Embed Size (px)
Citation preview

+Black Creek Community Health Centre
Diabetes Peer Support Group Project for the Black Caribbean Community
Live, Learn
And Share
In Partnership with:
Financially supported by:

+Live, Learn and Share - Background
Rates of diabetes in the Northwest part of Toronto, served by Black Creek Community Health Centre have higher rates of diabetes than in other parts of the city (ICES, 2007)
High rates of diabetes in African-Caribbean communities (8.5 %: CMAJ, 2010)
Clients and community have expressed desire to meet others living with diabetes in order to share experiences, decrease isolation, and learn management strategies.

+Live, Learn and Share
This project worked with community members in a participatory and inclusive process in order to develop a tool that is made byour community and used in our community.

+Peer Support Groups
Peer Support Groups are….
“…are informal networks of individuals who share a common experience or issue. Members get together to share support. The primary focus of self-help is emotional support, practical support and information exchange.”
People with diabetes supporting other people with diabetes.
Self-Help Resource Centre of Toronto www.selfhelp.on.ca

+Live, Learn and Share-Objectives
A culturally and ethnically-sensitive Training Guide developed by Caribbean community residents to help start Diabetes Peer Support Groups in our community and across Canada.
A group of trained, confident and active community residents knowledgeable about Diabetes Self-Management and Peer Support.
A documented evaluation of the project’s evolution and outcomes - Mina Singh, RN, PhD – Assistant Professor, School of Nursing, Faculty of Health, York University

+Live, Learn and Share-Process
An advisory committee was established, composed of 16 community members, and 8 health care professionals, and representatives of community agencies.
This committee provided input and informed the development of the training guide.
Based on the groups’ lived experiences, insight and expertise.

+Training Workshops - Diabetes
Provided by Black Creek CHC Diabetes Education Program – Diabetes Nurse Educator and Registered Dietitian
3 sessions (2.5 hours each)
Topics include: Diabetes Self-Management, Foot Care, Medications, Stress Management, Healthy Eating, Physical Activity, Blood Glucose Self-Monitoring.
Pre-Post Evaluation surveys – Knowledge based

+Training Workshops – Peer Support
Training provided by Self-Help Resource Centre
7 workshops (2 hrs each)
Topics include: An introduction to Peer Support, Communication, Group Planning, the Power of Listening, Dealing with Conflict and Evaluation.
Learned practical skills to help form, lead and maintain Peer Support Groups.

+

+Training Manual - Distribution
Distributed – Electronic and printed version available
Websites: Posted on Black Creek CHC website (www.bcchc.com) PHAC website, Canadian Diabetes Association, Ontario Health Promotion E-Bulletin
Distributed to Diabetes Education Programs, Central LHIN, Ministry of Health and Long-term Care, AOHC

+Some of our successes…
Diabetes Peer Support Group meets once a month at Black Creek Community Health Centre, with new members joining every month.
Attended CDA Professionals Conference (Edmonton) distributed copies of the manual to Diabetes Educators and organizations.
Group facilitator: Conference attendee and Radio Interview.
Central LHIN “LHINfo Minute” – Nov. 24 issue

+Live, Learn and Share - Phase 2
Phase 2: Spanish-speaking, South Asian, Vietnamese and Somali communities (November-March)
Include 2 workshops on Mental Wellness: Stigma, Race and Oppression, Stress Management, Depression and Anxiety (Across Boundaries)
Guide translated into Spanish, Urdu, Vietnamese and Somali

+
Live, Learn and Share
Thank You

+
Blackberry Healthcoaching &The Exercise Education & Training Program
Noah M.A. Wayne, MSc, CSEP CPT, PhD Candidate
School of Kinesiology & Health Science
Faculty of Health, York University
Black Creek Community Health Centre

+Worst case scenario…
Death by Budget Cut
PHOENIX, ARIZONA, USA — October 1, 2010(as reported in NY Times)
Arizona stopped financing certain transplant operations under the state’s version of Medicaid
Many doctors say decision amounts to a death sentence for low income patients
Lesson: in a health care system that does not economize, low income patients are hurt the most

+

+Current trend of Health Care spending in Ontario
In the past decade, the Ontario government’s health expenditure cost curve has grown by an average of 7.7% per year. The major categories of expenditures have grown on average, as follows:
– hospital expenditures by 6.5 % per year; – physician expenditure by 7.8 % per year; – drug expenditure by 9.2 % per year; – public health by 12.7 % per year; – and other institutions including long term care homes by
7.2 % per year.
Canadian Institute for Health Information, November 2009
+Diabetes as Pivotal: Taking a stand
Number of identified diabetics has increased by 50% (since 2002)
(MOHLTC, 2010)
Diabetes is on the rise. In 2007/08, approximately 969,000 Ontarians had diabetes. By 2010, that number may reach 1.2 million (Lipscombe 2007).
Although prevalence may be due to newly dx’ed cases or longevity, the diabetes population has increased from 7.5% (2002) to > 10% currently.
The Ontario Diabetes Strategy (ODS) aims to catalyze improved diabetes management
+Diabetes type 2 – economic consequences
Absence of ComplicationsNewly Diagnosed = $3115Subsequent Years = $2109
With ComplicationsYear of Event = $15,186 ($2,730-$34,470)Subsequent Years = $3,967 ($1,945-$10,038)
Death = $8,051-$8,556
O’Reilly, 2006

+Program Costs / Cost Savings
Yr. since Dx
Avg. health care
costs
5 % reduced
10 % reduced
20 % reduced
30 % reduced
40 % reduced
1 $5,329 $266 $532 $1,065 $1,598 $2,131
2 $4,155 $207 $415. $831 $1,246 $1,662
3 $3,998 $199 $399 $799 $1,199 $1,599
O’Reilly, 2006
1.2 million people with T2DM in 20105% reduction in care cost (3rd year from Dx) = $339 million $4.9 billion in 2010
Ontario Diabetes Cost Model

+Inactivity and health care usage
Physical inactivity increases hospital stays, and use of physician and nurse services
An inactive person:
Spends 38% more days in hospital
Uses 5.5% more family physician visits
13% more specialist services
12% more nurse visits
Health Economics. 2009; VOL.18: 885–901
+Physical activity & type 2 diabetes prevention
Only 52.5% of Canadians are at least moderately active during their leisure time
(CCHS, 2009)
Inactivity increases insulin resistance, which is intimately linked to type 2 diabetes
150 minutes of accumulated PA per week is associated with a ~60% decrease in the risk of type 2 diabetes
JAMA. 2003 ; VOL. 289(14), 1785-1791

+Physical activity and diabetes management
CDA Clinical Practice Guidelines, 2008

VHA Care Coordination / Home Telehealth
Comparisons made from one year prior to enrollment to 6 months post enrollment in remote patient monitoring program:19.74% reduction in hospital admissions25.31% reduction in bed days of care Patient Acceptance high – only 10% declined remote monitoringPatient satisfaction 86%Average cost $1,600 per patient per annum compared to $13,121 for primary care and $77,745 for nursing home care
TELEMEDICINE and e-HEALTH. 2008; VOL.14(10):1118-1126

+ Effects of Cell Phone Short-Message Service (SMS) on Antiretroviral Treatment (ART) Adherence in Kenya: A
Randomized Trial
N = 538 HIV-infected, antiretroviral (ART) -naive adults
initiating therapy in a randomized controlled trial (RCT)
A weekly short message service (SMS) cell phone intervention compared to standard of care at 3 HIV clinics
Patients assessed at 6 & 12 mo. visits post initiating ART
Primary outcomes:
self reported perfect ART adherence (>95% of doses by 30 day recall at both visits)
plasma HIV-1 viral RNA load suppression (< 400 copies/ml) at 12 mos.
Simple technology + Social engagement = health change
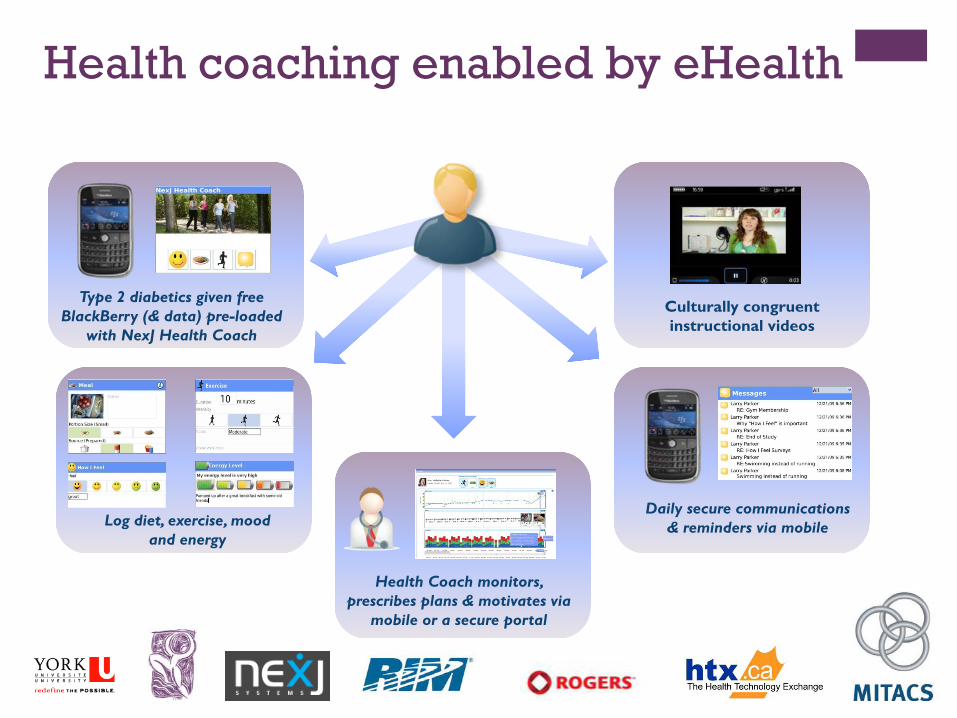
Type 2 diabetics given free BlackBerry (& data) pre-loaded
with NexJ Health Coach
Log diet, exercise, mood and energy
Health Coach monitors, prescribes plans & motivates via
mobile or a secure portal
Daily secure communications & reminders via mobile
Culturally congruent instructional videos
Health coaching enabled by eHealth

+eHELP Study - Measures
1 - arm study: 3 planned improved versions of Health Coach software
Anthropometrics:HbA1C measures: Baseline; 3 mo; 6 mo; 12 mo (post)Cholesterol (HDL, LDL)Pre/Post Exercise Blood Pressure, Blood Glucose LevelsBMI, Waist Circumference
Psychometric Measures: Baseline; 6 moProfile of Mood States-SF Vigor Scale (POMS-SF-V)Center for Epidemiologic Studies-Depression Scales (CES-D):Ryff Scale of Psychological Well-BeingSatisfaction with Life ScalePositive and Negative Affect ScheduleHospital Anxiety and Depression Scale

+Blackberry Healthcoach Software

+Meals

+Exercise

+How I Feel

+Exercise Education/Training Room

+Exercise Education/Training Room
Staff:Certified Exercise Physiologist - CSEPCertified Personal Trainers - CSEPKinesiology Student Volunteers
Responsibilities:Provide guidance, information and a safe learning environment for effective and safe exerciseEnrollmentScreening (PARQ + PARMEDx)SchedulingExercise TrackingMotivational phone calls to registrants

+Exercise Education/Training Room
December 9, 2010
434 registered community membersFunding for CEP and CPTs paid for through eHELP research funding (Ministry of Research and Innovation – Health Technology Exchange
Co-Principal Investigators: Paul Ritvo, Ph.D., Joseph Cafazzo, Ph.D.

+CHC Exercise Education Program
Exercise Education
Room
Seniors
Youth
DiabetesNew Mothers
Teens
+Next Steps...
Central LIHN call for proposals (HSIP) submitted Sept 3, 2010
• Total ask: $68,695
To expand the Exercise Education/Training Program and integrate into various clinical and promotion program areas in BCCHC
Funding would support full time exercise specialists (CEP & CPT) and associated program costs
In line with LIHN Funding Priorities: Health Equity & Chronic Disease Management
Currently partnered with North York General Hospital for eHELP study. Connections to Humber River Hospital through Diabetes Education Program

+Thank you.
Noah Wayne, M.Sc., CPT
PhD Candidate
School of Kinesiology and Health Science
York University
416-889-7289
Paul Ritvo, PhD CPsych
Associate Professor
School of Kinesiology and Health Science
York University
416-580-8021
Presentation to the Central LHIN
Community Engagement and the 100 Day Action Plan
December 14, 2010

Impetus and Approach• York Central Hospital Board sees community
engagement as high priority
• Community engagement approach initiated more than 2 years ago, now integrated into ‘how we do business’
• Aligned with Central LHIN and MOHLTC guidelines and consistent with hospital commitment to accountability and transparency

Operational Review

4
Our Context
• Recent completion of important part of a longer term transformative journey
• We raised the bar on many levels and made big strides towards a new normal: accountability, cost efficiency, strategic focus, while we maintain quality and service levels
• Although we have more to accomplish, we must ensure that we maintain our gains
• Reviewing the keys to our recent success will help us capture our learnings so we can continue to improve as we tackle new challenges

5
Future Planning
Culture of Safety
Balanced Budget
Wildly Important Goals for 2010/11
FROM TO

6
Community Engagement at YCHCommunity engagement is an ongoing process with an
individual or group that has a vested interest in YCH
It concentrates on building and strengthening internal and external relationships by opening doors to innovation,
creative problem solving, community trust and support, improvements in services and conflict resolution
7
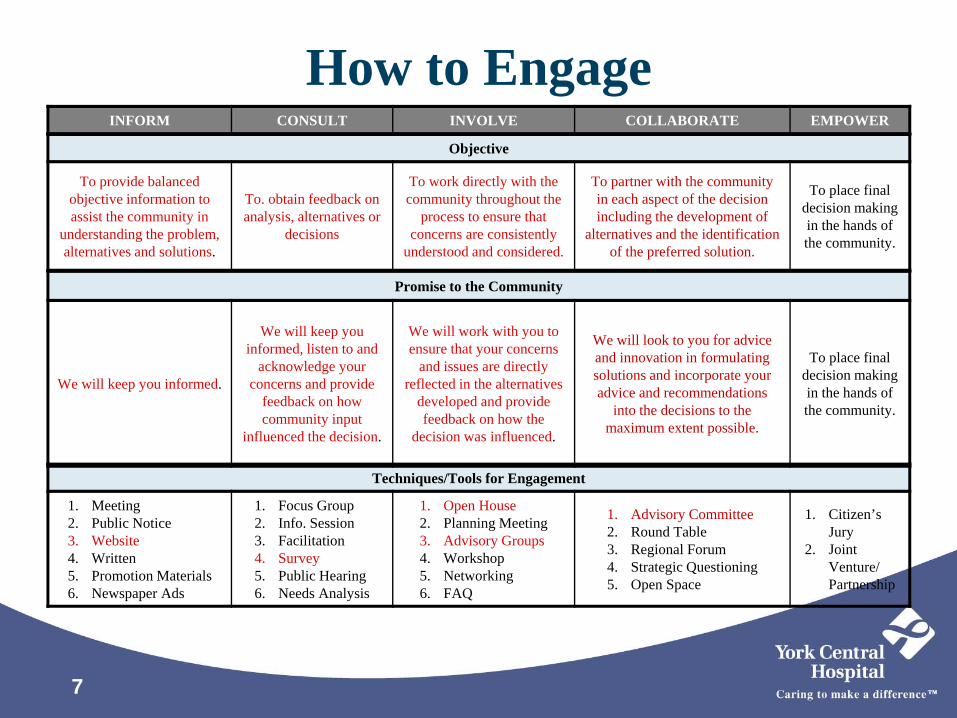
How to Engage
Techniques/Tools for Engagement
1. Meeting2. Public Notice3. Website4. Written5. Promotion Materials6. Newspaper Ads
1. Focus Group2. Info. Session3. Facilitation4. Survey5. Public Hearing6. Needs Analysis
1. Open House2. Planning Meeting3. Advisory Groups4. Workshop5. Networking6. FAQ
1. Advisory Committee2. Round Table3. Regional Forum4. Strategic Questioning5. Open Space
1. Citizen’s Jury
2. Joint Venture/ Partnership
Promise to the Community
We will keep you informed.
We will keep you informed, listen to and
acknowledge your concerns and provide
feedback on how community input
influenced the decision.
We will work with you to ensure that your concerns
and issues are directly reflected in the alternatives
developed and provide feedback on how the
decision was influenced.
We will look to you for advice and innovation in formulating solutions and incorporate your advice and recommendations
into the decisions to the maximum extent possible.
To place final decision making in the hands of the community.
INFORM CONSULT INVOLVE COLLABORATE EMPOWER
Objective
To provide balanced objective information to assist the community in
understanding the problem, alternatives and solutions.
To. obtain feedback on analysis, alternatives or
decisions
To work directly with the community throughout the
process to ensure that concerns are consistently
understood and considered.
To partner with the community in each aspect of the decision including the development of
alternatives and the identification of the preferred solution.
To place final decision making in the hands of the community.

8
Checklist to determine whether or not community engagement is required

9
Approach for stakeholder analysis

10
The 100 Day Journey
Insert updated Chart used in Richard’s Leader’s Forum presentation re From to Current State
From To
Year end deficits and one time solutions
Financial flexibility and stability for longer term
Culture of revenue seeking Culture of fiscal accountability and efficiency
Average among peers in quality, safety and patient satisfaction
Leaders safety, quality and patient satisfaction
Too many competing priorities Focus on Wildly Important Goals (WIGS) to achieve strategic directions
Organizational change Organizational stability
Operationally focused Strategic, future oriented, innovation focus

11
Preparing for Success
• Assembled Change Team and Developed 100 Day Action Plan
• Developed Communications and Engagement Plan
• Developed Action Plan Project Structure
• Identified Project Managers and Sponsors
• Assembled Project Teams

12
The Action Plan Project Structure

13
The Change Team
Jo-anne MarrDavid StolteDr. Victoria ChanDr. Larry GrossmanDr. Stan HermanDr. Nick VoudourisMelina CormierJennifer MillerBeth SnyderRichard Tam

14
Project Managers and Sponsors J. Miller
T. Rivera
B. Snyder
V. Chan
J. Marr
L. Grossman
R. Tam
D. Stolte
C. Johnson
S. Swartz
S. McLachlan
Y. Geverink
K. Jarvi
C. Avrich
C. Palmer

15
• Began building AWARENESS of the need for change beginning with open and transparent communications around our Operational Review
• We built on that understanding and sense of urgency by articulating both the risks of not changing as well as benefits of implementing required changes
• Launched 100 Day Action Plan supported by multi-faceted communications strategy with strong and highly visible executive leadership
Awareness Building

16
Internal Awareness
• Formally receive and endorse the Operational Review Report, posting the full report and its findings on special feature section on home page of intranet
• Continued to develop this section with regular updates, question and answer documents and Staff Forum presentations
• Organization wide e-mail messages/updates including Board Chair Message, From the Desk of the CEO messages, Change Team Communiqués

17
Internal Awareness

18
Internal Awareness

19
External Awareness
• Media releases and resulting coverage re Operational Review Report and Hospital Improvement Plan
• News paper ads leading to special HIP feature section on website with Community On-line Survey
• Funding announcement and media release re successful completion of 100-Day Plan

20
External Awareness

21
External Awareness
22
• We built DESIRE to support the change and increased personal motivation through individual and group engagement
• With the development of the Change Team we achieved a strong leadership coalition which emphasized a solutions focused approach
• Simultaneous engagement of both internal and external audiences helped to achieve greater understanding and support
• Frequent discussion and open sharing of progress updates helped to engage employees in change and reduce resistance
Desire Building

23
Special One-on-One or Group Meetings:• Medical Staff Association• Directors and Managers Forum• Physician Leaders Meetings• Fiscal Advisory Committee Meeting• General Staff Forums• Weekend and Night Staff Forums• Special Hospital, Foundation and Volunteer
Board Presentations
Internal Engagement

24
Internal Engagement

25
Internal Engagement –Project Teams
26
External Engagement• Meetings with/updates to LHIN, MPPs, MPs, Mayors and
Councils, Chamber of Commerce, Service Clubs, Community Service Partners, Spiritual Care Leaders, General Public
• Meeting with local Mental Health Service Providers around possible service role change regarding the hospital’s Child and Family Mental Health Services
• Special Hospital Improvement Plan (HIP) Section on homepage of website with On-line Community Survey re HIP
• Telephone Survey of 500 local residents
27
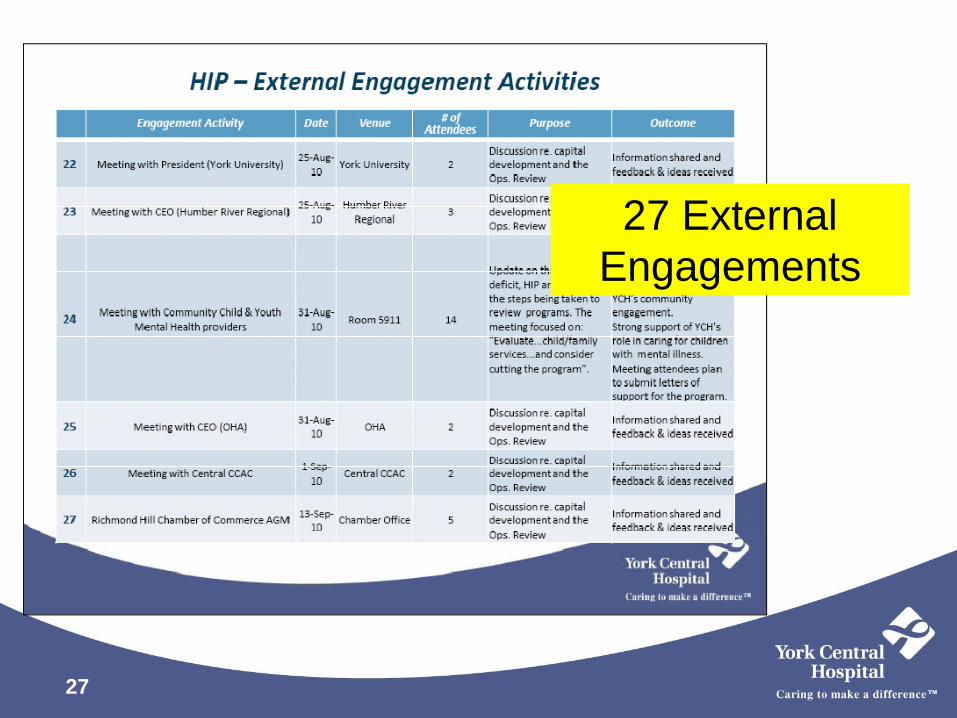
27 External Engagements

28
External
Engagement

29
External
Engagement
30
• We fostered the ABILITY to implement new skills and processes; moving from baseline competence toward skills fluency in both financial and process management skills
• Introduced monthly operational review meetings for all directors and managers supported by on-line templates to help leaders identify and develop strategies re areas for improvement
• Also continued to support ongoing initiatives in support of several Lean value streams in Surgery and Central Staffing during this same period
Fostering Ability

31 31
Monthlyperformance reviews
Weekly project updates
Daily visual management
32
Lean Teams

33
Reinforcing the Change• We are now in the process of REINFORCING the
change by integrating performance management mechanisms into our ongoing operations
• Held 100-day Action Plan Celebration to reinforce success, bring closure to period of intense level of focus and activity, reinforce confidence and capacity
• Continue with performance management processes and mine experience for continued learning and confidence-building

34
100 Day Celebration

35
100 Day Action Plan Dashboard
IndicatorBaseline
(Apr – July)August September October
At or better than
baseline?
Monthly Budget Deficit $1.0 M $0.64 M $0.57 M $0.05 M Yes
Patient Satisfaction (Would you recommend YCH?) 63 60 65 Available
soon Yes
Mortality Ratio (HSMR) 66 83 78 Available soon *
MRSA infection rate 0 0 0 0 Yes
CDI rate 0.28 0.31 0.32 0.41 No
VRE infection rate 0 0 0 0 Yes
ED Wait time indicators 3 of 4 3 of 4 3 of 4 2 of 4 No
Critical Incidents 0.75 3.0 0 3.0 No
Staff Absenteeism 4.2 3.5 4.7 4.0 Yes
Status Date: November 18, 2010
*within national benchmark levels

36
Action Plan Savings Update
36
Area of Focus Initiatives
SavingsTarget*
Savings in Progress*
Operational Efficiencies
Supply Chain $1 M $1 M
Bed Management and Patient Flow $1 M $1.6 M
Program Efficiency, Productivity and Performance $5.5 M $0.8 M
Management and Non-union Restructuring $0.5 M $0.5 M
Human Resources Efficiencies(e.g., decrease agency and OT)
$0.5 M $0.3 M
Total $8.5 M $4.2 M
November 1, 2010* Annualized amount


1
Central LHIN Community Engagement Optimizing Best Practices
Thomas O’ShaughnessyDirector, System Integration and Engagement
Central LHIN Board PresentationDecember 14, 2010

LHIN Role – Community Engagement
• Undertake ongoing engagement of the community, including the French and Aboriginal populations, and health service providers on priority setting and the development of the Integrated Health Service Plan
• Ensure that health service providers engage their communities on decisions and priorities (through provisions in Accountability Agreements)
• Enable ongoing advice from regulated health professionals by establishing a Health Professionals Advisory Committee
2

The Value of Engagement• A health system that reflects local needs and supports effective
use of resources
• Collaborative processes by which people are engaged in decision-making on issues that touch them directly
• Mutual education and dialogue – understanding public and provider perspectives of a high performing system and sharing system knowledge of its strengths, challenges and opportunities
• Transparency, openness and trust and enabling a better result (“good planning”)
3

Key Elements of Engagement 1. Providing information and knowledge
2. Providing opportunities for people to share their own ideas /opinion/feedback
3. Engaging in dialogue (to identify/resolve issues, answer questions, build consensus and support) and to partnership-build
4. Following up and demonstrating the impact/outcome of engagement every time
4
Towards LHIN-wide Best Practices • December 2009 – Steering Committee formed (LHIN CEOs
and Ministry representatives)
• January 2010 – Provincial Work Group formed to examine performance indicators and guidelines
• Spring 2010 – Work Group tasks complete and recommendations forwarded to Ministry & LHIN CEOs
• August 2010 – Ontario Ombudsman Report released
• December 2010 – Anticipated implementation of best practices to achieve and sustain high quality community engagement consistently across all LHINs
5

Provincial guidelines, tools and performance indicators • Proposed guidelines are based on public engagement
professional best practice
• Performance measures considered “Engaging with Impact” Report (MASS LBP)
• Guidelines/tools fulfill an obligation in the Ministry/LHIN Performance Agreement (MLPA)
• Will evolve over time as measurement becomes more sophisticated (i.e. more data, better target setting, better understanding of value in measurement)
6

Shared Definition of Community Engagement • Community engagement refers to the methods by which LHINs
and Health Service Providers interact, share and gather information from and with their stakeholders
• The purpose of community engagement is to inform, educate, consult, involve and empower stakeholders in both health care or health service planning and decision-making processes to improve the health care system
• Community engagement activities can be ongoing or project specific, outbound or inbound
7

Strategic Approach to Community Engagement
8
• Careful Planning and Preparation
• Demographic Diversity
• Collaboration and Shared Purpose
• Openness and Learning
• Transparency and Trust
• Impact and Action (participatory effort)
• Sustained Engagement and Participatory Culture
Adopted from the National Coalition for Dialogue and Deliberation

New Guidelines – An Overview • Each LHIN will publish an annual plan for community
engagement
• LHINs agree to use consistent planning process including early identification of interested communities
• Participants will be asked to evaluate their participation in every engagement activity
• LHINs will demonstrate how community inputs & outputs were tabled for decision-makers
9

Implementing Engagement Best Practices in Central LHIN • Central LHIN is currently working with Health Service Providers to
define community engagement expectations guided by provincial directions
• A Community Engagement evaluation tool that incorporates these criteria has also been developed and will be used to ensure alignment of provider community engagement with these principles , including through:
• Annual Health Service Provider Community Engagement Plans
• Performance/Health System Improvement Plans
• Health system integration per the Local Health System Integration Act 2006
10

• Development of annual plan that is publicly available and reviewed on a bi-annual basis
• Stakeholder assessment and individual community engagement informs any planned, unplanned or perceived change in access to services
• Engagement efforts are built upon year over year and progress is demonstrated by using best practices
• Each community engagement activity is evaluated to inform future planning (includes participant feedback)
• Results of community engagement initiatives are shared with provider decision-makers, including the Board
11
Proposed Health Service Provider Community Engagement Expectations

Key Central LHIN 2010/11 Engagement Strategies
12
Integrated Health Service Plan Launch Series o Five community engagement sessions across
Central LHIN during June – September 2010 with plans for similar engagements in 2011 (with focus on the consumer)
o 175 participants, including consumers and health service providers (multi-sector)
French and Aboriginal Engagemento Ongoing engagement with Chippewas
Reserve on Georgina Island and participation in Aboriginal GTA LHIN initiatives
o Will work with newly announced French Language Planning Entity
Better Engagement Through Technologyo Improving Central LHIN website (recently
updated to include additional bilingual components)
o Implementing on-line tools to enable independent consumer/provider feedback on key issues
Primary Care Engagement
o Established interdisciplinary Primary Care Action Group
o Goal is to enhance engagement and integration of primary care and support Integrated Health Service Plan implementation

Looking Forward to 2011/12 Engagement Priorities
• Enhancing collaboration and joint planning with community/social service and housing sectors regarding services for people with complex care needs
• Strengthening local quality improvement capacity to support the Excellent Care for All Act and other quality initiatives in partnership with the Ontario Health Quality Council
• Engaging our health service providers in a comprehensive strategy to improve patient transitions through the health system and improve Alternate Level of Care performance
• Expanding opportunities to regularly and directly engage Central LHIN consumers, including through quick-poll web technology
13