Embed Size (px)
Citation preview
Full Terms & Conditions of access and use can be found athttp://www.tandfonline.com/action/journalInformation?journalCode=iptp20
Download by: [University of Nevada Las Vegas], [Dr Emilio Puentedura] Date: 12 July 2016, At: 07:42
Physiotherapy Theory and PracticeAn International Journal of Physical Therapy
ISSN: 0959-3985 (Print) 1532-5040 (Online) Journal homepage: http://www.tandfonline.com/loi/iptp20
Combining manual therapy with painneuroscience education in the treatment ofchronic low back pain: A narrative review of theliterature
Emilio J. Puentedura PT, DPT, PhD & Timothy Flynn PT, PhD
To cite this article: Emilio J. Puentedura PT, DPT, PhD & Timothy Flynn PT, PhD (2016)Combining manual therapy with pain neuroscience education in the treatment of chroniclow back pain: A narrative review of the literature, Physiotherapy Theory and Practice, 32:5,408-414, DOI: 10.1080/09593985.2016.1194663
To link to this article: http://dx.doi.org/10.1080/09593985.2016.1194663
Published online: 30 Jun 2016.
Submit your article to this journal
Article views: 141
View related articles
View Crossmark data
Citing articles: 1 View citing articles

PERSPECTIVE
Combining manual therapy with pain neuroscience education in the treatmentof chronic low back pain: A narrative review of the literatureEmilio J. Puentedura, PT, DPT, PhDa, and Timothy Flynn, PT, PhDb
aDepartment of Physical Therapy, University of Nevada, Las Vegas, Las Vegas, NV, USA; bSchool of Physical Therapy, South College, Knoxville, TN, USA
ABSTRACTTeaching people with chronic low back pain (CLBP) about the neurobiology and neurophysiology oftheir pain is referred to as pain neuroscience education (PNE). There is growing evidence that whenPNE is provided to patients with chronic musculoskeletal pain, it can result in decreased pain, paincatastrophization, disability, and improved physical performance. Because the aim of PNE is to shiftthe patient’s focus from the tissues in the low back as the source of their pain to the brain’sinterpretation of inputs, many clinicians could mistakenly believe that PNE should be a “hands-off,”education-only approach. An argument can be made that by providing manual therapy or exercise toaddress local tissue pathology, the patient’s focus could be brought back to the low back tissues asthe source of their problem. In this narrative literature review, we present the case for a balancedapproach that combines PNE with manual therapy and exercise by considering how manual therapycan also be incorporated for interventions with patients with CLBP. We propose that as well asproducing local mechanical effects, providing manual therapy within a PNE context can be seen asmeeting or perhaps enhancing patient expectations, and also refreshing or sharpening body schemamaps within the brain. Ideally, all of this should lead to better outcomes in patients with CLBP.
ARTICLE HISTORYReceived 12 November 2015Revised 28 January 2016Accepted 5 May 2016
KEYWORDSBody schema; exercise;manual therapy;neuroscience; pain; patientexpectations
Introduction
According to a report from the Institute of Medicine,the financial toll of chronic pain, of which chronic lowback pain (CLBP) is the leading condition, is estimatedto cost between $365 and $560 billion per year(Committee on Advancing Pain Research, Care andEducation, 2011). CLBP is a highly prevalent condition,which imposes an enormous economic burden ontoday’s society. The suffering associated with CLBPcan reduce a person’s quality of life and lead to long-term disability, absenteeism from work, and excessivehealthcare utilization (Gore et al, 2012; Ibrahim,Tleyjeh, and Gabbar 2008; Melloh et al, 2008).
The first clinical practice guideline for the managementof low back pain was published in 1987 by theQuebec TaskForce (Spitzer, 1987). Since then, there has been exponen-tial growth in research in this area, with over 2500 clinicaltrials and more than 32 systematic reviews evaluatinginterventions for low back pain reported in the Cochranedatabase (Koes et al, 2010). A review of the latest clinicalpractice guidelines for CLBP finds consistent recommen-dations for supervised exercises, cognitive behavioral ther-apy and multidisciplinary treatment, but shows somediscrepancies for recommendations regarding spinal
manipulation (manual therapy) and drug treatment(Delitto et al, 2012; Koes et al, 2010).
A relatively new and promising approach in themanagement of CLBP has focused on teaching peopleabout the neurobiology and neurophysiology of pain,which is referred to as pain neuroscience education(PNE) (Butler and Moseley, 2013; Louw, Diener,Butler, and Puentedura, 2011; Puentedura and Louw,2012). Several randomized controlled trials and tworecent systematic reviews have reported favorable out-comes following PNE in patients with chronic pain interms of reduced pain, pain catastrophization, disability,and improved physical performance (Clarke, Ryan, andMartin, 2011; Louw, Diener, Butler, and Puentedura,2011; Moseley, 2002; Moseley, 2003a; Moseley, 2003b;Moseley, Nicholas, and Hodges, 2004). The focus of PNEis reconceptualization of pain by teaching patients moreabout the neurobiological and neurophysiological pro-cesses involved with their pain experiences versus focus-ing solely on tissue pathology. In the patient with CLBP,this pain reconceptualization attempts to help themunderstand that pain and tissue injury are differentconstructs (Moseley, 2004a, Moseley, 2005; Moseley,Nicholas, and Hodges, 2004).
CONTACT Emilio J. Puentedura, PT, DPT, PhD [email protected] Department of Physical Therapy, University of Nevada, Las Vegas, 4505 S.Maryland Parkway, Box 453029, Las Vegas, NV 89514-3029, USA.Color versions of one or more of the figures in this article can be found online at www.tandfonline.com/iptp.
PHYSIOTHERAPY THEORY AND PRACTICE2016, VOL. 32, NO. 5, 408–414http://dx.doi.org/10.1080/09593985.2016.1194663
© 2016 Taylor & Francis
Dow
nloa
ded
by [
Uni
vers
ity o
f N
evad
a L
as V
egas
], [
Dr
Em
ilio
Puen
tedu
ra]
at 0
7:42
12
July
201
6

Through their training and education, most manualtherapy clinicians are educated in the biomedical modelof pain (Kaltenborn and Lindahl, 1969; Maitland, 1973;Nijs et al, 2013). Underlying this traditional model of painis the assumption that there is a direct link between theamount of local tissue damage and the pain experiencedby the patient (Haldeman, 1990). Following this biome-dical model, manual therapy clinicians might concludethat addressing the underlying pathology (presumed bio-mechanical fault) should result in a reduction of symp-toms and subsequent recovery of normal function by thepatient. In the case of acute low back pain, where noci-ception from tissues in the low back is the dominant painmechanism, this approach seems appropriate and hasbeen shown to provide significant benefit when providedearly in the course of care (Childs et al, 2015; Fritz et al,2015; Rhon and Fritz, 2015). However, in the case ofCLBP, there is often little to no adherence to this biome-dical model of pain, and the local application of manualtherapy alone is rarely followed by any lasting reductionin symptoms and improvement in function (Delitto et al,2012; Gore et al, 2012; Rubinstein et al, 2011).
Manual therapists may therefore be left with a con-undrum when treating patients with CLBP. Currentevidence suggests that PNE can be effective, with theobjective being to deemphasize the tissues of the lowback as the dominant source of the problem and empha-size a deeper understanding of the pain experience as themeans to eventual recovery (Clarke, Ryan, and Martin,2011; Louw, Diener, Butler, and Puentedura, 2011). Onthe surface, this might suggest a “hands-off” approach totherapeutic interventions. An extension of this argumentis that any application of manual therapy interventionsto the low back would re-focus the patient on theirtissues (back) as the source of their chronic pain, andthereby undo any progress expected with PNE and exer-cise/activity. This “hands-off” approach may be seen as“swinging the pendulum” too far from the biomedicalmodel of pain (Jull and Moore, 2012).
The objective of this narrative is to review the literaturesupporting the inclusion of manual therapies in the ther-apeutic management of CLBP by re-thinking the value of“hands-on” interventions in combination with PNE andsupervised exercise. We propose the need to balance PNEwith manual therapy in the treatment of CLBP to meetpatient expectations and beliefs which may enhance thetreatment with an improved brain body schema.
How does manual therapy work?
Manual therapy can be defined as the provision ofmobilization/manipulation techniques to address mus-culoskeletal pain and dysfunction (American Physical
Therapy Association, 2004). The American PhysicalTherapy Association (APTA) defines manual therapytechniques as “skilled hand movements and skilledpassive movements of joints and soft tissue and areintended to improve tissue extensibility; increaserange of motion; induce relaxation; mobilize or manip-ulate soft tissue and joints; modulate pain; and reducesoft tissue swelling, inflammation, or restriction”(American Physical Therapy Association, 2014).Prevailing thoughts on the mechanisms of manual ther-apy propose a mix of three mechanisms—biomechani-cal, neurophysiological, and/or placebo effects (Bialoskyet al, 2009; Bialosky, Bishop, George, and Robinson,2011; Bishop, Bialosky, and Cleland, 2011). It is sug-gested that a transient, mechanical stimulus (spinalmanipulation) may create a chain of local biomechani-cal effects and neurophysiological effects mediatedthrough the peripheral nervous system, spinal cord,and higher centers. Traditionally, manual therapy inter-ventions are thought to be dependent upon bottom-up-mediated factors like stimulus intensity, but in recentyears greater attention has been drawn to top-down-mediated factors like the patient’s expectations(Gifford, 2013; Tiemann et al, 2015).
If we take the case of a patient with low back painreceiving a manual therapy intervention to their lumbarspine, the mechanical stimulus is theorized to causemovement at the spinal motion segments, which mayimprove segmental motion, decrease local tissue inflam-matory factors, and facilitate local muscular control(Colloca et al, 2006; Hsieh et al, 1995; Teodorczyk-Injeyan, Injeyan, and Ruegg, 2006). Providing jointmobilization to the lumbar spine can be viewed as a“bottom-up” approach because the therapist can besaid to be providing input into the nervous system inorder to change output from the brain (i.e., pain). Inother words, the therapist’s intent is to decrease noci-ceptive input into the system and thereby modulate thepain experience. But we should also consider the “top-down” effects, i.e., the brain and its integral role inproducing a pain experience (Figure 1).
There is very little evidence that manual therapyperformed under anesthesia is effective for CLBP(Digiorgi, 2013; Gordon, Cremata, and Hawk, 2014)and perhaps this is because we need to “manipulate”the brain, and not just the joints and other peripheraltissues, to bring about a change in the pain experience.Traditional thoughts about the mechanisms underlyingmanual therapy have alluded to the gate control theoryof pain (Nathan, 1976), whereby one sensory modality(joint mobilization) can modulate another (back pain).Additionally, the provision of rhythmic oscillations tolumbar motion segments in varying grades of depth can
PHYSIOTHERAPY THEORY AND PRACTICE 409
Dow
nloa
ded
by [
Uni
vers
ity o
f N
evad
a L
as V
egas
], [
Dr
Em
ilio
Puen
tedu
ra]
at 0
7:42
12
July
201
6

also be seen as graded exposure; however, these con-cepts fail to consider the importance of the patient’sbrain’s interpretation of the input and the changes thatmight be induced through the input of manual therapy.
Manipulating the brain
Enhancing patient expectations
There is ample evidence linking patients’ expectancies forrecovery and health outcomes (Auer et al, 2016; Iles,Davidson, Taylor, and O’Halloran, 2009). A patient thatexpects a particular treatment will help their pain is morelikely to experience improvement than a patient with lowerexpectations (Bishop, Bialosky, and Cleland, 2011;Puentedura et al, 2012). The positive expectation of benefitfrom a particular treatment intervention is often termedthe placebo effect or placebo response (Benedetti, 2013;Bialosky, Bishop, George, and Robinson, 2011). A morenuanced view of placebo is that it represents the limit pointof our current understanding of the mechanisms behindthe observed treatment effect. Thus, many factors maycontribute to the placebo response, such as the patient–therapist relationship, the patient’s expectations and needs,the patient’s personality and psychological state, the sever-ity and discomfort of the symptoms, the type of verbalinstructions, the treatment preparation characteristics, andthe clinical environmental milieu (Ross and Buckalew,1985). This suggests that whenever a treatment is given toa patient, it is not done so in a vacuum, but in a complex setof psychological states that vary from patient to patient andfrom situation to situation (Benedetti and Amanzio, 2013).That is, “placebo” treatment is not necessarily “no treat-ment” or a true control.
When manual therapy is provided to a patient withCLBP, it is administered along with a complex set ofphysical and psychological stimuli (including, but notlimited to tactile, verbal and non-verbal cues) whichimply to the patient that a clinical improvement shouldbe occurring shortly. These physical and psychosocialstimuli represent the context around the therapy andthe patient, and such a context may be as important asthe specific effect of the intervention. The contextualfactors that might affect the therapeutic outcome can berepresented by the characteristics of the treatment (handcontact, direction of movement, force), the patient’s andtherapist’s characteristics (treatment and pain beliefs, sta-tus, gender), the patient–provider relationship (sugges-tion, reassurance, and compassion), and the healthcaresetting (clinic and room layout) (Di Blasi et al, 2001).
An argument could be made that when a patientwith CLBP consults a manual therapist, they wouldexpect their painful area (back) to be touched/pal-pated/treated. Adopting a “hands off” PNE approachmay not necessarily meet those expectations and couldarguably induce a nocebo effect, thereby inducing nega-tive expectations and negative outcomes (Benedetti,2013). Do expert manual therapists enhance the posi-tive recovery expectations of their patients, either con-sciously or not? A study which examined thecharacteristics of 12 therapists who were classified aseither “expert” or “average,” based on the outcomes oftheir patients, found that the “expert” therapists wherenot distinguished by years of experience (Resnik andJensen, 2003). Instead, “expert” therapists had apatient-centered approach to care, characterized bycollaborative clinical reasoning and promotion ofpatient empowerment (Resnik and Hart, 2003; Resnik
Figure 1. Bottom-up-mediated factors (left) involve application of manual therapy interventions to the tissues in the context of theenvironment, whereas top-down-mediated factors (right) involve the patient’s thoughts, beliefs, and expectations (cognitions) abouttheir pain experience and the therapy interventions provided.
410 E. J. PUENTEDURA AND T. FLYNN
Dow
nloa
ded
by [
Uni
vers
ity o
f N
evad
a L
as V
egas
], [
Dr
Em
ilio
Puen
tedu
ra]
at 0
7:42
12
July
201
6

and Jensen, 2003). In other words, they showed theyreally cared about their patients; they listened to them,they empathized, and they worked with them to achievegoals set by their patients. Expert manual therapistsdemonstrate confidence in their manual skills andwhen observed performing manual therapy, they arewell-balanced, smooth in their movements, quick tolocalize treatment levels, and gentle in their deliveryof manual therapy techniques (Edwards et al, 2004;Hartman, 2014; Resnik and Hart, 2003; Wainwright,Shepard, Harman, and Stephens, 2011).
Somatosensory cortex—manual therapy as ameans to refresh body schema maps
There are many terms that define how the brain recog-nizes the self as “self.” These include body schema,image, identity, ownership, awareness, self-perception,etc. (Holmes and Spence, 2004; Makin, Holmes, andEhrsson, 2008), and these terms are often used in dis-tinct ways by different disciplines. Neurologist SirHenry Head (1861–1940) conducted pioneering workinto the somatosensory system (Head, 1920) andcoined the term “body schema” as the brain’s dynamicrepresentation of the body which is sculpted by exter-oceptive and interoceptive experiences. But it wasWilder Penfield (1891–1976) who is credited withestablishing the “map” of the human body (homuncu-lus) in the sensory and motor cortices (Penfield andRasmussen, 1950). Current evidence suggests that theserepresentational body maps are dynamically main-tained in the brain (e.g., neuroplasticity) and are nega-tively influenced by neglect, decreased movement, andpain (Maihöfner, Handwerker, Neundörfer, andBirklein, 2003).
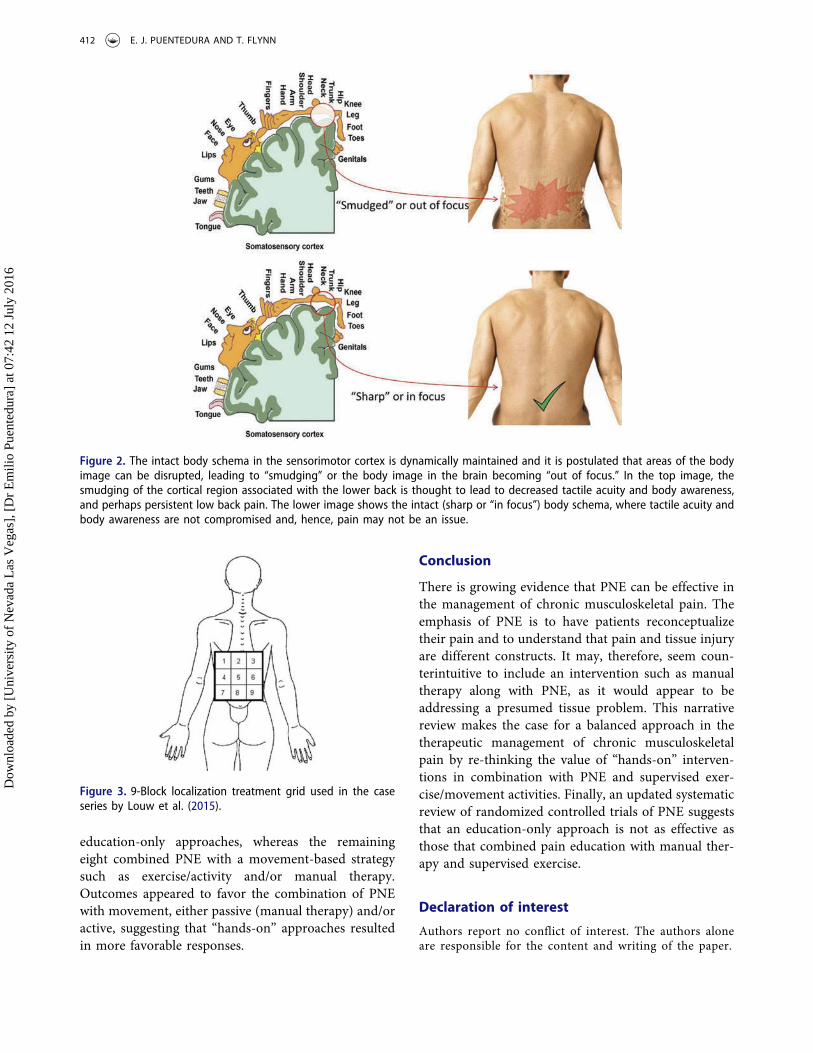
Recent research has shown that people withchronic pain demonstrate impairments in lateralityjudgements (identifying a body part as being orientedto the left or right), which is considered dependenton an intact body schema in the sensorimotor areasof the cortex (Bowering, Butler, Fulton, and Moseley,2014; Bray and Moseley, 2011; Elsig et al, 2014;Moseley, 2004b). Furthermore, body image is dis-rupted, and tactile acuity is decreased in the area ofusual pain in patients with CLBP (Moseley, 2008).This phenomenon has been referred to as “smudging”of the sensorimotor homunculus (Louw andPuentedura, 2013), and it is thought that retraininglaterality and tactile discrimination can “sharpen” or“refocus” the homunculus and lead to decreased pain(Moseley and Wiech, 2009; Moseley, Zalucki, andWiech, 2008) (Figure 2).
Getting patients with CLBP to make judgmentsabout which direction a trunk is facing in multipleimages, and having them localize light touch sensationsin discrete sections of their low back can be seen as a“top-down” approach. An argument could also bemade that the skillful delivery of manual therapy tothe low back motion segments, as long as they do notevoke a pain response, can assist in re-establishingtactile discrimination (e.g., assist in “localization” ofthe spinal motion segment) and thereby “sharpen” or“refocus” the homunculus related to the low back.Consider that the skillful delivery of manual therapyinvolves constant communication between the patientand therapist—“how does this feel here?”; “this is yourL4 spinous process”; “what if I push it this way?”; “howabout here at L5?”. It could be argued that the applica-tion of manual therapy in such a manner could linksensory and proprioceptive neural circuits within thebrain and help to refresh its representational bodymaps.
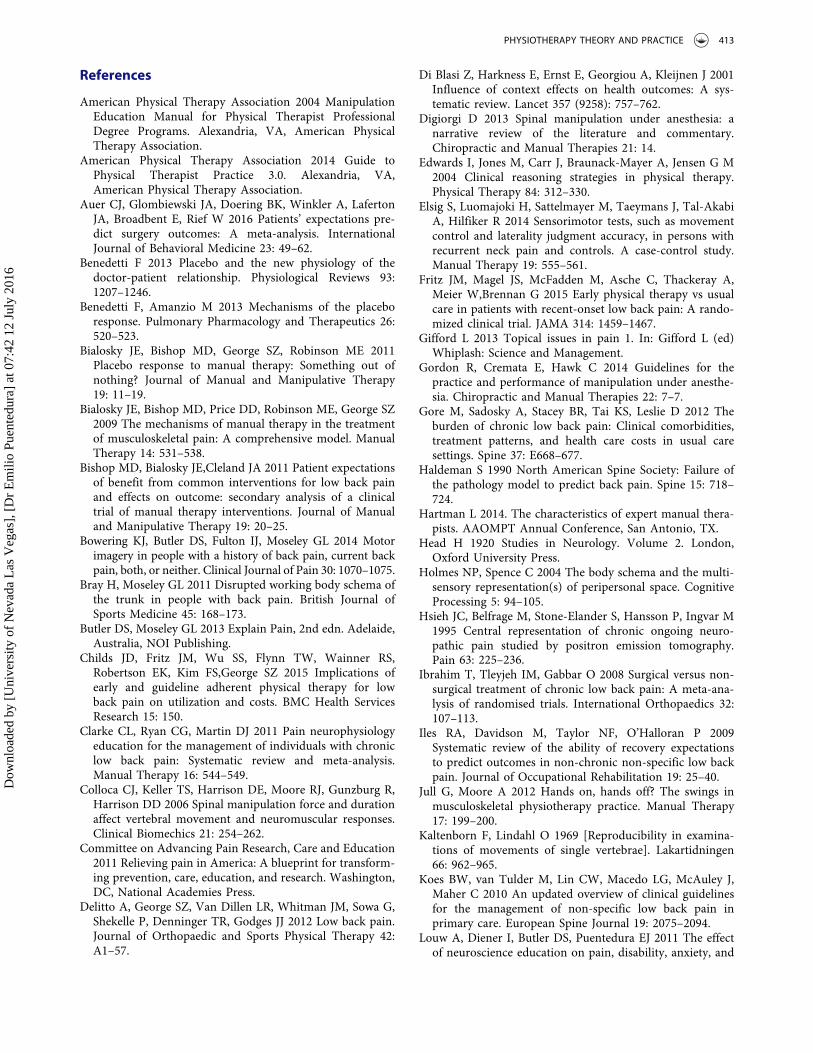
In a recent case series (Louw et al, 2015), researchersreported that a brief tactile intervention associated withbrain remapping resulted in immediate improvements inpain and spinal flexion range in 16 patients with CLBP.Patients were shown a picture of the homunculus andtold that it was a map of their body’s representation inthe brain. They were also taught that when persistentpain is present, the map can become “less sharp” asthose body parts are moved and used less, and thatsharpening or refocusing the map could reduce theirpain. By touching the back in various areas and sharpen-ing their attention to where they were being touchedwith a pen, the therapy would aim to “sharpen” the map.They used a 9-block grid and randomly stimulated the 9-blocks while asking for continuous feedback as to thelocalization of the stimulus (Figure 3) and found thatmean pain rating (0–10 scale) decreased by 1.91 (range0–6) and forward flexion improved by a mean of4.82 cm (range –1 to 21). The study demonstrated thatan intervention “devoid of physical movement and asso-ciated with cortical reorganization” (Louw et al, 2015)could decrease pain and cause an immediate increase inlumbar flexion range in patients with CLBP.
Emerging evidence suggests coupling PNE andmovement therapies
Finally, the systematic review of the efficacy of PNE forpain, function, disability, psychosocial factors, move-ment, and healthcare utilization in individuals withchronic musculoskeletal pain was recently updated(Louw, Zimney, Puentedura, and Diener, 2016). Intheir review of 13 studies, the authors found five were
PHYSIOTHERAPY THEORY AND PRACTICE 411
Dow
nloa
ded
by [
Uni
vers
ity o
f N
evad
a L
as V
egas
], [
Dr
Em
ilio
Puen
tedu
ra]
at 0
7:42
12
July
201
6
education-only approaches, whereas the remainingeight combined PNE with a movement-based strategysuch as exercise/activity and/or manual therapy.Outcomes appeared to favor the combination of PNEwith movement, either passive (manual therapy) and/oractive, suggesting that “hands-on” approaches resultedin more favorable responses.
Conclusion
There is growing evidence that PNE can be effective inthe management of chronic musculoskeletal pain. Theemphasis of PNE is to have patients reconceptualizetheir pain and to understand that pain and tissue injuryare different constructs. It may, therefore, seem coun-terintuitive to include an intervention such as manualtherapy along with PNE, as it would appear to beaddressing a presumed tissue problem. This narrativereview makes the case for a balanced approach in thetherapeutic management of chronic musculoskeletalpain by re-thinking the value of “hands-on” interven-tions in combination with PNE and supervised exer-cise/movement activities. Finally, an updated systematicreview of randomized controlled trials of PNE suggeststhat an education-only approach is not as effective asthose that combined pain education with manual ther-apy and supervised exercise.
Declaration of interest
Authors report no conflict of interest. The authors aloneare responsible for the content and writing of the paper.
Figure 2. The intact body schema in the sensorimotor cortex is dynamically maintained and it is postulated that areas of the bodyimage can be disrupted, leading to “smudging” or the body image in the brain becoming “out of focus.” In the top image, thesmudging of the cortical region associated with the lower back is thought to lead to decreased tactile acuity and body awareness,and perhaps persistent low back pain. The lower image shows the intact (sharp or “in focus”) body schema, where tactile acuity andbody awareness are not compromised and, hence, pain may not be an issue.
Figure 3. 9-Block localization treatment grid used in the caseseries by Louw et al. (2015).
412 E. J. PUENTEDURA AND T. FLYNN
Dow
nloa
ded
by [
Uni
vers
ity o
f N
evad
a L
as V
egas
], [
Dr
Em
ilio
Puen
tedu
ra]
at 0
7:42
12
July
201
6
References
American Physical Therapy Association 2004 ManipulationEducation Manual for Physical Therapist ProfessionalDegree Programs. Alexandria, VA, American PhysicalTherapy Association.
American Physical Therapy Association 2014 Guide toPhysical Therapist Practice 3.0. Alexandria, VA,American Physical Therapy Association.
Auer CJ, Glombiewski JA, Doering BK, Winkler A, LafertonJA, Broadbent E, Rief W 2016 Patients’ expectations pre-dict surgery outcomes: A meta-analysis. InternationalJournal of Behavioral Medicine 23: 49–62.
Benedetti F 2013 Placebo and the new physiology of thedoctor-patient relationship. Physiological Reviews 93:1207–1246.
Benedetti F, Amanzio M 2013 Mechanisms of the placeboresponse. Pulmonary Pharmacology and Therapeutics 26:520–523.
Bialosky JE, Bishop MD, George SZ, Robinson ME 2011Placebo response to manual therapy: Something out ofnothing? Journal of Manual and Manipulative Therapy19: 11–19.
Bialosky JE, Bishop MD, Price DD, Robinson ME, George SZ2009 The mechanisms of manual therapy in the treatmentof musculoskeletal pain: A comprehensive model. ManualTherapy 14: 531–538.
Bishop MD, Bialosky JE,Cleland JA 2011 Patient expectationsof benefit from common interventions for low back painand effects on outcome: secondary analysis of a clinicaltrial of manual therapy interventions. Journal of Manualand Manipulative Therapy 19: 20–25.
Bowering KJ, Butler DS, Fulton IJ, Moseley GL 2014 Motorimagery in people with a history of back pain, current backpain, both, or neither. Clinical Journal of Pain 30: 1070–1075.
Bray H, Moseley GL 2011 Disrupted working body schema ofthe trunk in people with back pain. British Journal ofSports Medicine 45: 168–173.
Butler DS, Moseley GL 2013 Explain Pain, 2nd edn. Adelaide,Australia, NOI Publishing.
Childs JD, Fritz JM, Wu SS, Flynn TW, Wainner RS,Robertson EK, Kim FS,George SZ 2015 Implications ofearly and guideline adherent physical therapy for lowback pain on utilization and costs. BMC Health ServicesResearch 15: 150.
Clarke CL, Ryan CG, Martin DJ 2011 Pain neurophysiologyeducation for the management of individuals with chroniclow back pain: Systematic review and meta-analysis.Manual Therapy 16: 544–549.
Colloca CJ, Keller TS, Harrison DE, Moore RJ, Gunzburg R,Harrison DD 2006 Spinal manipulation force and durationaffect vertebral movement and neuromuscular responses.Clinical Biomechics 21: 254–262.
Committee on Advancing Pain Research, Care and Education2011 Relieving pain in America: A blueprint for transform-ing prevention, care, education, and research. Washington,DC, National Academies Press.
Delitto A, George SZ, Van Dillen LR, Whitman JM, Sowa G,Shekelle P, Denninger TR, Godges JJ 2012 Low back pain.Journal of Orthopaedic and Sports Physical Therapy 42:A1–57.
Di Blasi Z, Harkness E, Ernst E, Georgiou A, Kleijnen J 2001Influence of context effects on health outcomes: A sys-tematic review. Lancet 357 (9258): 757–762.
Digiorgi D 2013 Spinal manipulation under anesthesia: anarrative review of the literature and commentary.Chiropractic and Manual Therapies 21: 14.
Edwards I, Jones M, Carr J, Braunack-Mayer A, Jensen G M2004 Clinical reasoning strategies in physical therapy.Physical Therapy 84: 312–330.
Elsig S, Luomajoki H, Sattelmayer M, Taeymans J, Tal-AkabiA, Hilfiker R 2014 Sensorimotor tests, such as movementcontrol and laterality judgment accuracy, in persons withrecurrent neck pain and controls. A case-control study.Manual Therapy 19: 555–561.
Fritz JM, Magel JS, McFadden M, Asche C, Thackeray A,Meier W,Brennan G 2015 Early physical therapy vs usualcare in patients with recent-onset low back pain: A rando-mized clinical trial. JAMA 314: 1459–1467.
Gifford L 2013 Topical issues in pain 1. In: Gifford L (ed)Whiplash: Science and Management.
Gordon R, Cremata E, Hawk C 2014 Guidelines for thepractice and performance of manipulation under anesthe-sia. Chiropractic and Manual Therapies 22: 7–7.
Gore M, Sadosky A, Stacey BR, Tai KS, Leslie D 2012 Theburden of chronic low back pain: Clinical comorbidities,treatment patterns, and health care costs in usual caresettings. Spine 37: E668–677.
Haldeman S 1990 North American Spine Society: Failure ofthe pathology model to predict back pain. Spine 15: 718–724.
Hartman L 2014. The characteristics of expert manual thera-pists. AAOMPT Annual Conference, San Antonio, TX.
Head H 1920 Studies in Neurology. Volume 2. London,Oxford University Press.
Holmes NP, Spence C 2004 The body schema and the multi-sensory representation(s) of peripersonal space. CognitiveProcessing 5: 94–105.
Hsieh JC, Belfrage M, Stone-Elander S, Hansson P, Ingvar M1995 Central representation of chronic ongoing neuro-pathic pain studied by positron emission tomography.Pain 63: 225–236.
Ibrahim T, Tleyjeh IM, Gabbar O 2008 Surgical versus non-surgical treatment of chronic low back pain: A meta-ana-lysis of randomised trials. International Orthopaedics 32:107–113.
Iles RA, Davidson M, Taylor NF, O’Halloran P 2009Systematic review of the ability of recovery expectationsto predict outcomes in non-chronic non-specific low backpain. Journal of Occupational Rehabilitation 19: 25–40.
Jull G, Moore A 2012 Hands on, hands off? The swings inmusculoskeletal physiotherapy practice. Manual Therapy17: 199–200.
Kaltenborn F, Lindahl O 1969 [Reproducibility in examina-tions of movements of single vertebrae]. Lakartidningen66: 962–965.
Koes BW, van Tulder M, Lin CW, Macedo LG, McAuley J,Maher C 2010 An updated overview of clinical guidelinesfor the management of non-specific low back pain inprimary care. European Spine Journal 19: 2075–2094.
Louw A, Diener I, Butler DS, Puentedura EJ 2011 The effectof neuroscience education on pain, disability, anxiety, and
PHYSIOTHERAPY THEORY AND PRACTICE 413
Dow
nloa
ded
by [
Uni
vers
ity o
f N
evad
a L
as V
egas
], [
Dr
Em
ilio
Puen
tedu
ra]
at 0
7:42
12
July
201
6
stress in chronic musculoskeletal pain. Archives of PhysicalMedicine and Rehabilitation 92: 2041–2056.
Louw A, Farrell K, Wettach L, Uhl J, Majkowski K, WedlingM 2015 Immediate effects of sensory discrimination forchronic low back pain: A case series. New Zealand Journalof Physiotherapy 43(2): 58–63.
Louw A, Puentedura EJ 2013 Therapeutic NeuroscienceEducation: Teaching Patients about Pain. Minneapolis,MN, OPTP.
Louw A, Zimney K, Puentedura EJ, Diener I 2016 The effi-cacy of pain neuroscience education on musculoskeletalpain: A systematic review of the literature. PhysiotherapyTheory and Practice 32: 332–355.
Maihöfner C, Handwerker HO, Neundörfer B, Birklein F2003 Patterns of cortical reorganization in complex regio-nal pain syndrome. Neurology 61: 1707–1715.
Maitland GD 1973 The treatment of joints by passive move-ment. Australian Journal of Physiotherapy 19: 65–72.
Makin TR, Holmes NP, Ehrsson HH 2008 On the otherhand: Dummy hands and peripersonal space. BehavioralBrain Research 191: 1–10.
Melloh M, Roder C, Elfering A, Theis JC, Muller U, Staub LP,Aghayev E, Zweig T, Barz T, Kohlmann T, Wieser S, JuniP, Zwahlen M 2008 Differences across health care systemsin outcome and cost-utility of surgical and conservativetreatment of chronic low back pain: A study protocol.BMC Musculoskeletal Disorders 9: 81.
Moseley GL 2002 Combined physiotherapy and education isefficacious for chronic low back pain. Australian Journal ofPhysiotherapy 48: 297–302.
Moseley GL 2003a Joining forces – combining cognition-targeted motor control training with group or individualpain physiology education: A successful treatment forchronic low back pain. Journal of Manual andManipulative Therapy 11: 88–94.
Moseley GL 2003b Unraveling the barriers to reconceptuali-zation of the problem in chronic pain: The actual andperceived ability of patients and health professionals tounderstand the neurophysiology. Journal of Pain 4: 184–189.
Moseley GL 2004a Evidence for a direct relationship betweencognitive and physical change during an education inter-vention in people with chronic low back pain. EuropeanJournal of Pain 8: 39–45.
Moseley GL 2004b Why do people with complex regionalpain syndrome take longer to recognize their affectedhand? Neurology 62: 2182–2186.
Moseley GL 2005 Widespread brain activity during anabdominal task markedly reduced after pain physiologyeducation: fMRI evaluation of a single patient with chroniclow back pain. Australian Journal of Physiotherapy 51: 49–52.
Moseley GL 2008 I can’t find it! Distorted body image andtactile dysfunction in patients with chronic back pain. Pain140: 239–243.
Moseley GL, Nicholas MK, Hodges PW 2004 A randomizedcontrolled trial of intensive neurophysiology education inchronic low back pain. Clinical Journal of Pain 20: 324–330.
Moseley GL, Wiech K 2009 The effect of tactile discrimina-tion training is enhanced when patients watch the reflectedimage of their unaffected limb during training. Pain 144:314–319.
Moseley GL, Zalucki NM, Wiech K 2008 Tactile discrimina-tion, but not tactile stimulation alone, reduces chroniclimb pain. Pain 137: 600–608.
Nathan P W 1976 The gate-control theory of pain. A criticalreview. Brain 99: 123–158.
Nijs J, Roussel N, Paul van Wilgen C, Koke A, Smeets R 2013Thinking beyond muscles and joints: Therapists’ andpatients’ attitudes and beliefs regarding chronic musculos-keletal pain are key to applying effective treatment. ManualTherapy 18: 96–102.
Penfield W, Rasmussen TL 1950 The Cerebral Cortex ofMan: A Clinical Study of Locailization of Function. NewYork, Macmillan.
Puentedura EJ, Cleland JA, Landers MR, Mintken PE, LouwA, Fernandez-de-Las-Penas C 2012 Development of a clin-ical prediction rule to identify patients with neck painlikely to benefit from thrust joint manipulation to thecervical spine. Journal of Orthopaedic and SportsPhysical Therapy 42: 577–592.
Puentedura EJ, Louw A 2012 A neuroscience approach tomanaging athletes with low back pain. Physical Therapy inSport 13: 123–133.
Resnik L, Hart DL 2003 Using clinical outcomes to identifyexpert physical therapists. Physical Therapy 83: 990–1002.
Resnik L, Jensen GM 2003 Using clinical outcomes to explorethe theory of expert practice in physical therapy. PhysicalTherapy 83: 1090–1106.
Rhon D, Fritz J 2015 Comparative early treatment effective-ness between physical therapy and usual care for low backpain (COMPETE): study protocol for a randomized con-trolled trial. Trials 16: 423.
Ross S, Buckalew LW 1985 Placebo agentry: Assessment ofdrug and placebo effects. In: White L, Tursky B, SchwartzGE (eds) Placebo: Theory, Research, and Mechanisms, pp67–82. New York, Guilford.
Rubinstein SM, van Middelkoop M, Assendelft WJ, de BoerMR, van Tulder MW 2011 Spinal manipulative therapy forchronic low-back pain. The Cochrane Database ofSystematic Reviews (2): CD008112.
Spitzer W 1987 Scientific approach to the assessment andmanagement of activity-related spinal disorders. A mono-graph for clinicians. Report of the Quebec Task Force onSpinal Disorders. Spine 12 (7 Suppl): S1–59.
Teodorczyk-Injeyan JA, Injeyan HS, Ruegg R 2006 Spinalmanipulative therapy reduces inflammatory cytokines butnot substance P production in normal subjects. Journal ofManipulative and Physiological Therapeutics 29: 14–21.
Tiemann L, May ES, Postorino M, Schulz E, Nickel MM,Bingel U, Ploner M 2015 Differential neurophysiologicalcorrelates of bottom-up and top-down modulations ofpain. Pain 156: 289–296.
Wainwright SF, Shepard KF, Harman LB,Stephens J 2011Factors that influence the clinical decision making ofnovice and experienced physical therapists. PhysicalTherapy 91: 87–101.
414 E. J. PUENTEDURA AND T. FLYNN
Dow
nloa
ded
by [
Uni
vers
ity o
f N
evad
a L
as V
egas
], [
Dr
Em
ilio
Puen
tedu
ra]
at 0
7:42
12
July
201
6