Embed Size (px)
Citation preview

The LiverJustin Harris OMS IV

Outline
• Anatomy
• Histology
• Physiology
• Liver Function Tests
• Pathophysiology

Anatomy• Blood supply
– Dual blood supply
– Portal Vein 75% blood supply (oxygen poor & nutrient rich)
– Hepatic Artery 25% blood supply (oxygen rich)
• Couinaud schemaGallbladder is between IV & V

Histology
• Liver Acinus
– Zone 1
• First to show bile duct occlusion changes
• First to regenerate
• Last to die from is-chemia
– Zone 2
– Zone 3
• First to show centrilobu-lar necrosis 2* to is-chemia with decreased CO

Reticuloendothelial Function
• Kupffer cells
– Make up 80-90% of fixed macrophages in the body reside within the liver sinusoidal lumen
• Ito/Stellate Cells
– Appear to be regulators of hepatocyte and endothelial cell function
– Activated in states of liver injury and increase fibrosis due to inhibition of apoptosis

Protein Synthesis
• Plasma Proteins
– Albumin
• ~10g/day are made (1/2 life is 22 days)
– Transferrin, haptoglobin, fer-ritin, hemopexin, & cerulo-plasmin
– Coagulation Factors
• Hepatocytes synthesize all clotting factors except VIII (synthesized by vascu-lar endothelium)

Drug Metabolism• Xenobiotics=> drugs/toxins not used in
normal metabolic pathways to maintain the integrity of a cell or tissue
• Phase I
– Oxidation, Reduction, Hydrolysis
– Cytochrome P450
• Phase II
– Conjugation

Hepatocyte Bile Formation
• Bile
– Bile Salts
– Phospholipids
– Conjugated Bilirubin
– Cholesterol
• Bile facilitates intestinal absorption of lipids and fat soluble vitamins
• Increase bile secretion
– Vagal stimulation, CCK, Gastrin, Glucagon

Liver Function Tests• Synthetic Function
– Albumin & Prothrombin Time
• Hepatocyte Injury
– AST
– ALT
• Secretory Function
– ALP
– GGT
– Bilirubin

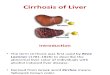
• Cirrhosis
• Characterized by destruction of hepatic parenchyma
– Replacement by fibrosis and regenerative nodules
• Causes:ETOH, Viral infections (Hep B&C), biliary obstruction, etc.
• Prognostic Tests
• MELD Score
• MELD= 3.78(serum bilirubin)+11.2(INR)+9.57(serum creatinine)+6.43
• Child-Turcotte-Pugh Classification
Hepatic Pathophysiology

Portal Hypertension
• Normal portal venous pres-sure (5-10mm Hg)
• Obstruction increases portal vein pressure and increases blood flow to the heart through collateral vessels
• Hallmark of Portal Hyper-tension
– Decreased intrahepatic NO
– Increased splanchnic NO

Acute Liver Failure
• Sudden loss of liver metabolic functions resulting in coagulopathy and encephalopathy
• Coagulopathy and acidosis are common = poor prognosis
• Hypoglycemia 2* to impaired gluconeogenesis in the liver
• Systemic hypotension may occur, even if there is a high CO, because of low SVR.

Summary
• Anatomy
• Histology
• Physiology
• Liver Function Tests
• Pathophysiology