] for these patients.
This study extends these findings with more patients and
longer follow-up. The initial good results are sustained for a
mean of 15 months for leaks, strictures, and fistulas. Stents
have become an integral part of care at our institution for
anastomotic complications after bariatric surgery.
A total of 17 patients were treated for acute anastomotic
leaks. We believe that stenting represents a clear
improvement of care in this patient group. Most did
extremely well. Although two patients developed stric-
tures, only one patient experienced long-term failure where
Table 4 Complications after
stent placementComplication No. of patients %
Patient-related complications (n = 26)
Failure of symptom resolution 4 15
Stricture after leak resolved 2 8
Fistula after leak resolved 1 4
Stent-related complications (n = 55)
Stent migration 22 40
Retrieved by endoscopy 18 33
Spontaneous passage through the GI tract 2 4
Laparoscopic extraction after failed trial of spontaneous passage 2 4
Others
Stent fracture requiring endoscopic removal 1 2
Stent kinking requiring endoscopic removal 1 2
Laparoscopic repair of enterotomy from stent removal 1 2
Laparoscopic extraction for mucosal incorporation after failed
attempts at endoscopic removal
1 2
Table 5 Factors affecting stent migration
Factor No. of
patients
Migration
rate (%)
p-Value
Stent type
Polyester 27 48 \0.005
Nitinol 28 32
Stent overlap
Single nitinol stent 14 38 \0.005
Overlapping nitinol stent 14 28
Stent length
Polyester stent \15 cm 14 54 \0.005
Polyester stent C15 cm 13 41
Stent length
Nitinol stent \12 cm 9 40 \0.005
Nitinol stent C12 cm 19 27
Learning curve
First 25 stents 25 64 \0.005
Last 30 stents 30 20
3
0
8
2
6
2
8
5
8
4
0
1
2
3
4
5
6
7
8
Dysphagia Reflux* Heartburn* Abdominalpain
Vomiting
Preop score
Postop score
* p < 0.05
Fig. 2 Comparison of mean pre- and postoperative symptom scores
for patients with stricture
518 Surg Endosc (2011) 25:515–520
123

the leak did not heal. This failure may have been prevented
by better mechanical clearing of abdominal contamination
at the time of the initial leak.
Treatment of strictures was not as uniformly successful.
The patients had significant pain after stenting, which
required stent removal at a median of 8 days after place-
ment. None of the patients have had revisional surgery, but
two of eight were considered failures due to the need for
further endoscopic dilation at a mean of 55 weeks. We
believe that stent therapy for strictures is beneficial and not
only decreases the need for revisional surgery but also the
number of endoscopic interventions required for symp-
tomatic control. So, in our experience, stent therapy has led
to a decrease in the number of interventions required for
symptomatic relief. The four patients treated by stenting
for fistula is a very limited experience. Three of the patients
did heal, while one required revisional surgery. Because of
the high risk of revisional surgery, we believe that stricture
and fistula patients are well served by a trial of stenting.
Migration away from the site of pathology continues to
be the major problem with endoscopic stenting as a treat-
ment modality [10]. With increased experience, we began
using longer and multiple overlapping stents. With this
strategy, our migration rate decreased to 27% (overlapping
covered nitinol stents) and we were able to approach the
migration rate for esophageal stents (24%), possibly due to
greater mucosal surface area in contact with the stents [3,
11–13]. Previous studies have shown that the main mor-
bidity of covered stents was migration while that for
uncovered stents was tissue ingrowth and difficult extrac-
tion [5, 6, 9]. Deployment of an uncovered stent within a
covered stent has been shown to reduce the migration rate
while avoiding tissue ingrowth [4]. These findings point to
the potential for slightly stiffer, less compliant, and longer
stents to help solve the problem of stent migration. The
nitinol (Alveolus) stents are designed with ‘‘antimigration’’
struts to minimize the amount of migration by inducing
impaling of the mucosa and providing better tissue
ingrowth. This may play a role in preventing migration.
Other techniques for stent fixation, including endoscopic
clip application or surgical suturing, failed in our hands.
We experienced a learning curve with the use of stents,
as evidenced by the lower migration rate (20%) with the last
30 stents. This can be attributed to refinements in technique,
attention to adequate coverage from the esophagus proxi-
mally to an adequately apposed segment of the jejunum
distally, willingness to deploy additional overlapping stents,
and use of longer stents to achieve the above purpose. It was
our impression that a larger-diameter stent decreased
migration rates. However, we did not have adequate num-
bers to demonstrate this conclusion statistically.
When migration occurs, it can usually be easily man-
aged. Most stents can be retrieved by upper endoscopy or
are passed through the GI tract. Surgical removal of the
migrated stent from the distal small bowel was only
required in two patients (8%), both with nitinol stents. This
is similar to the previously described rate in the literature.
Ko et al. reported on 888 patients with foregut stents
(including esophageal), with an 8% migration rate and a
4% surgical removal rate [7].
The optimal timing of stent duration is still unknown.
We did not see the problems that others have reported with
tissue hyperplasia at the ends of nitinol stents leading to
difficult extraction [14, 15]. We did have one patient who
required operative stent extraction due to mucosal incor-
poration after stenting for 16 weeks. Studies [14, 15] have
suggested routine stent removal no later than 6 weeks due
to the above-mentioned reason. Our current practice is to
leave stents in after leaks for 3–4 weeks. The time that
stents are left in for stricture is usually limited by
2
0
8
0
8
0
8
0
5
00
1
2
3
4
5
6
7
8
Dysphagia Reflux Heartburn Abdominalpain
Nausea
Preop score
Postop score
Fig. 3 Comparison of mean pre- and postoperative symptom scores
for patients with fistula
Table 6 Long-term outcome ([1 year) after stent placement for
bariatric complications
Mean
clinical
FU (weeks)
Mean
radiologic
FU (weeks)
Symptomatic
improvement
(%)
Failure
rate (%)
Leak (n = 17) 56 20 94* 6
Stricture (n = 6) 55 25 82 33
Fistula (n = 3) 89* 62* 75 33
FU follow-up
* Group significantly different from the other two groups
Surg Endosc (2011) 25:515–520 519
123

symptoms. Our preference is to leave them in for 8 weeks
if possible. Stents for chronic fistula are also left in 8 weeks
if tolerated well. Further studies are needed to better define
the optimal time for stent removal.
The strength of this study is that it is the largest clinical
experience with the longest follow-up for this patient
population to date, with encouraging outcomes. The pri-
mary weakness is the retrospective nature of the study.
Future studies are needed with long-term follow-up, espe-
cially in patients with strictures and fistulas, and also to
further elucidate the factors influencing stent migration.
Outcomes will likely be improved as stent manufacturers
customize stents for these indications.
Conclusions
Endoscopically placed covered stents are safe and effective
in treating acute leaks, chronic fistulas, and refractory
strictures after bariatric surgery. Covered stents are the
treatment of choice for acute leaks after bariatric surgery.
Stenting can provide rapid healing while simultaneously
allowing for oral nutrition and help prevent revisional
surgery in some patients with strictures. A small experience
suggests that stenting may contribute to healing for chronic
fistula. Stent migration, tissue ingrowth, and stent erosions
are problems and can potentially require surgical correc-
tion. There is room for improvement by the industry in
terms of stent design. We believe that use of endoscopi-
cally placed stents will become the preferred treatment for
bariatric patients with staple-line complications. Additional
studies are needed that address these complications and
occasional failures seen with stents.
Disclosures Authors Atif Iqbal, Brent Miedema, Archana Ra-
maswamy, Nicole Fearing, Roger DeLaTorre, Youngju Pak, Caleb
Steffen, and Klaus Thaler have no conflicts of interest or financial ties
to disclose.
References
1. Christou NV, Sampalis JS, Liberman M, Look D, Auger S,
McLean AP, MacLean LD (2004) Surgery decreases long-term
mortality, morbidity, and health care use in morbidly obese
patients. Ann Surg 240:416–423
2. Busetto L, Mirabelli D, Petroni ML, Mazza M, Favretti F, Segato
G, Chiusolo M, Merletti F, Balzola F, Enzi G (2007) Comparative
long term mortality after laparoscopic adjustable gastric banding
versus nonsurgical controls. Surg Obes Relat Dis 3:496–502
3. Radecke K, Gerken G, Treichel U (2005) Impact of a self-
expanding, plastic esophageal stent on various esophageal ste-
noses, fistulas, and leakages: a single-center experience in 39
patients. Gastrointest Endosc 61:812–818
4. Song GA, Kang DH, Kim TO, Heo J, Kim GH, Cho M, Heo JH,
Kim JY, Lee JS, Jeoung YJ, Jeon TY, Kim DH, Sim MS (2007)
Endoscopic stenting in patients with recurrent malignant
obstruction after gastric surgery: uncovered versus simulta-
neously deployed uncovered and covered (double) self-expand-
able metal stents. Gastrointest Endosc 65:782–787
5. Thompson AM, Rapson T, Gilbert FJ, Park KG (2004) Endo-
scopic palliative treatment for esophageal and gastric cancer:
techniques, complications, and survival in a population-based
cohort of 948 patients. Surg Endosc 18:1257–1262
6. Kim GH, Kang DH, Lee DH, Heo J, Song GA, Cho M, Yang US
(2004) Which types of stent, uncovered or covered, should be
used in gastric outlet obstructions? Scand J Gastroenterol
39:1010–1014
7. Ko HK, Song HY, Shin JH, Lee GH, Jung HY, Park SI (2007)
Fate of migrated esophageal and gastroduodenal stents: experi-
ence in 70 patients. J Vasc Interv Radiol 18:725–732
8. Salinas A, Baptista A, Santiago E, Antor M, Salinas H (2006)
Self-expandable metal stents to treat gastric leaks. Surg Obes
Relat Dis 2:570–572
9. Eubanks S, Edwards CA, Fearing NM, Ramaswamy A, de la
Torre RA, Thaler KJ, Miedema BW, Scott JS (2008) Use of
endoscopic stents to treat anastomotic complications after bari-
atric surgery. J Am Coll Surg 206:935–938
10. Fukumoto R, Orlina J, McGinty J, Teixeira J (2007) Use of
polyflex stents in treatment of acute esophageal and gastric leaks
after bariatric surgery. Surg Obes Relat Dis 3:68–72
11. Langer FB, Wenzl E, Prager G, Salat A, Miholic J, Mang T,
Zacherl J (2005) Management of postoperative esophageal leaks
with the polyflex self-expanding covered plastic stent. Ann
Thorac Surg 79:398–403
12. Hunerbein M, Stroszczynski C, Moesta KT, Schlag PM (2004)
Treatment of thoracic anastomotic leaks after esophagectomy
with self-expanding plastic stents. Ann Surg 240:801–807
13. Schubert D, Scheidbach H, Kuhn R, Wex C, Weiss G, Eder F,
Lippert H, Pross M (2005) Endoscopic treatment of thoracic
esophageal anastomotic leaks by using silicone-covered, self-
expanding polyester stents. Gastrointest Endosc 61:897–900
14. Eisendrath P, Cremer M, Himpens J, Cadiere GB, Le Moine O,
Deviere J (2007) Endotherapy including temporary stenting of
fistulas of the upper gastrointestinal tract after laparoscopic ba-
riatric surgery. Endoscopy 39:625–630
15. Song HY, Park SI, Do YS, Yoon HK, Sung KB, Sohn KH, Min
YI (1997) Expandable metallic stent placement in patients with
benign esophageal strictures: results of long-term follow-up.
Radiology 203:131–136
520 Surg Endosc (2011) 25:515–520
123